
Abstract
Introduction:
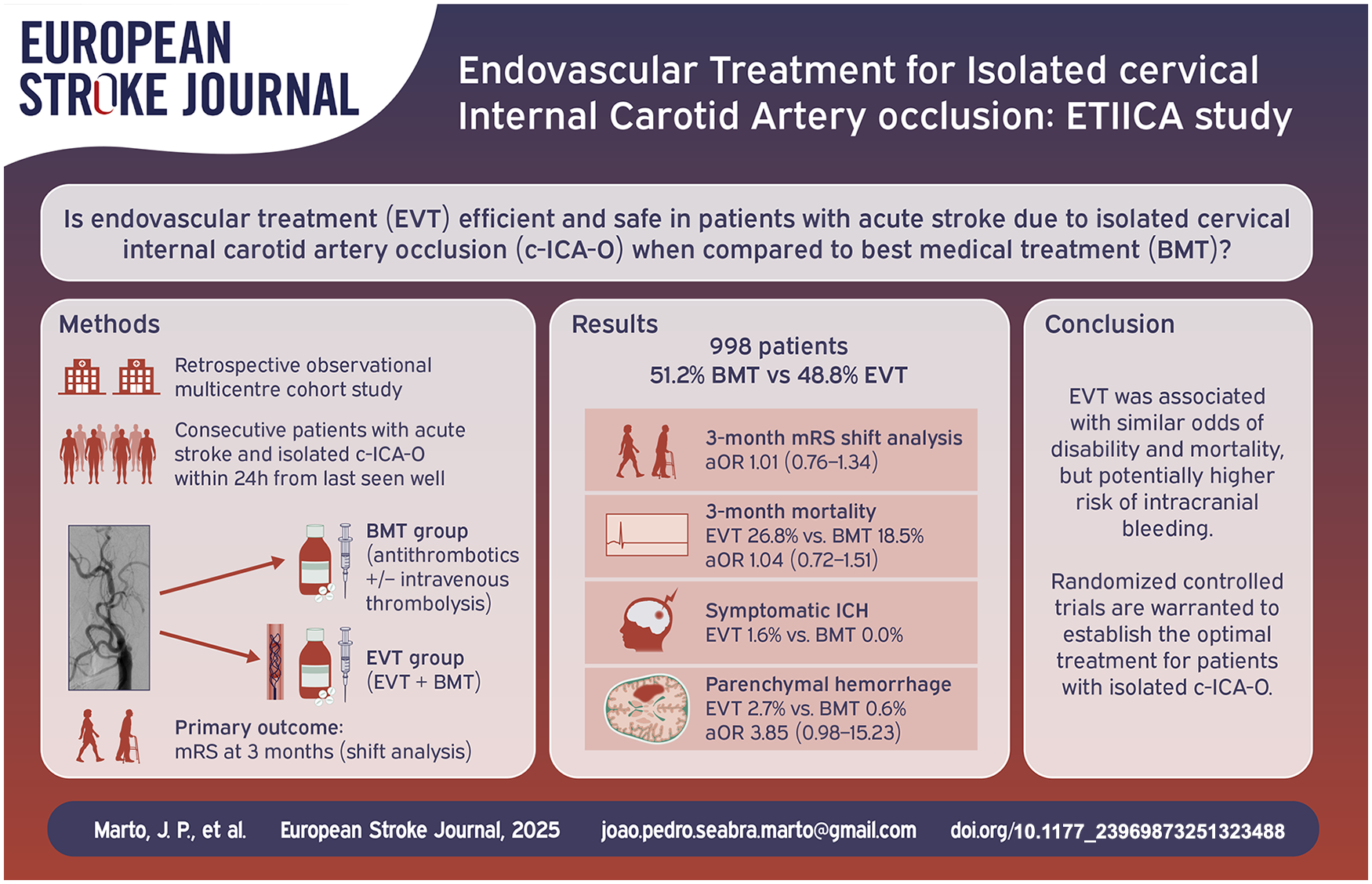
Evidence regarding the benefit of endovascular therapy (EVT) in patients with acute ischemic stroke (AIS) due to isolated cervical internal carotid artery occlusion (c-ICA-O) is lacking. We assessed the outcomes and safety of EVT in patients with isolated c-ICA-O.
Methods:
Retrospective multicenter cohort study of patients with an AIS due to isolated c-ICA-O, within 24-h since last-seen-well. Comparisons were made between EVT and best medical therapy (BMT). The primary outcome was 3-months modified Rankin Scale (mRS) ordinal shift. Secondary outcomes included 3-month favorable outcome (mRS 0–2, or return to pre-stroke mRS), symptomatic intracranial hemorrhage (sICH) and any parenchymal hemorrhage. Outcomes were compared combining inverse probability of treatment weighting with regression models and propensity score matching (PSM) as sensitivity analysis.
Results:
We analyzed 998 patients (66.2% male, mean age 71.1 ± 13.2 years). 487 (48.8%) patients received EVT and 511 (51.2%) received BMT. Patients receiving EVT had a higher admission NIHSS [13 (7–18) vs 5 (2–13)] compared to BMT. There was no difference between EVT and BMT groups in 3-month mRS shift (adjusted common odds ratio [OR], 1.01 [95% CI 0.76–1.34]) and favorable outcome (adjusted OR [aOR] 1.16 [95% CI 0.84–1.60]). No patient (0%) in the BMT group had sICH versus 1.6% in the EVT group. Parenchymal hemorrhage was numerically higher in EVT patients (2.7% vs 0.6%; aOR 3.85 [95% CI 0.98–15.23]). PSM analysis revealed similar results.
Discussion and conclusion:
In patients with isolated c-ICA-O, EVT was associated with similar odds of disability and intracranial bleeding compared to BMT. Randomized-controlled clinical trials in patients with isolated c-ICA-O are warranted.
Keywords
Introduction
Isolated cervical internal carotid artery occlusion (c-ICA-O) comprise approximately 2.5%–4% of acute ischemic stroke (AIS) patients treated with an arterial occlusion.1,2 The optimal treatment of isolated (c-ICA-O), that is, without associated intracranial artery occlusion, in AIS is unknown.3,4
In contrast to patients with anterior circulation tandem lesions, patients with isolated c-ICA-O were not included in any of the randomized-controlled clinical trials (RCTs) assessing safety and efficacy of endovascular treatment (EVT) in anterior circulation AIS. 5 In tandem occlusion, immediate EVT of the extracranial occlusion may be safe and associated with better clinical outcomes.6–10 In c-ICA-O, early neurological deterioration is seen, even if patients present initially with mild or remitting deficits, and these patients have unfavorable outcomes under best medical treatment (BMT).11–13
Previous smaller observational studies suggested that in patients with isolated c-ICA-O, EVT was feasible, while it remained to be shown whether EVT is associated with improved clinical outcomes and safety.2,14–17 Lack of control patients, small sample sizes, or significant imbalance in baseline characteristics between treatment groups have limited the conclusions of previous studies.2,14–17 For these reasons, the question whether EVT is effective and safe in patients with isolated c-ICA-O remains unanswered. We assessed the outcome and safety of EVT in patients with isolated c-ICA-O in comparison to BMT.
Methods
Study design and population
The Endovascular Treatment for Isolated Cervical Internal Carotid Artery Occlusion (ETIICA) study was an investigator-initiated, retrospective, multinational, cohort study conducted at 42 sites in Europe and North America. The study included consecutive patients with AIS and ipsilateral isolated c-ICA-O admitted to the participating hospitals from January 2018 to December 2022. All patients that presented with c-ICA-O within 24 h of last-seen-well were screened for eligibility by the contributing centers. C-ICA-O had to be clinically symptomatic (any acute, focal, neurological deficit attributable to the ipsilateral cerebral hemisphere) and located exclusively in the carotid bulb and/or ascending cervical carotid segment. Patients not receiving EVT were considered as BMT group. Patients receiving EVT regardless of other medical interventions were included in the EVT group. Consequently, use of IVT was allowed in both treatment groups.
Patients who received emergent carotid endarterectomy were not included in the study.
All investigators were requested to review admission vessel imaging of eligible patients to confirm the presence of an isolated c-ICA-O. Patients with concomitant intracranial ICA or other vessel occlusions were excluded. In addition, patients were excluded if initial digital subtraction angiography (DSA) series showed an intracranial ICA occlusion despite initial diagnosis of c-ICA-O (carotid pseudo-occlusion on initial imaging), 18 or high-grade cervical stenosis instead of complete occlusion. To achieve rigorous exclusion of patients without isolated c-ICA-O, the following instructions were sent to all participating centers: (1) In patients with isolated c-ICA-O there is usually an abrupt cut-off opacification at the proximal ICA. This contrasts with “pseudo-occlusions” where there is usually a gradual contrast decline, sometimes with a flame-shaped appearance that can mimic the pattern of a carotid artery cervical dissection.19,20 (2) Patients not receiving DSA, must be excluded, if (a) occlusion was located in the terminal segment of the internal carotid artery, (b) the ICA siphon presented with a hyperdensity in non-contrast CT (hyperdense vessel sign) or hypointensity on gradient echo or susceptibility-weighted MRI (susceptibility vessel sign). All additional available imaging performed during hospital admission (e.g. Doppler ultrasound) had to be reviewed to confirm the isolated c-ICA-O.
For all patients, decisions regarding IVT and immediate antithrombotic regimen were made according to local standards and treating physician’s decision. In EVT patients, decisions regarding treatment techniques, device selection, modality of anesthesia, and periprocedural medication were made as deemed appropriate by the treating physicians.
Imaging modality (CT or MRI) on admission followed local standard operating procedures and/or was at the discretion of the treating physician. The reporting of this study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 21
Study variables
All sites initially received information about inclusion and exclusion criteria, study variables, and study-specific definitions. Data was checked for consistency and completeness (J.P.M). After the first review, queries were sent as needed to confirm data accuracy and validity.
Study variables included demographics (age, sex, and pre-stroke modified Rankin Scale (mRS)), vascular risk factors and comorbidities, pre-existing medication, stroke severity at admission and at 24 h (assessed by the National Institutes of Health Stroke Scale (NIHSS)), lateralization (left vs right hemisphere), admission systolic and diastolic blood pressure, admission blood glucose, initial imaging modality, and baseline Alberta Stroke Program Early CT Score (ASPECTS). In patients with ASPECTS assessed by MRI one point was added. 22 We assessed the following time metrics: Last-seen-well (LSW) to hospital admission, hospital admission to start of acute treatment (door-to-needle and door-to-puncture time where applicable) and hospital admission to reperfusion. Additionally, data on 24-to-36-h follow-up imaging (presence of hemorrhagic transformation/intracranial hemorrhage), stroke etiology, mortality and mRS at 3 months were collected. In patients receiving BMT, the immediate antithrombotic regimen was assessed. In patients receiving EVT, use of general anesthesia, stenting procedure, distal embolization, final intracranial modified treatment in cerebral infarction (mTICI) score, and carotid patency at the end of procedure (occluded, stenosis > 70%, no stenosis or stenosis < 70%) were recorded. Data completeness for each variable is documented in Supplemental Material – Table 1.
Outcome measures
The primary outcome was the distribution of the mRS score at 3 months (ordinal shift analysis), assessed either at the outpatient stroke clinic or by structured telephone interview, by mRS-certified medical personnel. Secondary outcomes included favorable outcome (mRS 0–2 or return to pre-stroke mRS), dependency with unassisted ambulation (mRS 0–3), mortality at 3 months, and early neurological improvement at 24 h defined as an improvement in 4 or more points on the NIHSS from admission or a NIHSS of 0–1. Safety outcomes were symptomatic intracerebral hemorrhage (sICH) according to the SITS-MOST definition: a Type 2 parenchymal hemorrhage with deterioration in NIHSS increase ⩾ 4-points or death), 23 presence of parenchymal hemorrhage (Type 1 and 2 parenchymal hemorrhage) and presence of any hemorrhagic transformation (petechial hemorrhagic transformation or parenchymal hemorrhage). 24
Ethics
Participating centers were requested to anonymize their data before sending it to the coordinating center (Department of Neurology, Charité-Universitätsmedizin Berlin and Center for Stroke Research, Berlin Institute of Health, Berlin, Germany). According to the local ethics committee regulations and national laws, each center was responsible for obtaining ethical approval for data collection and data sharing. Informed consent was waived because of the retrospective nature of this study. The study was conducted according to the principles of the Declaration of Helsinki. The statistical analysis was performed on anonymized data by a statistician (P.G.) not participating in data collection or interpretation.
Statistical analysis
We presented the mean, standard deviation (SD), median, and interquartile range for continuous variables, depending on the distribution, and absolute numbers and percentages for categorical variables. We compared baseline characteristics between the EVT and BMT groups using a chi-square test for categorical variables and an independent t-test or Mann-Whitney U test for continuous variables, as appropriate. We applied the inverse probability of treatment weighting (IPTW) method for handling unbalanced baseline characteristics between the EVT and BMT groups. The weighted propensity scores were estimated from a logistic regression model, including clinically preselected variables as follows: age, sex, pre-stroke mRS, admission NIHSS, time from LSW to hospital admission, ASPECTS, stroke etiology, and IVT. The balancing of baseline characteristics before and after adjustment for IPTW was evaluated using the standardized differences approach and standardized differences < ±0.1 were considered to indicate an adequate balance between the EVT and BMT groups (Supplemental Material Figure 1). 25 For assessing the 3-month mRS between EVT and BMT groups, we performed a shift analysis (ordinal logistic regression) using inverted mRS as an ordinal outcome. For the remaining outcomes, we performed binary logistic regression analyses. Subgroup analyses were conducted for the 3-month mRS by testing an interaction between subgroup variables (IVT treatment [yes vs no], time from LSW-to-admission [<6 h vs ⩾6 h], admission NIHSS [⩾10 vs <10] and atherosclerotic stroke etiology [yes vs no] and treatment modality (BMT vs EVT). All models were adjusted using IPTW. Additional adjustments were made for unequally distributed factors, including dyslipidemia, statins, current smoking, and first imaging modality.
As a sensitivity analysis, a propensity score matching analysis was conducted. A nearest-neighbor matching algorithm was used to create matched pairs between the EVT and BMT groups. The balance of matching variables was assessed using standardized differences (see Supplemental Table 2). Out of the 487 EVT cases, only 266 (54.6%) could be matched with 266 out of 511 BMT cases (52.0%). This resulted in 532 patients matched into pairs with similar propensity score values. Mixed-effects ordered logistic regression was applied to compare the mRS ordinal outcomes between the groups, accounting for matched cases. Additionally, mixed-effects logistic regression was used to compare binary outcomes between EVT and BMT groups. Statistical testing was done within an exploratory framework at a two-sided significance level of α = 0.05; therefore, no multiple correction was done. We performed statistical analyses and graphics with Stata MP/18 (StataCorp, 2023, College Station, TX, USA).
Results
We included a total of 998 patients from 42 centers in Europe and North America. The mean age was 71.1 (SD 13.2) years, 661 (66.2%) patients were male, median stroke severity was moderate [NIHSS 9; IQR (3–17)] and 860 (86.2%) patients were previously independent (pre-stroke mRS 0–2). In our study, 487 (48.8%) patients received EVT and 511 (51.2%) patients received BMT.
Patients receiving EVT had higher prevalence of atrial fibrillation and heart failure, and lower prevalence of dyslipidemia, current smoking and previous stroke or TIA, than those receiving BMT. Patients receiving EVT had shorter time from LSW to hospital admission, higher admission NIHSS [13 (7–18) vs 5 (2–13)] and lower proportion of MRI as first imaging modality. Cardioembolism and undetermined stroke etiology were more common in patients receiving EVT, while large artery atherosclerosis was more common in patients receiving BMT.
IVT was performed in 202 (41.5%) patients in the EVT group and in 144 (28.2%) patients receiving BMT. Door-to-needle times did not differ between groups (Table 1).
Baseline characteristics, imaging, and treatment data.

EVT: endovascular treatment; BMT: best medical treatment; TIA: transient ischemic attack; Min: minutes; NIHSS: National Institutes of Health Stroke Scale; BP: blood pressure; ASPECTS: Alberta Stroke Program Early CT score; CT: computed tomography; MRI: magnetic resonance imaging; IVT: intravenous thrombolysis; mTICI: modified treatment in cerebral ischemia.
Values are presented as mean (standard deviation), as median (interquartile range) or as numbers (proportions).
In BMT patients not receiving IVT (n = 367), 172 (46.9%) received single antiplatelet therapy within the first 24-h, 82 (22.3%) dual antiplatelet therapy, and 88 (24.0%) therapeutic anticoagulation (including 27 patients with concomitant single antiplatelet therapy).
In the EVT group, median door-to-puncture time was 116 (61–204) min, and median door-to-reperfusion time was 195 (125–280) min. While in 399 patients (81.9%) the decision to perform EVT was made upon initial clinical and imaging evaluation, in 88 patients (18.1%), the decision to perform EVT was made only after clinical worsening.
General anesthesia was performed in 191 (39.2%) patients. Acute carotid stenting and isolated ballon angioplasty were performed in 235 (48.3%) and 33 (6.8%) patients, respectively. At the end of the procedure, 91 (18.7%) patients remained with the carotid occluded, 22 (4.5%) patients had a carotid stenosis ⩾ 70% and 374 (76.8%) patients had no stenosis or stenosis < 70%. A total of 143 patients (29.4%) had distal embolization during the procedure. Among those, final mTICI 2b–3 was achieved in 129 (90.2%) patients. Carotid endarterectomy or endovascular stenting within 3 months (after the qualifying event) were performed in 54 patients (5.4%), hereof 33 in the BMT and 21 in the EVT group.
In univariate analysis, patients in the EVT group had worse 3-month functional outcome (Figure 1). Also, they had lower odds of achieving favorable outcome and dependency with unassisted ambulation at 3-months, and higher rates of 3-month mortality, parenchymal hemorrhage or any hemorrhage. No patient in the BMT group had a sICH versus 8 (1.6%) in the EVT group (Table 2).
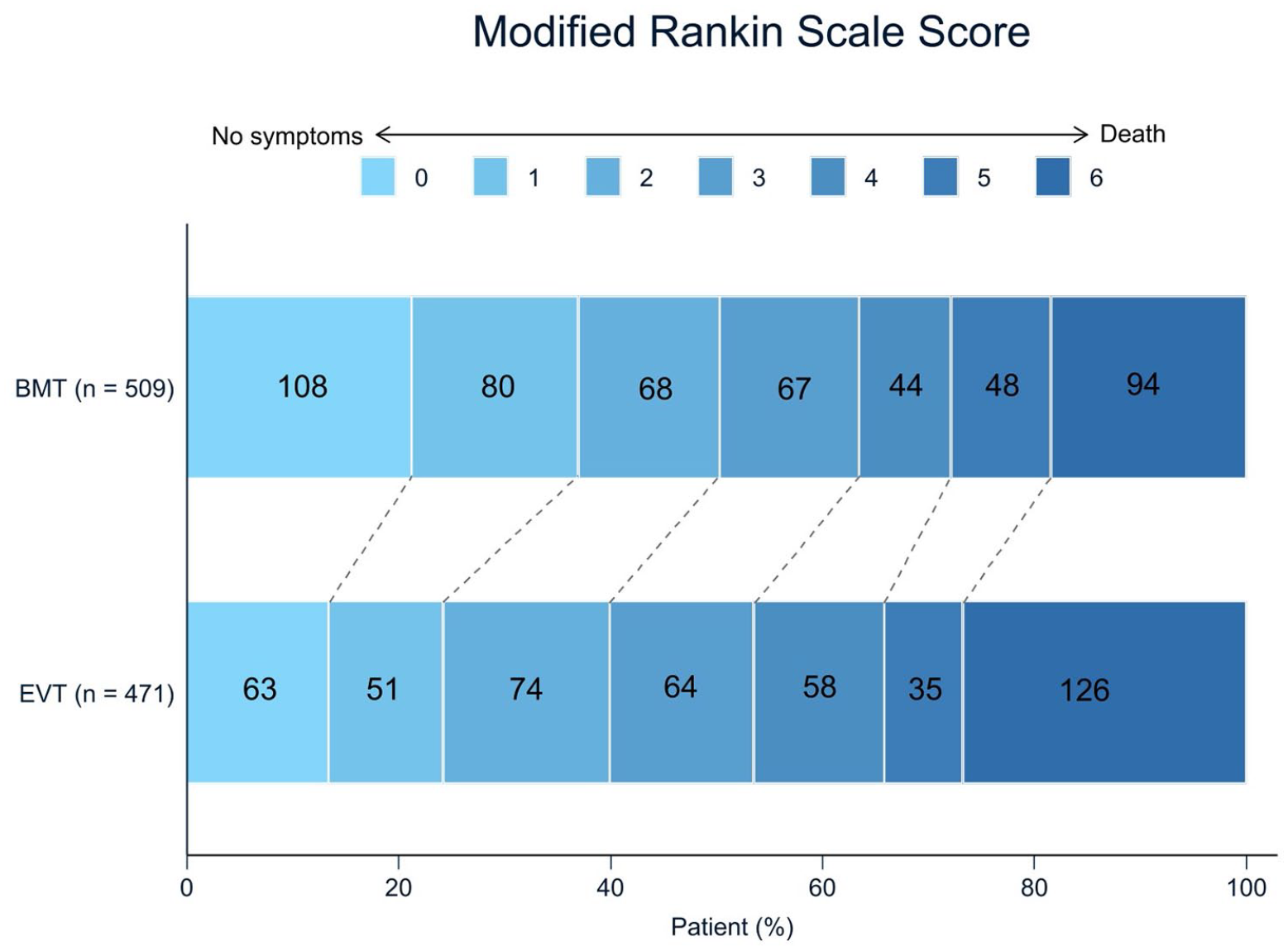
Modified Rankin Scale at 3 months according to treatment groups.
Outcome results.
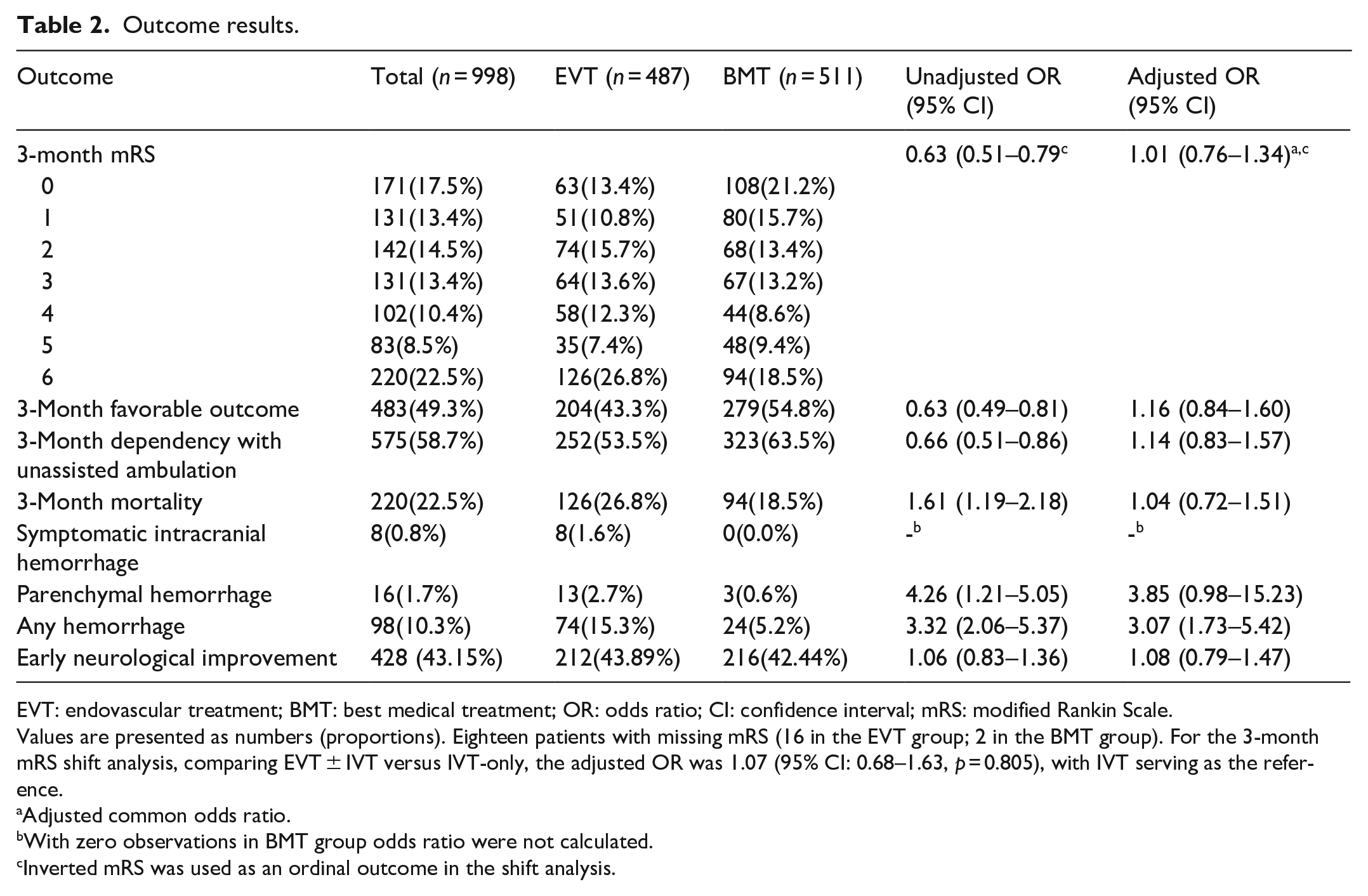
EVT: endovascular treatment; BMT: best medical treatment; OR: odds ratio; CI: confidence interval; mRS: modified Rankin Scale.
Values are presented as numbers (proportions). Eighteen patients with missing mRS (16 in the EVT group; 2 in the BMT group). For the 3-month mRS shift analysis, comparing EVT ± IVT versus IVT-only, the adjusted OR was 1.07 (95% CI: 0.68–1.63, p = 0.805), with IVT serving as the reference.
Adjusted common odds ratio.
With zero observations in BMT group odds ratio were not calculated.
Inverted mRS was used as an ordinal outcome in the shift analysis.
After adjustment for IPTW baseline characteristics were well balanced between groups (Supplemental Material Figure 1). Multivariable analysis showed no differences were between groups regarding 3-month functional outcomes (adjusted common OR 1.01 [95% CI 0.76–1.34]). Furthermore, no differences were found in favorable outcome, dependency with unassisted ambulation and mortality at 3-months. Rates of parenchymal hemorrhage were numerically higher in EVT patients, although not statistically significant (2.7% vs 0.6%; aOR 3.85 [95% CI, 0.98–15.23]). Presence of any hemorrhage was higher in the EVT group (15.3% vs 5.2%; aOR 3.07 [95% CI 1.73–5.42]) (Table 2).
In subgroup analyses, adjusted ordinal shift results remained similar depending on IVT treatment, LSW-to-door, admission NIHSS and atherosclerotic etiology (Figure 2).
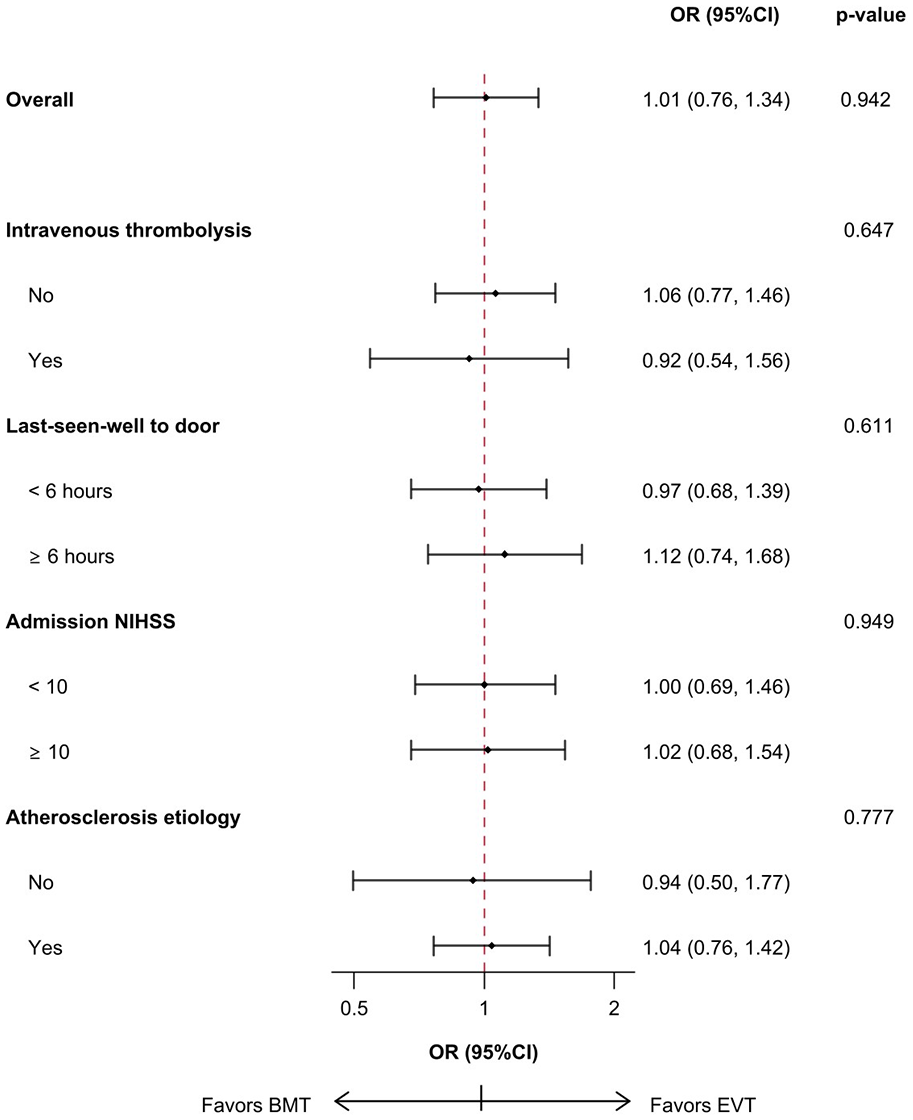
Forest plot for interaction analysis.
With regard to the presence of intracranial bleeding complications, we found no difference depending on IVT treatment for both parenchymal hemorrhage (p-value interaction: 0.370) or any hemorrhagic transformation (p-value interaction: 0.256).
In the sensitivity analysis using propensity score matching, 532 patients were matched in a 1:1 ratio (266 EVT, 266 BMT). After matching, no significant differences were observed between groups in baseline NIHSS [median NIHSS in the EVT group of 9 (5–15) vs median NIHSS in the BMT of 8 (3–17); standardized mean difference −0.050; p = 0.690], as in age, pre-stroke mRS, large artery atherosclerosis stroke etiology and IVT (Supplemental Material – Table 2). No differences were found between groups regarding 3-month functional outcomes (adjusted common OR 1.17 [0.86–1.58]), and for the secondary outcomes, the odds ratios were consistent with those reported in the IPTW analyses (Supplemental Material – Table 3).
Discussion
AIS with c-ICA-O can be associated with a poor prognosis and optimal treatment is yet to be defined. Given the expanding indications of EVT in the recent decade, endovascular reperfusion therapy could also be a therapeutic option in this specific patient subgroup. To our knowledge, this is the largest international multicenter cohort study assessing the outcomes and safety of EVT in IS patients with isolated c-ICA-O. Our study includes individual data of almost 1000 patients.
The key findings of our study were that EVT was associated with similar odds of disability at 3-month functional outcome compared to BMT. However, EVT was potentially associated with a higher risk of intracerebral bleeding when compared to BMT. Baseline imbalances in patients’ characteristics between treatment groups, particularly admission NIHSS, need to be considered when interpreting these results. However, our findings were consistent across several sensitivity analyses employing multiple statistical approaches, including ITPW and PSM.
Our results corroborate previous, smaller studies in which EVT was also associated with similar odds to achieve good functional outcomes.2,16,17 Of note, in our study, 3-month functional outcomes in patients receiving EVT were in general less favorable than previously reported (favorable outcome in 43.3% of patients vs 50%–73% in the literature).2,14–17 This finding may reflect different baseline characteristics of the studied populations. In our study, patients receiving EVT were older, had higher pre-stroke dependency and more severe strokes when compared to previous reports.2,14–17 Altogether, our data may represent a better estimate of real-world data including a broader heterogeneity of stroke patients, since we present a much larger and more diverse study multinational sample.
While our data does not support the widespread use of EVT for c-ICA-O, the poor prognosis of patients with isolated c-ICA-O receiving BMT needs to be recognized. Some reports describe that only 1 in 3 patients with isolated c-ICA-O achieves favorable outcome at 3 months.2,4,16,17 Reports vary, though, as the definition of BMT is heterogeneous, with several studies only including patients that received IVT,4,16 while others did not restrict BMT to IVT use.2,17 Given these inconsistencies and the importance of improving outcomes in isolated c-ICA-O patients, our study highlights that RCTs are needed to clarify whether EVT impacts clinical outcome in individuals with isolated c-ICA-O. Recently, the first RCT on EVT in patients with c-ICA-O was initiated in France (https://clinicaltrials.gov/study/NCT05832762).
Mortality was high in both groups and higher than previously reported in patients with isolated c-ICA-O. As suggested above, patients’ baseline characteristics are likely explanations for this finding.2,14–17 However, mortality was even higher than in our study in a multicenter study describing similar baseline characteristics on EVT patients with isolated c-ICA-O. 26
Technical outcomes reflect the particular difficulty involved in isolated c-ICA-O. Recanalization of the cervical ICA was achieved in 81.3% of patients, suggesting that EVT is feasible, but with room for improvement. Our findings are concordant with previous studies, reporting carotid recanalization rates between 78% and 82% of patients.2,27
With respect to safety outcomes, no patient in the BMT group had a sICH in comparison with 2.3% in EVT patients. Rates of sICH in patients receiving BMT for isolated c-ICA-O are generally low, ranging from 0% to 4%.2,16,17 This finding likely results from the fact that most patients with isolated c-ICA-O receiving BMT did not receive IVT (28% in our study, 15%–44% in previous studies).2,17 The low admission NIHSS in BMT patients may further contribute to low rates of ICH. In patients receiving EVT, prior reports have shown rates of sICH ranging from 0% to 7%,2,14,15,17,26 consistent with our results.
Of note, BMT patients had a higher rate of large artery atherosclerosis as stroke etiology which may signal bias by indication. The treating physicians’ may have assumed that patients with marked carotid bifurcation atherosclerosis or calcification had chronic lesions, which might be difficult to pass. Also, the anticipation of a more challenging technical procedure such as stenting combined with the necessity of more aggressive antithrombotic regimens, along with the knowledge that patients had a patent intracranial circulation, may have deterred clinicians from considering EVT. Finally, atherosclerotic carotid occlusions perceived as chronic can lead clinicians to understand the stroke mechanism as “hemodynamic,” and to favor medical interventions such as lying-flat head position, fluid administration and/or or use of vasoactive drugs. Previous studies also raised the question about treating symptomatic chronic c-ICA-O,28,29 with one study showing a successful recanalization rate of 58.7%. 29 Recanalization of symptomatic chronic occlusion was associated with an increased risk of sICH but with lower long-term risk of ipsilateral stroke. 29
The differences found between groups regarding risk factors, with higher prevalence of dyslipidemia and current smoking in the BMT group, and higher prevalence of atrial fibrillation and heart failure in the EVT group likely translates the differences in stroke etiology mentioned above.
Prespecified subgroup analyses were performed since previous studies have described that the benefits of EVT in isolated c-ICA-O could depend on stroke severity quantified by admission NIHSS, 17 or that stroke etiology can impact EVT outcome in patients with large-vessel intracranial occlusions. 30 However, no differences were found in our population as with other pre-treatment variables, namely IVT and time to hospital admission. As such, other subgroups of interest will need further assessment, as well as the impact of different treatment strategies.
Although no differences were found between treatment groups, we cannot exclude that it may be reasonable to offer medical therapy and close observation, with intervention if the patient deteriorates because of collateral failure or subsequent intracranial embolization. As such, predictors of clinical deterioration need to be defined and applied for a more patient-centered approach.31,32
The large number of patients across multiple countries, the rigorous statistical analysis incorporating sophisticated adjustments and subgroup analyses all form strengths of our study.
The retrospective design of our study has limitations. First, selection bias is evident, as reflected by the higher stroke severity and IVT rates in the EVT group. To mitigate this bias, we performed both IPTW and PSM analyses, along with subgroup analyses based on stroke severity and IVT use. Nonetheless, residual confounding may remain. This also applies to baseline imbalances in medical comorbidities, with patients in the EVT group having a higher prevalence of heart failure and atrial fibrillation.
Second, patients’ outcomes were assessed locally by unblinded adjudicators. Consequently, misclassification bias cannot be excluded. Third, differentiation of acute extracranial from intracranial carotid occlusion can be challenging on CTA and MRA.34 Rigorous measures were implemented to reduce the risk of misclassification. All baseline images had to be reviewed and specific recommendations to improve diagnostic accuracy were applied. While in patients undergoing DSA the risk of misdiagnosis is expected to be minimal, we cannot exclude misdiagnosis in the BMT.
Additional data regarding the patency and anatomical configuration of the circle of Willis, relevant to collateral capacity, could further help interpret our results. Moreover, we cannot exclude that small distal branch occlusions may have been missed and these may influence clinical outcomes. Nevertheless, the rate of “initially undiagnosed” distal branch occlusions are unlikely different between treatment groups and thus, probably a minor confounder. The lack of data on the use of distal protection devices and location of distal embolization, limits the interpretation of the risk and clinical impact of this complication. While patients with emergent carotid endarterectomy were excluded from our study, 5.4% of patients received carotid endarterectomy or stenting within 3 months, which might have impacted clinical outcomes. Finally, our study does not report outcomes beyond 3 months. Treatment modality might impact stroke recurrence not only in the early period, but also in the following course of months or even years. Thus, long-term follow-up would be a crucial element in future clinical trials.
Conclusion
In patients with isolated cervical internal carotid artery occlusion, endovascular treatment was associated with similar odds of disability and mortality, but potentially higher risk of intracranial bleeding. Baseline imbalances in patients’ characteristics between treatment groups, particularly admission NIHSS, need to be considered when interpreting these results, although our findings remained robust across different subgroups and several statistical approaches. Randomized-controlled clinical trials are warranted to establish optimal treatment for c-ICA-O.
Supplemental Material
sj-docx-1-eso-10.1177_23969873251323488 – Supplemental material for Endovascular treatment for isolated cervical internal carotid artery occlusion: ETIICA study
Supplemental material, sj-docx-1-eso-10.1177_23969873251323488 for Endovascular treatment for isolated cervical internal carotid artery occlusion: ETIICA study by João Pedro Marto, Christoph Riegler, Pimrapat Gebert, Tilman Reiff, Marek Sykora, Marcin Wiącek, David Pakizer, André Araújo, Adrien ter Schiphorst, João André Sousa, Arno Reich, Belen Flores Pina, Lukas Mayer-Suess, Cristina Hobeanu, Marialuisa Zedde, João Nuno Ramos, Georgios Tsivgoulis, Pedro Castro, Sven Poli, José Nuno Alves, Anne Dusart, Blanca Fuentes, Herbert Tejada Meza, Jelle Demeestere, Susanne Wegener, Lars Kellert, Patricia Calleja, Cristina Panea, Christoph Vollmuth, Liliana Pereira, Ronen R Leker, Timo Uphaus, Andrea Zini, Henrik Gensicke, Gauthier Duloquin, Taraneh Ebrahimi, Alexander Salerno, Cristina Tiu, Thanh N. Nguyen, Sebastian García-Madrona, Marta Bilik, Shadi Yaghi, Halina Sienkiewicz-Jarosz, Michał Karliński, Stefan Krebs, Eva Hurtíková, Nathalia Ferreira, João Sargento-Freitas, João Pinho, Isabel Rodriguez Caamaño, Elke Ruth Gizewski, Pierre Seners, Rosario Pascarella, Klearchos Psychogios, Alexandra Gomez Exposito, Sara Gomes, Flavio Bellante, Jorge Rodríguez-Pardo, Mario Bautista Lacambra, Robin Lemmens, Corinne Inauen, Johannes Wischmann, Fernando Ostos, Vlad Tiu, Karl Georg Haeusler, Miguel Rodrigues, Issa Metanis, Marianne Hahn, Maria Maddalena Viola, Simon Truessel, Yannick Bejot, Louisa Nitsch, Davide Strambo, Elena Oana Terecoasa, Mohamad Abdalkader, Alicia de Felipe, Farhan Khan, Caroline Arquizan, Manuel Ribeiro, Martin Roubec, Izabella Tomaszewska-Lampart, Julia Ferrari, Peter Ringleb and Christian H. Nolte in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of Hospital de Egas Moniz, Centro Hospitalar Lisboa Ocidental, and Charité – Universitätsmedizin Berlin, approved this study For all other centers, according to the local ethics committee regulations and national laws, each center was responsible for obtaining ethical approval for data collection and data sharing.
Informed consent
Informed consent was waived because of the retrospective nature of this study.
Guarantor
CN
Contributorship
JPM, CR, and CN researched literature and conceived the study. JPM checked the data for consistency and completeness. P.G conducted the statistical analysis. JPM, CR, PG, and CN wrote the first draft of the manuscript. All authors contributed with patient recruitment, reviewed and edited the manuscript and approved the final version of the manuscript
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.