
Abstract
Background:
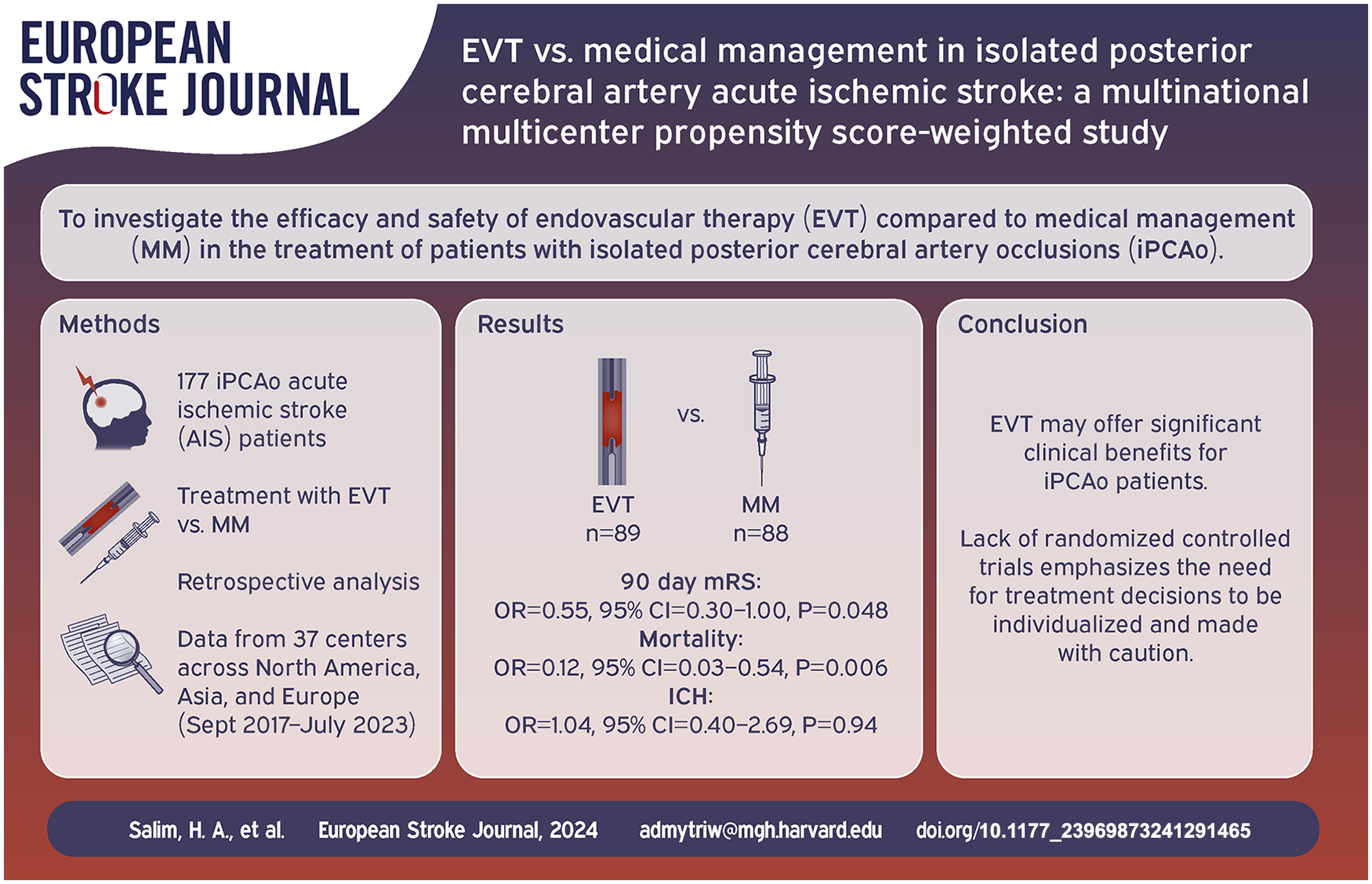
Despite the proven effectiveness of endovascular therapy (EVT) in acute ischemic strokes (AIS) involving anterior circulation large vessel occlusions, isolated posterior cerebral artery (PCA) occlusions (iPCAo) remain underexplored in clinical trials. This study investigates the comparative effectiveness and safety of EVT against medical management (MM) in patients with iPCAo.
Methods:
This multinational, multicenter propensity score-weighted study analyzed data from the Multicenter Analysis of primary Distal medium vessel occlusions: effect of Mechanical Thrombectomy (MAD-MT) registry, involving 37 centers across North America, Asia, and Europe. We included iPCAo patients treated with either EVT or MM. The primary outcome was the modified Rankin Scale (mRS) at 90 days, with secondary outcomes including functional independence, mortality, and safety profiles such as hemorrhagic complications.
Results:
A total of 177 patients were analyzed (88 MM and 89 EVT). EVT showed a statistically significant improvement in 90-day mRS scores (OR = 0.55, 95% CI = 0.30–1.00, p = 0.048), functional independence (OR = 2.52, 95% CI = 1.02–6.20, p = 0.045), and a reduction in 90-day mortality (OR = 0.12, 95% CI = 0.03–0.54, p = 0.006) compared to MM. Hemorrhagic complications were not significantly different between the groups.
Conclusion:
EVT for iPCAo is associated with better neurological outcomes and lower mortality compared to MM, without an increased risk of hemorrhagic complications. Nevertheless, these results should be interpreted with caution due to the study’s observational design. The findings are hypothesis-generating and highlight the need for future randomized controlled trials to confirm these observations and establish definitive treatment guidelines for this patient population.
Keywords
Introduction
Endovascular therapy (EVT) is a highly effective treatment for acute ischemic stroke (AIS) patients with anterior circulation large vessel occlusions (LVO) and basilar artery occlusions in both early and late time windows.1–5 Isolated posterior cerebral artery (PCA) occlusions (iPCAo) affect approximately 5%–10% of AIS patients.6,7 However, to date, no randomized controlled trial comparing endovascular therapy (EVT) with medical management (MM) for patients with iPCAo has been published, as these patients were not included in prior trials. While iPCAo patients tend to present with symptoms that are not well captured in the National Institutes of Health Stroke Scale (NIHSS), more proximal occlusions affecting the thalamus, cerebral peduncle, and primary visual cortex can lead to significant disability in these patients. 6
Intravenous thrombolysis (IVT) is considered the standard-of-care but is largely limited to patients who present within 4.5 h from symptoms onset,8,9 and results in recanalization in only 50% of patients. 10 Recent case-control studies of AIS patients with iPCAo, such as PLATO, 11 ACAPULCO, 12 and TOPMOST, 13 have shown conflicting results; these studies suggested higher rates of early neurological improvement and excellent clinical outcomes, but PLATO and ACAPULCO raised concerns over increased risk for symptomatic intracranial hemorrhage (sICH) and mortality with EVT. In this multicenter registry study, we sought to investigate the safety and outcomes of EVT compared to MM in AIS patients with iPCAo.
Methods
Our study is analysis within the Multicenter Analysis of primary Distal medium vessel occlusions: effect of Mechanical Thrombectomy (MAD-MT) registry.14–25 This manuscript adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 26
Ethical considerations and study approval
The institutional review board or local ethical standards committee at each of the 37 participating sites across North America, Asia, and Europe granted approval for this study. Due to the study’s retrospective nature, informed consent was waived. For all procedures, emergency consent was obtained, and in cases where patients were unable to provide consent, consent was obtained from legally authorized proxy when possible. All data from this study’s findings are available from the corresponding author upon reasonable request.
Study population and inclusion criteria
We focused on patients with acute ischemic stroke due to DMVO as previously described. Inclusion criteria were as follows: (1) iPCAo acute ischemic stroke patients with DMVO in the P1, P2, and P3 segments without additional occlusion in other cerebral artery. (2) Patients who underwent MM or EVT with or without adjunctive IVT. (3) Pre-stroke mRS of 0 or 1. We excluded patients who received intraarterial thrombolysis.
Data collection process
Data collection spanned from September 2017 to July 2023, involving consecutive patients treated with MM or EVT. This was a retrospective review of prospectively collected data. Local neurointerventionalists or vascular neurologists assessed angiographic treatment success before forwarding data to the MAD-MT consortium. Each center self-reported this data.
Variables and data documentation
We recorded comprehensive baseline clinical and demographic characteristics, including sex, age, hypertension, hypercholesterolemia, diabetes mellitus, atrial fibrillation, and smoking status. Hypercholesterolemia was defined as either a documented history of elevated low-density lipoprotein cholesterol (LDL-C) levels or the use of lipid-lowering medications as documented in patients’ records. Furthermore, we documented the pre-stroke mRS score, the occluded vessel and NIHSS at presentation. Additionally, patients were stratified into subgroups based on their occlusion location during the initial angiography, differentiating between medium (P1) and distal branches (P2, P3) of the posterior cerebral artery. 27
Additional data of interest encompassed antiplatelet and anticoagulation medication status. Patients were classified as being on antiplatelet therapy if they were taking any home antiplatelet medications (e.g. aspirin, clopidogrel, prasugrel, cilostazol, etc.) upon presentation. Similarly, patients were considered anticoagulated if they were on home vitamin K antagonists or direct oral anticoagulants at the time of presentation. Moreover, time from symptom onset to arterial puncture and recanalization, anesthesia type, access site (femoral or radial), and post-MT imaging modalities (CT, MR, or none) were recorded.
Procedural and technical details
Treatments included MM, which refers to the standardized care protocol for stroke which included IVT where applicable, management of risk factors, and secondary prevention measures, or EVT encompassed mechanical thrombectomy procedures, with or without adjunctive IVT in eligible patients.
Decisions regarding treatment modalities and other periprocedural details such as MT access site (femoral or radial artery), endovascular strategy (aspiration, stent retriever, combined or rescue techniques), number of passes, and final mTICI scoring were in accordance with the treating physician’s discretion and institutional protocols.
For IVT, it was given per standard guidelines, using either Alteplase or Tenecteplase. Alteplase was given at a standard dose of 0.9 mg/kg, with 10% of the total dose delivered as an initial bolus followed by an infusion of the remaining 90% over 60 min. Tenecteplase was administered in a single intravenous bolus at a dose of 0.25 mg/kg, infused over 5–10 s.
Outcomes
The primary outcome was the ordinal 90 days mRS score, with secondary outcomes including functional independence (mRS 0–2), excellent outcome (mRS 0–1), mortality (mRS 6), and day 1 post admission NIHSS score. Safety outcomes were hemorrhagic complications of any type and symptomatic intracerebral hemorrhage (sICH), defined according to “The Heidelberg Bleeding Classification.” 28
Statistical analysis
We employed Inverse Probability of Treatment Weighting (IPTW) to balance the distribution of confounding variables between the EVT and MM groups.29,30 The estimation of PS weights was conducted using generalized boosted modeling (GBM) methodology. GBM is a machine learning multivariate non-parametric regression technique that estimates the PS of individuals iteratively to maximize balance in observed covariables.31,32 GBM has the capability to integrate interactions among numerous factors, hence mitigating the potential for model misspecification.32,33 Prior studies have demonstrated that GBM provides superior performance compared to logistic regression in propensity score estimation.31,34
The model included sex, age, hypercholesterolemia, occlusion location, hypertension, diabetes mellitus, atrial fibrillation presence, antiplatelet or anticoagulants use, IVT, baseline NIHSS scores, and pre-stroke mRS scores, with the aim of estimating the average treatment effect (ATE). The mean Kolmogorov-Smirnov (KS.mean) statistic was employed as a stopping criterion for assessing and summarizing balance across pretreatment variables. A 10,000-tree GBM model with an interaction depth of 3, a shrinkage value of 0.01, and a bag fraction of 1 was utilized. The end propensity scores for the two treatments using observable covariates was estimated using the R-package twang. 35
The analyses used balance diagnostics for propensity score weights, as per known practices. 36 The diagnostic analysis primarily examined the absolute standardized mean difference (ASMD) between weighted and unweighted variables. In our analysis, we deemed any ASMD greater than 0.10 to indicate covariate imbalance.37,38 To minimize the mean square error a doubly robust estimation was employed, wherein additional adjustments were made for the covariates using weighted multivariable logistic regression analysis.31,39 All statistical analyses were performed using R Studio Version 4.2.2. No imputations were made, and adjustments for multiple testing were not performed.
Results
Baseline characteristics
The baseline characteristics of the included patients are summarized in Table 1. Our study included 177 iPCAo patients, with 88 in the MM group and 89 in the EVT group. The median age was higher in the EVT group compared to the MM group (74 vs 68 years, p = 0.047). Hypercholesterolemia was more prevalent in the MM group (59% vs 43%, p = 0.029), while diabetes was more prevalent in the MM group as well (40% vs 21%, p = 0.008). The baseline NIHSS was higher in the EVT compared to the BMT group (8 vs 6, p = 0.0006). The site of initial occlusion significantly differed between the groups, with medium (P1) occlusions being more common in the EVT group (48% vs 22%, p < 0.001). No significant differences were observed in sex distribution, hypertension, atrial fibrillation, smoking status, previous use of antiplatelet or anticoagulant drugs, or pre-stroke mRS.
Baseline characteristics of the included patients.
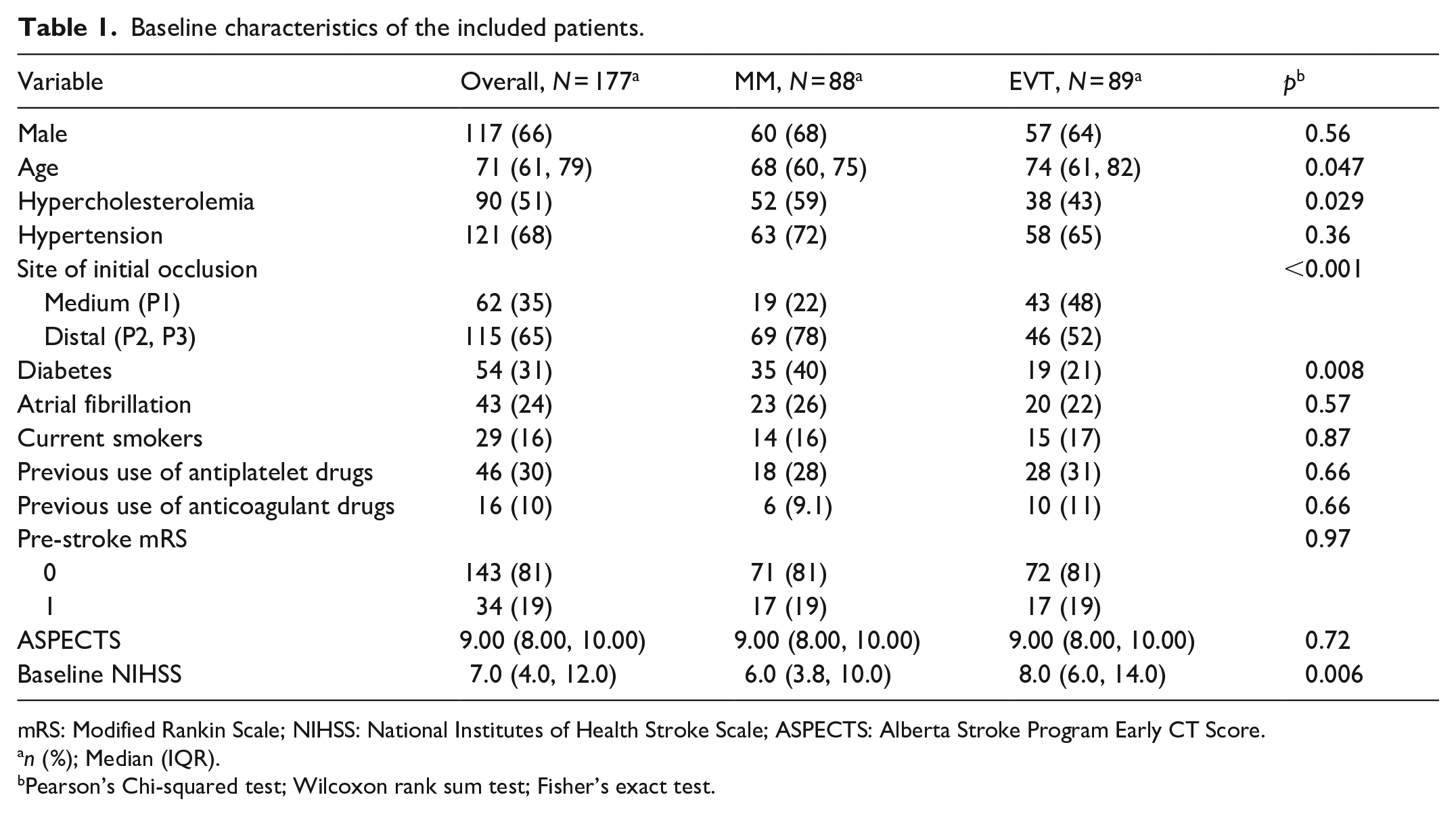
mRS: Modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; ASPECTS: Alberta Stroke Program Early CT Score.
n (%); Median (IQR).
Pearson’s Chi-squared test; Wilcoxon rank sum test; Fisher’s exact test.
Periprocedural details
Periprocedural details are presented in Table 2. IVT was administered more frequently in the MM group compared to the EVT group (63% vs 46%, p = 0.028). The median time from onset to IVT was 168 min overall, with no significant difference observed in the MM group compared to the EVT group (162 vs 170 min, p = 0.74). EVT techniques included aspiration (35%), stent retriever (11%), or both (54%). The medians of onset to arterial puncture, puncture to recanalization time, and onset to recanalization time were 300, 34, and 340 min, respectively.
Periprocedural details of the included patients.

IVT: intravenous thrombolysis; ASPECTS: Alberta Stroke Program Early CT Score; CS/LA: conscious sedation/local anesthesia; GA: general anesthesia.
n (%); Median (IQR).
Pearson’s Chi-squared test; Wilcoxon rank sum test; Fisher’s exact test.
Clinical and safety outcomes
Clinical outcomes following interventions are detailed in Table 3. Before any adjustment, no significant differences were observed in day 1 NIHSS scores, day 1 NIHSS shift, 90-day mRS scores of 0–1 and 0–2, 90-day mortality, sICH, or ICH of any type between the patients treated with MM versus EVT. However, there was a trend toward differences in types of ICH, with subarachnoid hemorrhage (SAH) being more common in the EVT group (5.7% vs 0%, p = 0.08).
Clinical outcomes following acute stroke interventions.
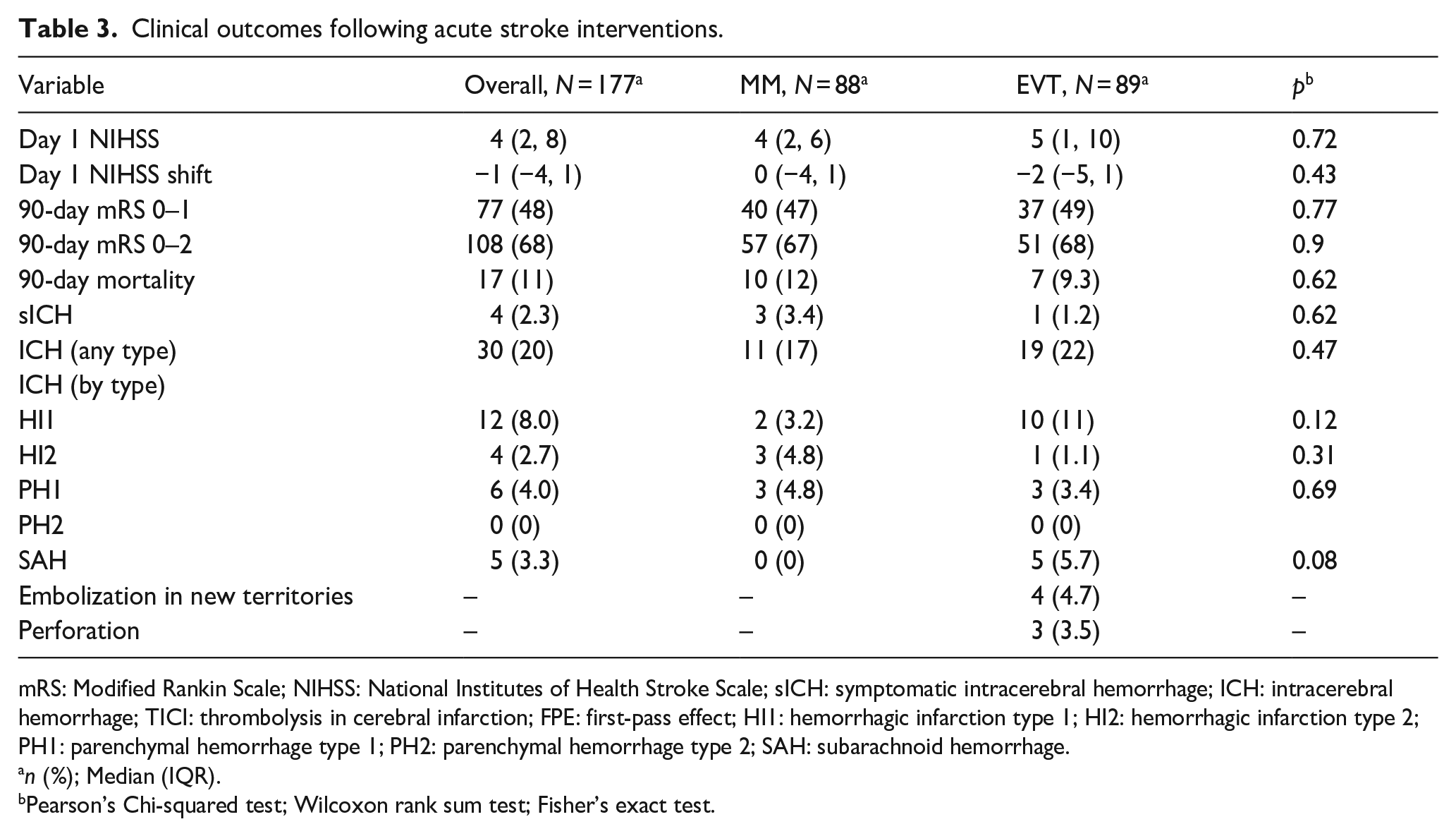
mRS: Modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; sICH: symptomatic intracerebral hemorrhage; ICH: intracerebral hemorrhage; TICI: thrombolysis in cerebral infarction; FPE: first-pass effect; HI1: hemorrhagic infarction type 1; HI2: hemorrhagic infarction type 2; PH1: parenchymal hemorrhage type 1; PH2: parenchymal hemorrhage type 2; SAH: subarachnoid hemorrhage.
n (%); Median (IQR).
Pearson’s Chi-squared test; Wilcoxon rank sum test; Fisher’s exact test.
Univariable and multivariable logistic regression and IPTW models
The analysis of the ordinal 90-day mRS scores did not indicate a statistically significant difference between EVT and MM in the univariable (OR = 0.86, 95% CI = 0.37–2.01, p = 0.73) or multivariable models (OR = 0.60, 95% CI = 0.32–1.11, p = 0.10). However, the IPTW model suggested a statistically significant benefit with EVT, demonstrating a 45% improvement in the odds of achieving a lower 90-day mRS score compared to MM (OR = 0.55, 95% CI = 0.30–1.00, p = 0.048; Table 4).
Univariable and multivariable logistic regression and IPTW evaluation of outcomes after EVT versus MM of posterior cerebral artery occlusion.
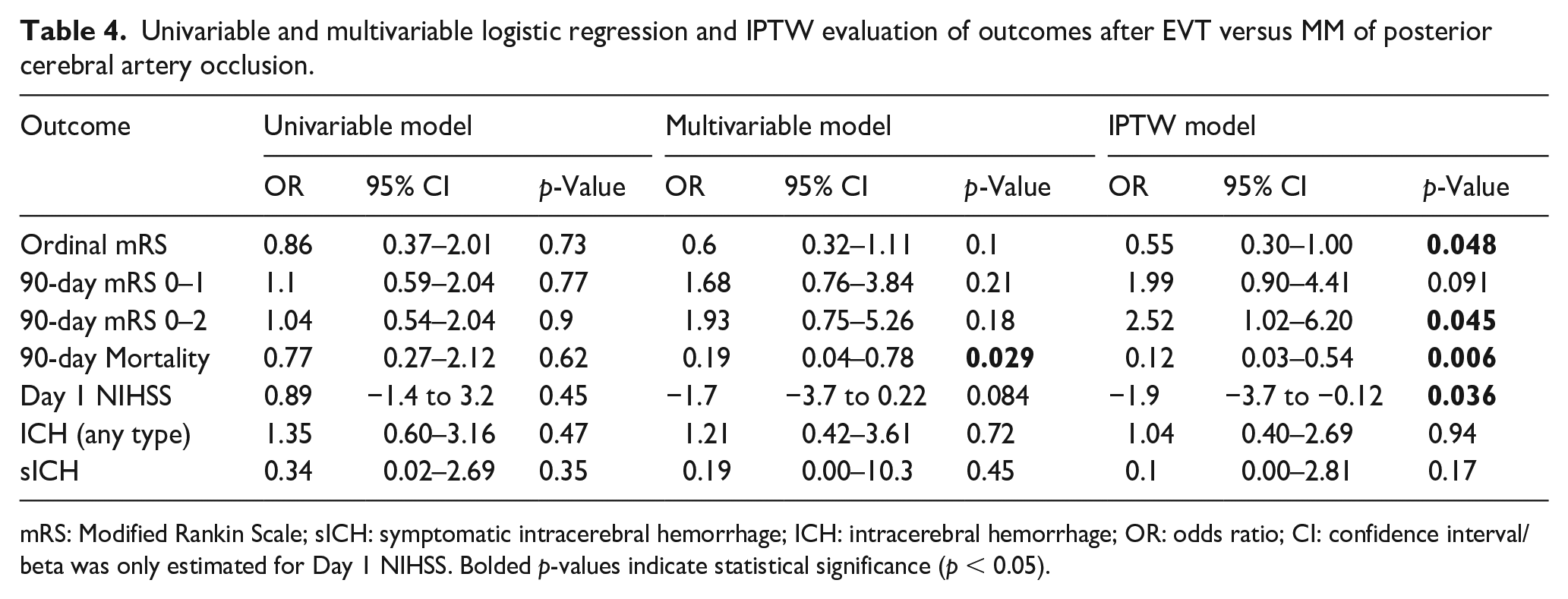
mRS: Modified Rankin Scale; sICH: symptomatic intracerebral hemorrhage; ICH: intracerebral hemorrhage; OR: odds ratio; CI: confidence interval/beta was only estimated for Day 1 NIHSS. Bolded p-values indicate statistical significance (p < 0.05).
For excellent 90-day outcome (mRS 0–1), the univariable model indicated no significant difference (OR = 1.1, 95% CI = 0.59–2.04, p = 0.77), while the multivariable model (OR = 1.68, 95% CI = 0.76–3.84, p = 0.21) and IPTW model (OR = 1.99, 95% CI = 0.90–4.41, p = 0.091) suggested a trend toward improved outcomes with EVT, though this did not reach statistical significance. However, the IPTW model revealed a significant benefit of EVT in achieving functional independence (mRS 0–2) at 90 days, with more than a twofold increase in the likelihood of this outcome compared to MM (OR = 2.52, 95% CI = 1.02–6.20, p = 0.045; Table 4).
Additionally, a significant reduction in 90-day mortality was observed with EVT. The multivariable model showed that the odds of death were 81% lower with EVT (OR = 0.19, 95% CI = 0.04–0.78, p = 0.029), and the IPTW model further supported this, indicating an 88% reduction in mortality risk (OR = 0.12, 95% CI = 0.03–0.54, p = 0.006). The change in the NIHSS score from admission to day 1 showed no significant difference in the univariable model (Beta = −0.89, p = 0.45) and the multivariable model (Beta = −1.7, p = 0.084) but indicated a significant improvement in IPTW model (Beta = −1.9, p = 0.036). The rates of any type of ICH and sICH did not show significant differences across the models (Table 4).
Discussion
In this propensity score-weighted analysis of 177 patients with early window iPCAo who underwent either EVT or MM, we found that EVT was associated with better clinical outcomes including lower day 1 NIHSS, lower 90-day mRS, and reduced risk of death. Furthermore, our results show that EVT can lead to very high recanalization rates in iPCAo patients (95% mTICI 2b or higher) with an average of two thrombectomy passes, and acceptable complication rates (4.7% embolization in a new territory, 3.5% vessel perforation). Importantly, our findings do not show an increased risk of sICH with EVT.
In the absence of randomized data, available data can be derived from large propensity-score analyzed registries such as TOPMOST 13 and PLATO. 11 TOPMOST included 184 matched patients with isolated PCA P2/3 segment occlusions and demonstrated a strong trend toward early NIHSS improvement, as well as a treatment effect of EVT in patients with baseline NIHSS of 10 or higher, and in patients who did not receive IVT. Rates of any ICH were similar in EVT compared to MM patients. PLATO included 1023 patients with isolated PCA P1, P2, or P3 segment occlusions, of whom 378 underwent EVT and 645 underwent MM. Like TOPMOST, PLATO demonstrated higher odds of early NIHSS decrease and excellent functional outcome with EVT. However, EVT patients in PLATO had higher rates of sICH and mortality (6.2% vs 1.7%, and 10.1% vs 5.0%, respectively), which raises concerns over safety of EVT in patients with isolated PCA occlusions. A meta-analysis on this topic confirmed higher odds of early neurological improvement and visual field recovery with EVT compared to MM, but failed to demonstrate a difference in 90-day functional outcomes. 40 Furthermore, a trend toward sICH without difference in mortality was reported. In contrast to these findings, another meta-analysis did not show any differences in early neurological improvement or 90-day functional outcomes but suggested increased mortality after EVT. 41
The results of the present study contribute to these conflicting data with regards to both efficacy and safety of EVT in patients with iPCAo. Our findings of higher odds of early NIHSS improvement and 90-day mRS 0–2 support the results of TOPMOST and PLATO that EVT in patients with isolated PCA occlusions leads to better functional outcomes. The fact that both our statistical models are consistent in their demonstration of an overall treatment effect with EVT compared to MM suggests robustness of our results. Similar to TOPMOST, and contrary to PLATO and ACAPULCO, we did not find increased rates of sICH other than trends toward SAH (5.7% vs 0.0%) and HI1 ICH (11% vs 3.2%). Importantly, our cohort does not confirm the higher rates of death found in PLATO; in contradistinction, our analysis demonstrated decreased odds of 90-day mortality after EVT. The better results in our study might at least partially be explained by higher recanalization rates (95% TICI 2B or higher in the present study compared to 79.3% in PLATO), suggesting differences in EVT technique and/or stroke etiology. 42
There are several limitations to this study, including its retrospective and non-randomized design that is susceptible to selection bias. Moreover, the mRS and NIHSS scales used as primary outcome measures in this study may not fully capture the extent of neurological consequences in iPCAo, particularly those related to visual, cognitive, and neuropsychological functions. Future research would benefit from incorporating more sensitive neuropsychological assessments and quality of life evaluations, which could provide a more comprehensive understanding of the impact of treatment on iPCAo stroke patients’ outcomes. We did not collect data on final infarct volumes, stroke etiology, or vision recovery. Furthermore, while control imaging was performed in all included cases as per protocol, the specific imaging modality for patients who underwent MM was not collected. Additional limitations include lack of site-specific information, which precludes site-level analyses, and lack of core-lab adjudication for vessel occlusion site, mTICI grading, and ICH grading. We included patients without prestroke disability in our analysis (mRS 0–1), whereas PLATO had broader inclusion of patients with pre-stroke mRS 0–3. Finally, there is no accepted reperfusion grading system for DMVOs, and mTICI grading was conducted at the discretion of each site.
Conclusion
In conclusion, our study indicates that EVT is associated with better early neurological improvement, improved 90-day clinical outcomes, decreased mortality, and no evidence of an increase in sICH and so may offer clinical benefits for patients with iPCAo, particularly given the high recanalization rates achieved (95% mTICI 2b-3). Nevertheless, these results should be interpreted with caution due to the study’s limitations including observational design and small sample size. The findings are hypothesis-generating and highlight the need for future randomized controlled trials to confirm these observations and establish definitive treatment guidelines for this patient population.
Footnotes
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Regenhardt serves on a DSMB for a trial sponsored by Rapid Medical, serves as site PI for studies sponsored by Penumbra and Microvention, and receives stroke research grant funding from the National Institutes of Health, Society of Vascular and Interventional Neurology, and Heitman Stroke Foundation. Dr. Guenego reports consultancy for Rapid Medical and Phenox, not directly related to the present work. Dr. Clarençon reports conflicts of interest with Medtronic, Balt Extrusion (consultant), ClinSearch (core lab), Penumbra, Stryker (payment for reading), and Artedrone (Board); all not directly related to the present work. Dr. Henninger received support from W81XWH-19-PRARP-RPA form the CDMRP/DoD, NS131756 and U24NS113844 from the NINDS, and NR020231 from the NINR and received compensation from Myrobalan, Inc. and General Dynamics during the conduct of this study unrelated to this work. Dr. Liebeskind is consultant as Imaging Core Lab to Cerenovus, Genentech, Medtronic, Stryker, Rapid Medical. Dr. Yeo reports Advisory work for AstraZeneca, Substantial support from NMRC Singapore and is a medical advisor for See-mode, Cortiro, and Sunbird Bio, with equity in Ceroflo. All unrelated to the present work. Dr. Griessenauer reports a proctoring agreement with Medtronic and research funding by Penumbra. Dr. Marnat reports conflicts of interest with Microvention Europe, Stryker Neurovascular, Balt (consulting), Medtronic, Johnson & Johnson, and Phenox (paid lectures), all not directly related to the present work. Dr. Puri is a consultant for Medtronic Neurovascular, Stryker NeurovascularBalt, Q’Apel Medical, Cerenovus, Microvention, Imperative Care, Agile, Merit, CereVasc, and Arsenal Medical, he received research grants from NIH, Microvention, Cerenovus, Medtronic Neurovascular, and Stryker Neurovascular, and holds stocks in InNeuroCo, Agile, Perfuze, Galaxy, and NTI. Dr. Tjoumakaris is a consultant for Medtronic and Microvention (funds paid to institution, not personally). Dr. Jabbour is a consultant for Medtronic, Microvention, and Cerus.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical committee that approved the establishment of this consortium: ERASME Hospital Ethics Committee, Ref No. 2021/312.
Informed consent
Informed consent from patients was waived due to retrospective study design.
Guarantor
Adam A Dmytriw.
Contributorship
H.S, B.P, V.Y, B.M, N.A, D.L, M.E, K.N, N.H, S.S, A.K, J.K, S.G, L.S, B.T, R.R, J.H, N.C, J.B, A.R, J.F, S.S, A.P, C.D, M.C, X.B, L.R, J.F, P.H, R.R, M.A, P.K, T.M, J.S, T.O, A.M, P.J, A.B, F.C, J.S, T.N, R.V, A.B, D.A, N.G, M.M, V.C, B.G, I.G, C.S, M.A, C.H, H.S, C.G, D.L, A.P, A.A, I.T, T.F, E.K, B.L, A.P, V.P, M.W, A.G, A.D. contributed to the conception and design of the work. H.S, B.P, V.Y, B.M, N.A, D.L, M.E, K.N, N.H, S.S, A.K, J.K, S.G, L.S, B.T, ., R.R, J.H, N.C, J.B, A.R, J.F, S.S, A.P, C.D, M.C, X.B, L.R, J.F, P.H, R.R, M.A, P.K, T.M, J.S, T.O, A.M, P.J, A.B, F.C, J.S, T.N, R.V, A.B, D.A, N.G, M.M, V.C, B.G, I.G, C.S, M.A, C.H, H.S, C.G, D.L, A.P, A.A, I.T, T.F, E.K, B.L, A.P, V.P, M.W, A.G, A.D. were involved in the acquisition of data, and data analysis and interpretation. H.S, B.P, V.Y, B.M, N.A, D.L, M.E, K.N, N.H, S.S, A.K, J.K, S.G, L.S, B.T, R.R, J.H, N.C, J.B, A.R, J.F, S.S, A.P, C.D, M.C, X.B, L.R, J.F, P.H, R.R, M.A, P.K, T.M, J.S, T.O, A.M, P.J, A.B, F.C, J.S, T.N, R.V, A.B, D.A, N.G, I.G, M.M, V.C, B.G, C.S, M.A, C.H, H.S, C.G, D.L, A.P, A.A, I.T, T.F, E.K, B.L, A.P, V.P, M.W, A.G, A.D. drafted the work and revised it critically for important intellectual content. All authors gave final approval of the version to be published and agree to be accountable for all aspects of the manuscript.
ORCID iDs
Data availability statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.