
Abstract
Introduction:
Hydrocephalus after aneurysmal subarachnoid haemorrhage (aSAH) is a common complication which may lead to insertion of a ventriculoperitoneal shunt (VPS). Our aim is to evaluate a possible influence of specific clinical and biochemical factors on VPS dependency with special emphasis on hyperglycaemia on admission.
Patients and methods:
Retrospective analysis of a monocentric database of aSAH patients. Using univariable and multivariable logistic regression analysis we evaluated factors influencing VPS dependency, with a special focus on hyperglycaemia on blood sample within 24 h of admission, dichotomised at 126 mg/dl. Factors evaluated in the univariable analysis were age, sex, known diabetes, Hunt and Hess grade, Barrow Neurological Institute scale, treatment modality, extra-ventricular drain (EVD) insertion, complications (rebleeding, vasospasm, infarction, decompressive craniectomy, ventriculitis), outcome variables and laboratory parameters (glucose, C-reactive protein, procalcitonin).
Results:
We included 510 consecutive patients treated with acute aSAH requiring a VPS (mean age 58.2 years, 66% were female). An EVD was inserted in 387 (75.9%) patients. In the univariable analysis, VPS dependency was associated with hyperglycaemia on admission (OR 2.56, 95%CI 1.58–4.14, p < 0.001). In the multivariable regression analysis after stepwise backward regression, factors associated with VPS dependency were hyperglycaemia >126 mg/dl on admission (OR 1.93, 95%CI 1.13–3.30, p = 0.02), ventriculitis (OR 2.33, 95%CI 1.33–4.04, p = 0.003), Hunt and Hess grade (overall p-value 0.02) and decompressive craniectomy (OR 2.68, 95%CI 1.55–4.64, p < 0.001).
Conclusion:
Hyperglycaemia on admission was associated with an increased probability of VPS placement. If confirmed, this finding might facilitate treatment of these patients by accelerating insertion of a permanent draining system.
Introduction
Aneurysmal subarachnoid haemorrhage (aSAH) is a bleeding into the subarachnoid space with a high mortality and morbidity.1,2 Several factors influence morbidity and therefore outcome after aSAH. Some of these factors are rebleeding, cerebral vasospasm (CVS), delayed cerebral ischaemia (DCI), cerebral infarcts and hydrocephalus. 1 Hydrocephalus is a well-known complication after aSAH. 1 It is thought to occur due to arachnoid adhesions or meningeal fibrosis caused by blood in the subarachnoid space, leading to an impaired cerebrospinal fluid (CSF) absorption with inflammation also playing a significant role in hydrocephalus development. 3 Hydrocephalus is associated with an increased risk of cognitive impairment, memory difficulties and therefore poor clinical outcome.4,5 As such, hydrocephalus is associated with a significant increase in morbidity and mortality in aSAH patients and warrants treatment, preferably early. In acute hydrocephalus diversion of the CSF is conducted via insertion of an extra-ventricular drain (EVD). If patients cannot be weaned and hydrocephalus persists a permanent system needs to be inserted, such as a ventriculo-peritoneal shunt (VPS). Incidence of post aSAH hydrocephalus has been reported to lie between 6% and 67%, up to 50% of patients end up needing a VPS.6–13 Several risk factors such as increased age, female sex, rebleeding, intraventricular haemorrhage, higher Fisher and Hunt and Hess (HH) grades have been reported.14–18 Only a few studies have looked at the association between hyperglycaemia and future VPS dependency and even less evaluated hyperglycaemia on admission.9–11 Hyperglycaemia after aSAH is common and most likely due to humeral activation including catecholamine release altering homoeostasis.19,20 VPS dependency due to hyperglycaemia might be due to several mechanisms such as inflammation, disruption of immune function and disruption of endothelial function.21–23 A previous study showed a strong correlation between hyperglycaemia on admission and hydrocephalus and suggested the affection of the neurohumoral pathway as an underlying mechanism. 24 All of these would lead to a decreased CSF resorption and in the end, if persistent, VPS dependency which potentially influences functional outcome after aSAH. A previous study has already established an association between hyperglycaemia and acute CSF reportion. 25 If hyperglycaemia is indeed established as an influencing factor on VPS dependency this could provide us with a potential treatment target (by influencing glucose levels).
Our aim was to assess the influence of hyperglycaemia and other clinical and biochemical factors on VPS dependency in patients with aSAH.
Patients and methods
Population
We included patients with aSAH who were prospectively and retrospectively recruited into our hospital-based aSAH registry between March 2006 and 2021. We excluded patients below the age of 18 years as well as patients deemed too poor to receive treatment for the ruptured aneurysm, patients with a subarachnoid haemorrhage due to another underlying cause such as, but not limited to, perimesencephalic or traumatic subarachnoid haemorrhage, aSAH due to arteriovenous malformation or mycotic aneurysm. We only included patients who were directly referred to our institution after the acute event excluding patients who were referred to our department after being treated in a different institution (Figure 1).
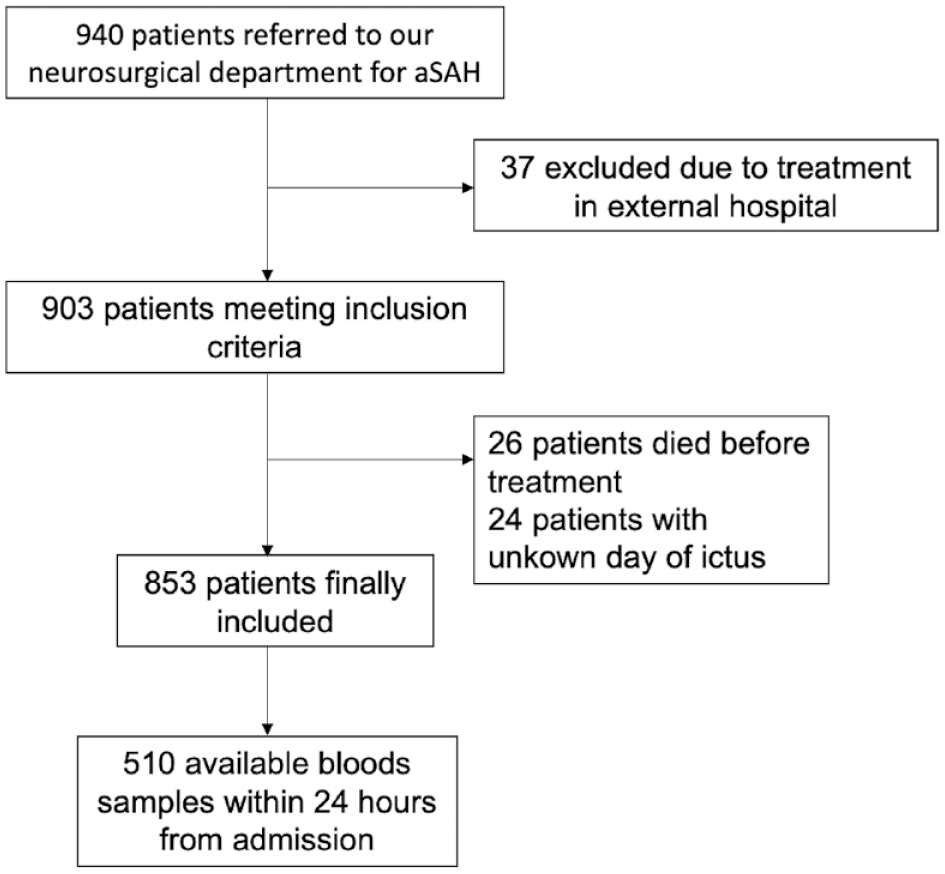
Patient flow chart.
Radiological data
Hydrocephalus was defined as an enlargement of the ventricular system which requires intervention by insertion of an EVD or lumbar drain (LD). 26 Patients who were not able to be weaned from an EVD or LD (deteriorating clinically when drainage amount was reduced, or EVD/LD closed and enlargement of the ventricles on imaging was shown) or patients who developed hydrocephalus later during the course (showing typical clinical signs as well as imaging findings) and improved clinically after lumbar puncture received a VPS.
We defined rebleeding as a repeated haemorrhage occurring from the ruptured aneurysm. Rebleeding had to be proven by imaging or mentioned in the neuroradiologist report. We defined symptomatic CVS as increase in flow velocity in transcranial cerebral doppler or when seen on digital subtraction angiography, CT angiography or MR angiography in conjunction with neurological symptoms. 27 We further defined cerebral infarction as radiologically visible infarcts not associated with any intervention within a 48 h time frame. 28 The Barrow Neurological Institute (BNI) scale was assessed as previously described. 29
Laboratory data
We defined hyperglycaemia on admission as a glucose value of >126 mg/dl within 24 h of admission as per previous studies and dichotomised it accordingly. 11 As EVD was inserted on different time points, we pre-specified the maximum glucose value in the CSF as the parameter of interest for the subgroup analysis in patients with available CSF. Our institution did not assess blood or CSF values at pre-specified time points when this study was conducted.
Shunt insertion
In our institution shunt insertion, usually referring to the insertion of a ventriculo-peritoneal shunt, is performed by inserting a proximal catheter into the lateral ventricle, usually using a right frontal approach, and tunnelling the catheter down to the right upper abdominal quadrant with insertion into the intraperitoneal space. As a standard, we use adjustable valves in order to be able to adapt to changes in a patients need in the volume of CSF to be drained. All patients undergoing VPS insertion received postoperative imaging to check the correct position of the shunt and exclude intraoperative complications. Timing of VPS insertion was not fixed but dependent on weaning success as well as protein levels in CSF which had to be <2 g/l. As is commonly known, if CSF protein levels are too high the shunt valve will get blocked. 30
Statistical analysis
We present continuous variables as mean with standard deviation (SD) in case of normal distribution or median with interquartile range (IQR) in case of non-normal distribution and categorical variables as count and percentage.
For the prediction of VPS dependency variables for multivariable analysis were chosen based on the univariable analysis and previous studies as well as plausibility. We adjusted the multivariable analysis with the prespecified variables age, sex, hyperglycaemia on admission, BNI Grading Scale to adjust for haemorrhage load as well as variables with a p-value of ⩽0.2 in the univariable analysis. The analysis focussed on early prediction of VPS dependency. After creating the initial model, we conducted a stepwise backward elimination regression analysis removing variables with a p-value of ⩾0.2. As a sensitivity analysis we conducted a propensity score matching to reduce the effect of confounders. We also conducted a sensitivity analysis by replacing hyperglycaemia on admission with the maximal glucose value during hospitalisation.
The level of statistical significance was set at 5% (p-value = 0.05). Statistical analysis was performed using STATA 15 (StataCorp. 2011. Stata Statistical Software: Release 15. College Station, TX: StataCorp LP).
Ethical approval
The study was approved by the local Research Ethics committee (186/20S). As no patient identifiable data is presented, no specific patient consent was needed for this retrospective study. This study follows the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Results
Baseline characteristics and univariable analysis are summarised in Table 1. We included a total of 510 aSAH patients with available laboratory data on admission: mean age was 58.3 years and 338 (69.6%) were female. Three hundred and fifty-five (69.6%) patients had hyperglycaemia >126 mg/dl within 24 h of admission. Twenty-five patients (4.9%) were known diabetic.
Patients demographics overall, with and without VPM dependency.
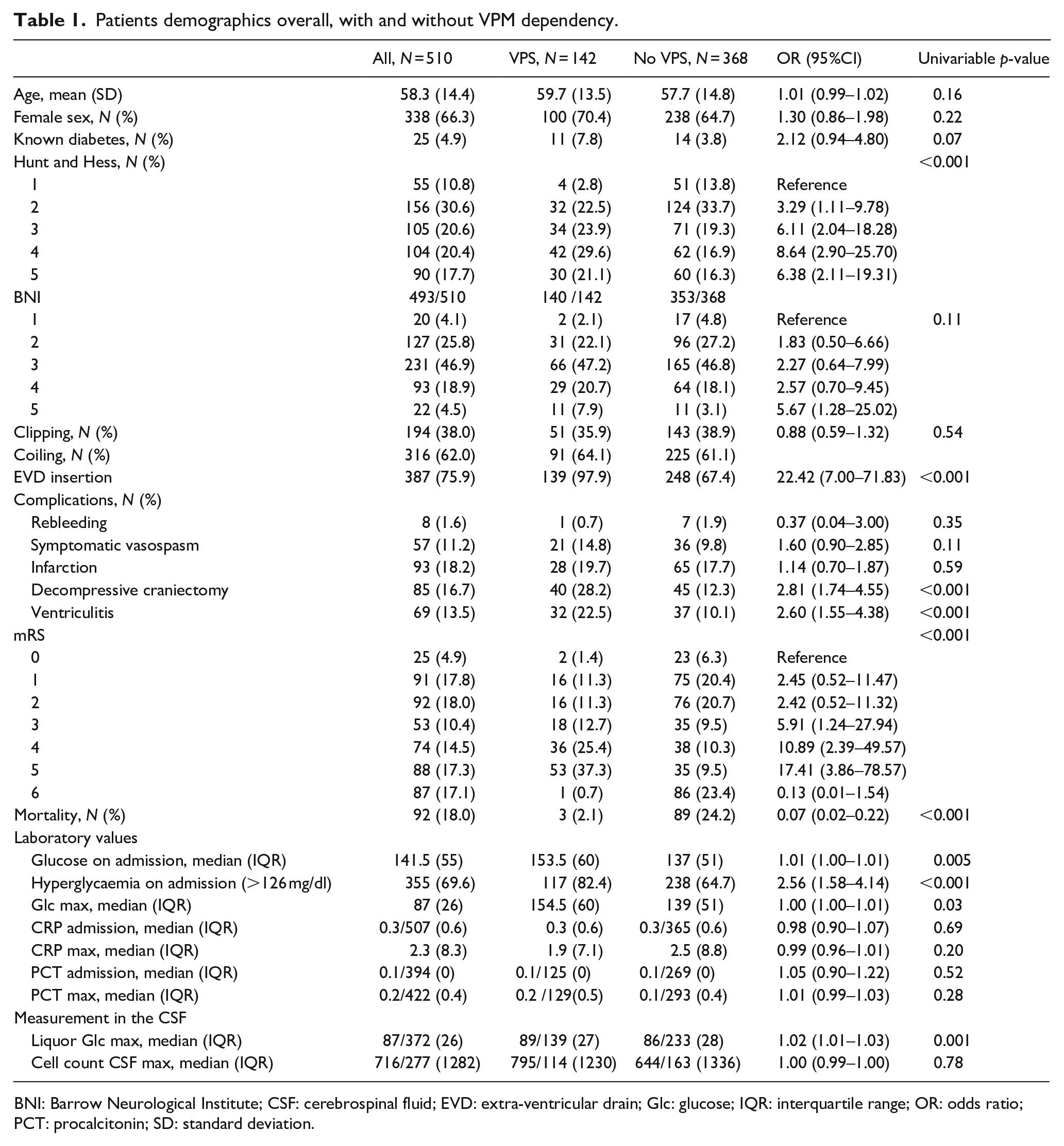
BNI: Barrow Neurological Institute; CSF: cerebrospinal fluid; EVD: extra-ventricular drain; Glc: glucose; IQR: interquartile range; OR: odds ratio; PCT: procalcitonin; SD: standard deviation.
Association of clinical and radiographic factors with ventriculo-peritoneal VPS dependency after aneurysmal SAH
In the univariable analysis (Table 1), factors associated with VPS dependency were: HH grade (increased likelihood of VPS dependency per HH grade, overall p-value <0.001), EVD insertion (OR 22.42, 95%CI 7.00–71.83, p < 0.001), decompressive craniectomy (OR 2.81, 95%CI 1.74–4.55, p < 0.001) and ventriculitis (OR 2.60, 1.55–4.38, p < 0.001).
Due to the correlation of EVD and VPS dependency we did not include EVD insertion into the multivariable model.
Influence of hyperglycaemia on admission on long-term ventriculo-peritoneal VPS dependency
Hyperglycaemia on admission dichotomised into >/<126 mg/dl was associated with VPS dependency (OR 2.56, 95%CI 1.58–4.14, p < 0.001). When evaluating glucose on admission as a continuous variable, it remained significantly associated with VPS dependency (OR 1.01, 95%CI 1.01–1.01, p = 0.005) indicating that likelihood of VPS dependency increases by 1.01 by each point of increase of glucose level. Similarly, maximal glucose during hospitalisation was associated with VPS dependency (OR 1.02, 95%CI 1.01–1.03, p = 0.04). In the propensity score matching adjusting for the same variables as in the multivariable model, dichotomised hyperglycaemia was significantly associated with VPS dependency (OR 1.11, 95%CI 1.00–1.22, p = 0.04).
In the subgroup of patients with available CSF (n = 365), maximum glucose level in the CSF was significantly associated with VPS dependency (OR 1.02, 95%CI 1.01–1.03, p < 0.001). As this measurement was not standardised and could be taken throughout the whole hospitalisation this was not included in the multivariable analysis.
Neither C-reactive protein nor procalcitonin levels on admission were associated with long-term VPS dependency (Table 1). We did also not find a significant association of VPS dependency by CSF cell count.
VPS dependency and outcome
The likelihood of permanent VPS dependency increased by increasing grade on the modified Rankin Scale (mRS, Table 1) except for mRS 6. Shunt insertion was associated with a decreased mortality (OR 0.07) while hydrocephalus was not associated with mortality (OR 1.02, 0.65–1.61, p = 0.93). Patients with a permanent VPS dependency had a longer hospital stay, measured in days, compared to those without permanent VPS dependency (OR 1.08, 95%CI 1.06–1.10, p < 0.001) and only three patients who died underwent VPS insertion.
Building a multivariable model
The initial multivariable model is presented in Table 2. We then conducted a stepwise backward elimination regression analysis and present our final multivariable model in Table 3. Dichotomised hyperglycaemia on admission (OR 2.02, 95%CI 1.19–3.44, p = 0.009), HH grade (overall p-value 0.01), ventriculitis (OR 2.36, 95%CI 1.36–4.11, p = 0.002) and decompressive craniectomy (OR 2.82, 95%CI 1.60–4.97, p < 0.001) were significantly associated with VPS dependency in the multivariable analysis. Except for HH grade 5, HH showed a gradual increase in OR with increasing grade compared to the reference group of HH 1. There was no significant interaction between hyperglycaemia and ventriculitis (p = 0.85).
Multivariable analysis for ventriculo-peritoneal VPS dependency prediction.
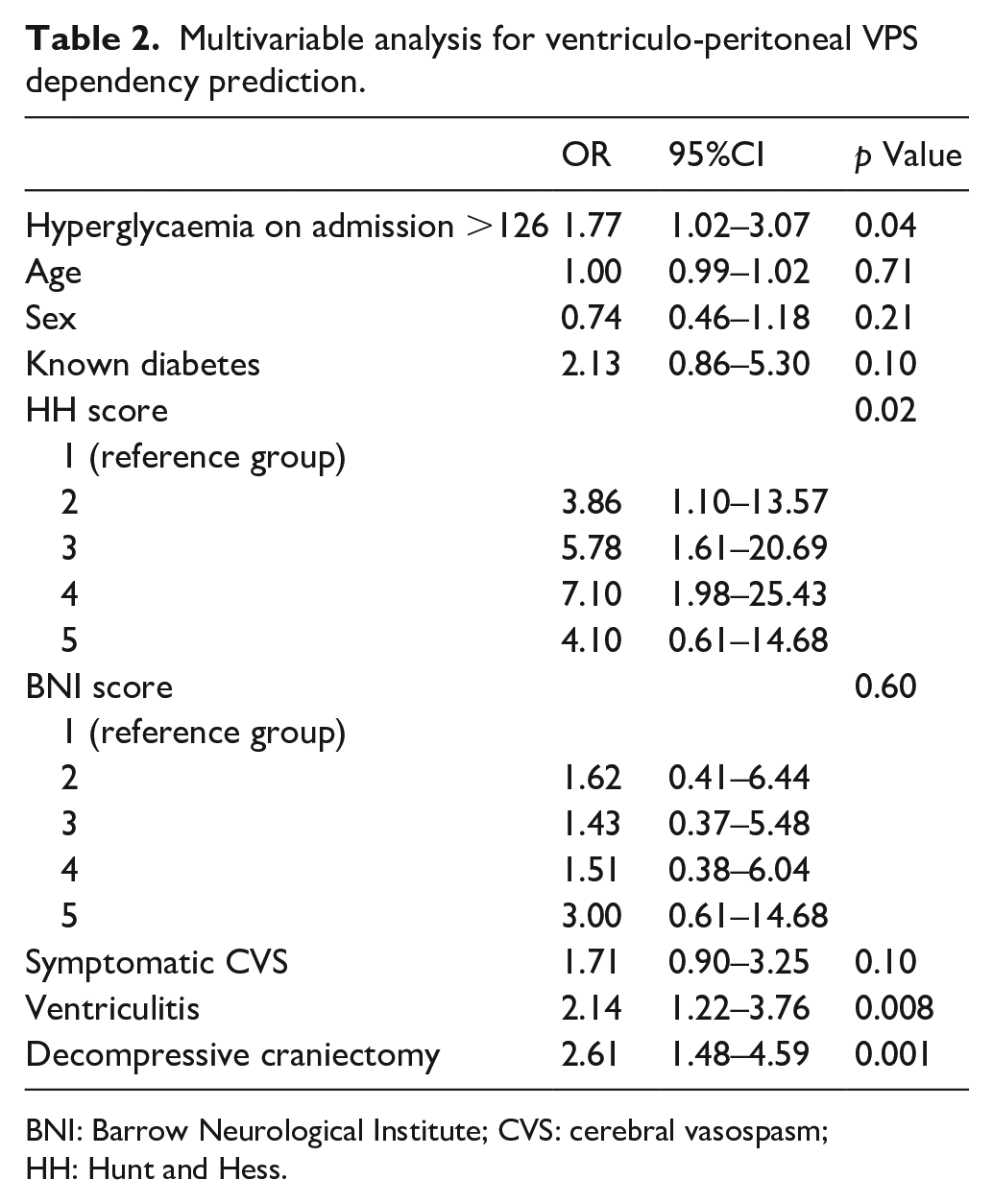
BNI: Barrow Neurological Institute; CVS: cerebral vasospasm; HH: Hunt and Hess.
Multivariable analysis for ventriculo-peritoneal VPS dependency prediction after stepwise backward regression analysis.
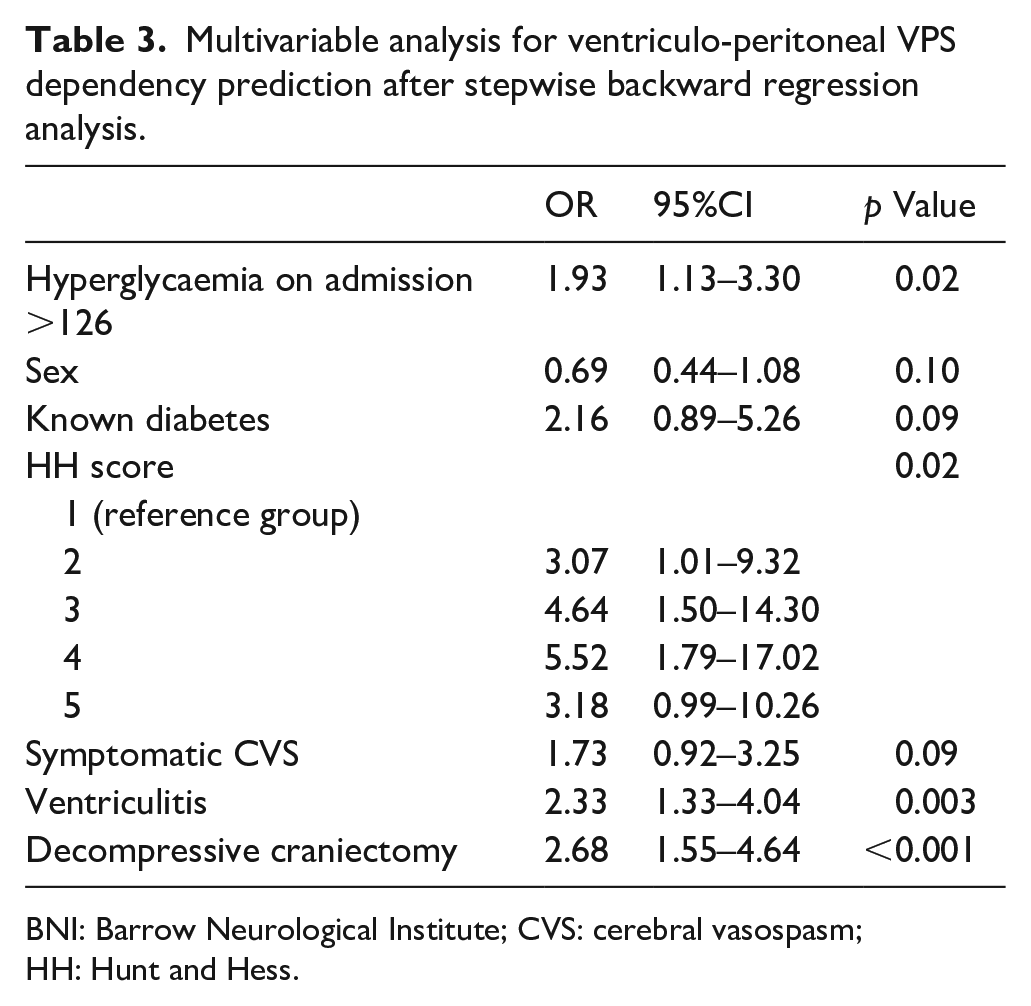
BNI: Barrow Neurological Institute; CVS: cerebral vasospasm; HH: Hunt and Hess.
In our sensitivity analysis adding CSF glucose to the multivariable model (n = 372), higher glucose value in the CSF was significantly associated with VPS (OR 3.72, 95%CI 1.41–9.79, p = 0.001). We included an interaction term between blood glucose and CSF glucose. Interestingly, there was not significant interaction (p = 0.49). The model did not significantly change otherwise.
Discussion
We assessed early available factors influencing VPS dependency after aSAH with a specific interest in hyperglycaemia on admission in order to evaluate the association of hyperglycaemia with VPS dependency. In our large observational study, patients with hyperglycaemia had a higher probability for VPS dependency confirmed by the multivariable analysis and propensity score matching, strengthening previous findings and supporting further research on this topic. Hunt and Hess grade, with higher grades having higher OR, as well as ventriculitis and decompressive craniectomy are all well-established contributors to VPS dependency and were also associated with VPS dependency in our cohort.
Our findings are in line with previous studies suggesting an association of hyperglycaemia and VPS dependency and strengthening a real association.11,25,31 Although resulting in fewer observations, CSF glucose levels were also associated with VPS dependency in our cohort, independently from blood glucose values, further confirming previously reported findings. 9 There are several reasons however, why our association might not be as strong as anticipated. Firstly, the effect might not be strong, needing a larger cohort to validate and confirm our findings. Another reason for the limited significance might be the stage at which hyperglycaemia might exhibit its influence. As suggested by a previous study the association between hyperglycaemia and CSF resorption might reflect an influence of hyperglycaemia on only acute CSF resorption problems but not on longer-term CSF resorption. 25 Or it might simply be an indicator of disease severity. 11 The fact that most of the other independent variables in the multivariable analysis where mainly indicators of disease severity supports this point. A previous study for example showed that patients with stress-induced hyperglycaemia had more intraventricular blood. 24 Thirdly, an unknown fraction of blood glucose levels on admission were most likely not fasting blood glucose levels. Hence, some of the observed hyperglycaemic cases might have been due to food intake and as such transitory. Whatever the reason for the effect of hyperglycaemia on VPS dependency is, it important to point out the influence glucose control in the emergency setting of aSAH patients could have on multiple issues including hydrocephalus and VPS dependency. Fourthly, a hypothesis explaining the stronger trend for glucose in CSF compared to blood despite it being available in a smaller subgroup might be that CSF glucose had a stronger influence on reabsorption and therefore impaired CSF drainage, probably by causing adhesions and reduction of CSF outflow through increased viscosity. 32 Lastly, our findings might be random. In order to assess whether the course of glucose levels during hospitalisation has an influence, repeated glucose measurements at standardised time points would be necessary. As laboratory measurements were not standardised only very limited data on glucose levels during the further hospital course was available. In a sensitivity analysis we analysed the influence of the highest measured glucose value on VPS dependency and found a significant association with VPS dependency. However, these glucose measurement could be taken at any time point and therefore the meaningfulness of this finding is limited and needs to be evaluated in further studies with standardised, repeated glucose measurements.
In order to measure CSF glucose, patients need to have an EVD or LD and repeated CSF sampling, which is associated with an increased rate of ventriculitis. Almost all patients in our cohort developing ventriculitis during their hospitalisation had an EVD (only eight without EVD had ventriculitis). Still, adjusting the multivariable model with ventriculitis, hyperglycaemia on admission remained significantly associated with VPS dependency. If serum hyperglycaemia is confirmed to be associated with VPS dependency in a larger independent cohort, this could have implications especially in the management of patients with EVD or LD as decisions to change to permanent drainage systems, such as VPS, could be taken earlier potentially decreasing complications associated with an external drainage system.
Also in line with previous findings is the association of VPS dependency with complications during the course of the disease. 33 Decompressive craniectomy, symptomatic vasospasms and their association with VPS dependency has previously been reported.33–35 A plausible underlying mechanism of symptomatic vasospasm and VPS dependency might be an increased blood load causing both an increased rate of symptomatic vasospasms and decreased CSF absorption.16,29,36 However, a higher grade on the BNI Grading Scale did not significantly influence VPS dependency in our multivariable analysis. On the other hand, decompressive craniectomy itself reflects a trauma most likely increasing VPS risk by impairing CSF drainage due to enhancing the development of adhesions and impaired venous drainage. 37 Then again, patients needing a decompressive craniectomy have higher HH grades and therefore higher VPS rates. Additionally, in our institution we tend to do early bone flap reimplantation before patients are transferred to the rehabilitation centre. This might have led to an increased VPS rate. In the end, the exact mechanism between decompressive craniectomy and VPS dependency remains unclear.
Lastly, we found a decreased mortality in patients with VPS dependency. This finding is most likely due to patients who die during the course of hospitalisation or are deemed to have too poor a prognosis do not undergo VPS insertion. Patients who die early die before VPS dependency would have been established or possible for example due to CSF being too high in proteins. 30 Also, patients with a poor prognosis where therapy is discontinued will not receive a VPS although they very likely would have needed one. This is supported by several findings: one, patients with permanent VPS dependency had a longer hospital stay compared to those without. Two, the association between mRS and VPS: Although mRS 6 (mortality) was associated with a decreased likelihood for VPS, most likely due to the above-mentioned explanation, an increased likelihood for VPS dependency was observed with increasing mRS grade.
Our study has limitations: as this was a retrospective analysis, we were not able to assess which patient was deemed to have too poor of a prognosis to receive a VPS. This is the most likely reason for patients with a VPS having a decreased mortality. HbA1c is not part of our standardised laboratory work-up and was therefore not available in our cohort. This needs to be evaluated in future studies as hyperglycaemia might be stress-induced and better tolerated by diabetic patients. Patients with hyperglycaemia receive treatment to decrease their glucose levels. As this was a retrospective analysis, we were not able to evaluate if the specific treatment did influence VPS dependency. Additionally, we were not able to assess the influence of the course of either serum or CSF glucose levels during hospitalisation as after admission, these were not taken regularly or at pre-specified time points. We therefore focused on glucose measurement on admission. These limitations need to be addressed in a larger, prospectively collected validation cohort with sampling at several, prespecified time points throughout the hospital stay. This would give the opportunity to assess whether the first 24 h are appropriate to make any indication on VPS dependency or whether a longer interval is important. Good quality data would additionally give us the opportunity to assess a potentially more appropriate cut-off value for glucose levels by being able to investigate the adequate cut-off using Area Under The Curve Receiver Operating Characteristic on a continuous glucose variable.
Conclusion
Hyperglycaemia on admission was associated with an increased likelihood of VPS dependency. This needs to be validated in a prospectively collected cohort with a standardised collection of laboratory parameters at prespecified time points. If these findings are confirmed, early treatment of hyperglycaemia might reduce VPS dependency rate and accelerate insertion of a permanent draining system in those who will still develop VPS dependency. This could decrease unnecessary interventions such as repeated EVD changes, EVD-associated infections and complications associated with it.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221147087 – Supplemental material for VPS dependency after aneurysmal subarachnoid haemorrhage and influence of admission hyperglycaemia
Supplemental material, sj-docx-1-eso-10.1177_23969873221147087 for VPS dependency after aneurysmal subarachnoid haemorrhage and influence of admission hyperglycaemia by Isabel Charlotte Hostettler, Nicole Lange, Nina Schwendinger, Gareth Ambler, Theresa Hirle, Samira Frangoulis, Dominik Trost, Jens Gempt, Kornelia Kreiser, Bernhard Meyer, Christof Winter and Maria Wostrack in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the local Research Ethics committee (186/20S). This study follows the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
Informed consent
As this is a retrospective study of a prospective collected database no informed consent was needed as per our ethics committee.
Guarantor
None.
Contributorship
None.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.