
Abstract
Purpose:
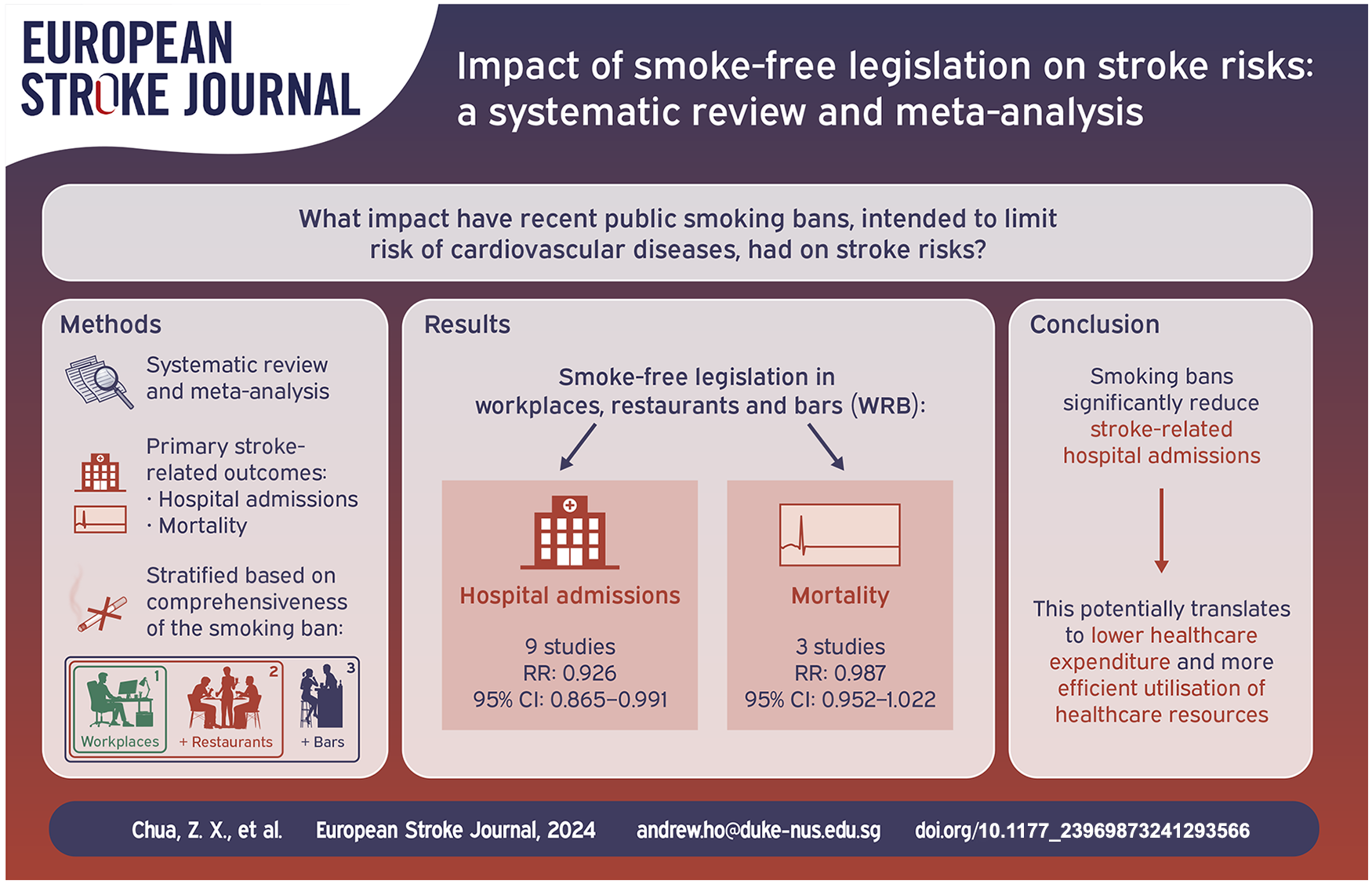
Secondhand smoke significantly increases the risk of cerebrovascular diseases, prompting recent public smoking bans. We aimed to ascertain the effects of smoke-free legislation on stroke incidence and mortality.
Methods:
We systematically searched Medline, Embase, Cochrane Library, and Scopus up to August 13, 2023, for studies reporting changes in stroke incidence following partial or comprehensive smoking bans. A random-effects meta-analysis was conducted on hospital admissions and mortality for stroke, stratified based on comprehensiveness of the ban ((i) workplaces-only, (ii) workplaces and restaurants, (iii) workplaces, restaurants and bars). The effect of post-ban follow-up duration was assessed visually by a forest plot, while meta-regression was employed to evaluate for any dose-response relationship between ban comprehensiveness and stroke risk.
Findings:
Of 3987 records identified, 15 studies analysing bans across a median follow-up time of 24 months (range: 3–67) were included. WRB bans were associated with reductions in the rates of hospital admissions for stroke (nine studies; RR, 0.918; 95% CI, 0.872–0.967) and stroke mortality (three studies; RR, 0.987; 95% CI, 0.952–1.022), although the latter did not reach statistical significance. There was no significant difference in the risk of stroke admissions for studies with increased ban comprehensiveness and no minimum duration for significant post-ban effects to be observed.
Discussion and conclusion:
Legislative smoking bans were associated with significant reductions in stroke-related hospital admissions, providing evidence for its utility as a public health intervention.
Introduction
Stroke is the second leading cause of death globally. 1 According to the World Stroke Organisation, the incidence of stroke exceeds 12.2 million patients annually and over 143 million years of healthy life are lost every year due to stroke-related deaths and disability. 2 Smoking is a strong independent risk factor of stroke. Studies performed across various populations have demonstrated that current smokers have at least a two- to fourfold increased risk of stroke compared with lifelong nonsmokers or ex-smokers who had quit smoking more than 10 years prior. 3 Moreover, secondhand smoke (SHS) exposure has been associated with adverse health effects. SHS, also known as environmental tobacco smoke or passive smoke, consists of smoke that is emitted during burning of tobacco-containing products and directly exhaled by the smoker. 4 SHS exposure has been reported to increase the risk and mortality of stroke by up to 30% and 100% respectively.5,6
Numerous countries have implemented smoke-free legislations in public areas to mitigate the deleterious effects of SHS exposure. However, smoke-free legislations in different regions vary in their degree of comprehensiveness. Comprehensive smoking bans have been implemented in workplaces, bars, restaurants, public transport, schools and hospitals, whilst partial smoking bans still allow for smoking in certain establishments. This has direct implications on the efficacy of legislative policies on the general population. 7 Additionally, there is a large variation in the scope and level of enforcement of such smoking bans among different cities and countries. Despite this, certain EU countries such as Switzerland,8,9 Ireland, 10 Scotland 11 and Sweden 12 have reported a clear reduction in SHS. There is also a notable positive effect on other health outcomes such as reduction in incidence of acute coronary events and respiratory diseases. 13
While the protective effects of smoke-free legislation on the incidence and mortality rates of cardiovascular and respiratory conditions are well defined,14–16 its effects on stroke are less clear. Several studies have reported a decrease in hospital admissions for stroke after the implementation of a smoking ban17–20 while others showed no significant change.21–24 One study 18 showed that Florida’s 2003 statewide law, which banned smoking in all workplaces and restaurants, was associated with a 18.1% (95% CI, 9.3–30.0) reduction in stroke hospitalisations over the period of 3 years. Conversely, a similar study in Canada 22 examined a 2003 province-wide smoking ban, encompassing public places and workplaces, and found a non-significant change of −3.04 (95% CI, −13.14, 7.06) admissions per 100,000 person-months in mean monthly stroke hospitalisation rates over 67 months.
In this systematic review and meta-analysis, we aimed to elucidate the effects of public smoking bans on the incidence and mortality rates of stroke, stratified by comprehensiveness of bans, length of follow-up and methodological quality.
Methods
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 Statement 25 and took reference from the Cochrane Handbook for Systematic Review of Interventions (version 6.3). 26 The study protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO, Record ID: CRD42024524342).
Search strategy
A thorough literature search was performed in Medline, Embase, Scopus and Central Cochrane databases from inception to 13th August 2023. A search was conducted for studies that reported associations of population level smoke free control policies in relation to stroke risk. Key search terms like ‘smoke-free policy’, ‘legislation bans’ and ‘stroke’ were included in our search strategy developed alongside the expertise of two medical information specialists (Medical Library, National University of Singapore and Medical Library, Nanyang Technological University). Reference lists of primary studies and systematic reviews were also reviewed for additional eligible studies. The detailed search strategy is available in the Supplemental Materials (eMethods).
Study selection
The research question was formulated using the PICOS (population, intervention, comparator, outcome, study type) 27 framework. The intervention group would comprise a general population situated within a geographical region in which a smoke-free ban was implemented, either partial or complete. Complete bans were defined as comprehensive smoking bans encompassing workplaces, restaurants and bars while partial bans referred to restrictions that do not fulfil the criteria for comprehensive bans. This group would be compared against control regions with no legislative smoking bans and control conditions without smoking as a risk factor. The primary outcomes were chosen to be any stroke-related population health outcomes including disease incidence, mortality rates and hospital admissions and discharges due to stroke. Study designs included observational studies (cross-sectional studies and cohort studies) and quasi-experimental studies (interrupted time series, uncontrolled before-and-after and controlled before-and-after).
Studies that met the following criteria for smoking bans were eligible: (1) the smoking ban must have been legislated at a local, regional or national level, (2) smoking was banned either completely in all settings including the hospitality sector or in specific areas, (3) smoking ban applied to both smokers and non-smokers, (4) outcomes reported were exclusively related to stroke or stroke with transient ischaemic attack (TIA) and were not combined with other unrelated medical diagnoses into a composite outcome. The following types of studies were excluded: (1) Systematic reviews; (2) Commentaries; (3) Case reports; (4) not in English; (5) studies that only investigated indirect measures to prohibit smoking, such as increasing the tobacco tax, advertising on the harmful effects of smoking, etc. (i.e. no form of comprehensive or partial ban established); (6) studies for which the full text of the article could not be retrieved for full evaluation; (7) studies that did not provide sufficient data about population size, the number of stroke mortality/incidence/deaths; (8) studies that did not report or present data that permitted estimating relative risk and confidence intervals; (9) studies on regions which had existing smoking bans in the pre-ban phase; (10) studies which reported only on transient ischaemic attack.
For each study, two authors independently reviewed the titles and abstracts. After excluding studies that did not meet the inclusion criteria, the full texts of the remaining studies were then independently screened by the same two authors to further assess eligibility. Discrepancies at each stage were resolved via discussion with all authors.
Data extraction
The following data was extracted from each study: proportion of population smoking, comprehensiveness of smoking ban, duration of study pre- and post-smoking ban, region that ban was implemented in, age, gender, population size, mean stroke admission rates, mean stroke discharge rates, mean stroke mortality rates, relative risk (RR) and confidence intervals (CI) comparing pre-ban versus post-ban stroke incidence, stroke incidence in control regions as well as change in incidence of non-smoking related control conditions. Two reviewers independently extracted data for each study and cross-checking was done by a third reviewer. The data extraction process was blinded, and discrepancies were resolved via consensus among all authors.
Study quality assessment
A comprehensive evaluation of bias in population-level observational studies was conducted using the Risk of Bias In Non-randomised Studies - of Exposures (ROBINS-E) 28 tool. The tool assessed the risk of bias in exposure effect estimates from individual observational studies that examine the effect of implementation of smoking bans on stroke incidence.29–31 Each included study was assessed in seven key domains– confounding factors, selection of participants, classification of exposures, departure from intended exposure, missing data, measurement of outcomes and selection of the reported result– with the risk of bias for each domain expressed as low, some concerns, or high. Two reviewers independently assessed the risk of bias for each study and all conflicts were resolved as detailed above.
Statistical analysis
Data analysis was conducted using R version 4.3.2 (The R foundation) 32 with the meta package version 7.0-0. 33 The Hartung Knapp Sidik-Jonkman estimator 34 served as our between-study variance estimator, and random-effects models were employed to account for anticipated inter-study heterogeneity. A p-value of 0.05 was chosen as the cutoff for statistical significance in this study.
Statistical heterogeneity was assessed using Cochran’s Q test and the I2 statistic. Cochran’s Q test was utilised to detect significant heterogeneity of intervention, with I2 > 50% indicating significant heterogeneity.
The RR was reported in only three studies.20,35,36 For these three studies, the gradual effects model was chosen to better represent the change over the entire follow-up period. The remaining 10 studies did not report RR and CI directly, thus various methods had to be employed to estimate them from the reported outcome. In five studies,19,37–40 the reported Incident Rate Ratio (IRR) and their respective CI served as an approximation of the RR. In two studies that applied a Poisson regression model,23,41 the results were reported as a percentage change which reflected the difference between the RR and the null value of 1.0. As such, we could convert the percentage changes back to RR by adding them to the null value (1.0). Likewise, the CI was obtained by adding the upper and lower limit to the null value. In one study, 22 RR and CI was estimated using the exponential of the change in trend of monthly admission rate obtained from the ARIMA model used in the study. In two studies,17,42 RR and CI was determined using a Poisson regression model accounting for temporal trends. For one study, 42 the effects of each phase of the smoking ban were isolated, and the final phase (workplaces, restaurants and bars bans) was directly compared with the pre-ban period. In all cases, the risk change associated with the law was always directly compared with the pre-ban period.
Included studies were categorised based on the outcomes measured and the comprehensiveness of the ban, with separate analyses conducted for every category with at least three or more studies. Meta-analysis was conducted on each study category to determine the significance of relative risk reduction.
Random-effects meta-regression utilising dummy variables coding for comprehensiveness of the law was performed to assess for its association with reductions in hospital admissions.
Visual analysis of the main forest plot with studies arranged in order of post-legislation follow-up length was used to assess for (i) any significant association in magnitude of risk reduction in stroke with length of follow-up and (ii) any minimum duration of follow-up for a significant post-ban effect to be observed. If a significant association was found, further regression analysis based on duration of follow-up would be performed.
Subgroup analysis was performed on studies which incorporated control regions (no smoking bans) and non-tobacco related conditions (e.g. cholecystitis, intestinal obstruction) in their study methodology as they adjusted for potential confounders such as secular trends and minimised internal validity threats to their study design.43,44 Further subgroup analysis was also performed on studies based on their risk of bias assessment using the ROBINS-E tool.
Finally, the risk of publication bias was assessed using funnel plots, Egger’s and Begg’s tests on our primary outcome of change in hospital admissions due to stroke.
Results
Study selection
A total of 3987 articles were retrieved from four databases, including 665 articles from PubMed, 2940 articles from Embase, 299 articles from Cochrane Library, and 83 articles from Scopus. 702 duplicates were removed, with a further 3258 articles excluded following the title and abstract sieve. Full text evaluation of the remaining 27 articles yielded 15 texts that met the inclusion criteria, of which 13 studies were eligible for meta-analysis. The number of references included and excluded at each screening stage are shown in a PRISMA flowchart (Figure 1).
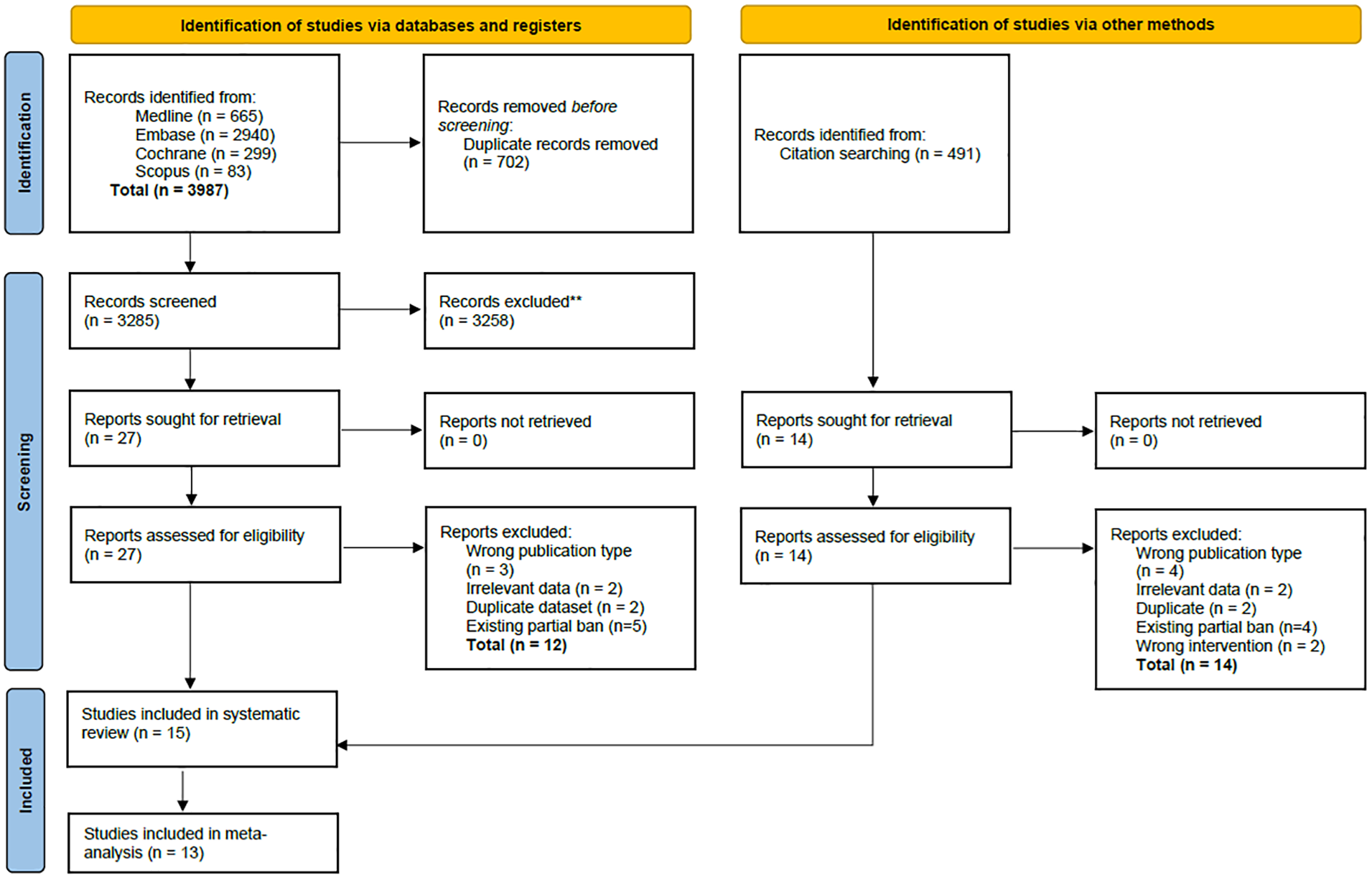
PRISMA flow diagram for review of effect of smoke-free legislation on stroke risks.
One paper 18 examined the smoke-free legislation in three US states (Florida, New York and Oregon) and only Florida had no county-level comprehensive smoke-free air laws in place before the statewide law was enacted. However, the paper did not provide sufficient data to evaluate the effect estimate. Another paper 45 did not provide the incidence of stroke events before and after the smoke-free ban was implemented necessary to calculate the RR. These two papers were hence not included in the meta-analysis.
Baseline characteristics
The characteristics of included studies (published between 2010 and 2022) are shown in Table 1 and eTable 1. Six studies23,35,37,38,40,45 were based in Europe, five17–19,22,42 in North America and four studies20,36,39,41 in East Asia. The scale of legislation differed between studies, with six studies35,37–40,45 analysing country-wide legislation, five20,23,36,41,42 city-wide, three17–19 state-wide and one 22 at the provincial level. Smoking legislation included in these studies did not encompass e-cigarette and vaping products. In terms of the statistical models used, nine studies18,20,22,23,35,36,40,41,45 were interrupted time series, four studies17,19,39,42 were controlled before-and-after and two studies37,38 were uncontrolled before-and-after.
Summary of study design and characteristics of included studies.

Not applicable.
Males and females.
Workplaces and restaurants.
Workplaces, restaurants and bar.
Among the 15 studies included in the analysis, 12 studies17,19,20,22,23,35–38,40,41,45 specifically investigated the impact of WRB bans on stroke risk. There was a single study 18 in the categories of WR and workplaces-only bans each. The remaining study 42 analysed three separate phases on a city-wide ban. Seven out of fifteen studies17,19,22,35,36,39,42 had accounted for non-tobacco related conditions and/or control regions.
Hospital admissions were the most commonly reported,17,18,22,23,36–39,41,42 followed by mortality rate,20,35,36 disease incidence,40,45 hospital discharge 19 and emergency transportations. 39 The median length of follow-up was 24 months (range: 3–67).
Three papers23,38,41 were evaluated to be of low risk, eight papers17,18,20,35,36,40,42,45 had some concerns and four papers19,22,37,39 were deemed to be of high risk (eTable 2) based on the ROBINS-E tool. 28
Meta analysis
Several studies examined more than a single region, 23 outcome 36 or stroke subtype 40 ; as such, 13 eligible studies yielded 16 effect estimates which were included in the final meta-analysis.
Nine studies assessed the association of comprehensive smoking bans involving WRB with the rate of hospital admission due to stroke. There was a significant reduction in the risk, with a RR of 0.918 (95% CI, 0.872–0.967) (Figure 2).
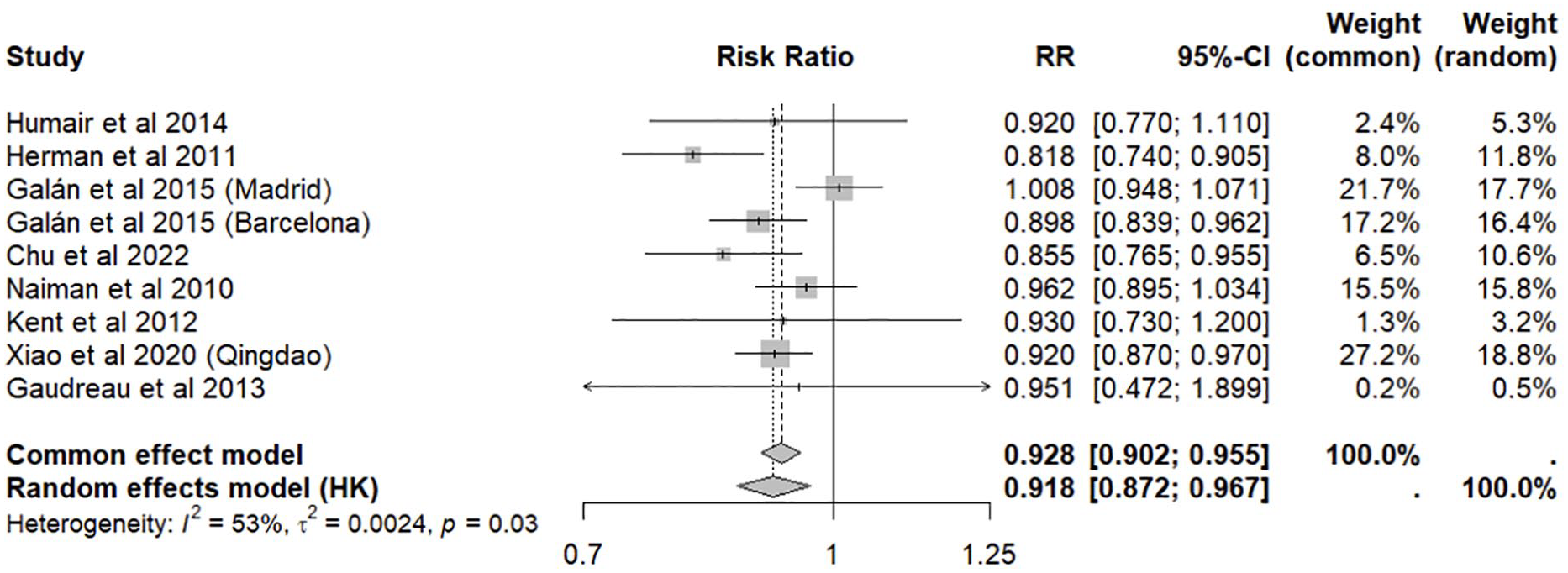
Meta-analysis of smoke-free legislation in workplaces, restaurants and bars (WRB) on stroke hospital admissions.
We observed a non-significant pooled reduction in stroke mortality with comprehensive smoking bans involving WRB in three studies (RR, 0.987; 95% CI, 0.952–1.022) (Figure 3).
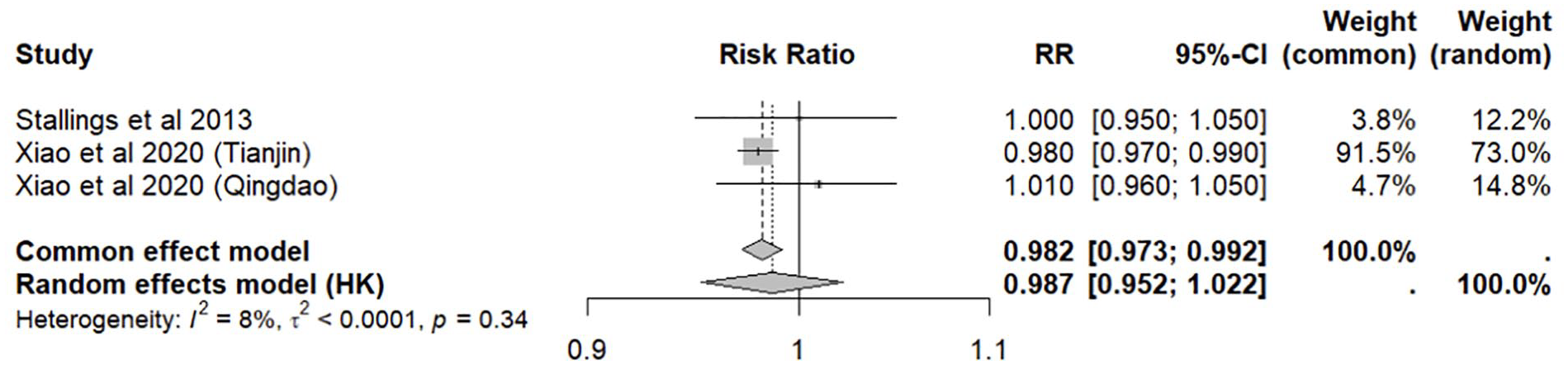
Meta-analysis of smoke-free legislation in workplaces, restaurants and bars (WRB) on stroke mortality.
Sensitivity analysis of studies accounting for non-smoking related conditions and/or control regions with no smoking bans (n = 4) revealed a similar effect estimate with reduced inter-study heterogeneity (RR, 0.906; 0.806–1.019; I2 = 55%) (Figure 4).
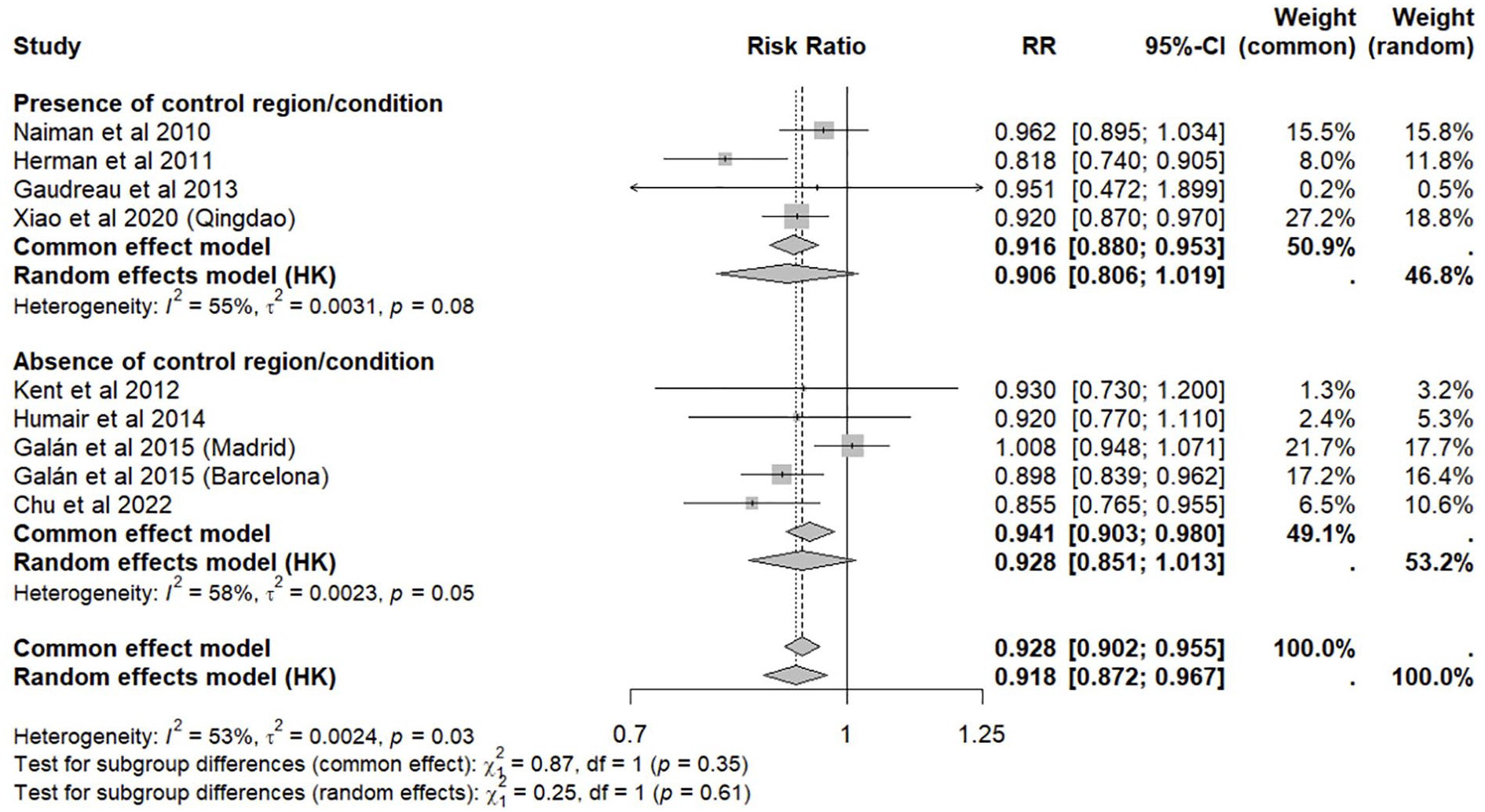
Meta-analysis of smoke-free legislation in workplaces, restaurants and bars (WRB) on stroke hospital admissions, stratified by presence or absence of control region and/or condition.
The subgroup meta-analysis by high-moderate (n = 6) versus low (n = 3) risk of bias showed no significant difference in pooled risk ratio between the two groups (p = 0.25) (eFigure 1).
In order to ascertain whether studies with longer follow-up duration produced larger effect sizes and to identify any minimum duration for a significant effect to be observed, we produced a forest plot with the studies arranged in ascending order of follow-up duration. There was no visual correlation between follow-up duration and effect sizes, hence we did not proceed with further analysis to interrogate this (eFigure 2).
The effect of more comprehensive bans on hospital admissions for stroke was determined using meta-regression with dummy coded variables representing the three main categories (W, WR, WRB) (eTable 3). Regression coefficients were found to be statistically insignificant.
The funnel plot appears asymmetrical, suggesting possible publication bias for studies examining hospital admissions due to stroke and comprehensive smoke-free bans in WRB (eFigure 3). However, Egger’s and Begg’s tests for regression intercept did not indicate a statistically significant publication bias (p = 0.516 and 0.835 respectively).
Discussion
This is, to our knowledge, the largest systematic review and meta-analysis focussed on ascertaining the effects of public smoke-free legislation on stroke risk specifically. After examining 15 studies of smoke-free legislations around the world, the main finding was that the implementation of comprehensive smoking bans involving WRB were associated with a significant reduction in stroke hospital admissions. We did not find evidence that this conclusion was affected by systemic bias in the included studies, follow-up duration or presence of controls. There were insufficient data points to draw conclusions about workplaces-only and WR bans.
While the effectiveness of public smoke-free legislations in reducing the risk of acute myocardial infarction 15 is well studied, the evidence regarding stroke is less conclusive. Findings from different regions vary, with some studies reporting reductions in both stroke-related hospital admissions17–19 and stroke mortality rates 20 following smoking bans, while others21–24 show no such effect. Factors including differences in the way the bans were designed, implemented, enforced and evaluated may explain these inconsistent findings. Discrepancies in findings may be influenced by the varying prevalence of strokes across different regions. For instance, Loomis and Juster reported that areas with a greater burden of stroke present greater potential for significant reduction in stroke-related hospital admissions. 18 Our meta-analysis, which pooled data from 13 eligible studies conducted across 15 diverse geographical areas, revealed a substantial and statistically significant decrease of 7.4% on average in the risk of stroke admissions. Our findings provide assurance that policy interventions effectively mitigate secondhand smoke exposure at a population level, consequently reducing the incidence of strokes. This makes sense in the context that a body of epidemiological research has identified secondhand smoke exposure as an important risk factor for stroke. 46
The inclusion of control regions and/or non-tobacco related conditions as non-equivalent dependent variables, which are not expected to respond to the intervention, but exposed to the same historical validity threats, 47 enhances the ability of studies to effectively control for confounding factors. 44 This approach taken by some studies enabled a more precise delineation of the impact of legislative policies on stroke risk. The subgroup analysis of these higher quality studies revealed a RR of 0.906 which is materially similar to that of our main analysis of 0.918, demonstrating that our effect estimate from the main analysis is robust. Moreover, the subgroup analysis of these studies yielded a lower interstudy heterogeneity, suggesting that the impact of smoking bans may have been underestimated in certain studies without adequate controls. Any future studies on smoke-free legislation health outcomes should include control conditions and control regions for greater internal validity to further substantiate their findings.
Although we did not find evidence amongst the included studies to show that a longer follow-up period post-smoking ban leads to greater effects on stroke risk, current evidence supports a temporal association between the introduction of national smoke-free bans and subsequent reductions in smoking-related morbidity and mortality, specifically cardiovascular risk. 13 Bans do require time for enforcement and compliance for their effects to show. 48 Similarly, effects may take time to accumulate; this explains the lack of significant change in stroke mortality seen amongst the pooled studies in which the median follow up length was only 2 years. Longitudinal studies examining more data points over longer follow-up periods are warranted to confirm this association and ascertain the true impact on stroke mortality.
Whilst originally intended, data limitations posed a significant challenge in uncovering a dose-response relationship to elucidate a possible link between comprehensiveness of smoke-free legislation and magnitude of stroke risk reduction. Regression analysis did not reveal any demonstrable relationship between the comprehensiveness of the smoking ban (W, WR and WRB) with the risk of hospital admission for stroke in the present study, but this is presumably due to the aforementioned data limitations (only one dataset each for workplaces-only and WR). However, we note that there is evidence from prior studies that the risk of SHS is dependent on the comprehensiveness of the smoke-free law implemented. 46 Future studies on upcoming laws implementing partial bans can help to augment this analysis for greater statistical power.
While smoke-free legislations are thought to reduce stroke risk through reduced SHS exposure for non-smokers, it is possible that another mechanism is through the reduction in the prevalence of smoking itself. While not specifically studied in our study, the contributing role of this possible mechanism is supported by multiple studies from Anglo-America, 49 Europe 50 and Asia 51 provide strong evidence that such legislation can lead to a modest decline in smoking rates. Notably, comprehensive bans have a greater effect on smoking cessation and prevalence compared to partial bans. However, this effect is often delayed due to the challenges of overcoming addiction and behavioural change. A study in Switzerland found it took a year for comprehensive bans to significantly reduce smoking rates, highlighting the importance of early implementation for maximum impact. 52
Various mechanisms through which smoking can increase the risk of stroke have been proposed. Smoking can lead to carotid atherosclerosis,53,54 endothelial dysfunction55–57 and inflammation, 58 and expose smokers to oxidative damage from highly reactive oxygen species generated by cigarette combustion. 59 A meta-analysis also demonstrated that smoking was associated with an increased risk of atrial fibrillation in a dose-dependent manner. 60 Studies have also shown that secondhand smoke can impact non-smokers to a significant and deleterious extent.61,62 Therefore, smoke-free bans are likely to confer benefits to the whole population.
Successful implementation of smoke-free legislation is multifactorial and is in part dependent on stringent enforcement of the ban by local law enforcers and public compliance of the ban.63,64 Mackay et al. 45 reported an initial benefit in ischaemic stroke reduction which partially reverted back to pre-legislative levels, a trend attributed to waning enforcement over time. In this regard, studies have demonstrated that the compliance of smoking bans can be improved through anti-tobacco educational campaigns to enhance smokers’ knowledge on health risks, 65 and signages and penalties for violations. 66 General attitudes towards smoking culture and tobacco industry play a huge role in the success of smoking bans, especially in regions where tobacco holds historical and economical importance.67–69 Furthermore, secondhand smoke exposure frequently occurs within homes, which falls outside public smoke-free legislation.70,71 This may have limited the effect of public smoking bans on reduction in stroke risk.
Recently, there has also been a dramatic increase in the use of alternative tobacco products and electronic nicotine delivery systems (ENDS) worldwide, such as vaping and e-cigarettes, which produce deleterious effects and are not necessarily covered within public smoking bans.72–74 More studies investigating the health impact of ENDS are needed in the future.
There has also been a growing trend of increasing ischaemic stroke incidence among younger individuals, 75 in which smoking prevalence likely plays a contributory role. 76 Existing studies have reported that the dose-response relationship between cigarette smoking and ischaemic stroke risk in both young men 77 and women 78 is the strongest compared to other age groups. Future studies should focus on the effect of smoking bans on the prevalence of ischaemic stroke rates in young people.
The present study demonstrated a significant decrease in hospital admissions for stroke with implementation of smoke-free laws and this potentially translates to lower healthcare expenditure and more efficient utilisation of healthcare resources. A similar effect has been observed in studies examining AMI-related hospitalisations and the cost savings of the smoking bans.79,80 This economic effect can be considered by policy makers when developing smoking-related legislation.
Limitations
Our study has several limitations. Firstly, differentiation of the impact of smoking bans on the risks of ischaemic and hemorrhagic stroke was not possible due to the lack of separation within most included studies regarding these two stroke types. Ischaemic and hemorrhagic strokes have different pathophysiologies and there may be value to disentangle them as separate outcomes. Likewise, some studies did not separate between transient ischaemic attack and stroke, and this may have diluted the actual effect of smoke-free legislation on stroke risk. Secondly, a majority of primary studies included in our review reported outcomes that were limited mainly to hospital admissions and mortality, while other adverse outcomes of stroke such as duration of hospitalisation or disability-adjusted life years (DALY) were not as commonly measured. Thirdly, studies that reported smoke free legislation other than in WRB and studies within administrative regions that already had a partial ban in place prior to comprehensive smoking bans were excluded to minimise inconsistencies in pre- versus post-ban analysis. As a result, the full effect of smoke free legislation implemented may be underestimated. Fourthly, we could not ascertain the effects on stroke risk in subpopulations of interest (e.g. age and gender) due to lack of data from the primary studies. Finally, the difference in timescales (data collected weekly vs monthly vs annually) between studies could have contributed in part to the heterogeneity observed in this study. Future research, in collaboration with epidemiologists, policymakers, and relevant stakeholders, would benefit from a standardised methodology to enhance utility for policymaking and ease of assessment, considering seasonal variations, autocorrelation, and other non-linear trends. The time scale should be made consistent across studies to allow for easier comparison (e.g. standardising to a monthly rate of hospital admission). Standardisation across studies will contribute to a more comprehensive understanding of the true effects of smoke-free laws on stroke, though we recognise the potential for collecting data at a finer time resolution will differ for resource-challenged settings.
Conclusion
This systematic review and meta-analysis found that legislative smoking bans in public spaces across different regions were associated with a reduced risk of hospital admission for stroke, supporting their role in public health policymaking.
Supplemental Material
sj-pdf-1-eso-10.1177_23969873241293566 – Supplemental material for Impact of smoke-free legislation on stroke risk: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-eso-10.1177_23969873241293566 for Impact of smoke-free legislation on stroke risk: A systematic review and meta-analysis by Zhuo Xun Chua, Chern Yeh Lai Amanda, Timothy Jia Rong Lam, Jamie Si Pin Ong, Shermane Yun Wei Lim, Shivaram Kumar, Mervyn Jun Rui Lim, Benjamin Yong Qiang Tan, Joel Aik and Andrew Fu Wah Ho in European Stroke Journal
Footnotes
Acknowledgements
We would like to express gratitude to Madam Rebecca Lavanie David, Senior Medical Librarian at Nanyang Technological University, and Madam Toh Kim Kee, Senior Medical Librarian at National University of Singapore, for their guidance in the search strategy design and literature search.
Correction (May 2025):
Article Type updated from Review Article to Systematic Review
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by Singapore Heart Foundation. T.J.R.L. is supported by the SingHealth Medical Student Talent Development Award.
Ethical approval
Not applicable as it is a systematic review.
Informed consent
Not applicable as it is a systematic review.
Contributorship
All authors reviewed and edited the manuscript and approved the final version of the manuscript. Study concept and design: AFWH. Acquisition, analysis, or interpretation of data: ZXC, CYLA, TJRL, JSPO, SYWL, SK. Drafting of the manuscript: ZXC, CYLA, TJRL, SYWL, SK. Critical revision of the manuscript for important intellectual content: ZXC, TJRL, MJRL, BYQT, JA, AFWH. Statistical analysis: ZXC, TJRL, JA, AFWH. Administrative, technical, or material support: ZXC, TJRL, MJRL, BYQT, JA, AFWH. Study supervision: AFWH.
Trial registration
Not applicable as it is a systematic review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.