
Abstract
Introduction:
Endovascular thrombectomy (EVT) combined with intravenous thrombolysis is the current standard treatment for acute large-vessel occlusion stroke. Beyond clear clinical benefits in the acute and post-acute phases, comprehensive evaluations of long-term outcomes, including home and workforce reintegration, remain limited. This study aimed to assess home and workforce reintegration 1 year post-EVT in a cohort of acute stroke patients and explore their association with health-related quality of life (HRQoL).
Patients and methods:
We conducted a prospective observational study of 404 patients undergoing EVT at a tertiary university medical center between October 2019 and December 2021. Patients’ functional outcomes were evaluated using the modified Rankin Scale (mRS), and HRQoL was assessed via the European Quality of Life Five Dimension Scale (EQ-5D). Data on occupational and living status were collected through standardized telephone interviews at 3- and 12-months post-treatment.
Results:
Of 357 patients with 12-month follow-up data, 33.6% had a favorable outcome (mRS 0–2). Among stroke survivors, the rate of home reintegration without nursing care was 42.1%, and workforce reintegration among previously employed patients was 43.3% at 12 months. Both outcomes were significantly associated with improved HRQoL. Lower neurological deficits and younger age were predictive of successful home and workforce reintegration.
Discussion and conclusion:
One year post-EVT, approximately 40%–50% of acute stroke patients successfully reintegrate into home and work settings. These findings underscore the need for ongoing support tailored to improving long-term reintegration and quality of life for stroke survivors.
Data access statement:
The data supporting the findings of the study are available from the corresponding author upon reasonable request and in accordance to European data privacy obligations.
Introduction
Endovascular thrombectomy (EVT) with intravenous thrombolysis is the standard of care for large-vessel occlusion stroke. 1 Among the randomized controlled trials firmly establishing this intervention, functional status as measured by the modified Rankin Score (mRS) at 3-month follow-up or its dichotomizations are usually considered as the primary outcome.2,3 Notably, the mRS is biased toward impairments of motor function and communication as compared to other domains, and does not capture all long-term impairments experienced by stroke survivors, as even patients without functional disabilities report difficulties returning to their daily activities.4,5 Return-to-work or workforce reintegration is considered an indicator of successful rehabilitation and is associated with well-being and a better quality of life, while the estimated socioeconomic costs of its failure are reported to be billions of dollars each year.6,7 Considering patient-driven outcome priorities, living at home represents an even more important outcome. 8 However, the frequency of home reintegration following EVT in patients with acute stroke remains unknown, and workforce reintegration after EVT has only been described for up to 3 months. 9
We aimed to evaluate the long-term outcomes after EVT regarding workforce and home reintegration in a monocentric cohort of 404 patients and its association with health-related quality of life (HRQoL).
Methods
Study cohort
This observational study included consecutive adult (18 years or older) patients undergoing EVT for large-vessel occlusion stroke at the University Hospital Bonn between 10/2019 and 12/2021. The study was approved by the ethics committee of the University of Bonn (054/16) and was performed in accordance with the Helsinki Declaration as revised in 2013.
The study was reported according to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist for cohort studies.
Data collection
Baseline, treatment, and outcome characteristics were determined from the medical records of the index hospitalization for acute stroke, as previously described.10,11 Functional outcome was assessed using the mRS. 2
For the collection of follow-up data, standardized telephone interviews were conducted at 3 and 12 months. The mRS and responses to the three-level European QoL-five dimensions (EQ-5D-3L) as well as assessment of occupational status and living status were obtained during the telephone interview from the patients or their next of kin. Occupational status was assessed using the following categories: employed, signed off sick, student, housewife or househusband, and retired. Baseline occupational status was assessed retrospectively at 3-month follow-up, while 3-month and 12-month occupational status were assessed at the respective time points. Accordingly, the occupational status of those deceased before 3-month follow-up remained undocumented. Living status was assessed using the following categories: living at home, receiving nursing care at home, and in a nursing home.
The EQ-5D-3L is an established instrument to assess quality of life and was used to evaluate self-reported HRQoL in our cohort, as described previously. 12 The EQ-5D utility index for each individual health state is based on a country-specific value set for each individual health state, where higher values indicate better HRQoL. As a representative validated Germany-specific value set is not available, the UK population value set was used, as previously described. 12 Death was assigned an index score of 0 per instrument validation, with 1 representing optimal health.
Study end points
The primary endpoint of this study was to describe return-to-work and return-to-home within 12 months of EVT for acute ischemic stroke.
Statistical analysis
A descriptive analysis was used for patient characteristics. Group differences were evaluated using Fisher’s exact test, Mann-Whitney U test, or unpaired Student’s t-test, as appropriate. Uni- and multivariable logistic regression analysis models were constructed to predict home and workforce reintegration. A two-sided probability value <0.05 was considered statistically significant. Analyses were performed with R (Version 4.2.1).
Results
Study cohort and baseline characteristics
Between 10/2019 and 12/2021, 404 consecutive patients were treated with EVT for acute ischemic stroke at a tertiary university hospital center. Among these, 12-month follow-up was available for 357 patients (88.6%, Figure 1). Comparing patients with 12-month follow-up to those lost to follow-up, no significant differences were detected with the exception of age: patients lost to follow-up were younger with a median age of 72 years (interquartile range [IQR], 59–81) compared to 78 years (IQR, 65–84, p = 0.024) in patients with follow-up (Supplemental Table 1).
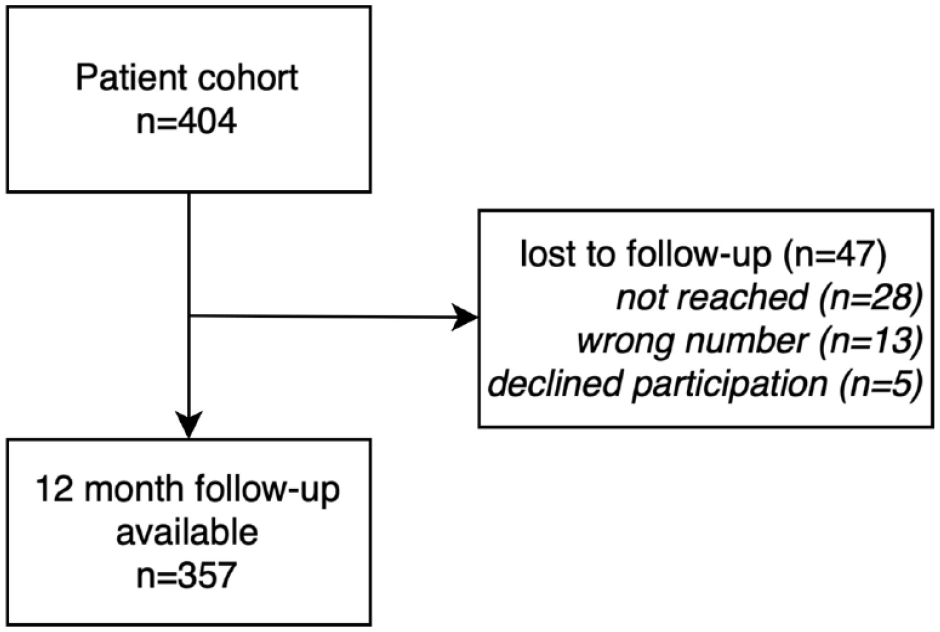
Patient inclusion flow chart.
A total of 357 patients were included in the final analysis. The median age was 78 years (interquartile range [IQR], 65–83), and 53% (n = 187) of patients were female. The median admission NIHSS score was 13 (IQR, 9–19). Intravenous thrombolysis was applied in 44.9% (n = 159) and EVT was successful in 84.7% (n = 294), defined as a mTICI of 2b or higher. Further baseline and treatment characteristics are presented in Table 1.
Baseline and treatment characteristics.
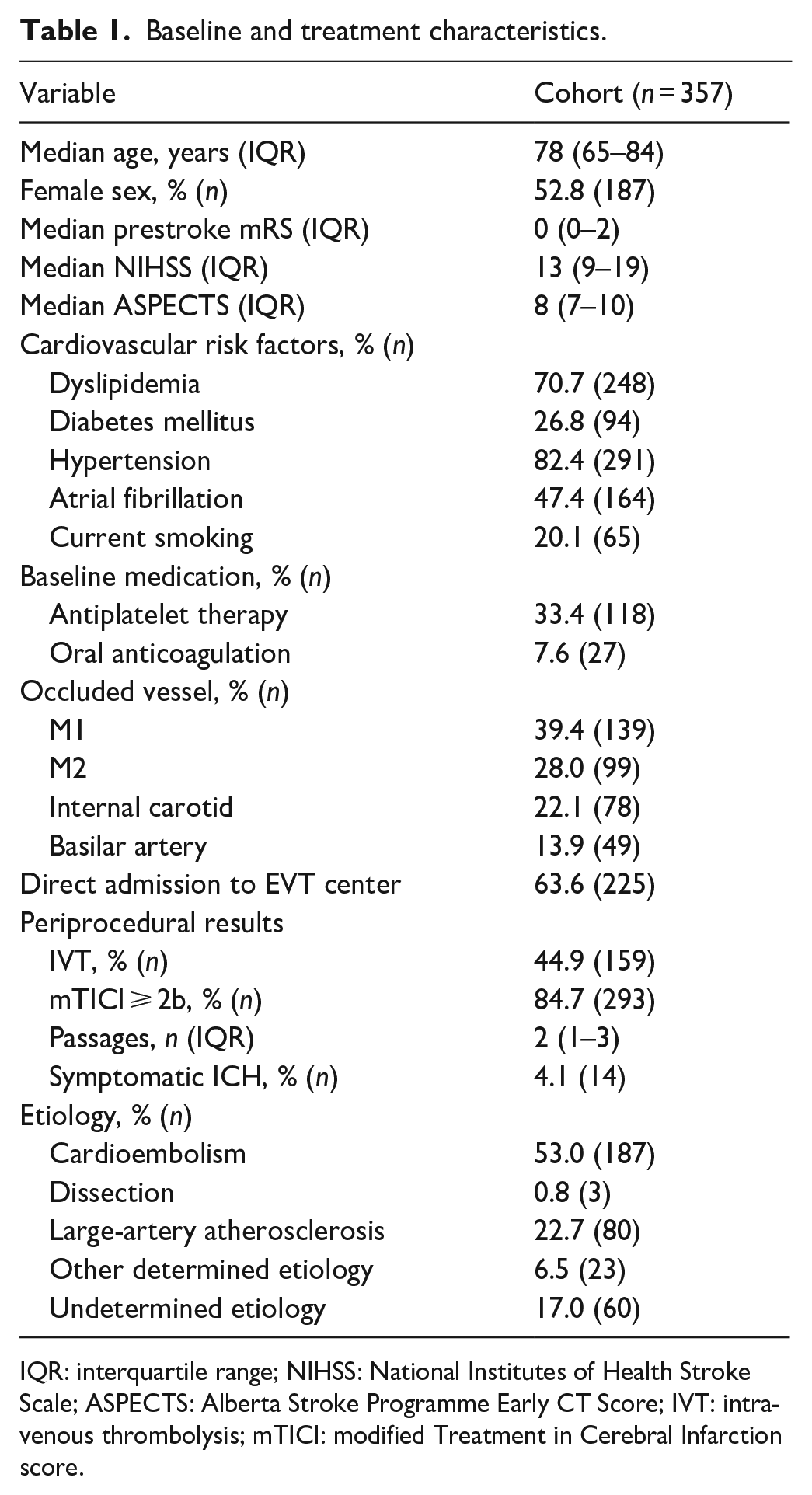
IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale; ASPECTS: Alberta Stroke Programme Early CT Score; IVT: intravenous thrombolysis; mTICI: modified Treatment in Cerebral Infarction score.
Functional outcomes after 12 months
At 12-month follow-up, 33.6% (n = 120) of patients had a favorable outcome defined as mRS 0–2, up from 30.6% (n = 120) at 3-month follow-up and 24.6% (n = 91) at discharge. Mortality was 42.0% (n = 150), compared to 32.4% (n = 127) at 3-month follow-up and 18.6% (n = 68) in hospital. The longitudinal course of the mRS from discharge until 12-month follow-up is illustrated in Figure 2(a). Compared to elderly patients (age > 65 years), younger patients were more likely to improve between 3-month and 12-month follow-up (any mRS improvement: 27.8% (n = 25) vs 14.9% (n = 39), p = 0.010, Figure 2(b)).
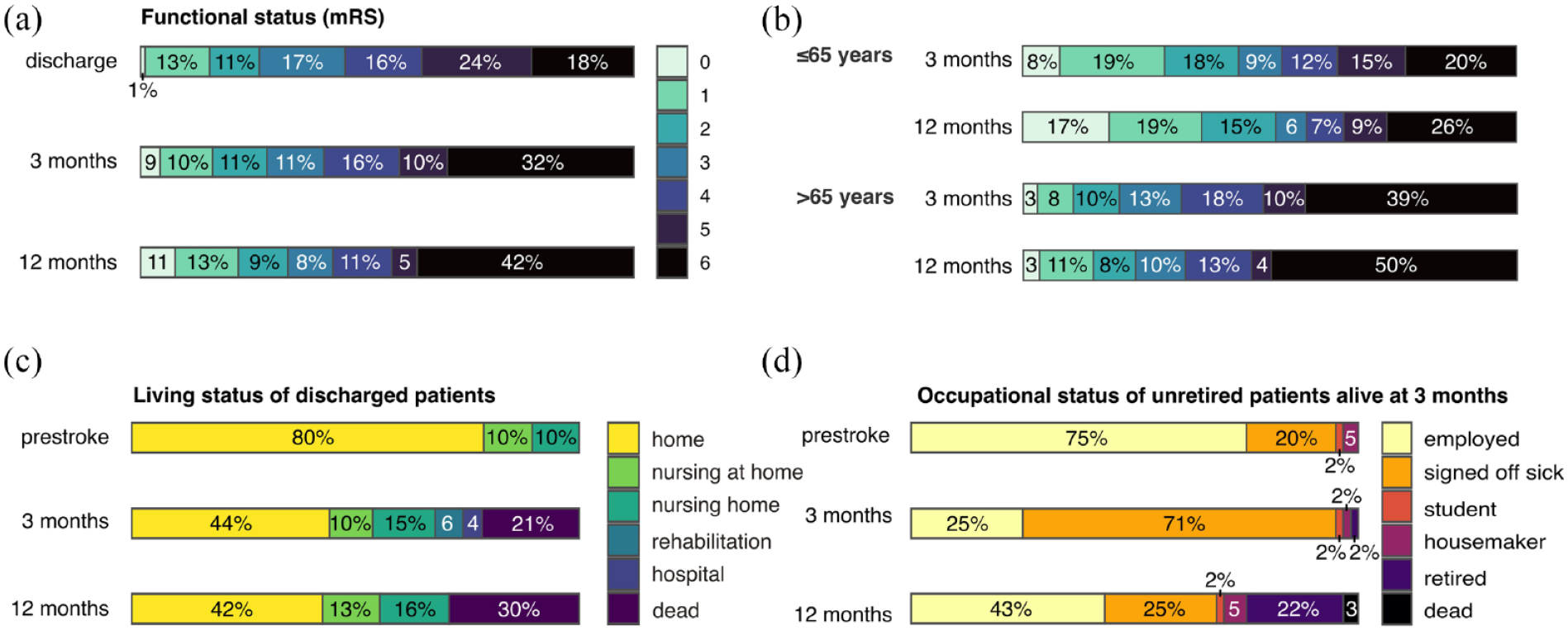
(a) Functional status at discharge, 3-month and 12-month follow-up as measured by the modified Rankin Score (mRS). (b) Functional status at discharge, according to patient age. (c) Living status before the index stroke and at follow-up. (d) Occupational status of surviving and previously unretired patients before the index stroke and at follow-up.
Return to home
Among patients discharged alive, 53.3% (n = 139) were living at home at 3-month follow-up, most without the need for nursing care (43.3% vs 9.6%). At 12-month follow-up, the number of patients living at home was similar with 54.8% (n = 143), 42.1% (n = 110) without and 12.6% (n = 33) with nursing care at home, respectively (Figure 2(c)).
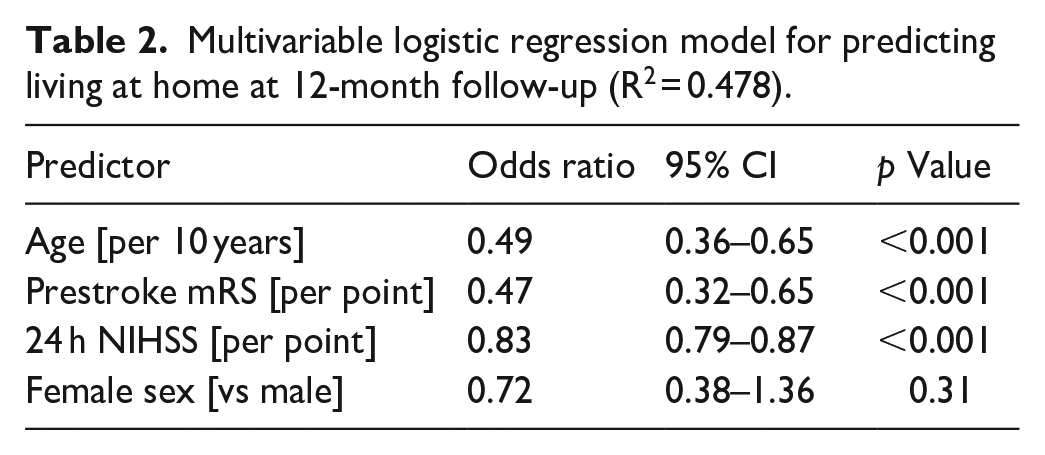
Based on the observation that women may have worse outcomes after EVT, 13 we hypothesized that living at home at 12-month follow-up differed between sexes. Indeed, women were less likely to live at home at 12 months than were men (31.0% vs 43.7%, p = 0.015). However, in multivariable analysis adjusting for prestroke mRS, age, and stroke severity after 24 h, sex was not predictive of living at home (Table 2). Stratifying patients by age quartile illustrates the impact of age on living status at 12-month follow-up, decreasing from 59% (n = 49) in patients aged < 65 years to 15.8% (n = 10) in patients aged 83 or older (Figure 3(a)), and the impact of NIHSS after 24 h on 12-month living status (Figure 3(b)).
Multivariable logistic regression model for predicting living at home at 12-month follow-up (R2 = 0.478).
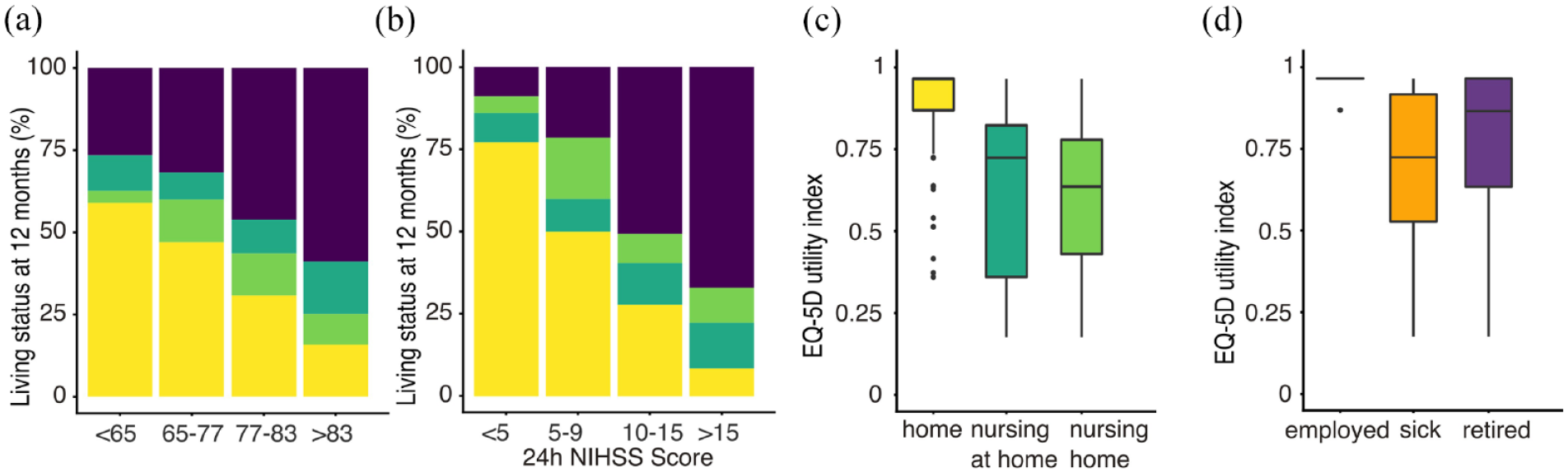
(a and b) Living status at 12-month follow-up according to age group and stroke severity as measured by the NIHSS after 24 h. (c and d) Quality of life as measured by the EQ-5D utility index, according to living status and occupational status at 12-month follow-up.
Return to work
Among patients discharged alive, 78.8% (n = 145) had already retired before the index stroke. Considering previously employed patients alive at 3-month follow-up, 70.6% (n = 47) were signed off sick at 3-month follow-up, and only 25.0% (n = 17) were able to return to work. At 12-month follow-up, return to work increased to 43.3% (n = 26), while 26.7.6% (n = 16) had retired or become a housewife or househusband. Excluding patients who were signed off sick already at baseline, workforce reintegration increased to 32.7% (n = 17) at 3-month and to 53.3% (n = 25) at 12-month follow-up. Among patients signed off sick at 3-month, 44.8% (n = 13) returned to work by 12-month follow-up. The longitudinal course of the patients’ occupational status is shown in Figure 2(d). In univariable logistic regression, age (OR 0.87, 95%CI 0.78–0.95) and stroke severity after 24 h (OR 0.82, 95%CI 0.66–0.95) were predictors of workforce reintegration.
Quality of life
Finally, we assessed the association of home and workforce reintegration with patient-reported quality of life at 12-month follow-up. The median 12-month EQ-5D utility index was 0.47 (IQR 0–0.96) in the entire study population and 0.87 (IQR 0.72–0.96) in the subgroup of patients alive at follow-up. Considering living status at 12 months, the median EQ-5D utility index was higher in patients living independently at home (0.98, IQR 0.87–0.96) as compared to receiving nursing care at home (0.64, IQR 0.43–0.78, p < 0.001) or living in a nursing home (0.72, 0.36–0.82, p < 0.001, Figure 3(c)). Similarly, workforce reintegration was associated with a median EQ-5D utility index of 0.96 (IQR, 0.96–0.96), which was significantly higher than that of patients who were signed off sick (0.72, IQR 0.53–0.92, p < 0.001) or retired (0.87, 0.63–0.96, p < 0.001, Figure 3(d)).
Discussion
By investigating physical and functional outcomes of EVT in stroke patients, our study emphasizes the importance of home and workforce reintegration as key indicators of recovery quality. The findings of our study underscore the significance of evaluating outcomes beyond traditional measures such as the mRS, particularly focusing on home and workforce reintegration. While mRS provides insight into functional recovery, it does not capture the complexities of stroke survivors’ lives post-treatment, including their ability to resume daily activities, return to work, and maintain independence in living at home. By leveraging a large monocentric prospective cohort of acute stroke patients receiving EVT, we show that home reintegration without nursing care occurs in only 42.1% of patients. While individual trajectories vary, the proportion of patients living independently at home was similar to 3-month follow-up and was predicted by stroke severity, age, and prestroke mRS. In contrast, workforce reintegration increased over time, illustrating the rehabilitation potential of working-age patients with stroke. Both home and workforce reintegration were associated with significantly higher HRQoL, emphasizing the importance of these outcome measures for patients.
Living independently at home is one of the most important outcome priorities for stroke patients. 8 Age, but not sex, significantly modified the perspective of patients to achieve this goal, which is in line with a recent healthcare data analysis. 14 Furthermore, the severity of neurological deficits as assessed by NIHSS after 24 h was an important predictor of home reintegration at 12 months. Accordingly, ongoing efforts to improve outcomes in acute stroke treatment clearly align with patients’ priorities. 15
Return to work was notably higher at 12-month as compared to 3-month follow-up. A previous GSR-ET analysis based on 3-month follow-up data reported return to work in 35.6% of previously employed working-age patients, while >90% of the remaining patients were still signed off sick. 9 Our data extend these findings to 1 year after EVT, when almost half of these patients were also able to return to work. The finding of successful return to work in 53% of previously employed patients is in line with a meta-analysis reporting workforce reintegration in 53% of unselected stroke patients often with lower severity stroke and mostly before establishing EVT as standard-of-care. 16 Considering that EVT is performed only in large-vessel occlusion stroke, that is, in the most severely affected subgroup of stroke patients, which are now able to achieve comparable outcomes, this high number again underlines the beneficial impact of EVT on patient outcomes.
This study also has limitations, including the monocentric nature of the cohort and the absence of further socioeconomic and psychosocial variables.17,18 Reintegration is not solely determined by physical recovery but is also significantly influenced by socioeconomic status, psychological well-being, and social support networks. Research suggests that patients with stronger social support systems exhibit better recovery trajectories, underscoring the role of family, community engagement, and social services in facilitating reintegration. 19 Moreover, psychological resilience and mental health, including the prevalence of post-stroke depression and anxiety, critically affect patients’ ability to reintegrate, suggesting a multidisciplinary approach to post-stroke care that includes mental health and social services.20,21
Future approaches may consider comprehensive datasets and multidimensional assessments to capture the complex trajectories of reintegration outcomes and its influencing factors. Additionally, longitudinal studies over extended periods could provide deeper insight into post-EVT workforce reintegration trajectories beyond the first year.
Conclusions
Long-term home and workforce reintegration represent patient-oriented outcomes achieved in 40%–50% of stroke patients treated with EVT. Lower neurological deficits and younger age are important predictors of successful reintegration.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241282875 – Supplemental material for Home and workforce reintegration one year after thrombectomy in acute stroke patients
Supplemental material, sj-docx-1-eso-10.1177_23969873241282875 for Home and workforce reintegration one year after thrombectomy in acute stroke patients by Felix J Bode, Nina A Zadon, Hannah Asperger, Niklas M Beckonert, Taraneh Ebrahimi, Louisa Nitsch, Julia Nordsiek, Julius N Meissner, Omid Shirvani, Sebastian Stösser, Christian Thielscher, Franziska Dorn, Nils C Lehnen, Gabor C Petzold and Johannes M Weller in European Stroke Journal
Footnotes
Acknowledgements
We acknowledge the contribution of all study nurses and extend our gratitude to the patients and their relatives for participating in the study.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FD Consultant for Microvention, Balt, Johnson&Johnson, received scientific grants from Johnson&Johnson; received speakers honoraria from Johnson&Johnson, Q’Apel, Tonbridge, Asahi, Acandis, Stryker, Microvention, Medtronic, Penumbra. FJB received speakers honoraria from AstraZeneca. NMB received travel grants from Sanofi and Viatris. All other authors report no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and was centrally approved by the institutional review board of the Ludwig-Maximilians University Munich (689-15) and institutional review boards according to local regulations.
Trial Registration: clinicaltrials.gov NCT03356392
Informed consent
Participants or their legal representatives gave informed consent as described in the initial study protocol.
Guarantor
FJB
Contributorship
FJB and JMW conceptualized and designed the study; NAZ acquired the data and JMW analyzed the data; FJB, NAZ and JMW wrote the first draft of the manuscript with input from all other authors. All authors approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.