
Abstract
Background:
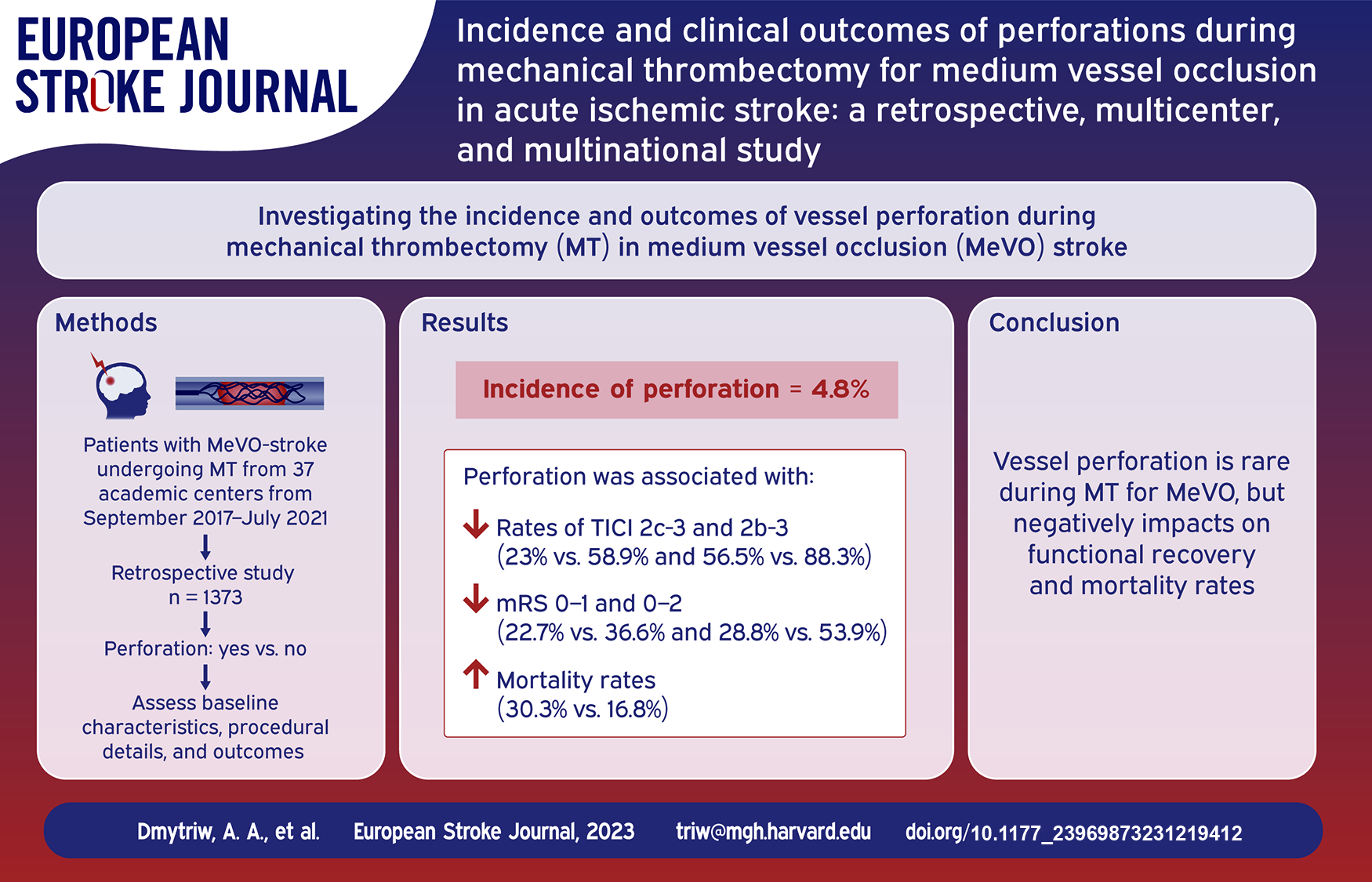
Mechanical thrombectomy (MT) has revolutionized the treatment of acute ischemic stroke (AIS) due to large vessel occlusion (LVO), but its efficacy and safety in medium vessel occlusion (MeVO) remain less explored. This multicenter, retrospective study aims to investigate the incidence and clinical outcomes of vessel perforations (confirmed by extravasation during an angiographic series) during MT for AIS caused by MeVO.
Methods:
Data were collected from 37 academic centers across North America, Asia, and Europe between September 2017 and July 2021. A total of 1373 AIS patients with MeVO underwent MT. Baseline characteristics, procedural details, and clinical outcomes were analyzed.
Results:
The incidence of vessel perforation was 4.8% (66/1373). Notably, our analysis indicates variations in perforation rates across different arterial segments: 8.9% in M3 segments, 4.3% in M2 segments, and 8.3% in A2 segments (p = 0.612). Patients with perforation had significantly worse outcomes, with lower rates of favorable angiographic outcomes (TICI 2c-3: 23% vs 58.9%, p < 0.001; TICI 2b-3: 56.5% vs 88.3%, p < 0.001). Functional outcomes were also worse in the perforation group (mRS 0–1 at 3 months: 22.7% vs 36.6%, p = 0.031; mRS 0–2 at 3 months: 28.8% vs 53.9%, p < 0.001). Mortality was higher in the perforation group (30.3% vs 16.8%, p = 0.008).
Conclusion:
This study reveals that while the occurrence of vessel perforation in MT for AIS due to MeVO is relatively rare, it is associated with poor functional outcomes and higher mortality. The findings highlight the need for increased caution and specialized training in performing MT for MeVO. Further prospective research is required for risk mitigation strategies.
Introduction
The transformative impact of mechanical thrombectomy (MT) on the management of acute ischemic stroke (AIS) patients with large vessel occlusion (LVO) has been well established. 1 As early as 2015, a series of five randomized clinical trials shed light on the significant advantages of MT over traditional treatment methods for LVO. 2 Since these seminal findings, the scope for MT indications has been continuously broadening.1,2 However, a noticeable gap exists in the literature regarding the efficacy of MT in AIS caused by medium vessel occlusion (MeVO).
Several ongoing randomized trials, such as DISTAL (EnDovascular Therapy Plus Best Medical Treatment (BMT) vs BMT Alone for MedIum VeSsel Occlusion sTroke, ClinicalTrials.gov Identifier: NCT05029414), DISTALS (Distal Ischemic Stroke Treatment With Adjustable Low-profile Stentriever, NCT05152524), DISCOUNT (Evaluation of Mechanical Thrombectomy in Acute Ischemic Stroke Related to a Distal Arterial Occlusion, NCT05030142), ESCAPE-MEVO (EndovaSCular TreAtment to imProve outcomEs for Medium Vessel Occlusions, NCT05151172), and FRONTIER-AP (Randomized controlled trial of the clinical outcome and safety of endovascular vs standard medical therapy for stroke with medium sized vessel occlusion), 3 aim to evaluate the benefit of MT in MeVO. Critics argue that MT’s effectiveness in MeVO may be compromised due to potential challenges like thinner vessel walls, increased vessel tortuosity, and the absence of specialized devices tailored for medium-sized vessels.4,5 These factors could increase the risk of complications such as hemorrhage, thereby reducing the procedure’s net clinical benefit.
One serious complication of MT is vessel perforation, which is often linked to poor functional outcomes including death. 6 Despite its clinical significance, data on perforation during MT is limited, particularly in the context of MeVO. 7 In cases involving medium-sized vessels, the dynamics of perforation might differ from those in large vessels. For example, the rate of blood flow during active extravasation might be slower, and the affected brain volume could be smaller if vessel occlusion is required to stop extravasation. 8
Therefore, this study sought to contribute to the evolving landscape by focusing on the incidence and outcomes of perforations during MT in AIS patients with MeVO. By doing so, we hope to provide clinicians with valuable insights that can guide treatment decisions for this specific, yet understudied, patient population.
Methods
The study received approval from the local ethical standards committee at each participating site, and informed consent from patients was waived. The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Setting and ethical approval
Characteristics and outcomes of patients with acute ischemic stroke due to medium vessel occlusions (MeVO) treated with MT or MT + IVtPA were collected at 37 academic centers in North America, Asia, and Europe. Data were collected between September 2017 and July 2021. Data for this study were collected prospectively and reviewed retrospectively. Institutional review board approval was obtained at each individual participating center. The local board-certified neurointerventionalist reviewed all cases before sending their data to the MAD MT consortium. They determined the angiographic treatment success before the data was sent to the consortium, which was self-reported by each center.
Data collection and outcomes
Baseline characteristics were recorded for patients. Baseline characteristics and risk factors of interest included sex (male or female), age, hypertension, hypercholesterolemia, diabetes mellitus, atrial fibrillation, and smoking status. Pre-morbid modified Rankin Scale (mRS) score and occlusion vessel were similarly recorded. The onset of stroke was trichotomized into witnessed, unknown, or wake-up stroke. NIHSS was recorded at the presentation. Baseline Alberta Stroke Program Early CT Score (ASPECTS) was collected per each institution’s protocol.
Procedural details of interest included antiplatelet and anticoagulation medication status, mothership versus drip-and-ship, time from onset to puncture and recanalization, vital sign readings (blood pressure, temperature, heart rate), glycemic readings, anesthesia type (general, sedation, or local), access site (femoral or radial), heparin administration, and imaging after MT (computed tomography (CT), magnetic resonance (MR), or none).
The primary outcome of interest was a good functional outcome defined as an mRS score of 0–2 measured at 90 days. Secondary outcomes of interest included first-pass effect (FPE) thrombolysis in cerebral infarction (TICI) scores, number of thrombectomy passes, and mRS scores at 90 days. mRS and TICI scores were adjudicated as per each institution’s protocol.
Procedural and technical details
Treatment consisted of MT alone or MT+ intravenous (IV) tissue plasminogen activator (tPA), (IVtPA). MT access site, either femoral artery or radial artery, was left to the individual operator’s discretion. Similarly, the number of passes was left to the treating physician’s discretion and institutional guidelines. Additionally, the operator determined the MT device selection and type (aspiration or stent-retriever).
Definitions
MVs were defined to encompass codominant or nondominant M2-segments, M3- and M4-segments of the MCA as well as the anterior cerebral artery (ACA) and posterior cerebral artery (PCA) and their branches, respectively. 4 MeVO was defined as occlusion of one or several of the above mentioned MVs. Perforation was confirmed by extravasation during an angiographic series.
Statistical analysis
Categorical variables were summarized as frequencies with percentages and compared using the Chi-square test. Continuous variables were summarized as medians with interquartile ranges (IQR) and compared using the Mann-Whitney U test. To address missing data, we employed the multiple imputation method with 10 imputations, ensuring robustness in our analysis. All statistical analyses were performed using R Studio version 4.2.2. For all statistical tests within the results synthesis, a p value of ⩽0.05 was used to indicate statistical significance.
Results
Baseline characteristics
The study encompassed 1373 AIS patients with MeVOs, of whom 66 (4.8%) incurred vessel perforation during MT. A detailed analysis revealed variations in perforation rates across different arterial segments: M3 segments showed a perforation rate of 8.9% (14/146), compared to 4.3% in M2 segments (46/1075), and 8.3% in A2 segments (3/36) (p = 0.612). The demographic and clinical characteristics were comparable across patients with and without perforations (Table 1). The median age for the cohort was 64 years (IQR: 47–79), with no statistically significant difference between perforation and non-perforation groups (p = 0.496). Sex distribution was balanced between the two groups, with 50.4% females in non-perforation group and 57.6% in the perforation group (p = 0.313). Pre-existing comorbidities such as hypertension (p = 0.622), hypercholesterolemia (p = 0.4), and atrial fibrillation (p = 0.36) did not show a statistically significant association with the incidence of perforation. Initial stroke severity, assessed via NIHSS and ASPECTS, was also comparable (p = 0.337 and p = 0.463, respectively).
Baseline characteristics of the included patients in the study.
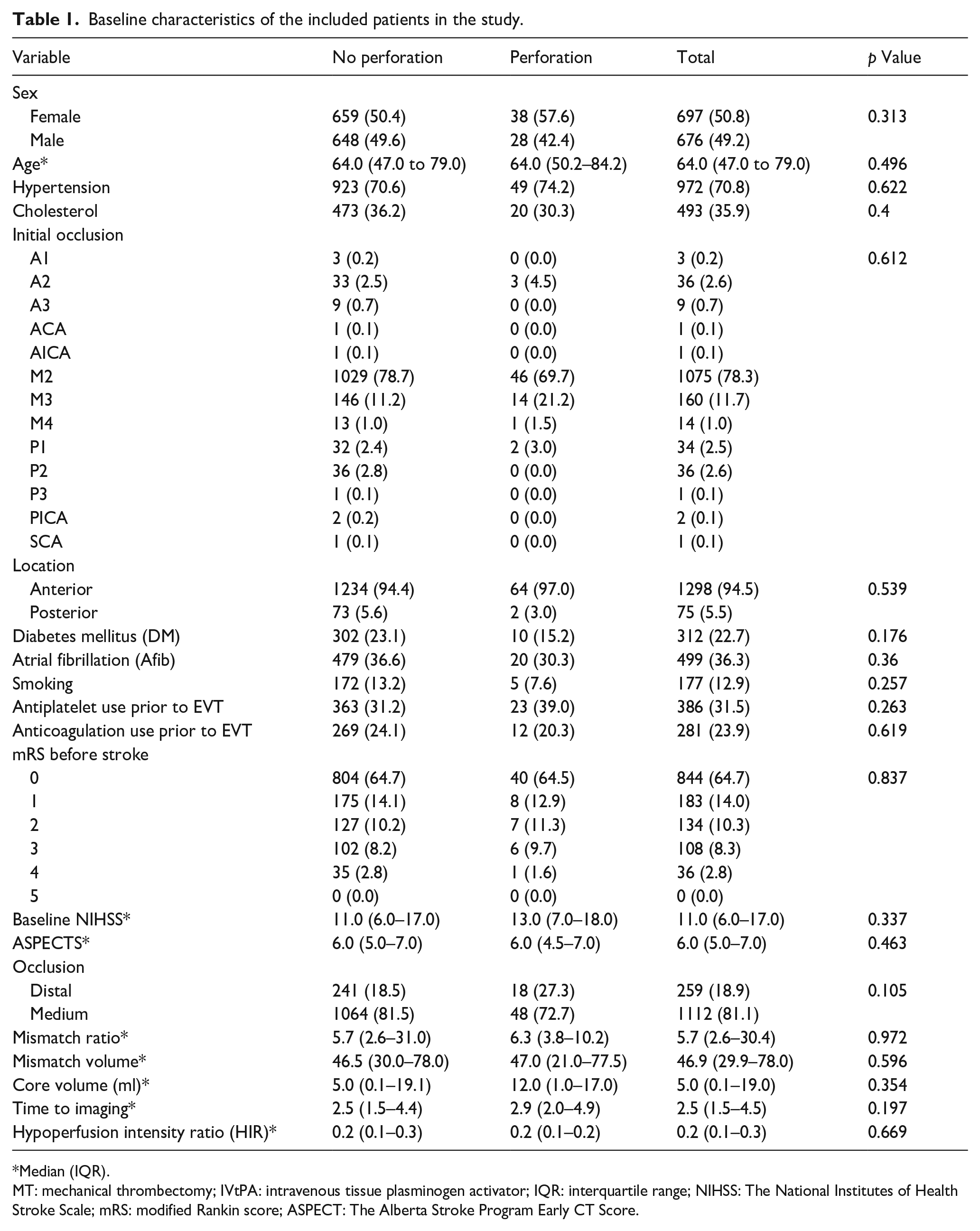
Median (IQR).
MT: mechanical thrombectomy; IVtPA: intravenous tissue plasminogen activator; IQR: interquartile range; NIHSS: The National Institutes of Health Stroke Scale; mRS: modified Rankin score; ASPECT: The Alberta Stroke Program Early CT Score.
Procedural Details
Various MT techniques were employed, including stent retrievers, aspiration, or a combination of both. The first-line technique had no significant influence on perforation incidence (p = 0.083). Pre-operative vital signs indicated a slight but significant elevation in systolic (157.5 (IQR: 143.5–180) vs 150 (IQR: 131.8–167), p = 0.012) and diastolic blood pressure (90 (IQR: 80–100) vs 83 (IQR: 74–95), p = 0.013) in the perforation group compared to non-perforation group. However, the two groups’ other procedural parameters, like time delays from stroke onset to arterial puncture and recanalization, were statistically similar (Table 2).
Periprocedural details of the included patients in the study.
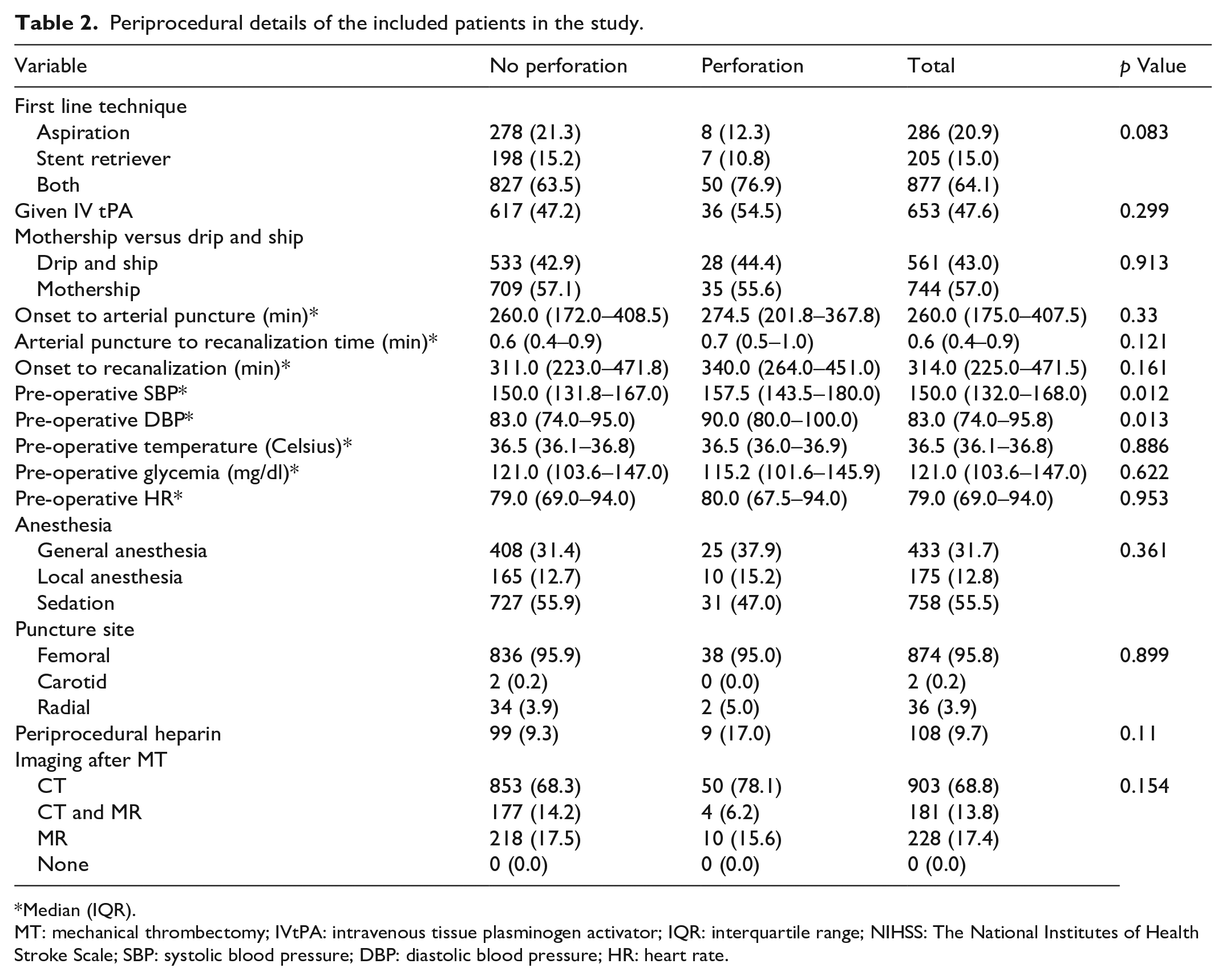
Median (IQR).
MT: mechanical thrombectomy; IVtPA: intravenous tissue plasminogen activator; IQR: interquartile range; NIHSS: The National Institutes of Health Stroke Scale; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate.
Outcomes
Angiographic and clinical outcomes differed significantly between the two groups. TICI scores of 2c-3 and 2b-3 were significantly less likely in the perforation group compared to the non-perforation group (14/66, 23% vs 757/1307, 58.9%; p < 0.001 and 35/66, 56.5% vs 1135/1307, 88.3%; p < 0.001, respectively). Patients with perforation were less likely to have an excellent outcome (mRS 0–1 at 3 months) than those without perforation (15/66, 22.7% vs 478/1307, 36.6%; p = 0.031). Similarly, the rate of good functional outcomes (mRS 0–2 at 3 months) was also significantly lower in the perforation group compared to non-perforation group (19/66, 28.8% vs 704/1307, 53.9%; p < 0.001) (Figures 1 and 2). In addition, the perforation group had a higher mortality rate than the non-perforation group (20/66, 30.3% vs 220/1307, 16.8%; p = 0.008). Hemorrhagic complications, including different types of intracranial hemorrhage (ICH), were notably higher in the perforation group (p < 0.001) (Table 3).
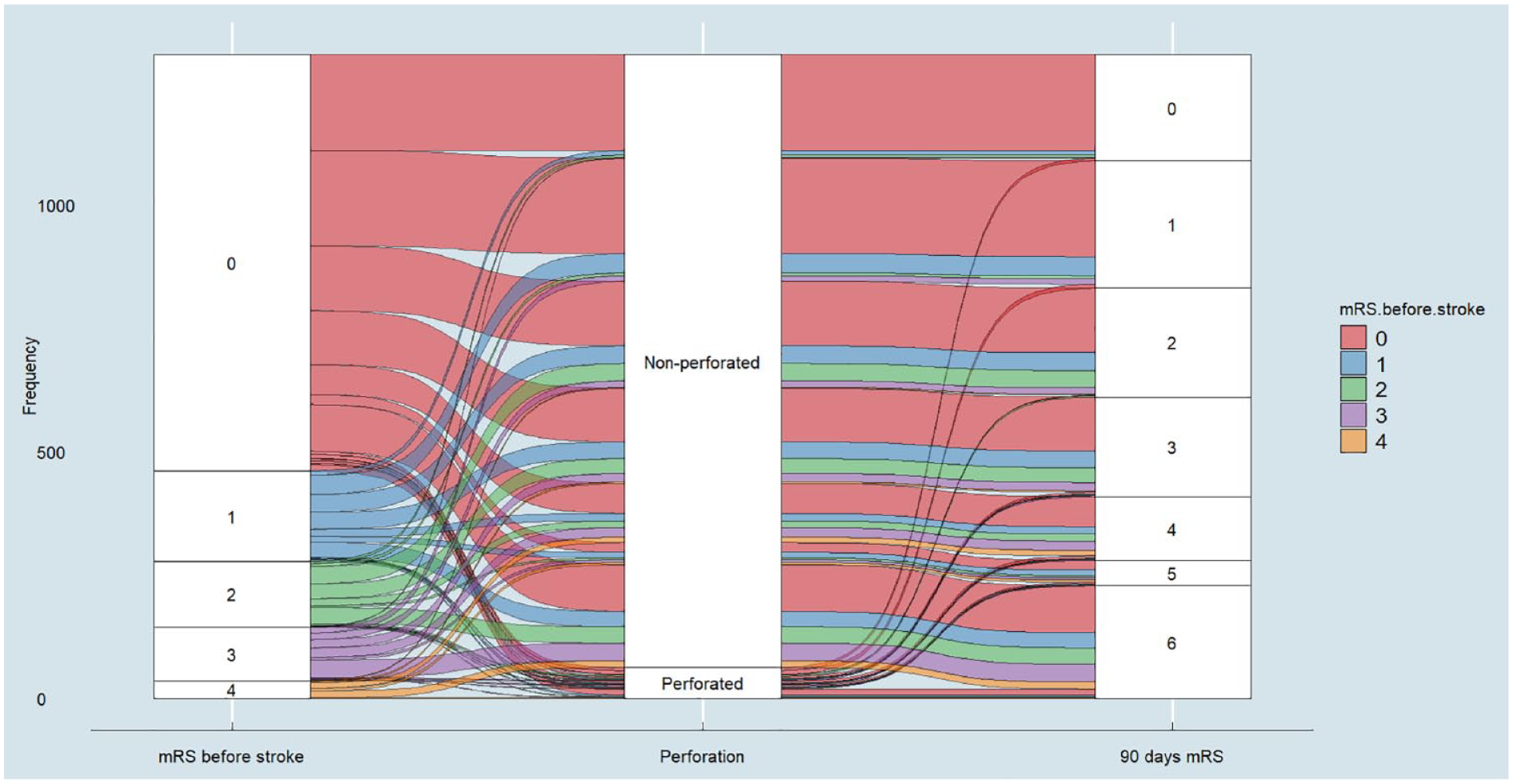
Sankey diagram depicts the transition of mRS scores before stroke versus 90 days after, grouped by perforation status. Colored streams represent the flow of patients from initial mRS scores (0–4) to 90-day outcomes (0–6).
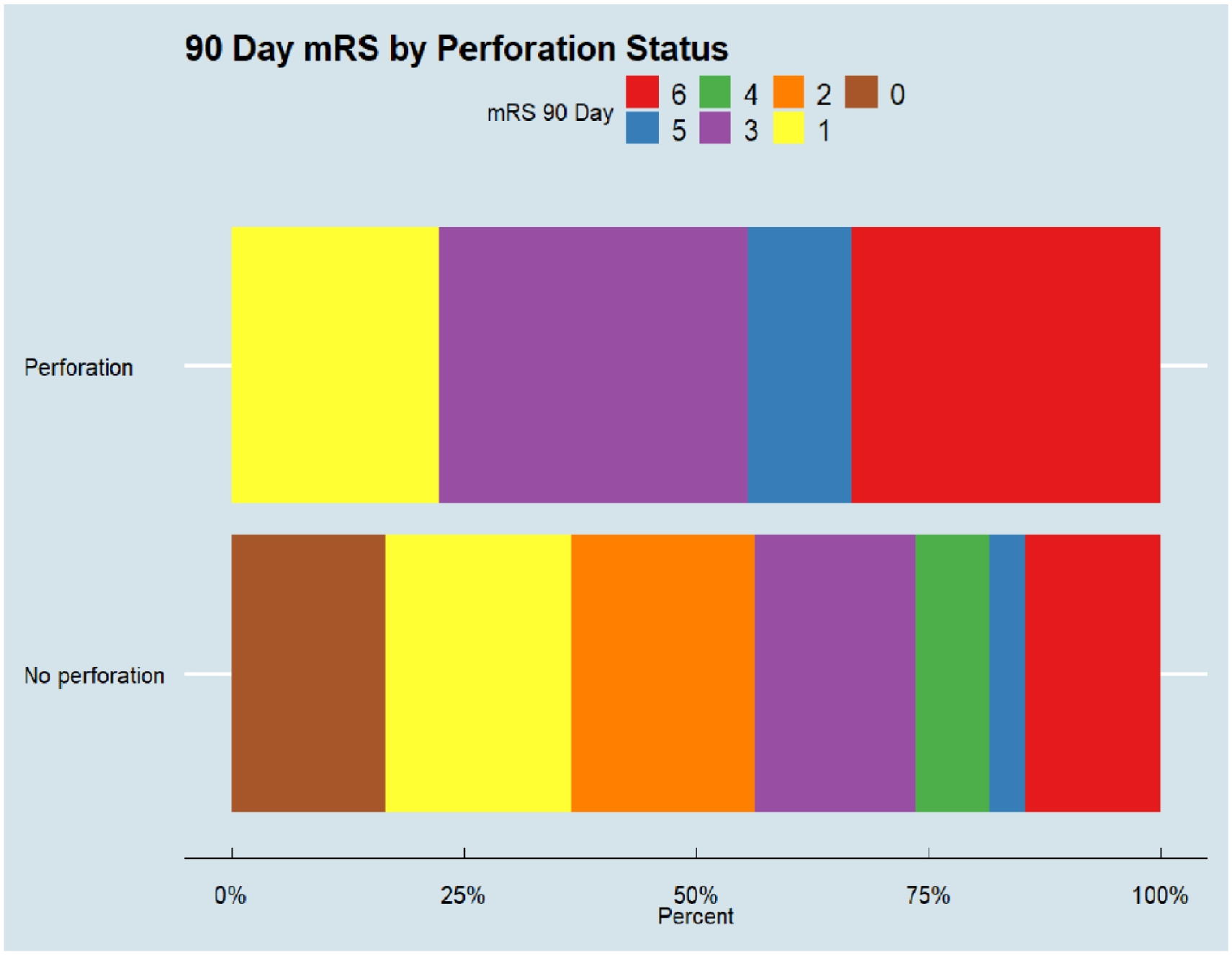
Bar charts display the percentage distribution of 90-day modified Rankin Scale (mRS) scores for stroke patients.
Treatment outcomes of the included patients in the study.
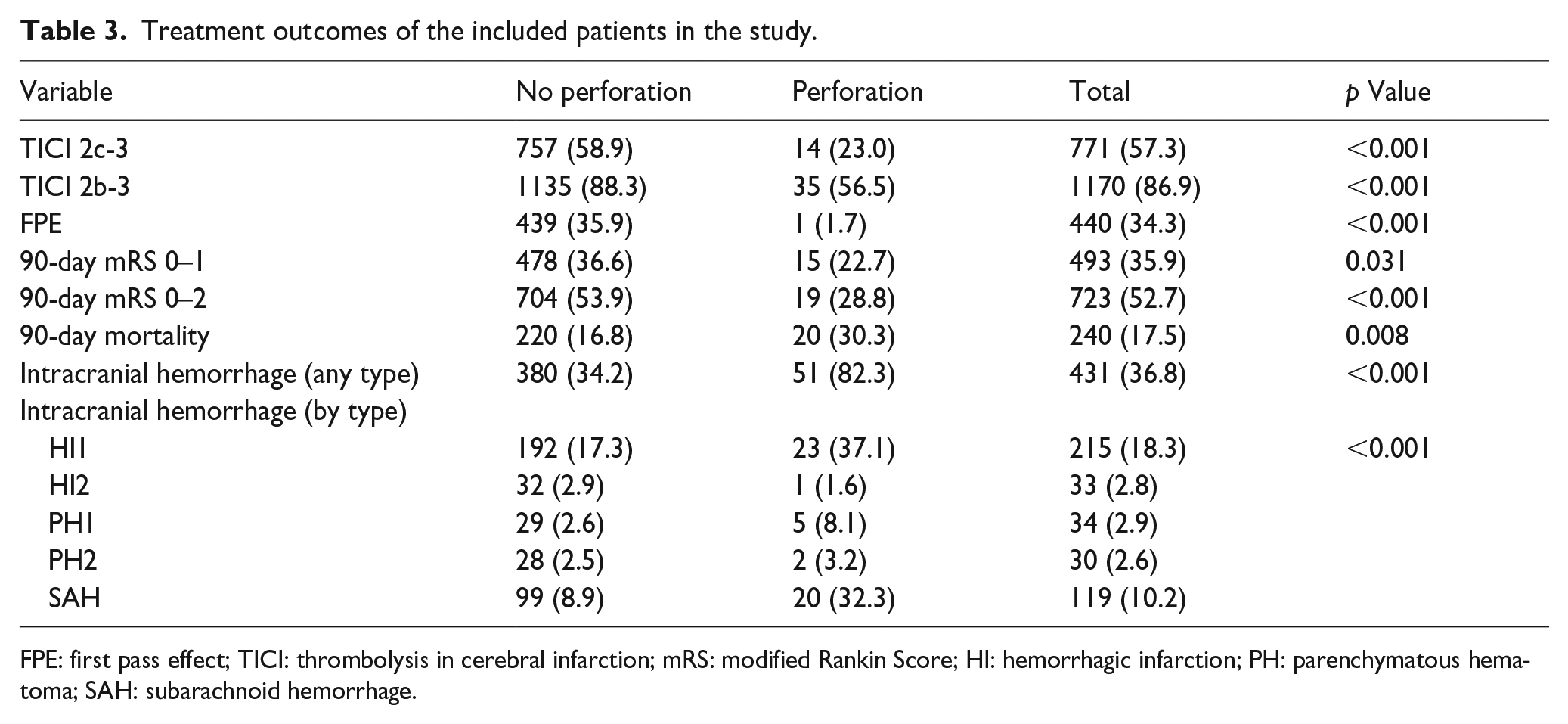
FPE: first pass effect; TICI: thrombolysis in cerebral infarction; mRS: modified Rankin Score; HI: hemorrhagic infarction; PH: parenchymatous hematoma; SAH: subarachnoid hemorrhage.
Discussion
In this multicenter, retrospective study, we observed an overall low 4.8% incidence of vessel perforation among AIS patients with MeVO undergoing MT. Vessel perforation was associated with poor functional outcomes, increased mortality rates, and higher hemorrhagic complications associated with perforation during MT.
Our results aligns with previous studies as they reported a frequency of perforation during thrombectomy of between 0.7% and 6.9%.7,8–22 Moreover, our study substantiates the hypothesis generated by Schulze-Zachau et al. 23 that a higher frequency of perforations might characterize MeVO thrombectomy.
Clinical evidence for EVT in DMVOs is still somewhat limited but growing. Randomized trials have largely focused on occlusions in the M2 segment of the middle cerebral artery (MCA), particularly those more proximal and larger, resembling M1 MCA occlusions. 24 Nevertheless, pooled data from multiple studies, such as the HERMES collaboration, indicated that EVT can benefit certain DMVOs, showing promising results in reperfusion and functional outcomes. 25
For DMVOs other than M2 MCA, most of the evidence stems from case series. For example, one single-center series showed that EVT achieved high reperfusion rates and had a low complication profile in patients with various types of DMVOs. 26
Several meta-analyses using nonrandomized data have recently assessed EVT’s benefit in MeVOs, suggesting promising safety and efficacy.27–33 However, the risk of perforation during mechanical thrombectomy remains a serious complication, often linked to poor functional outcomes or even mortality. 23
Schulze-Zachau et al. 23 discussed that functional outcomes were generally poor for patients experiencing perforation during MT. They reported that 15.8% of patients had an mRS score of 0–1 at 3 months and 25.7% had an mRS score of 0–2 at 3 months. Moreover, the mortality rate in their study was 50.5%. In the present study, 22.7% and 28.8% of patients had mRS scores of 0–1, 0–2, respectively. In addition, the mortality rate in the perforation group was 30.3%. Our findings in addition to Schulze-Zachau et al. 23 highlight the poor outcomes associated with perforation in MeVOs.
Our study has several limitations. First, the retrospective design inherently carries the risk of selection bias. Second, the study did not capture long-term outcomes beyond the 90-day follow-up, limiting our understanding of the lasting impact of perforations during MT on functional recovery and quality of life. Finally, while providing valuable insights into predictors of perforation, our multivariable logistic regression model may not have accounted for all potential confounding variables, such as operator experience or variations in institutional protocols.
Conclusion
In conclusion, this multicenter, retrospective study provides valuable insights into the incidence and clinical outcomes of perforations during MT in patients with AIS caused by medium vessel occlusion. Our findings indicate that while perforations are relatively rare, they are associated with poorer functional outcomes, higher mortality rates, and hemorrhagic complications. These results underscore the need for heightened awareness and possibly specialized training for managing the risks associated with MT in this specific patient population. Further prospective studies and randomized trials are warranted to substantiate these findings and develop risk mitigation strategies.
Footnotes
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Regenhardt serves on a DSMB for a trial sponsored by Rapid Medical, serves as site PI for studies sponsored by Penumbra and Microvention, and receives stroke research grant funding from the National Institutes of Health, Society of Vascular and Interventional Neurology, and Heitman Stroke Foundation. Dr. Guenego reports consultancy for Rapid Medical and Phenox, not directly related to the present work. Prof. Clarençon reports conflicts of interest with Medtronic, Balt Extrusion (consultant), ClinSearch (core lab), Penumbra, Stryker (payment for reading), and Artedrone (Board); all not directly related to the present work. Dr. Henninger received support from NINDS NS131756, during the conduct of the study. Dr. Liebeskind is consultant as Imaging Core Lab to Cerenovus, Genentech, Medtronic, Stryker, Rapid Medical. Dr. Nguyen reports advisory board with Idorsia. Dr. Yeo reports Advisory work for AstraZeneca, Substantial support from NMRC Singapore and is a medical advisor for See-mode, Cortiro, and Sunbird Bio, with equity in Ceroflo. All unrelated to the present work. Dr. Griessenauer reports a proctoring agreement with Medtronic and research funding by Penumbra. Dr. Marnat reports conflicts of interest with Microvention Europe, Stryker Neurovascular, Balt (consulting), Medtronic, Johnson & Johnson, and Phenox (paid lectures), all not directly related to the present work. Pr Sibon reports conflict of interest with Medtronic, Sanofi, Bayer, Boehringer-Ingelheim, Novartis, Novo-Nordisk, BMS-Pfizer (board and paid lectures), all not directly related to the present work. Dr. Yedavalli is a consultant for RAPID (Ischemaview, Menlo Park, CA). Dr. Vagal is a consultant for Viz AI. She is also PI of Imaging core lab for ENDOLOW study funded by Cerenovus (monies go to the institution). Dr. Gopinathan reports conflicts of interest with Microvention, Stryker Neurovascular, Medtronic, BD, Penumbra (paid lectures, workshops, and proctoring), all not directly related to the present work. Dr. Bernstock has an equity position in Treovir Inc., an oHSV clinical stage company and UpFront Diagnostics. JDB is also on the Centile Bioscience and NeuroX1 boards of scientific advisors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent and ethical approval
The study received approval from the local ethical standards committee at each participating site, and informed consent from patients was waived. The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Guarantor
Adam A. Dmytriw, MD, MPH, MSc.
Author contributions
A.A.D., B.M., H.S., S.G., J.E.S., H.K., M.A., P.J., P.K., T.N.N., J.J.H., R.W.R., N.M.C., J.D.B., A.S., K.E.N., A.A., L.M., A.D., F.B., G.F., A.R., S.S., C.M., J.F., A.L.K., A.S.P., C.D., P.T.K., M.C., G.M., J.B., X.B., I.S., S.N., N.H., T.R.M., C.J.S., J.D.R., T.O., S.D., L.L.Y., B.Y.Q.T., A.G., J.C.M.G., S.S.M., S.S., L.R., C.C., A.M., L.C., A.V., N.A., H.H.C.S., S.I.T., A.B., F.C., M.E., K.P., M.Q.C., N.R.G., M.A.M., J.J., V.C., A.T.S., V.Y., P.H., Y.A., B.G., C.P.S., C.H., R.K., M.K.O., C.J.G., A.J.T., C.Y.H., D.S.L., R.A.R., A.M.A., I.T., T.D.F., R.F., C.W., B.L., A.B.P., V.M.P. contributed to the conception and design of the work. A.A.D., B.M., H.S., S.G., J.E.S., H.K., M.A., P.K., T.N.N., J.J.H., R.W.R., N.M.C., J.D.B., A.S., K.E.N., A.A., L.M., A.D., F.B., G.F., A.R., S.S., C.M., J.F., A.L.K., A.S.P., C.D., P.T.K., M.C., G.M., J.B., X.B., I.S., S.N., N.H., T.R.M., C.J.S., J.D.R., T.O., S.D., L.L.Y., B.Y.Q.T., A.G., J.C.M.G., S.S.M., S.S., L.R., C.C., A.M., L.C., A.V., N.A., H.H.C.S., S.I.T., P.J., A.B., F.C., M.E., K.P., M.Q.C., N.R.G., M.A.M., J.J., V.C., A.T.S., V.Y., P.H., Y.A., B.G., C.P.S., C.H., R.K., M.K.O., C.J.G., A.J.T., C.Y.H., D.S.L., R.A.R., A.M.A., I.T., T.D.F., R.F., C.W., B.L., A.B.P., V.M.P. were involved in the acquisition of data, and data analysis, and interpretation. A.A.D., B.M., H.S., S.G., J.E.S., H.K., M.A., P.K., T.N.N., J.J.H., R.W.R., N.M.C., J.D.B., A.S., K.E.N., A.A., L.M., A.D., F.B., G.F., A.R., S.S., C.M., J.F., A.L.K., A.S.P., C.D., P.T.K., M.C., G.M., J.B., X.B., I.S., S.N., N.H., T.R.M., C.J.S., J.D.R., T.O., S.D., L.L.Y., B.Y.Q.T., A.G., J.C.M.G., S.S.M., L.R., C.C., A.M., L.C., A.V., N.A., H.H.C.S., S.I.T., P.J., A.B., F.C., M.E., K.P., M.Q.C., N.R.G., M.A.M., J.J., V.C., A.T.S., V.Y., P.H., Y.A., B.G., C.P.S., C.H., R.K., M.K.O., C.J.G., A.J.T., C.Y.H., D.S.L., R.A.R., A.M.A., I.T., T.D.F., R.F., C.W., B.L., A.B.P., V.M.P. drafted the work and revised it critically for important intellectual content. All authors gave final approval of the version to be published and agree to be accountable for all aspects of the paper.