
Abstract
Introduction:
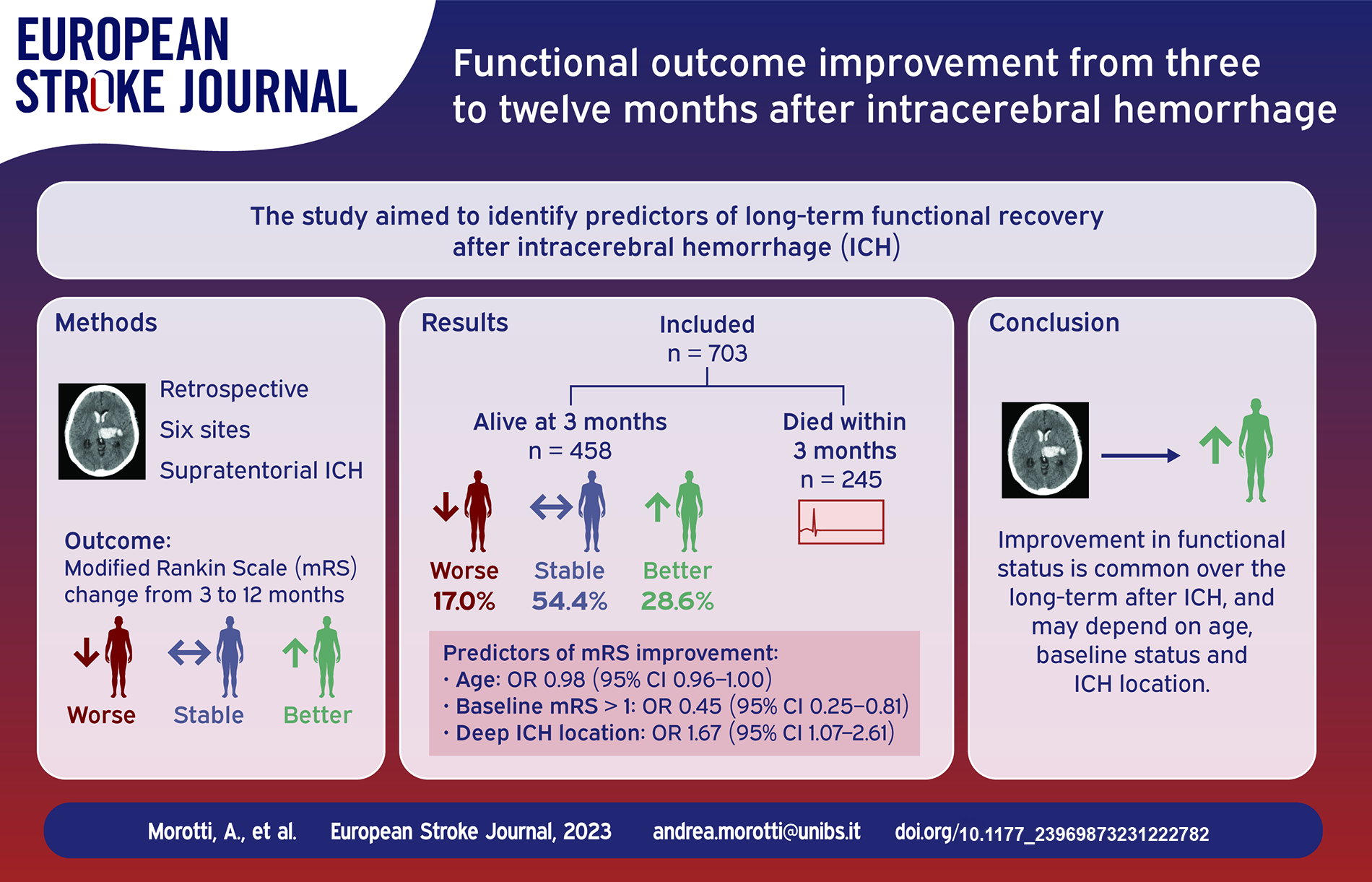
Most intracerebral hemorrhage (ICH) trials assessed outcome at 3 months but the recovery trajectory of ICH survivors may continue up to 1 year after the index event. We aimed to describe the predictors of functional outcome improvement from 3 to 12 months after ICH.
Materials and Methods:
Retrospective analysis of patients admitted to six European Stroke Centers for supratentorial ICH. Functional outcome was measured with the modified Rankin Scale (mRS) at 3 and 12 months. Predictors of functional outcome improvement were explored with binary logistic regression.
Results:
We included 703 patients, of whom 245 (34.9%) died within 3 months. Among survivors, 131 (28.6%) had an mRS improvement, 78 (17.0%) had a worse mRS and 249 (54.4%) had a stable functional status at 12 months. Older age and the presence of baseline disability (defined as pre-stroke mRS > 1), were associated with lower odds of functional outcome improvement (Odds Ratio (OR) 0.98 per year increase, 95% Confidence Interval (CI) 0.96–1.00, p = 0.017 and OR 0.45, 95% CI 0.25–0.81, p = 0.008 respectively). Conversely, deep ICH location increased the probability of long term mRS improvement (OR 1.67, 95% CI, 1.07–2.61, p = 0.023). Patients with mild-moderate disability at 3 months (mRS 2–3) had the highest odds of improvement at 12 months (OR 8.76, 95% CI 3.68–20.86, p < 0.001).
Discussion and Conclusion:
Long term recovery is common after ICH and associated with age, baseline functional status, mRS at 3 months and hematoma location. Our findings might inform future trials and improve long-term prognostication in clinical practice.
Introduction
Intracerebral hemorrhage (ICH) is a major cause of death and disability worldwide.1,2 Following ischemic stroke, the majority of ICH randomized controlled trials (RCT) assessed functional outcome at 3 months from the index event. 3 However, recent evidence suggested that the recovery trajectory of ICH patients is longer than ischemic stroke and a significant proportion of patients surviving the acute phase experience long term functional outcome improvement.4,5 The characteristics of ICH patients experiencing functional recovery beyond 3 months from the index event remain unclear. The aim of this study was to describe the frequency and predictors of functional outcome improvement from 3 to 12 months after acute ICH.
Methods
All the study procedures were approved by the local authorities at each participating institution: Arcispedale S. Anna, Ferrara, Italy (PN 26032009-15122011); IRCCS Mondino Foundation, Pavia, Italy (PN 0035588/22); ASST Spedali Civili, Brescia, Italy (PN 4067-08052020); IRCCS Istituto delle Scienze Neurologiche, Bologna, Italy (DL 196/2003); Charitè Hospital, Berlin, Germany (PN EA1/035/20) and University of Perugia/Azienda Ospedaliera Santa Maria Della Misericordia (DL 196/2003). Written informed consent was obtained by patients or caregivers, or waived by the Institutional Review Boards. Requests to access the dataset may be sent to the corresponding author.
Study population
Non-consecutive patients admitted for primary spontaneous non-traumatic ICH at six sites in Italy and Germany were retrospectively selected from ongoing ICH registries. For the present analysis patients were selected using the following inclusion criteria: (1) Supratentorial ICH, (2) age ⩾ 18, (3) availability of modified Rankin Scale (mRS) at 3 and 12 months. The main exclusion criteria were: (1) secondary ICH from traumatic brain injury or other intracranial disease ICH and (2) infratentorial ICH.
All participating sites were tertiary stroke centers with intensive care unit and neurosurgery availability, admitting unselected stroke patients, directly presented to the stroke hub or transferred from spoke sites.
Clinical and imaging variables
Demographics, history of hypertension, antithrombotic treatment, admission Glasgow Coma Scale score (GCS) and pre-stroke functional status were collected. Baseline disability before the index ICH was defined as mRS > 1. Functional outcome (mRS) at 3 and 12 months from the index event was assessed through follow-up telephone calls, outpatient service evaluations or querying the national social security databases only for mortality data in a minority of the included cases (two sites, <10% of the included population). All the mRS evaluations were performed by trained, blinded investigators.
All patients underwent baseline non-contrast CT scans and the imaging analysis included ICH volume calculation (semi-automated, computer-assisted planimetric softwares), intraventricular hemorrhage (IVH) presence and ICH location, classified as supratentorial lobar and deep. 6
Statistical analysis
Categorical variables were summarized as count (percentage) and compared with the χ2 test. Continuous variables were expressed as median (interquartile range, IQR) and compared using the Kruskal-Wallis test. The main analyses focused on patients alive at 3 months and the outcome of interest was any mRS improvement (⩾1 point mRS decrease) from 3 to 12 months. Predictors of mRS improvement were explored with multivariable binary logistic regression, including age, baseline ICH volume, admission GCS, IVH presence and variables with p < 0.1 in univariate analysis.3,7 We performed multiple secondary analyses. First, the main logistic regression model was repeated excluding patients with mRS = 0 at 3 months. Second, descriptive and logistic regression analyses were stratified by ICH location (deep vs lobar supratentorial ICH). Third, the mRS at 3 months, analyzed as a continuous variable, was included in the logistic regression model. Fourth, logistic regression model was repeated dividing the study population in three groups, based on the degree of disability at 3 months: none (mRS 0–1), mild/moderate (mRS 2–3) and severe (mRS 4–5) disability. 8 Every subject’s predicted probability of outcome improvement was calculated based on logistic regression estimates and expressed as a continuous variable ranging from 0 to 1. Fifth, the same predicted probability analysis was repeated excluding patients with mRS 0–1 at 3 months. Finally, we also explored the predictors of functional outcome worsening.
All the analyses were performed with SPSS version 21.0 (www.spss.com) and statistical significance was set at p < 0.05.
Results
We included 703 patients, of whom 245 (34.9%) died within 3 months. Table 1 illustrates the study population general characteristics and the cohort selection flowchart is illustrated in Figure 1. Excluded patients were younger, had lower GCS, higher rates of anticoagulant treatment and were less frequently on antiplatelet medications. The comparison between included and excluded patients is reported in detail in eTable 1.
Comparison between patients with mRS worsening, stability and improvement.
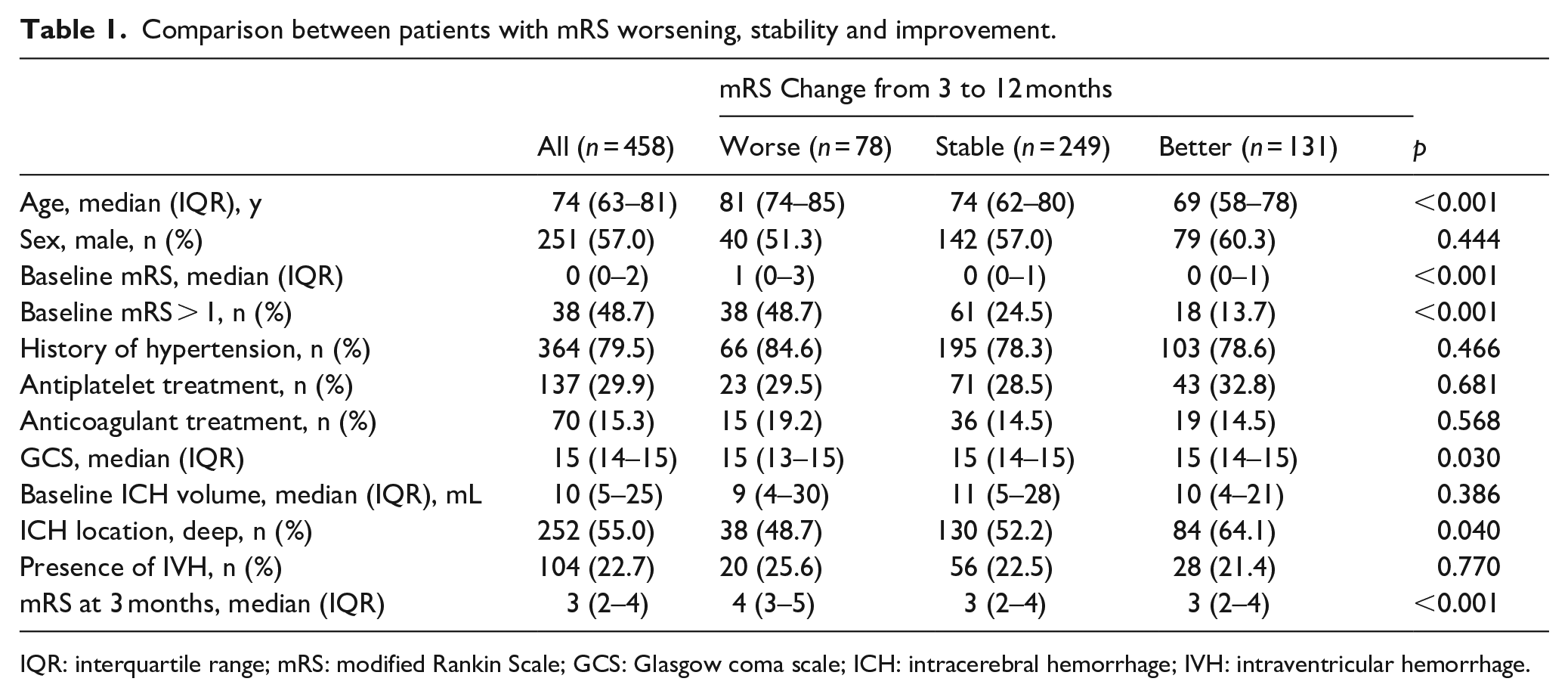
IQR: interquartile range; mRS: modified Rankin Scale; GCS: Glasgow coma scale; ICH: intracerebral hemorrhage; IVH: intraventricular hemorrhage.
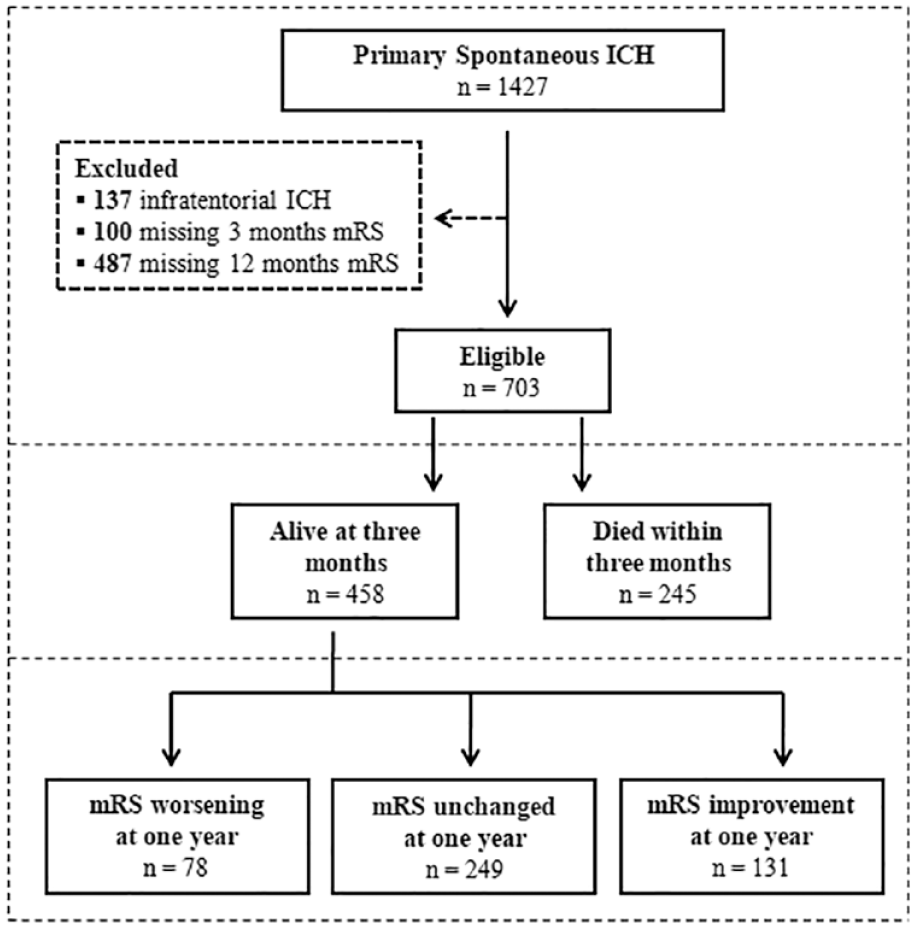
Selection flowchart.
Among patients alive at 3 months, 131 (28.6%) experienced long term mRS improvement whereas 78 (17.0%) had a worse mRS at 1 year and 249 (54.4%) maintained a stable functional status. Patients with mRS improvement were younger, had lower mRS before ICH and had more frequently deep hemorrhages, as shown in Table 1. Baseline, 3 and 12 months mRS distribution was similar between deep and lobar hemorrhages (all p for comparison > 0.1). Grotta bars showing the mRS distribution at 3 and 12 months in the entire population is shown in Figure 2 whereas the same analysis stratified by ICH location is reported in eFigure 1.
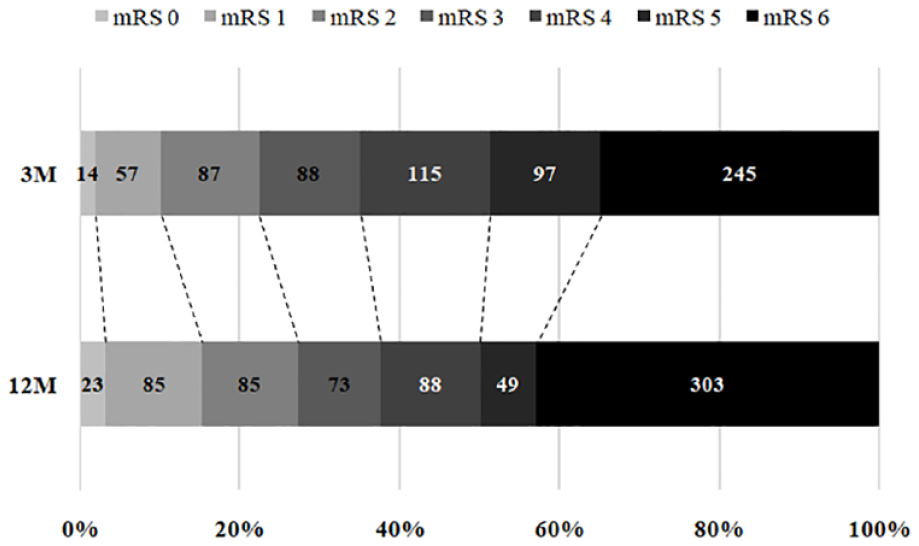
Grotta Bars showing mRS changes from 3 to 12 months.
Full raw data on functional outcome changes are reported in Table 2 for the entire population and in eTable 2 and 3 stratified by ICH location.
Functional outcome improvement stratified by 3 months outcome.
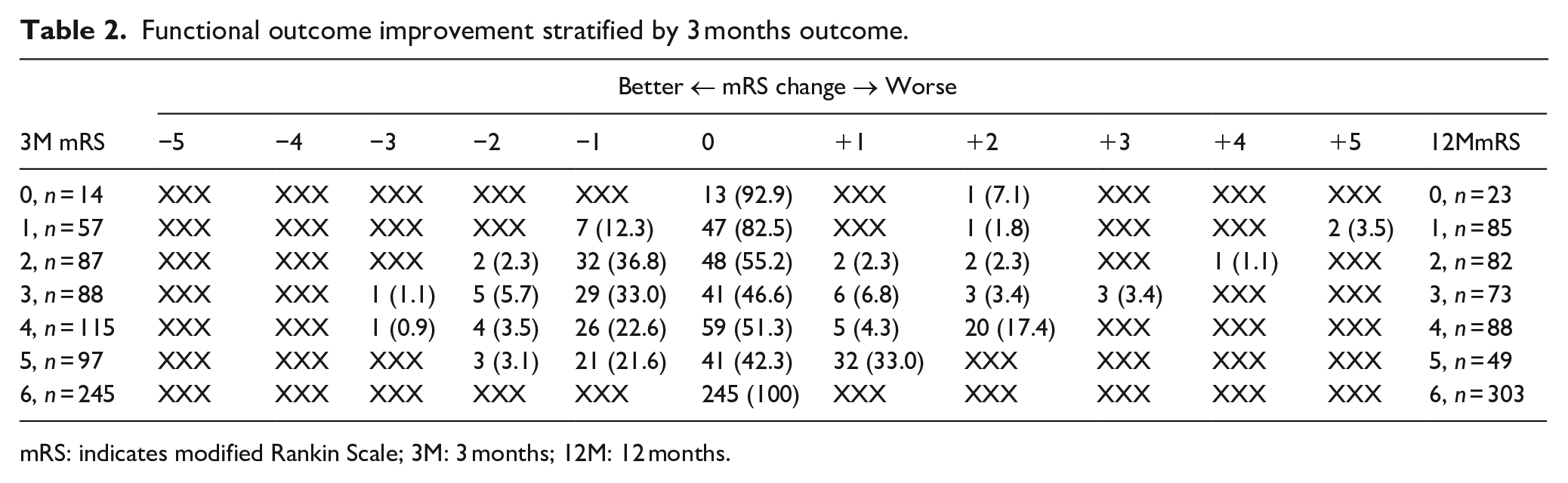
mRS: indicates modified Rankin Scale; 3M: 3 months; 12M: 12 months.
Table 3 illustrates the results of logistic regression. Older age and the presence of baseline disability (defined as pre-stroke mRS > 1), were associated with lower odds of functional outcome improvement (Odds Ratio (OR) 0.98 per year increase, 95% Confidence Interval (CI) 0.96–1.00, p = 0.017 and OR 0.45, 95% CI 0.25–0.81, p = 0.008 respectively). Conversely, patients with deep ICH had higher odds of long term mRS improvement (OR, 1.67, 95% CI, 1.07–2.61, p = 0.023). ICH volume and other acute phase severity indications such as GCS and IVH presence were not associated with mRS long term trajectory.
Predictors of functional outcome improvement from 3 to 12 months.
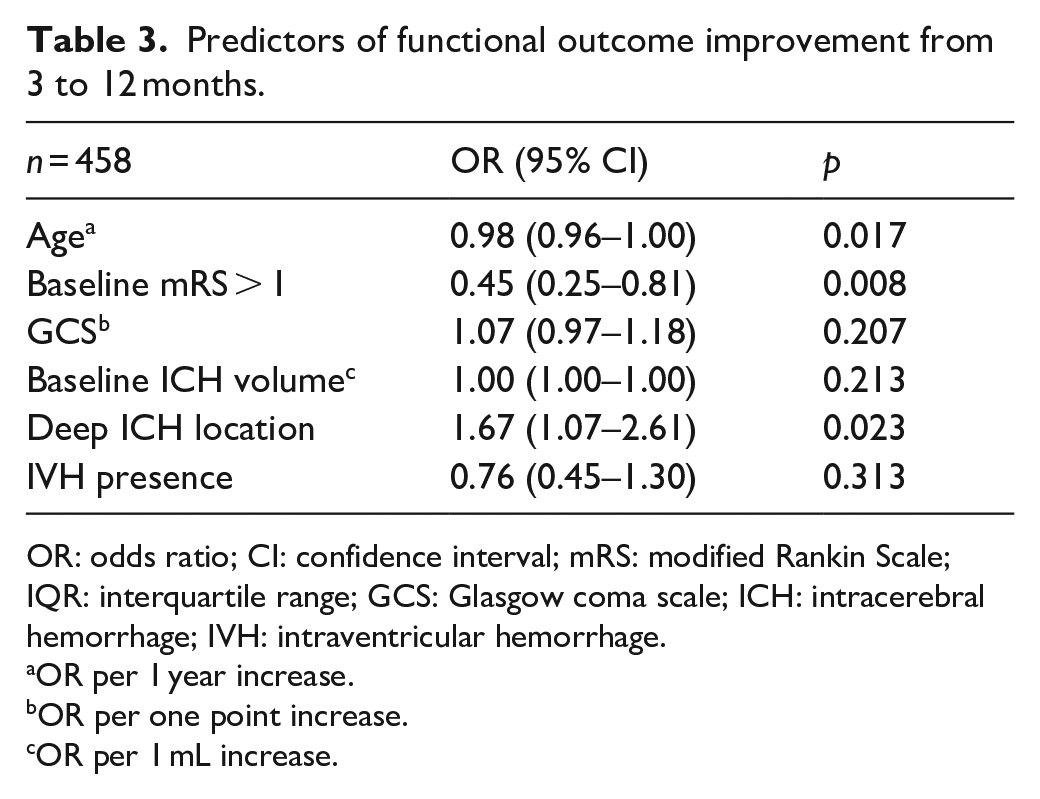
OR: odds ratio; CI: confidence interval; mRS: modified Rankin Scale; IQR: interquartile range; GCS: Glasgow coma scale; ICH: intracerebral hemorrhage; IVH: intraventricular hemorrhage.
OR per 1 year increase.
OR per one point increase.
OR per 1 mL increase.
These findings were confirmed in a sensitivity analysis excluding patients with mRS = 0 at 90 days, as reported in eTable 4. When the logistic regression model was stratified by location, age was the only predictor of improvement in deep ICH whereas baseline disability was independently associated with functional outcome recovery only in lobar bleedings, as reported in eTable 5.
Secondary analyses showed that the mRS at 3 months was directly and independently associated with the probability of improvement at 12 months (OR 1. 36, 95% CI 1.14–63, p < 0.001). However, the association between 3 months outcome and outcome improvement was not linear, as patients wild mild-moderate disability (mRS = 2–3) at 3 months had the higher frequency of long term functional outcome improvement (39.1% and 39.8% respectively, p < 0.001). This finding was confirmed in logistic regression (mRS = 0–1, Reference; mRS 2–3, OR OR 8.76, 95% CI 3.68–20.86, p < 0.001; mRS 4–5, OR 7.05, 95% 2.84–17.51, p < 0.001). The predicted probability of outcome improvement at 12 months, stratified by 3 months outcome is illustrated in Figure 3.
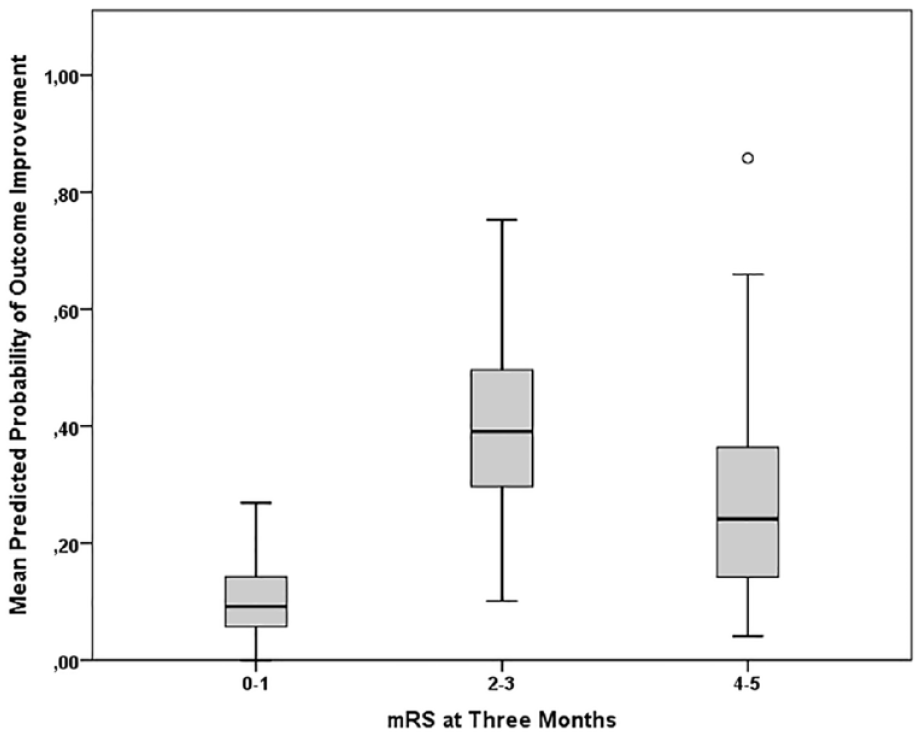
Predicted Probability of Outcome Improvement from 3 to 12 months after ICH.
This finding was confirmed after the exclusion of subjects with mRS 0–1 at 3 months (the mean predicted probability of functional outcome improvement was 39.4% in subjects with 3 months mRS 2–3 vs 25.9% in those with mRS 4–5 at 3 months, p = 0.005).
Finally, logistic regression with mRS worsening as the outcome of interest showed a direct association with advanced age and baseline disability and an inverse relationship with admission GCS, as reported in eTable 6.
Discussion
Functional outcome improvement at 1 year was common in our ICH cohort and occurred in more than one in four of patients alive at 3 months. Age, baseline mRS and ICH location were the main predictors of long term outcome improvement in our analysis. Functional outcome at 3 months was also directly associated with the probability of future recovery. However, the association between mRS at 3 months and improvement at 12 months was not linear, as the highest odds of recovery were observed in patients with intermediate degrees of disability.
The lower frequency of mRS improvement in older patients with higher baseline disability appears intuitive, as these patients have probably less room for recovery and might be at higher risk of functional decline and new events outside the acute phase. 9 Similar mechanisms might explain the observed highest odds of functional outcome amelioration in patients with moderate disability at 3 months. On one hand, these subjects have more room for future improvement compared with patients who have already achieved functional independence at 3 months. On the other hand, patients with severe disability at 3 months might be more likely to suffer from long term secondary complications and future functional decline.9,10
Conversely, the mechanisms underlying the relationship between deep ICH location and higher chances of mRS improvement remain unclear. This finding might simply reflect and interaction between age, baseline status and ICH location. However, the association between deep location and long term functional outcome improvement remained significant when accounting for these potential confounders. Differences in short term outcome might also explain the location-specific heterogeneity in long term recovery. Previous studies reported higher chances of better functional outcome at 3 months in lobar ICH and these patients might therefore have less room for further improvement at 1 year from the index event. 11 However, our findings do not support this hypothesis, as we did not observe significant mRS differences between deep and lobar ICH at all time points. Another possible, hypothesis generating explanation is that the different cerebral small vessel disease underlying deep and lobar ICH, might influence functional recovery after ICH. 12 Lobar ICH survivors might also be at higher risk of future functional outcome decline because of a greater incidence of ICH recurrence and cognitive impairment compared to deep ICH.1,9,13
Logistic regression stratified by ICH location showed a potential heterogeneity in predictors of functional outcome improvement, with age predicting functional recovery only in deep ICH and baseline disability only in lobar ICH. This finding might suggest the presence of different biological mechanisms of recovery, according to ICH location and underlying cerebral small vessel disease. An alternative, easier explanation to justify this finding is the limited statistical power in secondary analyses, because of the relatively small number of patients with the outcome of interest.
Another interesting finding of our study is the lack of association between acute phase severity indicators and mRS change from 3 to 12 months. This result is indirectly consistent with a recent analysis, showing that also patients with severe ICH have fair chances of good long term functional outcome if they survive the acute phase. 4
In a secondary analysis we explored predictors of long term functional outcome deterioration. Older age and baseline disability were directly associated with the risk of outcome worsening. Conversely, higher GCS was independently associated with reduced risk of outcome deterioration. The underlying mechanisms are still unclear. We hypothesize that patients with higher levels of consciousness might be more likely to actively engage in rehabilitative therapies and less prone to secondary complications, infections in particular.14,15
Our findings might have implications for clinical practice and future research. The observed high frequency of long term functional outcome improvement indirectly supports the recommendation for delayed prognostication and full medical support in acute ICH.3–5 Functional outcome after ICH should be evaluated beyond 3 months in future randomized trials, accounting for potential influencing factors such as ICH location. Additionally, it might be valuable to retrospectively assess the results of previous randomized trials that limited outcome assessment to the first months after onset. Finally, ICH prognostication should rely not only on acute phase severity indicators but also incorporate other factors that might impact long term recovery. 7
Some limitations should be acknowledged. First, around half of the screened patients were excluded, mainly for missing data on functional outcome, raising the possibility of selection bias and limiting generalizability. 16 Second, we were unable to evaluate and adjust our analyses for medical complications outside the acute phase, rehabilitation duration, intensity and quality. 14 Furthermore, other events not accounted for in our analysis might have influenced functional recovery, such as brain frailty, social support and cerebral small vessel disease pattern and burden.4,17,18 Third, we had no data on quality of life and patient-reported outcome measures. 19 Fourth, we were unable to provide a more granular classification of deeply located hemorrhages, in particular to identify patients with thalamic ICH that might have a higher risk of IVH and more severe prognosis. 20 Fifth, a higher risk of recurrence in lobar hemorrhages might explain the interaction between ICH location and the recovery trajectory and we were unable to account for this potential underlying mechanism. 21
Finally, the limited number of levels might make the mRS less sensitive to changes than other stroke outcome measurement tools. 22 Our findings are therefore best interpreted as hypothesis generating, warranting further investigations to characterize the underlying pathophyisiology.
Conclusion
More than one in four ICH patients alive at 3 months experience long term functional outcome improvement. Baseline disability and age were inversely associated with recovery whereas patients with deep bleedings had higher chances of better outcome at 1 year. The highest rates of long term functional recovery were observed in patients with moderate disability at 3 months from the index ICH. Our results might have implications for clinical practice and inform the design of future RCT.
Supplemental Material
sj-docx-1-eso-10.1177_23969873231222782 – Supplemental material for Functional outcome improvement from 3 to 12 months after intracerebral hemorrhage
Supplemental material, sj-docx-1-eso-10.1177_23969873231222782 for Functional outcome improvement from 3 to 12 months after intracerebral hemorrhage by Andrea Morotti, Jawed Nawabi, Andrea Pilotto, Maddalena Toffali, Giorgio Busto, Federico Mazzacane, Anna Cavallini, Michele Laudisi, Luana Gentile, Maria Maddalena Viola, Frieder Schlunk, Diletta Bartolini, Maurizio Paciaroni, Mauro Magoni, Chiara Bassi, Luigi Simonetti, Enrico Fainardi, Ilaria Casetta, Andrea Zini and Alessandro Padovani in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Morotti declared consulting and expert meeting honoraria for EMG-REG International and AstraZeneca. Jawed Nawabi is supported by the BIH Charité – Digital Clinician Scientist Program funded by Charité - Universitaetsmedizin Berlin, the Berlin Institute of Health and the German Research Foundation (DFG,Deutsche Forschungsgemeinschaft). Dr. Paciaroni received honoraria as a member of the speaker bureau of Sanofi-Aventis, iRhythm, Bristol Meyer Squibb, Daiiki Sankyo and Pfizer. Dr. Zini declared consulting and speaker fees from Boehringer-Ingelheim, Alexion-AstraZeneca and CSL Behring, Bayer, Angels Iniziative, Daiichi-Sankio.
All the other Authors report no disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Arcispedale S. Anna, Ferrara, Italy (PN 26032009-15122011); IRCCS Mondino Foundation, Pavia, Italy (PN 0035588/22); ASST Spedali Civili, Brescia, Italy (PN 4067-08052020); IRCCS Istituto delle Scienze Neurologiche, Bologna, Italy (DL 196/2003); Charitè Hospital, Berlin, Germany (PN EA1/035/20) and University of Perugia/Azienda Ospedaliera Santa Maria Della Misericordia (DL 196/2003).
Informed consent
Written informed consent was obtained by patients or caregivers, or waived by the Institutional Review Boards.
Guarantor
AM
Contributorship
AM designed the study, performed statistical analyses and drafted the manuscript. All authors collected data, analyzed images, reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.