
Abstract
Introduction:
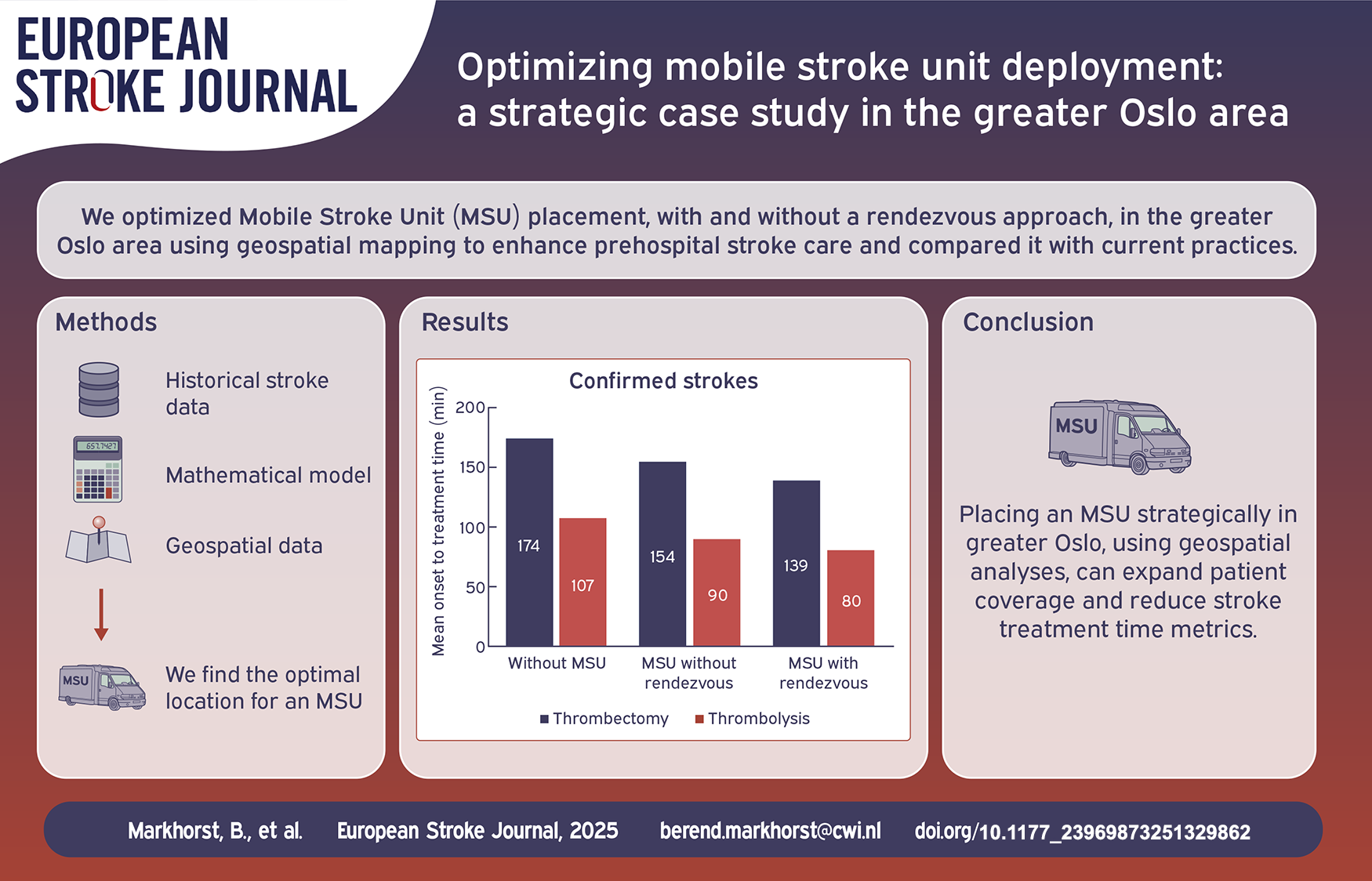
A Mobile Stroke Unit (MSU) enables prehospital acute stroke assessment, which leads to increased treatment rates and improved patient outcomes. However, for optimal utilization of the specialized resource, identifying the proper location for the MSU is crucial. Motivated by this, our goal was to find the optimal placement of an MSU in the greater Oslo area using geospatial mapping, and to explore how the location may influence acute stroke treatment.
Methods:
Historical data on suspected and confirmed strokes with the respective geospatial data and calculated travel times were analyzed using a mathematical optimization model based on the Maximum Coverage Location Problem (MCLP) and solved with the Gurobi solver. The model is universal and may be adapted to other regions and countries.
Results:
The optimal base location for a single MSU in the greater Oslo area would increase the coverage of stroke patients by 24%. The rendez-vous approach yields a more than doubled coverage for confirmed stroke patients. In the optimal location, the MSU has the potential to reduce time to thrombolysis by 28 minutes (28%) and time to thrombectomy by around 35 minutes (20%).
Conclusion:
Strategic placement of an MSU in the greater Oslo area significantly increases patient coverage and may reduce treatment times in acute stroke. Geospatial analyses have the potential to aid decision making on MSU location, optimize prehospital acute stroke assessment and improve patient outcomes.
Keywords
Introduction
In acute stroke, timely treatment is crucial for prognosis. Bringing advanced diagnostics and treatment into the prehospital field with mobile stroke units (MSU) have shown significant reductions in time to treatment and improvement in patient outcomes.1–3 An MSU is an ambulance equipped with a computed tomography (CT) scanner, a point of care laboratory and staffed with a specially trained stroke team enabling prehospital stroke assessment on-scene.1,4 MSUs also warrant accurate prehospital triage directly to comprehensive stroke centers (CSC), which avoids detrimental interhospital transfers, 5 and facilitates timely handling of stroke patients in need of specialized treatment like thrombectomy and neurosurgery.2,3
Benefits of MSU care can be expected to diminish with longer distance and travel time from MSU base to scene, but there is a lack of evidence for MSU services in rural and remote areas. In the metropolitan city of Berlin, relevant time savings were achieved up to a mean travel time of 18 min from the MSU base. 6 The operational range can increase using a rendez-vous system, where the MSU meets up en-route with a conventional ambulance. Using this system, the range of operations doubled to 20 km in an urban area, also doubling the number of patients reached by the MSU. 7
MSU systems with different operational models are proven timesaving and cost-effective in densely populated areas,8–10 however the optimal placement and operating radius of an MSU within these urban areas are not settled.
Geospatial analyses of infrastructure and emergency system data on acute stroke dispatch can optimize MSU positioning and service performance.11–13 This paper uses geospatial methods to explore the strategic placement of an MSU service in the densely populated greater Oslo area in South-East Norway, using historical data on confirmed acute stroke. We analyze the strategic placement of MSUs in the greater Oslo area considering patient coverage, and how the optimal location influences the time to acute stroke treatments.
Methodology
We present a detailed description and analysis of the data in Section “Data” and provide an elaborate explanation on the mathematical models in Section “Mathematical model.”
Data
We used the locations of confirmed strokes in Norway in 2022 provided by the Norwegian Stroke Registry. 14 The dataset includes 9,020 confirmed strokes (86% cerebral infarctions and 14% hemorrhages) in 2022, of which 3,121 were in the greater Oslo area. Figure 1 presents a heatmap illustrating the number of confirmed strokes per postal code within the Oslo area. To enhance readability, two reference points—the airport and the opera—have been included. The heatmap indicates that stroke occurrences are rare in most rural regions, and more concentrated in the city center.
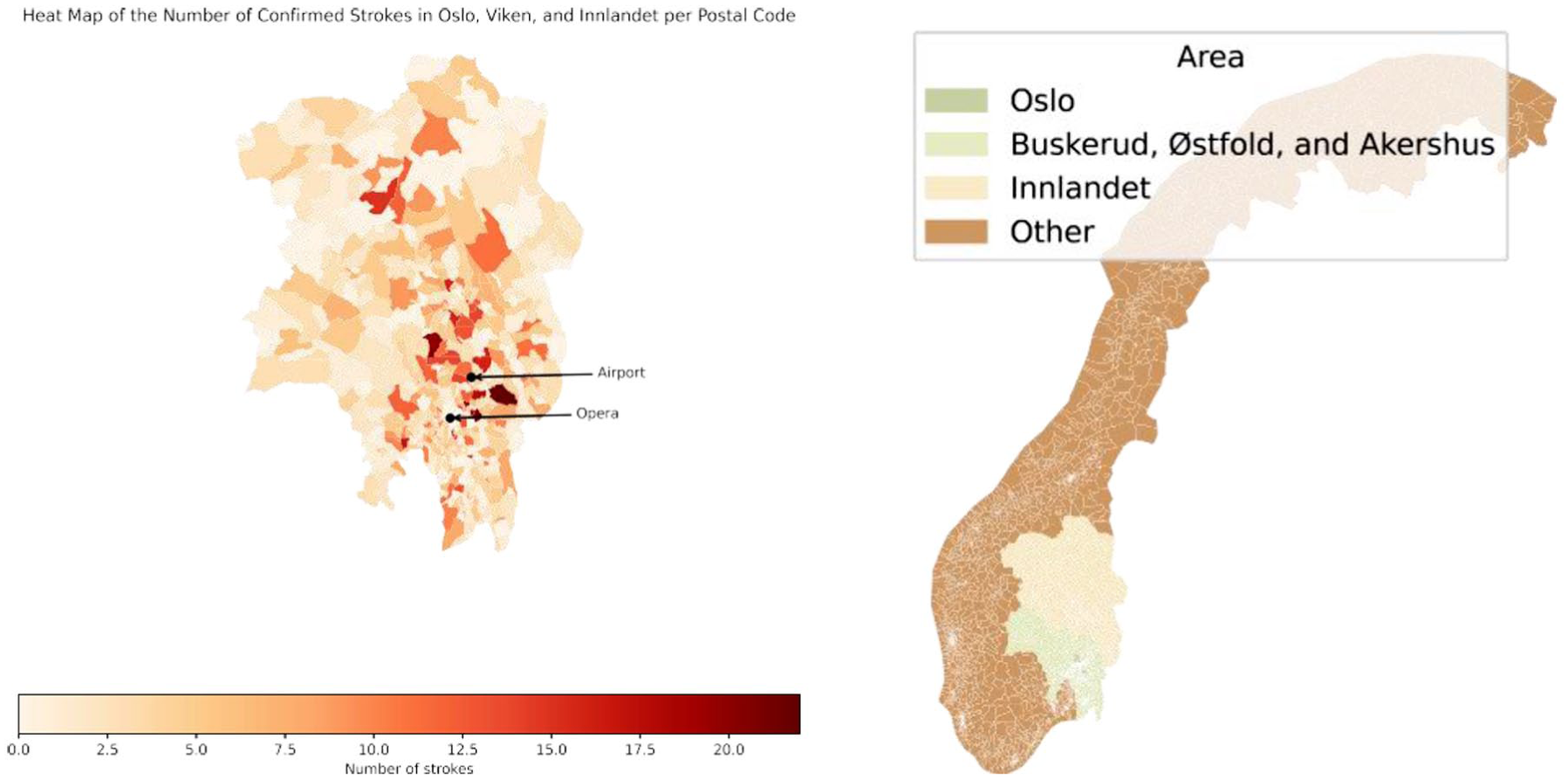
Heatmap for the number of confirmed strokes per postal code in the Oslo area and the Oslo area highlighted, indicating Oslo, Akershus, Buskerud, Østfold, and Innlandet.
The geographic data contained all 1,789 postal codes from Oslo, Akershus, Buskerud, Østfold and Innlandet – hereafter called the greater Oslo area. 15 The bottom right corner of Figure 1 shows the geographical region considered in the study. Via the shape files of these postal codes 16 and the Open Route Service Application Programming Interface (API) 17 we obtain travel times by car between all postal code centroids. For 19 remote postal codes this approach did not work as their centroids are not road accessible; we replaced those centroids by a manually obtained alternative. 18 The number of strokes in these regions is relatively low, so this replacement has a negligible effect on the final results.
Moreover, we used the postal codes for all existing ambulance bases and regional hospitals in the greater Oslo area. Figure 2 highlights these 62 bases and the 17 hospitals located within the studied area.
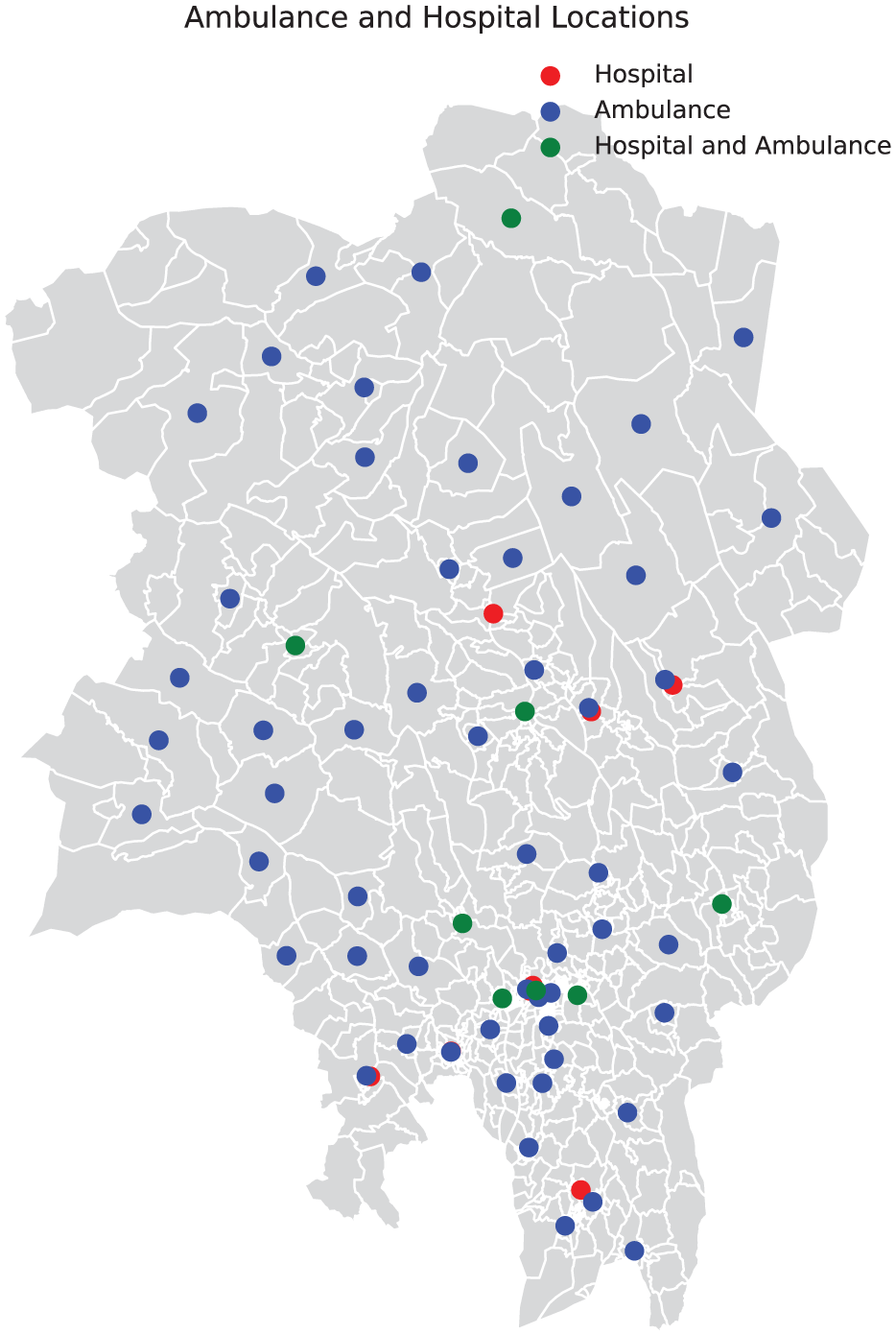
Postal codes with an ambulance base or a hospital.
All data and Python code is available from the corresponding author upon reasonable request.
Mathematical model
The current practice for conventional ambulances alarmed to acute stroke is an immediate dispatch, and rapid clinical evaluation and examination on-scene. If a stroke is suspected, rapid transportation to the closest hospital with acute stroke care is performed after a prenotification to the on-call stroke physician. An ambulance on-scene time of 24 minutes was used based on previously published data. 19 At the hospital, the patient will be met in the emergency room by a stroke team for a rapid clinical examination, radiological work-up with CT imaging and acute treatment will be initiated based on diagnosis and indication. An in-hospital door-to-needle time of 29 min was used based on previously published data. 20 In case of a large vessel occlusion (LVO) or intracerebral hemorrhage (ICH) eligible for intervention, the patient will undergo thrombectomy or neurosurgery at a CSC, which involves a secondary transfer for patients initially admitted by ambulance to a primary stroke center (PSC).
The MSU will be dispatched in parallel with a conventional ambulance to the patient scene, or rendez-vous. The MSU physician performs a clinical examination of the patient, and if indicated, a CT scan and acute treatment like thrombolysis will be initiated on-scene. An MSU door-to-needle time of 22 min was used based on previously published data. 20 The patient will either be transported to a PSC for further diagnostic work-up and treatment, or if indicated, directly triaged to a CSC for specialized treatment.
The model incorporates that stroke patients are always transported to the closest acute stroke facility; PSC, CSC, or MSU. The CSC OUH Rikshospitalet has a regional thrombectomy service for patients outside of Oslo, whereas the CSC OUH Ullevål is the local hospital for Oslo’s population. All acute stroke patients in the Oslo area were assumed to be transported directly to OUH Ullevål with conventional ambulance or MSU.
We formulated the problem of strategically placing an MSU in the greater Oslo area as a mathematical optimization model which we solve with the solver from Gurobi Optimization, 21 including the rendez-vous approach. 7 In this mathematical model, all of the decision variables are restricted binary (i.e. zero or one), making it particularly suitable for decision-making scenarios where options are discrete, such as choosing locations or making yes/no decisions.
In this context, the choice for this mathematical optimization model is driven by the need to make binary decisions about where to place MSUs and which postal codes they can cover within a specified time limit. This model allows us to efficiently solve this problem while adhering to the travel-time constraints.
The maximum coverage location problem
The Maximum Coverage Location Problem (MCLP) was introduced in 1974 and was recently applied in a stroke context.22,23 We implemented this mathematical model using our estimates for travel times, and the empirical stroke data set. The model also requires us to define a time threshold, which we set to 18 minutes driving time from base, as this has previously been described as the tolerated travel time for an MSU in an urban area. 6 The model subsequently places one MSU in the postal code that maximizes the number of stroke patients that are reachable within 18 minutes. We refer to this model as Model 1.
We next add the rendez-vous approach 7 into the mathematical formulation of Model 1. This is done by allowing a patient transfer from a conventional ambulance to an MSU. This involves constraining the total of the driving time of a regular ambulance from its base, the on-scene treatment time, and the driving time from the MSU. With this addition to Model 1, we obtain a new model, which we refer to as Model 2. It is implicitly assumed that the ambulance and the MSU can meet at any point in the Oslo area.
We implemented Model 1 and 2 in Python and solved them with Gurobi.
Summary
Our analysis for both thrombolysis and thrombectomy juxtaposes three different estimates obtained by different models. These estimates quantify the time for a patient to reach a suitable treatment facility, as described in Section “Mathematical model” and “The maximum coverage location problem.” The first model represents current practice, without an MSU. The second model utilizes a single MSU without rendez-vous and is extended in the third model with a rendez-vous approach.
Results
Optimal MSU bases
We first explore the optimal location for a single MSU, without considering the rendez-vous approach. By applying Model 1 to the stroke dataset, we identified optimal base location in postal code 1338 for confirmed stroke. The optimal location for the MSU, identified as postal code 1338 (Sandvika), would cover 17% (n = 33) more stroke patients compared to positioning the MSU at an existing ambulance base. With the rendez-vous approach, the number of covered patients receiving timely acute stroke care increases by 300%. In Figure 3, we show the locations of the three CSCs in the region and the postal code of the optimal base location.
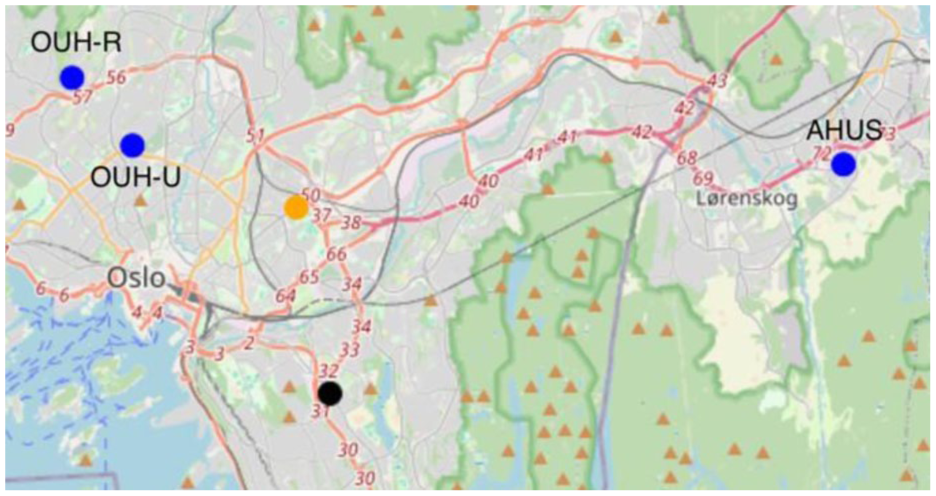
Three specialized hospitals (blue), the optimal MSU base based on the confirmed strokes (orange) and the optimal base with rendez-vous (black). OUH-R; Oslo University Hospital Rikshospitalet, OUH-U; Oslo University Hospital Ullevål, AHUS. Akershus University Hospital.
When running Model 2, we find that the optimal MSU base location is postal code 0680 (district Østensjø), shown in Figure 3.
Multiple MSUs
With the addition of more MSUs, we find diminishing returns in terms of coverage. While increasing the number of MSUs does improve coverage, the number of additional patients covered decreases relative to the number of MSUs deployed.
Sensitivity analysis
Next, we consider the sensitivity of the optimal solution from Model 2—specifically, whether small changes in the MSU’s location significantly affect patient coverability. Figure 4 visualizes this by showing the number of patients covered based on the MSU's postal code location. The results indicate that only a small portion of the area contains viable candidates for an optimal MSU base, suggesting that the solution is sensitive to location, with a few ideal placement options.
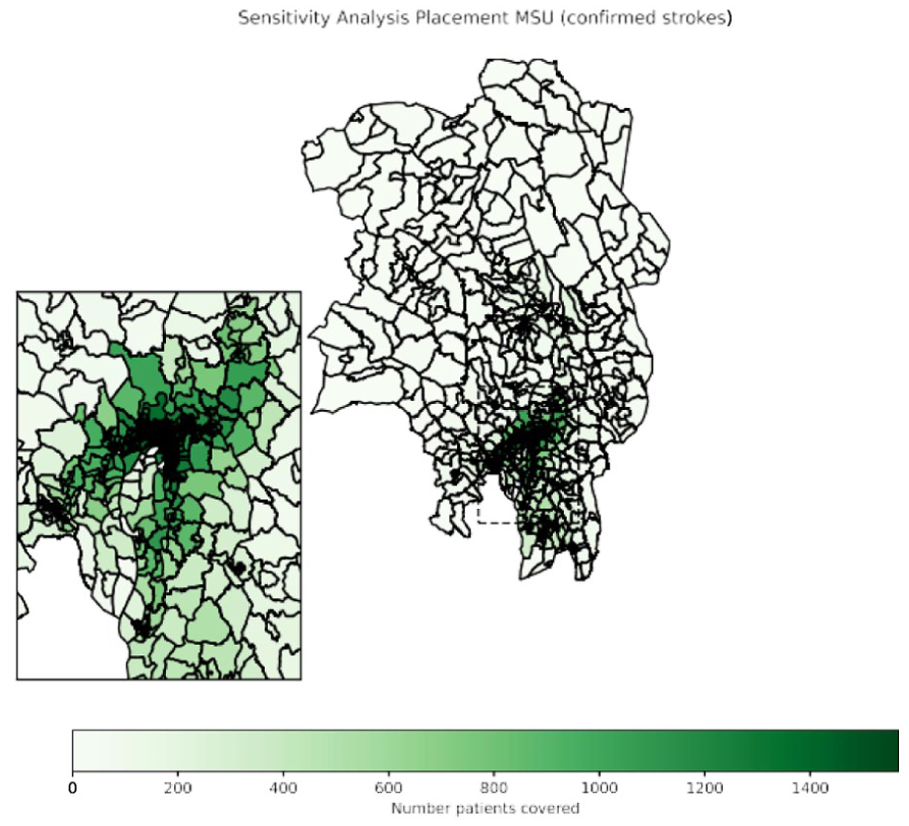
Sensitivity analysis on the placement of one MSU in the Oslo area. Darker green areas illustrate MSU base locations with higher patient coverage. MSU; mobile stroke unit.
For the three different transportation models mentioned in Section “Summary,” we show the resulting onset to treatment time in Table 1 and Figure 5. Adding an MSU has potential to reduce the onset to treatment time compared to the conventional ambulance system considerably. Finally, we observe that the standard deviations in Table 1 are relatively high compared to the means, both for time to thrombolysis and time to thrombectomy. For time to thrombolysis, our model predicts that the standard deviation would decrease when introducing an MSU.
Mean and standard deviation (SD) of onset to treatment time for thrombolysis and thrombectomy for three different ambulance approaches.

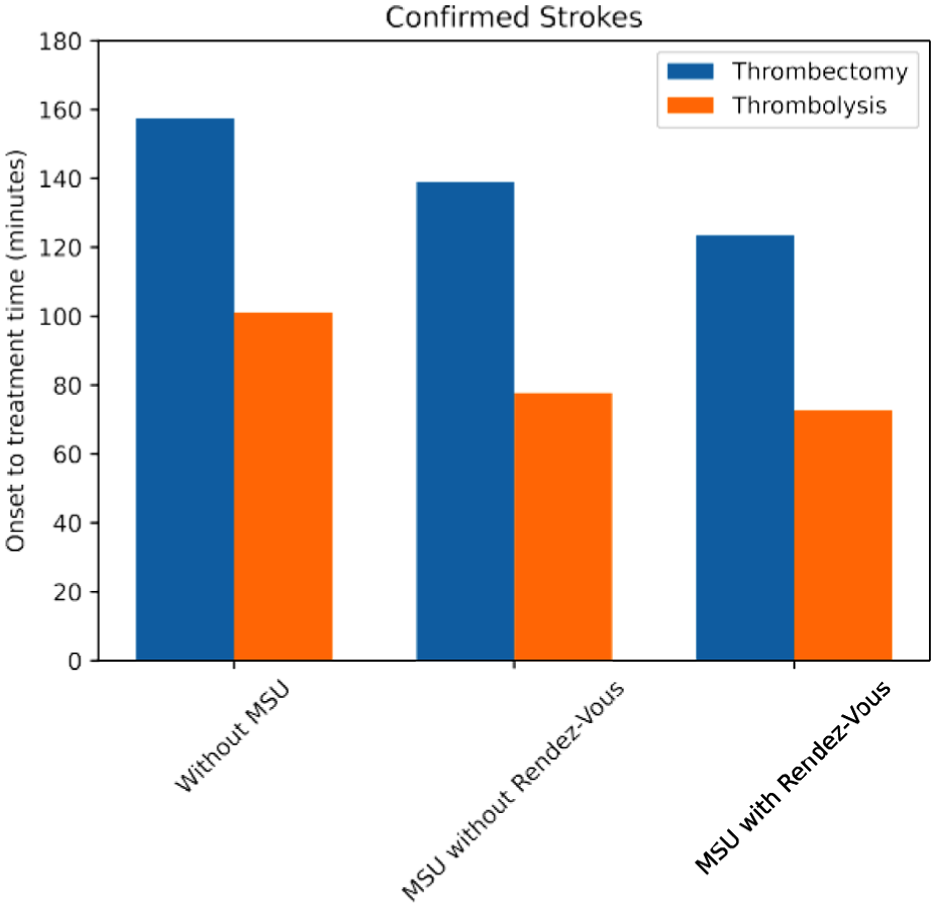
Distribution of time until stroke treatment starts, either in the Mobile Stroke Unit (MSU) or a specialized hospital. Three situations are compared: the as-is situation (without MSU) and using one MSU with and without rendez-vous.
Discussion
This is the first study to explore and highlight how optimizing the MSU base location substantially impacts stroke patient coverage and time to reperfusion treatments. By identifying the optimal geographical location for a single MSU in the greater Oslo area, we demonstrated that patient coverage could increase by 17% compared to using a current ambulance base. Using the rendez-vous approach shifted the optimal MSU location slightly while tripling the coverage of confirmed strokes. Although additional MSUs provide coverage gains, these returns diminished with every added MSU, indicating that a few well-placed MSUs would offer an effective balance of resource utilization and patient care. Additionally, the sensitivity analysis revealed that only a few geographical regions contain viable MSU placement options, reinforcing the importance of careful site selection. With the known pivotal role of time in acute stroke treatment, 24 optimal placement of the MSU base will potentially lead to improved patient outcomes as more patients are treated, and they are treated earlier.
The results indicate that MSUs significantly reduce the onset to treatment time, particularly when combined with a rendez-vous approach. MSUs may reduce the time to thrombolysis up to 25% compared to the standard ambulance transfer and in-hospital treatment. This aligns with results from previous real-life MSU studies showing significant reductions in time to thrombolysis. 3 Reducing the time to thrombolysis is crucial, as it leads to better functional patient outcomes.3,24 It is likely that an optimal MSU location would similarly reduce the time to acute treatments for ICH like antihypertensive drugs, reversal of anticoagulants and neurosurgery. MSUs are the only approach today enabling accurate stroke diagnostics and hyperacute treatment on-scene for both AIS and ICH patients.25,26 Improved functional outcomes have been reported for the entire stroke population of cerebral hemorrhages and ischemia following MSU care.2,3,27 One recent MSU substudy detected no difference in outcomes for patients with ICH, but the study was underpowered and not primarily designed for this outcome. 28 Meta-analyses have also shown that MSU care increases the proportion of LVO and ICH patients transferred to a CSC, but unlike in the current study, no time reductions were found.2,3 Reasons could include repeating imaging after hospital arrival and no “direct to angio suite” protocols. 3 In streamlined MSU systems, reductions in door-to-puncture times of more than 50 min have been reported. 29
This paper shows that MSUs have the potential to significantly reduce the time to specialized treatments as it enables field triage directly to CSCs avoiding secondary transfers. This effect is naturally larger in areas without the closest hospital being a CSC. The decision for placement of the MSU should consider both impact on patient coverage and potential time reductions to standard and specialized treatment for the entire stroke population.
In European guidelines, 3 MSUs are suggested over conventional care for suspected stroke patients, and cost-effectiveness is proven for MSU care in densely populated areas across countries, Norway included.8,9,30 Still, few European countries have operative MSUs and no MSU service is fully implemented and reimbursed in local health systems. Geospatial studies can aid decision making on geographical placement of MSUs and illustrate how MSUs would impact the stroke pathway, patient coverage and treatment times. Hence, solid geospatial studies may facilitate MSU implementation.
Several limitations could impact the robustness and applicability of the findings. We used postal code centroids as a proxy for patient locations. While this simplification allows for computational feasibility, it overlooks geographical variability, which could be relevant within large postal codes. This introduces potential biases in our analysis of travel times and coverage. Finally, our estimates for response-time improvements are based on the entire study area, not only those postal codes that benefit from the MSU placement. Therefore, our numbers can be viewed as conservative, in the sense that the effect would have appeared larger if we had only reported for those postal codes within the MSU’s catchment area.
We did not account for prehospital decision delay or additional in-hospital time delay other than the DNT of 29 min in secondary transfers. Decision times and inter-hospital transfers often cause substantial delays indicating that our estimates are conservative.31–33 Based on previous research in metropolitan Berlin, we restricted the MSU catchment area to 18 min driving from the base station. 6 Another study reported that MSU care in Melbourne would still be time beneficial at an operating range of up to 76 min from base location. 13 The optimal operating range in the studied geographical area could differ from the Berlin study, but we did not explore this further.
Our analyses involved stroke data from 2022, which raises concerns about temporal variability as we did not incorporate data over multiple years. However, the pandemic and also a large clinical trial running in the EMS in the Oslo area from 2019 to 2021, 19 had huge impact on stroke pathways, and 2022 should be more representative.
We did not incorporate dynamic traffic data, and blue light driving. Ambulances with blue lights are generally faster than regular traffic, but this varies with rush hour congestion. For simplicity, we excluded this from driving times, making our findings conservative. Additionally, we did not consider economic factors, staffing capabilities, and the availability of other infrastructures, such as fire stations. Including these in the future studies could yield even more realistic outcomes.
The models used in this study reflect that the ambulance closest to the patient is always available when needed. Literature shows that a modest amount of concurrency conflicts does not significantly influence optimal base locations. 34
Conclusion
Strategic placement of an MSU in the greater Oslo area may significantly increase patient coverage and reduce treatment times in acute stroke. Geospatial analyses have the potential to aid decision making on MSU location and optimize prehospital acute stroke care.
Footnotes
Acknowledgements
We thank Jasper van Doorn estimating the travel times used in this study and Ruurd Buijs for insightful discussions. We thank the Norwegian Stroke Registry and Oslo University Hospital for providing empirical stroke data.
Correction (December 2025):
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: BM was funded by a grant (ref. TWM.BL.019.002) from the Dutch Research Council (NWO).
Informed consent
Not applicable.
Ethical approval
Not applicable. We do not work with study participants, hence informed consent and an ethical statement were not applicable to our work.
Consent to participate
Not applicable. We do not work with study participants, hence informed consent and an ethical statement were not applicable to our work.
Guarantor
The
Contributorship
BM was responsible for the analyses and wrote the first draft together with KL. CJ, MRH, RvdM, and KL revised the manuscript. CJ and KL supervised and managed the project, and KL provided the data. All authors approved the final version of the manuscript.
Data availability
The data and code are available upon request.