
Abstract
Introduction:
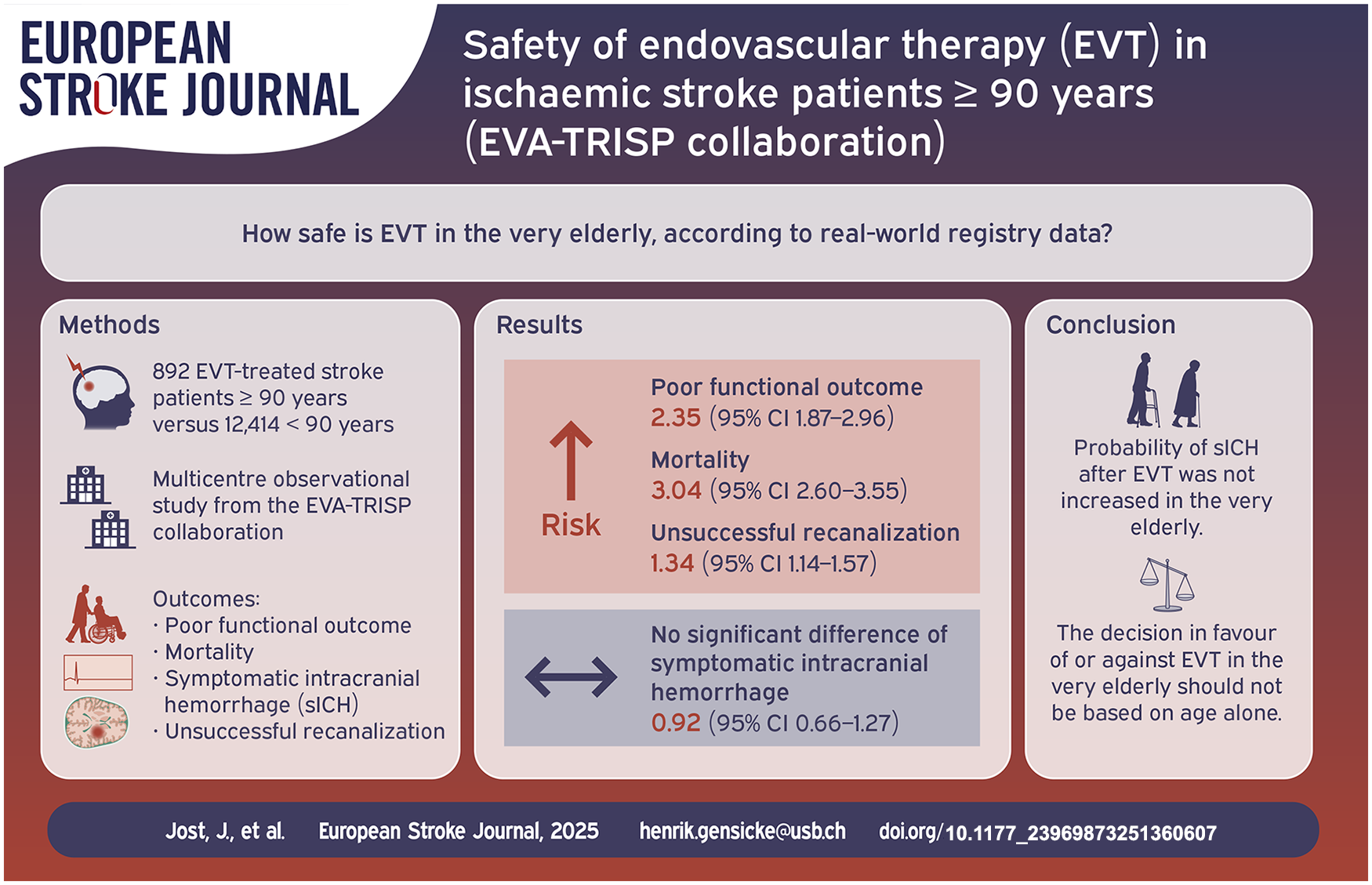
Data on safety of endovascular therapy (EVT) in the very elderly are scarce. Using data from a large prospective EVT registry, we aimed at providing better evidence for EVT decision-making in patients aged 90 years and older.
Patients and methods:
In this multicentre observational study from the EVA-TRISP collaboration outcomes were compared between patients aged ⩾90 years with those aged <90 years using multivariate logistic regression analysis and reporting odds ratios and 95% confidence intervals. Outcomes were occurrence of poor functional outcome in survivors (modified Rankin Scale (mRS) 3–5 if pre-stroke mRS 0–2 and mRS higher than pre-stroke mRS if pre-stroke mRS 3–5), mortality at 3 months after stroke, unsuccessful recanalization (mTICI 0–2a) and symptomatic intracranial hemorrhage (sICH, defined by ECASS-II-/III-criteria).
Results:
Of 13,306 eligible patients, 892 were ⩾90 years old (6.7%). The very elderly had a higher median National Institutes of Health Stroke Scale (NIHSS) on admission (16 vs 14) and were more likely to have a pre-stroke mRS of 3–5 (38.0% vs 8.7%). The odds of poor functional outcome (ORadjusted 2.35 (95%-CI 1.87–2.97); 61.6% vs 38.7%), death (ORadjusted 3.04 (95%-CI 2.60–3.55); 53.9% vs 21.3%) and unsuccessful recanalization (ORadjusted 1.34 (95%-CI 1.14–1.57); 32.4% vs 27.2%) were higher in patients aged ⩾90 years. The odds of sICH did not differ (ORadjusted 0.92 (95%-CI 0.66–1.28); 5.1% vs 5.0%).
Discussion and conclusion:
EVT-treated stroke patients ⩾90 years had higher odds of poor functional outcome, mortality and unsuccessful recanalization than younger patients. However, the probability of sICH after EVT was not increased. The decision in favor of or against EVT in the very elderly should not be based on age alone.
Introduction
Endovascular therapy (EVT) has changed the clinical outcome of patients with acute ischemic stroke due to large vessel occlusion (LVO). Multiple randomized controlled trials (RCTs)1–7 have shown a beneficial effect of EVT on functional outcome (measured by the modified Rankin Scale, mRS) 90 days after stroke onset. However, data from RCTs on EVT-treated patients are limited, with only 91 patients aged ⩾80 years in the RCTs pooled in HERMES 8 and only 42 patients aged ⩾85 years in a HERMES substudy. 9 Older age was an exclusion criterion in several RCTs2,5,7 probably due to the assumed higher rate of intracranial hemorrhage. 10 To date, there are no data from RCTs on EVT in nonagenarians. Another important limitation of RCTs on EVT in the elderly is that patients with relevant pre-stroke disability were excluded from all except one RCT (MR CLEAN). 1 However, pre-stroke disability is frequent in the elderly stroke population (25%–50% of patients). 11 Data on safety of EVT in nonagenarians consists mainly of observational studies with small sample sizes ranging from 18 to 203 patients ⩾90 years and two meta-analyses. The studies were heterogeneous in regard to the comparison groups and outcomes.12–25 Therefore, despite those studies, age remained one of the most relevant factors for withholding EVT in daily routine in a 2019 survey 26 and there is no consensus on the decision-making process of performing EVT in patients aged ⩾90 years.
The aim of our study was to explore the safety of EVT in patients aged ⩾90 years with an acute ischemic stroke due to a LVO in a large real-world population (using data from the EVA-TRISP collaboration).
Methods
For this study, we used prospectively collected data from 16 centers of the EndoVAscular treatment and ThRombolysis for Ischemic Stroke Patients (EVA-TRISP) collaboration (Supplemental Table S1). EVA-TRISP is an academic multicentre international collaboration with a defined structure, processes and methodology to generate a pooled data registry based on data provided by each participating center. 27 As done in previous analyses of the database,28,29 data for the following variables were used: patient demographics (age, sex, baseline-independency (mRS 0–2), 30 and baseline mRS), stroke characteristics (National Institutes of Health Stroke Scale (NIHSS) on admission, 31 territory of stroke (anterior, posterior or both), occluded vessel and/or segment (internal carotid artery, medial cerebral artery M1 or M2, anterior cerebral artery, posterior cerebral artery, basilar artery, vertebral artery or any other occlusion), initial ASPECT score, 32 time from onset to groin or, if unknown time from last seen well to groin), treatment characteristics (use of IVT in addition to EVT (=bridging therapy), EVT complications, intraarterial thrombolysis therapy (=EVT thrombolysis), mechanical treatment (=stent retriever, aspiration, distal retriever, intracranial balloon angioplasty, permanent intracranial stent alone or in combination), use of general anesthesia, number of passes), systolic blood pressure and glucose levels at admission, medical history 33 (previous ischemic stroke, coronary artery disease, atrial fibrillation, diabetes mellitus, hypertension, hypercholesterolemia, smoking status (active or stopped less than 2 years ago), prior platelet aggregation inhibition, prior oral anticoagulation) and stroke etiology according to Trial of Org 10,172 in Acute Stroke Treatment (TOAST) 34 criteria.
Outcomes were poor functional outcome in survivors (up to mRS 5), death (mRS 6) at 3 months after stroke onset, unsuccessful recanalization and symptomatic intracranial hemorrhage (sICH). Poor functional outcome, or the level of disability after stroke, was expressed by the mRS and defined as: a mRS score of 3–5 for patients who had a pre-stroke mRS 0–2 or a mRS higher than the pre-stroke mRS for patients with a pre-stroke mRS 3-5.35,36 Post-stroke mRS score was assessed at 3 months via outpatient consultations or telephone calls with patients and/or relatives. As different definitions of poor outcome are common, we also analyzed a simpler but often used alternative definition (poor outcome = mRS 3–6, including deceased patients) as a secondary outcome. sICH was defined, using the European Cooperative Acute Stroke Study (ECASS) II and III criteria, as extravascular intracranial blood on imaging associated with clinical worsening (an increase in NIHSS of more than four points (ECASS II)) or leading to death and was considered to be the cause of clinical deterioration (ECASS III).37,38 The criteria used were those provided by the centers, which in most centers were the ECASS II criteria. If both were available, the ECASS II classification was preferred. Follow-up imaging (MRI or CT scan) was performed usually at 24 h after treatment or earlier in case of clinical worsening. 27 Unsuccessful recanalization of the occluded intracranial vessel was defined by the modified treatment in cerebral infarction (mTICI) 39 scale 0–2a. Recanalization status was assessed by digital subtraction angiography.
Data were collected from January 2015 to January 2023. Patients with missing data on age or 3-month mRS were excluded.
Statistical analyses
Statistical analyses were performed with R (Version 4.4.0) 40 and R Studio (Version 2023.12.1, build 402). 41 In addition, the following packages were used: “finalifit” and “pheatmap” for missing data pattern analysis,42,43 “mice” for the mice-imputation, 44 “MatchThem” for propensity score matching, 45 “cobalt” for propensity score diagnostics, 46 “tidyverse” for data processing. 47
We investigated the association of age with the outcomes by using age as a categorical variable, comparing patients aged ⩾90 years with those aged <90 years.
Exploratory data analysis
Continuous data were summarized using the median and interquartile range (IQR) and binary data were summarized as percentages. The Mann-Whitney U test was used to compare continuous variables and the χ2 test was used for categorical data. Both raw and adjusted p-values (Bonferroni’s method) are reported. No formal p-value cut-off was defined to assume statistical significance, instead effect sizes and p-values are discussed.
Data cleaning and missing data imputation
The absolute and relative numbers of missing data are reported for all baseline characteristics and outcome variables. We performed limited data cleaning by overwriting logically impossible values and extremely implausible values as missing values (“NA”) as reported in the results section.
To minimize the bias caused by a complete case analysis we performed a multiple imputation by chained equations (MICE) imputation on the dataset containing all variables reported in Table 1. We followed a “multiple imputation, then delete” approach, thus we also used the rows where one or more of the four outcomes were missing for imputation, but we did not use these rows for the analysis of the missing outcomes, that is, the analysis was performed only on reported and not on imputed outcomes. This approach is robust against poor imputation of the outcome and tends to reduce variability in the analysis. 48 We imputed 100 datasets with 30 iterations per dataset. Numerical data were imputed by predictive mean matching, binary outcomes by logistic regression. All models were calculated on each imputed dataset and the results were pooled according to Rubin’s rules. 49
Baseline characteristics.

NIHSS: National Institutes of Health Stroke Scale; sICH: symptomatic intracerebral hemorrhage (according to ECASS II/III criteria).
Poor functional outcome in survivors = modified Rankin Scale 3–5 for patients with a pre-Stroke mRS 0–2 or an mRS 4–5 for those with a pre-Stroke-mRS 3–5. Alternative poor functional outcome overall = mRS 3–6. The Mann-Whitney U test was used to compare continuous variables and χ2 test was used for categorical data. Adjusted p-values are derived from Bonferronis correction applied across the complete table. Missing data are given per group (young vs old) separately.
Including strokes in both anterior and posterior territories.
Statistical modeling
The association of old age (⩾90 years) with the main outcomes was estimated by calculating odds ratios (OR) with 95% confidence intervals (95% CI), using multivariable binary logistic regression models. Models were adjusted for well-known confounders described in the literature. The models for poor outcome and death at 3 months were adjusted for NIHSS at admission,50,51 sex, 52 EVT complications, 51 unsuccessful recanalization,50,51 prestroke mRS,51,53 bridging therapy, 54 admission glucose, 55 prior atrial fibrillation, 56 prior ischemic strokes, 51 and time to groin 57 (10 covariates total). The model for sICH was adjusted for sex, 58 NIHSS at admission,51,59 EVT complications, 51 bridging therapy, 51 admission systolic blood pressure 59 and last seen well to groin time51,58,59 (six covariates total). The model for incomplete recanalization was adjusted for sex60,61, NIHSS at admission,60,61 use of general anesthesia during EVT, 62 bridging therapy,60,61 admission systolic blood pressure,60,61 prior atrial fibrillation,60,61 prior diabetes mellitus60,61 and last seen well to groin time60,61 (eight covariates total).
The main analysis is the full models using the imputed data set. The following sensitivity analyses were performed: (i) The same models were also calculated using only the complete cases to assess the bias caused by the missing data and their imputation. (ii) Using the imputed data sets, simpler models using only NIHSS on admission and the pre-stroke mRS were calculated for all four outcomes to assess the potential gain from using more complex models. (iii) Using the imputed data sets, inversed propensity score matching was performed to reduce the potential influence of between-group differences in key baseline variables on the outcome analyses. We matched patients according to their propensity to be in the old or young age group. The propensity score was based on the complex models and patients were matched in a 4:1 ratio with nearest-neighbor matching within a caliper of 0.05 standard deviations of the propensity score. We report the unadjusted and adjusted covariate balancing. We then performed unadjusted logistic regression analyses in the matched dataset to assess differences in the four outcomes. (iv) Using the imputed data set and the full models we investigated the alternative definition of poor outcome (mRS 3–6, including patients deceased within 3 months after the stroke).
The following subgroup analysis were performed for all four main outcomes using the imputed data set and the full models: (i) patients with reported ASPECT scores available adding the ASPECT score to the full models as additional independent variable, (ii) only patients aged ⩾90 years and analyzing the effects of prestroke disability (mRS 0–2 vs 3–5), site of infarction (anterior vs posterior, excluding patients with both) and stroke etiology (large artery atherosclerosis vs cardioembolic, excluding patients with any other etiology).
Furthermore, to assess an age-dependent effect, the average marginal effect was calculated for all four outcomes based on the complex models and conditioned on age groups summarized per decade.
Ethics statement and data sharing policy
The study was approved by the ethics committee in Basel, Switzerland. Each participating center additionally has received the local ethical consent in its country. Datasets generated or analyzed within the present study are available from the corresponding author upon reasonable request. In any such case, data sharing will be subject to individual patient consent processes in the participating centers. The final decision on data sharing will be made by consensus of the EVA-TRISP collaborators.
Results
Out of a total of 14,618 patients, data from 13,306 patients (91.0%) were eligible for analysis (2 (0.01%) excluded due to missing age, 1304 (8.9%) due to missing 3-month mRS, 8 (0.05%) due to being stroke mimics (Figure 1, Supplemental Table S1)). Of those, 892 patients (6.7%) were ⩾90 years of age and 12,414 (93.3%) were <90 years of age. During data cleaning, 46 data points were replaced with missing values (“NA”) due to non-meaningful values (Figure 1).
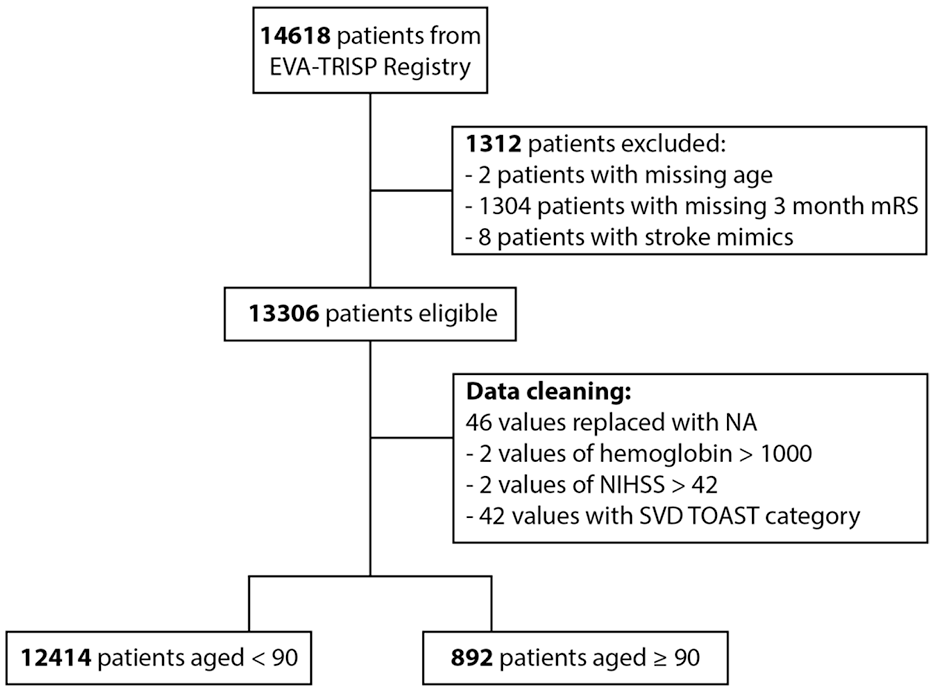
Diagram of patient in- and exclusion and data cleaning.
Baseline characteristics
In patients aged ⩾90 years, the median age was 92 years (IQR 91–94) and 73 years (IQR 63–81) in the comparison group. Patients aged ⩾90 years were more often women (68.9% vs 46.9%), more often had a pre-stroke disability (38.0% vs 8.7%), presented with a higher NIHSS on admission (median 16 (IQR 11–21) vs 14 (IQR 8–19)) and presented more often with strokes in the anterior (95.7% vs 90.6%) and less often with strokes in the posterior territories (6.5% vs 12.2%; Table 1, Supplemental Table S2A for details on stroke territories). The elderly patients had similar rates of bridging therapy, intraarterial thrombolysis, mechanical treatment, usage of general anesthesia and complications during EVT compared to the control group (Table 1, Supplemental Table S2B for details on EVT complications). The number of passes during EVT was only reported in a limited number of cases (24.3% of young and 19.5% of elderly patients) but there was no evidence of a difference between the study groups (Table 1).
Patients aged ⩾90 years presented with a slightly higher systolic blood pressure (median 159 mmHg (IQR 138–178) vs 150 mmHg (IQR 131–170)) but with similar glucose levels (Table 1).
The rate of patients with prior ischemic stroke(s) was similar in both groups (12.6% ⩾ 90 years vs 14.4%). While patients aged ⩾90 years were more likely to have a history of coronary artery disease (21.8% vs 17.2%), atrial fibrillation (61.4% vs 34.7%) and arterial hypertension (84.3% vs 67.1%), they were less likely to have diabetes mellitus (13.2% vs 19.1%) and hypercholesterolemia (41.3% vs 48.5%) and were decisively less likely to be current smokers (1.7% vs 20.8%). Patients aged ⩾90 years were more likely to receive antiplatelet therapy before the index stroke (38% vs 28.3%) while the rates of oral anticoagulation before stroke were only marginally higher in the elderly (23.2% vs 19.7%). (Table 1).
Furthermore, stroke etiologies differed between the groups with patients aged ⩾90 years more likely to have cardioembolic strokes (64.9% vs 43%) and less likely to have large artery atherosclerosis (11.0% vs 19.8%; Table 1).
Regarding the main outcomes, there was strong evidence that patients aged ⩾90 years had higher frequencies of poor outcome at 3 months in survivors (61.6% vs 38.7%) and death at 3 months (53.9% vs 21.3%). Also, the alternative definition of poor functional outcome (mRS 3–6, including deceased patients) was more often in elderly patients (88.4% vs 54%). There was weak evidence for a higher rate of unsuccessful recanalization in the elderly (32.4% vs 27.2%) while the rate of sICH did not differ between the two groups (5.1% vs 5.0%; Table 1).
The distribution of the mRS at baseline and after 3 months in patients ⩾90 years and <90 years is illustrated in Supplemental Figure S1.
Missing data and multiple imputation
Over all data given in Table 1, only 10.8% of data was missing (i.e. 89.2% data completeness). This was mainly caused by variables not reported by all centers. The most relevant variables with considerable proportion of missing data were ASPECT score (54.7% missing data) and recanalization status (21.1%). Other variables were territory of infarction (20.0%), EVT complications (31.4%), number of passes (76.00%), coronary artery disease (9.5%) and the TOAST categories (7.6%). Without these variables, only 4.1% of the data was missing (i.e. 95.9% data completeness). The main source of missing data was non-reporting by specific centers, and we therefore assumed that the missing data was missing at random. We calculated the multiple imputations using chained equations with 100 imputations with 30 iterations.
Multivariable logistic regression models
Using the imputed datasets and the covariates described above we calculated binary logistic regression models. This revealed a larger risk for poor outcome in survivors (OR = 2.35; 95%-CI 1.87–2.97, p < 0.001), death (OR = 3.04; 95%-CI 2.60–3.55, p < 0.001) and unsuccessful recanalization (OR = 1.34; 95%-CI 1.14–1.57, p < 0.001) in patients aged ⩾90 years compared to patients aged <90 years (Figure 2). There was no difference in the rate of sICH (OR = 0.92; 95%-CI 0.66–1.28, p = 0.618; Figure 2). The full model results showing all variables are presented in Supplemental Table S3. The strongest binary predictors of poor outcome at 3 months were unsuccessful recanalization (OR = 2.13; 95%-CI 1.9–2.4, p < 0.001) and the age group. The strongest binary predictors of death at 3 months were the age group, complications during EVT (OR = 1.73 (95%-CI 1.51–1.99, p < 0.001) and unsuccessful recanalization (OR = 1.67; 95%-CI 1.5–1.86, p < 0.001). The strongest binary predictors of unsuccessful recanalization were the age group and atrial fibrillation (OR = 0.86 (95%-CI 0.79–0.95, p = 0.002). The strongest binary predictor of sICH was complications during EVT (OR = 3.47; 95%-CI 2.84–4.23, p < 0.001).

Effect of age group (old vs young) on outcomes.
Sensitivity analyzes
The following sensitivity analyzes for the main outcomes were performed: (i) complete case analysis, (ii) simpler models using only NIHSS on admission and the pre-stroke mRS as covariates and using the imputed datasets, (iii) propensity score matching (as shown in Supplemental Figure S2), and (iv) using an alternative definition of poor outcome (mRS 3–6 vs mRS 0–2). Propensity scores weighted modeling approaches were not possible due to lacking similarity of the groups. We therefore performed a propensity score matching with a ratio of 4:1. A higher ratio did not further increase the number of used cases. Matching was successful and more than 99.0% of the patients aged ⩾90 years could be matched, the remaining 1% of the elderly patients were removed from this analysis. Distribution of the unadjusted and adjusted covariates are given in the supplements (Supplemental Figure S3). All three sensitivity analyses (i–iii) supported the evidence from the main analysis above. The alternative outcome of mRS 3–6 versus mRS 0–2 revealed a higher risk in the elderly compared to the younger patients (OR = 3.90; 95%-CI 3.10–4.91, p < 0.001).
Subgroup analyzes
The ASPECT score was available in 45% of patients (n = 6033). Including the ASPECT score as a covariate in the model, the following odds ratios were calculated for poor outcome (OR 2.20, 95%-CI 1.61–3.00; p < 0.001), death (OR 3.00, 95%-CI 2.38–3.77; p < 0.001), sICH (OR 0.88, 95%-CI 0.55–1.40; p = 0.591) and unsuccessful recanalization (OR 1.35, 95%-CI 1.08–1.70; p = 0.009).
Among the elderly patients, pre-stroke dependency was associated with poor outcome in survivors but not with death, sICH and unsuccessful recanalization. There was no evidence for a difference in any of the outcomes regarding the stroke territory (anterior vs posterior circulation) or stroke etiology (cardioembolic vs large artery atherosclerosis; Supplemental Table S4).
Age varying effect on outcomes
Using the covariates of the full models above and the imputed datasets, we calculated predictive margins. We did not perform a formal test but only report a qualitative assessment of the results, which should be cautiously interpreted due to the larger confidence interval especially in the elderly patients. The risk of poor functional outcome or death increased steadily in patients with increasing age over the decades without apparently reaching a plateau effect. The probability for unsuccessful recanalization also increased with age with a seeming plateau between 60 and 89 years of age, before increasing again for patients aged ⩾90 years. The probability of sICH increased up to age 60 but visually stagnated thereafter (Figure 3).
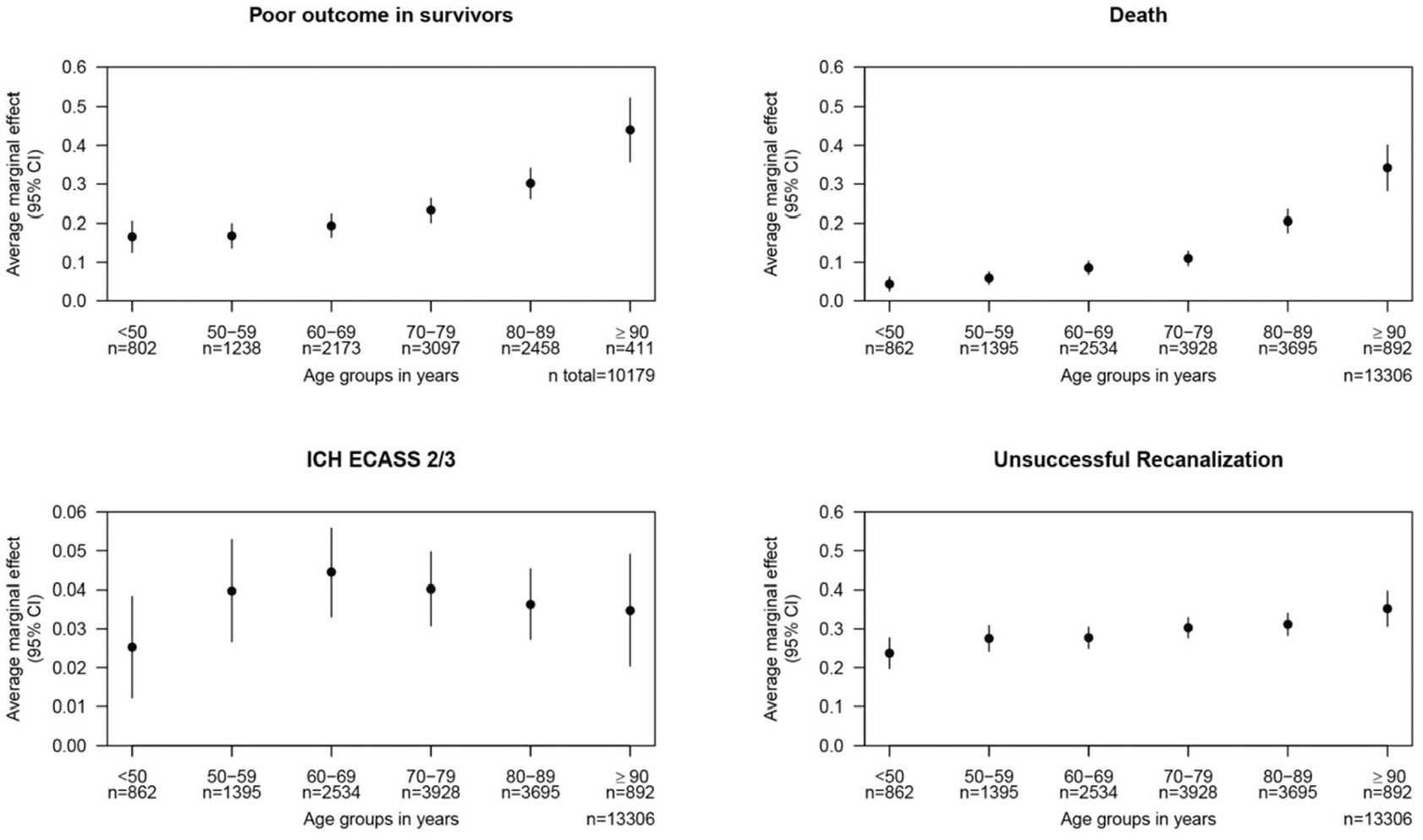
Marginal effects of age groups summarized in decades on the outcomes.
Discussion
The main findings of the current study include (1) EVT-treated stroke patients ⩾90 years had an increased probability of poor functional outcome in survivors and death within the first 3 months after stroke as well as a higher risk of unsuccessful recanalization after EVT. (2) The probability of symptomatic intracranial hemorrhage did not differ between patients aged ⩾90 years and aged <90 years.
Evidence from RCTs for benefit of EVT in the elderly is low and especially lacking for those aged ⩾90 years. Furthermore, elderly patients in RCTs likely do not represent those of the real-world because relevant pre-stroke disability had been an exclusion criterion in almost all of the trials. 11 For patients aged ⩾80 years, a HERMES subgroup analysis 8 for a mRS distribution shift at 90 days (improvement of 1 or more points) showed a treatment effect favoring EVT in patients aged ⩾80 years. Subgroup analyses for the outcomes mRS score 0–2 at 90 days and mortality also indicated a treatment effect in favor of EVT. However, no analysis was presented for sICH. 8 A more recent analysis of the HERMES collaboration 9 focused on outcomes in patients ⩾85 years (77 of 1764 patients). While the probability of poor functional outcome (mRS 5–6: 42.9% vs 74.3%) and mortality (31% vs 54.3%) at 90 days was lower in the intervention group, the frequency of sICH (7.1% vs 5.7%) was similar. Also, when comparing patients aged ⩾85 years to those aged <85 years, no significant differences in the frequency of sICH (7.1% vs 3.6%) and complete recanalization (75% vs 75.5%) were shown, although the absolute (and almost twice as large) difference in the frequency of sICH probably has clinical significance.
While the frequency of sICH in the elderly in the HERMES study was comparable to that in our study, the frequency of poor functional outcome and death was lower in HERMES. This difference is likely explained by a higher proportion of pre-stroke independent patients and younger patients (cut-off at 85 years instead of 90 years in our sample), as well as a different definition of poor functional outcome (mRS 5–6) in HERMES 9 compared to our study. Although in our study complete recanalization was less frequent in patients aged ⩾90 years compared to the younger group, rates are comparable to those in the elderly of the HERMES study (patients aged >85 years, 75%) 9 which underlines the plausibility of our data.
When comparing our results with those from other observational studies of the Endovascular Treatment in Ischemic Stroke Registry (ETIS) and German Stroke Registry–Endovascular Treatment (GSR-ET), the frequency among EVT-treated nonagenarians of poor functional outcome (mRS 3–6; 88.4% in EVA-TRISP, 87.3% in ETIS (n = 76 nonagenarians) 14 and 85.8% in GSR-ET (n = 203 nonagenarians) 15 ), death (53.9% in EVA-TRISP 46.5% in ETIS and 48.9% in GSR-ET), unsuccessful recanalization (32.4% in EVA-TRISP, 28.4% in ETIS and 24.1% in GSR-ET), and sICH (5.1% in EVA-TRISP, 6.8% in ETIS and 3% in GSR-ET) were similar but tendentially worse outcomes in EVA-TRISP. This might be explained by the large proportion of patients with pre-stroke dependency (pre-stroke mRS ⩾3) in EVA-TRISP of 38% and a median pre-stroke mRS of 2. In contrast, patients with pre-stroke dependency were excluded from the ETIS study and less frequent in the GSR-ET study (patients with pre-stroke mRS >3 were excluded and the median pre-stroke mRS was 1).
Furthermore, one meta-analysis, including 657 EVT-treated nonagenarians, found a frequency of poor functional outcome (mRS 3–6) of 78.4%, mortality of 44.4%, unsuccessful recanalization of 19.2% and sICH of 3.5%. 25 In this study, the rate of poor functional outcome and unsuccessful recanalization was lower than the rates in our study which might be explained by a higher frequency of pre-stroke independency in these studies. However, information on pre-stroke functional status was not provided by the meta-analysis.
Previously, another meta-analysis has compared outcomes of EVT-treated nonagenarians with those of younger stroke patients. 24 Poor functional outcome (mRS 3–6; 82.6%) and mortality (38.9%) at 90 days were significantly higher in nonagenarians than in younger patients but no significant differences were observed in rates of unsuccessful recanalization and sICH. However, the relevance of this study is limited by the heterogeneity among the included studies and lack on information of the pre-stroke functional status.
Our study included a large population of EVT-treated patients aged ⩾90 years (n = 892). This allowed us to better characterize this population, and show differences not only in stroke outcome, but also in pre-stroke functional status, comorbidities and stroke etiology. We found that 38% of EVT-treated patients ⩾90 years were pre-stroke functionally dependent (pre-stroke mRS >2). Furthermore, we found an approximately twofold higher incidence of atrial fibrillation, a corresponding 1.5-fold higher rate of cardioembolic stroke and furthermore, older patients were less likely to suffer from diabetes, hypercholesteremia and were less likely to be active smokers. We hypothesize that this may stem from a double selection bias: (i) The older patients in our database may have benefited from a genetic and/or environmental background to even reach such a high age and (ii) the older patients were obviously deemed fit enough to receive endovascular therapy for reasons other than their age. As our data included only patients who received endovascular therapy, we have no information for which patients it was withheld and why.
The strengths of our study are (1) the large population of EVT-treated patients aged ⩾90 years (n = 892) which allows a comprehensive adjustment for confounding parameters; (2) high data completeness (of baseline characteristics); (3) multicentre and multinational design which increases the generalizability of our results; (4) our results were robust when restricted to complete cases, when analyzed with simpler model or with IPSM or in the subgroup with ASPECT score available, which underlines the reliability of our findings.
Our study has the following limitations: (1) The data were collected in European countries and in Israel. Thus, certain risk factors may be different in other regions. (2) We do not have a control group without EVT, thus we cannot estimate the effectiveness of EVT in the very elderly. (3) Compared with RCTs, cohort studies naturally have a higher risk of bias due to the lack of randomization. Therefore, the results of our study should be interpreted with caution. (4) two different scores (ECASS II/III) were used for defining sICH, which may limit the comparability of the results somewhat. Nevertheless, the vast majority was defined by the ECASS II (96.6%) criteria. (5) Despite the overall high data completeness, some important variables (i.e. ASPECTS and status of recanalization) had a considerable proportion of missing data.
Conclusion
EVT-treated stroke patients ⩾90 years had higher odds of poor functional outcome, mortality and unsuccessful recanalization than younger patients. However, the probability of sICH after EVT was not increased. The decision in favor of or against EVT in the very elderly should not be based on age alone.
Supplemental Material
sj-docx-1-eso-10.1177_23969873251360607 – Supplemental material for Safety of endovascular therapy in ischemic stroke patients ≽90 years: A cohort study from the EVA-TRISP collaboration
Supplemental material, sj-docx-1-eso-10.1177_23969873251360607 for Safety of endovascular therapy in ischemic stroke patients ≽90 years: A cohort study from the EVA-TRISP collaboration by Jasmine Jost, Lukas Enz, Martina B Goeldlin, Philipp Baumgartner, Davide Strambo, Nabila Wali, Nicolas Martinez-Majander, Georg Kägi, Laura Vandelli, Christoph Riegler, Danna Krupka, Matteo Paolucci, Mauro Magoni, Giovanni Bianco, Hamza Jubran, Dejana R Jovanovic, Tomas Klail, Laura P Westphal, Alexander Salerno, Leon A Rinkel, Laura Mannismäki, Tolga Dittrich, Livio Picchetto, Regina von Rennenberg, Miguel Serôdio, Stefano Forlivesi, Dikran Mardighian, Carlo W Cereda, Ronen R Leker, Visnja Padjen, Mira Katan, Marios-Nikos Psychogios, Urs Fischer, Tomas Dobrocky, Mirjam R Heldner, Patrik Michel, Paul J Nederkoorn, Sami Curtze, Gian Marco De Marchis, Guido Bigliardi, Christian H Nolte, João Pedro Marto, Andrea Zini, Alessandro Pezzini, Susanne Wegener, Marcel Arnold, Stefan T Engelter and Henrik Gensicke in European Stroke Journal
Footnotes
Acknowledgements
NA.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Georg Kägi has received modest honoraria for travel and advisory board from Bayer, Bial and Zambon and a research grant from the Swiss Heart Foundation, Swiss Parkinson Foundation, Swiss National Science Foundation. Dejana R Jovanovic has received speaker honoraria from Boehringer-Ingelheim, Bayer and Pfizer and Medtronic. Carlo W Cereda has received modest honoraria for scientific advisory board from Bayer, Boehringer-Ingelheim and iSchemaview; Research grants from the Swiss Heart Foundation. Ronen R. Leker has received speaker honoraria from Pfizer, BI, Abott, iSchema View, Medtronic and Novo Nordisk and advisory board honoraria from Novo-Nordisk and research grant from the Israeli Science Foundation. Visnja Padjen has received speaker honoraria from Medtronic and Boehringer Ingelheim. Urs Fischer reported research support of the Swiss National Science Foundation and the Swiss Heart Foundation. Research grants from Medtronic (BEYOND SWIFT, SWIFT DIRECT) and from Stryker, Rapid medical, Penumbra, Medtronic and Phenox (DISTAL), Boehringer Ingelheim (TECNO). Member of a clinical event committee (CEC) of the COATING study (Phenox). Member of the data and safety monitoring committee (DSMB) of the TITAN, LATE_MT, IN EXTREMIS and RapidPulse trials. Mirjam R Heldner has received research grants from the Swiss Heart Foundation, from the SITEM Insel support funds and from the Swiss National Science Foundation. Patrik Michel has received funding from the Swiss National Science Foundation and Swiss Heart Foundation. Consulting and speaker fees from Medtronic. Paul J Nederkoorn has received funding from the Dutch heart foundation for acute stroke intervention trials in the Collaboration for New Trials in Stroke (CONTRAST) consortium. Sami Curtze: No relevant disclosures. Gian Marco De Marchis: No relevant disclosures. Guido Bigliardi has received funding for scientific advisory board from Daiichi-Sankyo. Christian H Nolte has received research grants from German Ministry of Research and Education, German Center for Neurodegenerative Diseases, German Center for cardiovascular Research, and speaker and/or consultation fees from Alexion, Astra Zeneca, Bristol-Myers Squibb, Novartis and Pfizer Pharma. João Pedro Marto: No relevant disclosures. Andrea Zini has received funding for speaker honoraria and consulting fees from Boehringer-Ingelheim, Pfizer, Daiichi-Sankyo and CSL Behring, for scientific advisory board from Bayer, Boehringer-Ingelheim, PIAM and Astra Zeneca. Alessandro Pezzini: No relevant disclosures. Susanne Wegener received research funds by the Swiss National Science Foundation, the UZH Clinical research priority program (CRPP) stroke, the Swiss Heart foundation, the Zurich Neuroscience Center (ZNZ), a speaker honorarium honoraria from Amgen (2018), Springer (2021), Teva Pharma (2021) and a consultancy fee from Bayer (2019) and Novartis (2021). Marcel Arnold received Speaker honoraria from Bayer, Boehringer Ingelheim, and Covidien; Scientific advisory board honoraria from Amgen, Bayer, Boehringer Ingelheim, BMS, Pfizer, Covidien, Daichy Sankyo, Nestlé Health Science and Novartis. Research grants from the Swiss Heart Foundation and the Swiss National Science Foundation. Stefan T Engelter has received funding for travel or speaker honoraria from Bayer, Boehringer Ingelheim and Daiichi-Sankyo. He has served on scientific advisory boards for Bayer, Boehringer Ingelheim, BMS/Pfizer, and MindMaze and on the editorial board of Stroke. His institutions have received an educational grant from Pfizer, compensation from Stago for educational efforts and research support from Daiichi-Sankyo, the Science Funds [Wissenschaftsfonds] of the University Hospital Basel, the University Basel, from the “Wissenschaftsfonds Rehabilitation” of the University Hospital for Geriatric Medicine Felix Platter, the “Freiwillige Akademische Gesellschaft Basel,” the Swiss Heart Foundation, and the Swiss National Science Foundation. Henrik Gensicke has received research support from the Swiss National Science Foundation, AbbVie, Merz and Ipsen, and advisory board honoraria from Daiichi Sankyo and AbbVie, and funding for travel from BMS/Pfizer. All other authors report no conflicting interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the ethics committee in Basel, Switzerland.
Informed consent
Datasets generated or analyzed within the present study are available from the corresponding author upon reasonable request. In any such case, data sharing will be subject to individual patient consent processes in the participating centers. The final decision on data sharing will be made by consensus of the EVA-TRISP collaborators.
Guarantor
HG.
Contributorship
JJ, LE, and HG researched literature and conceived the study. LE was involved in data analysis. JJ wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.