
Abstract
Introduction
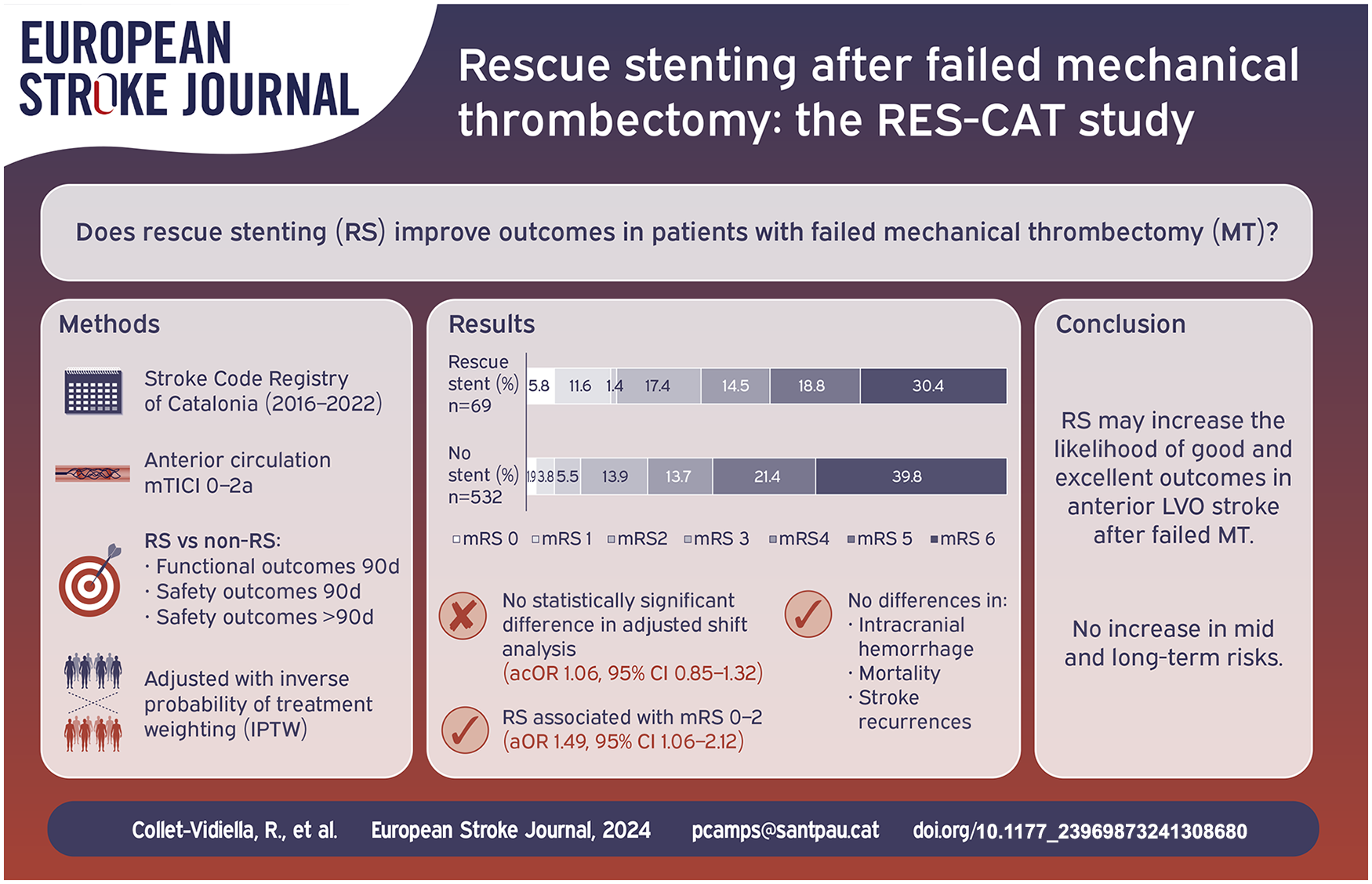
The efficacy of intracranial rescue stenting (RS) following failed mechanical thrombectomy (MT) in large-vessel occlusion (LVO) stroke remains uncertain. We aimed to evaluate clinical outcomes of RS in patients with anterior circulation LVO stroke following unsuccessful MT.
Patients and methods
We conducted a retrospective analysis using the Stroke Code Registry of Catalonia (January 2016–March 2022), a prospective, population-based registry including patients treated at 10 comprehensive stroke centers. We compared outcomes between patients who received RS and those who did not after failed MT. The primary outcome was the shift in 90-day functional status, assessed by the modified Rankin Scale (mRS), adjusted for confounders using inverse probability of treatment weighting (IPTW). Secondary outcomes included good (mRS ⩽ 2 or 3 if baseline mRS was 3) and excellent (mRS ⩽ 1) outcomes, ischemic recurrences, hemorrhagic transformation, and 90-day mortality.
Results
Of 601 patients, 69 underwent RS. RS did not significantly impact the 90-day mRS shift (adjusted common odds ratio [acOR] 1.06, [95% CI 0.85–1.32]; p = 0.613). However, RS was associated with higher rates of good (18.8% vs 11.7%; aOR 1.41, [95% CI 1.00–1.99]; p = 0.048) and excellent outcomes (17.4% vs 5.7%; aOR 2.90, [95% CI 1.89–4.43]; p < 0.001). Symptomatic intracranial hemorrhage (9.4% vs 7.4%; p = 0.507) and 90-day mortality (30.4% vs 39.8%; p = 0.135) were similar between groups. Stroke recurrence (4.2% vs 1.7%; p = 0.247) showed no significant difference at 33-month follow-up.
Discussion and conclusion
RS may increase the likelihood of good and excellent outcomes in anterior LVO stroke after failed MT, without increasing long-term risks. Further randomized trials are warranted for comprehensive validation.
Keywords
Introduction
Mechanical thrombectomy (MT) has significantly improved outcomes in acute ischemic stroke due to large-vessel occlusion (LVO).1–3 However, 17%–29% of patients experience unsuccessful recanalization, defined by a modified Thrombolysis in Cerebral Ischemia (mTICI) score of 0–2a.1,4 Successful recanalization is a key predictor of favorable outcomes in LVO-related stroke.5,6 As such, when MT fails, rescue therapies such as intracranial stenting, angioplasty, and antithrombotic drugs are often considered to restore blood flow and improve outcomes.
The use of rescue intracranial stenting (RS) after failed MT has shown potential benefits in retrospective studies.7–10 Much of the early evidence comes from studies conducted in centers with predominantly Asian populations, where intracranial atherosclerotic disease (ICAD) is a more frequent cause of stroke, limiting their generalizability.8,9,11 More recent studies from large cohorts from the United States, however, have also reported improved functional outcomes and lower mortality with RS compared to medical management alone.12,13 Nevertheless, no consensus exists on the optimal treatment strategy after failed MT. Furthermore, previous studies have focused on 90-day outcomes, leaving the long-term implications of RS, including stent patency and clinical outcomes, largely unexplored.
This study aimed to assess both the acute and long-term outcomes in patients with anterior circulation LVO who underwent RS after failed MT. We hypothesized that RS improves functional outcomes in these patients.
Patients and methods
This study followed the STROBE (Strengthening The Reporting of OBservational studies in Epidemiology) statements. 14
Study design and population
The RES-CAT cohort study was derived from the Stroke Code Registry of Catalonia, a prospective, population-based, and mandatory registry that systematically collects data on all patients with an activated stroke code in Catalonia, a region in Spain with approximately 8 million inhabitants. Endovascular treatment is performed at 10 comprehensive stroke centers across the region. We identified all patients who underwent MT for acute ischemic stroke between January 2016 and March 2022. Enrolment criteria were: (1) age ⩾18 years, (2) prior mRS 0–3, (3) anterior circulation LVO involving the terminal internal carotid artery or the M1/M2 segments of the middle cerebral artery, and (4) failed MT, defined as an mTICI score of 0–2a. A low National Institutes of Health Stroke Scale (NIHSS) value was not an exclusion criterion. Patients without available mRS at 90 days were excluded.
Data collection and assessment
Most data were sourced from the Stroke Code Registry of Catalonia, including demographic characteristics, risk factors, baseline clinical and radiological data, reperfusion treatment, thrombectomy outcomes, symptomatic intracranial hemorrhage (sICH), and functional outcomes at 90 days. Additional information regarding the long-term follow-up (>90 days), antiplatelet regimen during MT and angiographic follow-up were collected from participating centers’ electronic health records. All data were anonymized before being sent to the coordinating center.
As the study was retrospective, MT procedures followed each center’s routine clinical practice. When MT failed, RS was performed at the discretion of the stroke team, with no pre-specified limit on thrombectomy attempts before RS deployment. Clinical, radiological, and thrombectomy outcomes, including mTICI scores, were evaluated per each center’s protocol. The 90-day mRS was evaluated through a phone call by a certified central assessor who was blinded to the treatment procedures. Long-term follow-up, including stent patency, was conducted according to each center’s protocol, with the last follow-up defined as either the most recent clinical evaluation at the referring hospital or death.
Outcome measurement
We compared efficacy and safety outcomes in patients with and without RS. The primary outcome was the shift in the mRS score at 90 days. Secondary outcomes included good functional outcomes at 90 days (mRS score ⩽ 2 for patients with a baseline mRS ⩽ 2 and of 3 for those with a baseline mRS of 3), excellent functional outcomes at 90 days (mRS ⩽ 1 for patients with a baseline mRS of ⩽1), and stroke or transient ischemic attack recurrences during follow-up. Safety outcomes included sICH, defined as an intracranial hemorrhage with an increase of ⩾4 in the NIHSS score or resulting in death, 15 and 90-day mortality. We also analyzed a composite outcome combining stroke recurrences and mortality within 30 days and any stroke recurrences beyond 30 days, as in the SAMMPRIS trial. 16 Procedure characteristics and complications, and the angiographic follow-up data for RS patients were also described.
Statistical analysis
Statistical analyses were performed using STATA version 17.0 (StataCorp, College Station, TX). Categorical variables are presented as absolute frequency (n) and percentages (%), while quantitative variables are presented with means and standard deviations (SD) or medians and interquartile ranges (IQR), as appropriate. Normality of continuous variables was assessed using histograms and the Shapiro–Wilk test. We compared clinical and radiological characteristics between the RS group and non-stenting groups using χ2, t-Student, and Mann–Whitney U tests as suitable. To explore the relationship between RS and the primary outcome we performed a shift analysis using ordinal logistic regressions. Brant test was performed to test that the parallel regression assumption was accomplished. To account for the retrospective and multicenter design, Inverse Probability of Treatment Weighting (IPTW) was used to adjust for confounders. The propensity score for RS was calculated via multiple logistic regression, including age, baseline NIHSS, ASPECTS, prior thrombolysis, atrial fibrillation, and pre-stroke mRS, given their potential impact on the decision to perform RS or on the outcomes.
Secondary efficacy outcomes (good and excellent functional outcomes as defined in the previous section) were analyzed using binary logistic regression, adjusted with IPTW. Time-to-event analyses for stroke recurrences and the composite outcome were performed using log-rank tests and Cox regression. Missing data were excluded, and a two-tailed p-value <0.05 was considered significant.
Standard protocol approvals, registrations, and patient consents
The Hospital de la Santa Creu i Sant Pau Hospital ethical standards committee approved this study (IIBSP-RES-2022-18), and all study procedures were conducted in accordance with the Declaration of Helsinki. Because of the retrospective nature of the study, the need for written informed consent was waived.
Results
Of 5167 MT procedures in Catalonia during the study period, 622 patients presented failed MT. The 90-day mRS was available for 601 patients, 69 with RS and 532 in the non-RS group (Figure 1). Compared to non-RS patients, RS patients were younger (mean age 67 vs 73; p < 0.001), and had less atrial fibrillation (4.5% vs 22%; p < 0.001). They also had lower baseline NIHSS (median 13 vs 17; p = 0.002), more atherothrombotic stroke etiology (69.6% vs 20.5%; p < 0.001), and longer time from last known well to puncture (507 min vs 255; p < 0.001, Table 1). RS patients had less preprocedural thrombolysis (19.4% vs 37%; p = 0.004), fewer passes (3 vs 4; p = 0.021), higher use of general anesthesia (35.8% vs 10.3%; p < 0.001), and a higher re-occlusion rate during endovascular treatment after prior recanalization with conventional devices (36.9% vs 18.4%; p < 0.001).

Flow chart.
Univariable comparison of baseline characteristics according to whether rescue stenting was used or not.

ASPECTS: Alberta Stroke Program Early Computed Tomography Score; IQR: interquartile range; LKW: last-known well; M1: first segment of middle cerebral artery; M2: second segment of middle cerebral artery; mRS: modified Rankin Scale; mTICI: modified Thrombolysis in Cerebral Infarction; NIHSS: National Institutes of Health Stroke Scale; SD: standard deviation; TIA: transient ischemic attack; TICA: terminal internal carotid artery; TOAST: Trial of Org 10172 in Acute Stroke Treatment.
Primary outcome
RS patients had a median 90-day mRS of 4 (IQR: 3–6), compared to 5 (IQR: 4–6) in non-RS patients (p = 0.026). Unadjusted shift analysis showed better outcomes for RS patients (unadjusted cOR of 0.59 [95% CI 0.37–0.93]; p = 0.022; Figure 2). However, after adjusting with IPTW (Supplemental Figure S1 and S2), RS was no longer associated with better mRS scores (adjusted cOR of 1.06 [95% CI 0.85–1.32]; p = 0.613).
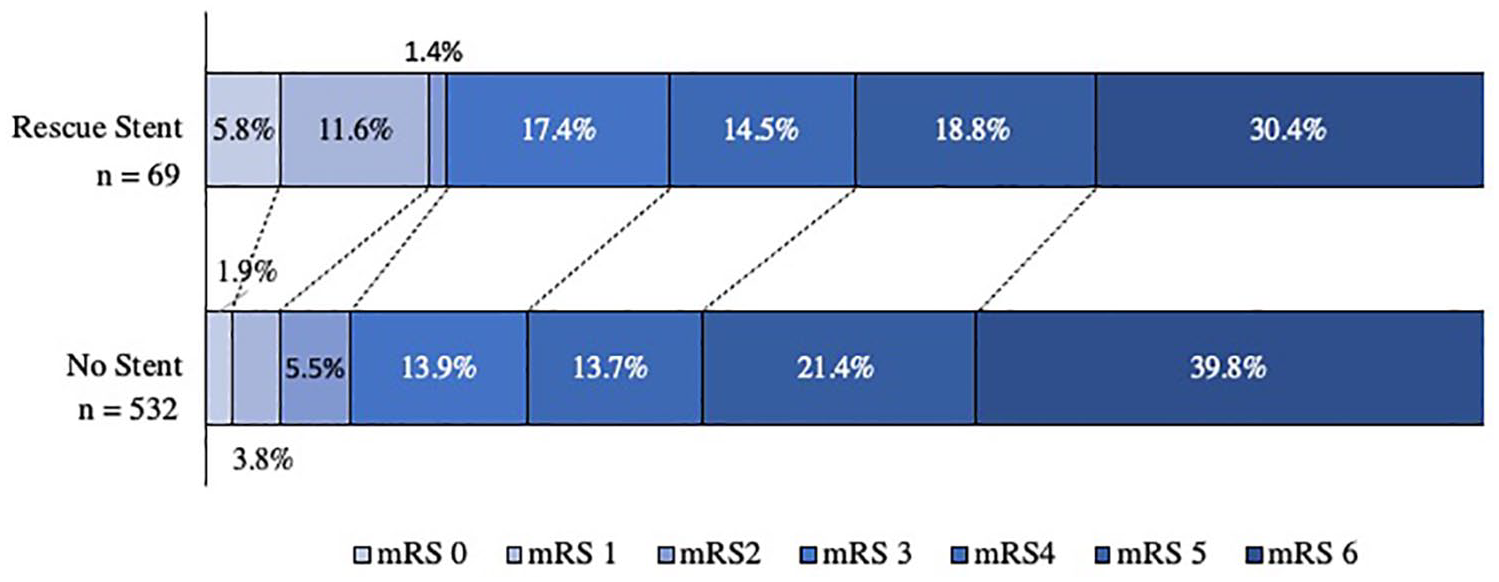
Modified Rankin Scale (mRS) at 90 days, comparing patients who received rescue stenting and those who did not.
Secondary outcomes
RS patients had higher rates of good and excellent outcomes at 90 days than non-RS patients (18.8% vs 11.7%, and 17.4% vs 5.7%, respectively). After IPTW adjustment, RS significantly increased the likelihood of good outcomes (adjusted OR, 1.41 [95% CI 1.00–1.99]; p = 0.048) and excellent outcomes (adjusted OR, 2.90 [95% CI 1.89–4.43]; p < 0.001, Table 2). The absolute risk reduction for good and excellent outcomes were 7.1% and 11.7%, yielding a number needed to treat (NNT) of 14 and 9, respectively.
Comparison of secondary outcomes, safety, and procedure outcomes between patients who received rescue stenting and those who did not.

aOR: adjusted odds ratio; CI: confidence interval; mRS: modified Rankin Scale.
mRS score 0–2/3 includes patients with mRS 0–2 and 3 if their premorbid mRS was 3; sICH, symptomatic intracerebral hemorrhage.
Adjusted using inverse probability of treatment weighting considering the following variables: age, baseline NIHSS, ASPECTS score, prior thrombolysis, atrial fibrillation, and prior mRS.
Safety outcomes
sICH rates were similar between groups (9.4% vs 7.4%; aOR, 1.17 [95% CI 0.74–1.83]; p = 0.507). There was a trend towards lower mortality at 90 days with RS, but it did not reach statistical significance (30.4% vs 39.8%; aOR, 1.21 [95% CI 0.94–1.57]; p = 0.135). RS was significantly associated with a higher rate of distal embolization (6.0% vs 1.5%; p = 0.014) but not with vessel perforation (3.0% vs 8.3%; p = 0.126) or dissection (0% vs 2.3%; p = 0.214, Table 2).
Long-term outcomes
Follow-up data were available for 353 of 367 patients alive at 90 days, 48 in the RS group. Median follow-up time was 494 days (IQR: 353–835) for RS patients and 1084 days (IQR: 595–1615) for non-RS patients. Seven patients had stroke recurrences after 90 days, two from the RS group, with no significant differences between groups (4.2% vs 1.7%; p = 0.247). Both recurrences in the RS group occurred in the target vessel. During follow-up, the composite outcome occurred in 194 (32.3%) patients, 19 (27.4%) in the RS group, and 175 (32.9%) in the non-RS group (p = 0.37, Figure 3). There was no intracerebral hemorrhage (ICH) during follow-up beyond 90 days in either group, and rates of myocardial infarction and extracranial hemorrhage were similar (0% vs 2.0%; p = 0.325 and 4.2% vs 2.3%; p = 0.450, respectively; Table 3).
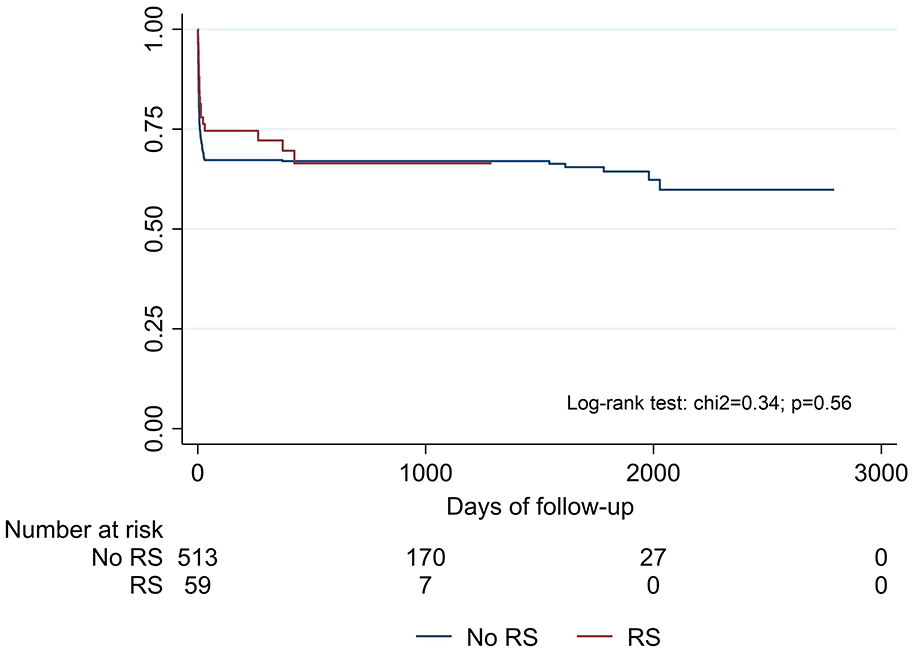
Kaplan–Meier survival curves for the composite outcome (stroke recurrences and mortality during the first 30 days after the stroke plus any stroke recurrences beyond 30 days).
Follow-up data beyond 90 days in patients who received rescue stenting and those who did not.

ICH: intracerebral hemorrhage; IQR: interquartile range.
Univariate analysis.
Procedure characteristics and angiographic outcomes
During the RS procedure, parenteral antiplatelet therapy was administered to 58 patients (84.1%). Almost half of the patients (42.9%) received tirofiban only, while 26.8% received parenteral aspirin and 30.4% received both.
Recanalization after RS was successful (mTICI 2b-3) in 51 patients (73.9%). Thirteen (25.4%) had good functional outcomes at 90 days compared to none of the patients without successful recanalization after stenting (Supplemental Figure S3). Twelve patients (23.5%) with successful recanalization achieved excellent outcomes. There were no major differences in antiplatelet use between patients with successful and unsuccessful RS (Supplemental Table S1).
Angiographic follow-up was available for 42 patients (60.8%). Reocclusion occurred in five patients (16.1%) with successful recanalization, two within 48 h. Additional details on angiographic follow-up are in Supplemental Table S1.
Discussion
This population-based study did not show a benefit of RS regarding the primary outcome, the shift in the 90-day mRS. However, similar to a recent study, 13 RS was associated with higher odds of achieving good (mRS: 0–2 or 3 if baseline mRS was 3) and excellent (mRS: 0–1) functional outcomes compared to medical management after failed MT. We did not find any differences between groups regarding sICH rates, mortality, or long-term stroke recurrence.
RS benefits were previously suggested by studies from Asian populations,8,9 with recent data from United States indicating that RS may also improve outcomes in more diverse populations.12,13 However, a recently published Chinese clinical trial found no benefit of RS or angioplasty following failed MT, potentially due to additional thrombectomy attempts and tirofiban use in control patients. These factors may have improved outcomes in the control arm, limiting the trial’s capacity to detect significant differences. 17
Our findings align with this trial, as RS did not improve mRS at 90 days. 17 This contrasts with findings from the SVIN registry, which reported improved outcomes with RS. 13 In the SVIN registry, 31% of RS patients achieved a mRS ⩽ 2, compared to 18.8% in RES-CAT. 13 The SVIN study reported a higher successful reperfusion rate (83.1% vs 73.9%), which may partly explain the difference. 13 Moreover, regional variations in RS usage may have impacted the study’s power: in the SVIN cohort, 42% of patients received RS after failed MT, compared to only 11% in RES-CAT. 13
Despite no shift in 90-day mRS, we found higher rates of good and excellent outcomes with RS after IPTW adjustment, consistent with previous studies.8,9,12,13 The NNT was 14 for a good outcome and 9 for an excellent outcome.
As observed in previous works,7–9,12,17,18 sICH rates did not differ between groups. This is a common concern with RS, given the need for antiplatelet medications to prevent intra-stent thrombosis. Although not statistically significant, mortality was lower in the RS group, a finding that had also been reported previously.7,9,12,13
Long-term outcomes showed no significant differences in stroke recurrence or hemorrhagic events during follow-up, adding valuable data beyond the usual 90-day window. While our data beyond 90 days includes only 48 RS patients, more than 75% were followed for over a year. Among RS patients, only two patients (4.2%) experienced stroke recurrence after 90 days, suggesting a low stent failure rate in the long term. However, the RS group had a shorter median follow-up time (494 vs 1084 days), likely reflecting the increased use of RS in recent years.
The RES-CAT study’s strength lies in its population-based design, capturing all consecutive patients with a stroke code in Catalonia, enhancing generalizability. Additionally, our primary outcome, the mRS at 90 days, was centrally assessed by a certified blinded evaluator, reducing bias. Finally, we used IPTW to account for confounders, acknowledging that the decision to perform RS could be influenced by physician choice and patient characteristics.
However, we acknowledge several limitations in our study. First, the retrospective collection of data beyond 90 days could have introduced biases such as missing data or loss to follow-up. Moreover, RS protocols were not pre-specified. These decisions were at the discretion of each clinician or center, based on their own experience and patient characteristics, which could have generated selection bias. In our cohort, patients who received RS had lower rates of atrial fibrillation (often treated with anticoagulants) and prior thrombolysis, two factors linked to higher hemorrhage risk that may have led clinicians to avoid using RS. However, we attempted to reduce these and others confounding factors by adjusting with IPTW. Additionally, no pre-specified protocols were established for angiographic follow-up. Third, we did not specifically investigate whether MT failure was due to ICAD or other causes. Nevertheless, recent data suggests that RS improves outcomes regardless of the underlying etiology. 13 Not knowing the cause of MT failure could also introduce selection bias, as some patients in the non-RS group, such as those with access issues, may not be eligible for RS. Another important point is the lack of detailed data on the use of balloon angioplasty in the non-RS group. While it is likely that only a small number of patients in this group underwent balloon angioplasty, the absence of precise information prevents us from fully assessing its potential impact on outcomes. However, given its presumed limited use, we believe it is unlikely to substantially influence the overall findings of the study. Finally, we did not track certain stroke risk factors during follow-up, which could influence recurrence rates.
In conclusion, rescue stenting may improve the chances of achieving good and excellent functional outcomes in patients with an anterior ischemic stroke due to LVO and failed MT. Furthermore, it appears to be safe in both the mid-term and long-term. These findings can assist clinicians in deciding whether to use RS following failed MT. Further randomized clinical trials are needed to provide more definitive insights into the efficacy of this procedure.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241308680 – Supplemental material for Rescue stenting after failed mechanical thrombectomy: The RES-CAT study
Supplemental material, sj-docx-1-eso-10.1177_23969873241308680 for Rescue stenting after failed mechanical thrombectomy: The RES-CAT study by Roger Collet-Vidiella, Pol Camps-Renom, Ana Núñez-Guillén, Helena Quesada, Federica Rizzo, Noelia Rodriguez-Villatoro, Sergio Amaro, Laura Llull, Daniel Santana, Edgardo Estrada, Alan Flores, Mikel Terceño, Saima Bashir, María Hernández-Pérez, Sebastià Remollo, Oriol Barrachina-Esteve, David Cánovas, Elio Vivas, Ana Rodríguez-Campello, Gerard Mauri, Francisco Purroy, Anna Ramos-Pachón, Marina Guasch-Jiménez, Daniel Guisado-Alonso, Luis Prats-Sánchez, Alejandro Martínez-Domeño, Álvaro Lambea-Gil, Garbiñe Ezcurra-Díaz, Jordi Branera-Pujol, José Pablo Martínez-González, Lavinia Dinia, Mercè Salvat-Plana, Natalia Pérez de la Ossa, Carlos A. Molina, Pere Cardona and Joan Martí-Fàbregas in European Stroke Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Hospital de la Santa Creu i Sant Pau Hospital ethical standards committee approved this study (IIBSP-RES-2022-18). All procedures were conducted in accordance with the national law, the 1964 Declaration of Helsinki and its later amendments and the recommendations of the guidelines on Good Clinical Practice and Good Epidemiological Practice.
Informed consent
Because of the retrospective nature of the study, the need for written informed consent was waived.
Guarantor
RCV
Contributorship
JMF conceived the study. RCV, PCR, ARP, MGJ, DGA, LPS, AMD, ALG, GED, JBP, JMG, LD, and JMF were involved in the protocol development, gaining ethics and regulatory approvals. RCV, ANG, HQ, FR, NRV, SA, LL, DS, EE, AF, MT, SB, MHP, SR, OBE, DC, EV, ARC, GM, FP, MSP, NPO, CM, and PC were involved in data acquisition. RCV curated the data. RCV and PCR conceived the statistical plan and analyzed the data. RCV, PCR and JMF interpreted the results. RCV wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Data availability
Anonymized data not published within this article will be made available from the corresponding author upon reasonable request.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.