
Abstract
Introduction:
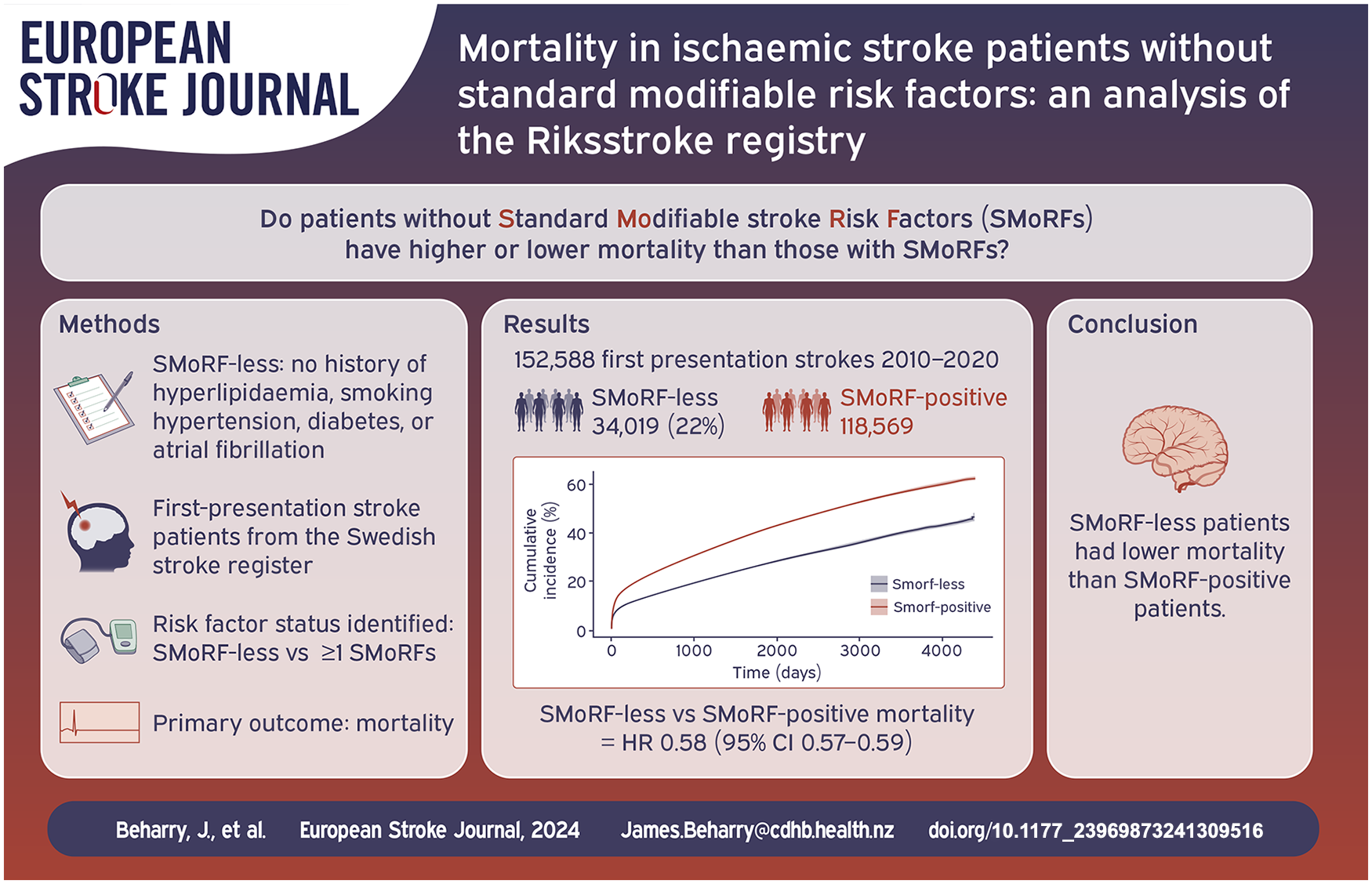
Little is known of the long-term prognosis of patients with acute ischaemic stroke in the absence of standard modifiable stroke risk factors (SMoRFs). In acute coronary syndromes, patients without modifiable risk factors have a higher mortality rate. We analysed data from the Swedish Stroke Register to determine survival of patients without SMoRFs following an ischaemic stroke.
Patients and methods:
We identified adult patients with first-presentation acute ischaemic stroke between 2010 and 2020. Patients were considered to possess a SMoRF if they had one of: hypertension, diabetes, hyperlipidaemia, atrial fibrillation or an active smoking history. We compared mortality in patients with and without SMoRFs following first-presentation ischaemic stroke using cox regression models. We also assessed the combined endpoint death and dependency (mRS 3–6) at 3 months via logistic regression models.
Results:
Of 152,588 patients with ischaemic stroke, hypertension (58.7%) and atrial fibrillation (27.3%) were the most common risk factors. 34,019 patients (22.3%) had no SMoRFs. After a first-presentation ischaemic stroke, patients without SMoRFs had a lower risk of death than patients with one or more SMoRFs (HR 0.58 [95% CI 0.57–0.59]). The absence of SMoRFs was associated with lower odds of death and dependency at 3 months in logistic regression models (OR 0·60 [95% CI 0.58–0.62]).
Conclusion:
One in five patients with acute ischaemic stroke had no standard modifiable stroke risk factors. These patients have lower risk of death compared to patients with one or more SMoRFs.
Introduction
Hypertension, diabetes, hyperlipidaemia, and active smoking are recognised as standard modifiable risk factors in coronary artery disease and ischaemic stroke.1–3 A registry study investigating the ‘Swedish Web-System for Enhancement and Development of Evidenced-Based Care in Heart Disease Evaluated According to Recommended Therapies’ (SWEDEHEART) found that 14.9% of patients with first-presentation ST-elevation myocardial infarction (STEMI) did not have any of the standard modifiable cardiovascular risk factors, collectively known as ‘SMuRFs’. At 1 month, patients without SMuRFs had higher all-cause mortality compared to patients with at least one SMuRF. 4 While modifiable cardiovascular risk factors are implicated in the majority of ischaemic strokes, similar to coronary artery disease, a minority of patients presenting with stroke do not have vascular risk factors.1,5–7
‘SMuRF-less’ patients do not have a history of diabetes, hypertension, hyperlipidaemia, and are not active smokers.
4
There has been limited literature describing ‘SMuRF-less’ patients who present with ischaemic stroke, and the incidence of recurrent stroke and mortality outcomes are unknown.5,6 As such, outcomes in SMuRF-less patients may have implications for secondary prevention.
8
In addition to SMuRFs, atrial fibrillation is a significant risk factor in ischaemic stroke.
9
SMoRFs (
Using data collected in the national Swedish stroke registry, we assessed the prevalence, mortality and recurrent stroke rates of SMoRF-less patients presenting with a first ever ischaemic stroke, and performed a comparative analysis with patients with one or more SMoRFs.
Methods
Data source and study population
The Swedish Stroke Register, Riksstroke, collects clinical data on all patients in Sweden presenting with an acute stroke. The register, which performs well in validation studies, was established in 1994, and over 20,000 stroke events are recorded yearly.10–12 All hospitals providing acute stroke care in Sweden contribute data to Riksstroke, and the estimated coverage of all acute stroke events is >90%.11–13
We identified patients 18 years or older presenting between 2010 and 2020 (inclusive) with a first-ever presentation of ischaemic stroke. Riksstroke collects data during a patient’s inpatient stroke admission in addition to patient reported outcome measures at 3 months and 1 year.10,13 Data related to the acute admission are entered from hospital charts. This includes relevant demographics (age and sex), level of consciousness on admission (alert, drowsy or unconscious), the presence or absence of stroke risk factors, treatment details relating to the use of intravenous thrombolysis or endovascular thrombectomy and secondary prevention upon discharge. Pre-stroke accommodation (own accommodation or institutional living including nursing home care or equivalent) and whether assistance is required to perform personal activities of daily living (p-ADL) is also recorded. Dependence for p-ADL is defined by one or more of: assistance moving around indoors, assistance toileting, and assistance dressing. Three month and 1-year follow-up data are based on patient questionnaires that are either completed at a follow-up visit or over the phone by the treating hospital, or alternatively, by the patient or family and returned by mail. 13 A modified Rankin Scale (mRS) transformation algorithm uses functional measures reported at 3 months to classify patients as functionally independent (mRS 0–2) or dead or dependent (mRS 3–6). 14 Riksstroke also collects mortality data by individual patient data linkage with the Cause of Death Register managed by the National Board of Health and Welfare. This register is considered to have close to complete coverage of all deaths in Sweden. 15
Definition of SMuRF and SmoRF cohorts
Collection of data related to stroke risk factors in Riksstroke include: diabetes, hypertension, hyperlipidaemia, smoking status and atrial fibrillation. Previously known or recently identified diabetes mellitus was based on medical records or testing during the hospital stay. A history of hypertension was determined based on whether a patient was on treatment for hypertension at the onset of stroke, and a history of hyperlipidaemia where the patient was on treatment with a statin at the onset of stroke. A past history or new diagnosis of atrial fibrillation (including intermittent fibrillation or flutter) was based on medical records or in-hospital testing. Active smoking status was defined as having one cigarette or more/day or having quit during the last 3 months. ‘SMuRF-less’ patients were defined as those without a history of diabetes, not treated with anti-hypertensives or statin at the onset of stroke, and who are not active smokers. ‘SMoRF-less’ was defined as ‘SMuRF-less’ patients with no past history or new diagnosis of atrial fibrillation. ‘SMoRF-positive’ patients have one or more of the following: hypertension, hyperlipidaemia, diabetes, active smoking or atrial fibrillation. The primary aim of our study was to compare patients stratified by SMoRF status.
Outcomes
The primary outcome was time to death after first-presentation ischaemic stroke. Follow-up completion was defined as either the individuals date of death or December 2020. Secondary outcomes included recurrent stroke and the combined outcome of death or dependence (corresponding to mRS 3–6) which was measured at 3 months.
Recurrent stroke for any individual was defined by a further event recorded in the Swedish Stroke Register.
Statistical analysis
Categorical and dichotomous variables were summarised as frequencies and percentages. Numerical variables were summarised as a median (IQR). Correspondingly, Chi-square and Mann Whitney-U were used when evaluating baseline patient characteristics in SMoRF-less patients compared to SMoRF-positive patients.
We used cumulative incidence functions to calculate crude incidence of death and recurrent stroke at 1 month, 3 months and 1 year. We used cause specific Cox regression models to assess the risk of death and recurrent stroke and also included Fine-Grey subdistribution hazard models to account for death acting as a competing risk for recurrent stroke. Hazard ratios (HR) from conventional cause-specific Cox regression models are reported, and HRs from the subdistribution models are included in
In addition to univariable models, we used multivariable models to adjust for possible confounders and mediators in in two steps. In the first step, we adjusted for imbalances in age and sex. In the second step we performed additional adjustment for both confounders and mediators including; level of consciousness on admission, pre-stroke institutional living and personal activities of daily living (p-ADL) dependency. Age was added as a continuous covariate. We assessed the linear assumption by adding a quadratic term (age 2 ). This had no major influence on the model coefficients, so the simpler model, including age as a linear term was chosen.
While the primary comparison groups were SMoRF-less patients compared to patients with one or more SMoRFs (SMoRF-positive), we also performed several sensitivity analyses. We first compared outcomes in SMuRF-less patients compared to patients with one or more SMuRFs, where patients with atrial fibrillation were included in both groups. We then compared SMuRF-less patients to patients with one or more SMuRFs excluding patients with atrial fibrillation from both groups. An additional age stratified analysis of death and recurrent stroke with a cut-off of 55 years was completed. We also compared outcomes in female and male patients separately.
During the regression estimation, if any of the covariates used in the model was missing for a given individual, that individual was omitted from the analysis (complete case analysis). In the full multivariable regression, 6366 (4.17%) individuals had a missing value in any of the covariates.
A two-sided p-value of less than 0.05 was considered to indicate statistical significance. Statistical analysis was completed using R version 4.2.0. 16 Cumulative incidence functions and sub-distribution hazard models were estimated using ‘tidycmprsk’ and ‘cmprsk’ packages.17,18 The cause-specific model was estimated using the ‘survival’ package. 19
Data sharing, ethics approval and registration
The authors declare that all data and methodological detail are available within the article and online supplement. This study is based on data from a third party (Riksstroke) and its use has been approved by the Swedish ethical review Authority (reference number 2022-03707-01). According to Swedish legislation, data cannot be made available for use beyond what has been approved by the ethical review board. Therefore, the data cannot be made publicly available. Data may be made available from Riksstroke (contact via
Results
During the study period, 152,588 patients presented with a first ever ischaemic stroke and the median follow-up time was 3.3 years (IQR 1.2–6.4). Of these patients, 34,019 (22%) were SMoRF-less. The percentage of patients presenting with a first ever stroke who were SMoRF-less remained similar across the study period (Supplemental Table 5). Table 1 summarises baseline characteristics including demographics, pre-stroke function, and acute treatment in all groups. The median age was 72 years (IQR 61–81) in SMoRF-less patients and 77 years (IQR 69–85) in patients with one or more SMoRFs. The median age of female patients was 80 (IQR 70–87), and the median age of male patients was 73 (IQR 70–87). Males made up 52.1% of all patients presenting with first-ever stroke and represented a greater proportion of SMoRF-less patients (54.6%) compared to SMoRF positive patients (51.3%). Hypertension was the most common risk factor (58.7%), followed by atrial fibrillation (27.3%), hyperlipidaemia (22.5%), diabetes (20.6%), and active smoking (15.7%). Compared to SMoRF-less patients, SMoRF-positive patients were more likely to present with depressed conscious state (drowsy or unconscious) and were less likely to receive thrombolysis or experience symptomatic intracranial haemorrhage. There was no difference in treatment with endovascular clot retrieval.
Baseline characteristics stratified by SMoRF status.

SMoRF: standard modifiable stroke risk factor; IQR: interquartile range; NA: not applicable; sICH: symptomatic intracranial haemorrhage.
Analysis of SMoRF-less compared to SMoRF-positive patients
SMoRF-less patients had a lower risk of death than SMoRF-positive patients (HR 0.58 [95% CI 0.57–0.59]) (Figure 1, Supplemental Table 2). The risk death was lower in SMoRF-less patients compared to SMoRF-positive patients at 1 month (6.64% vs 10.6%, RR 0.63 [95% CI 0.6–0.7]), 3 months (9.22% vs 14.6%, RR 0.63 [95% CI 0.61–0.65]), and 1 year (13.2% vs 20.9%, RR 0.63 [95% CI 0.61–0.65]) (Supplemental Figure 1). In adjusted survival models, SMoRF-less status continued to be associated with a lower risk of death than SMoRF-positive status after adjustment for age and sex (HR 0.74 [95% CI 0.72–0.75]), and after further adjustments for level of consciousness at admission, institutional living and p-ADL dependency (0.74 [95% CI 0.73–0.76]) (Supplemental Tables 3 and 4).
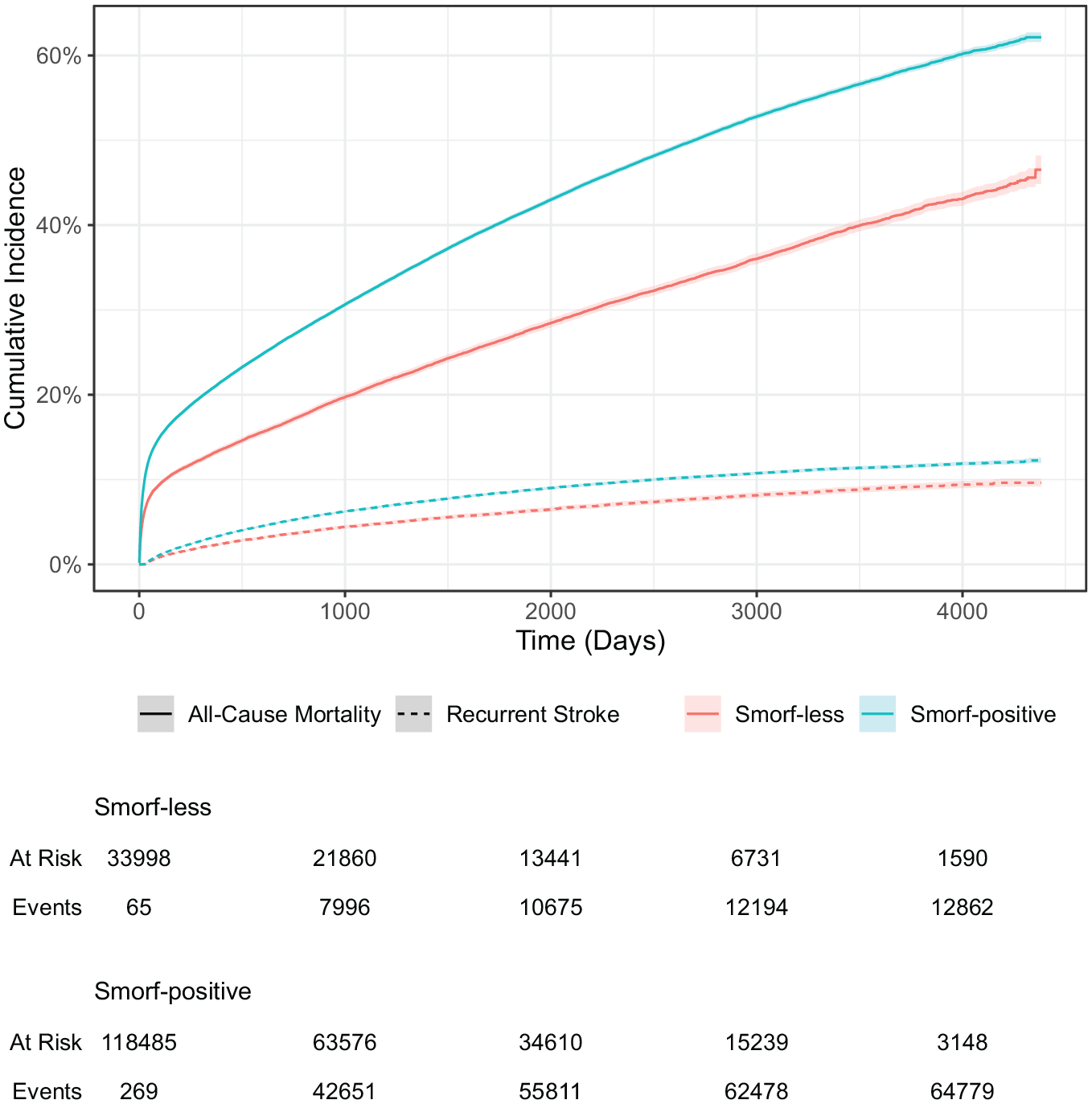
Cumulative incidence curves for risks of a second stroke or death, stratified by SMoRF-status.
In females, the risk of death was 12.6% at 1 month and 24.4% at 1 year in SMoRF-positive patients, and 7.8% and 15.5% respectively in the SMoRF-less female cohort (HR 0.58 [95% CI 0.56–0.59]). In males, the risk of death was 8.47% at 1 month and 17.6% at 1 year in SMoRF-positive patients, and 5.66% and 11.2% respectively in the SMoRF-less male cohort (HR 0.59 [95% CI 0.58–0.60]) (Supplemental Figure 3). Age-stratified analysis revealed a more pronounced difference in patients under 55 years of age (HR 0.55 [CI 0.48–0.64]) than in older patients (HR 0.66 [95% CI 0.65–0.67]).
The rate of recurrent stroke at 1 year was 2.27% in SMoRF-less patients and 3.23% in SMoRF-positive patients (Figure 1, Supplemental Figure 2). The risk of recurrent stroke was lower in SMoRF-less patients compared to SMoRF-positive patients (HR 0.63 [95% CI 0.60–0.66]), and remained lower following adjustment for age and sex (HR 0.71 [CI 0.68–0.74]), and subsequent additional adjustment for level of consciousness at admission, institutional living and p-ADL dependency (HR 0.71 [95% CI 0.68–0.75]).
In crude logistic regression models assessing death and dependency at 3 months, SMoRF-less status was associated with a lower risk of death or dependency (OR 0.60 [95% CI 0.58–0.62]). After initial adjustment for age and sex, SMoRF-less status remained independently associated with a lower risk of death or dependency at 3 months (OR 0.80 [95% CI 0.77–0.83]). These findings continued to remain consistent with additional adjustments for level of consciousness at admission, institutional living and p-ADL dependency (OR 0.80 [95% CI 0.77–0.83]).
Analysis of SMuRF-less compared to SMuRF-positive patients
SMuRF-positive patients are defined by a history of one or more of the following: hypertension, hyperlipidaemia, diabetes or active smoking. SMuRF-less patients have no history of standard modifiable cardiovascular risk factors. Patients with atrial fibrillation are therefore included in both comparator groups when stratified by SMuRF status. When the groups compared were defined by SMuRF status, SMuRF-less patients had lower mortality compared to patients with one or more SMuRFs (HR 0.72 [95% CI 0.71–0.74]). Recurrent stroke was also lower in SMuRF-less patients compared to SMuRF positive patients (HR 0.66 [95% CI 0.64–0.69]. When all patients with atrial fibrillation were excluded from the analysis, SMuRF-less patients had lower mortality compared to SMuRF-positive patients (HR 0.76 [95% CI 0.74–0.77]). When considering only patients with atrial fibrillation, SMuRF-less patients with atrial fibrillation had lower mortality than SMuRF-positive patients with atrial fibrillation at 1 year (30.3% vs 32%, RR 0.95 [95% CI 0.91–0.96]) and follow-up completion (HR 0.84 [95% CI 0.81–0.87]) (Supplemental Figure 4).
Discussion
We present the largest comprehensive registry study exploring the relationship between an absence of standard modifiable stroke risk factors and outcome following first-presentation ischaemic stroke. Over 150,000 patients presented with a first ever ischaemic stroke during the 11-year study period, and one in five of these patients had no recognised SMoRFs. SMoRF-less patients presenting with first-presentation ischaemic stroke had significantly lower short and long-term mortality than patients with one or more SMoRFs, although the incidence of death in patients both with and without risk factors was high. The rate of recurrent stroke was also lower in SMoRF-less patients when compared to SMoRF-positive patients.
There have been few reports investigating the relationship between mortality following ischaemic stroke and an absence of common stroke risk factors. A study including almost 5000 consecutive patients from the ASTRAL (Acute Stroke Registry and Analysis of Lausanne) stroke registry reported long-term outcome in patients without established vascular risk factors as defined by the INTERSTROKE and Global Burden of Disease stroke risk factor studies.1,5,20 Unadjusted mortality at 1 year was similar in patients with and without established vascular risk factors, and an adjusted model examining mortality and recurrent stroke revealed worse outcomes in patients without established risk factors. A single-centre retrospective study including only patients less than 65-years of age found no difference in in-hospital mortality comparing SMuRF-positive patients and SMuRF-less patients, but did not report long-term outcomes. 6 Despite our finding that one in five patients presenting with first-presentation ischaemic stroke are SMoRF-less and have an appreciable mortality rate, they are under-represented in current literature.
Our primary outcome analysis revealed higher mortality in SMoRF-positive patients compared to SMoRF-less patients with increasing divergence of mortality rate over time. While mortality was lower in SMoRF-less patients, a significant proportion (13.2%) of patients were dead at 1 year. Females had higher mortality than male patients, where one in four SMoRF-positive females were dead 1 year following a first ischaemic stroke compared to one in six SMoRF-positive males. In Sweden between 2010 and 2020 the average death rate in patients 70–79 years-of-age was just over 2300 per 100,000 population per year, meaning mortality in patients following first-presentation ischaemic stroke is significantly higher than baseline population death rates. 21 Mortality rates reported in other contemporary studies following first-presentation ischaemic stroke are similar to our findings.22–24 Rates of recurrent stroke, were relatively low compared to mortality, which has also been demonstrated in other studies.22,25 It is important to note there is underreporting of recurrence within the first 28 days of stroke in the Swedish Stroke register, primarily due to the difficulties differentiating whether further symptoms represent a new or recent event. Recurrent stroke did not appear to drive ongoing mortality rates in patients who initially survived a first ischaemic stroke in our study. We did not investigate cause of death. Following a non-fatal ischaemic stroke, important causes of death identified in other large cohorts have included cardiac disease, respiratory disease (acute infections and chronic obstructive pulmonary disease) and malignancy.23,26 This has implications for secondary prevention and highlights the importance of managing comorbidities such as other cardiovascular disease, and potentially screening for other conditions such as malignancy in some patients.5,23 Our age stratified analysis revealed significantly higher mortality in SMoRF-positive patients compared to SMoRF-less patients younger than 55-years of age, but further investigation including examination of specific stroke aetiologies in this cohort is needed.
Our analysis also suggests atrial fibrillation is associated with increased mortality following first-presentation ischaemic stroke. Roughly one in three patients with atrial fibrillation were dead 1 year following a first ischaemic stroke. High rates of mortality in patients with atrial fibrillation and ischaemic stroke have been previously described.27,28 We did not investigate cause of death in our study, and we are therefore unable explore any possible differences in the distribution of various causes of death between patients with and without atrial fibrillation following a first-presentation ischaemic stroke.
A study analysing data from the SWEDEHEART registry found that mortality 1 month after first-presentation STEMI is higher in SMuRF-less patients compared to those with one or more SMuRFs. 4 This difference was driven primarily by cardiovascular mortality, with the most likely specific mechanism being arrhythmia. Mortality remained higher in SMuRF-less patients until roughly 9 years following the index event, but female SMuRF-less patients had higher mortality at complete follow-up compared to SMuRF-positive females. Our findings are not consistent with this same phenomenon and several possibilities for this exist. Firstly, the vast majority of myocardial infarction is caused by culprit vessel atherosclerotic disease, whereas the pathogenesis in cerebral infarction is more varied. 29 While atherosclerotic disease is implicated in stroke frequently, cardioembolic aetiologies are also common. Despite some similarity in risk factor association between stroke and myocardial infarction, these inherent differences in underlying aetiology likely alter the interaction between the presence of relevant risk factors and prognosis following an event. We were unable to stratify patients by underlying stroke pathogenesis using the widely used TOAST criteria as these data are not collected in the Swedish Stroke register. Additionally, arrhythmia following cardiac tissue damage is specific to myocardial infarction, and no comparable fatal complication exists following cerebral infarction, although there is some evidence that infarction in the right insular region may have cardiac effects. 30 Given our primary focus was comparing patients as defined by SMoRF status (with inclusion of atrial fibrillation as a risk factor) any direct comparisons between the findings of our study and those in the cardiac literature describing patients without standard modifiable cardiovascular risk factors must be made cautiously. 4 We did perform additional sensitivity analysis defining comparison groups by SMuRF status, both including and excluding patients with atrial fibrillation. This revealed lower mortality in SMuRF-less patients with ischaemic stroke compared to SMuRF-positive patients.
Both SMuRF-less and SMuRF-positive female patients had almost double the mortality rate of equivalent male patients at 30 days following STEMI. Our data has also shown a higher mortality in female patients than male patients (12.9% and 24.4% at 1 month and 1 year respectively in SMoRF-positive female patients compared to 8.47% and 17.6% at 1 month and 1 year respectively in male patients). In our cohort the median age of females was higher than males in patients presenting with a first ever stroke which at least in part explains this difference in mortality. In other studies examining sex differences in the Swedish stroke registry, mortality differences between males and females were less profound following age adjustment. 31 Regardless, the higher mortality following both ischaemic stroke and STEMI in females highlights the importance of future research into other potential causes for these differences and may also indicate the need for sex specific management in both disease processes.
Our study has a number of strengths. We included over 150,000 patients from the Swedish Stroke registry making this the largest and most comprehensive study of first-presentation ischaemic stroke in patients without risk factors. The Riksstroke registry also has high coverage (>90%) of all stroke events in Sweden, and data quality is considered to be accurate. 12 Data linkage with the Swedish Cause of Death Register, a register with close to complete coverage, has allowed us to assess individual patient mortality at multiple time points.
Limitations of our study include the definition of some SMoRFs, with a patient considered to have a pre-stroke diagnosis of hypertension or hyperlipidaemia if they had been treated with an antihypertensive or lipid lowering therapy prior to admission with first-presentation stroke. This may mean some patients with previously undiagnosed or untreated hypertension or hyperlipidaemia may be mis-classified. We did not have data to allow for a biochemical diagnosis of diabetes or hyperlipidaemia. While baseline rates of hypertension are similar to other studies in similar patient populations, rates of hyperlipidaemia are lower than expected.4–6 This could possibly be explained by poor adherence to statin therapy observed in some cohorts. 32 Our study did not assess all risk factors associated with stroke, and in addition, we were unable to report stroke mechanism. 1 National Institutes of Health Stroke Scale (NIHSS) was not routinely recorded for patients throughout the study period, meaning in adjusted models, level of consciousness, which has shown to be a good approximation for NIHSS, acted as a surrogate for stroke severity. 33 Furthermore, ethnicity data was not collected, meaning our results may not be generalisable.
In conclusion, the risk of death following a first-ever ischaemic stroke is higher in patients with standard modifiable stroke risk factors (SMoRFs) compared to those without risk factors. The need for improved knowledge regarding mechanisms and risk factors for stroke is illustrated by the 20% of first-time stroke patients with no SMoRFs. In contrast to the higher early mortality in SMuRF-less STEMI patients compared to those with traditional risk factors, SMoRF-less stroke individuals were observed to have improved outcomes compared to those with at least one standard modifiable stroke risk factor. Further efforts are needed to identify new stroke mechanisms and risk factors, so that more effective primary prevention approaches that reduce stroke and its associated mortality are available to patients with and without conventional risk factors.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241309516 – Supplemental material for Mortality in ischaemic stroke patients without standard modifiable risk factors: An analysis of the Riksstroke registry
Supplemental material, sj-docx-1-eso-10.1177_23969873241309516 for Mortality in ischaemic stroke patients without standard modifiable risk factors: An analysis of the Riksstroke registry by James Beharry, Vignan Yogendrakumar, Guilherme W. F. Barros, Stephen M Davis, Bo Norrving, Gemma A Figtree, Geoffrey Donnan, Mia von Euler and Marie Eriksson in European Stroke Journal
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SD reports personal fees from Amgen, Boehringer Ingelheim, Medtronic, Abbot, and CSL Behring. BN reports personal fees for DSMB work for Simbec-Orion.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Ethical approval for this study was obtained from the Swedish ethical review Authority (reference number 2022-03707-01).
Informed consent
Informed consent was not sought for the current study. Riksstroke has been approved by the Regional Ethical Review Board at Umeå University. All included patients have been informed about registration in Riksstroke. Patients are informed that their data may be used for research purposes and that they can opt out or withdraw their data at any time.
Guarantor
JB
Contributorship
GD, SD, and GF conceived the study. All authors contributed to study design and methodology. ME and MvE submitted and gained ethics approval from the national ethics review authority. ME and GB contributed to formal data analysis. JB, VY, GB, and ME drafted the manuscript. JB led drafting of the manuscript and the editing process. All authors contributed to interpretation of results and to editing of the final manuscript. All authors approved the manuscript content and approved the submission.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability
According to Swedish legislation, data cannot be made available for use beyond what has been approved by the ethical review board. Therefore, the data cannot be made publicly available. Data may be made available from Riksstroke (contact via
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.