
Abstract
Purpose:
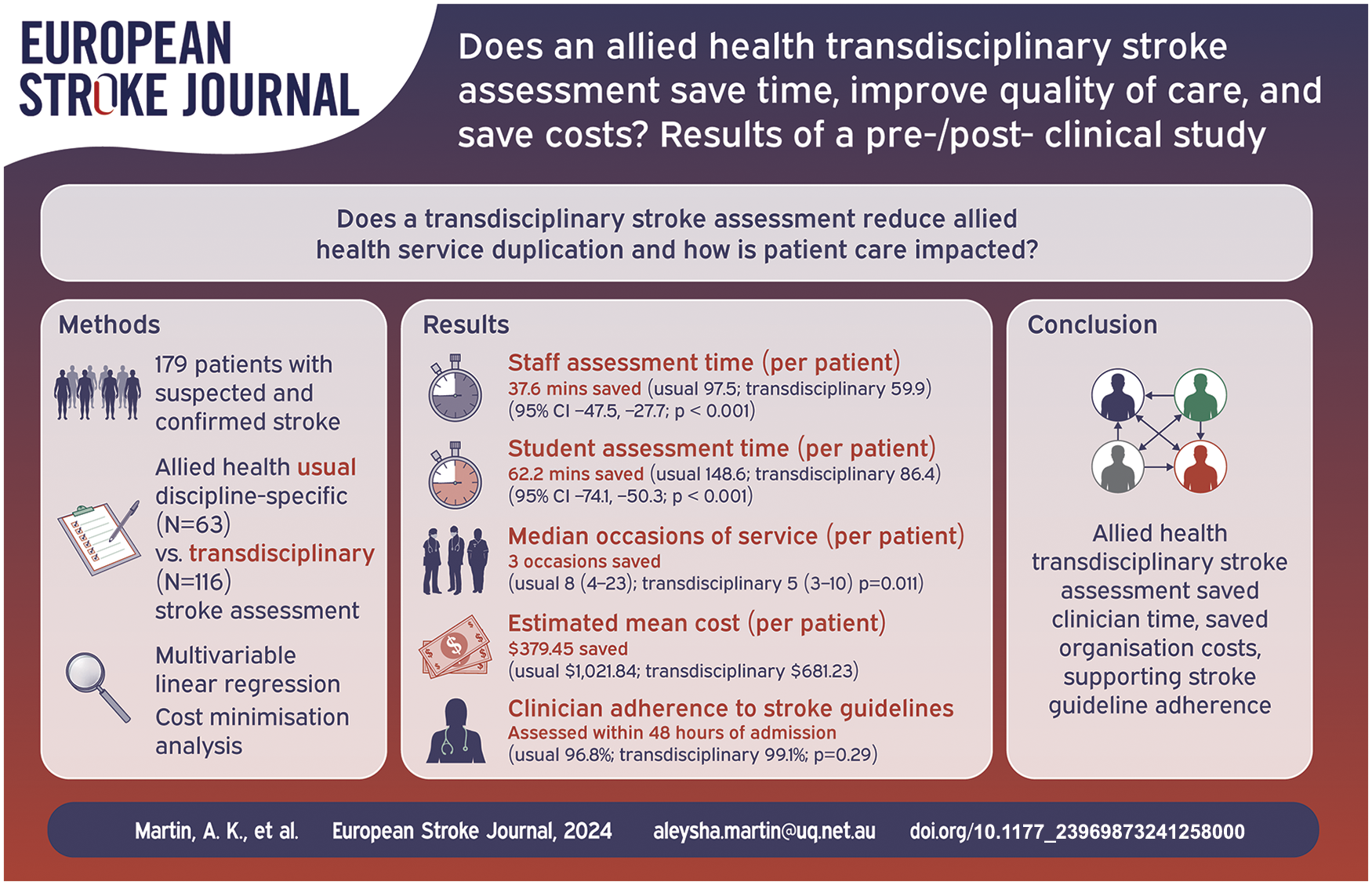
Demand for stroke services is increasing. To save time and costs, stroke care could be reorganised using a transdisciplinary assessment model embracing overlapping allied health professional skills. The study compares transdisciplinary assessment to discipline-specific allied health assessment on an acute stroke unit, by evaluating assessment time, quality of care, and cost implications.
Method:
The pre-/post- clinical study used non-randomised groups and 3-month follow-up after hospital admission. Patients with confirmed/suspected stroke received usual discipline-specific allied health assessment (pre-implementation phase) or the novel transdisciplinary assessment (post-implementation phase). Staff/student assessment times (primary outcome) and medical record data (secondary outcomes) were collected. Time differences were estimated using multivariable linear regression controlling for confounding factors. Cost minimisation and sensitivity analyses estimated change in hospital resource use.
Findings:
When the transdisciplinary assessment was used (N = 116), compared to usual assessment (N = 63), the average time saving was 37.6 min (95% CI −47.5, −27.7; p < 0.001) for staff and 62.2 min (95% CI −74.1, −50.3; p < 0.001) for students. The median number of allied health occasions of service reduced from 8 (interquartile range 4–23) to 5 (interquartile range 3–10; p = 0.011). There were no statistically significant or clinically important changes in patient safety, outcomes or stroke guideline adherence. Improved efficiency was associated with an estimated cost saving of $379.45 per patient (probabilistic 95% CI −487.15, −271.48).
Discussion and conclusion:
Transdisciplinary stroke assessment has potential for reorganising allied health services to save assessment time and reduce healthcare costs. The transdisciplinary stroke assessment could be considered for implementation in other stroke services.
Introduction
Sustainability of healthcare services, including stroke care, is a global priority. In 2022, the World Stroke Organisation reported 12.2 million new strokes occurred each year, and the number of people who experience a stroke in their lifetime has increased by 50% over the last 17 years. 1 As demand for stroke care increases, with concomitant costs rising, the way stroke services are provided must be reviewed and streamlined for efficiencies across teams.
Allied Health Professionals (AHPs) including physiotherapists, occupational therapists and speech pathologists constitute one team that delivers stroke services. Stroke guidelines recommend that AHPs complete assessment and mobilise patients within the first 48 h of hospital admission. 2 Questions and tasks are often duplicated between AHP assessments 3 due to overlapping clinical skills and knowledge4,5 and stroke care is delivered according to professional group agendas and regulations that constrain scopes of practice.6,7 To reduce duplication, AHPs could embrace their overlapping skills, and assessment could be reorganised and centred around the needs of people with stroke. To achieve this, a transdisciplinary model of assessment could be used.
Transdisciplinary models require AHPs to share skills and combine elements of their roles, allowing one clinician to complete a patient-centred occasion of service on behalf of the wider team. 8 The authors have defined transdisciplinary models elsewhere. 8 Theoretically, transdisciplinary models can be designed in many ways, however, there are few exemplars. A recent scoping review was the first synthesis of allied health hospital-based transdisciplinary models and identified nine unique models. 5 Collectively, the studies provided preliminary evidence that allied health transdisciplinary models could improve use of staff time, reduce adverse event numbers (such as patient falls), and reduce hospital re-presentations. 5 Two studies were based on Acute Stroke Units (ASUs) but did not report empirical evaluation methods or economic evaluations. 5 To our knowledge, no other examples of transdisciplinary models on ASUs have been published. We sought to demonstrate the value of ASU-based allied health transdisciplinary models and determine if transdisciplinary assessment is a feasible solution towards optimising allied health stroke services.
Aims and hypothesis
The aim was to evaluate time saved, quality of care (patient safety, patient outcomes, and AHP adherence to stroke guidelines), and cost implications when an allied health transdisciplinary assessment was utilised at the Mater Hospital Brisbane (MHB) ASU. We hypothesised that compared to usual discipline-specific allied health stroke assessment, a Transdisciplinary Initial Neurological Screening Assessment (TINSA) would reduce allied health assessment time by at least 20 min without reducing the quality of care.
Patients and methods
The study methods have been published elsewhere 3 and a summary follows.
Study design and setting
The single-centre study, based at an Australian ASU, used a pre-/post-implementation design with non-randomised groups and follow-up at 3 months after hospital admission. “Implementation” is defined as the date at which the TINSA was integrated into the care pathway of a patient cohort. Cross-sectional analytic measures were selected to compare and evaluate four phases of time between February 2021 to December 2022 (Figure 1). At first, only patients with TIA and mild stroke were included, to support the AHPs safely learning the new model of assessment. In Phase 1 (from February 2021), patients with TIA or mild stroke were assessed using usual assessment. Following a 1-month transition period (in August 2021), in which the TINSA was introduced and embedded into workflows, patients with TIA or mild stroke were assessed using the TINSA (Phase 2 from September 2021). After the TINSA was implemented, patients with moderate and severe stroke were included in the next two phases. Concomitantly with Phase 2, patients with moderate or severe stroke received usual assessment (Phase 3 until June 2022) before the TINSA was fully implemented (Phase 4 until December 2022). All participants were followed-up by telephone at 3 months after hospital admission (between May 2021 and March 2023).
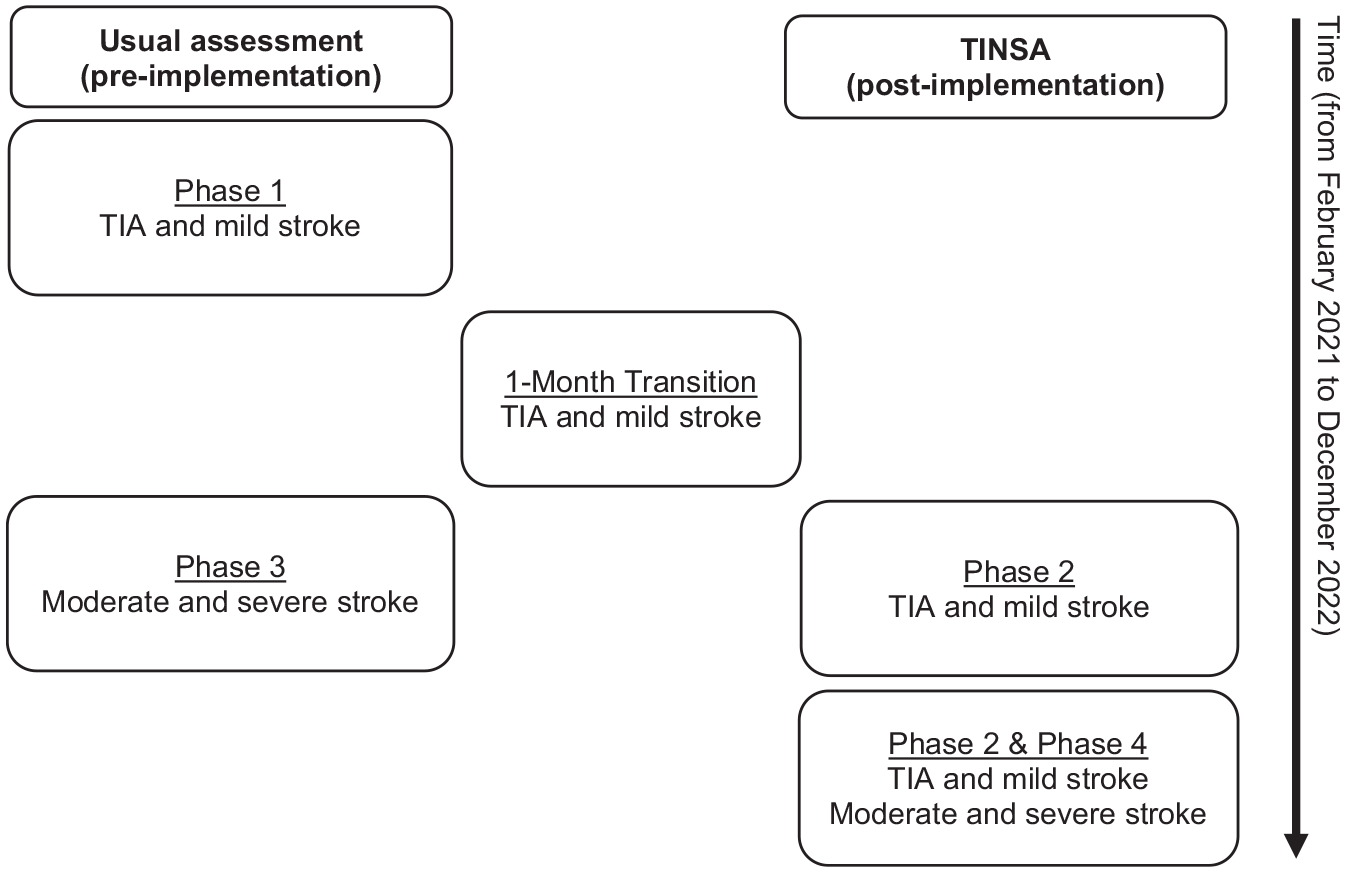
Pre-/post-study design with four phases.
Participants and recruitment
Participants with suspected (i.e. awaiting imaging results) or confirmed stroke were recruited and allocated to a study phase depending on severity of stroke symptoms and the month of admission to the ASU, as described above. Participants were excluded if admitted to the ASU outside of usual business hours or weekends/public holidays; and/or when allied health assessment was completed before ASU admission. Each patient could be included only once in the study.
Usual care
Usual assessments consisted of separate physiotherapy, occupational therapy and speech pathology assessments completed by staff and students.
Intervention
The TINSA, co-designed by the health professionals at the ASU, combined usual allied health assessments and was administered by a trained physiotherapist or occupational therapist (staff or student). The TINSA includes tasks/questions across domains of social situation, previous function, home environment, cognition, communication, swallowing, vision/perception, respiratory function, upper and lower limbs, functional mobility, and mood. A published copy is available online. 3 TINSA results were documented in the medical record, and no other changes were made to patient care.
Outcome measures
The primary outcome was length of assessment time. AHP staff and students timed their independent assessments including reading the medical record, administering the assessments, and documenting results. Students were expected to take longer than staff to complete the assessment. Other measures were collected via retrospective medical record audits including participant characteristics (e.g. gender, age, language, stroke type), measures of time (e.g. occasions of service, length of stay, number of AHPs involved) and measures of care quality (e.g. patient falls, hospital readmission, missed referrals, relevant national stroke guidelines, discharge destination). Patient outcomes were assessed at 3 months after hospital admission using the EQ-5D-3L. A full list of outcome measures is published elsewhere. 3
Analysis
Data from pre-implementation Phases 1 and 3 (usual assessment) were combined and data from post-implementation Phases 2 and 4 (TINSA) were combined to evaluate differences between assessment methods across all stroke presentations (mild, moderate and severe). Data from the transition phase were excluded from the analysis due to possible learning effects. Group characteristics were described using number (%) for categorical data, mean (standard deviation) for approximately normally distributed continuous data and median (interquartile range) for non-normally distributed continuous data. Group differences were investigated using Pearson’s chi-squared test or Fisher’s exact test for categorical variables and the two-sample t-test or Mann-Whitney U test for continuous variables. For the primary outcome, assessment time differences between groups were estimated using multivariable linear regression. An interaction term was used to investigate suspected differences between staff and students (effect modification). Other variables (such as primary language, cognition, stroke type, stroke severity, and if the full assessment was completed) were considered for the model based on clinical knowledge of what could influence assessment time, tested individually, included in a preliminary model if p ⩽ 0.30, and then sequentially removed from highest to lowest p-value. All significant (p < 0.05) or confounding variables were retained in the final model. The assumptions of normality of residuals, constant variance and independence were checked, and a sensitivity analysis determined influence of potential outliers. Stata 15.1 (Stata Corp, College Station, TX) was used for statistical analysis.
The cost minimisation analysis estimated the change in the cost of completing a stroke assessment from the perspective of the health sector after supporting the claim of equivalent assessment effectiveness and patient safety results (i.e. no statistically significant or clinically important differences between groups for patient safety or patient outcomes). 9 All variables with statistically significant differences representing the use of hospital resources were included in the determination of cost-savings resulting from the adoption of TINSA. We assumed the ASU was serviced by six transdisciplinary clinicians (two senior physiotherapists and one senior occupational therapist at MHB HP4.2 wage rate of $61.2532/hour with 3.3 years average job tenure; two junior physiotherapists and one junior occupational therapist at MHB HP3.4 wage rate of $47.6349/hour (rotating 6-monthly); salary oncost rate of 30%; 201 stroke admissions per year 10 ; once-off transdisciplinary training; and that completing usual assessment accounted for three of the total occasions of service (i.e. three separate allied health assessments) and the TINSA accounted for one of the total occasions of service. Total cost of assessment, training, and occasions of service were calculated by multiplying the assessment time, training time and the number of occasions of service by the hourly wage rate.
A one-way deterministic sensitivity analysis was used to determine the key drivers of the cost outcome. Inputs were varied to represent: the most/least number of stroke admissions over the last 5 years, only senior AHPs administering the TINSA, students completing the TINSA under supervision of a HP3.4 or HP4.2 clinician, and annual transdisciplinary training. Assessment time and occasions of service were varied using 95% confidence intervals to probabilistically determine the 95% confidence interval for the cost-saving. Reduced length of stay was explored as an additional scenario.
Results
Participant characteristics
A total of 63 participants were recruited into the pre-implementation usual assessment group and 116 participants were recruited into the post-implementation TINSA group (Table 1). Participant characteristics across groups were similar, except there were less haemorrhagic stroke presentations in the TINSA group (0%) compared to the usual assessment group (6%; p = 0.020).
Participant characteristics.
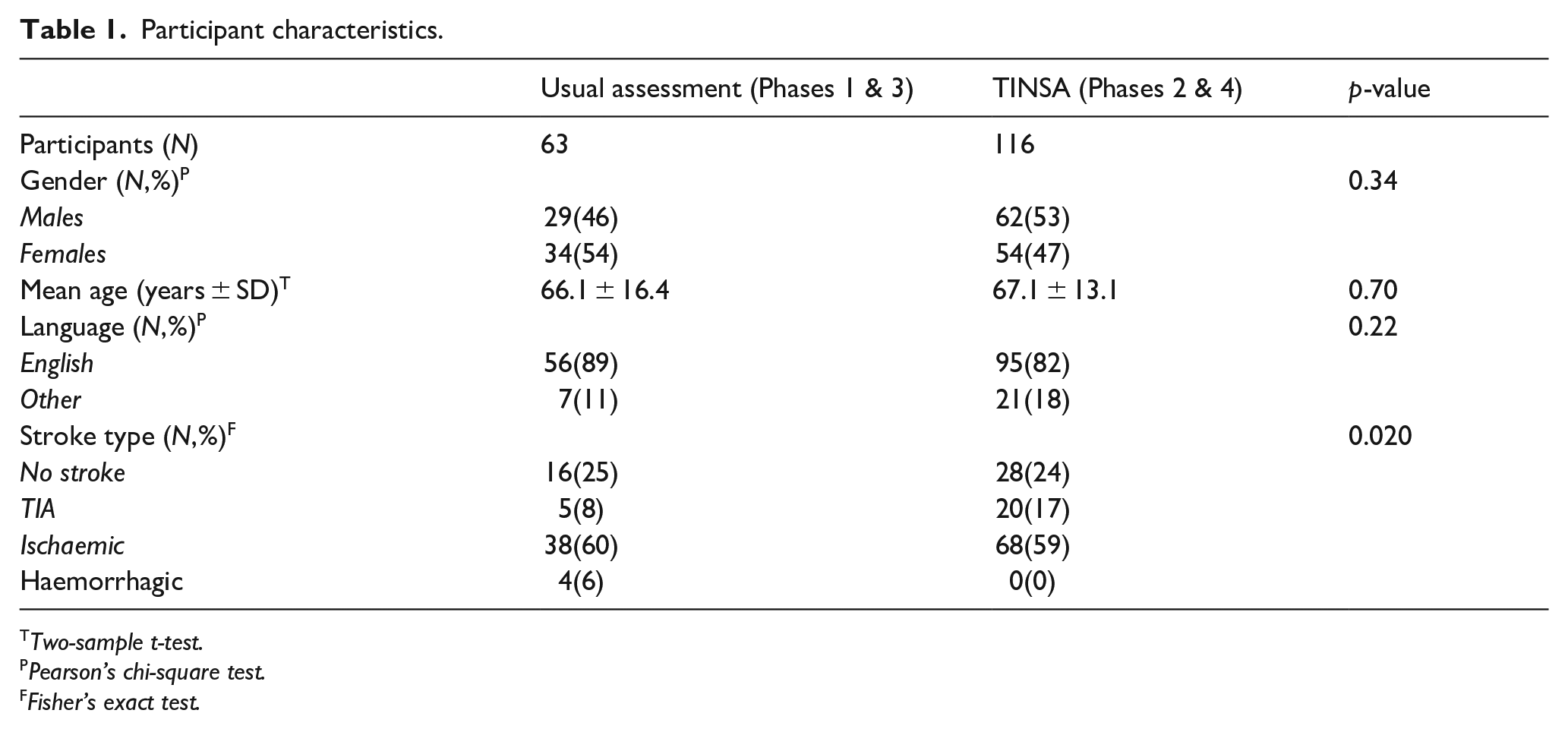
Two-sample t-test.
Pearson’s chi-square test.
Fisher’s exact test.
Primary outcome: Assessment time
The final multivariable model for assessment time included assessor (staff/student), patient sex and age. An interaction term between staff/student and pre-/post- was statistically significant (p = 0.002) indicating that the effect of the TINSA was different for staff and students. On average, staff completed the TINSA in 59.9 min, which was 37.6 min faster (95% CI −47.5, −27.7; p < 0.001) than usual assessment (97.5 min) (Table 2). On average, students completed the TINSA in 86.4 min, which was 62.2 min faster (95% CI −74.1, −50.3; p < 0.001) than usual assessment (148.6 min). On average, assessment took 7.3 min longer (95% CI 0.9, 13.7; p = 0.026) for female patients compared to males and 0.2 min longer (95% CI 0.05, 0.43; p = 0.012) for every year increase in age. While there were fewer haemorrhagic stroke presentations (0% compared to 6%) and more TIA presentations (17% compared to 8%; p = 0.020) in the TINSA group, stroke type was not a significant or confounding variable when tested in the regression model. That is, we found that assessment time differences were similar whether stroke type was adjusted for or not. Linear regression assumptions of normality of residuals, independence and constant variance were met. Potential outliers were investigated and shown not to be influential.
Multiple linear regression model for assessment time.
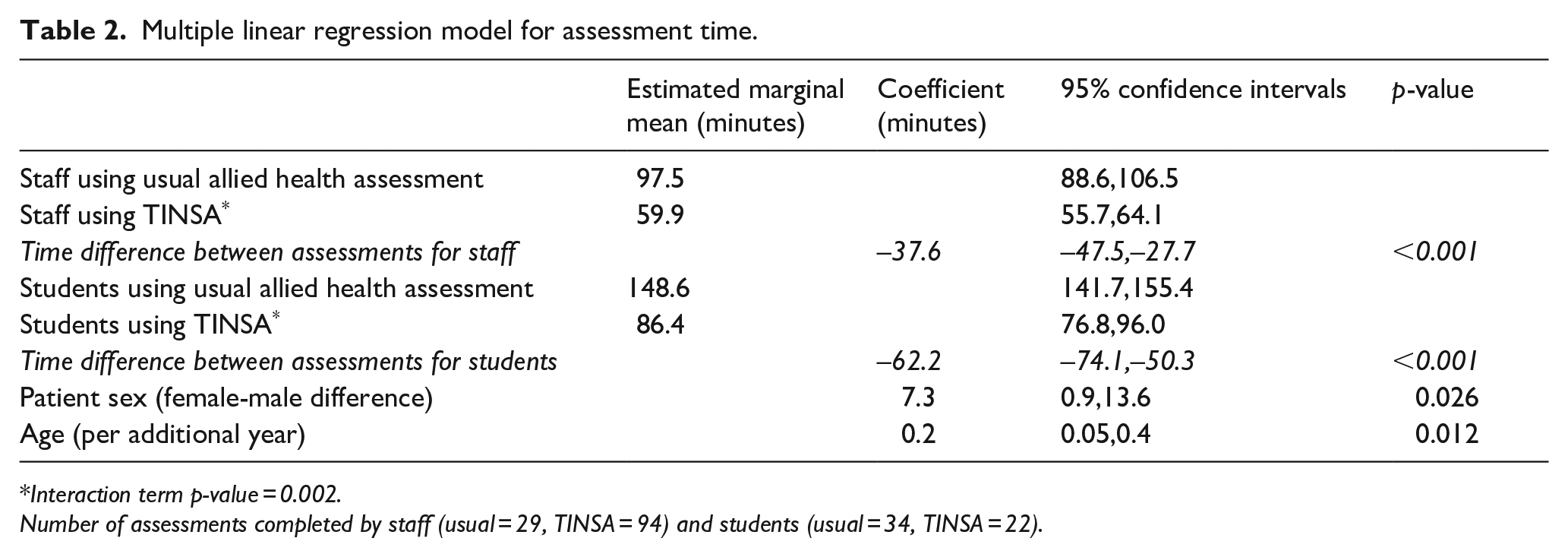
Interaction term p-value = 0.002.
Number of assessments completed by staff (usual = 29, TINSA = 94) and students (usual = 34, TINSA = 22).
Time savings and AHP involvement
The median number of occasions of service by AHPs was lower in the TINSA group (5, IQR: 3–10 per admission) compared to the usual assessment group (8, IQR: 4–23; p = 0.011) (Table 3). Overall, when the TINSA was used there were fewer AHPs involved (p = 0.001), most significantly for occupational therapists and physiotherapists who were involved in 100% of usual assessments, but 84.5% (p < 0.001) and 87.1% (p = 0.003) of TINSAs, respectively. The median number of occasions where no further AHP input was required after initial assessment decreased from 1 (0–2) when usual assessment was used to 0 (0-0) when the TINSA was used (p < 0.001).
Secondary outcomes related to time and allied health professional involvement.
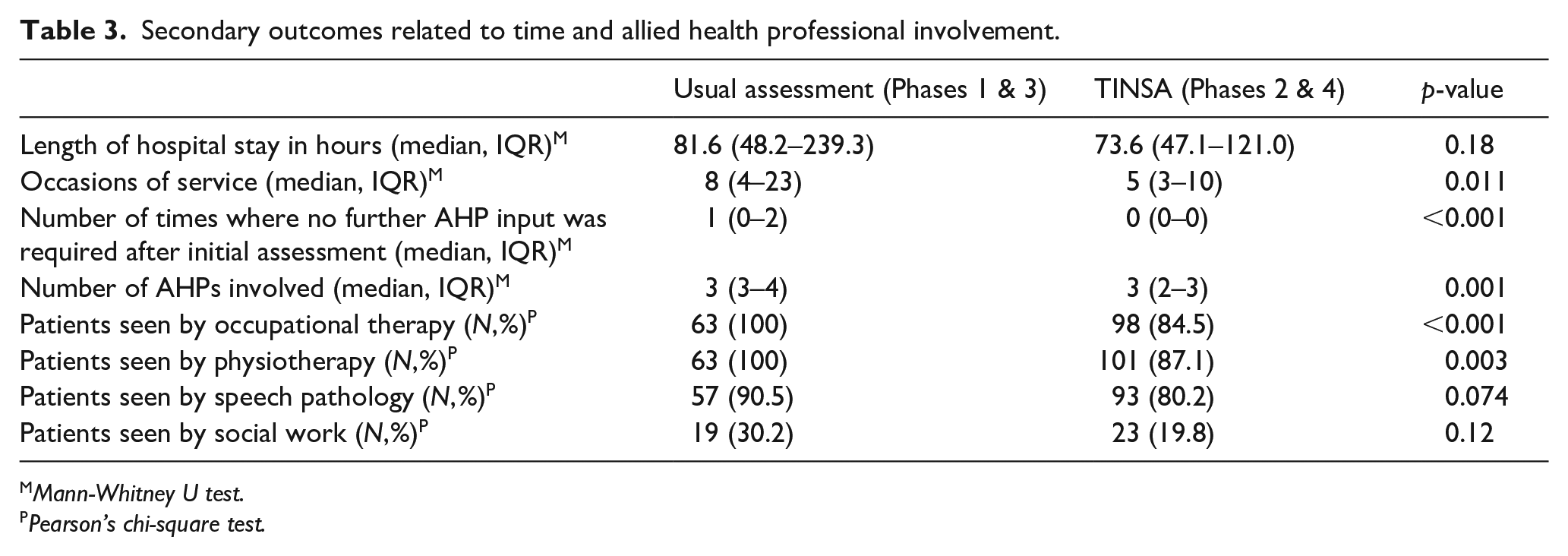
Mann-Whitney U test.
Pearson’s chi-square test.
Quality of care (guideline adherence, patient safety and outcomes)
The number of missed allied health referrals (i.e. when a referral is documented but not actioned) was no different for usual assessment (N = 5, 7.9%) compared to the TINSA (N = 16, 13.8%; p = 0.24) (Table 4). There was no statistically or clinically significant change in other measures of care quality when the TINSA was used, including patient falls and unplanned re-admissions (Table 4). Adherence to key stroke guidelines was the same or better when the TINSA was used, such as the number of patients who received the mobility assessment within 48 h of admission (92.1%–99.1%; p = 0.021). The discharge destination was unaffected by assessment method (p = 0.61).
Secondary outcomes related to quality of care.
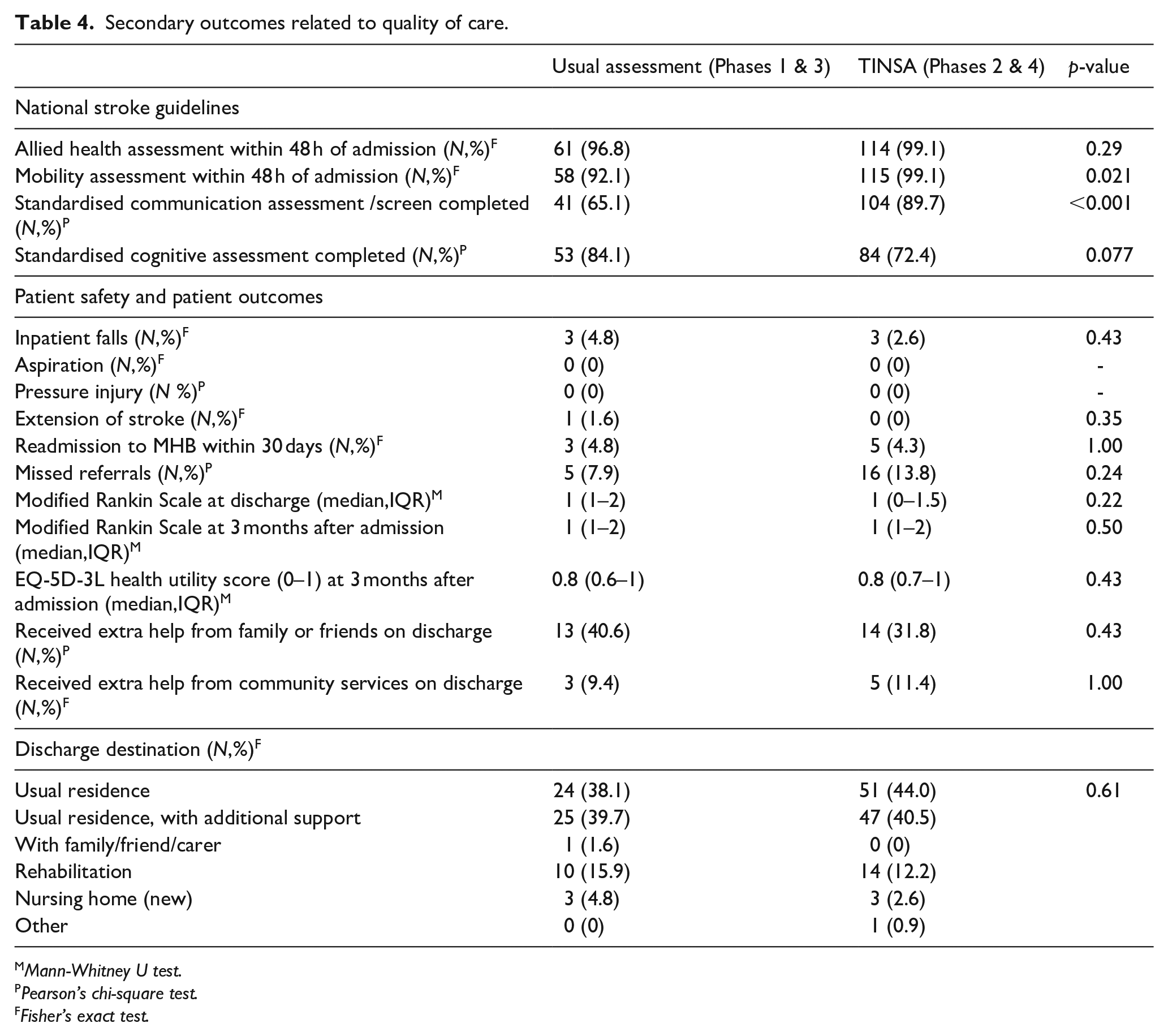
Mann-Whitney U test.
Pearson’s chi-square test.
Fisher’s exact test.
Cost implications
The base case mean cost saving was $379.45 per patient (probabilistic 95% CI −487.15, −271.48), totalling an annual saving of $76,268.82 for the 7-bed ASU (Table 5). The change in specific cost components (i.e. assessment time, training time, occasions of service, wage rate, number of junior/senior clinicians) is detailed in Table 5. For each sensitivity analysis scenario, using the TINSA was still found to be less costly compared to usual assessment in the base case (Table 6). Cost savings were marginally smaller when training was completed six monthly ($5.05 less) and when students used the TINSA under the supervision of a junior AHP ($38.03 less) or senior AHP ($79.61 less). Cost savings were greater when only senior AHPs were involved ($31.71–$62.83 more).
Cost minimisation analysis (2022/23 AUD prices).
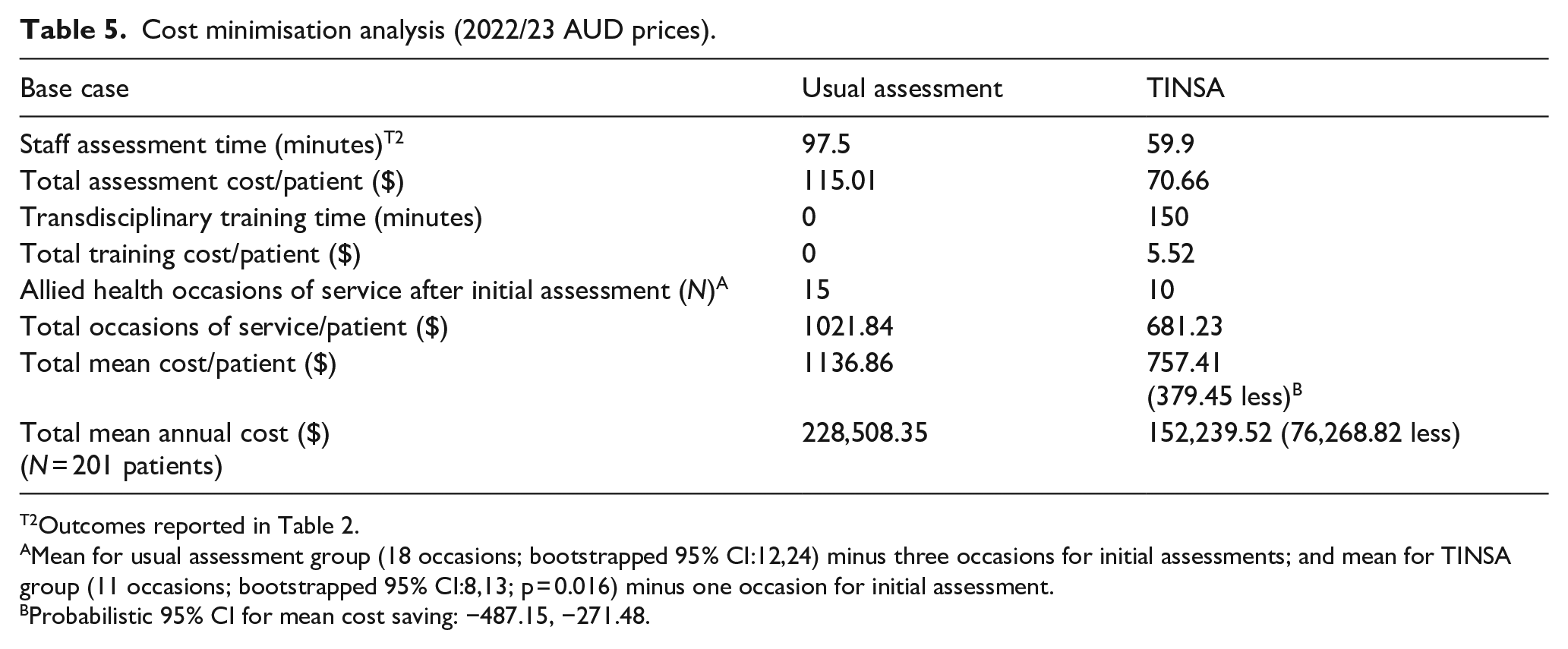
Outcomes reported in Table 2.
Mean for usual assessment group (18 occasions; bootstrapped 95% CI:12,24) minus three occasions for initial assessments; and mean for TINSA group (11 occasions; bootstrapped 95% CI:8,13; p = 0.016) minus one occasion for initial assessment.
Probabilistic 95% CI for mean cost saving: −487.15, −271.48.
One-way sensitivity analysis (2022/23 AUD prices).
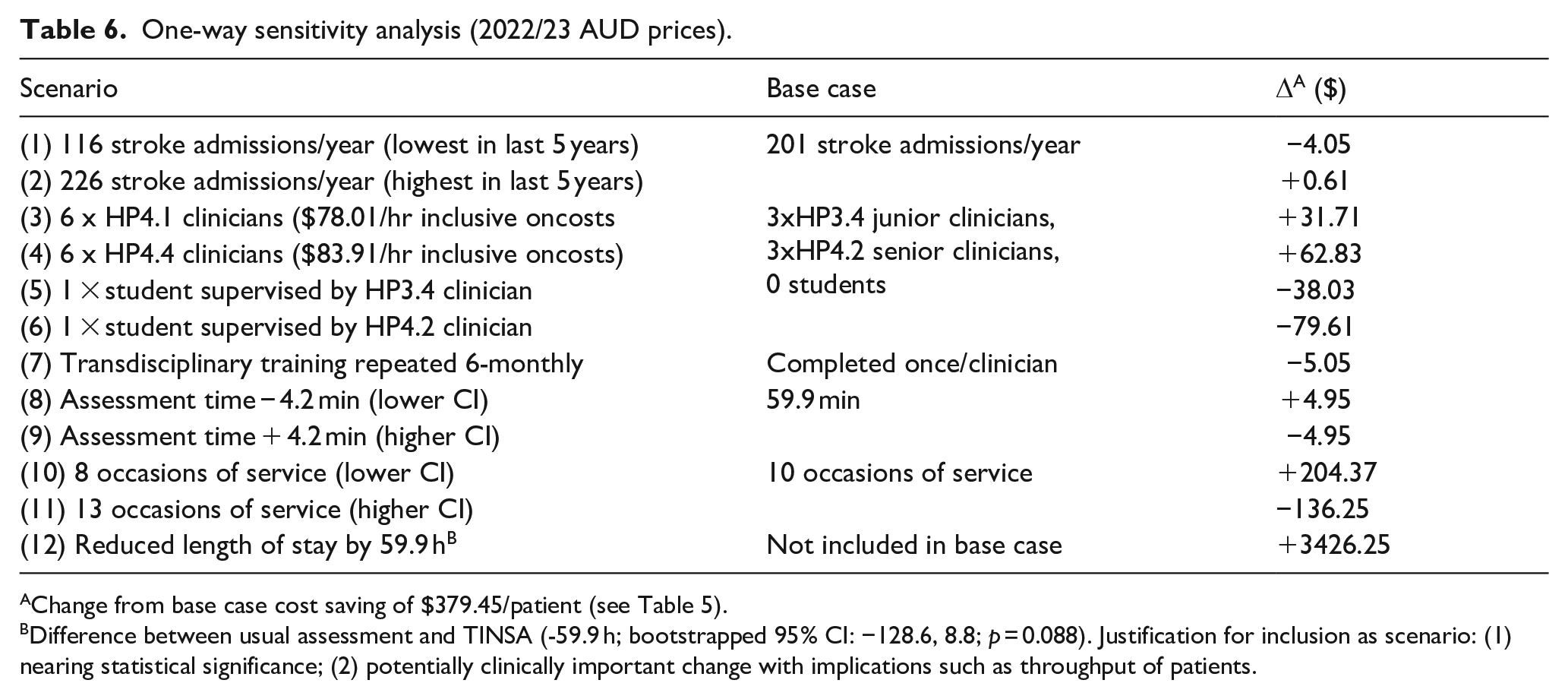
Change from base case cost saving of $379.45/patient (see Table 5).
Difference between usual assessment and TINSA (-59.9 h; bootstrapped 95% CI: −128.6, 8.8; p = 0.088). Justification for inclusion as scenario: (1) nearing statistical significance; (2) potentially clinically important change with implications such as throughput of patients.
Discussion
The primary hypothesis was confirmed. The results provide empirical evidence that a transdisciplinary assessment reduces assessment time, lessens costs and maintains care quality in an acute stroke unit.
Time savings and AHP involvement
Our study found that the TINSA saved a substantial amount of assessment time per patient for staff (37.6 min) and students (62.2 min). The result aligns with previous studies that found AHPs spent less time completing clinical tasks when a transdisciplinary model was used in hospital settings. 5 For example, Watterson et al. 6 found a significant mean time saving of 2.31 h in AHP time per patient (p < 0.001). There are important implications when time is saved. For patients with stroke, time saved could be redirected to starting therapy earlier within existing staff complement. Using a transdisciplinary stroke assessment as a strategy to fast-track rehabilitation has international relevance, for example, commencing rehabilitation within 48 h is recommended in Australia, the United Kingdom and Ireland.2,11
Role release is a key feature of transdisciplinary models. 8 When the TINSA was used, role release contributed to streamlined AHP stroke services and lessened workloads, demonstrated by reduced occasions of service provided by fewer AHPs. For example, when the TINSA was used, occupational therapists and physiotherapists were required to release the role of assessing every stroke patient. In addition, AHP stroke services were more purposeful as, when the TINSA was used, there were fewer occasions where no further AHP input was required after the initial assessment. That is, when using the TINSA patient rehabilitation and discharge needs were identified, and ensuing AHP referrals and input were more specific and targeted. Our findings could be a unique outcome for ASUs, as other studies in different settings (e.g. general medical wards) have found no difference in the number of AHPs involved in usual and transdisciplinary care.5,6,12
Quality of care
Quality healthcare involves providing the right services, while avoiding overservicing and underservicing. The balance is important to evaluate as there is an underservicing risk if a clinician completing transdisciplinary tasks lacks the clinical skills to identify and address patient needs. Our results demonstrated that using the TINSA streamlined AHP services (as discussed above), while the greater number of missed referrals (i.e. an indication of potential underservicing) was not statistically significant. As the study was not powered to evaluate underservicing as the primary outcome, missed referrals could be more likely when the TINSA was used and further evaluation is required. Alternatively, greater numbers of missed referrals could simply indicate an unexpected benefit of robust cross-checking, that is, sometimes AHP referrals were generated but not actioned once the referred practitioners reviewed TINSA results. This outcome may have occurred due to the referral prompts on the TINSA being too sensitive, or the referral reason was no longer valid (e.g. a cognitive assessment no longer being indicated when there was no evidence of stroke after imaging). Considering overservicing and underservicing together was a novel approach that has not been considered concurrently in other transdisciplinary studies.5,12
Across other measures (e.g. unplanned readmissions and inpatient falls) there were no statistically significant or clinically important differences between assessment methods. The results align with other studies where no statistically significant differences were found between groups for unplanned re-presentations to emergency departments or hospital.5,6,12 The results provide reassurance for AHPs working in transdisciplinary roles. For example, while mobilising a patient for the first-time after stroke is beyond usual occupational therapy scope of practice, our inpatient falls data suggest this was a safe practice.
Our study demonstrated excellent adherence with AHP-relevant stroke guidelines. While some results were limited due to ceiling effects, our results compare well to Australian Clinical Stroke Registry data. When the TINSA was used, 99.1% of study participants were mobilised and received transdisciplinary stroke assessment within 48 h of admission, which is above the national mean (65%, 79% respectively) and the achievable benchmark (80%, 92% respectively).10,13 When the TINSA was used, significantly more patients received standardised communication assessments or screens (89.7%, p < 0.001), which is likely due to the inclusion of a standardised communication screen in the TINSA often missed in routine practice. Concurrently, fewer standardised cognitive assessments were completed, although this result was not statistically significant (72.4%, p = 0.77) and is largely explained by the 24% of participants in the TINSA group being diagnosed with no stroke on imaging and so cognitive assessment was not clinically indicated. Excellent guideline adherence is an important outcome as integrating evidence-based guidelines into clinical practice is challenging. 14 The TINSA could be a useful tool to improve use of AHP resources and thereby AHP adherence to stroke guidelines in other ASUs.
Cost-savings implications
A significant cost saving was demonstrated when the TINSA replaced usual assessment. Only one other transdisciplinary cost analysis has been published, which was undertaken in a general medical ward and did not include a sensitivity analysis. 6 Watterson et al. 6 reported $112.66 was saved per patient in AHP costs (time savings multiplied by relevant senior wage), and $2877 was saved in length of hospital stay costs (per diem cost multiplied by length of stay). Our AHP cost saving per patient considered more variables, was larger than $112.66, and increased compared to the base case when the more expensive senior wage rate (HP4.1–4.4) was applied. Our results could support transdisciplinary roles being funded at senior wage rates, to acknowledge the complex clinical skills required. We also explored the reduced length of stay as an additional scenario due to potentially important clinical implications. For example, early hospital discharge could avoid hospital-acquired complications of infection and falls, and provide earlier access to care for another patient.
Limitations
The pre-/post- study design was selected for pragmatic reasons. Stakeholder consultation showed staff preferred using one type of assessment at a time, to avoid adverse outcomes such as delayed assessment or implementation resistance stemming from confusion regarding which assessment to use for which patient. While a Randomised Controlled Trial would have been preferable from an evidence quality perspective, we attempted to control for group differences by adjusting for the most important potential differences. For example, there were fewer haemorrhagic stroke presentations and more TIA presentations in the TINSA group than in the usual care group. While adjustment for stroke type did not substantially change the estimated assessment time difference between TINSA and usual care, it is possible that these differences could have led to an overestimation of the time difference between TINSA and usual care. Second, while instruction and training were provided to staff, self-timed assessments could be inaccurate if the AHP neglected to record the information in real time. However, any timing inaccuracies were expected to be similar during usual assessment and TINSA study phases. Finally, statistical analysis and generalisability of results were restricted by participant numbers. For example, subgroup analyses to investigate assessment group differences by stroke severity were not completed due to the small number of patients presenting with moderate/severe stroke during the study period. The Queensland Ambulance Service guidelines direct all patients presenting with moderate to severe stroke symptoms to a hospital with clot retrieval infrastructure (i.e. not the study site). 15
Conclusion
The study represents the first empirical evaluation of an allied health transdisciplinary stroke assessment implemented in an ASU. The results confirm the TINSA as a time saving, effective and safe assessment method that has potential to support AHP adherence with stroke guidelines and reduce organisational healthcare costs. The TINSA is an effective tool that could help AHPs provide affordable, sustainable and high-quality stroke services as more people in an ageing population are expected to experience stroke in the future.
Implications for clinical practice
AHPs, healthcare managers and leaders and policymakers could consider implementing the TINSA (or similar transdisciplinary tool) in their stroke service. The TINSA could be implemented within existing staffing arrangements to achieve the benefits presented. The TINSA is suitable to use with patients with any stroke presentation, although more research is indicated for patients with moderate to severe stroke. The TINSA could be used in healthcare services for streamlining AHP services to free-up staff time and occasions of service, which could be redirected to providing important healthcare to more/other patients.
Implications for research
Further empirical research in other settings, including other acute stroke units, is needed to confirm the study results. Future evaluations could replicate the methods used in this study and utilise the comprehensive list of outcome measures. While beyond the scope of our study, other evaluations could also measure how AHP time saved is re-directed to other occasions of patient care. Future studies should focus on recruiting larger numbers of patients experiencing moderate to severe stroke symptoms to confirm the results of this study. Additional cost analyses should be conducted to better understand and compare potential cost savings across hospitals and health services. Assessment time for junior and senior staff (in addition to students) could be estimated to improve the accuracy of the cost estimates.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241258000 – Supplemental material for Does an allied health transdisciplinary stroke assessment save time, improve quality of care, and save costs? Results of a pre-/post- clinical study
Supplemental material, sj-docx-1-eso-10.1177_23969873241258000 for Does an allied health transdisciplinary stroke assessment save time, improve quality of care, and save costs? Results of a pre-/post- clinical study by Aleysha K Martin, Alison Griffin, Alexandra L McCarthy, Theresa L Green, P Marcin Sowa and E-Liisa Laakso in European Stroke Journal
Footnotes
Acknowledgements
This work was undertaken as part of AKM’s Doctor of Philosophy enrolment at Faculty of Medicine, The University of Queensland. The authors acknowledge the acute stroke team at Mater Hospital Brisbane (Beth Houghton, Julia Matthews, Lucy Lyons, Jody Ebenezer, Georgia Gray, Marie McCaig, Ashley McGuire, Brendon Glenn) and Active Rehabilitation Physiotherapy (Caitlin Humphreys, Karl Harm, Simon Freestone, Martin Leet) who collaborated to co-produce and/or implement the transdisciplinary assessment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AKM received external peer-reviewed funding for this work from National Health and Medical Research Council under Postgraduate Scholarship [2005351, Oct 2020-2023] and Queensland Health under Health Practitioner Research Scheme [AH002682, July 2021-June 2022]. AKM received internal funding for this work from Mater Foundation/Mater Research Institute under Betty McGrath Health Services Research Seeding Grant [2613, Jan 2021-Dec 2023] and The University of Queensland under Research Training Programme [3769499089, Oct 2020-June 2024]. The trial sponsor is Mater Misericordiae Ltd. The funders and sponsor had no role in study design, study execution, data collection, data analysis and interpretation, decision to submit results, or preparation of manuscript.
Informed consent
Informed written consent to participate in the study was obtained from all participants before taking part in study activities. Where written consent was not possible, verbal consent was obtained via phone call or written consent via mail.
Ethical approval
The study protocol was submitted to the Mater Misericordiae Ltd HREC (HREC/MML/66933, approved 4 November 2020) and RGO (MSSA/MRGO/66933, approved 14 February 2021).
Guarantor
AKM
Contributorship
AKM: funding acquisition, conceptualisation of study, preparing study methods and design, data collection/analysis, primary contributor to manuscript writing, reviewing, and editing. E-LL, PMS, AG, TLG, and ALM: study methods design, and manuscript reviewing and editing. PMS and AG: data analysis. Final manuscript approved by all authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.