
Abstract
Introduction:
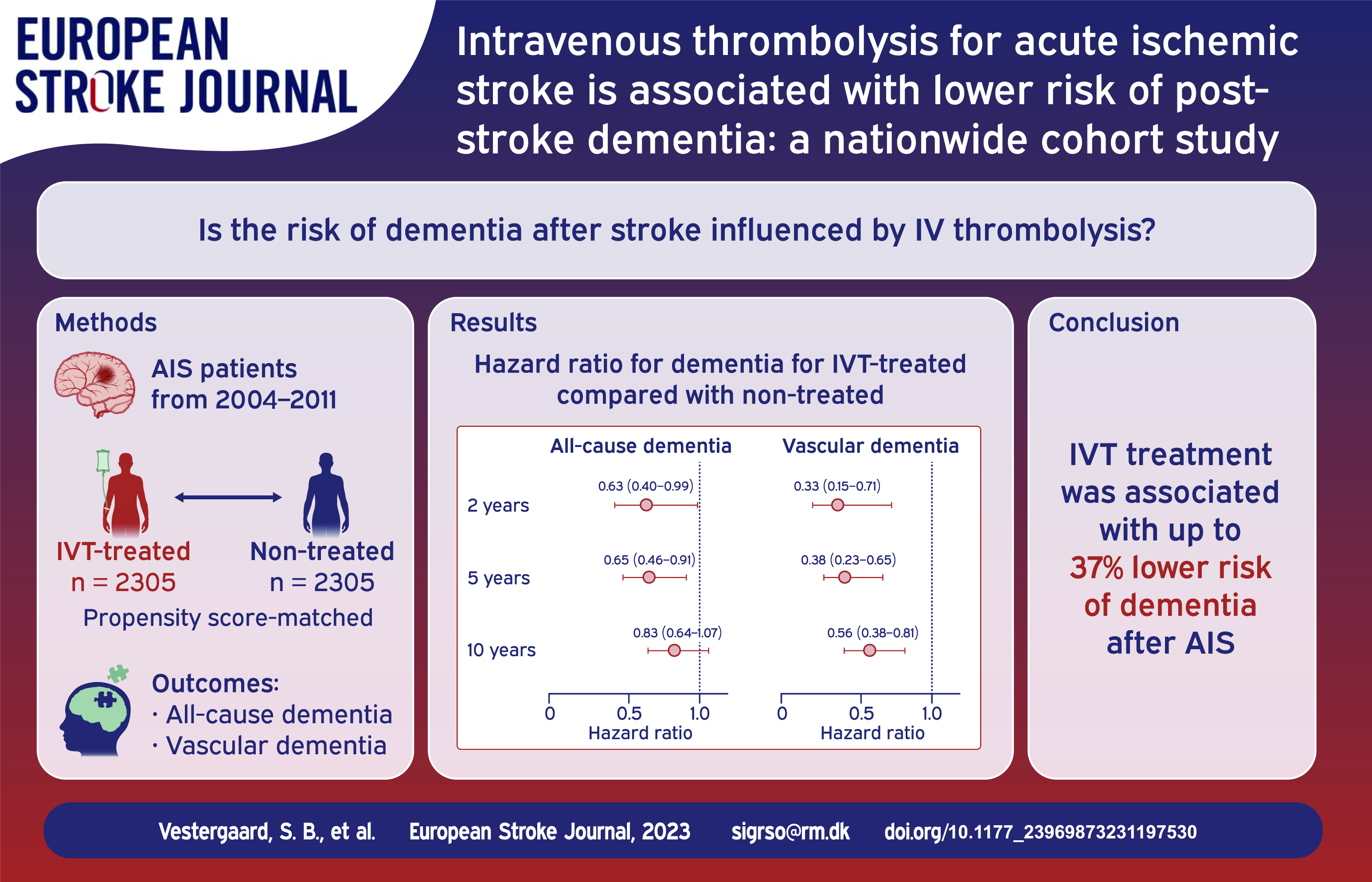
Dementia after stroke is common and is a great concern for patients and their caregivers. The objective was to investigate if intravenous thrombolysis (IVT) for acute ischemic stroke (AIS) was associated with lower risk of dementia after stroke.
Patients and methods:
When IVT was introduced in Denmark, not all eligible patients were treated due to restricted access. We conducted a nationwide register-based cohort study of all patients with AIS in Denmark from 2004 to 2011. IVT-treated patients were propensity score-matched with comparable non-treated patients. Cox proportional hazards regression was used to estimate the hazard ratio (HR) for all-cause and vascular dementia 2, 5, and 10 years after stroke.
Results:
Of the 5919 patients eligible for the study, 2305 IVT-treated patients were propensity score-matched with 2305 non-treated patients. Mean (SD) age was 66.6 (13.3) and 61.2% were male. Rate of all-cause dementia was lower for the IVT-treated 2 years (8.4/1000 person years (PY) vs 13.6/1000 PY, HR 0.63 (0.40–0.99)) and 5 years after stroke (7.3/1000 PY vs 11.4/1000 PY, HR 0.65 (0.46–0.91)). 10 years after stroke, the rates of all-cause dementia remained in favor of IVT (8.0/1000 PY vs 9.8/1000 PY, HR 0.83 (0.64–1.07)). IVT-treated had lower rates of vascular dementia 2 years (2.4/1000 PY vs 7.4/1000 PY, HR 0.33 (0.15–0.71)), 5 years (2.3/1000 PY vs 6.2/1000 PY, HR 0.38 (0.23–0.65)), and 10 years after stroke (3.0/1000 PY vs 5.4/1000 PY, HR 0.56 (0.38–0.81)).
Conclusion:
IVT treatment was associated with lower long-term risk of both vascular and all-cause dementia after AIS.
Introduction
Cognitive impairment after stroke is common.1,2 For many patients with stroke, cognitive impairment will progress to dementia. Indeed, the dementia risk among stroke survivors is more than doubled compared with the risk in the general population.3–6 Dementia is of great concern for stroke patients and their caregivers, as it is associated with lower quality of life and increased morbidity and mortality.7,8
Dementia after stroke may develop for various reasons. The stroke lesion can be strategically located 9 ; or it can be part of small-vessel disease and may accelerate an ongoing cognitive decline.10,11 Finally, increased stroke severity and increased lesion size are risk factors for dementia. 6 These mechanisms all indicate that reperfusion treatment of acute ischemic stroke (AIS) may reduce the risk of dementia after stroke.
Reperfusion treatment with intravenous thrombolysis (IVT) is an effective treatment of AIS with an established effect on functional outcome.12–14 Though stakeholders stress the need for more research into post-stroke cognitive outcomes, 15 the effect of IVT on dementia after stroke is not well studied. So far, only small clinical studies have investigated the effect of IVT on post-stroke cognitive decline, not dementia, and only one regional cohort study has investigated dementia after stroke.16,17 This emphasizes the need for more and larger studies in this field.
When IVT was introduced in Denmark, not all IVT-eligible patients were treated due to restricted treatment access. 18 In this nationwide register-based cohort study we have utilized this historical setting to compare IVT-treated patients with a group of comparable patients with AIS who did not receive IVT as a natural experiment. The aim was to investigate if IVT treatment was associated with a lower long-term risk of dementia after stroke.
Methods
Design, setting, and data sources
This was a nationwide register-based cohort study of all patients with AIS in Denmark from 2004 to 2011. Denmark has a universal health care system offering all Danish residents free health care.
When IVT treatment was introduced in Denmark in 2004, it was only accessible at two stroke centers and only during daytime. The availability gradually increased until it was a nationwide 24-h service by 2008. 18
The Danish Stroke Registry (DSR) was used to identify the study population and was the main data source. The DSR contains prospectively collected data on all patients admitted to a stroke center in Denmark. In Denmark, all patients with AIS are admitted to public hospitals. All departments treating stroke patients are obliged to register patient data in the DSR. Stroke diagnoses in the DSR are specialist verified with a sensitivity of 97%. 19 All Danish residents have a unique personal identifier number, which was used to link individual-level data between the DSR and other public Danish registries. 20 The National Patient Registry (NPR) and the Psychiatric Central Research Register (PCRR) were used to obtain diagnosis codes. They contain diagnosis codes from all encounters at Danish hospitals and clinics.21,22 Redeemed prescriptions was obtained from the Register of Pharmaceutical Sales. The Danish Civil Registration System was used to find dates of birth, emigration, and death. Educational levels were obtained from Statistics Denmark.
Population
All adults admitted with AIS in Denmark between 2004 and 2011 were included. For patients with more than one AIS in the study period, the first stroke was considered the index stroke. Patients were divided into two groups: the IVT-treated patients and comparable patients with AIS who did not receive IVT, referred to as non-treated patients. IVT-treated patients were patients with AIS who were admitted to and received IVT at a stroke center within 4.5 h from symptom onset. To ensure sufficient sample size, the a priori specified inclusion period for this group was from 01-01-2004 to 12-31-2011. 23 Alteplase was the only thrombolytic agent approved in Denmark in this time period. The non-treated patients were patients admitted with AIS to a stroke center without receiving IVT. To reduce risk of confounding by indication, this group was limited to those admitted between 01-01-2004 and 12-31-2006 to a stroke center without IVT-services at the time. The non-treated patients were not necessarily transported by an emergency ambulance. To account for this, they were included up to 6 h from symptom onset to hospital arrival. Patients living in nursing homes were excluded. Exclusion criteria for both groups were: unknown time of last known well, missing admission time, dementia diagnosis prior to index stroke, endovascular thrombectomy, and tourists without a Danish personal identifier number. Patients were followed until first dementia diagnosis, emigration, death, or until 2, 5, and 10 years after index stroke.
Post-stroke dementia
We evaluated risk of dementia at 2, 5, and 10 years after stroke. Dementia diagnoses were divided into all-cause dementia and vascular dementia based on International Classification of Diseases 10th Revision diagnoses from the NPR (Supplemental Table 1). The specificity of a dementia diagnosis in the NPR is 86%. 24 In Denmark, a dementia diagnostic evaluation is primarily done by specialists in neurology, psychiatry, or geriatrics at public clinics.
Covariates
Age at index stroke, sex, cohabitant status, smoking status, type of residence, time from symptom onset to admission, and medical history of hypertension, diabetes, atrial fibrillation, prior stroke or TIA, prior myocardial infarction, and peripheral arterial disease were obtained from the DSR. If medical history was missing, NPR diagnoses registered up to 10 years before index stroke were used (Supplemental Table 1). In addition, if information about hypertension or diabetes was missing the Register of Pharmaceutical Sales was searched for prescriptions redeemed from 5 years before to 30 days after index stroke (Supplemental Table 1). History of smoking was defined as current or former smoking registered in the DSR. Stroke severity measured on the Scandinavian Stroke Scale (SSS) was obtained from the DSR. The SSS ranges from 0 to 58 with a lower score indicating greater stroke severity. 25 Educational level was defined by the highest attained education at the year of index stroke. Educational levels were defined according to the International Standard Classification of Education (ISCED) 201126 and divided into: low (primary and lower secondary education, ISCED 0–2), medium (upper secondary or vocational education, ISCED 3–4), and high (short, medium, or long higher education, ISCED 5–8). Quality of in-hospital stroke care was defined by proportion of the following indicators fulfilled (if indicated): admission to a stroke center within 24 h, head CT or MRI performed, platelet inhibitors prescribed, anticoagulation therapy prescribed, physiotherapy assessment, occupational therapy assessment, and nutritional screening.
Statistical analyses
The covariates cohabitation, type of residence, smoking status, stroke severity, and educational level had missing values. For these variables, multiple imputation with chained equations (MICE) was used to predict the missing values using either predictive mean matching or logistic regression. The following independent variables were included in the MICE: age, sex, educational level, cohabitation, type of residence, stroke severity, history of stroke or TIA, myocardial infarction, depression, smoking, hypertension, atrial fibrillation, diabetes, peripheral arterial disease, congestive heart failure, IVT-treatment, death, and the Kaplan Meier estimates for dementia and death. 27 Thirty imputations with 10 iterations were performed resulting in 30 imputed datasets. 28 A propensity score for receiving IVT was calculated for each patient in each imputed dataset using a logistic regression based on the following independent variables: age, sex, educational level, cohabitation type of residence, stroke severity, history of stroke or TIA, myocardial infarction, depression, smoking, hypertension, atrial fibrillation, diabetes, peripheral arterial disease, and congestive heart failure. IVT-treated patients were matched by their propensity score with non-treated patients in a 1:1 ratio using the nearest neighbor method with a caliper of 0.2. An absolute standardized difference <0.1 was considered to support the assumption of balance between the groups. The imputed and matched datasets were pooled to estimate hazard ratios (HR) and 95% confidence intervals for all-cause and vascular dementia for the IVT-treated patients compared with the non-treated patients using Cox proportional hazards regression with cluster robust variance considering death a competing risk. 29 Cumulative incidence curves were plotted for all-cause and vascular dementia with one imputed dataset. Further, two sensitivity analyses were conducted; first a complete case analysis only including patients without missing data, second an analysis of the IVT-treated patients with index stroke 2004–2008 compared with the non-treated patients. Regression analyses stratified by stroke severity (mild stroke (SSS score ⩾45) vs moderate to severe stroke (SSS score <45)) were conducted to explore the potential differential effect of IVT on dementia risk according to stroke severity. In addition, Cox proportional hazards regressions including the interaction term between stroke severity category (mild vs moderate to severe) and IVT treatment were performed. A significance level of <5% was considered statistically significant. All analyses were performed using R version 4.2.2.
Data availability
According to Danish data protection regulation, data for this study cannot be shared publicly. However, the Danish Health Authority can grant data access to researchers from authorized institutions.
Results
Participants and baseline characteristics
Between 2004 and 2011, 62,388 patients with incident AIS were identified (Figure 1). The final study population consisted of 5919 patients; 2367 IVT-treated patients and 3552 non-treated patients. Before matching, the IVT-treated patients were younger and more often male, they had a higher educational level, greater stroke severity, and lower time from symptom onset to hospital arrival (Table 1). Moreover, the IVT-treated patients were less likely to live alone and less likely to have a history of heart failure, prior stroke or TIA compared with the non-treated patients. Propensity score-matching resulted in a final study population of 4610 patients; 2305 IVT-treated and 2305 non-treated patients (average numbers across all imputed datasets) (Figure 1). Overall, mean age was 66.6, 2820 (61.2%) were male, median [IQR] SSS score was 43 [28–52], and median [IQR] time from symptom onset to hospital arrival was 1.8 [1.1–2.9] h (Table 1). After matching, baseline characteristics were balanced between the groups. A Love plot displaying the covariate balance across all imputed datasets and histograms of the distribution of propensity scores before and after matching are shown in Supplemental Figure 1 and 2, respectively.
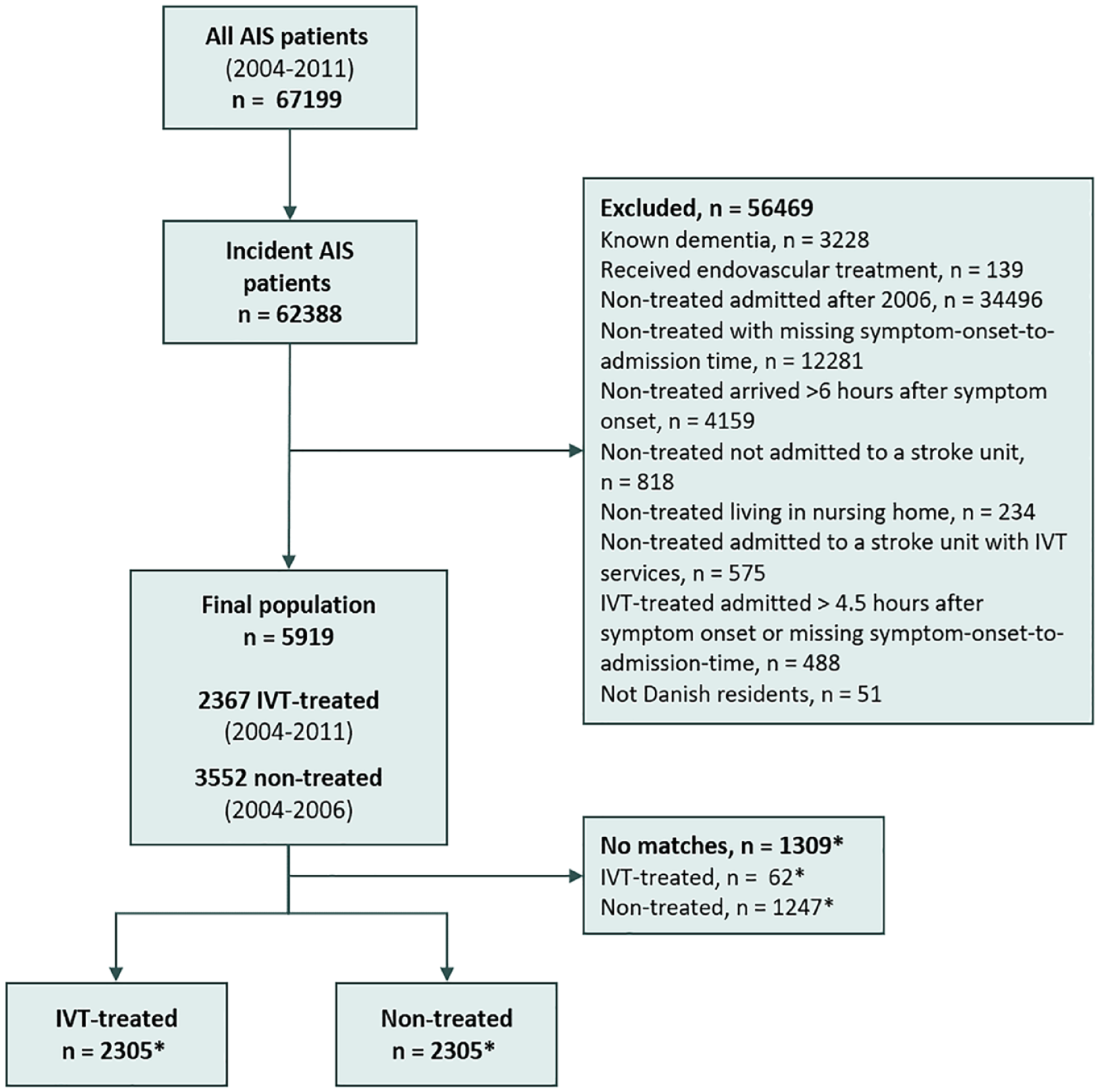
Flow-chart of study patients.
Baseline characteristics of study patients before and after propensity score matching.
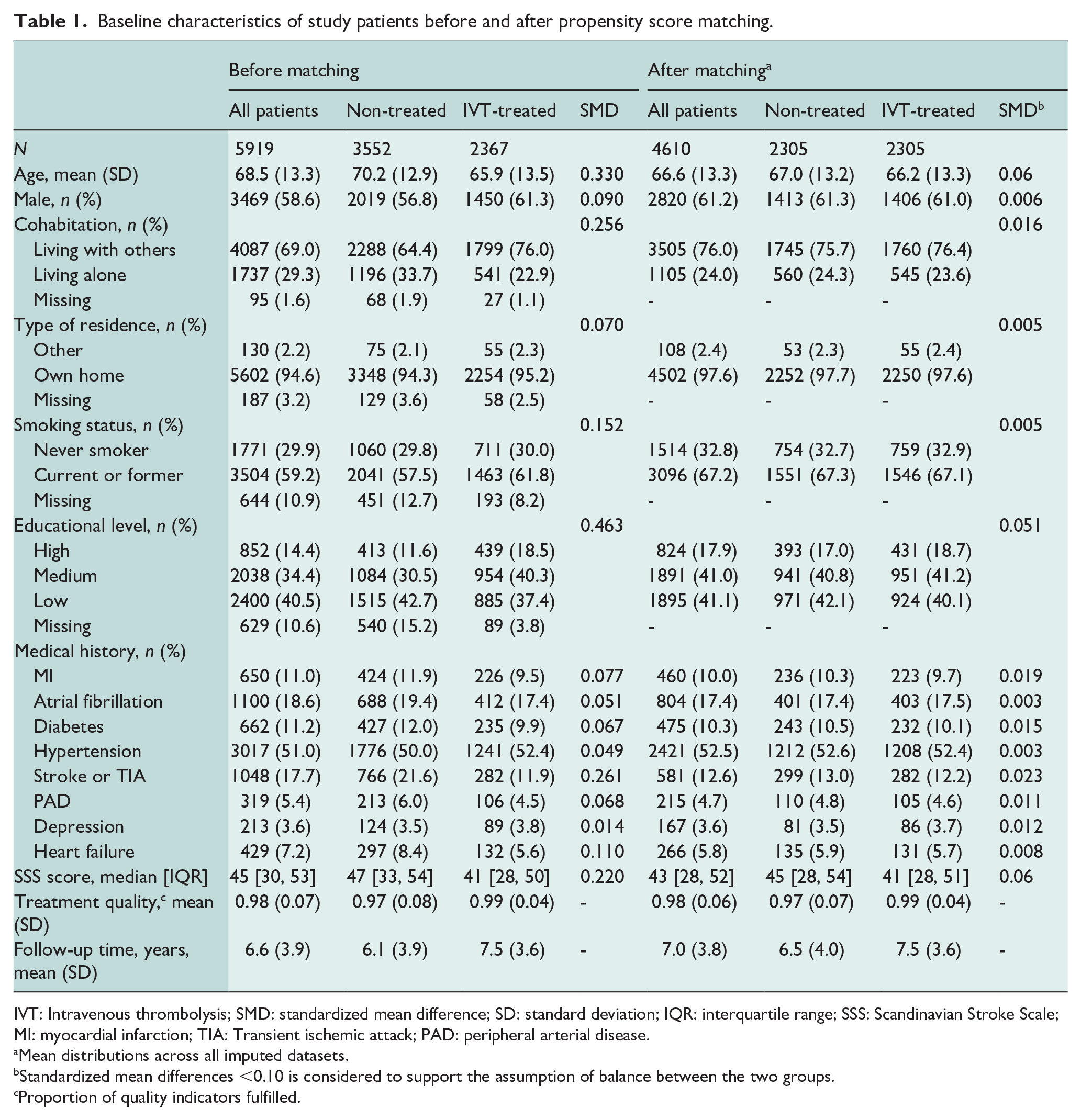
IVT: Intravenous thrombolysis; SMD: standardized mean difference; SD: standard deviation; IQR: interquartile range; SSS: Scandinavian Stroke Scale; MI: myocardial infarction; TIA: Transient ischemic attack; PAD: peripheral arterial disease.
Mean distributions across all imputed datasets.
Standardized mean differences <0.10 is considered to support the assumption of balance between the two groups.
Proportion of quality indicators fulfilled.
Post-stroke dementia
All-cause dementia was observed in 284 (6.2%) of patients within 10 years after stroke. Median [IQR] time from AIS to dementia diagnosis was 5.1 [2.0–8.8] years. Risk of all-cause dementia was lower for the IVT-treated patients compared with the non-treated patients 2 years (8.4/1000 person years (PY) vs 13.6/1000 PY, HR 0.63 (0.40–0.99)) and 5 years after stroke (7.3/1000 PY vs 11.4/1000 PY, HR 0.65 (0.46–0.91)) (Table 2). Ten years after stroke, the rates of all-cause dementia remained in favor of IVT treatment (8.0/1000 PY vs 9.8/1000 PY, HR 0.83 (0.64–1.07)). IVT-treated patients had lower risk of vascular dementia compared with non-treated patients both 2 years (2.4/1000 PY vs 7.4/1000 PY, HR 0.33 (0.15–0.71)), 5 years (2.3/1000 PY vs 6.2/1000 PY, HR 0.38 (0.23–0.65)), and 10 years after stroke (3.0/1000 PY vs 5.4/1000 PY, HR 0.56 (0.38–0.81)). Figure 2 shows the cumulative incidence curves for all-cause and vascular dementia after stroke.
Rates and hazard ratios of all-cause dementia and vascular dementia for IVT-treated compared with non-treated patients.
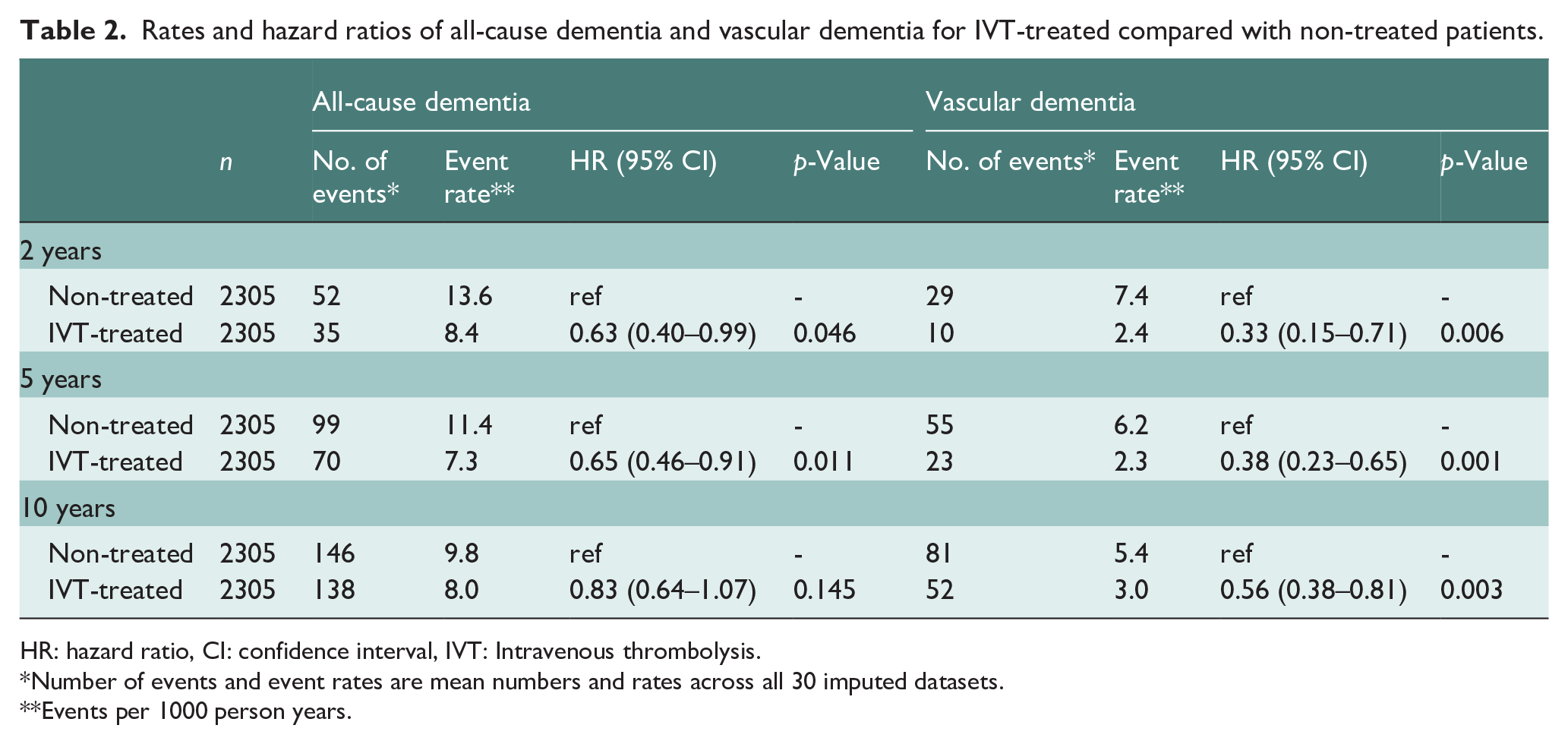
HR: hazard ratio, CI: confidence interval, IVT: Intravenous thrombolysis.
Number of events and event rates are mean numbers and rates across all 30 imputed datasets.
Events per 1000 person years.
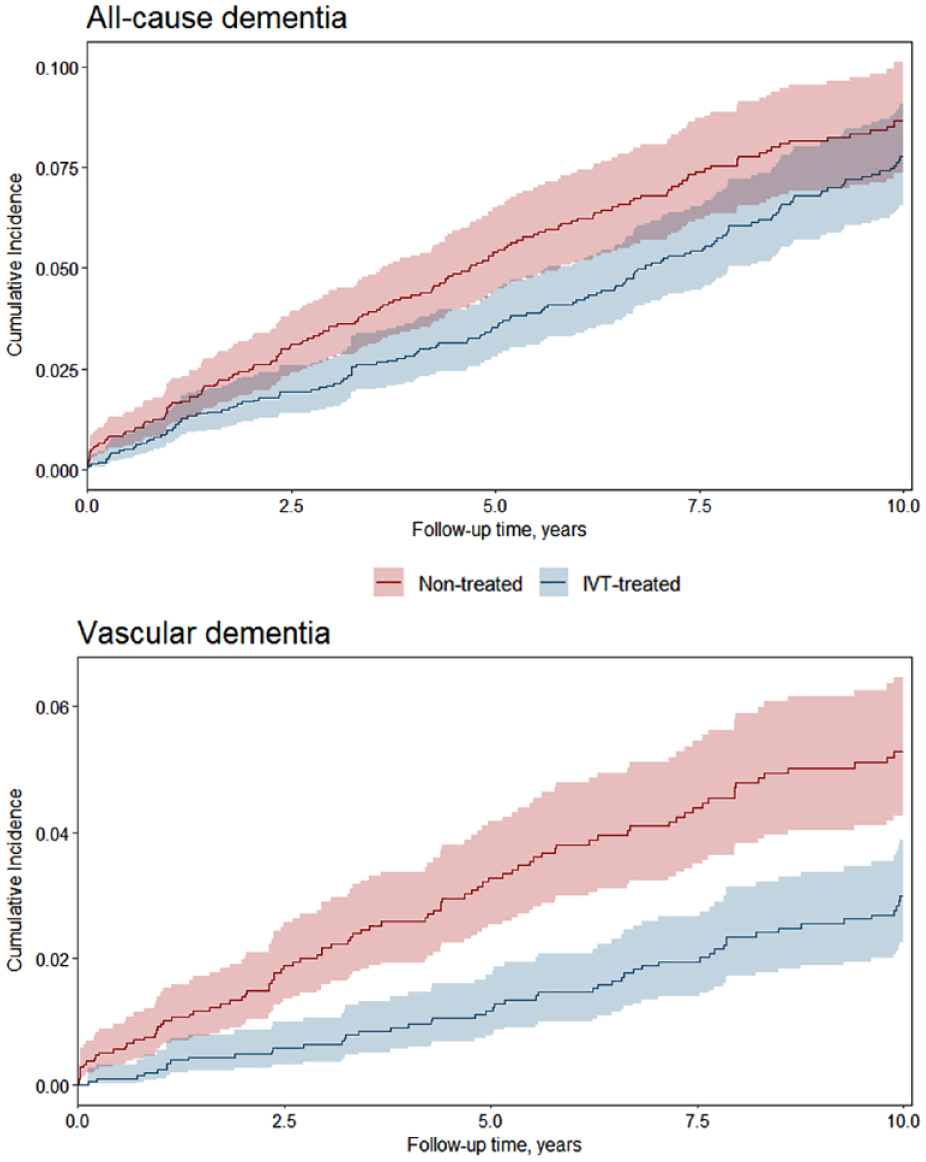
Cumulative incidence curves for all-cause dementia and vascular dementia for the IVT-treated patients (blue, n = 2305) compared with the non-treated patients (red, n = 2305). The curves represent data from one imputed dataset.
Two sensitivity analyses were conducted (Supplemental Table 2). The analysis including only patients with complete data (n = 3464) showed similar results for both all-cause dementia and vascular dementia. When only the IVT-treated patients admitted between 2004 and 2008 were included and matched with non-treated patients, it resulted in a study size of 1212 patients (average across all imputed datasets). The hazard ratios for all-cause and vascular dementia in this population were comparable to those found in the primary analyses, however, the results were not statistically significant.
According to stroke severity, study patients were divided into patients with mild stroke (mean n = 2143) and patients with moderate to severe stroke (mean n = 2467). The stratified analyses showed that IVT treatment for patients with moderate to severe stroke was associated with lower risk of both all-cause dementia and vascular dementia at 2, 5, and 10 years after stroke (Figure 3 and Supplemental Table 3). For patients with mild stroke, the HR for vascular dementia remained in favor of IVT-treatment, however the associations were no longer statistically significant. While the HR for all-cause dementia for patients with mild stroke were in favor of IVT-treatment only 5 years after stroke (Figure 3 and Supplemental Table 3). Analyses of the interaction between IVT treatment and stroke severity showed an interaction between IVT treatment and moderate to severe stroke on the risk of all-cause dementia 10 years after stroke (Supplemental Table 4).
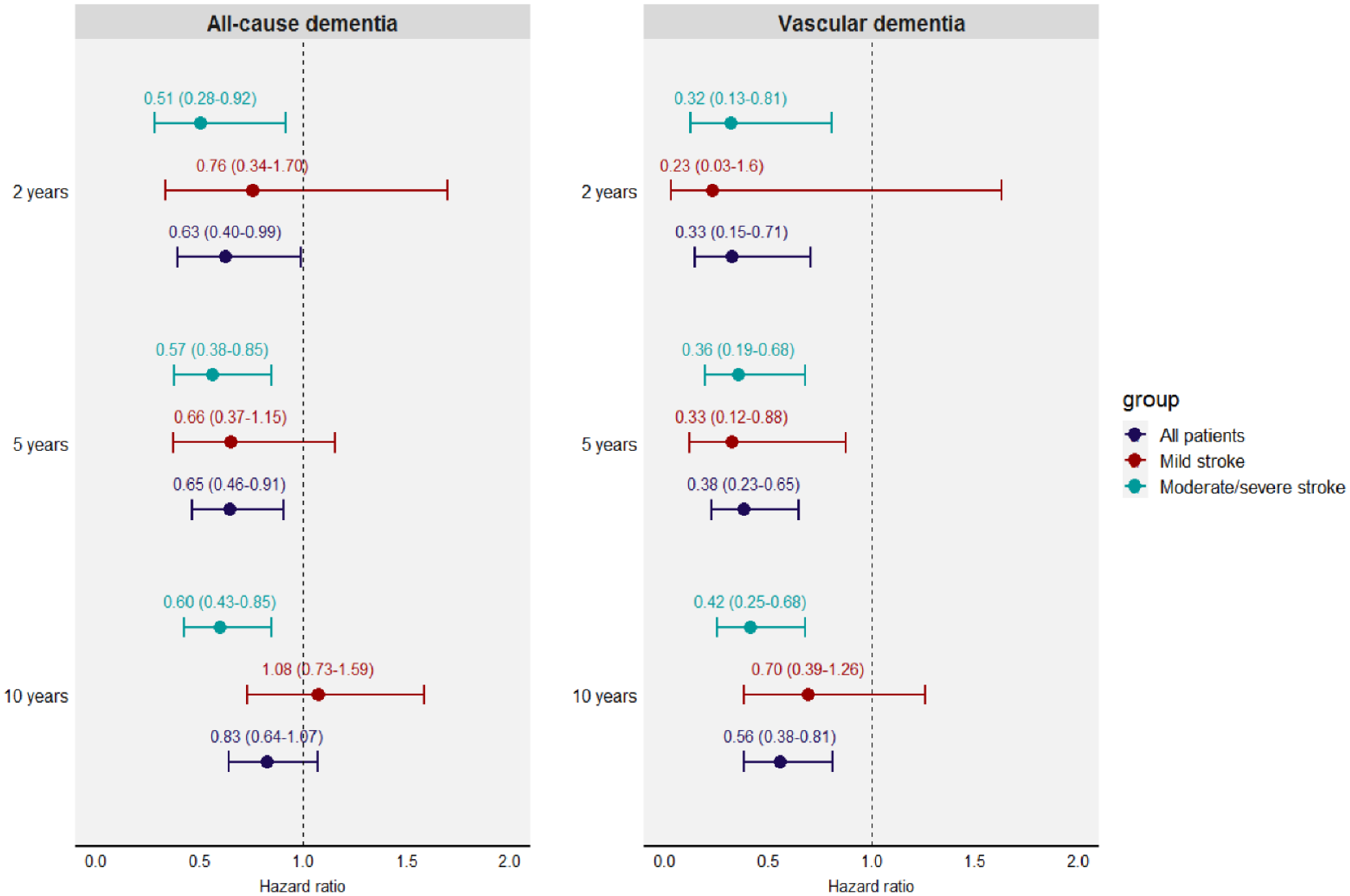
Hazard ratios for all-cause dementia and vascular dementia for IVT-treated compared with non-treated.
Discussion
In this nationwide propensity score-matched cohort study we found that IVT treatment of AIS was associated with up to 37% lower risk of all-cause dementia after stroke. We compared IVT-treated patients with a control group of comparable patients with AIS who did not receive IVT and found that risk of all-cause and vascular dementia was lower for IVT-treated patients up to 10 years after stroke. The associations were observed both among patients with mild and with moderate to severe stroke, though they may be stronger among patients with moderate to severe stroke.
Until recently, only smaller clinical studies have investigated the effect of IVT on post-stroke cognition. Possibly due to small sample sizes (n = 45–92), none of these studies could show an effect.16,30–32 In addition, none included dementia as the outcome. Recently, Cerasuolo et al. published a retrospective cohort study from a regional stroke registry investigating the association between IVT treatment and post-stroke dementia. 17 Similar to our findings, they found that IVT treatment was associated with lower risk of dementia after stroke. We chose to investigate risk of vascular dementia separately, to increase the likelihood that the dementia diagnoses were related to cerebrovascular disease. We could therefore confirm the findings of Cerasuelo et al. in a nationwide cohort and with a more specific vascular dementia endpoint. In addition, we accounted for the important confounding effect of educational level, and presented results stratified by stroke severity.
We found a lower incidence rate of dementia than reported in other studies.2,4–6,17 Several explanations for this finding are possible. Since, initially, IVT was not recommended for individuals older than 80 years, 33 the patients in our matched cohort were relatively young. The mean age was thus 67, potentially making these patients less susceptible to be diagnosed with dementia within 10 years. 34 Secondly, many suffering from dementia are undiagnosed. 35 This diagnosis gap will not be detected in register-based studies in contrast to clinical studies performing cognitive tests. Finally, the NPR only holds records from public hospitals and clinics. We could therefore not account for patients diagnosed at their general practitioner.
A major strength of the study is that it was based on nationwide registers with high external validity and low rates of missing values. Further, the gradual way in which IVT was introduced in Denmark was used to design a natural experiment, allowing us to accurately define a control group of non-treated patients, who would potentially have been IVT-eligible, had they arrived at a stroke center with IVT-services. This, in addition to the propensity score-matched design, reduced risk of selection bias and confounding by indication. Despite the strong design, we cannot rule out risk of residual confounding effects by unmeasurable differences between the two groups. We did not have imaging data on the patients and could therefore not account for lesion location or stroke etiology in the propensity-score model. Moreover, patients with pre-stroke dementia diagnosed at their general practitioner would likely be patients with severe dementia with limited access to dementia clinics. These patients may also be less likely to receive IVT. We tried to limit this bias by excluding nursing home residents. We could not account for patients being diagnosed with dementia at their general practitioner after stroke. However, this potential differential misclassification of post-stroke dementia would likely drive our results toward the null, as we believe that the IVT-treated patients would be more likely to be diagnosed at dementia clinics due to a more thorough post-stroke follow-up.
Another limitation of our study was the differing inclusion periods leading to risk of selection bias. However, the sensitivity analysis of IVT-treated patients admitted 2004–2008 showed similar HR estimates as the main analyses. In addition, the quality of the in-hospital stroke care was comparable between the two groups, further reducing this concern.
As stated, the patients in our study were younger compared with the average stroke population. Further, we do not have specific information on race or ethnicity, although the majority of this Danish stroke cohort are of Northern European descent. This may limit the generalizability of our results and a dementia incidence difference of the same magnitude might not be observed in an older or more ethnic diverse population. Nevertheless, the relative incidence rate estimated by HR may be generalizable. In addition, acute stroke treatment has evolved since 2011, potentially impacting the overall post-stroke dementia incidence rate. On the other hand, this should not impact the proposed effect of IVT on dementia risk.
IVT could have differential effects on dementia risk according to stroke severity or etiology. Results from our stratified analyses indicate that the association between IVT and lower risk of dementia exist across all stroke severities, but that it may be stronger among patients with moderate to severe stroke. However, the study was not powered to detect differences in such subgroups, and we did not have information about stroke etiology to investigate subtypes of stroke. Our results therefore warrant studies of how IVT may affect dementia risk differently according to stroke severity and etiology. Finally, our results encourage the implementation of cognitive measures and post-stroke dementia as outcomes in future stroke trials examining the effects of reperfusion treatments.
In conclusion, IVT treatment for AIS in routine clinical practice was associated with lower risk of all-cause dementia and vascular dementia after stroke. Cognitive outcomes should be considered when evaluating the effects of reperfusion treatments in AIS.
Supplemental Material
sj-docx-2-eso-10.1177_23969873231197530 – Supplemental material for Intravenous thrombolysis for acute ischemic stroke is associated with lower risk of post-stroke dementia: A nationwide cohort study
Supplemental material, sj-docx-2-eso-10.1177_23969873231197530 for Intravenous thrombolysis for acute ischemic stroke is associated with lower risk of post-stroke dementia: A nationwide cohort study by Sigrid Breinholt Vestergaard, Christina C Dahm, Hanne Gottrup, Jan Brink Valentin, Søren Paaske Johnsen, Grethe Andersen and Janne Kærgård Mortensen in European Stroke Journal
Supplemental Material
sj-pdf-1-eso-10.1177_23969873231197530 – Supplemental material for Intravenous thrombolysis for acute ischemic stroke is associated with lower risk of post-stroke dementia: A nationwide cohort study
Supplemental material, sj-pdf-1-eso-10.1177_23969873231197530 for Intravenous thrombolysis for acute ischemic stroke is associated with lower risk of post-stroke dementia: A nationwide cohort study by Sigrid Breinholt Vestergaard, Christina C Dahm, Hanne Gottrup, Jan Brink Valentin, Søren Paaske Johnsen, Grethe Andersen and Janne Kærgård Mortensen in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Aase og Ejnar Danielsens Fond, Central Region Denmark Research Foundation, and Lizzi og Mogens Staal Fonden.
Ethical approval and informed consent
The study was approved by the Danish Data Protection Agency (2019-899/10-0033). According to Danish law neither patient consent nor ethical approval is required for register-based studies.
Guarantor
SBV and JM.
Contributorship
All authors conceived the study. SBV and JV performed the data analyses. SBV wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.