
Abstract
Introduction:
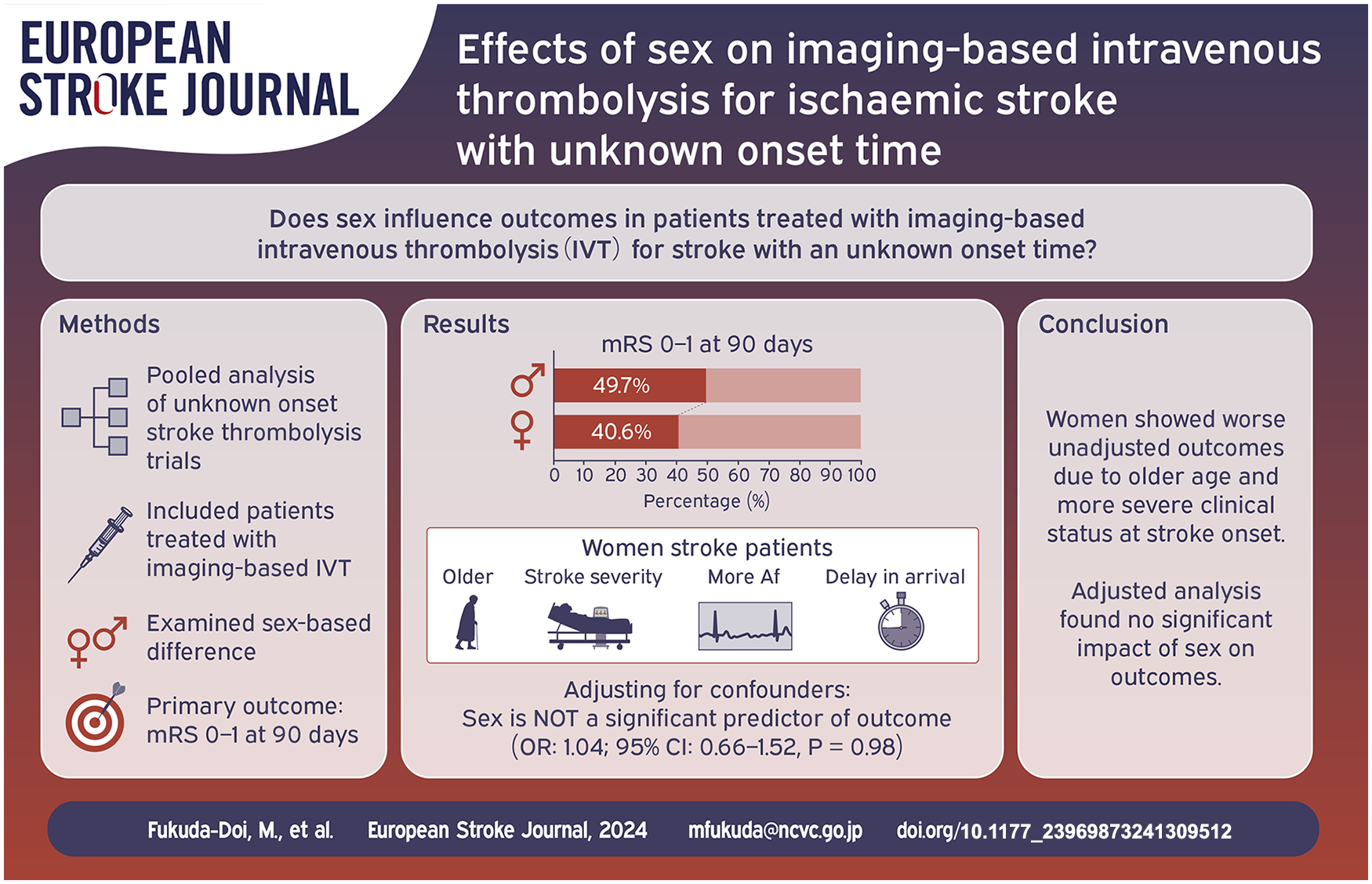
The effects of imaging-based intravenous thrombolysis on outcomes based on patient sex remain unclear. We aimed to investigate whether outcomes among patients with stroke with an unknown onset time and treated with imaging-based intravenous thrombolysis are influenced by their sex.
Patients and Methods:
This study was a pooled analysis of individual patient-level data acquired from the Evaluation of unknown Onset Stroke thrombolysis trials. Patients treated with imaging-based intravenous thrombolysis for stroke with an unknown onset time were included. The primary outcome was a favourable outcome (modified Rankin Scale score 0–1) at 90 days. The sex-based difference in outcomes was studied using mixed-effect logistic or ordinal regression models, considering potential heterogeneity across trials.
Results:
Out of 509 patients in total, 204 (40.1%) were women. Compared with men, women were older and more likely to have atrial fibrillation. Baseline National Institutes of Health Stroke Scale score was higher and hours from last-known-well to treatment were longer for women than for men. Favourable outcomes occurred less often among women than among men. However, multivariate adjustment revealed a non-significant association between female sex and favourable outcome (adjusted odds ratio: 1.04 [95% confidence interval: 0.66–1.52], p = 0.98).
Discussion and conclusion:
Pooled data from the included clinical trials showed that women with ischaemic stroke with an unknown onset time had worse functional outcomes following imaging-based intravenous thrombolysis than did men. However, this sex-based difference can be explained by the higher age and more severe clinical status at onset among women.
Introduction
The aetiology, incidence, and outcome of stroke differ between men and women.1,2 Although age-adjusted stroke incidence is lower in women than in men, women have a higher lifetime stroke risk than men because of their longer life expectancy, as stroke incidence is higher at older ages than at younger ages. Women have worse functional outcomes and lower health-related quality of life following a stroke than men. Inconsistent results regarding sex differences in clinical outcomes after intravenous thrombolysis (IVT) for patients with acute ischaemic stroke have been reported. Several post-hoc analyses of clinical trials have demonstrated comparable clinical outcomes between sexes.3–5 In contrast, pooled analyses of stroke registries suggest that women have poorer functional outcomes after IVT than men.6,7 The Safe Implementation of Treatments in Stroke-International Stroke Thrombolysis Register revealed that men had a higher risk of symptomatic intracerebral haemorrhage (ICH) and mortality than women. 8 However, these studies have focussed on IVT within 4.5 h of onset; hence, patients with an unknown time of symptom onset were excluded.
Our recent systematic review and meta-analysis of individual patient data (IPD) (Evaluation of unknown Onset Stroke thrombolysis trials (EOS)) demonstrated that imaging-based IVT, determined by a diffusion-weighted imaging-fluid attenuated inversion recovery (DWI-FLAIR) mismatch in magnetic resonance imaging (MRI) or perfusion mismatch in either MRI or computed tomography (CT), improved the functional outcome at 90 days for patients who had a stroke with an unknown time of onset. Although the p-value for the statistical interaction of sex on the functional outcome was non-significant, the efficacy of alteplase was inconclusive among women, whereas in men, alteplase significantly increased the odds of a favourable outcome. However, uncertainty remains on how sex differences affect the odds of an excellent recovery following an imaging-based selection protocol for IVT for patients who had a stroke with an unknown onset time. By analysing the data from cooperative and high-quality international trials, this study aimed to investigate whether the clinical futures and outcomes among patients who had an ischaemic stroke with an unknown onset time and were treated with imaging-based IVT are based on their sex.
Patients and methods
This study comprised a secondary pooled analysis of IPD acquired from the EOS collaboration, a systematic review and meta-analysis of clinical trials (PROSPERO, CRD42020166903), compared imaging-based IVT using alteplase versus standard care or placebo for adult patients who had stroke with an unknown onset time. 9 Four RCTs (WAKE-UP, 10 EXTEND, 11 THAWS12,13 and ECASS-4 14 ) one single-arm trial, MR WITNESS, 15 provided de-identified IPD for analysis. Only patients treated with imaging-based IVT for stroke with an unknown onset time were included in this study.
The obtained IPD included patient demographics, baseline clinical features (National Institutes of Health Stroke Scale (NIHSS) score, onset type, and time course from last-known-well (LKW) to IVT), imaging details ( occlusion site, infarct core volume), and outcomes such as haemorrhagic events following IVT, mortality, and 90-day functional outcomes. The primary outcome was a favourable functional recovery at 90 days, defined by a modified Rankin Scale (mRS) score of 0–1. Secondary outcomes included an mRS shift towards better function and death within 90 days.
Baseline characteristics were compared between men and women. Categorical variables are expressed as proportions (%) and continuous variables as means ± standard deviations or medians (interquartile ranges (IQRs)), as appropriate. Chi-squared tests were used for categorical variables, while t-tests or Mann–Whitney U tests were applied for continuous variables. Mixed-effect logistic or ordinal regression models adjusted for age, atrial fibrillation, NIHSS score, infarct core volume, LVO presence and LKW-to-IVT time, with trial as a random intercept effect were used to evaluate associations between sex and outcomes. Multiple imputations were used for missing data, with sensitivity analyses conducted without imputation.
The EOS dataset did not include individual premorbid mRS scores. Four trials (WAKE-UP, EXTEND, THAWS and ECASS-4) excluded patients with a premorbid mRS score > 1, while MR WITNESS included 11 patients with scores ⩾ 2. To minimise bias, a sensitivity analysis excluding MR WITNESS was performed. Subgroup analyses were done for variables like age, atrial fibrillation, previous stroke, antiplatelet use, alteplase dose, NIHSS score, LVO presence, infarct volume, and time from LKW to IVT. Odds ratios with 95% confidence intervals were calculated, and p < 0.05 was considered significant. Analyses were conducted using STATA/SE 16.1 (StataCorp LLC., College Station, TX, USA).
Results
From the five clinical trials, data from 509 patients treated with imaging-based IVT were included for analysis (Figure 1). Among the patients, 204 (40.1%) were women. Compared with men, the women were significantly older (70 ± 12 years vs 67 ± 13 years, p = 0.003) and more likely to have atrial fibrillation (27.6% vs 17.2%, p = 0.005). A higher percentage of women were taking antiplatelet medications at baseline (45.5% vs 36.4%, p = 0.045, Table 1).
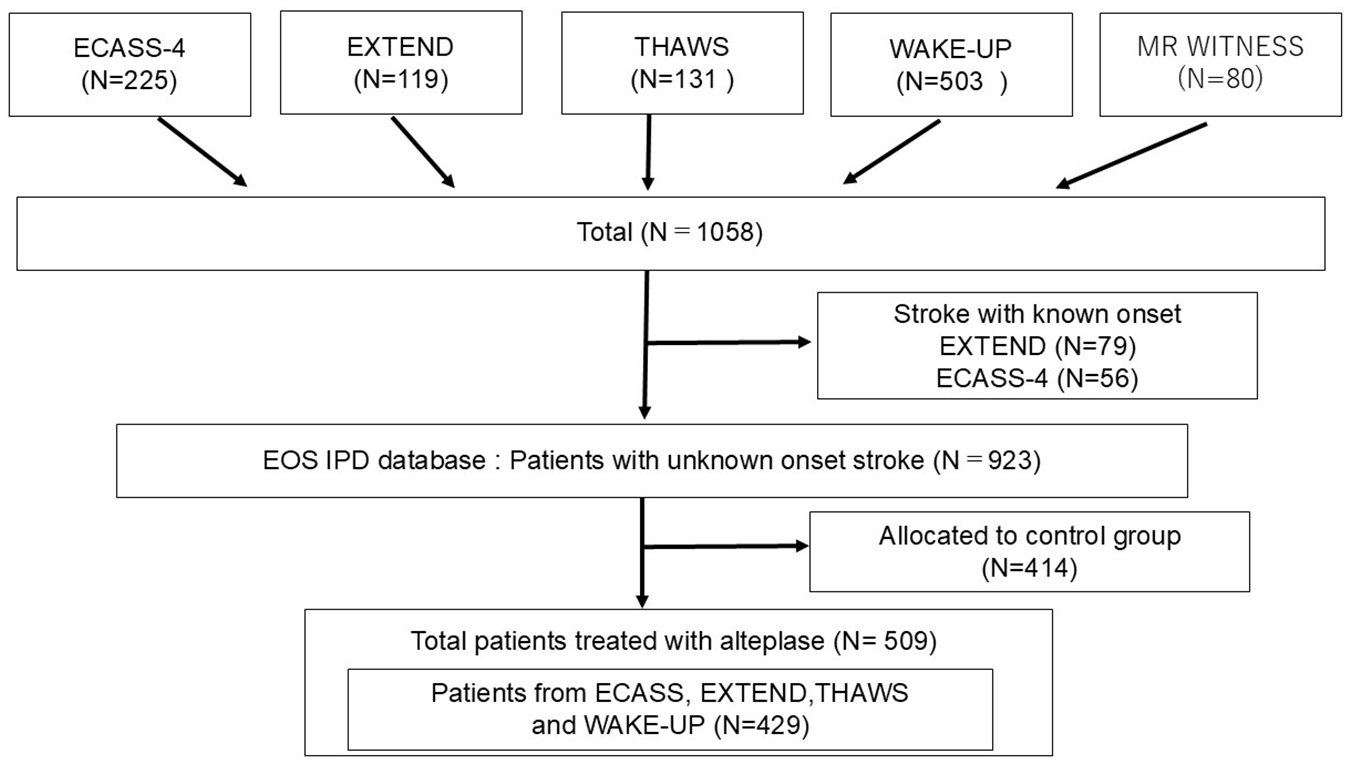
Data flow diagram.
Baseline characteristics of patients.

SD: standard deviation; TIA: transient ischaemic stroke; NIHSS: National Institutes of Health Stroke Scale; LKW: last-known-well.
Their baseline NIHSS score was higher (8.0 [IQR, 5–15] vs 6.0 [IQR, 4–11], p < 0.001), and LVO was more frequently observed (33.6% vs 20.4%, p = 0.004), whereas their infarct core volumes were comparable (2.8 [IQR, 0.9–16.3) ml vs 2.5 [IQR, 0.7–9.9] ml, p = 0.29). A significantly greater time delay in treatment from LKW was observed in women (11.2 [IQR, 9.3–12.9] h vs 10.3 [IQR, 8.1–11.9] h, p < 0.001) than in men; however, the duration from symptom recognition to IVT treatment was comparable (3.3 [IQR, 2.6–4.2] h vs 3.3 [IQR, 2.6–4.1] h, p = 0.87) between the sexes.
The distribution of mRS score based on sex is shown in Figure 2. Favourable outcomes (mRS 0–1) occurred in 80 (40.6%) women and 150 (49.7%) men (p = 0.047). Among the patients, 19 (9.6%) women and 15 (5.0%) men died within 90 days (p = 0.042). Symptomatic ICH following IVT was observed in four (2.0%) women and eight (2.6%) men (p = 0.63). Multivariate adjustment revealed that female sex was not significantly associated with favourable functional outcomes (adjusted OR, 1.04 [95% CI, 0.66–1.52]; p = 0.98) or death (adjusted OR, 1.24 [95% CI, 0.57–2.68]; p = 0.59; Table 2).
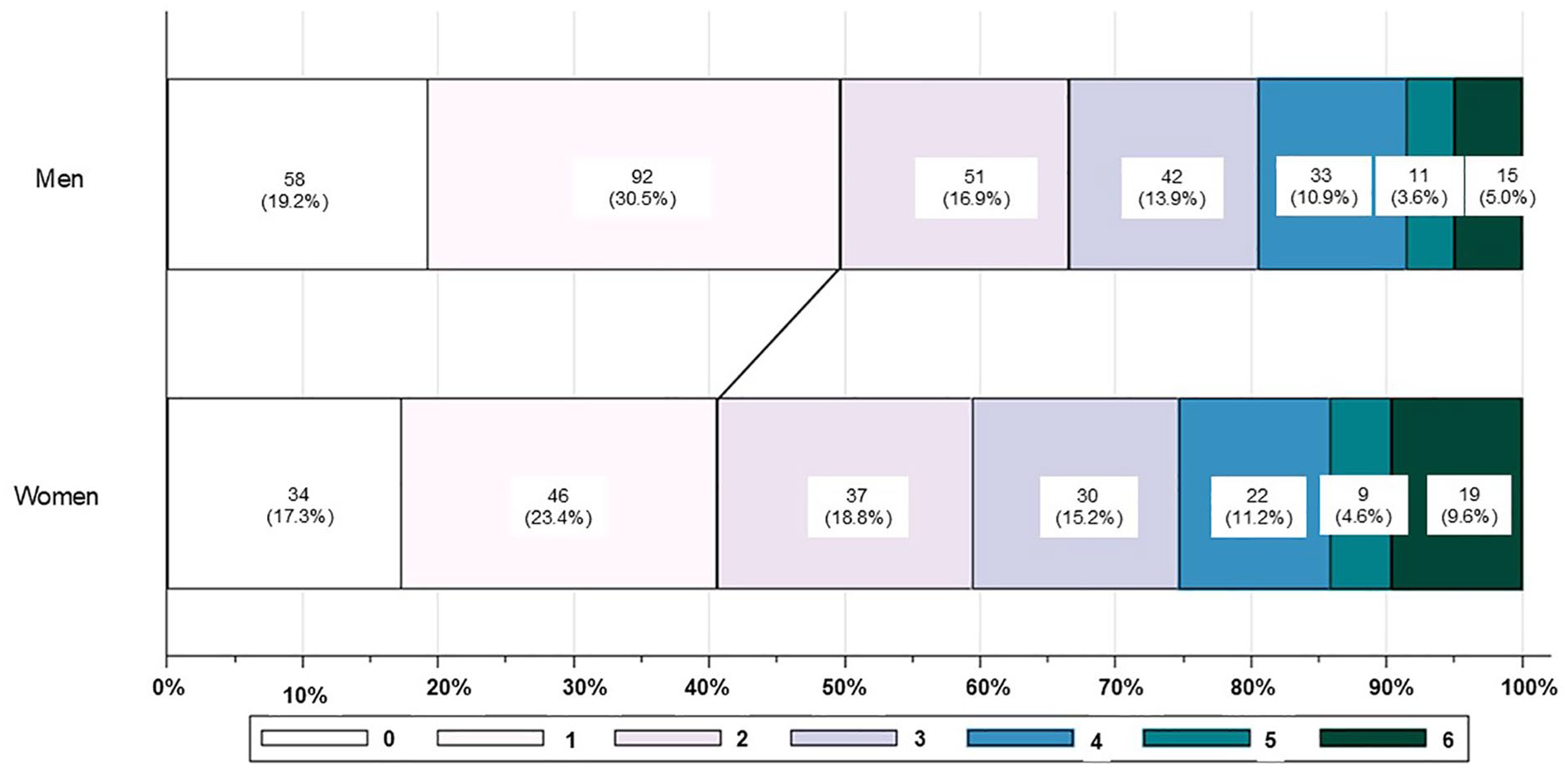
Modified Ranking Scale (mRS) distribution at 90 days based on sex.
Sex difference in outcomes (all trials included).
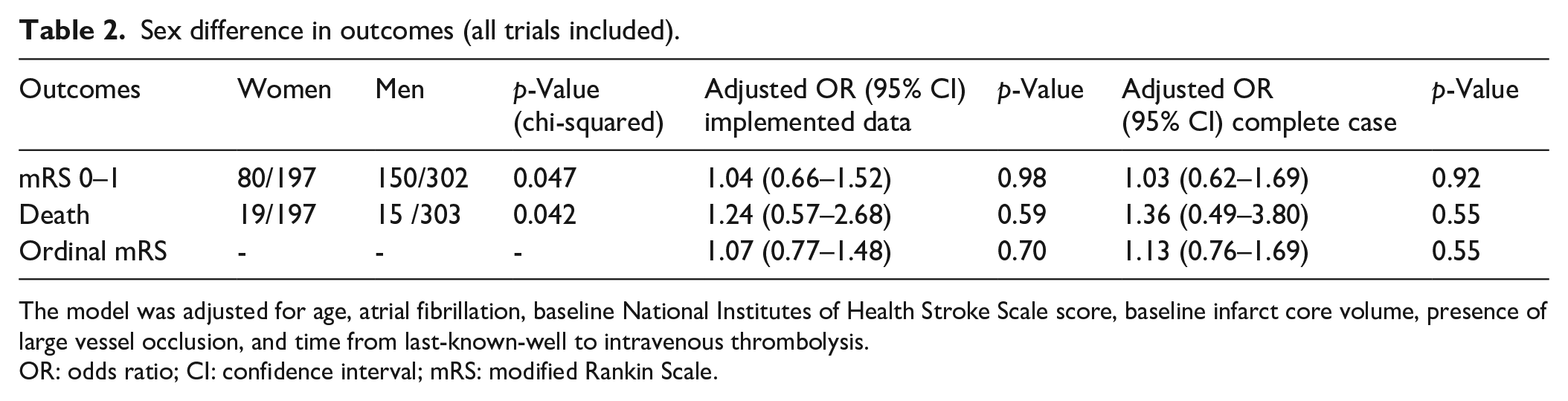
The model was adjusted for age, atrial fibrillation, baseline National Institutes of Health Stroke Scale score, baseline infarct core volume, presence of large vessel occlusion, and time from last-known-well to intravenous thrombolysis.
OR: odds ratio; CI: confidence interval; mRS: modified Rankin Scale.
Female sex was not significantly associated with a shift towards a better functional outcome (common OR, 1.07 [95% CI, 0.77–1.48]; p = 0.70). The sensitivity analyses for complete cases are summarised in Table 2. The results from the four RCTs, excluding MR WITNESS, are shown in Table 3.
Sex difference in outcomes (MR WITNESS excluded).
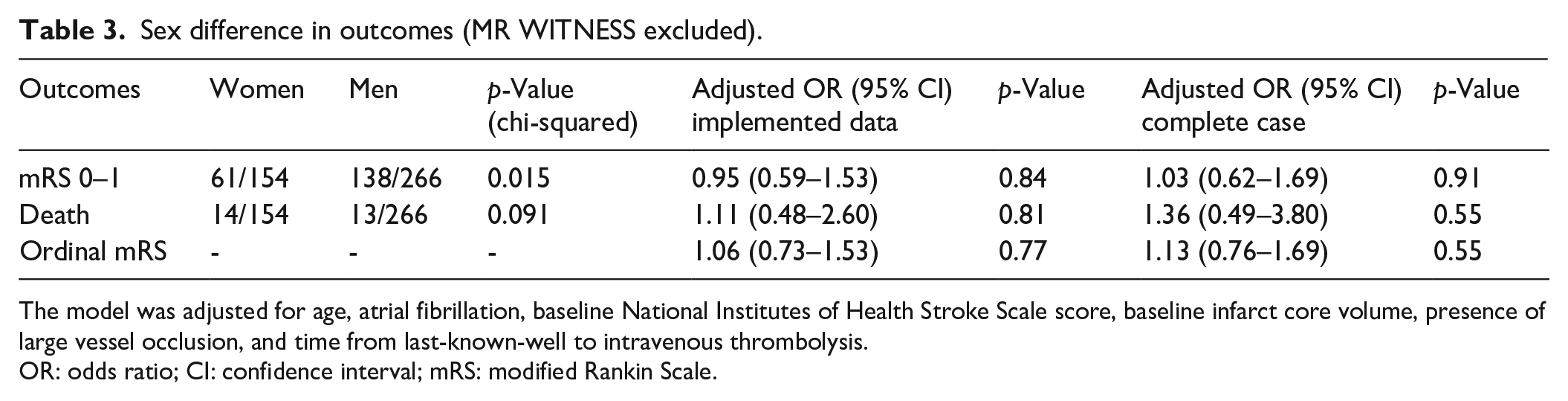
The model was adjusted for age, atrial fibrillation, baseline National Institutes of Health Stroke Scale score, baseline infarct core volume, presence of large vessel occlusion, and time from last-known-well to intravenous thrombolysis.
OR: odds ratio; CI: confidence interval; mRS: modified Rankin Scale.
No significant effect modification was observed by each subgroup on the association between sex and favourable clinical outcome (Table 4).
Odds ratios for favourable clinical outcomes (mRS 0–1) by subgroups.
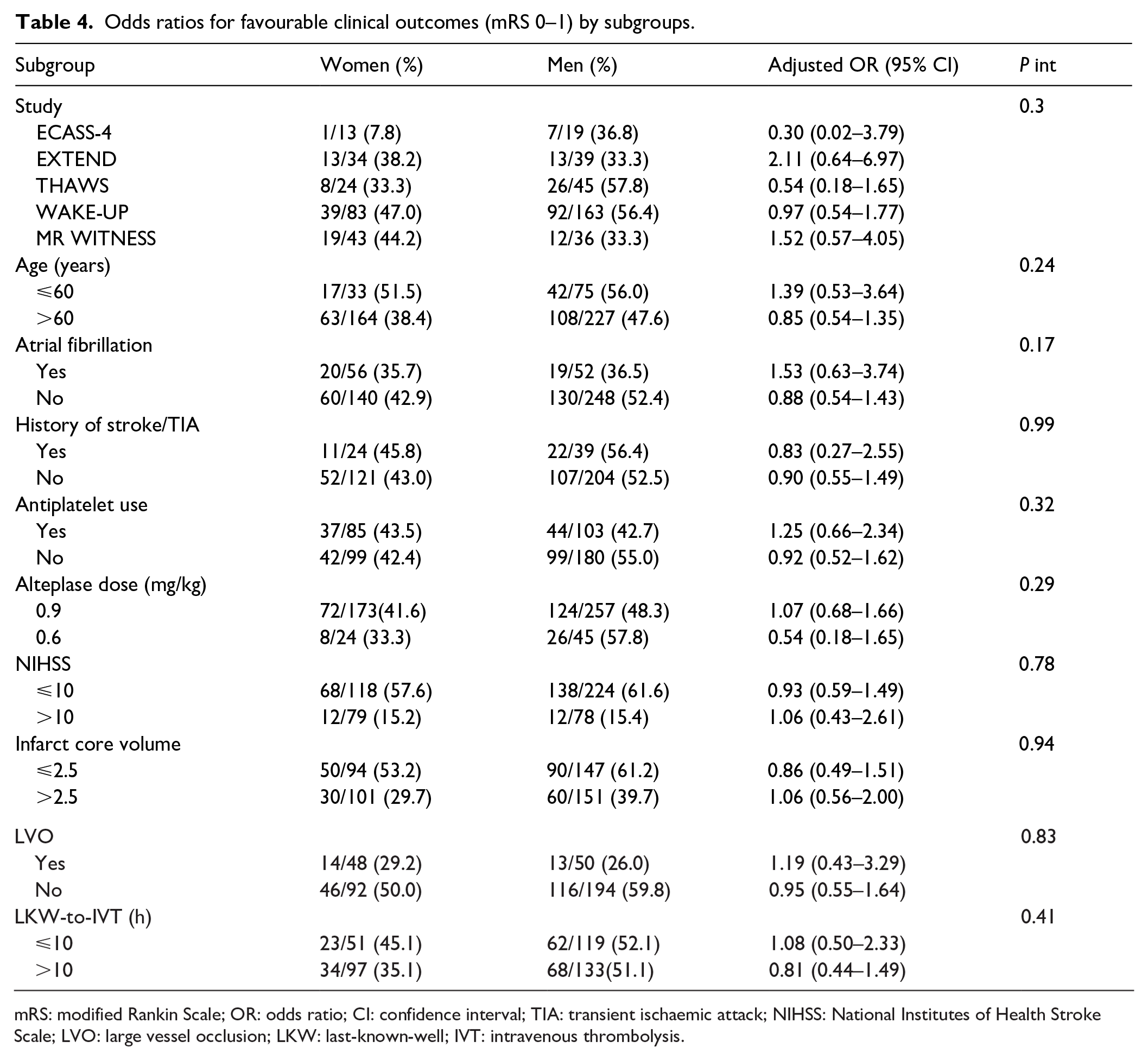
mRS: modified Rankin Scale; OR: odds ratio; CI: confidence interval; TIA: transient ischaemic attack; NIHSS: National Institutes of Health Stroke Scale; LVO: large vessel occlusion; LKW: last-known-well; IVT: intravenous thrombolysis.
Discussion
This is the first pooled analysis of IPD from five clinical trials (four RCTs and one single-arm trial) to investigate the sex-based difference in functional outcomes following imaging-based IVT for patients with stroke with an unknown onset time. The present study showed that women were less likely to have favourable outcomes and more likely to die at 90 days following imaging-based IVT. However, these associations did not persist after adjusting for relevant confounders, and no significant differences in the clinical outcomes were observed between the sexes.
Our results indicate that the poor outcomes in women were not due to female sex per se, but rather due to other comorbidities or health conditions that existed prior to the stroke, which may be more prevalent or have a greater impact on women. In our study, the women were older and more likely to have hypertension and atrial fibrillation. Our findings that women had higher NIHSS scores and more LVO at diagnosis suggest that the clinical status of women is already more severe than that of men upon arrival at the hospital. Although the stroke subtype was unavailable in our data set, we would expect that women would be more likely to have a cardioembolic stroke, the most severe subtype, since they are more likely to have concomitant atrial fibrillation and LVO. It is known that women > 65 years of age with atrial fibrillation are at an exceptionally high risk for subsequent stroke events. 16 Women with atrial fibrillation are typically older, have more comorbidities than men, are more often symptomatic, and experience a worse quality of life due to more severe strokes.17,18 Women may benefit from timely detection and appropriate management of atrial fibrillation. However, it has also been noted that women with atrial fibrillation have a 2.8-fold increased risk of ICH compared to that of men with atrial fibrillation. 17 Since women are more likely to have hypertension, appropriate anticoagulation therapy and aggressive blood pressure control are also important.
In our study, the time from LKW to treatment, especially from LKW to symptom recognition, was found to be longer in women. Taking a longer time before activating the emergency system in women is seemingly inconsistent with the expected high prevalence of cardioembolic strokes, which would be easier to detect due to their typically sudden symptom manifestation and completion. The possible explanation is that the characteristics of such women include older age, prestroke disability, higher stroke severity, and socioeconomic factors such as a greater chance of living alone or being widowed. Observational studies on acute stroke have also shown that delayed hospital arrival for women is more common than for men.18,19 The higher prevalence of women living alone has also been identified as a risk factor for their late arrival in the event of stroke. 20
Time from onset to treatment can affect not only the efficacy but also the eligibility for IVT treatment. Previous studies suggest that delayed arrival of women at the hospital may make them ineligible for thrombolysis. A recent meta-analysis showed that although the sex difference narrowed over time, women with acute stroke were still less likely to be treated with IVT. 21 Our study demonstrated that delayed arrival remains consistently crucial, even for patients undergoing imaging-based IVT.
Reassuringly, the time from symptom recognition to treatment was comparable between the sexes, demonstrating that there is not any implicit bias in treatment activation once patients reach the hospital. For conventional IVT, although fewer data are available on sex differences in door-to-needle times, they suggest an insignificant or minimal contribution of sex in the delay for intravenous tissue plasminogen activator treatment.9,22
Our results indicate a comparable (p = 0.29) median baseline infarct core volume between women (2.8 ml [IQR 0.9–16.3]) and men (2.5 ml [IQR 0.7–9.9]). Previous studies on patients treated with conventional IVT have shown the median baseline infarct core volumes by DWI as 18 ml (Echoplanar Imaging Thrombolytic Evaluation Trial) 23 and as 10 ml (Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution). 24 Among these studies, patients with a mismatch in imaging had a favourable clinical response following IVT compared to placebo. The infarct core volumes of the patients in our study were smaller than that for most mismatched patients in the above-mentioned studies. Although the enrolled women had longer time intervals from LKW to treatment and more severe clinical status, no significant differences were observed in their infarct core volumes compared with those of men. This may be due to the nature of the clinical trials, in which the eligibility for treatment is strictly controlled. In other words, it is possible that only women with clinically favourable conditions, such as abundant collateral flow, were enrolled in the trials. A larger number of women could have been excluded from imaging-based IVT because they already had extensive infarction upon hospital arrival. Thus, proactive medical and social interventions specifically for women may help more of them to adapt to IVT and improve their overall outcomes.
The strength of this study lies in the meta-analysis of highly qualifying pooled IPD from multiple RCTs and a single-arm trial that compared the efficacy and safety of imaging-based IVT against a placebo or standard care. Nevertheless, several limitations also exist in our study. First, a cautious interpretation of the results is advised because of an unspecified post-hoc analysis. Second, this study lacks information regarding initial vascular occlusion from the ECASS4 and MR WITNESS trials and the treatment time course from the MR WITNESS trial. However, we conducted multiple imputations to account for any missing data, including the outcomes and covariates. For the sensitivity analysis, we also performed complete case analyses and found consistency in the results. Third, data of individual premorbid mRS score are not included in the EOS dataset. Although the number of patients with an mRS score of ⩾2 was small (N = 11), we added the sensitivity analysis to minimise the confounding effect of premorbid mRS score on outcomes and acquired similar results. Fourth, the inclusion of a relatively small number of women in this study may raise concern about their underrepresentation in clinical trials and, therefore, the generalisability of the results.
In conclusion, pooled data from the clinical trials show that women with ischaemic stroke with an unknown onset time had a lower chance of good functional outcomes following imaging-based IVT. However, this sex-based difference can be explained by the higher age and more severe clinical status of women at stroke onset. Proactive medical and social interventions reducing pre-stroke comorbidities in women may potentially lead to improved outcomes after stroke. Further investigation is warranted to identify the causal factors that contribute to poorer outcomes in women following imaging-based IVT.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MK reports personal fees from Mitsubishi Tanabe Pharma and Daiichi-Sankyo and research support from Daiichi-Sankyo and Nippon Boehringer Ingelheim, all of which are outside of the submitted work. GT reports grants and personal fees from Bayer, personal fees from Acandis, Boehringer Ingelheim, Bristol Myers Squibb, Pfizer, Daiichi Sankyo, Portola, and Stryker outside of the submitted work. MI reports personal fees from Daiichi Sankyo, Bayer, Bristol Myers Squibb, and Nippon Boehringer Ingelheim outside of the submitted work. CG reports personal fees from Amgen, Bayer Vital, Bristol Myers Squibb, Boehringer Ingelheim, Sanofi Aventis, Abbott, and Prediction Biosciences outside of the submitted work. SMD reports personal fees from Abbott, Boehringer Ingelheim, Bayer, Tide Pharmaceuticals, and Medtronic and grants from the National Health and Medical Research Council of Australia outside of the submitted work. GAD reports grants from the National Health and Medical Research Council Australia during the conduct of the study and personal fees from Allergan, Amgen, Bayer, Boehringer Ingelheim, Pfizer, and Servier outside of the submitted work. WH reports grants from Boehringer Ingelheim. PR reports grants from Boehringer Ingelheim during the conduct of the study and personal fees from Bayer, Boehringer Ingelheim, Pfizer, and Daiichi Sankyo outside of the submitted work. OW reports grants from the NIH, grants and non-financial support from Genentech during the conduct of the study, and personal fees from Penumbra and Genentech outside of the submitted work. OW has a patent ‘Delay-compensated calculation of tissue blood flow’ (US Patent 7,512,435; March 31, 2009) with royalties paid to General Electric, Siemens, Olea Medical, and Imaging Biometrics. LHS reports grants from the National Institute of Neurological Disorders and Stroke (NINDS) and Genentech during the conduct of the study and personal fees from Genentech, Medtronic, and LifeImage outside of the submitted work and served on data safety monitoring boards for Penumbra and the Charite Hospital B_PROUD trial of mobile stroke units. SW reports grants from the NIH (Grant P50NS051343) during the conduct of the study and personal fees from Genentech outside of the submitted work. KT reports grants from the Japan Agency for Medical Research and Development during the conduct of the study and personal fees from Daiichi-Sankyo, Bayer Yakuhin, Bristol Myers Squibb, Otsuka, and Novartis outside of the submitted work. Others: nothing to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Japan Agency for Medical Research and Development (JP24lk0221186, JP23lk0221171).
Ethical approval
All participating sites for all included trials were approved by the relevant local ethics committees.
Informed consent
Written informed consent was obtained from the subjects or their legally authorised representatives according to national and local regulations, including an exception of explicit informed consent in emergency circumstances.
Trial registration
Not applicable.
Guarantor
MFD
Contributorship
MFD MK, KT, KM, MI, and SY contributed to the conception and design of the study; MFD, and GT contributed to the acquisition and analysis of data; MFD MK, KT, KM, MI, SY, GT, MJ, CG, SMD, GAD, HM, WH, PR, OW, LHS, and SW contributed to drafting the text or preparing the figures.