
Abstract
Introduction:
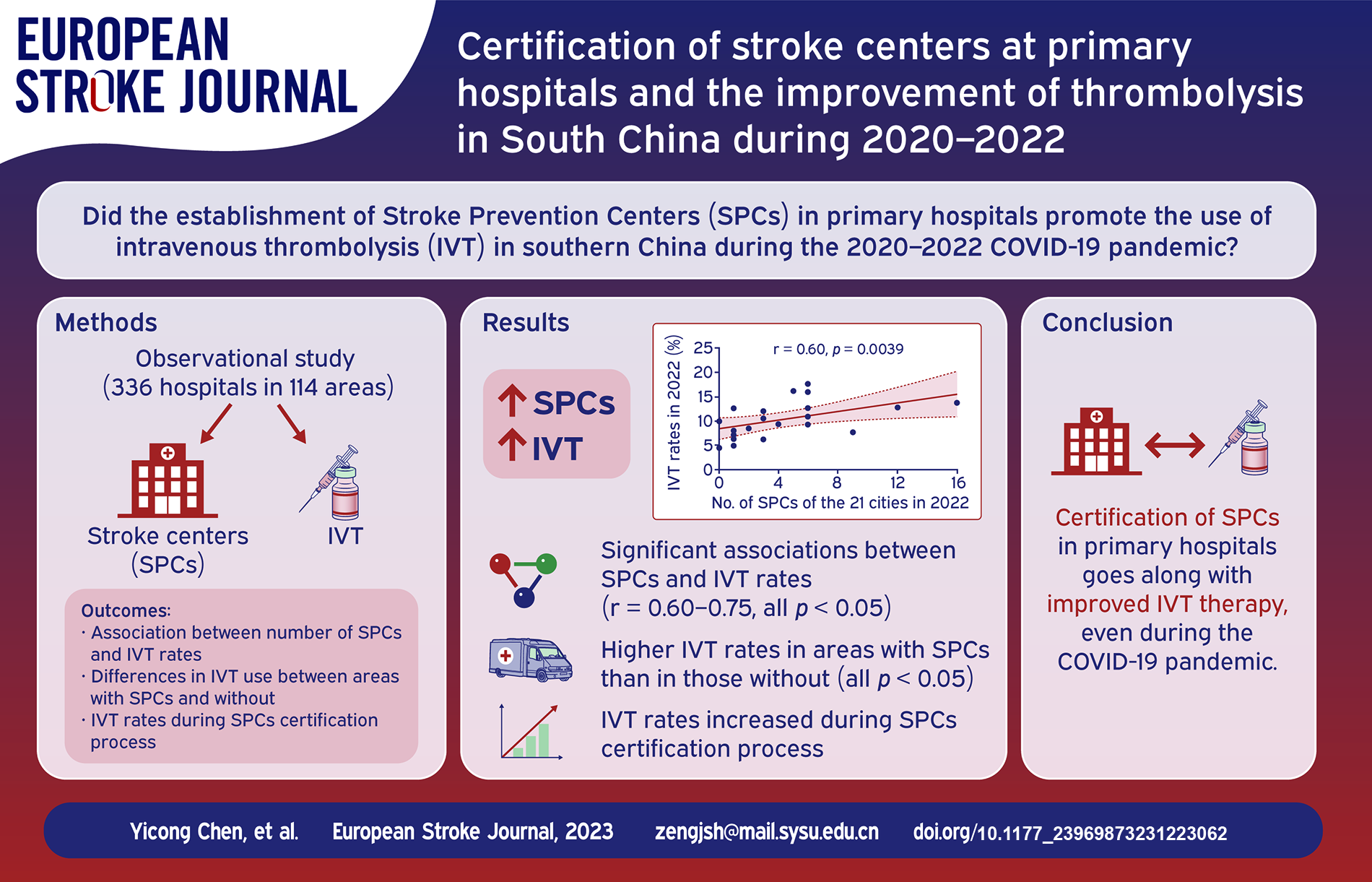
IVT use declined globally in 2020 due to the Corona Virus Disease 2019 (COVID-19) pandemic, but it increased in South China. This study was conducted to evaluate the association of establishing Stroke Prevention Centers (SPCs) at primary hospitals with IVT increase in South China.
Materials and methods:
We conducted a longitudinal observational study across 336 hospitals in 114 areas in South China during 2020–2022. Data regarding certified stroke centers, IVT volumes, and IVT rates were collected. Correlations between IVT rates and the number or density of stroke centers were accessed. IVT use was compared among areas with different levels of stroke centers or on different certification process.
Results:
During 2020–2022, there were 83, 125, and 152 stroke centers, with 26, 65, and 92 SPCs, respectively. IVT therapies were 12,795, 17,266, and 20,411, representing a 29.8% increase/year (all p < 0.001). IVT rates increased from 7.2% in 2020 to 8.8% and 10.4% in 2021 and 2022, demonstrating a 22.2% increase/year (all p < 0.001). IVT rates correlated with the number and density of SPCs (all p < 0.05). IVT rates were higher in areas equipped with SPCs than in those without stroke centers (all p < 0.05). IVT rates consistently increased during the SPC certification process from 1 year before through the certification and subsequent maintenance (both p < 0.05).
Discussion and conclusion:
Well-organised SPCs and IVT therapy demonstrated substantial increase during the 3-year period. Certification of SPCs at primary hospitals is associated with improved IVT therapy in South China even with city lockdown during COVID-19 pandemic.
Introduction
Well-organized stroke center care is associated with increased intravenous thrombolysis (IVT) therapy and improved neurological outcomes in patients with acute ischemic stroke (AIS) in developed countries.1–4 Stroke center certification was officially launched in China in 2015. The framework of stroke centers in China is divided into two levels, including Advanced Stroke Centers (ASCs, similar to Comprehensive Stroke Centers) and Stroke Prevention Centers (SPCs, similar to Primary Stroke Centers). 5 Guangdong Province is the most economically developed provinces in South China, but the use of IVT for AIS is limited. The certification of ASCs at large hospitals, carried out in Guangdong Province in 2016, resulted in a substantial increase in IVT rates from 2.0% to 6.1% during 2016–2019. 4 However, the IVT rates in Guangdong Province was still much lower than that in developed countries. Only 10%–20% of patients with stroke reach the hospital within 3 h in China. 6 The rapid transportation of rural residents with stroke symptoms to large ASCs in urban areas is difficult, and this was further magnified with the advent of the Corona Virus Disease 2019 (COVID-19) pandemic during 2020–2022 due to city lockdowns. In addition to prehospital delay, many medical centers, especially the primary hospitals in rural areas in Guangdong Province, were unable to accurately evaluate the severity of the condition and rapidly conduct acute reperfusion therapy for patients with AIS. The certification of SPCs began in Guangdong Province in 2019. 4 A global decline in IVT volumes (6.1% decline) has been reported during the first year of the COVID-19 pandemic.7,8 Interestingly, we found a sustained increase in IVT rates in Guangdong Province in the same period. 4 Nonetheless, the long-term effects of SPC certification on the use of IVT during the COVID-19 pandemic are unknown. The objective of this study was to report the stroke center certification and IVT utilization and evaluate the association between certified stroke center and estimated IVT rates in Guangdong Province during 2020–2022 with COVID-19 pandemic.
Methods
Study design
This was a longitudinal observational study evaluating the establishment of stroke centers and use of IVT in Guangdong Province during 2020–2022, and then assessing whether certification of SPCs was associated with promoting thrombolytic therapy. This study was approved by the Ethics Committee for Clinical Research and Animal Trials of the First Affiliated Hospital of Sun Yat-sen University.
Stroke center certification
The stroke center certification program was officially carried out in China in 2015. 5 Certification of stroke centers is the most import task of this program, and it also includes green channel construction, appropriate technical training, regional rescue assistance, and public education of stroke. 4 The framework of stroke centers in China is divided into two levels, ASCs and SPCs. 5 In Guangdong Province, the certification of ASCs and SPCs was launched in 2016 and 2019, respectively. 4 An ASC is required to be a tertiary care medical hospital with a completion of >60 cases of IVT annually, whereas an SPC is required to be a secondary care medical hospital (primary hospital) with a completion of >30 cases of IVT annually. 4 Detailed requirements for certifying ASCs and SPCs in China are provided in our previous study (Int J Stroke. 2022; 17: 559–565, Supplemental Text 1). Implementing thrombolytic therapy is a critical index for certification requirement and annual evaluation of ASCs and SPCs.
Data sources and variable assessment
Data were obtained from the database of patients with AIS receiving thrombolytic therapy with recombinant tissue plasminogen activator (rt-PA) in 336 hospitals distributed across 114 urban/rural areas in 21 cities in Guangdong Province from 2015 to 2022. We collected the numbers of patients receiving IVT with rt-PA, estimated the numbers of patients with AIS according to previous epidemiological survey data, 9 and then calculated the IVT rates during 2020–2022. The number of residents in Guangdong Province from 2020 to 2022 was obtained from the seventh National Population Census of China and CEI data (https://ceidata.cei.cn/; Supplemental Table S1). Stroke incidence was 197.3 per 100,000 person-years in Guangdong Province, with ischemic stroke accounting for 78.1%. 9 The number of patients with AIS was estimated by multiplying the number of residents by stroke incidence and the proportion of ischemic stroke. The estimated annual IVT rate was calculated as the number of patients with IVT divided by the number of patients with AIS in the corresponding year.
Data on certified ASCs and SPCs in Guangdong Province during 2020–2022 were obtained from the Stroke Prevention and Treatment Engineering Committee of the National Health Commission of the People’s Republic of China. We calculated the number of ASCs and SPCs at both the urban/rural areas and city levels. The density of ASCs/SPCs (per million people) was calculated as the number of ASCs/SPCs divided by the resident population in the corresponding year.
IVT volumes with IVT rates and certification of stroke centers in 2020 versus 2021 and in 2021 versus 2022 were compared, respectively. Correlations between IVT rates and the number or density of stroke centers (SPCs/ASCs) were assessed. Differences in IVT use were compared among 114 urban/rural areas with regard to the presence of three different levels of stroke centers (without stroke centers, with SPCs only, with ASCs only or ASCs plus SPCs). In addition, dynamic alterations in IVT utilization during the process of SPCs versus ASCs certification were evaluated.
Statistical analysis
The Kolmogorov–Smirnov formal test was used to assess data distribution. Categorical variables were presented as numbers with percentages, whereas continuous variables were presented as medians with interquartile ranges (IQR) because of their non-normal distribution. The Wilcoxon rank-sum test was used to compare the differences in IVT volumes, IVT rates, and number of certified stroke centers. The Kruskal–Wallis H test was used to assess the variations in IVT rates in areas with different levels of stroke centers and in the process of certification of SPCs/ASCs. Spearman’s correlation analysis was performed to analyze the correlation between IVT rates and the number or density of stroke centers. All statistical analyses were performed using SPSS 25.0 (SPSS Inc., Chicago, IL, USA). Significance level was set at p < 0.05.
Results
Stroke center certification
There were totally 83, 125, and 152 certified stroke centers during 2020–2022, representing a 41.6% increase/year (all p < 0.001, compared with that in 2020; Table 1). We observed this increase in the total number of stroke centers in both the rural and urban areas. The number of certified SPCs increased from 26 to 92, whereas that of certified ASCs only changed from 57 to 60 during 2020 to 2022. Of note, the number of SPCs exceeded that of ASCs in 2021 (65 vs 60) and 2022 (92 vs 60). A more rapid increase was detected in the number of certified SPCs than that of certified ASCs (per area increase: 0 [IQR 0–1] vs 0 [IQR 0–0]; p < 0.001). Moreover, the number of SPCs accounted for 87.5% (7/8), 94.1% (16/17), and 94.1% (16/17) in rural areas, respectively, whereas it only accounted for 25.3% (19/75), 45.4% (49/108), and 51.2% (62/121) in urban areas during 2020–2022, respectively (Figure 1).
Use of IVT and certification of stroke centers during 2020–2022.
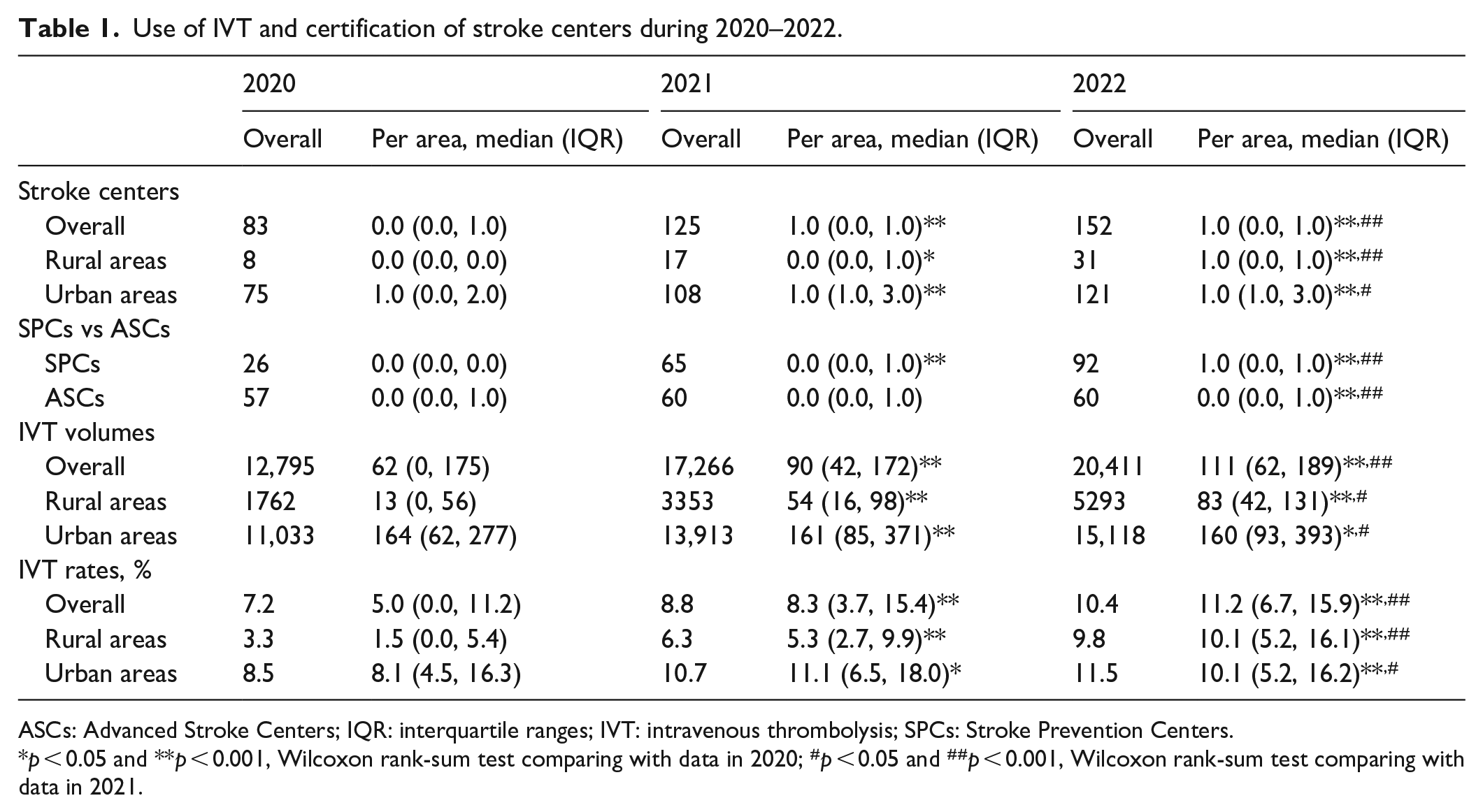
ASCs: Advanced Stroke Centers; IQR: interquartile ranges; IVT: intravenous thrombolysis; SPCs: Stroke Prevention Centers.
p < 0.05 and **p < 0.001, Wilcoxon rank-sum test comparing with data in 2020; #p < 0.05 and ##p < 0.001, Wilcoxon rank-sum test comparing with data in 2021.
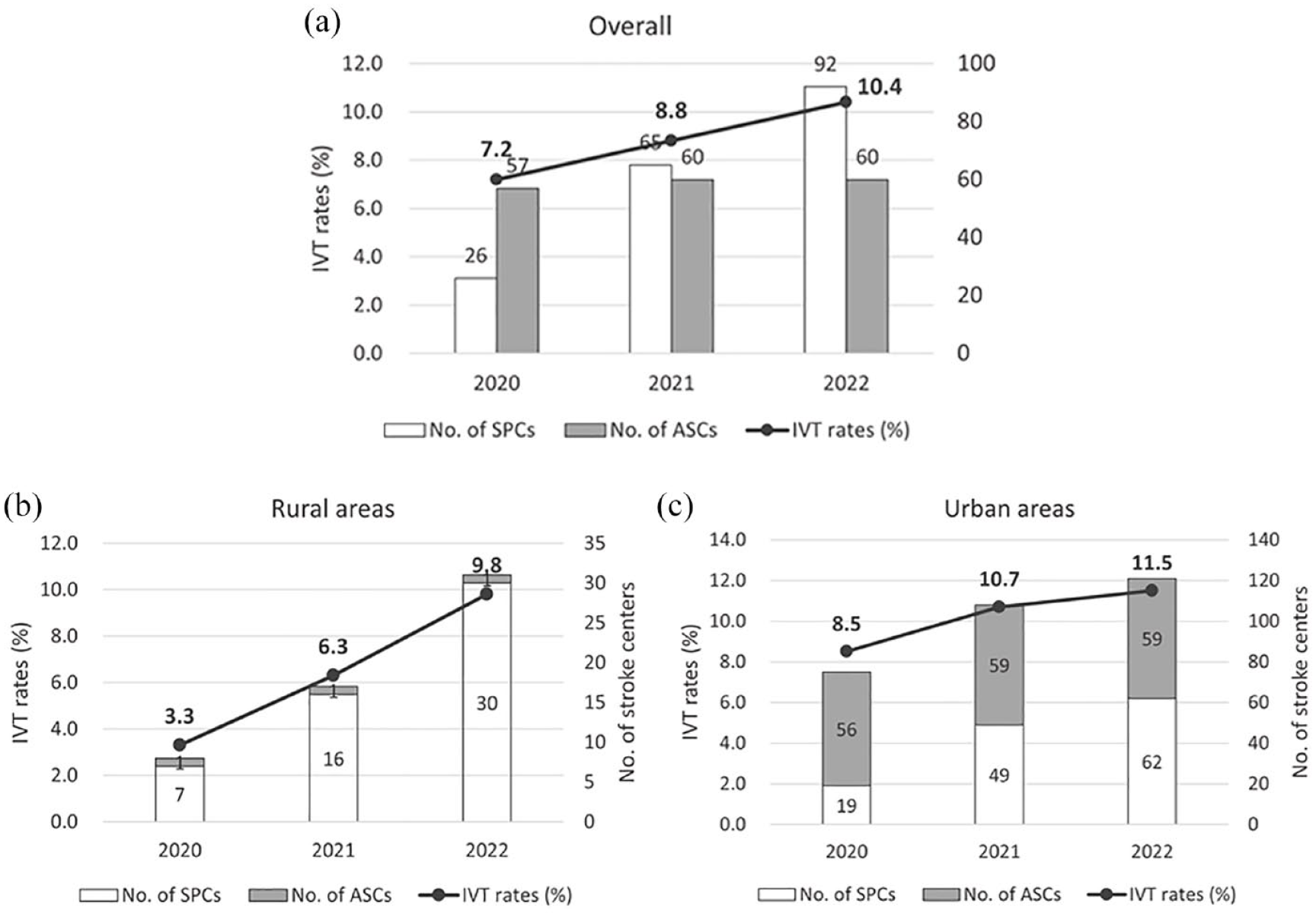
IVT rates and certification of stroke centers during 2020–2022: (a) overall, (b) rural areas, and (c) urban areas.
IVT use
We found that 12,795 (per area 62 [IQR 0–175]) IVTs with rt-PA were performed in 2020 compared with 17,266 (per area 90 [IQR 42–172]) in 2021 and 20,411 (per area 111 [IQR 62–189]) in 2022, representing a 29.8% increase/year (all p < 0.001, compared with that in 2020; Table 1). A significant increase in IVTs was observed in both rural and urban areas during 2020–2022 (all p < 0.05; Table 1). We detected a faster growth rate in IVT volumes in rural areas than that in urban areas (77.0% [IQR 21.0%–362.0%] vs 29.5% [IQR −7.3% to 75.5%], p = 0.011; Table 2).
Comparison of the IVT use in rural and urban areas in Guangdong Province during 2020–2022.
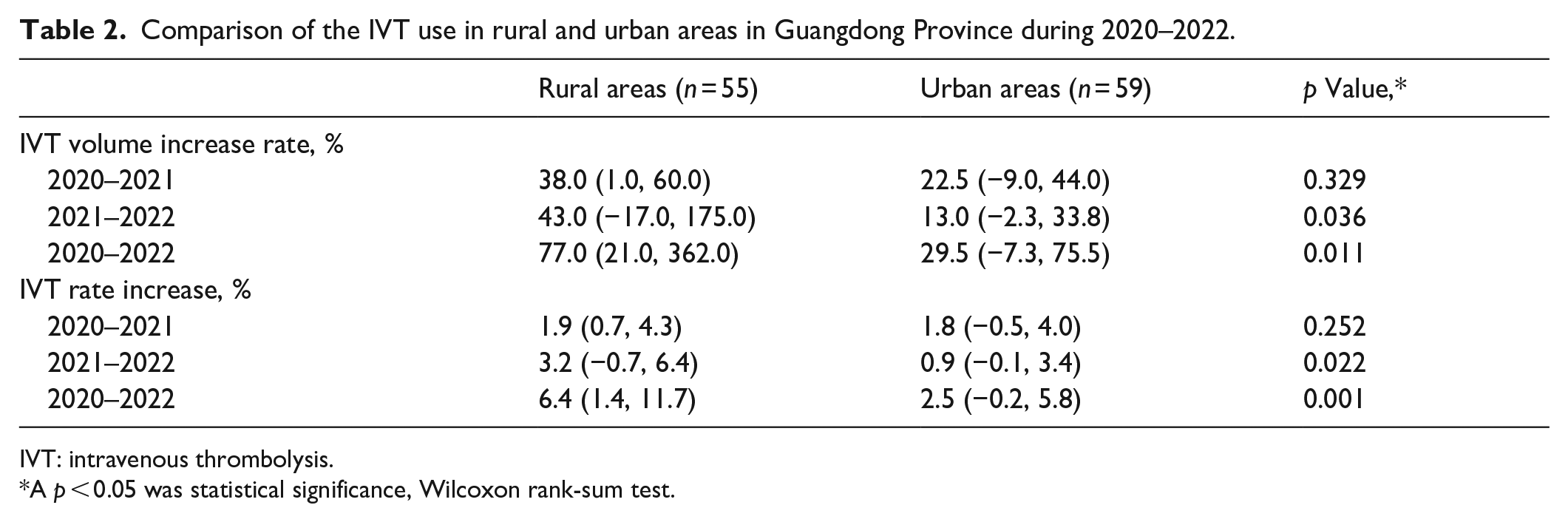
IVT: intravenous thrombolysis.
A p < 0.05 was statistical significance, Wilcoxon rank-sum test.
We further detected that annual IVT rates increased by 7.2% in 2020 versus 8.8% in 2021 versus 10.4% in 2022, demonstrating a 22.2% increase/year (all p < 0.001 compared with that in 2020; Table 1 and Figure 1(a)). In particular, the observed absolute increase in IVT rates was greater in rural areas than in urban areas (6.4% [IQR 1.4%–11.7%] vs 2.5% [IQR −0.2% to 5.8%], p = 0.001; Table 2 and Figure 1(b) and (c)), although an increase was observed in both rural and urban areas (all p < 0.05; Table 1).
Correlations between IVT and SPC certification
Significant correlations were identified between the increased IVT rates and number of SPCs during 2020–2022 (2020: r = 0.72, p = 0.0002; 2021: r = 0.66, p = 0.0011; and 2022: r = 0.60, p = 0.0039; Figure 2(a1)–(c1)). IVT rates were associated with the number of ASCs in 2020 (r = 0.44, p = 0.0462; Figure 2(a2)); however, these associations were not found in 2021 or 2022 (both p > 0.05; Figure 2(b2)–(c2)). Significant correlations were also observed between IVT rates and the density of SPCs from 2020 to 2022 (2020: r = 0.75, p < 0.0001; 2021: r = 0.69, p = 0.0005; and 2022: r = 0.75, p < 0.0001; Figure 2(a3)–(c3)), but not observed between IVT rates and the density of ASCs (both p > 0.05; Figure 2(a4)–(c4)).
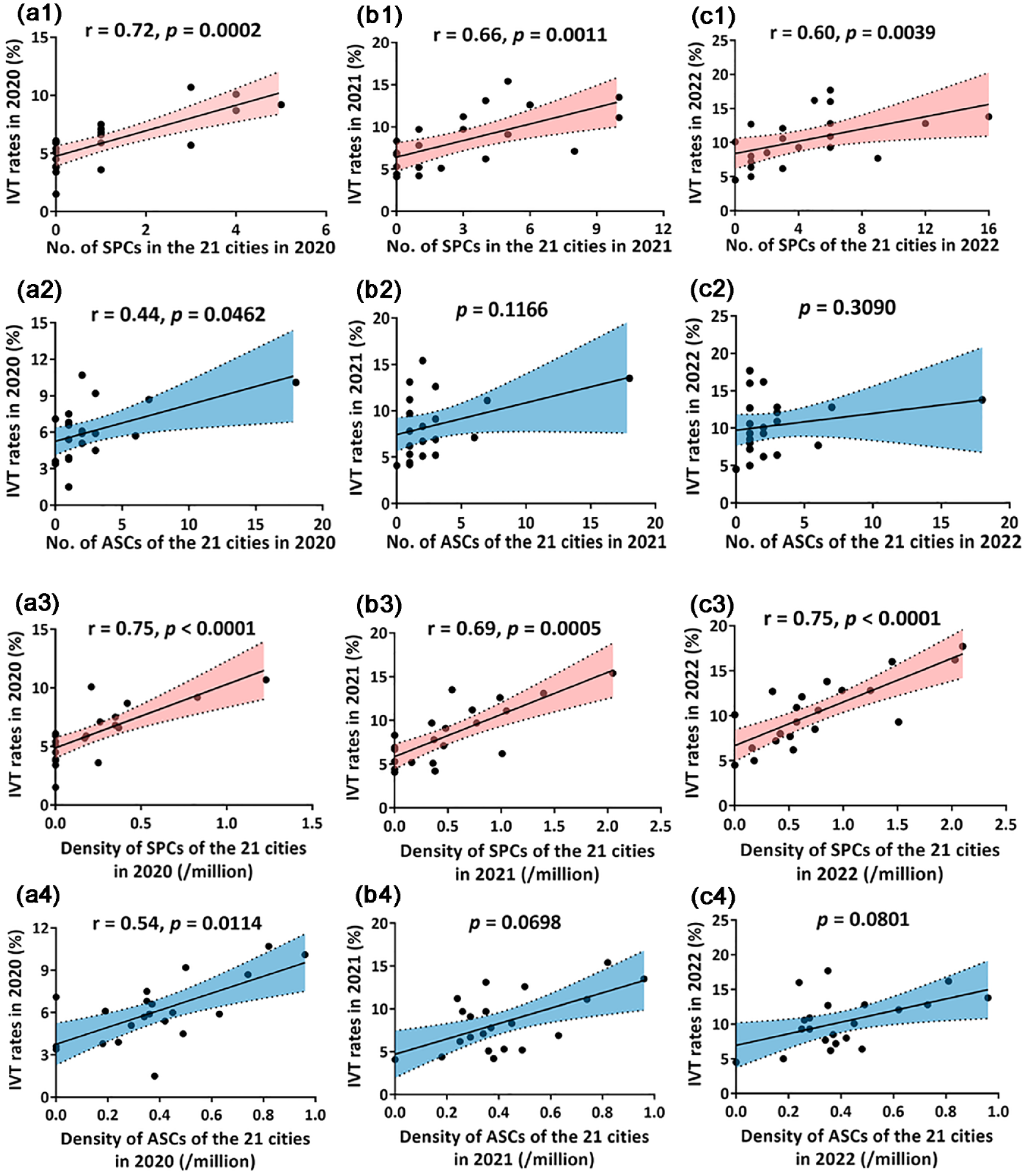
Correlations between IVT rates and the number/density of stroke centers during 2020–2022. (a1–c1) IVT rates and the number of SPCs; (a2–c2) IVT rates and the number of ASCs; (a3-c3) IVT rates and the density of SPCs; (a4–c4) IVT rates and the density of ASCs. Data was calculated with Spearman’s correlation analysis. r: correlation coefficient; p: p value. A p < 0.05 was statistical significance.
IVT in areas with different levels of stroke centers
We compared the use of IVT in 114 urban/rural areas with different levels of stroke centers (Table 3). The percentage of urban/rural areas without stroke centers declined from 57.9% (66/114) to 29.8% (34/114) during 2020–2022, whereas that of areas with SPCs only increased from 14.0% (16/114) to 40.4% (46/114). Remarkably higher IVT rates were observed in areas with SPCs only compared with those in areas without stroke centers during the 3-year period, representing absolute increases of 8.2% (9.7% vs 1.5%, p2 < 0.001), 5.0% (9.9% vs 4.9%, p2 < 0.001), and 3.5% (12.4% vs 8.9%, p2 = 0.005), respectively. However, we did not detect any differences in IVT rates in areas with SPCs only compared with those with ASCs only or ASCs plus SPCs during the 3-year period (all p3 ⩾ 0.05, Table 3). This non-difference was also consistent in areas with SPCs only compared with those with ASCs only (all p > 0.05; Supplemental Table S2). Moreover, we noticed that in rural areas dominated by SPCs, the use of IVT was evidently more frequent than those without SPCs (all p < 0.05; Supplemental Table S3).
Comparison of IVT rates in 114 urban/rural areas with stroke centers at different levels during 2020–2022.
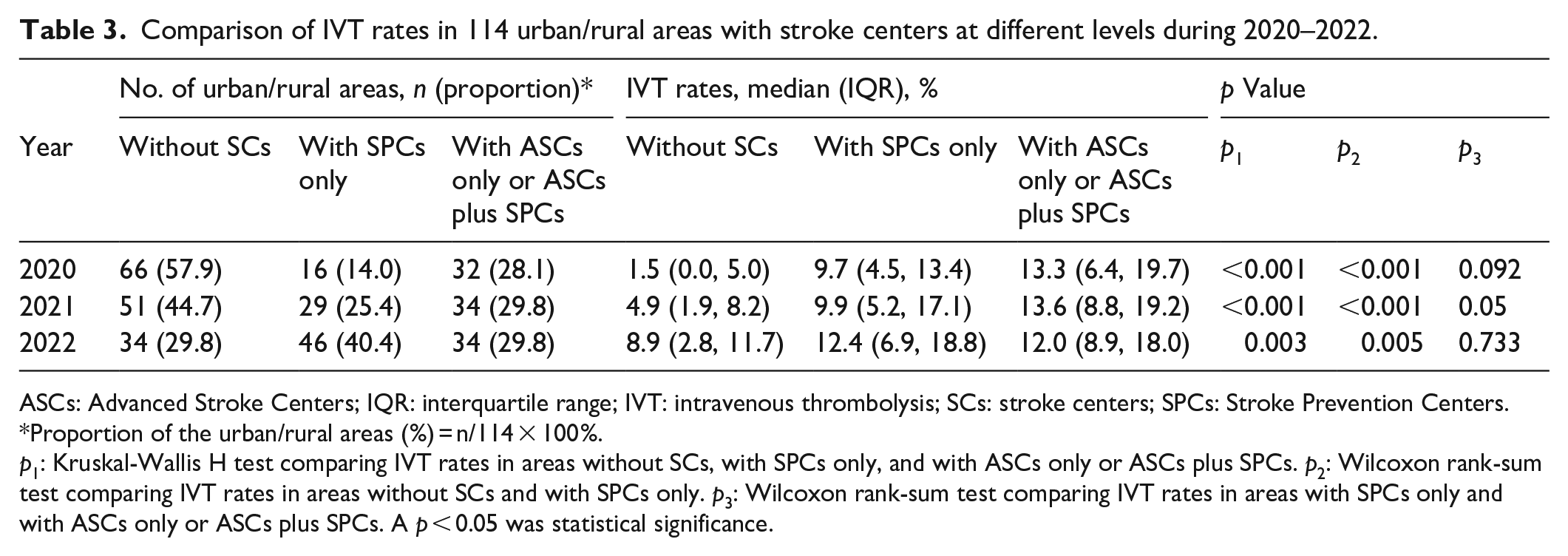
ASCs: Advanced Stroke Centers; IQR: interquartile range; IVT: intravenous thrombolysis; SCs: stroke centers; SPCs: Stroke Prevention Centers.
Proportion of the urban/rural areas (%) = n/114 × 100%.
p1: Kruskal-Wallis H test comparing IVT rates in areas without SCs, with SPCs only, and with ASCs only or ASCs plus SPCs. p2: Wilcoxon rank-sum test comparing IVT rates in areas without SCs and with SPCs only. p3: Wilcoxon rank-sum test comparing IVT rates in areas with SPCs only and with ASCs only or ASCs plus SPCs. A p < 0.05 was statistical significance.
IVT increased with SPC certification process
IVT rates in areas with SPCs only was 5.3% (IQR 1.8%–11.0%) 1 year prior to certification, similar to that in areas without stroke centers (3.4% [IQR 0.7%–8.1%], p = 0.155). IVT rates substantially increased in areas with newly stablished SPCs from 1 year before certification (5.3% [IQR 1.8%–11.0%]), through the certification year (10.4% [IQR 4.4%–14.7%], p = 0.012 vs 1 year before certification), and until 1 year after certification (12.9% [IQR 8.2%–19.9%], p = 0.042 vs the certification year; Figure 3(a)). However, this increase was not observed during the ASCs certification process (Figure 3(b)).
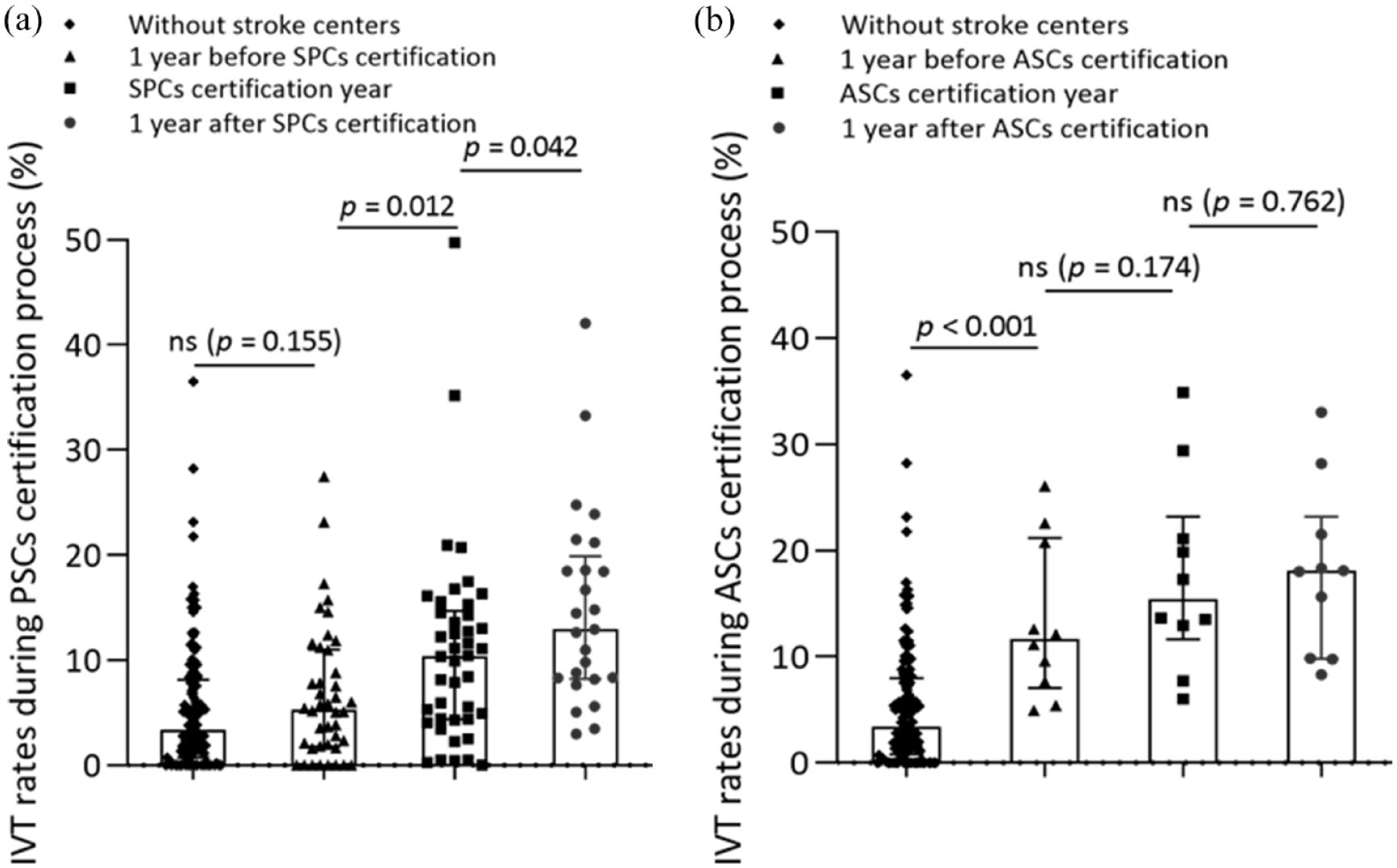
Utilization of IVT at the process of SPCs and ASCs certification during 2020–2022. (a) SPCs certification process. Data was comparing by Wilcoxon rank-sum test, a p < 0.05 was statistical significance. (b) ASCs certification process. Data was comparing by Wilcoxon rank-sum test, and a p < 0.05 was statistical significance.
Discussion
In this study, we observed a significant increase in certified stroke centers, IVT volumes, and IVT rates in Guangdong Province during 2020–2022. IVT rates were more relevant with the number and density of SPCs than that of ASCs during the 3-year period. Consistently, greater IVT use was conducted in areas equipped with SPCs than in those without. In addition, IVT rates have continuously increased in areas with SPCs from 1 year before through the certification process and subsequent maintenance. These results suggested the great contribution of SPC certification in the improvement of IVT in South China even with city lockdown during COVID-19 pandemic.
The use of IVT in China was limited; to address this, the stroke center certification program was officially launched in 2015. The types of stroke centers in China include ASCs (similar to Comprehensive Stroke Centers) and SPCs (similar to Primary Stroke Centers). 5 The first ASC in Guangdong Province was established in 2016, with a total of 40 certified ASCs (39/40 distributed in urban areas) functioning until 2019, resulting in an increase in IVT rates from 2.0% to 6.1% in the corresponding years. 4 However, the annual IVT rate in Guangdong Province remained low. Although Guangdong Province is the most developed province with the highest gross regional income in South China, a large part of its population resides in mountainous rural areas with less-developed healthcare services, which cannot be certified as ASCs. Only 10%–20% of patients with stroke reach hospitals within 3 h in China. 6 Notably, a total of 25.4% (29/114) areas did not conduct IVT with rt-PA in Guangdong Province in 2020. The possible reasons were as follows: (1) Most of these areas are remote rural areas, where low awareness of IVT and less accessible transportations delayed arrivals to hospitals for patients with stroke. (2) Limited medical resources and lack of a green channel for stroke resulted in longer in-hospital delays in these uncertified hospitals. (3) We only calculated the use of IVT with rt-PA in this study. Urokinase, which is also used for IVT in China, 10 is much cheaper than rt-PA, and some patients might choose urokinase instead of rt-PA due to economic capacity. Additionally, we could not exclude that some patients who went to hospitals in near areas with certified stroke centers instead of the local uncertified hospitals. Moreover, with the outbreak of COVID-19, city lockdowns and less accessible transportation restricted patients with stroke from admission to ASCs in the urban areas. In order to improve acute perfusion therapy in patients with AIS, establishing SPCs in local qualified hospitals was urgent.
The establishment of well-organized SPCs advocated IVT use. The establishment of a primary stroke center at a community hospital was demonstrated to substantially increase the proportion of patients receiving thrombolytic therapy for ischemic stroke. 11 Primary stroke center certification was associated with an overall improvement in the quality of stroke care, in addition to promoting the use of IVT.1,3,12–17 Besides, primary stroke centers were reported to have better performance in the procedural metrics for rt-PA administration than non-primary stroke centers in a large contemporary telestroke cohort.18,19 In China, certified SPCs are required to be secondary hospitals that can complete >30 cases/year of IVT with door-to-needle time (DNT) within 60 min.20,21 The certification of stroke centers in Guangdong Province remained ongoing from 2020 to 2022, resulting in an increase in the number of SPCs from 26 to 92 and an increase in that of ASCs from 57 to 60. A remarkable increase in IVT volumes and IVT rates was observed during 2020–2022. IVT rates were correlated more with the number and density of SPCs than with that of ASCs. In addition, areas equipped with certified SPCs demonstrated markedly higher IVT rates than those without. Moreover, the SPC certification process promoted a long-term increase in the use of IVT from 1 year before to 1 year after certification, while this increase was not obvious in the ASC certification process. As required by the standards of a certified SPC, a designed green channel and a fluent hospital workflow for stroke promote the administration of IVT.20,21 These findings demonstrate the significant contribution of certified SPCs to the improvement of IVT in Guangdong Province over the 3-year period.
The certification of SPCs played a more significant role in promoting IVT in rural areas than in urban areas. In Guangdong Province, a large population, mainly older adults, resides in mountainous rural areas equipped with less-developed healthcare services and medical teams not trained to deal with stroke. Moreover, it is difficult for mountainous residents to rapidly access medical or nonmedical transportation to tertiary hospitals in urban areas as soon as a stroke symptoms occur. 22 The annual IVT rates for AIS were <5% in 2019 in the rural west (Yangjiang, Maoming, and Zhanjiang) and northwest (Qingyuan and Zhaoqing) of Guangdong Province, 4 which were much lower than those in urban areas. IVT rates demonstrated a larger increase in rural (3.3%–9.8%) than urban (8.5%–11.5%) areas during 2020–2022. Besides, SPCs occupied increasingly higher proportions in the rural (87.5%–94.1%) than the urban (25.3%–51.2%) areas. These results suggest that the increasing designated SPCs was associated with the improvement of IVT in rural areas in Guangdong Province.
Establishing SPCs had a greater effect on the improvement of IVT during the COVID-19 pandemic. The COVID-19 pandemic overwhelmed the healthcare system and exhausted the medical resources worldwide, raising a huge challenge for the administration of IVT for stroke. 8 Globally, IVT volumes remarkably declined by 6.1% in the first year of the COVID-19 pandemic compared with the previous year.7,8,23,24 Centers with high volumes of patients with COVID-19 had greater decreases in the volume of admissions of patients with stroke compared with those with low volumes of patients with COVID-19. 7 In China, a 48.9% and 24.7% reduction in IVTs for stroke was observed in Wuhan 25 and Wenzhou, 26 respectively, during the first wave of the COVID-19 pandemic in 2020. City lockdowns and less accessible transportation caused the admission of more patients with stroke to local hospitals, especially if the initial stroke symptoms were mild. 25 Interestingly, as shown in our recent study, IVT volumes and rates consistently increased in Guangdong Province in 2020. 4 Guangdong Province was one of the most severely affected provinces by COVID-19 in China (secondary to Wuhan and Shanghai), 27 and city lockdowns were implemented. 27 A global shift from larger to lower volumes of admission of patients with stroke was reported during the pandemic.7,8 In Guangdong Province, a higher number of patients with AIS arrived at the hospital within 3 h of onset in rural compared with that in urban areas (14.2% vs 12.7%) in 2020. 28 This put a heavy burden on local hospitals with respect to medical resources for stroke care and to perform acute perfusion therapy. However, a shortage of stroke team members, a slow-down in evaluations, and practicing precautionary procedures during the pandemic might have excluded some stroke admissions with a tense time window from thrombolytic therapy.25,26,29 The COVID-19 pandemic also prolonged the DNT and caused worse functional outcomes for patients with stroke who received IVT.25,26,30 Interestingly, a substantial increase in volume and annual rates in IVT as well as the number of certified SPCs were observed in Guangdong Province over the 3-year period of the pandemic. These findings emphasize the significance of advocating for SPCs, presenting a successful framework for stroke care under demanding social conditions.
This study had a few limitations. Although we robustly showed the variation in IVT during 2020–2022, our study did not provide data regarding intracranial hemorrhage or interventions of mechanical thrombectomy, as the pandemic also influenced their volumes.7,8 We also could not analyze the impact of SPC certification on overall stroke care, such as the DNT of thrombolysis, intracranial hemorrhage transformation, and patient outcomes, due to population-level data. Owing to an observational design, the observed increase in IVT use may also be influenced by other confounding factors, such as publication education of stroke, appropriate technical training, and regional rescue system construction in these years. This observational study was a hypothesis generating study, and identified an association but not a causal relationship. Moreover, we acknowledge that apart from the dynamic changes of stroke incidence itself, the COVID-19 pandemic and its mortality rate could also modify the incidence of stroke. Considering the lack of exact data regarding stroke incidence during 2020–2022, we used the data based on the latest and largest epidemiological investigation of stroke in China. 9 Prospective studies are needed to evaluate the effects of certified SPCs on overall stroke care and long-term prognosis.
Conclusions
Stroke centers (especially SPCs) and IVT use were substantially increased in Guangdong Province during 2020–2022. IVT rates were significantly associated with the number and density of SPCs instead of ASCs. Areas equipped with SPCs showed greater IVT use than those without, demonstrating a continuous increase in IVT rates during the certification process. Establishing SPCs at primary hospitals is associated with promotion of IVT use in South China even during the COVID-19 pandemic.
Supplemental Material
sj-docx-1-eso-10.1177_23969873231223062 – Supplemental material for Certification of stroke centers at primary hospitals and the improvement of thrombolysis n South China during 2020–2022
Supplemental material, sj-docx-1-eso-10.1177_23969873231223062 for Certification of stroke centers at primary hospitals and the improvement of thrombolysis n South China during 2020–2022 by Yicong Chen, Qingfeng Lei, Jiaoxing Li, Jianle Li, Yinxin He, Jingjing Li, Shihui Xing, Yuhua Fan and Jinsheng Zeng in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Natural Science Foundation of China (82130035, 81971103, 82371308), the Basic and Applied Basic Research Foundation Natural Science Foundation of Guangdong Province (2021A1515012216), Sun Yat-sen University Clinical Research 5010 Program (2018001), the Kelin Star Talent Support Program of the First Affiliated Hospital, Sun Yat-sen University (R08014), the Guangdong Provincial Key Laboratory of Diagnosis and Treatment of Major Neurological Diseases (2020B1212060017), Guangdong Provincial Clinical Research Center for Neurological Diseases (2020B1111170002), Guangdong Province International Cooperation Base for Early Intervention and Functional Rehabilitation of Neurological Diseases (2020A0505020004), Guangdong Provincial Engineering Center for Major Neurological Disease Treatment, Guangdong Provincial Translational Medicine Innovation Platform for Diagnosis and Treatment of Major Neurological Disease, Guangzhou Clinical Research and Translational Center for Major Neurological Diseases (201604020010).
Ethical approval
This study was approved by the Ethics Committee for Clinical Research and Animal Trials of the First Affiliated Hospital of Sun Yat-sen University.
Informed consent
Not suitable.
Guarantor
Jinsheng Zeng
Contributorship
YC, QF, and JS researched literature and conceived the study. YC, QF, JX, and JL were involved in protocol development, gaining ethical approval, data collection, and data analysis. YC and QF wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.