
Abstract
Introduction:
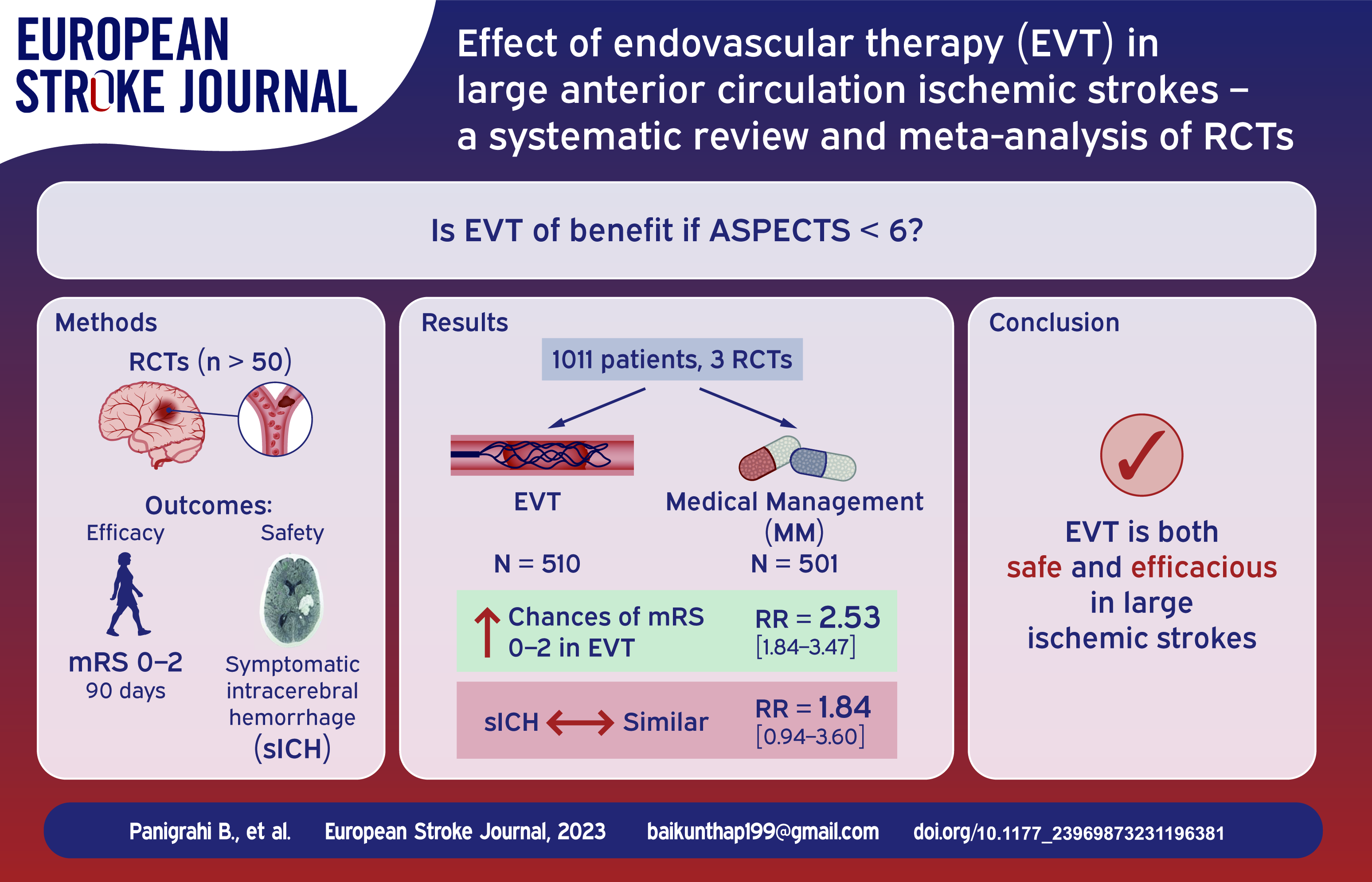
The benefit of endovascular treatment in large anterior circulation ischaemic strokes with low ASPECTS score (<6) is uncertain. Recent randomised studies have demonstrated the benefit of endovascular treatment (EVT) in large ischaemic strokes. The present meta-analysis aims to assess the combined effect of these studies on efficacy and safety of endovascular treatment in this group of patients.
Materials and methods:
We conducted a systematic review and meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. Databases MEDLINE, PubMed, EMBASE, SCOPUS, Google Scholar, Tripdatabase were searched for randomised controlled trials with at least 50 participants from inception until February 16, 2023. The primary efficacy outcome analysed was the relative risk of functional independence defined as mRS – 0–2 at 90 days. Secondary efficacy outcomes included early neurological improvement, death due to any cause at 90 days and proportion of patients requiring decompressive hemicraniectomy. The primary safety outcome was the risk of developing symptomatic intracerebral haemorrhage (sICH).
Results:
A total of three studies (RESCUE Japan-LIMIT, SELECT 2 and ANGEL ASPECTS) involving 1011 patients; 510 in the EVT arm and 501 in the medical management (MM) arm met the defined criteria (ASPECTS-3-5). The combined RR for the primary outcome of mRS 0–2 was 2.53 [1.84–3.47] (p = <0.0001) favouring EVT over MM. The primary safety outcome of sICH was not significant in the EVT arm with a combined RR of 1.84 [0.94–3.60] (p = 0.5157). Mortality rates were similar in both arms (26.67% in EVT arm vs 27.94% in MM arm) with a combined RR of 0.95 [0.78; 1.16] (p = 1.000).
Conclusion:
In patients with Large vessel occlusion (LVO) and low ASPECTS (3–5), EVT was associated with higher likelihood of achieving functional independence and early neurologic improvement but did not provide any mortality benefit.
Background and purpose
Endovascular therapy is currently the standard of care in patients with acute ischaemic stroke due to large vessel occlusion (LVO) and can be considered up to 24 h (in selected patients) from the onset of symptoms. The American Heart Association (AHA)/American Stroke Association (ASA)) 2018 guidelines recommend mechanical thrombectomy with a stent retriever or direct aspiration in the 0–6 h window period if patients meet defined criteria including ASPECTS of ⩾6. 1 In the 6–24 h window, endovascular therapy is recommended in patients meeting the DAWN 2 or DEFUSE3 3 eligibility criteria.
The benefit and safety of endovascular therapy (EVT) in patients with acute ischaemic strokes in the anterior circulation with a large infarct (ASPECTS < 6) is an important knowledge gap in current stroke management guidelines. Such patients are usually managed conservatively and decompressive surgery is advised if they deteriorate clinically or radiologically. 4 The futility of EVT in these cases is based on assumptions rather than evidence as most of these patients have traditionally been excluded from trials of EVT. There has been an interest in offering EVT in large strokes after observational studies showed benefit of EVT in the ASPECTS 3–5 group. The present systematic review assesses the current evidence from randomised controlled trials on the efficacy of EVT in patients with large anterior circulation strokes due to Large Vessel Occlusion (LVO). The objective of the study in the PICO format is summarised in the Supplemental Material (eTable).
Materials and methods
Overview
We used the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement for reporting systematic reviews and meta-analyses as a guide for this study. The protocol for the review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) database. (CRD42023400675).
Selection criteria
Inclusion criteria of the studies were randomised controlled trials with a minimum sample size of 50, age >18 years, baseline mRS-0–1, acute ischaemic stroke within 24 h of last known well, NIHSS > 6, strokes involving the anterior circulation, large infarct core defined as an Alberta Stroke Program Early Computed Tomography (ASPECT) Score of 5 or below or a core volume of >70 mL on computed tomography perfusion or diffusion-weighted magnetic resonance imaging, use of endovascular therapy with any device with or without bridging IV Thrombolytic agent and articles written in English language. Exclusion criteria for the studies were observational cohort studies, case series, unavailable primary efficacy and safety outcome data (modified Rankin scale at 90 days and rates of symptomatic Intracranial haemorrhage(sICH)).
Data extraction
A comprehensive preliminary search was performed by two authors (BP and STH ) independently in the MEDLINE, PubMed, EMBASE, SCOPUS, Google Scholar, Tripdatabase and the Cochrane databases from inception until February 16, 2023 for the identification of published literature on the topic and also to confirm the absence of any published previous systematic reviews and meta-analyses, and any ongoing systematic review and meta-analysis on the same topic in PROSPERO using the following MeSH terms – Endovascular treatment, Mechanical Thrombectomy, Endovascular therapy, Revascularisation, Reperfusion, Ischaemic Stroke, Acute, Ischaemic Stroke, Large Vessel Occlusion, ASPECTS, Large core, modified Rankin Scale with filters to include only Randomised Controlled Trials (RCT). Duplicates were removed after identification. Titles and abstracts were reviewed independently by two authors (BP and STH) to evaluate for inclusion and screening of full text. Any discrepancy was resolved by the third author (RB). Full texts were retrieved for further consideration for inclusion in the study. We did not have access to individual patient data sets of the studies included.
Outcomes
The primary efficacy outcome extracted was the relative risk of functional independence defined as mRS – 0–2 at 90 days. Secondary efficacy outcomes extracted were Early neurological improvement (ENI) defined as a decrease in NIHSS by 8 points or more or 0–1 if NIHSS < 8 at 24–36 h, death due to any cause at 90 days and the proportion of patients requiring decompressive hemicraniectomy at any time post the intervention or on standard medical care. The primary safety outcome extracted was the risk of developing symptomatic ICH defined as per the respective study definition. Other explanatory variables studied were the rates of systemic thrombolysis used and effect on outcomes.
Assessment of risk of bias
After the selection of the relevant studies, the data was extracted on MS Excel by two authors independently (BP and STH). The information extracted were: the first author of the study, year of publication, number of patients, age at diagnosis, baseline characteristics of the patients, mRS outcomes at 3 months, NIHSS at 24 h, risk of symptomatic ICH, need for decompressive surgery and mortality. Any discrepancy among the observers was resolved in consultation with the third author (RB). The ROB2 tool was used to assess the risk of bias of the studies included.
Statistical analysis
Statistical analyses were performed using R project for statistical computing; https://www.r-project.org/. Both fixed and random-effects models were used in view of expected heterogeneity to be present due to known differences in stroke patient characteristics and symptom definitions. The overall effect estimate and 95% CI were used to generate Forrest plots. Statistical heterogeneity was assessed by the Higgin I2 statistics. We considered study-level estimates to be heterogeneous if the I2 value was >50% I2 from 50% to 75% was considered as substantial heterogeneity, and I2 >75% was indicated as considerable heterogeneity.
We did not explore further possible causes of heterogeneity among study results and also we did not do subgroup analysis or meta-regression due to limited number of studies and data variables.
We conducted a sensitivity analyses to assess robustness of the synthesized results by performing leave one study out analysis and presenting a consolidated result for the primary outcome. Certainty in the body of evidence was judged using the GRADE CRITERIA (Table 1) (https://www.gradeworkinggroup.org/).
GRADE tool for certainty of evidence.
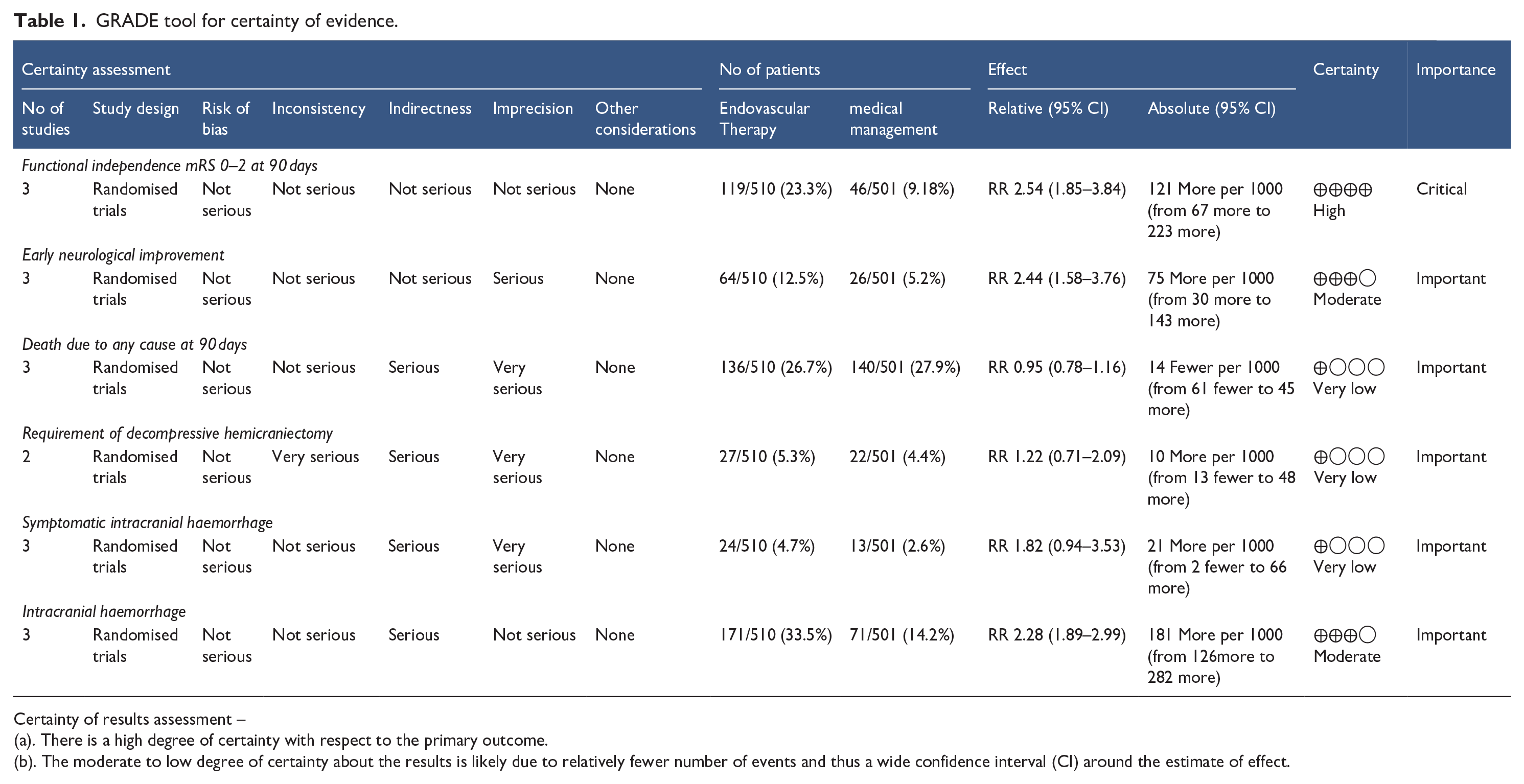
Certainty of results assessment –
(a). There is a high degree of certainty with respect to the primary outcome.
(b). The moderate to low degree of certainty about the results is likely due to relatively fewer number of events and thus a wide confidence interval (CI) around the estimate of effect.
Results
Study selection
A total of 613 studies were identified and 234 duplicates were removed. Three hundred seventy-nine studies were screened for eligibility of which 341 were excluded as 14 were in languages other than English, 73 were Retrospective studies, 58 were systematic reviews and meta-analysis and 196 studies did not meet inclusion criteria. Thirty-eight studies underwent full text screening and a total of three randomised studies ( RESCUE Japan-LIMIT, 5 SELECT 2 6 and ANGEL ASPECTS 7 ) involving 1011 patients; 510 in endovascular therapy (EVT) arm and 501 in medical management (MM) arm met the defined inclusion and exclusion criteria. The details are outlined in the PRISMA flowchart (Figure 1).
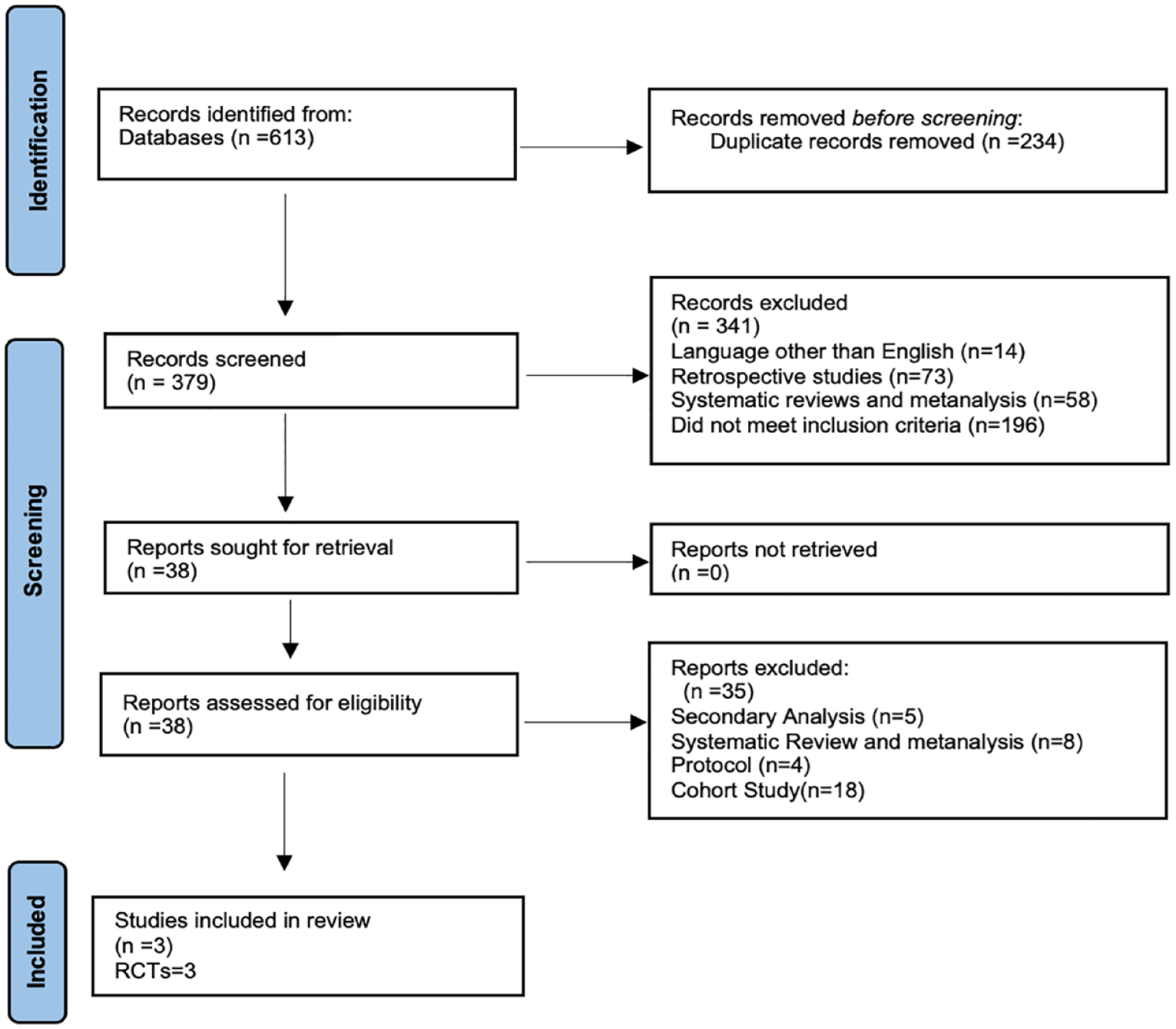
PRISMA flowchart.
Study characteristics
The baseline characteristics of the patients included in the studies are summarised in Table 2. No significant differences in the baseline characteristics were seen among the EVT and MM arms in the studies included. The rates of IV thrombolysis ranged from 17.2% to 28.6% among patients included across groups.
Baseline characteristics of the patients included.
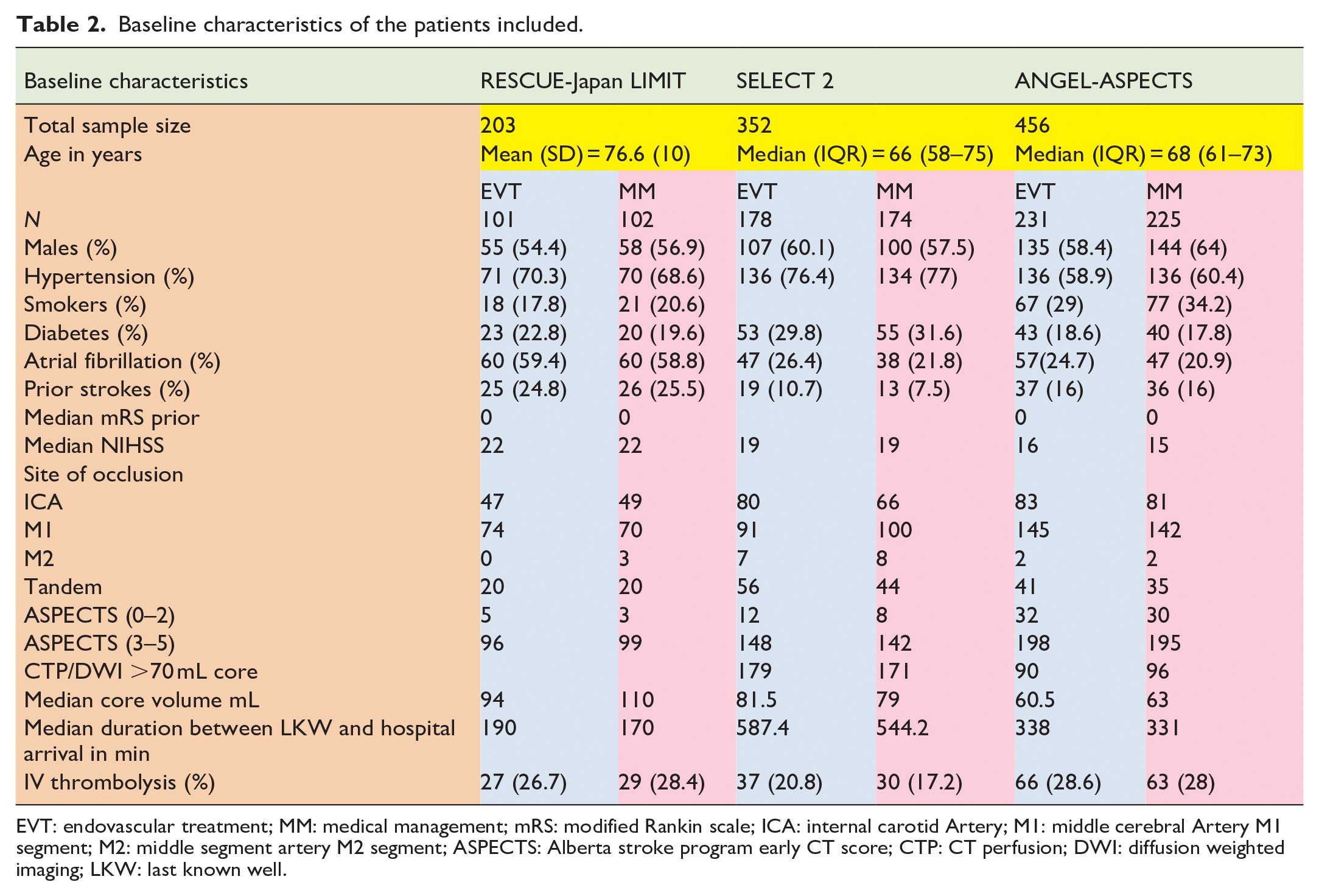
EVT: endovascular treatment; MM: medical management; mRS: modified Rankin scale; ICA: internal carotid Artery; M1: middle cerebral Artery M1 segment; M2: middle segment artery M2 segment; ASPECTS: Alberta stroke program early CT score; CTP: CT perfusion; DWI: diffusion weighted imaging; LKW: last known well.
Risk of bias assessment of the included studies
All the three trials included had a low risk of bias in the randomisation domain. There were some concerns in the risk of bias due to deviations from the intended interventions (effect adhering to intervention) as the participants were aware of the intervention and their carers or people delivering the interventions were also aware of intervention groups. There was a low risk of bias in the outcome data as data was available for >95% of the participants in the study. The outcome assessors were blinded to the intervention in all the three trials but there is a possibility of measurement error or misclassification bias as the certification status for measurement of primary outcome was not mentioned explicitly in any of the three trials. The outcome was analysed according to a prespecified plan.
Outcomes
Functional independence mRS 0-2 at 90 days
The primary efficacy outcome of mRS 0–2 at 90 days was achieved in 119/510 (23.3%) patients in the EVT group and 46/501(9.18%) in the MM group (Table 3). The combined relative risk for the primary outcome utilising the fixed and random effects model were 2.54 [1.85–3.48] and 2.53 [1.84–3.47] respectively favouring EVT (p = <0.0001) (Figure 2).
Outcomes of the three trials included.
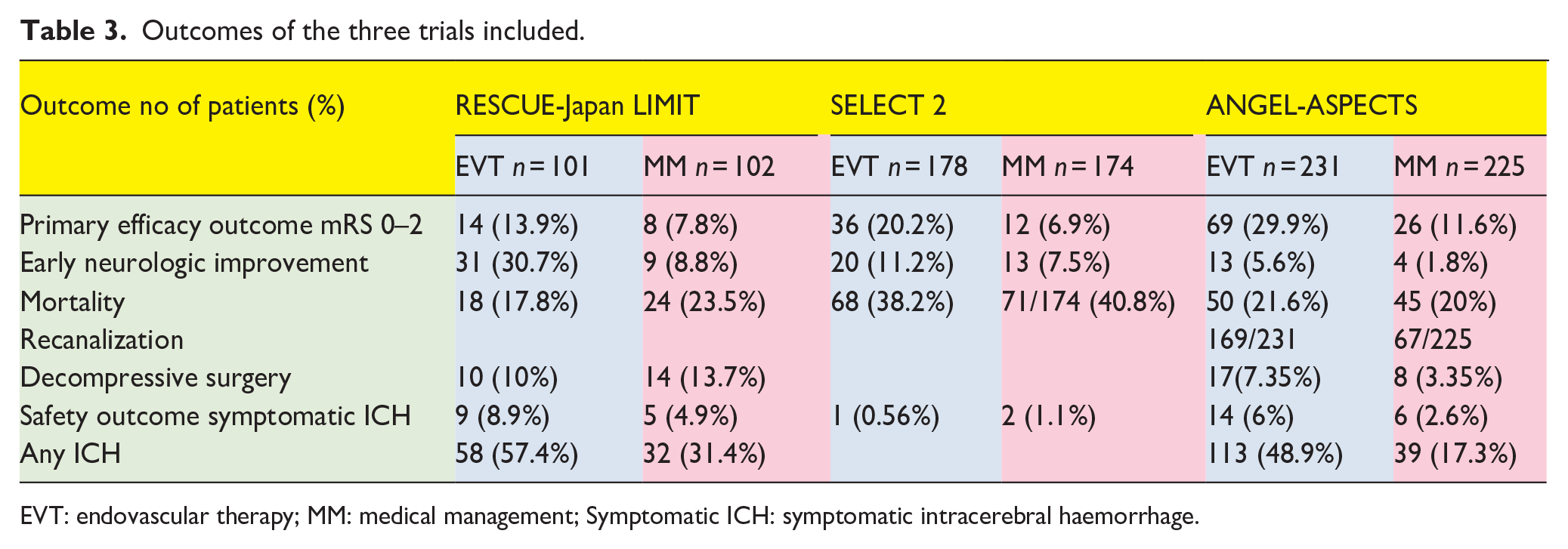
EVT: endovascular therapy; MM: medical management; Symptomatic ICH: symptomatic intracerebral haemorrhage.
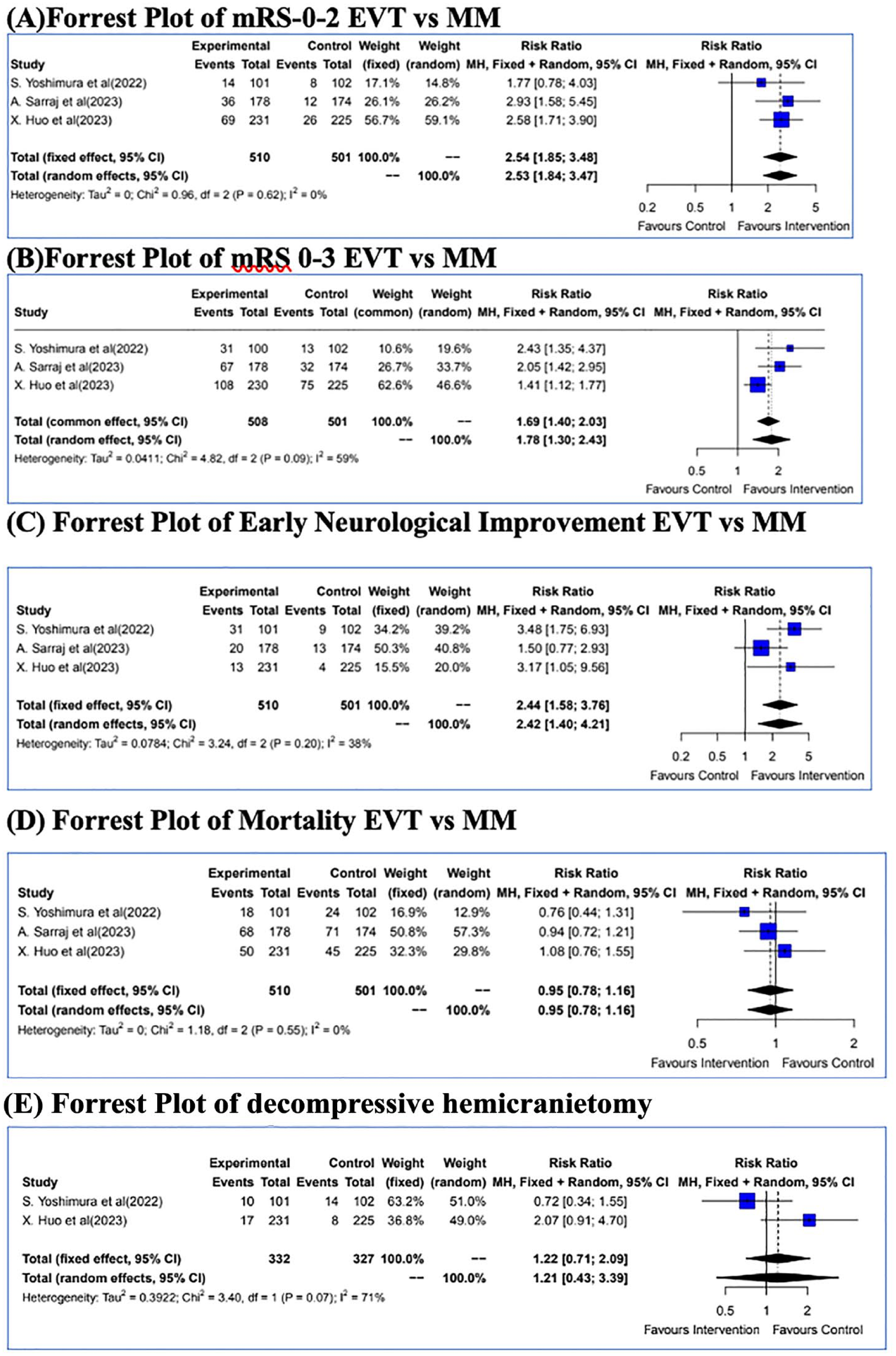
Forrest plot of the efficacy outcomes: (A) Forrest Plot for mRS 0-2; (B) Forrest Plot for mRS 0-3; (C) Forrest Plot for Early Neurological Improvement; (D) Forrest Plot of Mortality; (E) Forrest Plot of decompressive hemicraniectomy.
A mRS 0–3 at 90 days was seen in 206/510 (40.4%) patients in the EVT group and 120/501 (23.9%) patients in the MM arm (Figure 3). The combined RR for this outcome being 1.69 [1.40–2.03] using a fixed and random effects model favouring EVT (p = 0.0007).
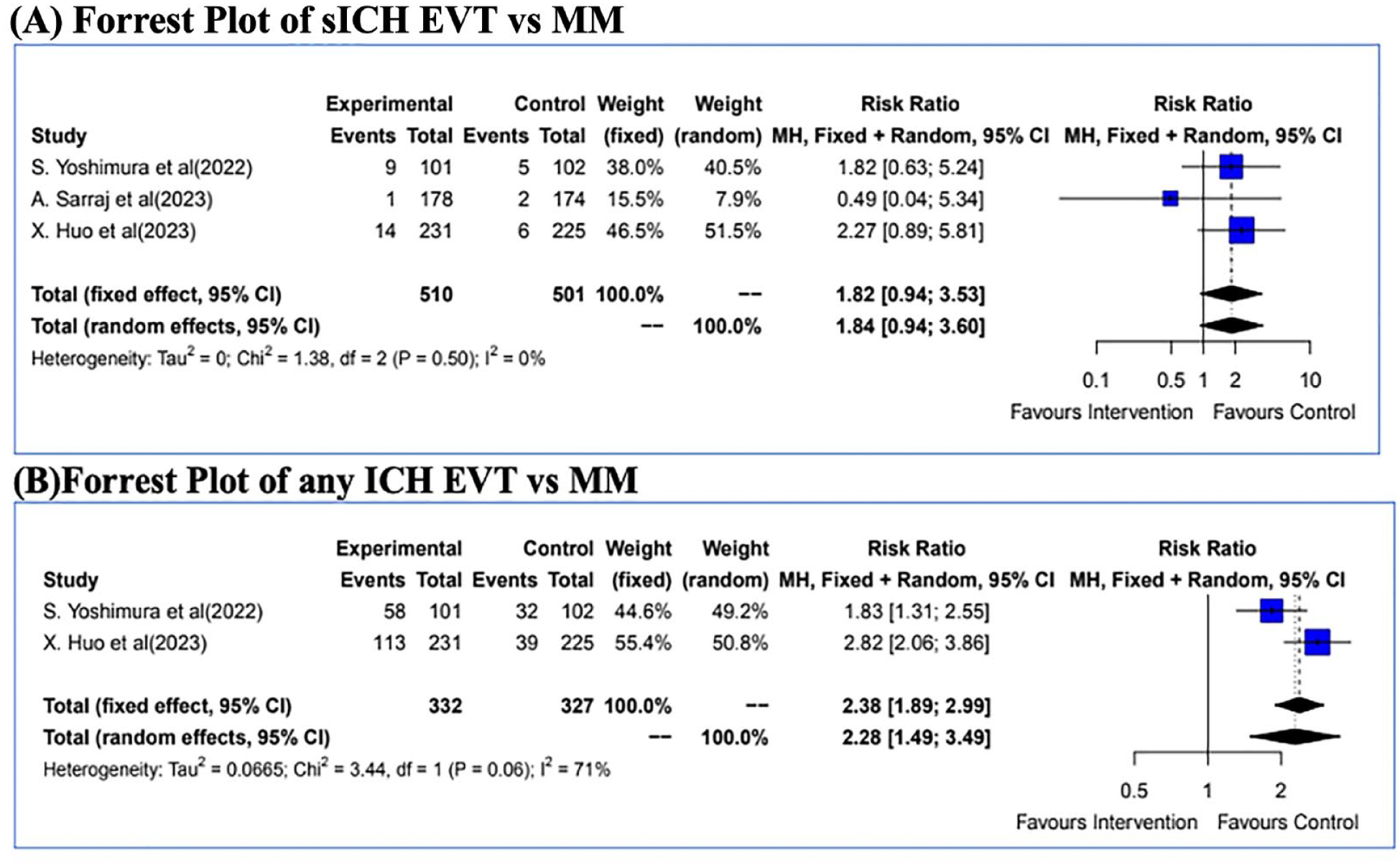
Safety outcomes: (A) Forrest Plot of sICH ; (B) Forrest Plot of any ICH..
Early neurologic improvement (ENI)
The secondary efficacy outcome of early neurologic improvement (ENI) was observed in 64/510 (12.55%) patients in the EVT arm and in 26/501 (5.19%) patients in the MM arm (Table 3).
The combined RR for ENI utilising the fixed and random effect model was 2.44 [1.58–3.76] and 2.42 [1.40–4.21] respectively, favouring EVT (Figure 2).
Death due to any cause at 90 days
A total of 136/510 (26.67%) patients died in the EVT arm as compared to 140/501 (27.94%) in the MM arm with a combined RR of 0.95 [0.78; 1.16] (fixed and random effects models) (p = 1.000) (Figure 2).
Decompressive hemicraniectomy
Decompressive surgery was required in 27/332 (8.13%) patients in the EVT arm as compared to 22/327 (6.72%) patients in the MM arm with a combined RR by fixed and random effects models of 1.22 [0.71–2.09] and 1.21 [0.43–3.39] respectively (p = 1.000).
Symptomatic ICH
The primary safety outcome of symptomatic ICH was seen in 24/510 (4.7%) patients in the EVT arm as compared to 13/501 (2.6%) patients in the MM arm with a combined RR by fixed and random effects models of 1.82 [0.94–3.53] and 1.84 [0.94–3.60] respectively (p = 0.5157) (Figure 3).
Any ICH was seen in 171/332 (51.5%) patients in the EVT arm as compared to 71/327 (21.71%) patients in the MM arm with a combined RR by fixed and random effects models of 2.38 [1.89–2.99] and 2.28 [1.49–3.49] respectively (p = 0.0007).
Thrombolysis
Among a subset of patients undergoing thrombolysis a combined risk ratio of benefit was 3.37 [1.54–7.41] favouring thrombolysis (Figure 4).
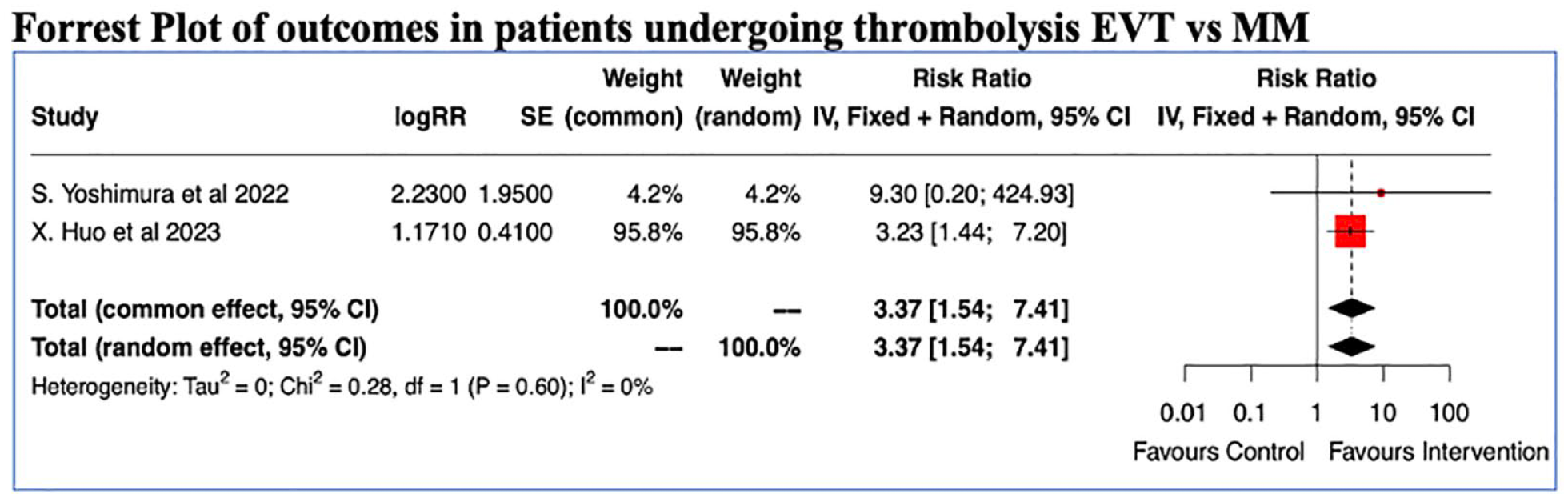
Thrombolysis and EVT outcomes.
Discussion
This analysis provides evidence for the benefit of EVT among patients with large ischaemic strokes involving the anterior circulation. Such patients undergoing EVT are 2.53 times more likely to achieve functional independence as compared to standard medical care. Considering the likelihood of relatively poor prognosis in these patients, a higher chance of achieving mRS of 0–2 is reassuring. (Figure 2) The Absolute risk reduction (ARR) is the absolute difference in outcomes between one group (usually the control group) and the group receiving treatment. The Number Needed to Treat (NNT) is the number of patients you need to treat to prevent one additional bad outcome and is the inverse of ARR. In our study the pooled ARR with EVT for achieving a mRS of 0–2 at 3 months was 14.12% yielding a NNT of 7.1. This is significant considering that the HERMES collaboration demonstrated an absolute risk reduction of 19.5% yielding a NNT of 5.1 for achieving the same outcome. 8 These findings are consistent with a previous meta-analysis including 17 studies and 1378 patients with an ASPECTS 0–6 and a higher odds of mRS 0–2 in the EVT arm (OR 4.76, p = 0.01). 9
Functional Recovery after an ischaemic stroke is dependent not only on the amount of the tissue that can be potentially salvageable but by the location of the infarct as an infarct affecting the corticospinal tracts would lead to a greater motor disability as assessed by the modified Rankin scale. The ASPECTS score assigns similar weightage to both eloquent and non-eloquent cortices and a strategic salvage of the eloquent cortices may explain the benefit of EVT in patients with low ASPECTS. 10 Another issue about the ASPECTS score is its inter-rater agreement which may vary with the site of ischaemia. Areas like the basal ganglia and the insular cortex which may have sharp definitions from the surrounding regions are relatively easy to demarcate compared to other regions. 11 The internal capsule due to its inherent hypoattenuation may be difficult to interpret. The M1-M6 region interpretation may also be limited due to beam hardening artefacts in view of their proximity to the skull.11–14 Furthermore, vulnerability to ischaemic changes due to hypoperfusion varies between different locations of the brain, with the insular cortex, precentral gyrus and basal ganglia being the most sensitive.
Moreover the degree of inter-rater agreement is not known from the published data of the selected trials for the meta-analysis.
An important thing to note is that estimation of core volumes were heterogenous across the studies with some studies using CT perfusion and some using MRI based core estimation. Consider the RESCUE-Japan LIMIT study which included patients with both CT or MRI ASPECTS of 3–5 which is a major source of concern as different imaging modalities have different sensitivities and specificities and therefore are likely to have introduced misclassification bias into the study results. Similarly the SELECT 2 and ANGEL-ASPECTS used CT perfusion, NCCT ASPECTS and ADC based estimation of core volumes which introduces significant bias in the study results. Access to individual patient data and usage of propensity scores could have been useful in generating separate analysis groups utilising different imaging modalities.
Another important predictor of the outcome is the collateral status of the patient although most patients with low ASPECTS have poor collaterals but as many as one-third may present with adequate collaterals. 15 When collateral status was assessed in low ASPECTS patients, those with poor collaterals had a median mRS score of 5 despite successful recanalization, while patients with good collaterals showed a median mRS score of 2 after successful recanalization.16,17Although collateral status information was not mentioned in the trials, it is likely that patients who had a good outcome had good collaterals.
CT Perfusion, particularly in the early time window tends to overestimate the core volume. Theoretically, after sudden stoppage of blood supply to a region in the brain, the cells distal to the arterial occlusion undergo oxygen deprivation, resulting in a compensatory increase in CBF (Cerebral blood flow). Over time, these compensatory mechanisms fail, leading to a progressive decline in CBF and CBV (Cerebral blood volume), with transformation of the penumbra into irreversibly damaged tissue. Due to continued cellular oxygen deprivation, disruption of the blood brain barrier ensues, leading to the influx of ions and subsequently the net water uptake (NWU) a surrogate marker of vasogenic cerebral oedema. A high NWU would indicate a greater vasogenic oedema and more likely to have a poor outcome with recanalization. In patients with large CBV deficits, but low NWU, the compensatory mechanisms are largely maintained and the core lesion is likely ‘reversible’. On the other hand, those with large CBV lesions and high NWU have more likely crossed the threshold into irreversible tissue damage. This is known as the ‘ghost infarct core’ phenomenon, and is particularly common in the early time window. 18 NWU can be assessed using a NCCT scan using special analytical software programmes and basically quantifies the reduction in Hounsfield units and when taken together to CTP-based core estimation could provide a more accurate picture of both lesion size and stage of infarction at admission. 18 In a previous study, core-overestimation was more likely to occur in patients with large perfusion cores and low NWU at baseline. This could have possibly occurred in the trials as a subgroup of patients might have had a low NWU at baseline and thus high overestimated cores and could likely have benefitted from recanalization. 18
SELECT2 and ANGEL-ASPECTS studies were prematurely terminated and may have led to an overestimation of benefit as the target sample size was smaller than anticipated and underpowered for subgroup analyses. The benefit of EVT in patients of extremely poor ASPECTS (0–2) is still remains unknown due to inadequate number of patients in the 0–2 group and the lack of outcome data in the group for analysis.
Although the absolute reasons for benefit of EVT in large strokes remains elusive, further studies are needed to know which subset of these large strokes are more likely to benefit from EVT.
Changing the yardstick of outcomes changes the risk ratios as can be seen in the Forrest plots. (Figure 2) The primary outcome for the RESCUE-Japan LIMIT was mRS of 0–3 whereas the other trials used a shift analysis for the primary outcome. This is the reason why the outcome results in the mRS 0–3 are better than in mRS 0–2. Considering that large infarcts are likely to be associated with poor prognosis a mRS of 0–3 may also be an acceptable outcome as has also been used in trials in Intracerebral Haemorrhage (ICH).19,20
Safety was demonstrated in previous meta-analysis and the results of the present study confirms that the rates of symptomatic ICH were same in both arms although the risk of any ICH was higher in the EVT arm. However, interpretation of safety results also warrant caution as symptomatic intracranial haemorrhage was defined differently across trials. The SELECT2 for example defined symptomatic intracranial haemorrhage as parenchymal haematoma associated with at least a 4-point increase in the NIHSS score within 24 h whereas the RESCUE-Japan LIMIT used the same assessment within 48 h and the ANGEL-ASPECTS used the Heidelberg bleeding classification of intracranial haemorrhage within 48 h. 21 A uniform definition across trials would have been better for comparing the safety outcomes in this study.
Another factor with respect to the safety benefit of EVT in low ASPECTS patients could be related to the reduction of brain oedema and malignant mass effect, leading to reduced rates of decompressive hemicraniectomy.22,23
An interesting point to note is that even in patients with a low ASPECTS thrombolysis was associated with good outcome contrary to the assumptions. (Figure 4) Although definite conclusions cannot be drawn from the present study in view of the analysis based on the relative risks and the absolute numbers and individual patient data was not available for knowing recanalization rates the study does provide some insights into safety of Intravenous Thrombolysis in this often excluded group of patients. Large scale studies are needed to conclusively prove benefit.
We conducted the analysis of the evidence for the outcomes using the GRADE methodology and it showed high certainty of the intervention with respect to the primary outcome that is, functional independence mRS 0–2 at 90 days.
The limitation of this study is the non-representation of observational studies and we did not have access to individual patient data that would have provided evidence for subgroups of patients likely to benefit from EVT.
Conclusion
In patients with LVO and low ASPECTS (3–5), EVT within 24 h of onset was associated with higher likelihood of achieving functional independence and early neurologic improvement but did not provide any mortality benefit in patients with large ischaemic core The rates of symptomatic ICH were similar in both the groups whereas the risk of any ICH was significantly higher in the EVT arm.
Supplemental Material
sj-docx-1-eso-10.1177_23969873231196381 – Supplemental material for Effect of endovascular therapy in large anterior circulation ischaemic strokes: A systematic review and meta-analysis of randomised controlled trials
Supplemental material, sj-docx-1-eso-10.1177_23969873231196381 for Effect of endovascular therapy in large anterior circulation ischaemic strokes: A systematic review and meta-analysis of randomised controlled trials by Baikuntha Panigrahi, Subhangi Thakur Hameer, Rohit Bhatia, Partha Haldar, Agrata Sharma and Madakasira Vasantha Padma Srivastava in European Stroke Journal
Supplemental Material
sj-docx-2-eso-10.1177_23969873231196381 – Supplemental material for Effect of endovascular therapy in large anterior circulation ischaemic strokes: A systematic review and meta-analysis of randomised controlled trials
Supplemental material, sj-docx-2-eso-10.1177_23969873231196381 for Effect of endovascular therapy in large anterior circulation ischaemic strokes: A systematic review and meta-analysis of randomised controlled trials by Baikuntha Panigrahi, Subhangi Thakur Hameer, Rohit Bhatia, Partha Haldar, Agrata Sharma and Madakasira Vasantha Padma Srivastava in European Stroke Journal
Footnotes
Acknowledgements
None.
Author’s note
The protocol for the review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) database (CRD42023400675).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable as the study is a meta-analysis.
Informed consent
Not applicable as the study is a meta-analysis.
Guarantor
BP.
Contributorship
BP and RB conceived the study. BP, STH, RB major role in acquisition of data, data interpretation, drafting of the initial manuscript editing and submission. PH did the data analysis, manuscript review and editing. AS and MVP did manuscript review and editing. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.