
Abstract
Introduction:
Inflammation is an emerging target for secondary prevention after stroke and randomised trials of anti-inflammatory therapies are ongoing. Fibrinogen, a putative pro-inflammatory marker, is associated with first stroke, but its association with major adverse cardiovascular events (MACE) after stroke is unclear.
Materials and Methods:
We did a systematic review investigating the association between fibrinogen and post-stroke vascular recurrence. Authors were invited to provide individual-participant data (IPD) and where available we did within-study multivariable analyses with adjustment for cardiovascular risk factors and medications. Adjusted summary-level data was extracted from published reports from studies that did not provide IPD. We pooled risk ratios (RR) by random-effects meta-analysis by comparing supra-median with sub-median fibrinogen levels and performed pre-specified subgroup analysis according to timing of phlebotomy after the index event.
Results:
Eleven studies were included (14,002 patients, 42,800 follow-up years), of which seven provided IPD. Fibrinogen was associated with recurrent MACE on unadjusted (RR 1.35, 95% CI 1.17–1.57, supra-median vs sub-median) and adjusted models (RR 1.21, 95% CI 1.06–1.38). Fibrinogen was associated with recurrent stroke on univariate analysis (RR 1.19, 95% CI 1.03–1.39), but not after adjustment (RR 1.11, 95% CI 0.94–1.31). The association with recurrent MACE was consistently observed in patients with post-acute (⩾14 days) fibrinogen measures (RR 1.29, 95% CI 1.16–1.45), but not in those with early phlebotomy (<14 days) (RR 0.98, 95% CI 0.82–1.18) (Pinteraction = 0.01). Similar associations were observed for recurrent stroke.
Discussion and Conclusion:
Fibrinogen was independently associated with recurrence after stroke, but the association was modified by timing of phlebotomy. Fibrinogen measurements might be useful to identify patients who are more likely to derive benefit from anti-inflammatory therapies after stroke.

Introduction
The global prevalence of stroke exceeded 100 million individuals in 2019 1 with recent estimates projecting a further increase in the burden of stroke in the coming decades. 2 Survivors of first stroke are at high risk of recurrent stroke, myocardial infarction and vascular death, despite contemporary prevention treatments, with estimated rates of approximately 30% at 5 years. 3 Consequently there is an unmet need to develop new secondary prevention strategies after stroke and targeting inflammation is a promising strategy. Clinico-pathological, 4 laboratory, 5 and imaging data 6 support a role for inflammation in the pathogenesis of recurrence after stroke. Anti-inflammatory therapies, such as colchicine and canakinumab, reduce the risk of major adverse cardiovascular events (MACE) including stroke in patients with coronary artery disease.7,8
The conversion of fibrinogen to insoluble fibrin is the final step of the coagulation cascade, leading to clot formation. Fibrinogen has several other additional pro-thrombotic effects, including stimulation of platelet aggregation and increased blood viscosity. 9 Fibrinogen is also an inflammatory marker, synthesised by hepatocytes in response to upstream interleukin-1ß (IL-1ß)-IL-6 signalling. Fibrinogen has several inflammatory and pro-atherogenic effects including enhancement of platelet activation, adhesion molecule expression on vascular endothelial cells, enhanced macrophage infiltration into plaque, increased monocyte expression of pro-inflammatory cytokines (IL-1ß, TNFα) and chemokine expression by vascular endothelial cells.10,11 Plasma fibrinogen is associated with first stroke and coronary events in apparently-healthy individuals. 12 Genetic epidemiology studies have also shown that fibrinogen is associated with an increased lifetime risk of large-artery and small vessel stroke. 13 However, the association of fibrinogen with recurrent events after stroke is unclear. A previous systematic review was limited by variability in the definition of inflammatory marker exposure, incomplete adjustment for confounding variables, and insufficient statistical power to examine important subgroups. 14 In this updated meta-analysis we have pooled individual participant data (IPD) from seven prospective studies with summary-level data from four other cohort studies and investigated the association between post-stroke fibrinogen levels and recurrent vascular events. We also explored the influence of age, sex, timing of blood draw, stroke severity, and stroke subtype on associations with recurrence.
Methods
Systematic review
To identify all relevant studies, we first did a systematic review of studies investigating the association between blood inflammatory markers, measured after ischaemic stroke or TIA, and the risk of recurrent stroke/MACE. Details of eligibility criteria, search strategy, and data extraction have been previously described. 14 Briefly, two reviewers searched EMBASE, Ovid Medline and conference proceedings for eligible studies (Web-supplement). Main eligibility criteria were studies of ⩾50 patients with ischaemic stroke/transient ischaemic attack (TIA), inflammatory markers measured post-event, and reported associations with recurrent stroke or MACE. The protocol was published on PROSPERO (CRD42018116190). This manuscript is written according to PRISMA-IPD guidelines (Web-supplement). 15
Data extraction
Authors of eligible studies identified by systematic review were invited to provide IPD for the Blood Inflammatory markers in Stroke Collaboration (BISC). Details of data harmonisation and study oversight for BISC are provided in the Web-Supplement and have been previously described. 16 Stroke mechanism was categorised at a study-level using Trial of ORG 10172 in Acute Stroke Treatment (TOAST) 17 criteria. Data extraction procedures for included studies not providing IPD are previously described. 14
Outcomes
The pre-specified outcomes for this analysis were: (1) any MACE (first event of either recurrent stroke, major coronary event or vascular death) (2) first recurrent stroke which occurred after blood sampling (for definitions see Web-Supplement).
Risk of bias
The quality in prognosis studies (QUIPS) tool was used to assess the risk of bias (Web-Supplement). 18
Statistical analysis
For studies providing IPD we explored the relationship between fibrinogen and co-variates (including demographics, cardiovascular risk factors and medications). The relationship with continuous co-variate data was analysed by plotting the mean concentrations of fibrinogen within each tenth of the co-variate distribution and the degree of association examined using Spearman’s rank correlation. For categorical variables, differences in fibrinogen concentrations were analysed using the Mann-Whitney U-test.
For studies providing IPD, estimates of association (hazard or odds ratios) of the baseline levels of fibrinogen with recurrent events were calculated separately within each study after identical adjustment for potential confounding variables. For prospective cohort studies, adjusted hazard ratios (HR) were estimated from multivariable Cox proportional hazards regression, with time to first recurrence as the dependent variable. For the single nested case-control study within a randomised trial (Perindopril Protection Against Recurrent Stroke Study (PROGRESS)), 19 the adjusted odds ratio (OR) was calculated using a conditional logistic regression model. HRs or ORs were assumed to approximate the same relative risk (because the outcome is rare) and were collectively summarised as risk ratios (RRs). The proportional hazard assumption was tested by visual examination of survival curves for studies with time-to-event data available. In the multivariable analysis of IPD, we adjusted for age, sex, hypertension, smoking, diabetes mellitus, atrial fibrillation, coronary artery disease, statin therapy, anti-thrombotic use, and trial arm (where appropriate). Variables included in the adjusted model were pre-specified. For studies not providing IPD we extracted adjusted effect estimates from published reports. 14 Meta-analysis of published summary data with that of IPD was only possible for studies that provided uniform effect measures. Four large studies had published summary RRs for recurrence dichotomised according to median fibrinogen concentrations. Therefore we replicated this statistical approach in the 7 studies providing IPD and calculated RRs for recurrence in each study stratified by median fibrinogen concentrations. We then pooled study-level effect estimates from all 11 studies by random effects meta-analysis with inverse variance weighting. 20
Pre-specified subgroup analyses were performed using cox proportional hazards or conditional logistic regression (as appropriate) to estimate adjusted RRs according to age, sex, index event severity, and time to phlebotomy, with between-group differences formally assessed using Cochran’s Q. Where possible, we performed subgroup analyses with fibrinogen expressed on a continuous scale (per g/l) in accordance with recommendations on prognostic factor measurement. 21 All analyses were done using Stata Version 16.
Results
Study selection
The systematic literature search identified 2515 non-duplicate records. After title and abstract screening, 130 studies were selected for full text review. 14 This identified 18 studies. After contacting corresponding authors, seven studies comprising 6789 patients and 16,028 person-years of follow-up agreed to provide IPD.22–28 Four additional studies29,30 with published summary-data were identified for inclusion in the meta-analysis, each of which reported unadjusted and adjusted associations with recurrent MACE or stroke by comparing supra-median with sub-median fibrinogen levels. Of the remaining seven studies, reasons for exclusion from this meta-analysis were: (1) no effect estimate reported (four studies); (2) no exposure definition reported (two studies); and (3) exposure definition using arbitrary threshold (one study). The final sample included 11 studies with 14,002 patients with 42,800 years of follow-up (Figure 1). No study was considered at high risk of bias in any domain of the QUIPS tool (Web-Supplement).
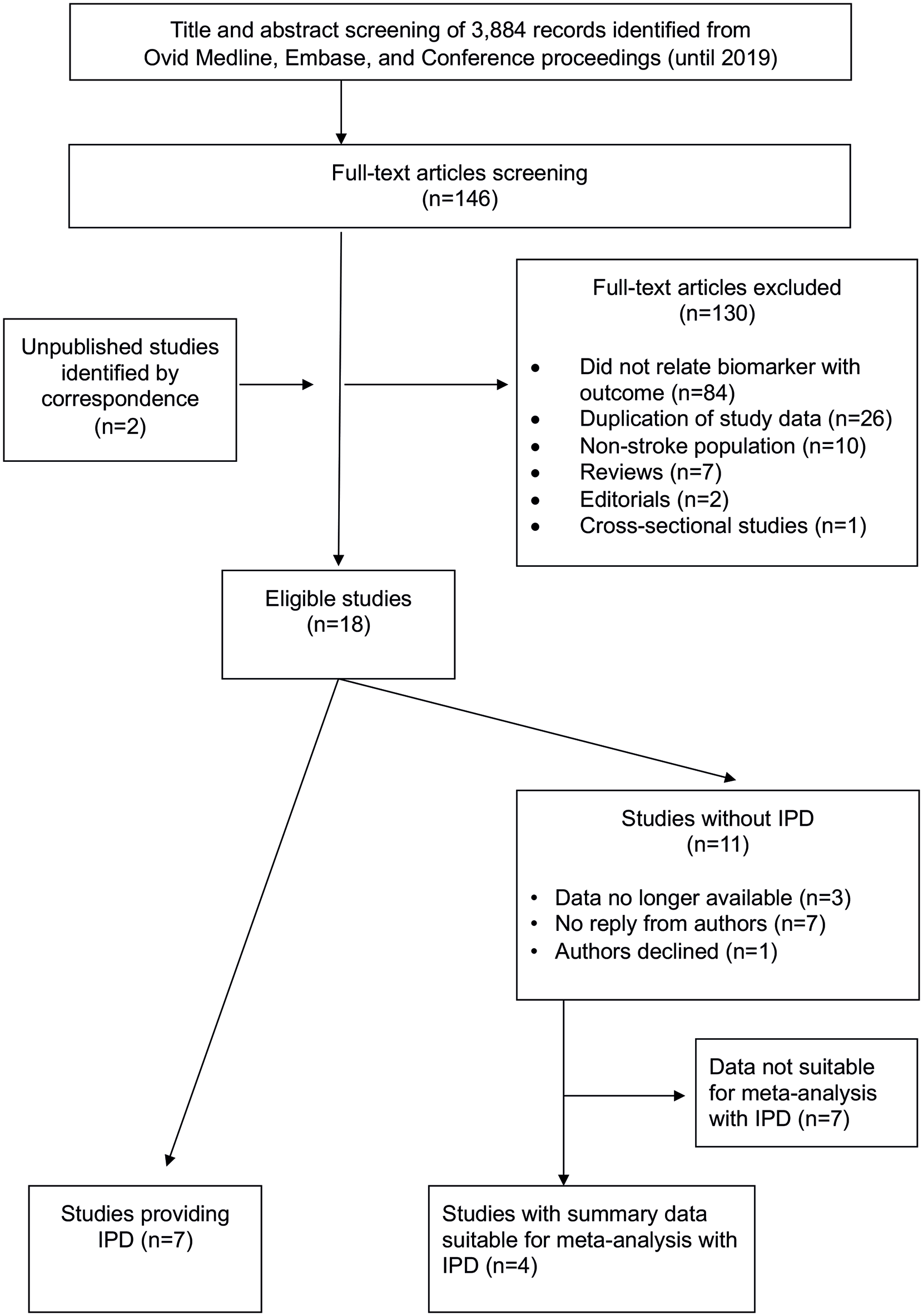
PRISMA flow-chart for study inclusion.
Study characteristics
Characteristics of included studies are provided in Table 1 and Web-Supplement. Of the 11 studies, seven were prospective cohort studies, three were RCTs, and one was a nested case-control study within an RCT. Six studies restricted eligibility to non-disabling strokes (n = 4) or TIAs only (n = 2). The duration of follow-up ranged from 90 days to 10.8 years. The median time to phlebotomy was ⩽14 days in five studies and >14 days in six studies.
Characteristics of included studies.
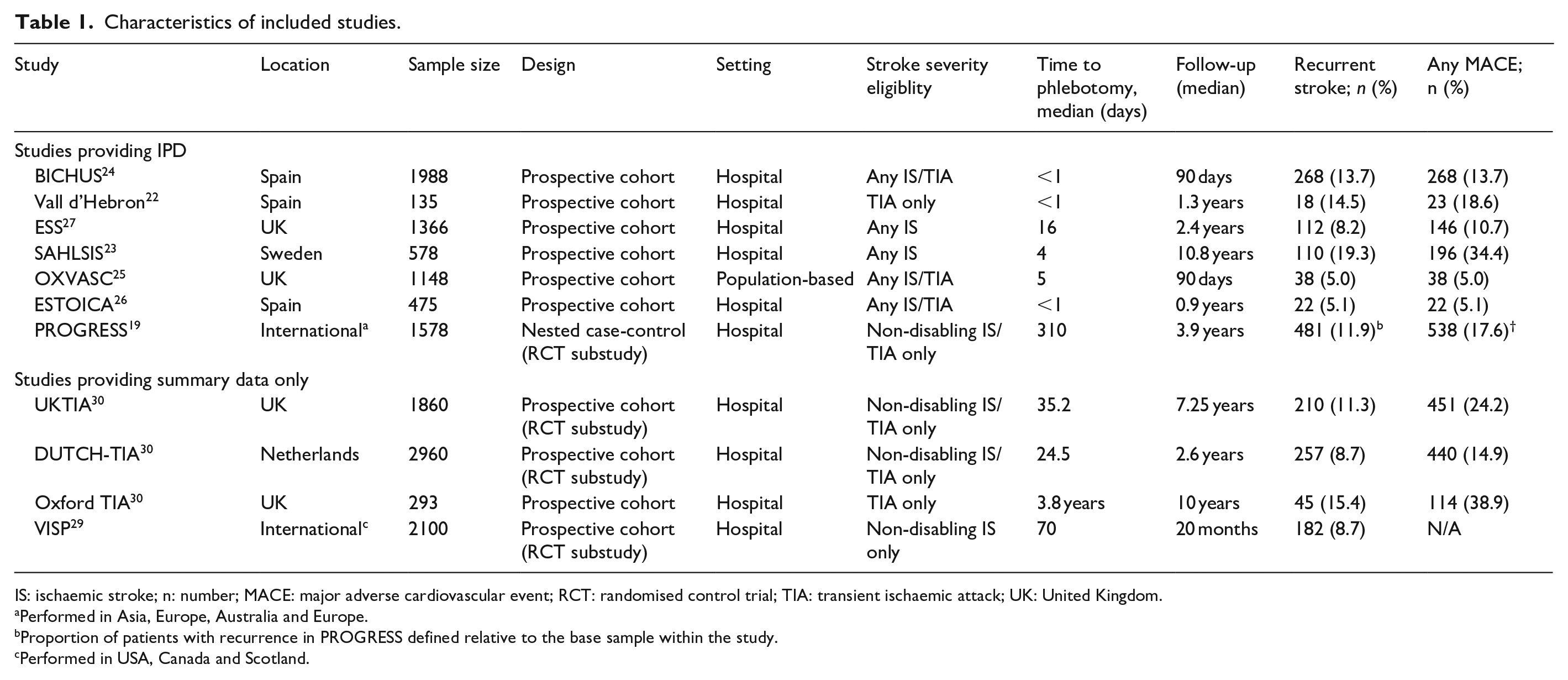
IS: ischaemic stroke; n: number; MACE: major adverse cardiovascular event; RCT: randomised control trial; TIA: transient ischaemic attack; UK: United Kingdom.
Performed in Asia, Europe, Australia and Europe.
Proportion of patients with recurrence in PROGRESS defined relative to the base sample within the study.
Performed in USA, Canada and Scotland.
Associations with fibrinogen concentrations
In the IPD cohort, the median fibrinogen was 4.27 g/l (interquartile range (IQR) 3.6–5.0). Fibrinogen levels were associated with female sex, age, NIHSS, diabetes mellitus, hypertension, atrial fibrillation, and coronary disease (p < 0.001 for all). Levels were lower in patients with TIAs compared with ischaemic stroke (p < 0.001) and higher in patients taking statins pre-event (p < 0.007). Fibrinogen concentrations inversely correlated with LDL and HDL (p < 0.001). Fibrinogen concentrations tended to be higher in cardio-embolic and large artery stroke compared with stroke due to small vessel occlusion or undetermined aetiology (p < 0.001) (Web-Supplement). A weak inverse correlation was observed between fibrinogen and duration from index event to phlebotomy (rho −0.05, p = 0.001).
Plasma fibrinogen and recurrence
In the summary data meta-analysis of all 11 studies there was a total of 1743 recurrent strokes and 2236 recurrent MACE outcomes. Supra-median fibrinogen (vs sub-median levels) was associated with a higher risk of recurrent MACE (RR 1.35, 95% CI 1.17–1.57, p = 0.0001, I 2 = 54.0). After adjustment for age, sex, cardiovascular risk factors, and secondary prevention medication use, the association remained statistically significant (RR 1.21, 95% CI 1.06–1.38, p = 0.006, I 2 = 37%). Similar results were found for recurrent stroke on unadjusted analysis (RR 1.19, 95% CI 1.03–1.39, p = 0.03, I 2 = 41.6%), but this was no longer significant after adjustment (RR 1.11, 95% CI 0.94–1.31, p = 0.22, I 2 = 45%) (Figure 2). Details of the variables included in the adjusted models in the four studies not providing IPD are provided in the Web-Supplement.
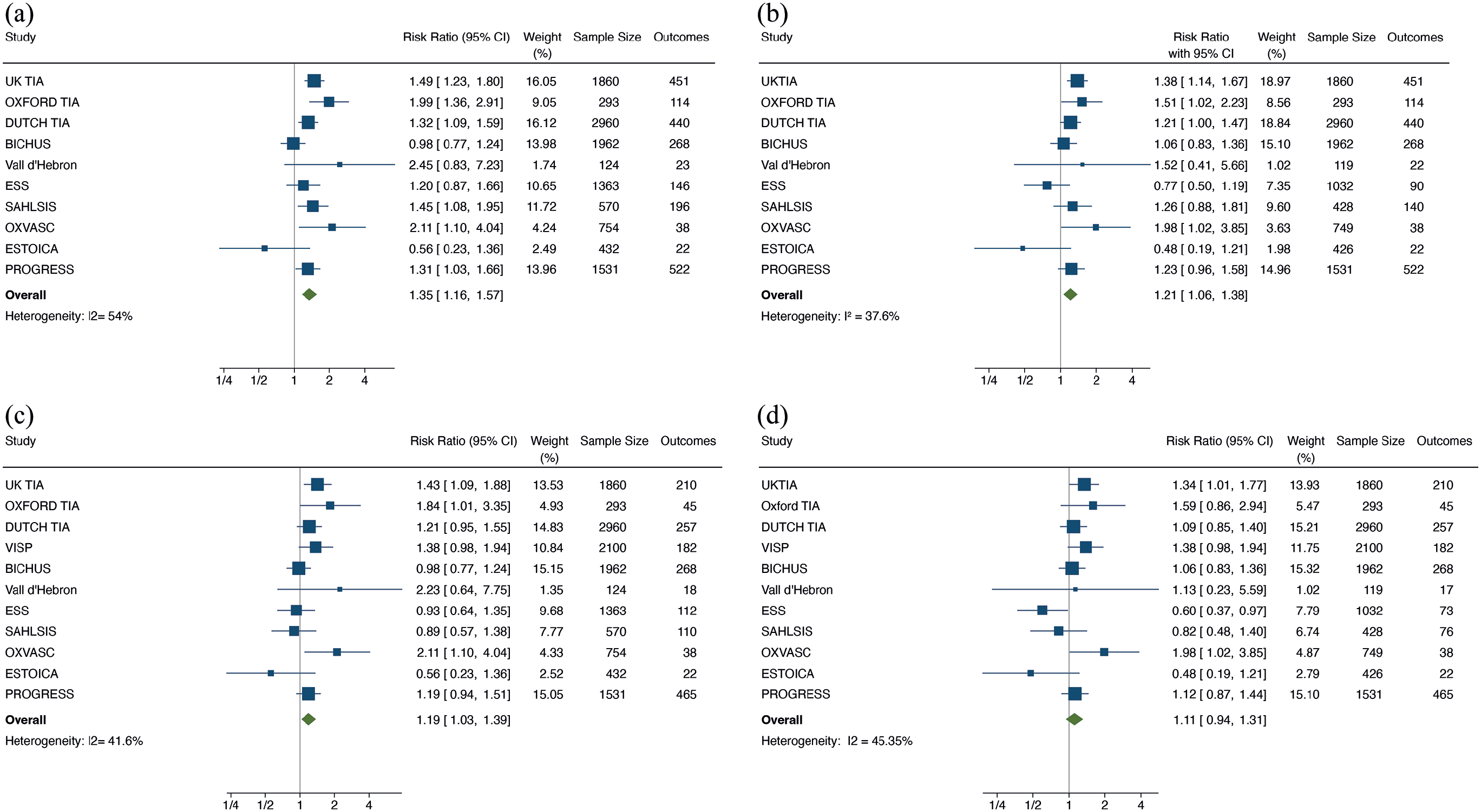
Fibrinogen and risk of recurrence. Fibrinogen and risk of: (a) MACE on unadjusted analysis, (b) MACE on adjusted analysis, (c) recurrent stroke on unadjusted analysis, and (d) recurrent stroke on adjusted analysis. The analysis compares supra-median fibrinogen levels with sub-median levels. The UKTIA, OXFORD TIA, and DUTCH TIA studies adjusted for age, sex, CAD, smoking, diabetes, anti-thrombotics, body weight, blood pressure, and total cholesterol. The VISP trial adjusted for treatment group, age, race, sex, smoking, body mass index, diabetes, hypertension, and LDL.
Subgroup analysis
We examined the association between plasma fibrinogen and recurrent events according to the timing of blood sampling after index stroke. Fibrinogen was independently associated with recurrent MACE in the post-acute phase (>14 days) after index event (RR 1.29, 95% CI 1.16–1.45, p < 0.0001, supra- vs sub-median, I 2 = 0%), but not in the acute phase (0–14 days) (RR 0.98, 95% CI 0.82–1.18, p = 0.85) (Pinteraction = 0.01) (Figure 3). Consistent findings were observed for the outcome of recurrent stroke (post-acute RR 1.27, 95% CI 1.15–1.42 vs acute RR 0.92, 95% CI 0.75–1.12, Pinteraction 0.005)) (Web-Supplement).
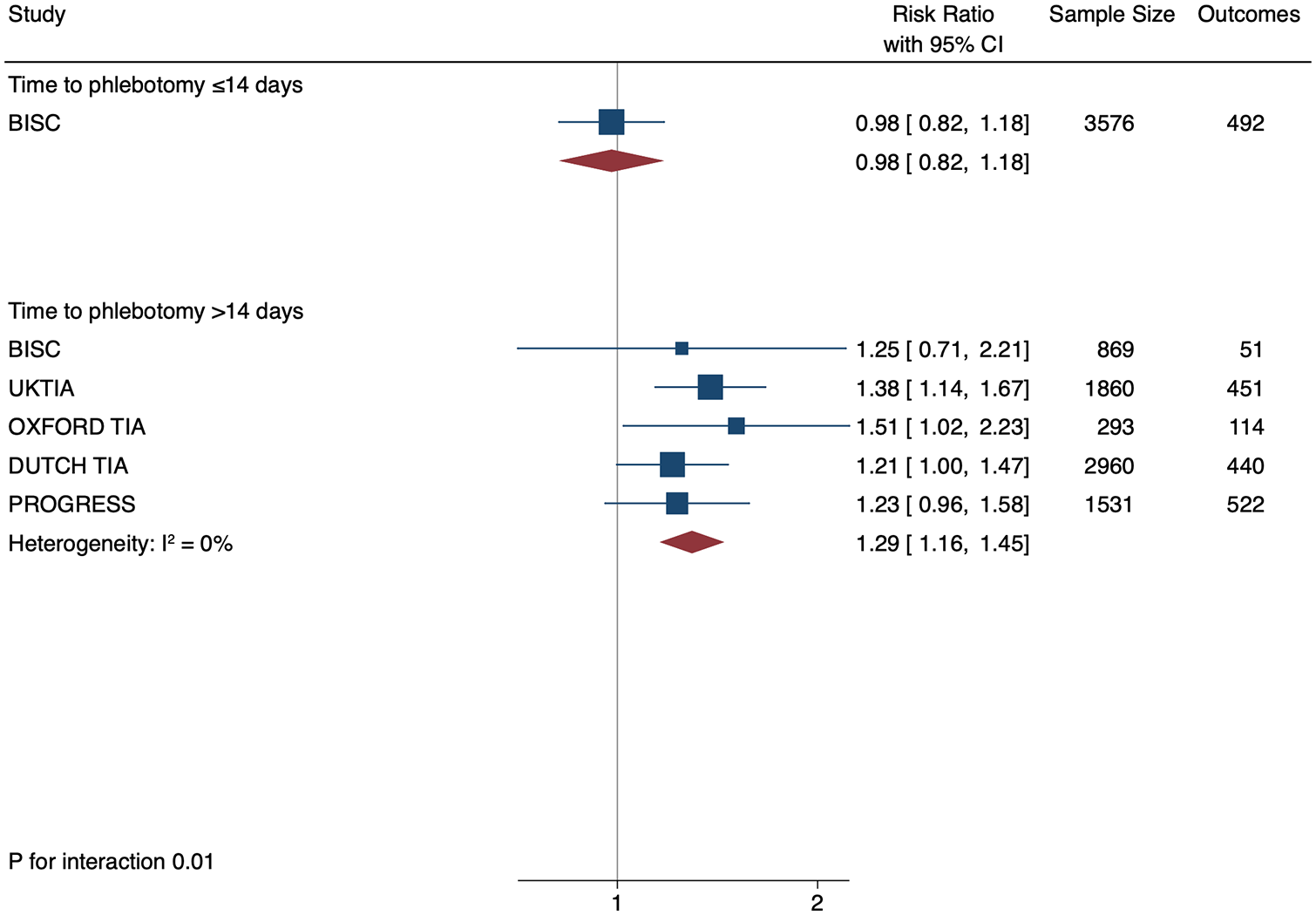
Subgroup analysis according to time to phlebotomy. Data shown are derived from pooling the IPD dataset with summary-level data from studies not providing IPD. Early phlebotomy refers to sample measurement <14 days from index event and late phlebotomy refers to sampling ⩾14 days. Data for BISC are presented as a single estimate due to statistical convergence of effect estimates on per-study analysis. Data for time to phlebotomy was missing in 278 patients in BISC.
Subgroup analyses according to age, sex, stroke mechanism, and NIHSS were done in the patients from the studies providing IPD for whom data was available. Fibrinogen was associated with recurrence in males (RR 1.09, 95% CI 1.00–1.19, p = 0.049 per g/l increase) but not in females (RR 0.89, 95% CI 0.72–1.10, p = 0.29) (Pinteraction = 0.08). There was no evidence of heterogeneity in subgroups stratified according to age, stroke severity, or index event mechanism (Web-Supplement).
Sensitivity analysis
We explored for the influence of a single study on the overall results and found that our findings were not altered by the removal of one study at a time from the meta-analysis (Web-Supplement).
Discussion
Using summary data from 14,002 patients and 11 studies we demonstrated that fibrinogen was associated with recurrent MACE in patients with a previous ischaemic stroke or TIA. On subgroup analysis this association was dependent on the timing of phlebotomy. Fibrinogen levels were not associated with recurrence when measured in the acute phase after stroke but were strongly associated with both recurrent stroke and recurrent MACE when measured in the post-acute phase. This association was robust after adjusting for cardiovascular risk factors and secondary prevention medication.
This data is in keeping with classical 12 epidemiological and genetic 13 studies that support an association between fibrinogen and first-ever stroke. In addition to its pro-thrombotic function, fibrinogen is also an acute phase reactant which is synthesised by hepatocytes in response to IL-6 activation in response to pro-inflammatory stimuli, including atherosclerosis. Fibrinogen levels increase in the setting of several cardiovascular risk factors 31 and exerts downstream atherogenic effects, including endothelial activation, monocyte recruitment, and LDL deposition. 11 Our results are also consistent with several recent observational studies that demonstrate independent associations between other blood inflammatory markers, such as IL-6 and CRP, and recurrent MACE after stroke. 16 Anti-inflammatory therapies, such as colchicine and canakinumab, have proven benefit in reducing recurrent events in coronary disease.7,8 Our findings contribute further data supporting the potential benefit of anti-inflammatory therapies for prevention after stroke, which to date are unproven. Our results also have implications for the design of future RCTs in stroke. The contribution of inflammatory mechanisms to recurrence may vary between individual patients after stroke. It is possible, but yet unproven, that blood inflammatory markers may be used to identify patients who are most likely to benefit from anti-inflammatory therapies. Measurement of fibrinogen in the post-stroke convalescent phase may contribute towards strategies for individualised patient selection in future RCTs.
Although the precise reason for the neutral association between fibrinogen and vascular recurrence in the acute phase is unclear, we speculate that it may be explained by the confounding effect of the systemic inflammatory response to brain infarction or due to transient alterations in fibrinogen isoform expression after stroke which leads to an increase in γ′ fibrinogen. 32 This transient alteration in fibrinogen expression may be important as, unlike total fibrinogen, γ′ fibrinogen has anti-thrombotic effects and is associated with a reduced stroke risk. 13
We also observed an association between fibrinogen and recurrent events in men but not in women. The significance of this finding is unclear as the formal test for interaction fell short of statistical significance. It is possible that this finding reflects greater inflammatory or thrombotic activation in men compared with women. Males have higher atherosclerotic plaque burden than females and imaging studies using positron-emission tomography have suggested greater plaque inflammation in men than in women. 33 However, we cannot exclude the possibility that this finding was due to chance. Future studies on sex-specific associations between fibrinogen and vascular recurrence are needed.
Our study has several strengths. The sample size was large, which ensured adequate statistical power and allowed for subgroup analyses which were not possible in earlier studies. Summary data and IPD were identified by systematic review which ensured a comprehensive data synthesis. Studies included in the meta-analysis were of high quality and low risk of bias. Access to IPD in seven of the 11 studies allowed standardised definitions of exposure, outcome, and co-variates, and enabled a more comprehensive multivariate analysis to control for confounding variables, compared to previous studies. 14 Our findings are consistent with evidence from laboratory, genetic, epidemiological, and imaging studies which clearly demonstrate the important of inflammatory mechanisms in stroke pathogenesis and recurrence.
We acknowledge some limitations. We cannot fully exclude the low possibility of residual confounding. However, we feel that this is unlikely to have significantly influenced our findings as we adjusted for all major cardiovascular risk factors and secondary prevention medications. Fibrinogen levels were associated with NIHSS and stroke subtype. Due to missing data, it was not possible to include these variables in the adjusted models for recurrent events. However, there was no evidence of an interaction for recurrent MACE on subgroup analysis according to stroke severity or subtype. We did not measure γ′ fibrinogen levels or perform serial fibrinogen measurements which may have provided insights into the mechanism of the reduced association with recurrent MACE in the acute phase. As included studies used independent protocols, laboratory assays were not standardised across studies. Future studies should validate our findings using standardised assays. The contribution of fibrinogen to recurrence risk may be in part due to its pro-thrombotic effects and may not entirely reflect a pro-inflammatory state.
Conclusion
Fibrinogen levels measured after ischaemic stroke or TIA were associated with recurrent major adverse cardiovascular events and recurrent stroke when measured in the post-acute setting, but not when measured in the first 14 days after stroke. Fibrinogen measurements might be useful to identify patients who are more likely to derive greater benefit from anti-inflammatory therapies after stroke. However, this hypothesis would need to be tested in future RCTs using a biomarker-led approach to patient selection.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241246489 – Supplemental material for Plasma fibrinogen and risk of vascular recurrence after ischaemic stroke: An individual participant and summary-level data meta-analysis of 11 prospective studies
Supplemental material, sj-docx-1-eso-10.1177_23969873241246489 for Plasma fibrinogen and risk of vascular recurrence after ischaemic stroke: An individual participant and summary-level data meta-analysis of 11 prospective studies by John J McCabe, Cathal Walsh, Sarah Gorey, Katie Harris, Pablo Hervella, Ramon Iglesias-Rey, Christina Jern, Linxin Li, Nobukazu Miyamoto, Joan Montaner, Annie Pedersen, Francisco Purroy, Peter M Rothwell, Catherine Sudlow, Yuji Ueno, Mikel Vicente-Pascual, William Whiteley, Mark Woodward and Peter J Kelly in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M. Woodward has done consultancy work for Amgen and Freeline. W. Whiteley has done consultancy work for Bayer and Viatris, data/safety monitoring for several clinical trials (ICAD-CATIS, TEMPO-2, PROTECT-U, CHOSEN, PAX-D, INTERACT-3), is a clinical lead for the Scotish Stroke Research Network, and received compensation from UK Courts for expert witness services. P.J. Kelly is the principal investigator of the CONVINCE trial. P.Rothwell reports compensation from Bristol-Myers Squibb for data and safety monitoring services; compensation from Abbott Vascular, Sanofi US Services Inc. and Bayer for consultant services.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought as this study was a systematic review.
Informed consent
Informed consent was not sought for the present study because this was a systematic review.
Trial registration
Not applicable as this study was a systematic review and did not require registration.
Guarantor
JMc
Contributorship
All authors contributed to drafting the manuscript and interpreting the results. M Woodward, C Walsh, J McCabe, and K Harris contributed to the statistical analysis. All authors contributed equally to study conception.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.