
Abstract
Introduction:
We evaluated the effects of prior antiplatelet use (APU) on futile reperfusion (FR) after endovascular treatment (EVT) in acute ischemic stroke.
Material and methods:
We consecutively collected data of 9369 patients with acute ischemic stroke from four university-affiliated multicenter registry databases over 92 months. We enrolled 528 patients with acute stroke receiving EVT. Among them, we defined FR in subjects as a 3-month modified Rankin Scale score of >2 despite successful reperfusion after EVT. We classified patients into two groups: prior APU and no prior APU. We used propensity score matching (PSM) to overcome the imbalance in multiple covariates between the two groups. After PSM, we compared the baseline characteristics between the two groups and performed multivariate analysis to determine whether prior APU affected FR and other stroke outcomes.
Results:
The overall FR rate in the present study was 54.2%. In the PSM cohort, the FR was lower in the prior APU group than that in the no prior APU group (66.2% vs 41.5%, p < 0.001). In the multivariate analysis using the PSM cohort, prior APU significantly reduced the risk of FR (odds ratio (OR), 0.32; 95% confidence interval (CI), 0.18–0.55; p = 0.001) and stroke progression (OR, 0.38; 95% CI, 0.15–0.93; p = 0.03). Prior APU was not associated with symptomatic hemorrhagic transformation in this study.
Conclusion:
Prior APU potentially reduced FR and stroke progression. Further, prior APU was not associated with symptomatic hemorrhagic transformation in patients receiving EVT. APU pretreatment can be a modifiable predictor of FR in clinical practice.
Introduction
Endovascular treatment (EVT) has become a crucial treatment in acute ischemic stroke with large vessel occlusion according to recent guidelines since the mid-2010s. 1 With advanced techniques, devices, and extended eligibility for EVT according to updated trials, stroke outcomes have greatly improved after EVT.2,3 Nonetheless, futile reperfusion (FR), a poor functional outcome despite successful reperfusion after EVT, 4 has been reported in up to 67% of clinical trials.5–9 This phenomenon can be explained by poor collateral circulation, re-occlusion, reperfusion injury, and hypoperfusion.10,11
To overcome FR, several studies evaluated the clinical and imaging predictors affecting FR in order to identify patients vulnerable to FR after EVT10–14; however, since these predictors were post-stroke factors, it is difficult to use them for the assessment of FR in an acute stroke setting. Rather, interventionists need to evaluate modifiable pre-stroke predictors or management to reduce FR.
Antiplatelet agents, which are commonly used in clinical practice, affect clot formation, platelet aggregation, and endothelial inflammation; consequently resulting in improved intravascular stability and microvascular reperfusion.15–17 Hence, antiplatelet agents are used as adjunctive drugs in the periprocedural setting and can be valuable for studying the effect of prior antiplatelet use (APU) on FR based on these mechanisms. However, evidence on whether prior APU is associated with FR after EVT remains scarce.
Using a multicenter registry database, we aimed to evaluate the effects of prior APU on FR and stroke outcomes after EVT.
Methods
Subjects
We consecutively enrolled patients with acute ischemic stroke in four university-affiliated multicenter registry databases between March 2015 and January 2022. In this study, we identified patients with acute ischemic stroke with large artery occlusion of the anterior circulation who received EVT. Among those EVT-treated patients, we confirmed the successful reperfusion of modified Thrombolysis in Cerebral Infarction (mTICI) grade 2b or 3. Patients underwent EVT according to the protocols of each institution based on recent EVT guidelines. We excluded the following: (1) patients with a pre-stroke mRS score >2, (2) patients without follow-up brain computed tomography (CT) or magnetic resonance imaging within 24 h of stroke onset, (3) patients with an Alberta Stroke Program Early CT Score <6, (4) patients with interval from stroke onset to groin puncture over 12 h of onset, (5) patients not undergoing multiphasic CT angiography (mCTA), and (6) patients without a 3-month modified Rankin Scale (mRS) score.
Data collection and definition of parameters
We obtained demographic, clinical, laboratory, and outcome data from the web-based registry databases of the four institutions. Data on prior APU and types of antiplatelet agents administered were obtained from the registry database. Prior APU was defined as the use of any antiplatelet agent before hospitalization, and was identified by neurologists and at the pharmacy department of each institution. We classified the type of the antiplatelet agents as aspirin, clopidogrel, cilostazol, and others. Dual APU was defined by a prescription of two antiplatelet agents of different types during hospitalization. The collateral status was classified as good, intermediate, and poor, which was assessed by imaging protocols of the Calgary Stroke Program using mCTA. 18 Collateral status was quantified by two experienced vascular neurologists (Y Kim and S-H Lee) in a double-blinded manner (intraclass correlation coefficient (ICC), 0.89; p < .001). The infarct volume confirmed by diffusion weighted imaging was calculated using Medical Image Processing and Visualization software (version 7.3.0, National Institutes of Health, Bethesda, MD, USA).
The primary outcome measure was the occurrence of FR, which was defined as a 3-month mRS score of 3–6 despite successful reperfusion (mTICI 2b–3) after EVT. Two trained vascular neurologists (Y Kim and S-H Lee) reviewed the angiography data to confirm the mTICI grade in a double-blinded manner (ICC, 0.86; p < 0.001). The secondary outcome was early neurological deterioration (END). Moreover, END was defined as an increment of at least 1 point in motor power or a total National Institute of Health Stroke Scale (NIHSS) score deterioration of ⩾2 points within 7 days of hospitalization as compared to the initial NIHSS score. We categorized the etiology of END as follows: (1) symptomatic hemorrhagic transformation (END-SHT) and (2) stroke progression (END-prog) after EVT. 19 Hemorrhagic transformation was defined according to European Cooperative Acute Stroke Study criteria. 20 Two vascular neurologists (M Lee and S-H Lee) reviewed the END data to confirm END-SHT and END-prog in a double-blinded manner (ICC, 0.89; p < 0.001).
Statistical analysis
We hypothesized that prior APU would decrease the risk of FR after EVT. With respect to the primary and secondary outcome measures, prior APU and no prior APU groups were compared using Pearson’s chi-squared test for categorical variables and Student’s t-test or Mann–Whitney U test for continuous variables.
To reduce the possible imbalance of covariates and confounding factors between the two groups, we performed propensity score matching (PSM). The propensity score for each group was defined as the probability of the presence of prior APU, given the patients’ initial demographics, vascular risk factors, and laboratory values in the baseline logistic regression analysis. Based on these propensity scores, the prior APU and no prior APU groups were matched 1:1 using the nearest neighbor method. Using the PSM cohort, we performed logistic regression analysis to evaluate the effects of prior APU on outcomes. We additionally adjusted for significant covariates with the clinical plausibility of the outcomes. Statistical analyses were performed using IBM SPSS version 21.0 software (IBM Corporation, Armonk, NY, USA) and moonBook and MatchIt of R version 4.0.3 (R Core Team 2020, R Foundation for Statistical Computing, Vienna, Austria).
For the sensitivity analysis, we evaluated the independent effects of prior APU on outcome measures, and performed a binary logistic regression analysis using the total cohort. Moreover, we performed the same analysis to determine whether prior APU had different effects according to the stroke subtypes (cardioembolism and non-cardioembolism). Variables for adjustment in the multivariate analysis were selected if their p values were <0.1 in comparison according to the presence of prior APU, and if their associations with each outcome variable were clinically plausible. Crude and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated.
Results
Among the 9369 consecutive patients with acute ischemic stroke, 706 (7.5%) received EVT due to large artery occlusion of the anterior circulation. Of the 706 patients, 528 who met the inclusion criteria were enrolled in this study (Figure 1). Among the enrolled patients, 24.6% (130/528) were on prior APU. Of those who were on prior APU, 79% (103/130) and 21% were on single and dual antiplatelet use, respectively. The doses of antiplatelet agents were as follows: aspirin 100 mg daily, clopidogrel 75 mg daily, cilostazole 200 mg daily, and others (ticlopidine 500 mg daily and dypiridamole 200 mg daily, triflusal 600 mg daily). Among the patients on single antiplatelet use, aspirin and clopidogrel were used in 67% (69/103) and 29% (30/103) of the patients, respectively. Among the patients on dual antiplatelet use, a combination of aspirin and clopidogrel was used in 81% (22/27) of the patients. Patients with prior APU were older; had more prior stroke, hypertension, and coronary heart disease; used more prior statins; and had less prior anticoagulation (Table 1). The final infarct volume was lower in the prior APU group than no prior APU group (10.8 cm3 vs 14.3 cm3, p = 0.001). In addition, patients with FR were older, more likely to be male, and had a longer interval from the onset to arrival and groin puncture, severe stroke symptoms, several comorbidities, and poor collateral status (Supplemental Table 1).
Baseline characteristics according to presence of prior APU.
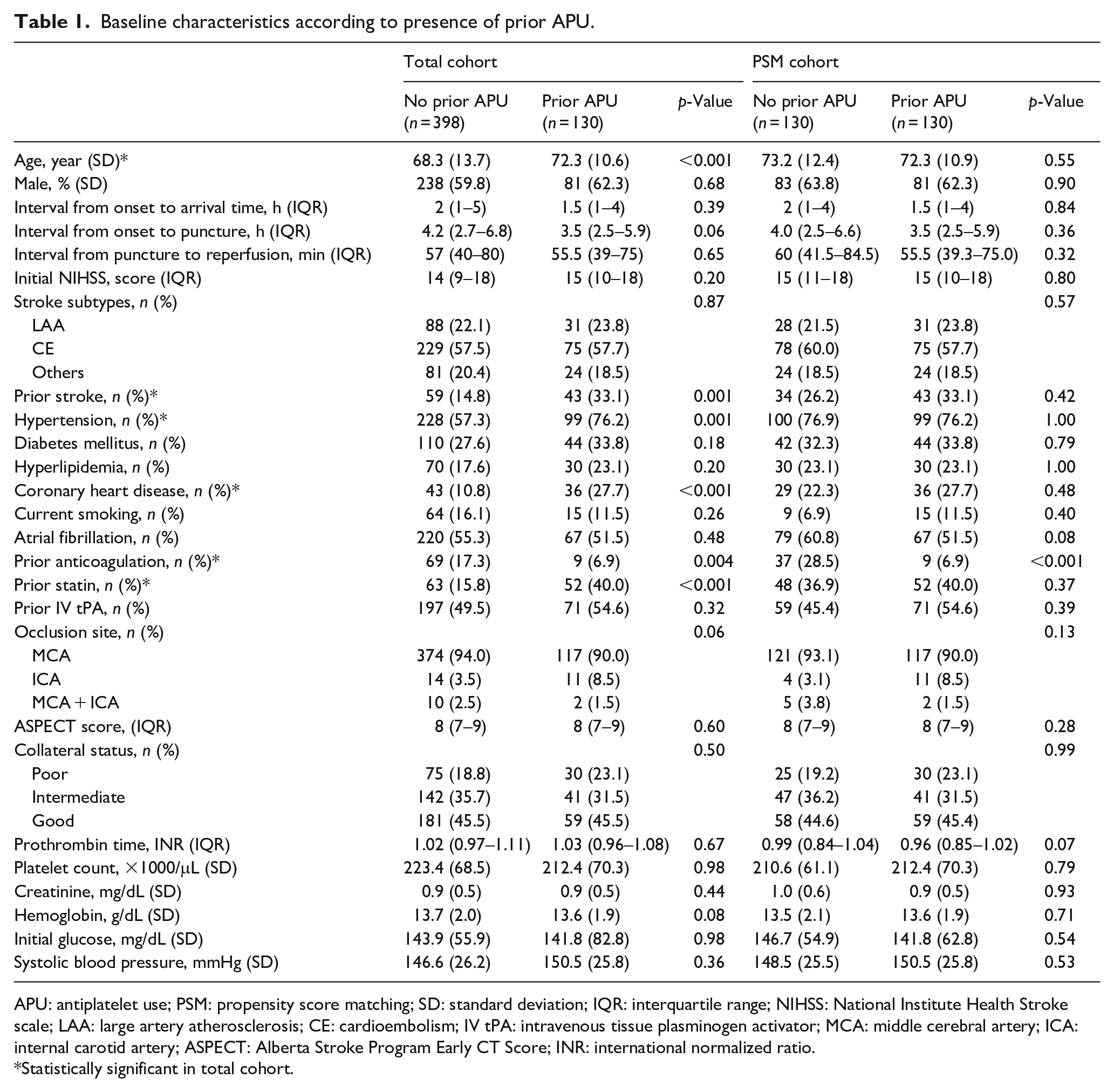
APU: antiplatelet use; PSM: propensity score matching; SD: standard deviation; IQR: interquartile range; NIHSS: National Institute Health Stroke scale; LAA: large artery atherosclerosis; CE: cardioembolism; IV tPA: intravenous tissue plasminogen activator; MCA: middle cerebral artery; ICA: internal carotid artery; ASPECT: Alberta Stroke Program Early CT Score; INR: international normalized ratio.
Statistically significant in total cohort.
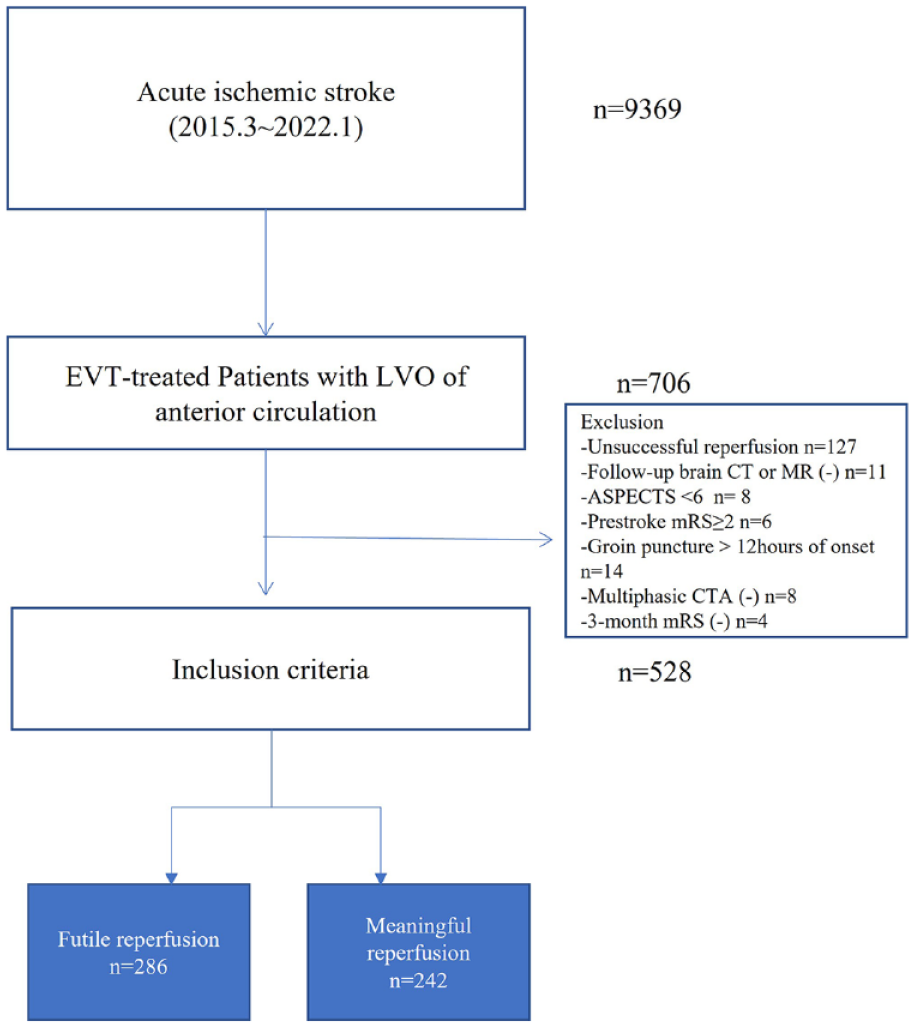
Flow chart of study.
After PSM, 130 patients who were on prior APU were matched 1:1 with patients who were not on prior APU. In the PSM cohort, the baseline characteristics of the two groups were similar and reasonably balanced (Table 1).
The overall FR rate was 54.2% (286/528) in the total cohort. In the total cohort, the FR rate was lower in the prior APU group than that in the no prior APU group (58.3% vs 41.5%, p < 0.001). In the PSM cohort, the FR rate was also lower in the prior APU group than that in the no prior APU group (66.2% vs 41.5%, p < 0.001, Figure 2). The END-SHT was not significantly different between the two groups in either the total or PSM cohort. In addition, END-prog was not different between the two groups in either the total or PSM cohort. In the logistic regression model using the PSM cohort, prior APU reduced the risk of FR (OR, 0.32; 95% CI, 0.18–0.55; p = 0.001) and END-prog (OR, 0.39; 95% CI, 0.15–0.93; p = 0.03 (Table 2)). In addition, no association was found between prior APU and END-SHT (OR, 0.65; 95% CI, 0.22–1.91; p = 0.43). In a sensitivity analysis using the total cohort, prior APU reduced FR, but was not associated with END-SHT and END-prog (Supplemental Table 2). In addition, prior APU was also associated with a reduction in FR with both cardioembolism and non-cardioembolism (Supplemental Table 3).
Logistic regression showing impact of prior APU on outcomes in PSM cohort.
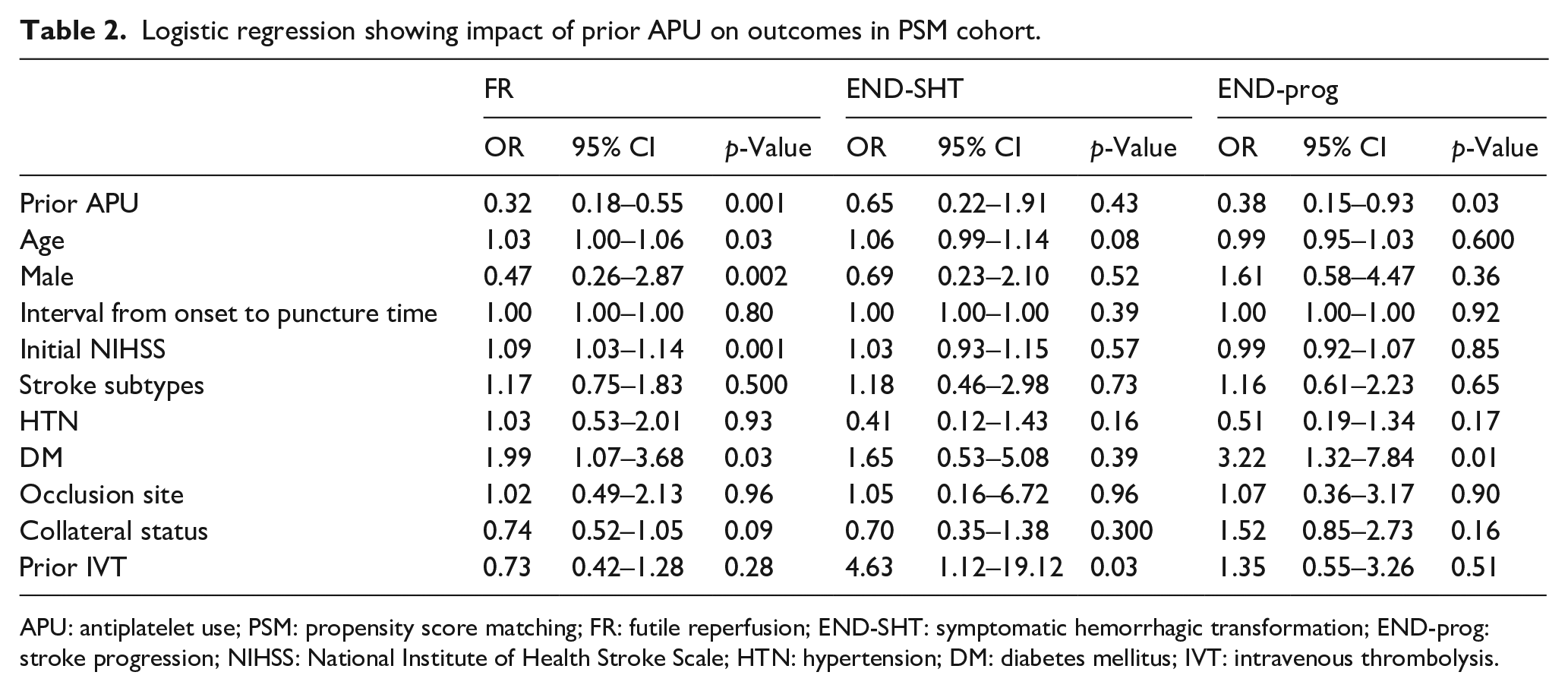
APU: antiplatelet use; PSM: propensity score matching; FR: futile reperfusion; END-SHT: symptomatic hemorrhagic transformation; END-prog: stroke progression; NIHSS: National Institute of Health Stroke Scale; HTN: hypertension; DM: diabetes mellitus; IVT: intravenous thrombolysis.
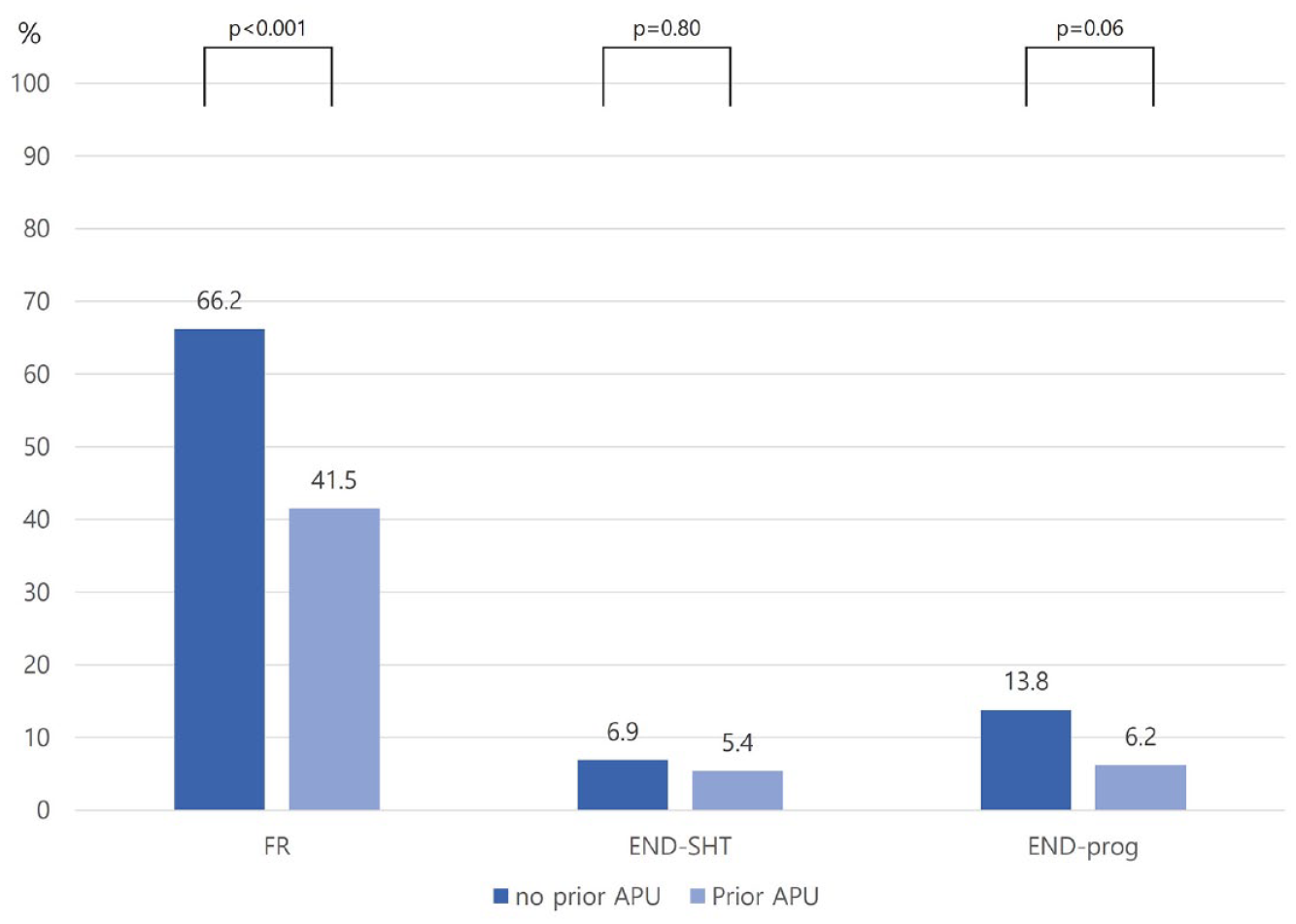
Distributions of outcomes according to prior APU (using PSM cohort).
Discussion
The main findings of this study were as follows: (1) subjects with prior APU before EVT had a lower FR rate in both the total and PSM cohorts than those without prior APU, (2) prior APU could reduce the risk of FR and END-prog after EVT, and (3) prior APU was not associated with END-SHT after EVT.
Despite the development of EVT techniques and devices and the increasing reperfusion rate after EVT, FR rate remains higher in several randomized controlled trials and observational studies. The following pathophysiological mechanisms can be attributed to FR in clinical and in vivo studies: microvascular occlusion and distal thrombosis, microvascular injury via capillary stalls caused by neutrophil stuck in the ischemic core and penumbra, and macrovascular constriction by inflammatory reactions.21–24 Several studies have shown that APU can reduce the intravascular inflammatory process causing thrombus formation and platelet aggregation, thereby promoting neuroprotective effect after cerebral ischemia.25–28 In addition, antiplatelet agents are thought to enhance endothelial microcirculatory reperfusion by attenuating platelet activity. 29 Hence, APU contributes to endothelial stabilization by ameliorating microcirculatory reperfusion, removing distal clots, and halting subsequent microthrombi formation that is aggravated by vessel wall injury via EVT. 15 Considering the aforementioned mechanisms of FR and APU in acute ischemic stroke, antiplatelet agent pretreatment may be theoretically reliable to prevent FR after EVT.
The overall FR rate (54.2%) in this study was comparable to that observed in other previous studies. With the growing interest in FR in clinical practice, several previous studies have investigated the predictors of FR after EVT.10,11,13,30 Factors associated with patients such as older age, baseline stroke severity, pre-stroke disability, chronic brain disease, and radiological factors such as distal thrombus migration, occlusion site, and collateral status were strong predictors of FR. Most of these predictors are not modifiable in acute stroke settings. Although antiplatelet agents are commonly used in clinical practice, clinicians are hesitant to administer antiplatelet agents systemically before or during EVT because of conflicting results regarding the association between APU and stroke outcomes. 31 Previous studies investigated the effects of prior APU on stroke outcomes using a general EVT-treated population.32,33 Since the concept of FR does not consider the periprocedural factors (i.e. types of devices, workmanship of technique, numbers of retriever passing), 4 our study, which used the PSM cohort, can provide useful clinical information on a novel modifiable factor, that is, pretreatment with antiplatelet agents, for reducing FR after EVT.
Notably, our study showed that APU was not associated with hemorrhage after EVT. Although HT is a leading cause of poor outcomes after reperfusion therapy, several studies evaluating whether pretreatment antiplatelet agents increased the risk of HT after IVT or EVT showed contradicting results.32–35 Particularly, since our study only included subjects who had successful reperfusion, HT could be more vulnerable in our subjects through reperfusion injury after EVT. 36 The results of previous studies using EVT-treated stroke patients should be validated by procedural factors (e.g. type of retrievers, technique, workmanship of interventionist) to generalize the safety of APU. In this study, our multivariate analysis using the concept of the FR and PSM cohorts can be helpful in considering the safety issue of prehospital APU in patients with acute ischemic stroke who had successful reperfusion after EVT. Further clinical trials are warranted for further clarification in this regard.
Although we used data from a consecutive multicenter registry, our study has some limitations. First, despite PSM balancing the covariates between groups, unmeasured confounding factors could hinder the generalization of our results. Second, our study did not evaluate the effects of dual APU on FR and other outcomes because of the small sample size of subjects on dual APU. Third, despite clinicians assessing the types of antiplatelet agents, the duration of use of prehospital antiplatelet agents and drug compliance data were not available in our cohort. Fourth, because it was difficult to introduce CT perfusion and RAPID programs for internal reasons, multiphasic CTA was implemented as a suboptimal solution. Although CT perfusion data was not available in this study, the final infarct volume was significantly lower in the prior APU group. After adjusting the variables that included final infarct volume, the association between prior APU and FR remained (OR (95% CI); 0.29 (0.18–1.48)), and the infarct volume was not affect to FR (OR (95% CI); 1.00 (0.99–1.01)). Moreover, all centers belong to the same foundation and share the same multiphasic CTA protocol, which represents a strength of this study.
In conclusion, our study using PSM shows that prior APU decreases the risk of FR and stroke progression. In addition, prior APU is not associated with SHT after EVT. Among several predictors of FR, our study highlights the effects of prior APU as a modifiable predictor for improving FR after EVT. Further randomized trials are warranted to evaluate the efficacy and safety of prior APU in patients treated with EVT.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221144814 – Supplemental material for Effects of prior antiplatelet use on futile reperfusion in patients with acute ischemic stroke receiving endovascular treatment
Supplemental material, sj-docx-1-eso-10.1177_23969873221144814 for Effects of prior antiplatelet use on futile reperfusion in patients with acute ischemic stroke receiving endovascular treatment by Jong-Hee Sohn, Chulho Kim, Minwoo Lee, Yerim Kim, Hee Jung Mo, Kyung-Ho Yu and Sang-Hwa Lee in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from Samjin Pharmaceuticals, partly supported by the Basic Science Research Program of the National Research Foundation of Korea (NRF-2021R1G1A1013767) and a grant from the Korea Health Technology R&D project of the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (HR21C0198). The funding organizations did not participate in the design, conduct, or analysis of the study or in the preparation of the manuscript.
Ethical approval
The collection of clinical information from the registry to monitor and improve the quality and outcomes of stroke care was performed with informed consent and was approved by the local institutional review board (IRB). (Chuncheon Sacred Heart Hospital IRB no.2022-08-021, Hallym University Sacred Heart Hospital IRB no. 2021-03-008, Kangdong Sacred Heart Hospital IRB no. 2021-06-001, and Dongtan Sacred Heart Hospital IRB no. 2022-03-002).
Informed consent
The use of the registry database and the additional medical records for this study was approved by the IRB of the four centers without the need for informed consent from patients because of the study participants’ anonymity and minimal risk to patients.
Guarantor
S-H Lee
Contributorship
Jong-Hee Sohn: Conceptualization, methodology, formal analysis, investigation, writing, and original draft preparation. Sang-Hwa Lee: Conceptualization, data curation, original draft, review and editing, and supervision. Chulho Kim: Data curation and review and editing. Yerim Kim: Data curation and review and editing. Hee Jung Mo: Data curation and review and editing. Minwoo Lee: Data curation and review and editing. Kyung-Ho Yu: Data curation and review and editing.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.