
Abstract
Purpose:
The optimal anesthetic approach in the endovascular treatment (EVT) of patients with posterior circulation large vessel occlusion (PC-LVO) strokes is not clear. Little data has been published and no randomized clinical trials have been conducted so far. We aimed to perform an updated meta-analysis to compare clinical and procedural outcomes between conscious sedation (CS) and general anesthesia (GA).
Methods:
We reviewed the literature of the studies reporting CS and GA in patients with endovascularly-treated PC-LVO. The primary outcome was the functional outcome at 3 months measured using the modified Rankin Scale (mRS). A good functional outcome was defined as having a mRS 0–2. Secondary outcomes were mortality at 3 months, final successful recanalization (modified Thrombolysis in Cerebral Infarction (mTICI) scale from 2b to 3) and complete recanalization (mTICI of 3) and times from stroke onset to EVT completion. Random-effects models were completed to pool the outcomes and the I2 value was calculated to assess heterogeneity.
Findings:
Eight studies with a total of 1351 patients were included. The pooled results reveal that CS use was associated with higher rates of good outcome (OR 2.41, 95% CI 1.58–3.64, I2 = 49.67%) and with lower mortality at 3 months (OR 0.48, 95% CI 0.28–0.82, I2 =57.11%). No significant differences were observed in the final reperfusion rates, procedural duration, and time from stroke onset to EVT completion.
Conclusion:
In this meta-analysis, GA was associated with significantly lower rates of functional independence at 3 months in patients with PC-LVO strokes.
Keywords
Introduction
The efficacy and safety of endovascular treatment (EVT) on posterior circulation large vessel occlusion (PC-LVO) have been recently demonstrated in ATTENTION and BAOCHE trials. 1 However, the best anesthetic strategy in these procedures is still unknown and current guidelines recommend either anesthetic approach. 2
The use of general anesthesia (GA) and conscious sedation (CS) has been assessed in clinical trials and meta-analyses in anterior circulation strokes EVT with variable results.3–10
In contrast, the impact of the anesthesia strategy on PC-LVO is poorly understood, since no clinical trials have been conducted so far. Only some retrospective and single-center prospective studies have explored the effect of each anesthesia use on posterior circulation strokes.11–19 Because of the low data available and the current debate on anesthesia management, we performed this meta-analysis to investigate the impact of the anesthetic approach and outcomes in patients with endovascularly treated PC-LVO.
Methods
Literature search strategy, study selection, and eligibility criteria
Three data bases (PubMed, Cochrane and Embase) were consulted to identify comparative studies on GA versus CS in endovascular stroke thrombectomies published before August 10, 2021.
The study was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines and also to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) proposal.20,21
Risk of bias assessment and data extraction
In this meta-analysis, the risk of bias assessment was performed using the Newcastle Ottawa Scale (NOS). 22
The following variables were extracted from the studies if available: year and country of study, prospective or retrospective design, study recruitment period, sample size, sex, age, baseline NIHSS, occlusion artery location, anesthetic approach (CS vs GA), rates of successful and complete recanalization at the end of the procedure, complications during the procedure, times from stroke onset to EVT completion, clinical outcome according to the modified Rankin Scale (mRS) at 3 months, and mortality at 3 months.
Outcome variables
The primary outcome of this meta-analysis was good functional outcome (mRS ⩽ 2) at 3 months.
The secondary outcomes were mortality at 3 months, successful recanalization (mTICI 2b–3) and complete recanalization (mTICI 3) at the end of the EVT, time from stroke onset to EVT completion, and time from arterial puncture to EVT completion (procedure duration).
Statistical analysis
Since the number of studies included in the meta-analysis was relatively small, a random-effects model with the restricted maximum likelihood (REML) estimation method was implemented. The results were expressed as odds ratios (OR) for binary outcomes and mean differences for continuous outcomes with their respective 95% confidence intervals (CIs). For continuous outcomes, if the study reported results as median and interquartile range, these were converted to mean and SD based on a quantile method. 23 Forest plots were used to graphically represent the weighted ORs/mean differences of outcomes.
Heterogeneity between summary data was evaluated using Higgins et al. (I2) test statistics. I2 values of 25%, 50%, and 75% indicate low, moderate and high heterogeneity, respectively. 24
The stability of the pooled conclusions was assessed using sensitivity analyses through the sequential removal of each individual study (Supplemental Figure S2). 25
Publication bias was not assessed due to the limited number of publications. STATA software was used to perform all the statistical analyses in this study (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC.). R software was used to plot the results of the sensitivity analyses.
Ethics
Given that this study is a systematic review and meta-analysis, informed consent and ethics approval were not required.
Results
Literature search results
A total of 284 articles were found on the initial search. Of these, 270 were excluded from the analyses on the grounds of duplication, case reports, not being written in English, and vertebrobasilar LVO occlusion not being reported. None of these studies were randomized clinical trials. Finally, 14 studies were evaluated and 6 were excluded due to lack of outcomes or not reporting the specific data regarding the anesthesia approach. The flow chart is available in the Supplemental Material (Supplemental Figure S1).
The characteristics of the studies included in this meta-analysis are set out in Table 1.
Characteristics of studies included in the meta-analysis.
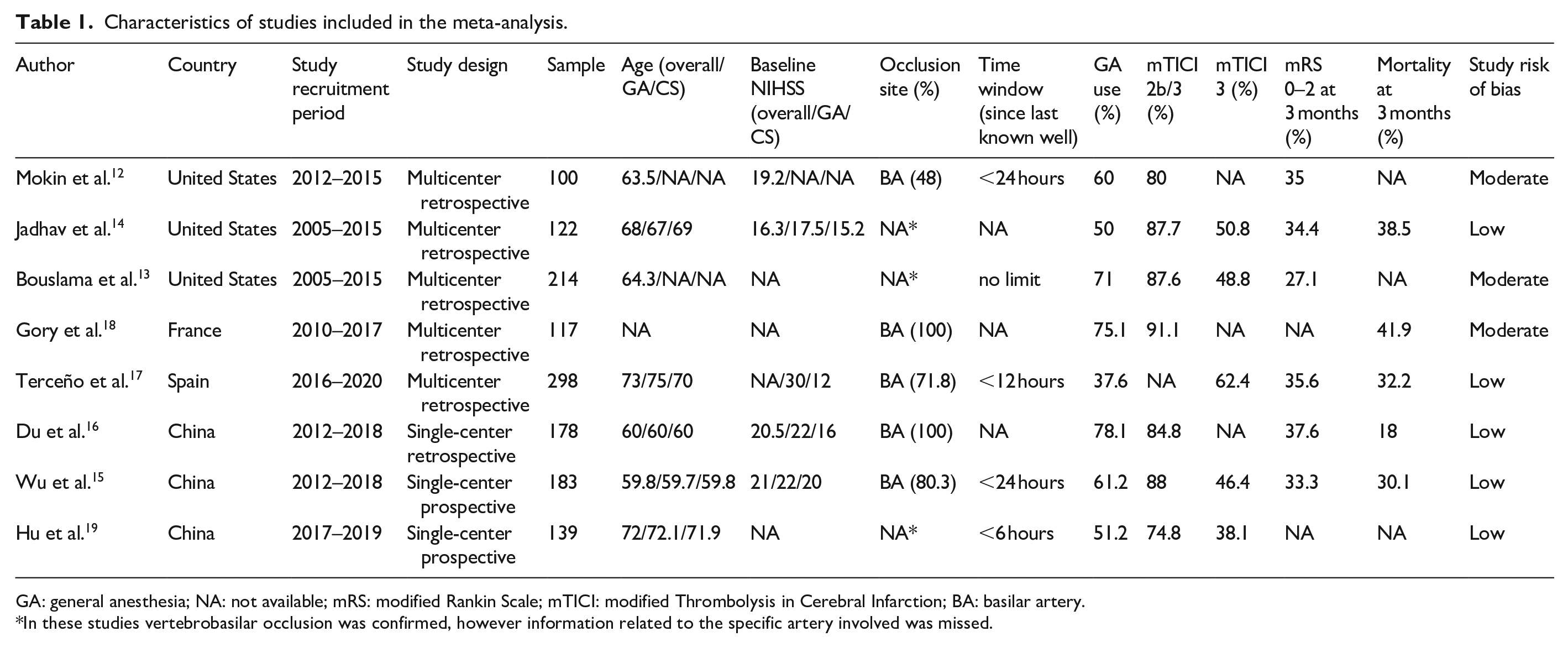
GA: general anesthesia; NA: not available; mRS: modified Rankin Scale; mTICI: modified Thrombolysis in Cerebral Infarction; BA: basilar artery.
In these studies vertebrobasilar occlusion was confirmed, however information related to the specific artery involved was missed.
Quality of studies
Eight studies were selected for the meta-analysis, of these, six were retrospective and two were prospective series. We identified five multi-center and three single-center series. Five studies were rated as high-quality based on the Newcastle-Ottawa quality assessment criteria (Supplemental Material, Table S1). According to this classification, the overall risk of bias is low.
Primary outcome
Five studies included the clinical outcome assessed by the mRS at 3 months. The pooled analysis reveals a significant benefit of CS with higher rates of functional independence (OR 2.41, 95% CI 1.58–3.67), with mild heterogeneity (p = 0.10, I2 = 49.67%) (Figure 1(a)).
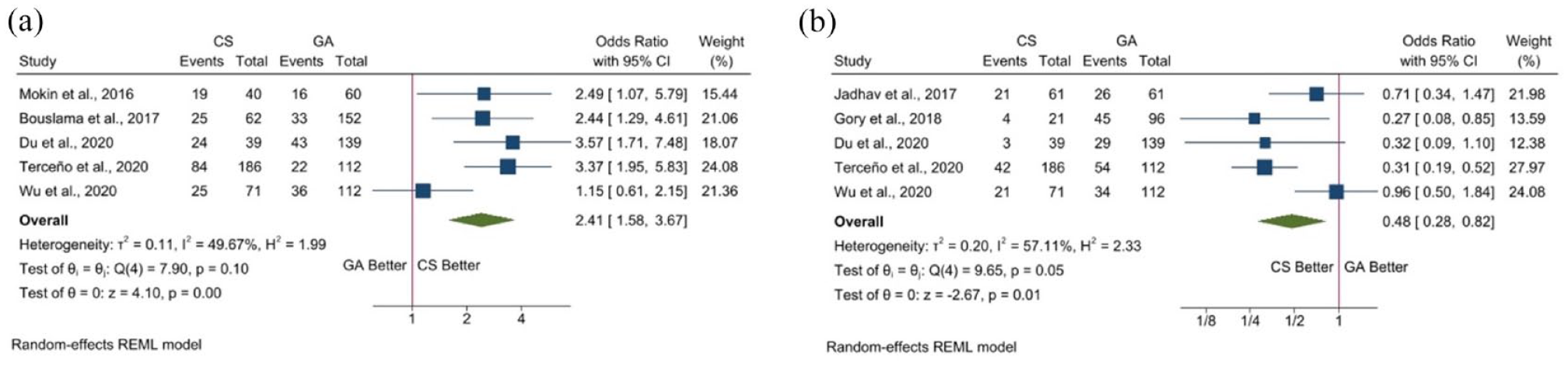
Forest plots for outcomes at 3 months: (a) mRS 0–2 and (b) mortality.
The sensitivity analysis showed that no individual study significantly influenced the rate of good outcome at 3 months (Supplemental Figure S2).
Secondary outcomes
We also observe a benefit of CS in terms of mortality. All five studies included in the analysis show higher rates of mortality in patients treated with GA and in three the differences were statistically significant. The pooled result confirms this data with higher mortality in the GA group (OR 0.48, 95% CI 0.28–0.82) with moderate heterogeneity (p = 0.10, I2 = 57.11%) (Figure 1(b)).
Four studies report data regarding the final recanalization rates. No significant differences were observed in terms of successful recanalization (OR 1.05, 95% CI 0.66–1.65) and there was no heterogeneity (p = 0.85, I2 = 0%) (Figure 2(a)). We observed similar results in the complete recanalization rates, with a mild tendency benefiting GA, although no significant differences were detected in the pooled analysis (OR 0.92, 95% 0.68–1.24) and there was no heterogeneity (p = 0.58, I2 = 0%) (Figure 2(b)).
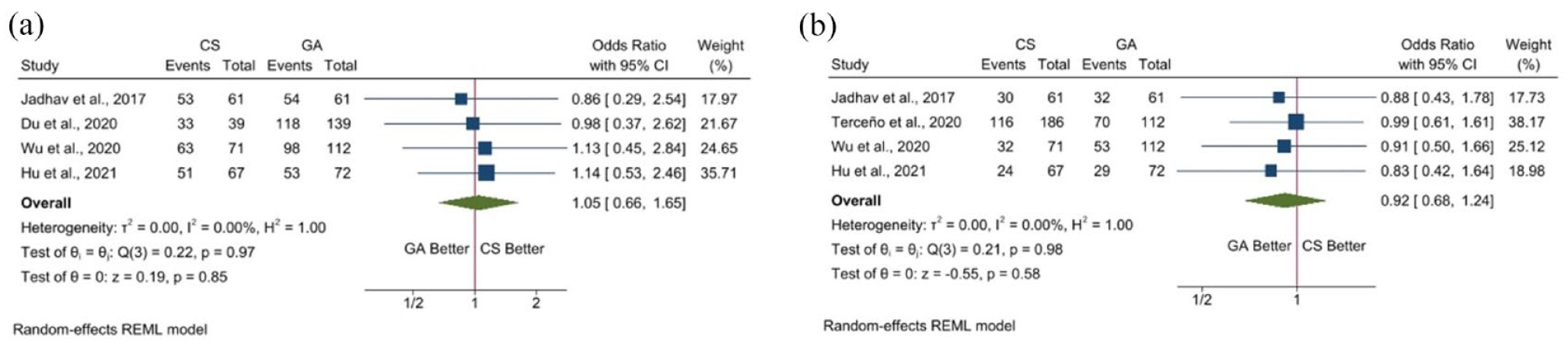
Forest plots for recanalization: (a) final successful recanalization (mTICI 2b–3) and (b) final complete recanalization (mTICI 3).
We have also analyzed data regarding times from procedure duration and stroke onset to recanalization. Patients treated under GA showed a lower duration of procedure, although no statistical differences were observed in the pooled analysis (OR 5.27, 95% CI −2.34 to 12.89) and the heterogeneity was mild (p = 0.17, I2 = 43.47%) (Figure 3(a)).

Forest plots for duration of procedure (a) and time from stroke onset to recanalization (b).
The three studies that reported data of times from stroke onset to recanalization found no differences between groups (OR −12.15, 95% CI −54.52 to 30.21) with no heterogeneity (p = 0.57, I2 = 0%) (Figure 3(b)).
A summary of the main results of this meta-analysis is given in Table 2.
Meta-analysis of outcomes according to anesthetic approach.
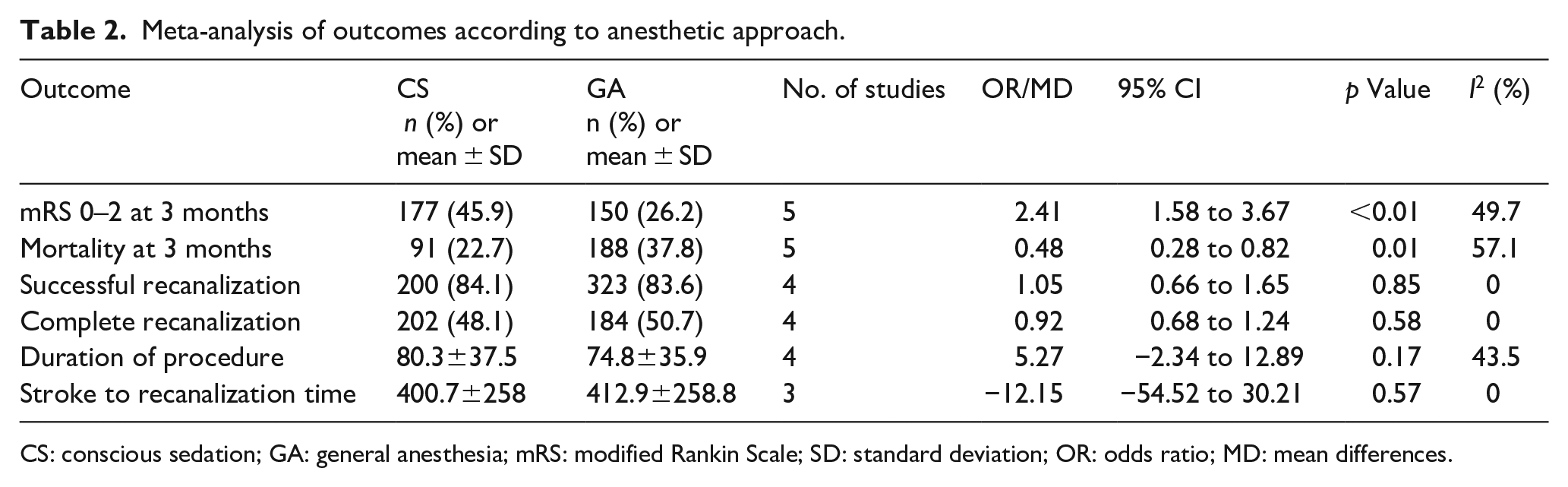
CS: conscious sedation; GA: general anesthesia; mRS: modified Rankin Scale; SD: standard deviation; OR: odds ratio; MD: mean differences.
Study heterogeneity
Moderate heterogeneity (I2 > 50%) was only observed for the mortality outcome. Low heterogeneity (I2 < 50%) was observed for functional independence and the duration of the procedure. Finally, no heterogeneity (I2 = 0%) was detected for the recanalization rates and the time from stroke onset to recanalization (Table 2).
Discussion
In this meta-analysis we report an association between GA use and poor clinical outcome in patients with PC-LVO treated endovascularly, with lower odds of functional independence at 3 months and higher mortality. There were no differences in successful reperfusion rates and any stroke to recanalization times. To the best of our knowledge, this is the first meta-analysis evaluating the effect of the anesthetic approach during EVT in patients with PC-LVO with a low overall risk of bias.
Some randomized clinical trials (RCT) have tried to compare the efficacy of GA and CS or local anesthesia (LA) in patients with anterior circulation LVO (AC-LVO) with variable results. In the SIESTA trial, the authors demonstrated the superiority of GA in achieving a good functional outcome after EVT with no differences in mortality between groups, although the primary outcome of this trial was the neurological improvement 24 h after EVT for which no differences were observed. 4 The GOLIATH trial failed to demonstrate differences in infarct growth between groups, but the GA group achieved better outcomes. 5 In the 2 other RCT conducted so far (ANSTROKE and CANVAS), no differences between GA and CS were observed.6,7 In the individual pooled meta-analysis that included the first 3 RCT with 368 patients studied, GA was identified as a predictor of good outcome (OR 1.58, 95% CI 1.09–2.29) for an ordinal shift on the mRS at 3 months and for mRS:0–2 (OR 2.16, 95% CI 1.31–3.54). 8
However, this potential benefit of GA over CS has not been observed in large population studies nor in non-RCT meta-analyses.3,9 Actually, the results of these three meta-analyses are in line with our meta-analysis in PC-LVO patients.
Finally, a recent meta-analysis that included 7797 patients from eight non-randomized studies found no differences between GA and CS regarding functional outcomes at 3 months. 10
Information related to the anesthetic approach in patients with PC-LVO is much less well-known. No clinical trials have been conducted so far, although CANVAS-2 is an RCT that is recruiting patients with PC-LVO and results are expected to be completed in December 2023 (ClinicalTrials.gov Identifier: NCT03317535). 11 Only a few prospective and retrospective series have been published, while no meta-analyses have been conducted to date.
Most of these studies failed to demonstrate statistical differences between anesthetic approaches, however, a tendency of a benefit in avoiding GA is observed in most of them. In a retrospective analysis of 100 patients, Mokin et al. reported lower rates of functional independence in the GA group (26.7% vs 47.5%, p = 0.053), however, GA was not associated with clinical outcome in the multivariate analysis. 12 Similar results were published by Bouslama et al. with 214 patients studied retrospectively. They identified smoking, low baseline NIHSS and successful recanalization with good outcome, but not any particular anesthetic approach. 13 This group also conducted a retrospective matched case-control study with 122 patients, analyzing the effect of CS or elective GA on clinical outcome. The results showed no differences between the two groups. 14 Two Asian groups have recently published studies outlining their experience. Wu et al. prospectively studied 183 patients, with no differences in the primary outcome (median mRS at 90 days). 15 In contrast, Du et al. reporting data from 178 patients with basilar artery occlusion, identified the use of GA as an independent variable associated with poor outcome (OR 0.31, 95% CI 0.13–0.75). 16 Our group has also published a study setting out our experience. In a retrospective multicenter analysis of 298 patients with PC-LVO from the CICAT registry, we identified GA as an independent predictor of poor outcome (OR 3.11, 95% CI 1.34–7.2). Patients from the GA group were less likely to be functionally independent at 3 months compared to the CS group (19.7% vs 45.2%, p < 0.001). 17 In both studies multivariable analysis was adjusted by baseline characteristics, such as age and NIHSS.
This meta-analysis reveals an association between GA use and worse functional outcome in patients with PC-LVO with mild heterogeneity between the studies included in the analysis.
Mortality has been assessed in several studies. The results also point to a potential harm of GA with higher rates of mortality in all studies, although only one study has specifically evaluated mortality and its association with GA. Gory et al. studied predictors of mortality after EVT in 117 consecutive patients with basilar artery occlusions. Patients that died during follow-up had more frequently been treated with GA (91.7% vs 75.1%, p = 0.028), however, this association did not remain significant in the multivariable analysis. 18 The pooled analysis of our study also confirms this data with a statistical association being found between GA use and mortality at 3 months. In this outcome, a moderate heterogeneity (I2 > 50%) was observed that is likely related to the study of Wu et al. 15
In our meta-analysis, we did not find differences in final reperfusion rates (both successful and complete recanalization). Most of the studies show higher rates of complete recanalization in the GA group, although no statistical differences are observed. These results contrast with some AC-LVO trials and the meta-analysis of these, since a significant association between GA use and successful recanalization has been observed.5,7,8
With respect to the duration of the procedure, the results of the present meta-analysis were in line with the meta-analysis of clinical trials in anterior circulation, 8 with shorter times being observed in the GA group with no statistical differences, although this does not have an impact on the clinical outcome. Finally, the analysis of the data of time from stroke onset to reperfusion was similar in the two groups.
Despite the considerable number of published studies, no precise hypotheses have been able to account for the potential association between GA use and worse clinical outcome. One possible explanation is that the worse outcome is a result of the expected arterial hypotension due to GA use, especially in the anesthetic induction period. The drop in blood pressure during EVT prior to arterial recanalization has been extensively associated with large final cerebral infarction and worse clinical outcome.26,27 Likewise, the endovenous use of some anesthetic agents has been associated with arterial hypotension and a negative impact on collateral circulation, resulting in an infarct growth. 28 Although these drugs could cause arterial hypotension, the impact on intracranial vasculature perfusion can vary. 29 Given this, the relationship between a drop in blood pressure and neurological outcome could be explained by the use of particular anesthetic agents, rather than the choice of GA or CS as an anesthetic approach. There is no evidence that a potential correlation between GA use and arterial hypotension might result in a worse outcome. Unfortunately, there are currently no studies in PC-LVO patients available in this field.
While one of the main reasons for using GA in EVT of stroke is the airway control, AC-LVO meta-analyses failed to demonstrate that the use of GA was better than CS, since the CS group was associated with more respiratory infections and longer intensive care unit stays.3,8,9
Although the data in the studies included in the meta-analysis related to both neurological and non-neurological procedural complications are insufficient to be analyzed, no significant differences were observed in two of these studies when comparing GA with CS as the anesthetic approach for EVT completion.15,19
Limitations
Our meta-analysis has some limitations. The number of studies included is relatively low, most of them are retrospective series, and no clinical trials are reported in the literature. The heterogeneity is substantial in some outcomes, although the risk of bias was reasonably excluded. Furthermore, since it was not possible to extract sufficient data from these studies related to complications during the endovascular treatment, such as intracranial hemorrhage and respiratory infections, this part of the analysis could not be performed. Also, differences in anesthetic regimen during the EVT between studies could have some impact on final results.
Finally, the moment at which oral intubation is performed may have an impact on the clinical outcome since those patients with worse neurological status on onset are more likely to be intubated prior to EVT. In this meta-analysis, three of the studies excluded patients intubated prior to EVT, however, their results are in line with the pooled analysis. In two of these studies the clinical outcome was significantly worse in patients treated with elective GA,14,16 whereas the other study did not show differences between the CS and GA elective groups. 19 Finally, in two other studies included in this meta-analysis, GA was independently associated with worse clinical outcome, after adjusting by baseline characteristics including age, NIHSS and time from stroke onset to recanalization,15,17 while GA was not associated with good outcomes, compared to CS, in any of the studies.
Conclusions
To the best of our knowledge, this is the first meta-analysis assessing the effect of GA and CS during endovascular treatment in patients with PC-LVO. GA was associated with significantly lower rates of functional independence at 3 months, together with higher mortality. It would be interesting to conduct a randomized clinical trial to evaluate the effect of anesthesia in this group of patients.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221127738 – Supplemental material for General anesthesia versus conscious sedation during endovascular treatment in posterior circulation large vessel occlusion: A systematic review and meta-analysis
Supplemental material, sj-docx-1-eso-10.1177_23969873221127738 for General anesthesia versus conscious sedation during endovascular treatment in posterior circulation large vessel occlusion: A systematic review and meta-analysis by Mikel Terceño, Saima Bashir, Juan Cienfuegos, Alan Murillo, Víctor Augusto Vera-Monge, Laura Pardo, Montserrat Reina, Carme Gubern-Mérida, Dolors Puigoriol-Illamola, Laia Carballo, Anna Costa, Maria Buxó, Joaquín Serena and Yolanda Silva in European Stroke Journal
Supplemental Material
sj-jpg-3-eso-10.1177_23969873221127738 – Supplemental material for General anesthesia versus conscious sedation during endovascular treatment in posterior circulation large vessel occlusion: A systematic review and meta-analysis
Supplemental material, sj-jpg-3-eso-10.1177_23969873221127738 for General anesthesia versus conscious sedation during endovascular treatment in posterior circulation large vessel occlusion: A systematic review and meta-analysis by Mikel Terceño, Saima Bashir, Juan Cienfuegos, Alan Murillo, Víctor Augusto Vera-Monge, Laura Pardo, Montserrat Reina, Carme Gubern-Mérida, Dolors Puigoriol-Illamola, Laia Carballo, Anna Costa, Maria Buxó, Joaquín Serena and Yolanda Silva in European Stroke Journal
Supplemental Material
sj-png-2-eso-10.1177_23969873221127738 – Supplemental material for General anesthesia versus conscious sedation during endovascular treatment in posterior circulation large vessel occlusion: A systematic review and meta-analysis
Supplemental material, sj-png-2-eso-10.1177_23969873221127738 for General anesthesia versus conscious sedation during endovascular treatment in posterior circulation large vessel occlusion: A systematic review and meta-analysis by Mikel Terceño, Saima Bashir, Juan Cienfuegos, Alan Murillo, Víctor Augusto Vera-Monge, Laura Pardo, Montserrat Reina, Carme Gubern-Mérida, Dolors Puigoriol-Illamola, Laia Carballo, Anna Costa, Maria Buxó, Joaquín Serena and Yolanda Silva in European Stroke Journal
Footnotes
Acknowledgements
We would like to thank Andrew Hughes for his help in the linguistic revision of this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Spanish Stroke Research Network RETICS RD16/0019/0003.
Informed consent
Since the present manuscript is related to a systematic review and meta-analysis, informed consent is not required.
Ethical approval
Since the present manuscript is related to a systematic review and meta-analysis, ethical approval is not required. Data related to our series, was regulated by our Local Ethical Committee.
Guarantor
The guarantor of this meta-analysis is Dr. Joaquin Serena.
Contributorship
All authors reviewed and edited the manuscript and approved the final version of the manuscript
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.