
Abstract
Introduction:
There is uncertainty whether patients with a cerebral cavernous malformation (CCM) should undergo conservative or surgical treatment, resulting in practice variation among hospitals. Our objective was to report clinical outcomes of patients with primarily conservatively managed CCMs.
Patients and methods:
This single-center cohort study included consecutive adult CCM patients, diagnosed in 2000–2023, who underwent conservative management as primary treatment strategy. Data were extracted from medical records, and we systematically conducted telephone and questionnaire follow-up. Functional status was assessed on the modified Rankin Scale (mRS).
Results:
Of 345 patients, we included 265 patients with a CCM (median age 46 years; 45% male). At baseline, 131 (49%) patients presented with symptomatic hemorrhage (SH), and 134 (51%) with other symptoms or asymptomatically. During 58 months (IQR 35–94) median follow-up, 51 (19%) patients experienced a SH, 33 (12%) a seizure, and 13 (5%) focal neurological deficits. Fourteen (5%) patients underwent intervention (surgery n = 11, radiosurgery n = 4). Presentation with SH was associated with higher annual bleeding rates (6.0% vs 1.5%, p < 0.001), and higher cumulative 5-/10-year bleeding risks (31%/41% vs 7%, p < 0.001). Brainstem CCM was associated with higher cumulative 5-/10-year bleeding risks (27%/38% vs 17%/21%, p = 0.038). Nineteen (7%) patients died; two (0.8%) directly attributable to CCM. Of 246 surviving patients, 205 (83%) completed the questionnaire. At follow-up, 172/224 (77%) patients were functionally independent (mRS score ⩽2).
Discussion and conclusion:
The majority of conservatively managed CCM patients remained free of a SH during follow-up. Few patients required intervention, and death attributable to the CCM was rare. These data may help patient counseling and treatment decisions.

Keywords
Introduction
Cerebral cavernous malformations (CCMs) are intracranial vascular malformations that may cause hemorrhage, seizures and focal neurological deficits (FNDs). 1 CCMs have an estimated prevalence of 0.5%, 2 and can occur solitary or as multiple lesions, as well as in coexistence with a developmental venous anomaly (DVA). 3 The majority of CCMs are sporadic, while around 20% of the cases are familial. 4 Due to widespread availability of MRI, detection rates of CCMs are rising, 5 and CCMs are increasingly detected incidentally. 6
Treatment strategies of CCMs include surgery, radiotherapy and conservative management. The optimal treatment approach remains unknown, resulting in considerable practice variation. 7 At our institute, we employ conservative management as the primary treatment strategy for patients with a CCM. Some guidelines, however, recommend surgery for accessible symptomatic CCMs and solitary asymptomatic CCMs, unless the risk of the intervention is deemed exceptionally high. 6 On the other hand, some studies demonstrate that surgery is associated with worse outcomes, advocating that the primary approach should be conservative, even for patients who present with hemorrhage.8,9
There is a paucity of studies that examine the outcomes of a relatively unselected cohort of patients with a CCM who were managed conservatively. The predominantly conservative approach at our institute provides the opportunity to evaluate this treatment strategy and gain insight into the natural history of CCMs. As such, the objective of this study was to systematically analyze the outcomes of patients with primarily conservatively managed CCMs.
Methods
Design and patient selection
This was a retrospective observational single-center cohort study. We consecutively included patients with a CCM, diagnosed at our hospital between January 2000 and May 2023, and who were managed conservatively as the primary treatment strategy. We excluded patients who primarily underwent surgery or radiotherapy after CCM diagnosis. Patients who underwent an intervention (surgery or radiotherapy) after an initial conservative strategy were included. We further excluded children (age < 18 years), spinal cavernous malformation (unless in combination with CCM), or patients with a follow-up duration of <6 months (unless within this time-interval the patient died due to their CCM).
Cases were extracted from our prospective neurovascular registry. In order to identify cases not captured in this registry, we additionally searched the hospital medical record system using International Classification of Diseases (ICD) 10 codes (i.e. Q28.2 and Q28.3). 10 Each diagnosis of CCM was confirmed on MRI by a certified neuroradiologist. The Institutional Review Board of the Amsterdam UMC exempted this study from formal approval due to its observational design (W22_196 # 22.244). For the reuse of clinical data, we carried out an opt-out procedure in 2023. All patients who completed the questionnaire provided written informed consent. This article is written in accordance with the STROBE guidelines for observational studies. 11
Data collection and outcomes
Baseline characteristics were extracted from the medical records and included demographics, mode of presentation, medications, and lesion characteristics. Lesion characteristics were location of the CCM, number of CCMs, size of the (largest) CCM on axial T2-weighted MRI sequences, and presence of any associated DVA. Cases were considered familial if confirmed by genetic testing, if the patient had a first-generation family member with a CCM, or if the patient had five or more CCMs which could not be explained by another cause (e.g. history of cranial radiation).
Outcomes of interest were: symptomatic hemorrhage (SH), seizures and FNDs during follow-up, interventions (surgery or radiotherapy), functional independence, and death. SH was defined as an acute or subacute onset of symptoms (headache, epileptic seizure, impaired consciousness, or new/worsened FNDs referable to the anatomic location of the CCM) accompanied by radiological, pathological, surgical, or cerebrospinal fluid evidence of recent extra- or intralesional hemorrhage, as stipulated in a previous study. 1 Seizures or FNDs were classified as such if a concomitant hemorrhage was absent on MRI sequences. Functional status was assessed on the modified Rankin Scale (mRS), which ranges from 0 (no symptoms) to 6 (death). 12 Functional independence was defined as mRS scores of ⩽2.
All data related to study outcomes, except for the mRS scores, were initially retrieved from the medical records, and subsequently verified during systematic telephone follow-up from March to May 2023 by the first author, inviting all patients to participate in a structured questionnaire (Supplemental Appendix 1). The mRS scores were exclusively determined using the questionnaire. In case of discrepancy between the medical records and questionnaire, we requested documentation from the referring hospital. The local hospital or general practitioner was also contacted if a patient did not complete the questionnaire, in case of missing data, or to obtain a cause of death.
Statistical analysis
Data are presented descriptively. In univariable analyses, we tested whether the variables age, sex, presentation with SH, medications, familial nature, multiple CCMs, brainstem CCM, CCM size, and associated DVA were associated with a SH during follow-up. The unpaired t-test was used for parametrical continuous data, the Mann–Whitney U-test for non-parametrical continuous data, and the Chi-squared test for categorical data. To test whether continuous data were normally distributed the Shapiro–Wilk test was used. The Bonferroni correction was used to account for multiple testing. In a multivariable logistic regression model we tested associations of the variables presentation with SH, brainstem CCM, CCM size, and age with functional independence at last follow-up.
We calculated annual bleeding rates per patient, in which censoring occurred after the first symptomatic hemorrhage during follow-up. We conducted Kaplan–Meier survival analyses to the first SH or seizure during follow-up, and determined cumulative risks at 5-year and 10-year time points. In addition to the analysis of SH during follow-up and functional independence in the full cohort, we also evaluated groups based on the mode of presentation (presentation with SH vs presentation with other or no symptoms) and location of the CCM (brainstem vs non-brainstem). Annual bleeding rates were compared using the Chi-squared test. 13 Survival analyses were compared using the log-rank test. Statistical analyses were done using IBM SPSS Statistics version 28, 14 and MedCalc Statistical Software version 22. 15
Results
We identified 345 patients with a cavernous malformation (Figure 1). Sixty-eight patients were excluded because of age <18 years (n = 27), opted-out/no consent (n = 12), exclusively spinal cavernous malformation (n = 15), or a follow-up duration of <6 months (n = 14). Two other patients with <6 months of follow-up were included because they suffered a fatal SH caused by a CCM. Of the remaining 277 patients, 12 (4%) patients were excluded because the primary treatment strategy was surgery (n = 11) or radiotherapy (n = 1). Details of these 12 patients are provided in Supplemental Appendix 2.
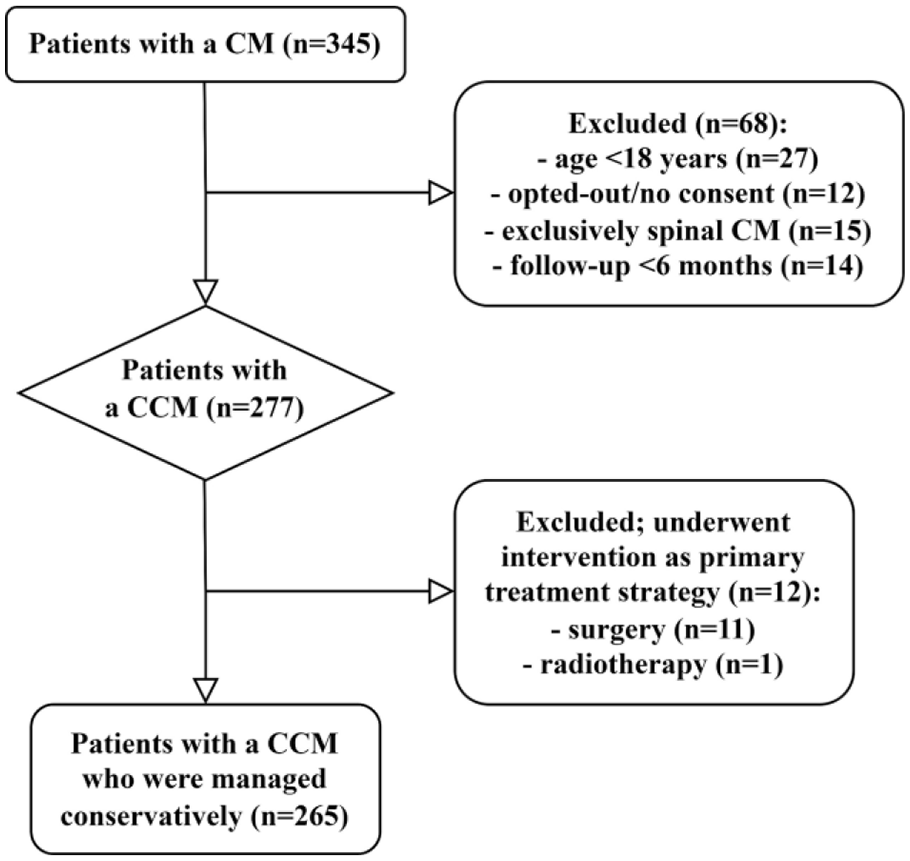
Flow diagram of patient selection.
Of 265 patients with a CCM included in the analysis, median age at presentation was 46 years (IQR 35–58) and 120 (45%) patients were male (Table 1). At baseline, 131 (49%) patients presented with a SH, and the remaining patients with a seizure (21, 8%), FNDs (8, 3%), or incidentally (105, 40%). Multiple CCMs occurred in 74 (28%) patients and 41 (15%) cases were familial. Sixty-six (25%) patients had a brainstem CCM. Patients who presented with a SH were younger (p = 0.006), and less frequently familial cases (p < 0.001) than patients who presented with other or no symptoms.
Baseline characteristics of all patients, and of patients who presented with or without SH.
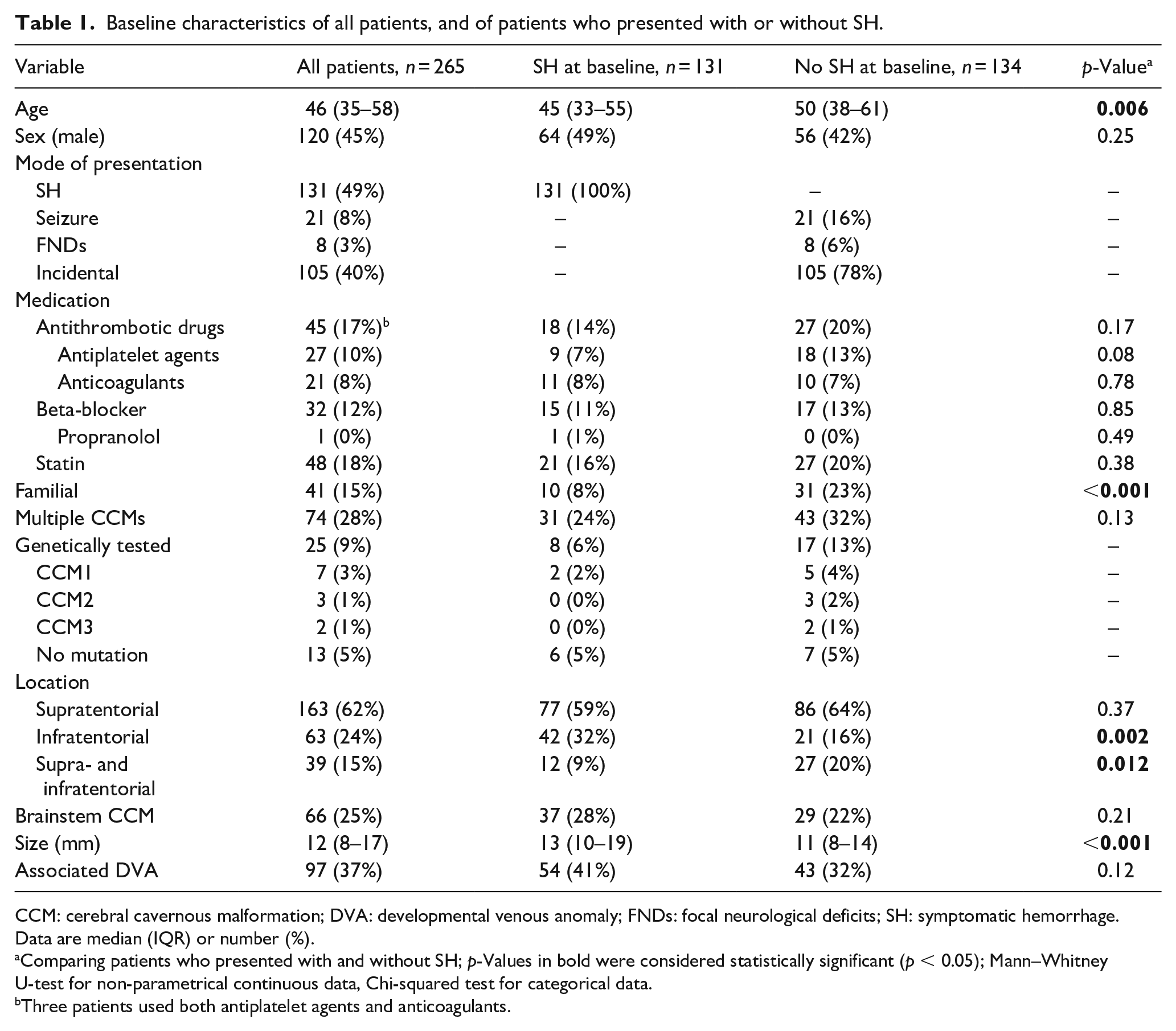
CCM: cerebral cavernous malformation; DVA: developmental venous anomaly; FNDs: focal neurological deficits; SH: symptomatic hemorrhage.
Data are median (IQR) or number (%).
Comparing patients who presented with and without SH; p-Values in bold were considered statistically significant (p < 0.05); Mann–Whitney U-test for non-parametrical continuous data, Chi-squared test for categorical data.
Three patients used both antiplatelet agents and anticoagulants.
Patients were followed-up for a median of 58 months (IQR 35–94). Follow-up results were collected for all patients and no data were missing. Mortality status was also available for all patients, and causes of death could be retrieved for all but one patient. At follow-up, 246 (93%) patients were alive. Of surviving patients, 205 (83%) completed the questionnaire after a median follow-up of 62 months (IQR 38–97). The remaining patients were consulted by telephone, except 6 (2%) patients who could not be reached.
During follow-up, 51 (19%) patients experienced a SH, 33 (12%) a seizure, and 13 (5%) FNDs (Table 2). Fourteen (5%) patients underwent intervention (surgery n = 11, radiosurgery n = 4 (1 both)), of whom 12 had initially presented with SH. Reasons for intervention were: recurrent SH (n = 8), persistent FNDs (n = 1), medically intractable epilepsy (n = 1), severe headache (n = 1), and patient’s preference (n = 1). Two patients were incidentally diagnosed, and despite remaining asymptomatic, surgery was initiated because the CCM grew on follow-up imaging. Further details are provided in Supplemental Appendix 3. Nineteen (7%) patients died during follow-up. Death attributable to the CCM occurred in two patients, who both presented with a SH caused by a brainstem CCM. Details on causes of death are provided in Supplemental Appendix 4.
Events during follow-up.
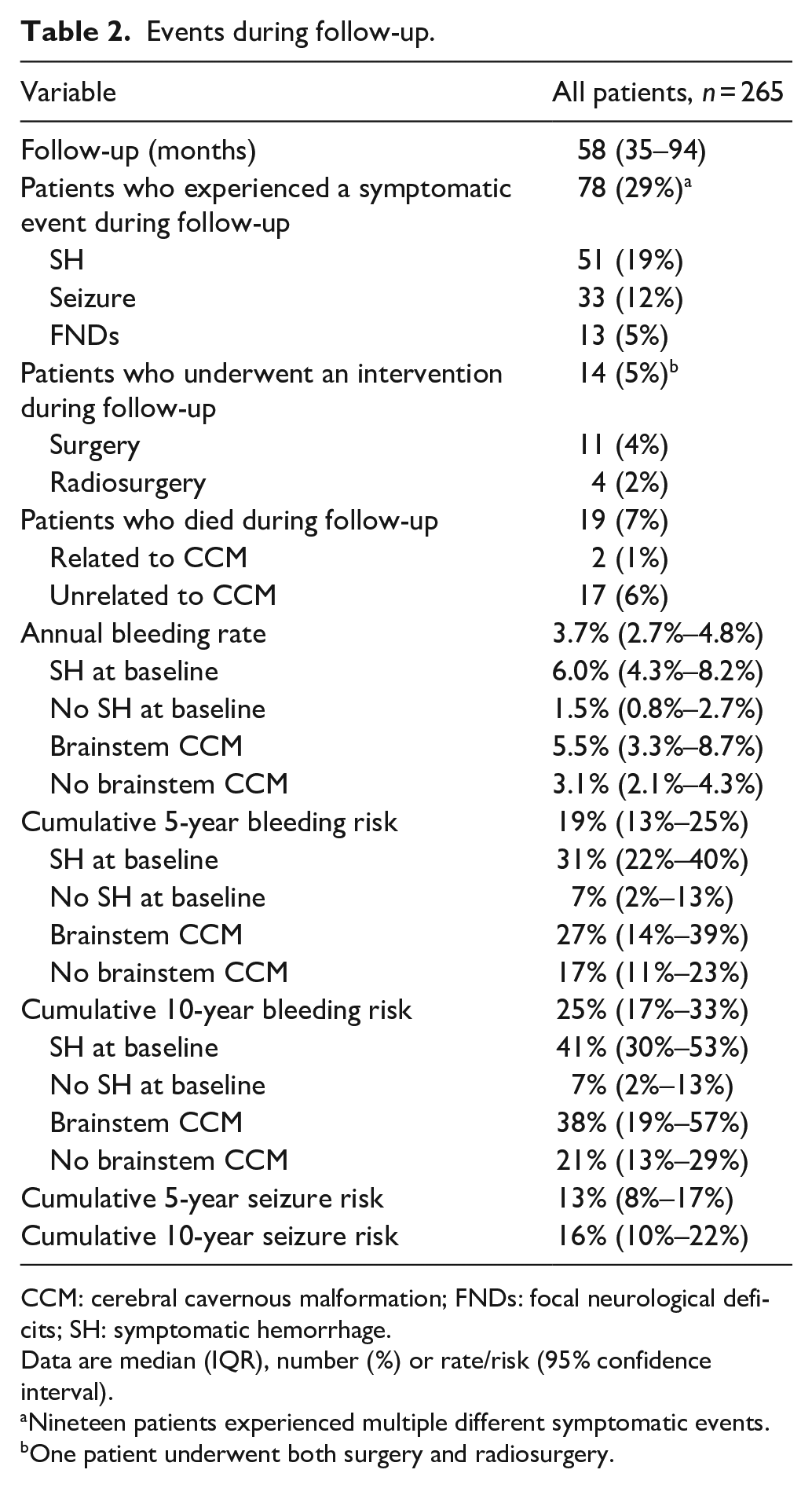
CCM: cerebral cavernous malformation; FNDs: focal neurological deficits; SH: symptomatic hemorrhage.
Data are median (IQR), number (%) or rate/risk (95% confidence interval).
Nineteen patients experienced multiple different symptomatic events.
One patient underwent both surgery and radiosurgery.
The annual bleeding rate was 3.7% (95% CI 2.7%–4.8%). Multiple SHs occurred in 23 (9%) patients, with most (n = 16) experiencing two SHs, while only a few (n = 7) experienced three or more SHs. Cumulative 5-year and 10-year bleeding risks were 19% (95% CI 13%–25%) and 25% (95% CI 17%–33%), respectively (Figure 2). Cumulative 5-year and 10-year seizure risks were 13% (95% CI 8%–17%) and 16% (95% CI 10%–22%), respectively.
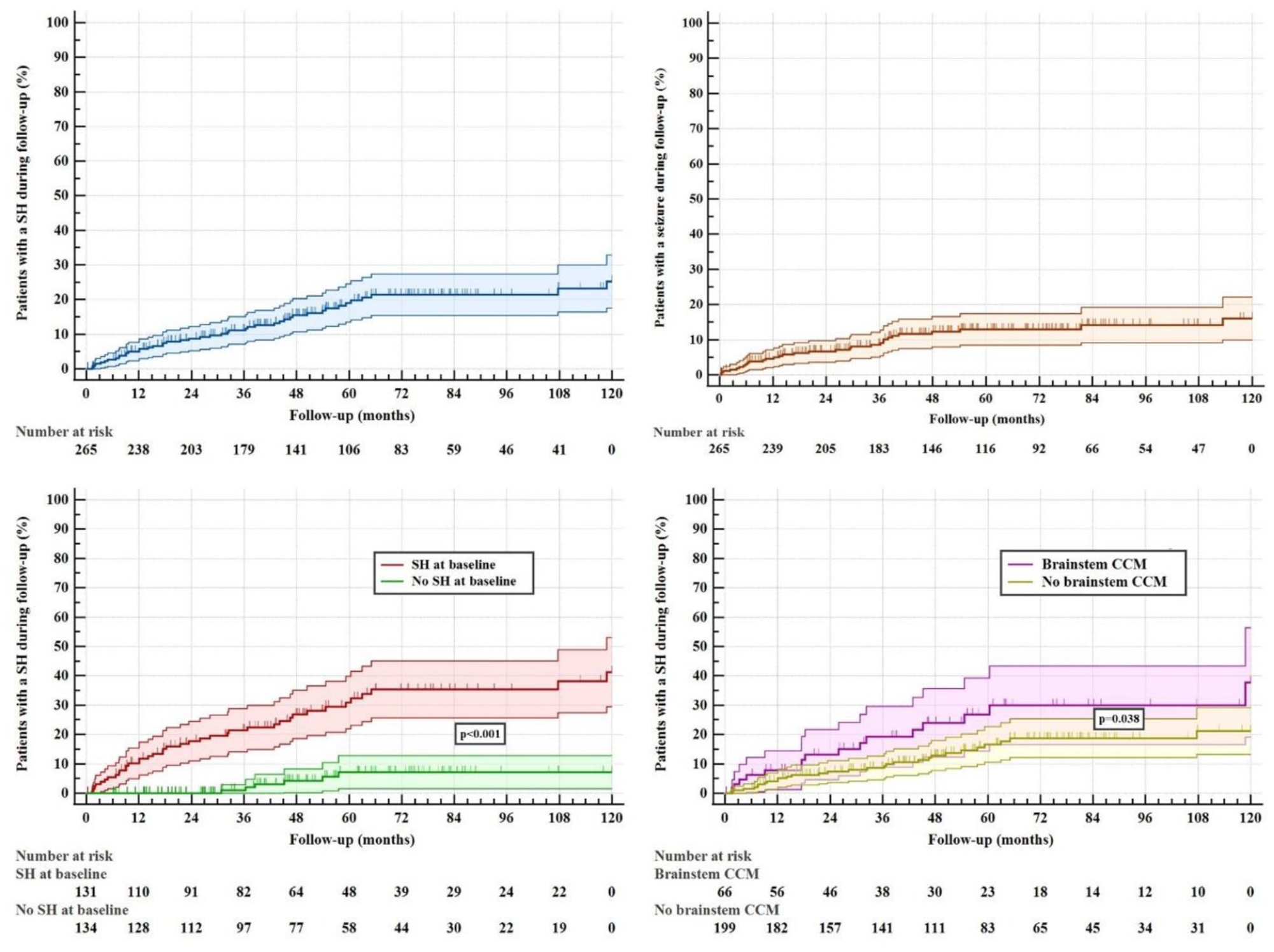
Kaplan–Meier analyses of patients with a SH or seizure during follow-up (%), with their 95% confidence intervals, during 10 years of follow-up; upper left: all patients in the cohort who experienced a SH during follow-up (blue); upper right: all patients in the cohort who experienced a seizure during follow-up (orange); bottom left: comparing SH during follow-up in patients who presented with SH (red) and without SH (green), higher rates of SH during follow-up were experienced by patients who presented with SH compared to those who did not, p < 0.001, log-rank test; bottom right: comparing SH during follow-up in patients with a brainstem CCM (purple) and without a brainstem CCM (yellow), higher rates of SH during follow-up were experienced by patients with a brainstem CCM compared to those without a brainstem CCM, p = 0.038, log-rank test.
SH during follow-up occurred more often in patients who had also presented with SH (40/51, 78%; annual bleeding rate 6.0%, 95% CI 4.3%–8.2%; cumulative 5-year risk 31%, 95% CI 22%–40%, and 10-year risk 41%, 95% CI 30%–53%) than in patients who presented with other or no symptoms (11/51, 22%, p < 0.001; annual bleeding rate 1.5%, 95% CI 0.8%–2.7%, p < 0.001; cumulative 5-year and 10-year risks 7%, 95% CI 2%–13%; p < 0.001). In addition to presentation with SH, size of the CCM was also associated with SH during follow-up, in which larger CCMs increased the risk (p = 0.002, Table 3).
Univariable analyses of variables associated with a SH during follow-up.
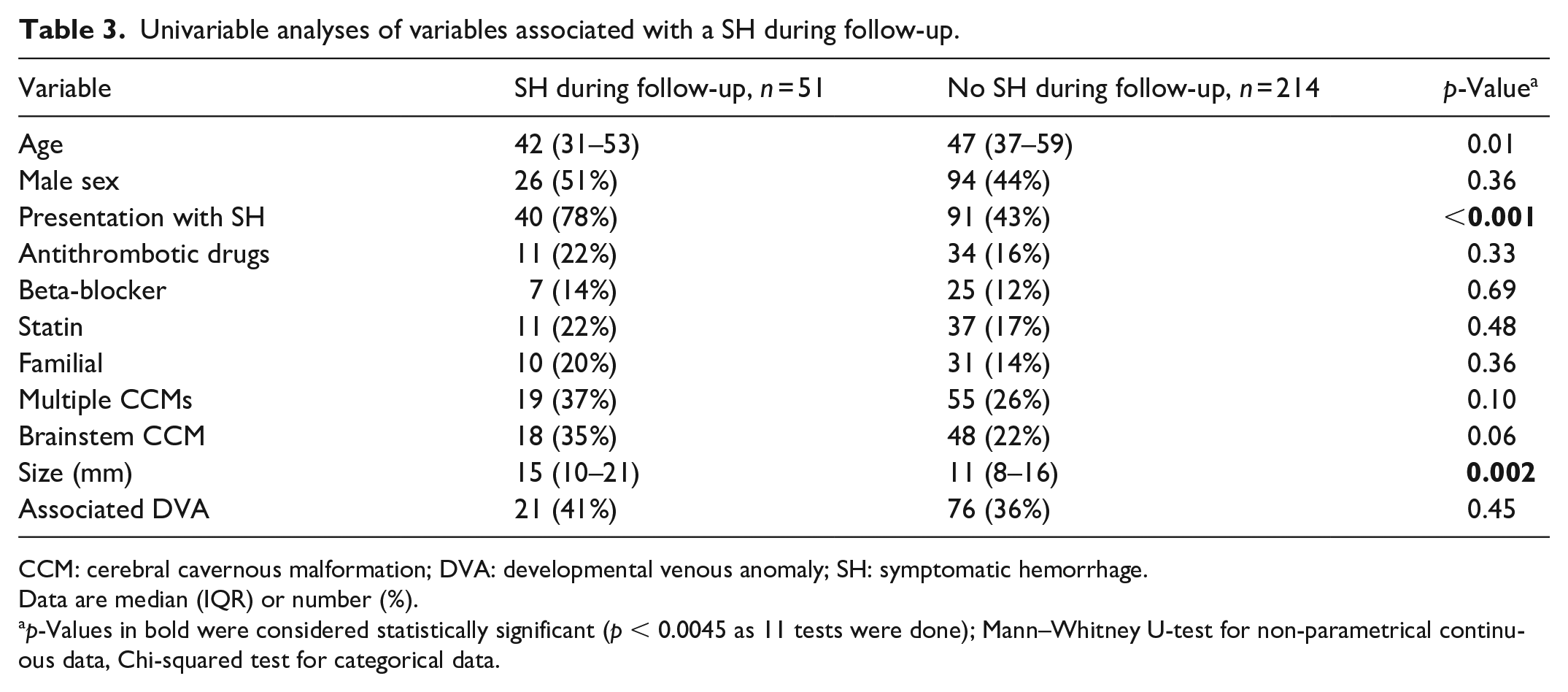
CCM: cerebral cavernous malformation; DVA: developmental venous anomaly; SH: symptomatic hemorrhage.
Data are median (IQR) or number (%).
p-Values in bold were considered statistically significant (p < 0.0045 as 11 tests were done); Mann–Whitney U-test for non-parametrical continuous data, Chi-squared test for categorical data.
Patients with a brainstem CCM had higher cumulative 5-year and 10-year risks (27%, 95% CI 14%-39%, and 38%, 95% CI 19%–57%, respectively) than patients without a brainstem CCM (17%, 95% CI 11%–23%, and 21%, 95% CI 13%–29%, respectively, p = 0.038). However, brainstem CCM was not associated with higher annual bleeding rates (5.5%, 95% CI 3.3%–8.7%, vs 3.1%, 95% CI 2.1%–4.3%, respectively, p = 0.05), or with a SH during follow-up in univariable analysis (18/51, 35%, vs 48/214, 22%, p = 0.06).
Of the 224 patients for whom an mRS score was available (n = 205 participants, n = 19 deceased patients), 172 (77%) patients were functionally independent at last follow-up (Figure 3). Proportions of functional independence did not differ between patients who presented with SH (79/107, 74%) and patients who presented with other or no symptoms (93/117, 79%, p = 0.32), and between patients with brainstem CCM (39/57, 68%) and without brainstem CCM (133/167, 80%, p = 0.08). Patients with a brainstem CCM who presented with a SH, however, were significantly less often functionally independent (20/32, 63%) than other patients (152/192, 79%, p = 0.039).
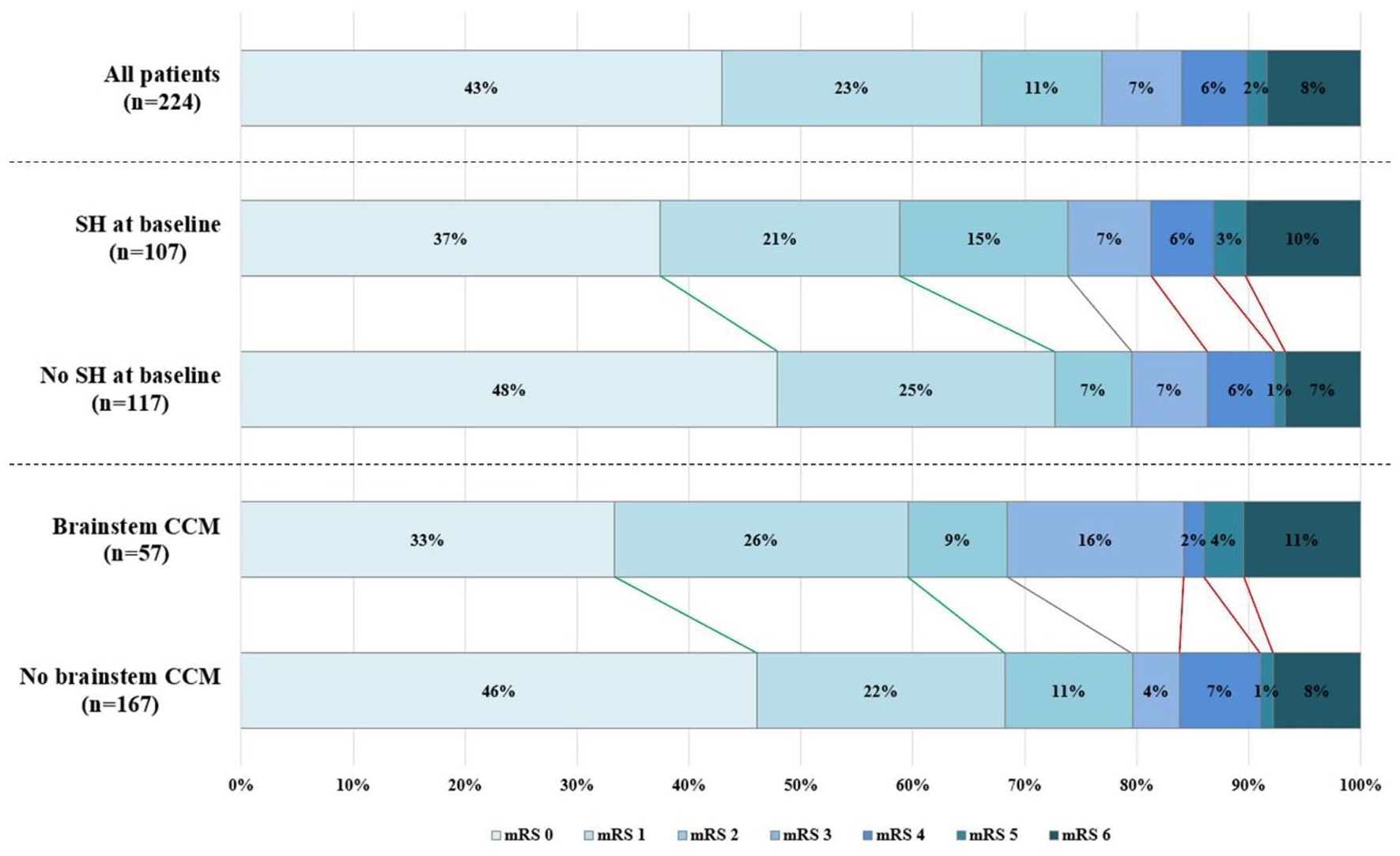
Scores on the modified Rankin Scale (mRS) at last follow-up; top: all patients in the cohort, 172/224 (77%) patients were functionally independent; middle: comparing patients who presented with SH and without SH, proportions of functional independence did not differ (79/107, 74%, vs 93/117, 79%, respectively, p = 0.32, Chi-squared test); bottom: comparing patients with a brainstem CCM and without a brainstem CCM, proportions of functional independence did not differ (39/57, 68%, vs 133/167, 80%, respectively, p = 0.08, Chi-squared test).
In a multivariable logistic regression model for functional independence (Supplemental Appendix 5), brainstem CCM and younger age (1-year decrements) were independent predictors for a poor functional outcome (OR 0.42, 95% CI 0.20–0.89, p = 0.023, and OR 1.04, 95% CI 1.02–1.07, p < 0.001, respectively). Interestingly, larger size (1-mm increments) was positively associated with functional independence at last follow-up (OR 1.06, 95% CI 1.00–1.11, p = 0.036). SH at baseline was not associated.
Discussion
In this retrospective cohort study, we evaluated conservative management as a primary treatment strategy for patients with a CCM. SH during approximately 5 years of follow-up occurred in less than one in five patients, and more often in patients who presented with SH, or those with a brainstem CCM. Approximately three-quarters of patients were functionally independent at follow-up. Death due to the CCM was rare, and only 1 out of 20 conservatively managed patients underwent an intervention during follow-up.
The policy at Amsterdam UMC is to manage CCMs conservatively as much as possible. Only 4% of patients underwent an intervention as a primary treatment strategy, and only 5% during follow-up, while in similar studies rates of 19%–48% are reported.16–18 Intervention after an initial conservative strategy occurred mostly because of a recurrent SH. Only two patients underwent surgery because of seizures or FNDs during follow-up. Reluctance to implement conservative management following a diagnosis of CCM may be driven by concerns about the development of symptoms requiring future interventions. This study shows that the clinical course of CCMs might be more favorable than previously thought, but longer follow-up is necessary to reach definitive conclusions.
Less than 1% of patients died due to the CCM, which is in line with other studies. One study reported death due to the CCM in 1/139 (0.7%) untreated patients, which occurred 30 days after a first SH. 5 Similarly, in two other studies that included patients who underwent an intervention, death due to CCM or treatment occurred in less than 1% of the patients.19,20
Rates of SH during follow-up were higher in patients who presented with SH compared to those who did not, which is analogous to previous studies.16,18 Flemming et al. reported an overall rate of 2.3%, which is slightly lower than our study. 17 This difference may be explained by our higher proportions of patients who presented with SH (49% vs 25%) or who had multiple CCMs (28% vs 18%). In contrast, Dammann et al. found a higher overall rate of 6.0% in their study on solitary sporadic CCMs. 18 An explanation may be that their patients had larger CCMs (15 vs 12 mm) and more often brainstem CCMs (28% vs 25%). The current study demonstrated that these variables were associated with an increased risk of SH, as did previous studies.16,17,21 Surprisingly, however, multivariable analysis revealed that larger CCM size unexpectedly emerged as a predictor for functional independence.
Increased risk of SH during follow-up after presenting with SH appeared to be most striking in the first years of follow-up. At 5 years of follow-up, our 5-year estimated cumulative risks (19% in all patients, 31% after presentation with SH, 7% after presentation with other symptoms or incidentally) were lower compared to the study of Dammann et al. (25%, 41%, 9%, respectively). 18 This also may be explained by the high number of brainstem and large CCMs in their study. Another meta-analysis, however, reported marginally lower 5-year risks (16%, 26%, 4%, respectively), 16 but this study contained patients who presented with either SH or FNDs, and the median follow-up duration was shorter (3.5 years).
After a median follow-up of 5 years, three out of four patients were functionally independent. This is lower than in a study of Kim et al. (91%) who determined mRS scores of untreated patients after a SH in the past year (median time from SH to assessment of mRS was 3.6 months, IQR 1.8–6.3). 22 However, these authors only included patients who were alive, while our cohort also contained deceased patients. The proportion of functionally independent patients in our study was comparable with the study of Dammann et al. (70%), who annually assessed whether mRS scores decreased after a SH. 18
The presented variables associated with a SH during follow-up could inform treatment selection for patients with a CCM. Patients who did not present with a SH or lack a brainstem CCM might be more readily selected for conservative management. However, presentation with a SH caused by a brainstem CCM does not necessarily imply that intervention is the preferred treatment strategy. Periprocedural risks are particularly pronounced with brainstem CCMs, as illustrated in a previous systematic review. 23 Selecting patients for intervention thus remains challenging, and requires careful consideration of each individual case based on patient characteristics and surgical accessibility.
Our study has some limitations. First, its retrospective design and execution in a single reference center may have led to selection bias. Mild cases may not have been referred to our tertiary hospital, potentially leading to overestimated event rates. Extrapolation of the results should therefore be done with caution. Second, although numbers were small, including patients with a fatal hemorrhage within 6 months of follow-up, while excluding other patients with less than 6 months of follow-up, potentially introduced bias due to inconsistent criteria used in the numerator versus the denominator. Third, calculated rates and risks were unadjusted, leaving them susceptible to potential confounding by characteristics we could not account for. Fourth, while response rates to the questionnaire were high, approximately 17% of the patients did not complete the questionnaire. These patients may have scored differently from the patients in our analyses. On the other hand, only 2% were not reached, and we retrieved the cause of death for all but one patient. No other data were missing. Fifth, although functional outcome scales provide a standardized objective measurement, they may insufficiently capture quality of life and subjective wellbeing of patients.
Our understanding of CCM treatment stands to evolve with upcoming results of a randomized controlled pilot trial comparing conservative management to intervention, of which a protocol has been published recently. 24 Promising alternatives to reduce the risk of symptomatic hemorrhage are beta-blockers,25,26 and antithrombotic therapy. 27 Future research could explore prognosis of untreated CCMs in the very long term including longitudinal assessment of functional status at prespecified time-points and following a SH to monitor potential recovery. Additionally, development of a risk model to predict the occurrence of a SH could contribute to patient counseling and treatment selection for CCM.
Conclusion
More than four out of five patients with a CCM who were primarily managed conservatively remained free of a SH during approximately 5 years of median follow-up. Risk of a SH during follow-up was increased in patients who presented with SH, or who had a brainstem CCM. Death attributable to the CCM was rare and three-quarters of patients were functionally independent at follow-up. These data may help patient counseling and treatment decisions for patients with a CCM.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241246868 – Supplemental material for Clinical course of patients with conservatively managed cerebral cavernous malformations
Supplemental material, sj-docx-1-eso-10.1177_23969873241246868 for Clinical course of patients with conservatively managed cerebral cavernous malformations by Abel Clemens Adriaan Sandmann, Marinus Abraham Kempeneers, René van den Berg, Dagmar Verbaan, William Peter Vandertop and Jonathan M. Coutinho in European Stroke Journal
Supplemental Material
sj-docx-2-eso-10.1177_23969873241246868 – Supplemental material for Clinical course of patients with conservatively managed cerebral cavernous malformations
Supplemental material, sj-docx-2-eso-10.1177_23969873241246868 for Clinical course of patients with conservatively managed cerebral cavernous malformations by Abel Clemens Adriaan Sandmann, Marinus Abraham Kempeneers, René van den Berg, Dagmar Verbaan, William Peter Vandertop and Jonathan M. Coutinho in European Stroke Journal
Footnotes
Acknowledgements
This study received the Arthur Fonville Award for Stroke Research.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JMC received financial support from the Dutch Heart Foundation, Medtronic, Bayer and Boehringer (all fees were paid to his employer), and is co-founder and shareholder of TrianecT. RvdB has a non-personal hospital consultancy at Johnson & Johnson (CERENOVUS). All other authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was waived for ethical approval by the Institutional Review Board of the Amsterdam UMC because it did not fall under the scope of the Medical Research Involving Human Subjects Act (WMO). This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Informed consent
For the reuse of clinical data, we carried out an opt-out procedure. All patients who completed the questionnaire provided written informed consent.
Trial registration
Not applicable.
Guarantor
JMC.
Contributorship
ACAS conducted the study and wrote the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.