
Abstract
Introduction:
In the context of modern guideline-based strategies, new validations of prognostic scores for predicting early stroke risk are needed. We aimed to compare the validity of the ABCD series scores and assess the incremental values of risk components for predicting in-hospital stroke events in patients with transient ischemic attack (TIA).
Patients and methods:
We abstracted data from the Chinese Stroke Center Alliance (CSCA), a nationwide registry with 68,433 TIA patients admitted within 7 days of symptom onset from 1476 hospitals. TIA was defined by time-based criteria according to the World Health Organization (WHO). The discrimination of ABCD, ABCD2, ABCD2-I, and ABCD3 scores for predicting in-hospital stroke events was assessed by the area under the receiver-operating characteristics curves (AUC). The incremental predictive values of added risk predictor were determined by net reclassification improvement (NRI) and integrated discrimination improvement (IDI).
Results:
A total of 29,286 TIA patients were included, of whom 1466 (5.0%) had in-hospital stroke events. Compared with ABCD2-I score (AUC 0.79, 95% confidence interval [CI] 0.77–0.80), ABCD (AUC 0.58, 95% CI 0.57–0.60), ABCD2 (AUC 0.58, 95% CI 0.56–0.59), and ABCD3 (AUC 0.58, 95% CI 0.56–0.60) had lower predictive utility. An incremental value was observed when adding infarction on DWI (IDI = 0.0597, NRI = 1.1036) into ABCD2 score to be ABCD2-I.
Conclusion:
The traditional scales utilizing medical history (ABCD, ABCD2, and ABCD3 scores) show fair ability for predicting in-hospital stroke events after TIA, but the ABCD2-I score, which adds infarction on DWI, improves the predictive ability.
Introduction
Subsequent stroke after a transient ischemic attack (TIA) often occurs early with 2.1%–5.2% risks during the first 7 days.1,2 Thus, ABCD series clinical risk scores have been developed and widely used to stratify subsequent stroke risk and identify high-risk TIA patients.
Based on the earlier evidence for clinical variables associated with increased stroke risk, the ABCD score was derived as a six-point score with age, blood pressure, clinical features, and duration of symptoms. 3 The ABCD2 score was further established by adding diabetes mellitus as a risk component. 4 Since the presence of abnormal findings on neuroimaging has been suggested to be strongly associated with higher early stroke risk,5,6 infarction on diffusion-weighted images (DWI) was added to the ABCD2 score to establish the ABCD2-I score. 7 Moreover, dual TIA was incorporated into the ABCD2 score to establish the ABCD3 score. 8
Although some of these four scores have been externally validated by many studies with relatively a small sample size.9 –11 To date, systematic and detailed validations of these four scores concurrently in the same large-scale cohorts are lacking. 12 In addition, the management, including treatments and prevention strategies of TIA patients, have been significantly changed over time which may challenge the predictive utility of ABCD series scoring systems.
We aimed to assess the external validity and directly compare the predictive utility of the four ABCD series scores for in-hospital subsequent stroke events after TIA in a large-scale Chinese cohort. In addition, we also assessed the incremental value of each adding predictor in these scoring systems.
Methods
Study population
Data were retrospectively abstracted from the Chinese Stroke Center Alliance (CSCA), a nationwide multicenter, prospective, hospital-based registry with a total of 1,006,798 acute stroke or TIA patients recruited from 1476 hospitals in China. Individuals over 18 years old were admitted continuously within 7 days of symptoms onset between August 1, 2015 and July 31, 2019. The protocol for the details of the registry was published previously.13,14 For the current analysis, we included patients who had a diagnosis of TIA at admission confirmed by a neurologist based on the traditional time-oriented definition, which was defined as neurological symptoms of supposed cerebrovascular origin lasted less than 24 h according to the World Health Organization (WHO). 15 There are some patients with transient focal neurological symptoms which are not due to focal cerebral ischemia, such as epileptic seizures, migraine, hypoglycemia, drunk. Those patients were not included in the registry because the standard TIA diagnosis was based on medical history, symptoms, and Physical examination by experts. The diagnosis relies heavily on the patient’s account of their history and on expert interpretation of that history. In the emergency department, fasting glucose testing, physical examination, medical history and presentations, as well as laboratory tests will be performed, in particularly, whether the symptoms correspond to cerebral territory, and TIA diagnosis will be differentiated from by other TIA mimics. Individuals who had a history of prior stroke, missing data on key clinical characteristics (age, blood pressure, diabetes mellitus, clinical features, duration of symptoms, or dual TIA), neuroimaging (DWI information), or major outcome information (subsequent stroke events) were excluded, leaving 29,286 patients as the final study population (Supplemental Figure).
Data collection
Data were collected from medical records in routine clinical practice by trained neurologists and uploaded to a web-based patients data collection and management tool (Medicine Innovation Research Center, Beijing, China). We obtained information of patients’ demographics, medical history, clinical symptoms, laboratory tests, DWI signal, medications strategy, in-hospital outcomes. The whole process had no influence on the clinical practice.
Definitions and outcomes
Training programs on the detailed definition of each category were provided online and offsite for all investigators. Hypertension was defined as a systolic blood pressure (SBP) >140 mmHg or diastolic blood pressure (DBP) >90 mmHg or use of antihypertensive medication before. Fasting blood glucose greater than 126 mg/dL (7.0 mmol/L) with diabetes symptoms or current use of hypoglycemic drugs were defined as diabetes mellitus. Dyslipidemia was defined as low-density lipoprotein cholesterol (LDL-C) >160 mg/dL (4.13 mmol/L) or current use of lipid lowering drugs. Dual TIA was defined as TIA requiring medical attention plus at least one other TIA in the preceding 7 days. The history of smoking, atrial fibrillation and myocardial infarction were also collected. Early antithrombotics was defined as aspirin, clopidogrel, or aspirin and clopidogrel use in 48 h after admission. DWI hyperintensity was recorded as positive if the image had at least one acute cerebral ischemic lesion judged by the local neuroradiologist or stroke physician.
The ABCD score (low-risk 0–2, medium-risk 3–4, and high-risk 5–6) was calculated as follows: age ⩾60 years (1 point); blood pressure ⩾ 140/90 mmHg (1 point); clinical features of unilateral weakness (2 points) or speech impairment without weakness (1 point); duration of symptoms ⩾60 min (2 point) or 10–59 min (1 point). On the basis of the ABCD score, diabetes mellitus (1 point) was added as an additional component to calculate the ABCD2 score (low-risk 0–3, medium-risk 4–5, and high-risk 6–7). Furthermore, acute DWI hyperintensity (3 points) was incorporated into the ABCD2 score to establish the ABCD2-I score (low-risk 0–3, medium-risk 4–6, and high-risk 7–10), and dual TIA within 7 days (2 points) was added to ABCD2 score to form the ABCD3 score (low-risk 0–3, medium-risk 4–5, and high-risk 6–9).
The primary outcome of this study was subsequent stroke events (including ischemic and hemorrhagic stroke) after TIA during hospitalization. Stroke events were judged by local neurologists based on the definition described as a rapidly developed clinical symptom of focal (or occasionally global) disturbance of cerebral function, lasting more than 24 h or until death, with no apparent non-vascular cause, and confirmed on the basic of medical records. 16
Statistical analysis
Quantitative variables with normal distribution were described as mean ± SD, while those with skewed distribution were described as median (interquartile range). For the extensive data set, p < 0.05 indicates statistical significance, but the result may not have clinical significance. Therefore, baseline characteristics and outcomes were compared using the absolute standardized difference (ASD). An ASD ⩾10% was considered to be clinically significant. 17
The discrimination of ABCD, ABCD2, ABCD2-I, and ABCD3 scores for predicting in-hospital stroke events was assessed by the AUC or C-statistics, and the calibration was evaluated by comparing the in-hospital stroke events rates among different risk score groups (low, medium, and high) for each score system. The incremental predictive values of added risk predictor were determined by net reclassification improvement (NRI) and integrated discrimination improvement (IDI). 18 NRI means the net increase versus decrease in risk categories among patients with subsequent stroke events minus that among patients without stroke events. IDI means the difference in Yates slopes between models, in which the Yates slope is the mean difference in predicted probabilities between patients with stroke events and patients without stroke events. 19
Results
Clinical characteristics of the subjects
The included and excluded patients were largely comparable except that the included patients had higher proportion of early antithrombotic therapy. A similar situation was observed between the included patients and those who excluded due to lack of DWI scan (Supplemental Tables 1 and 2).
Of the 29,286 included patients, baseline characteristics were shown in Table 1. A total of 1466 (5.0%) patients experienced subsequent stroke events during hospitalization. When compared with patients who did not have in-hospital stroke events, they had a higher proportion of men (63.6% vs 57.6%, ASD = 12.3%), higher prevalence of history of smoking (42.4% vs 33.5%, ASD = 18.4%), hypertension (60.0% vs 54.4%, ASD = 11.3%), lower prevalence of dyslipidemia (4.3% vs 7.0%, ASD = 11.7%), prior TIA (9.5% vs 13.8%, ASD = 13.4%), and more patients were treated with dual antiplatelet therapy (68.4% vs 51.2%, ASD = 35.6%), but lower prevalence of patients were treated with aspirin alone (20.5% vs 29.9%, ASD = 21.8%) or clopidogrel alone (4.3% vs 6.9%, ASD = 11.3%).
Clinical characteristics of included patients.
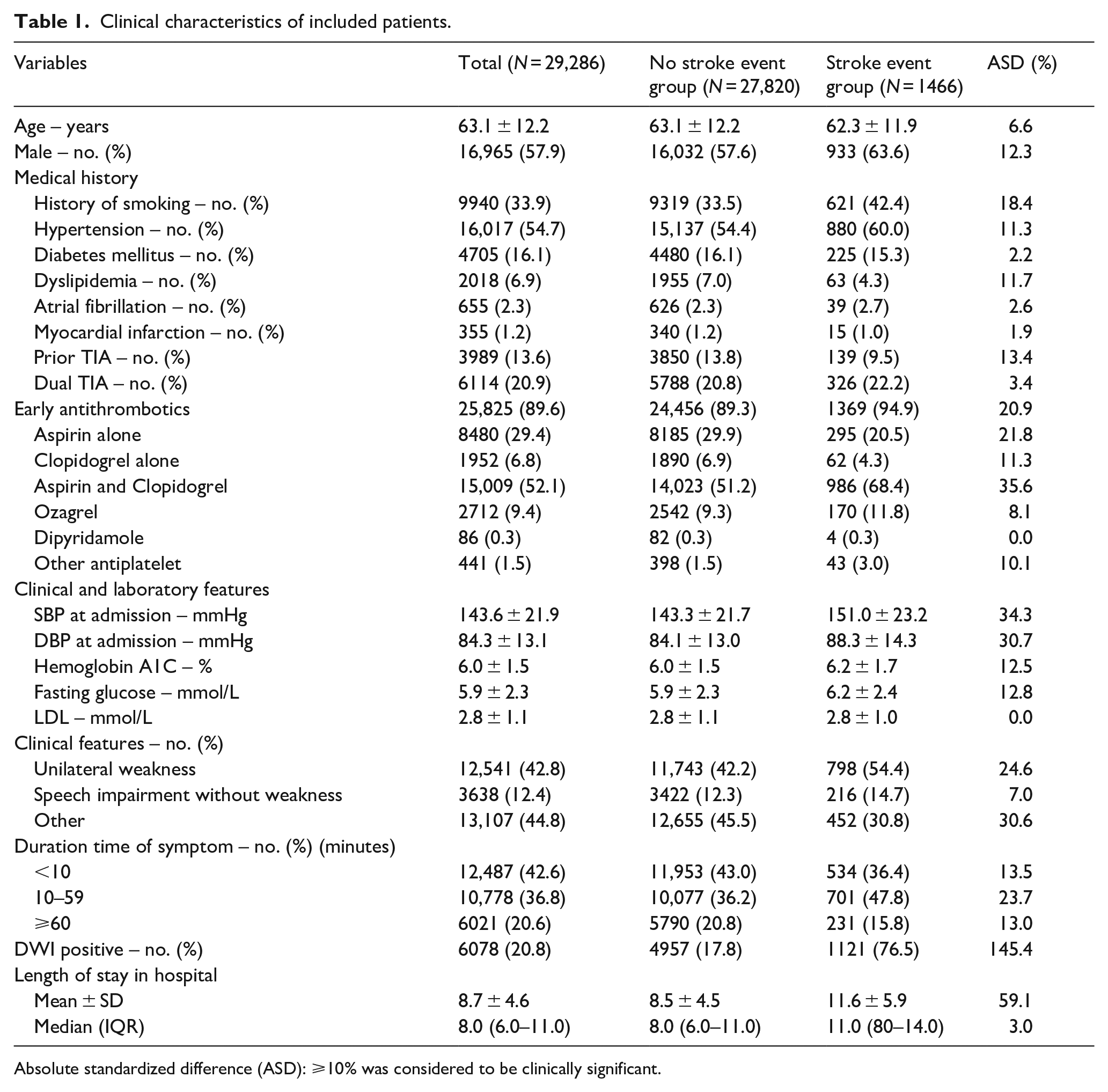
Absolute standardized difference (ASD): ⩾10% was considered to be clinically significant.
SBP and DBP on admission were higher in patients who had subsequent stroke events than that in patients who did not have (151.0 ± 23.2 vs 143.3 ± 21.7 mmHg, ASD = 34.3%; 88.3 ± 14.3 vs 84.1 ± 13.0 mmHg, ASD = 30.7%, respectively). The proportions of clinical features such as unilateral weakness (54.4% vs 42.2%, ASD = 24.6%), duration time of symptom (<10 min [36.4% vs 43.0%, ASD = 13.5%], 10–59 min [47.8% vs 36.2%, ASD = 23.7%], ⩾60 min [15.8% vs 20.8%, ASD = 13.0%]) showed significant differences between the two groups. Particularly, the proportion of DWI positive in stroke event group was as four times as that in no stroke event group (76.5% vs 17.8%, ASD = 145.4%). We also compared the differences between included patients having DWI lesions and those with no lesions. As shown in Supplemental Table 3, patients having DWI lesions had a higher proration of patients who were treated with aspirin and clopidogrel (59.9% vs 50.0%, ASD = 20%), but less treated with aspirin alone (23.2% vs 31.0%, ASD = 17.6%), and less patients had the history of prior TIA (9.5% vs 13.8%, ASD = 13.4%).The length of hospital stay was longer in the patients with DWI lesions (9.6 ± 5.1 vs 8.4 ± 4.4, ASD = 25.2%).
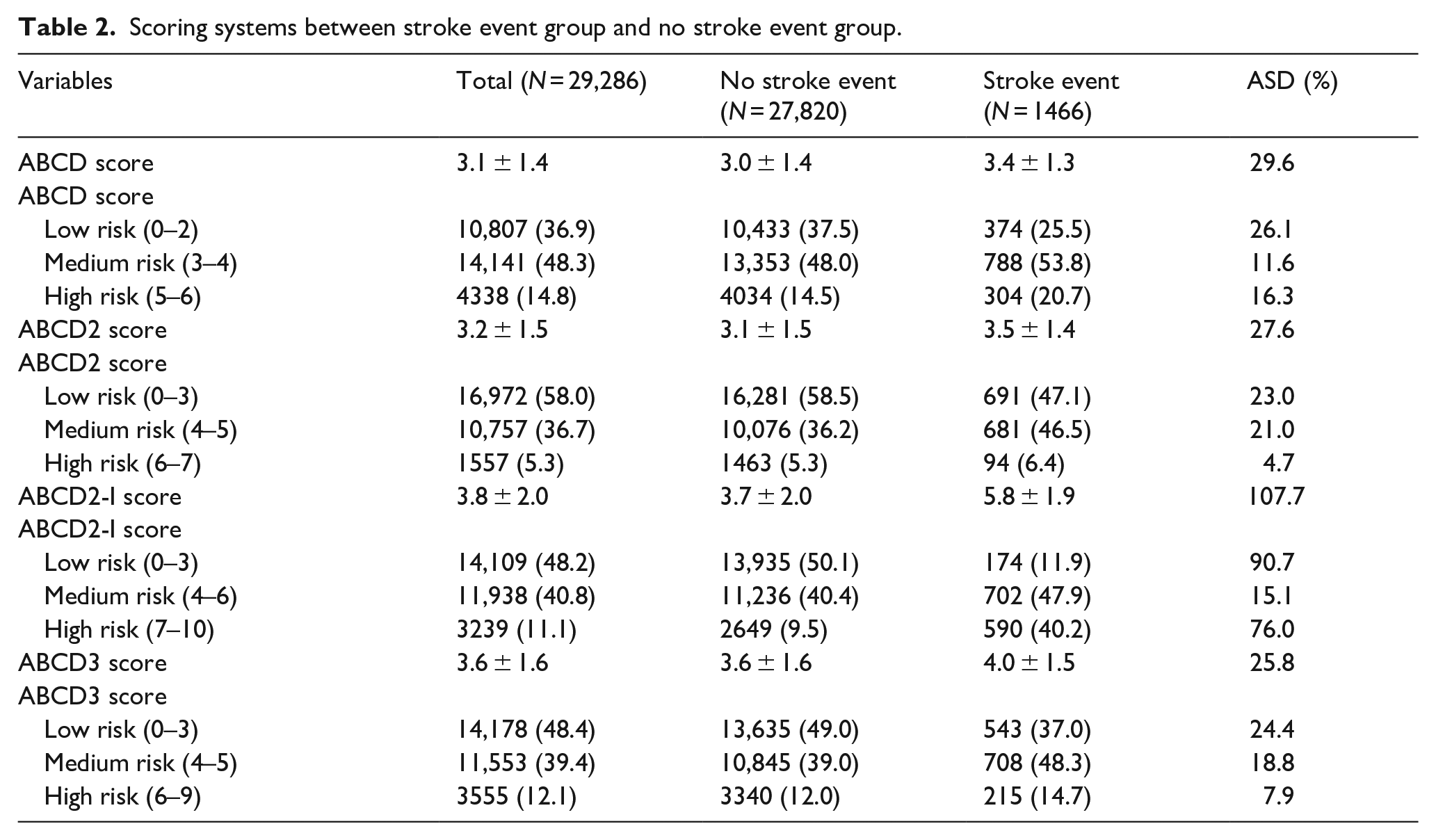
As shown in Table 2, the mean ± SD of ABCD score, ABCD2 score, ABCD2-I score, and ABCD3 score for the total study population were 3.1 ± 1.4, 3.2 ± 1.5, 3.8 ± 2.0, and 3.6 ± 1.6, respectively. Patients who had subsequent stroke events had higher ABCD, ABCD2, ABCD2-I, ABCD3 scores than the patients with no stroke events (ABCD score: 3.4 ± 1.3 vs 3.0 ± 1.4, ASD = 29.6%; ABCD2 score: 3.5 ± 1.4 vs 3.1 ± 1.5, ASD = 27.6%; ABCD2-I score: 5.8 ± 1.9 vs 3.7 ± 2.0, ASD = 107.7%; ABCD3 score: 4.0 ± 1.5 vs 3.5 ± 1.6, ASD = 25.8%). More patients were classified into the high-risk group in patients with stroke event than those without. Figure 1 demonstrated that the higher the risk group determined by the ABCD score and ABCD2-I score, the higher the rates of in-hospital stroke events. The risk groups based on the ABCD2-I score showed significantly better discrimination. For stroke risk stratified by the ABCD2 score, the in-hospital stroke event rates were 4.1%, 6.3%, and 6.0% in the low-, medium-, and high-risk group, respectively. When stratified by the ABCD3 score, the rates were 3.8%, 6.1%, and 6.0% in the low-, medium-, and high-risk group, respectively. The ABCD2 score and ABCD3 score did not show significant distinction, especially between the medium-risk and high-risk categories.
Scoring systems between stroke event group and no stroke event group.
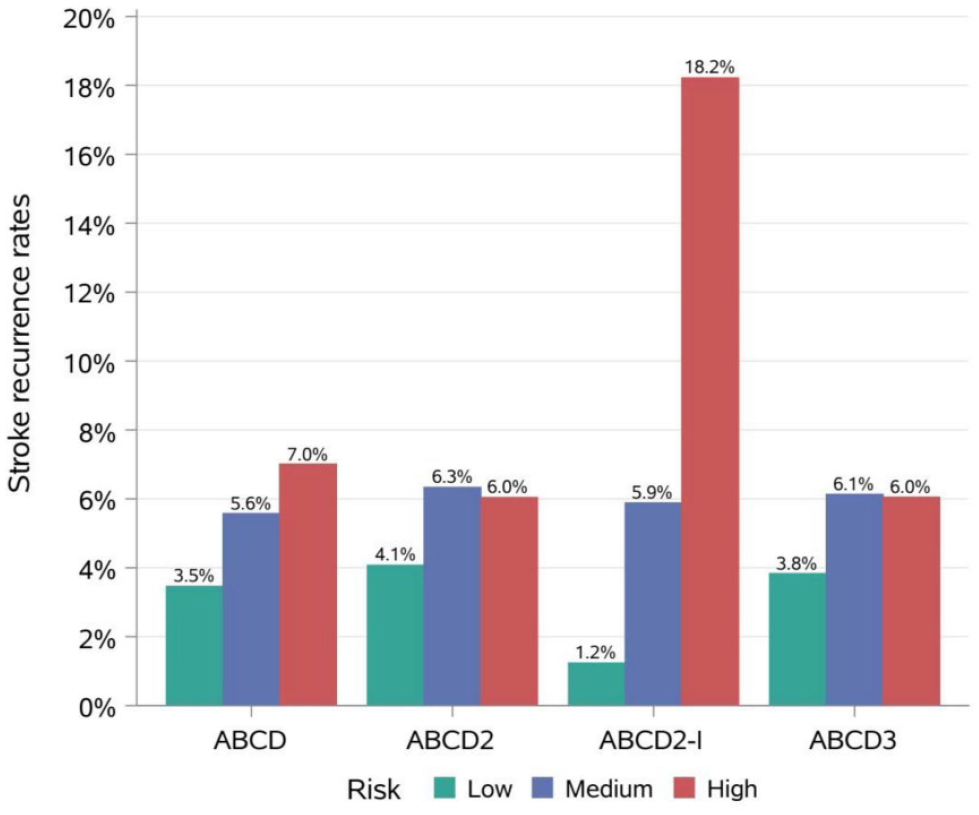
Classification of patients from low, medium, and high categories of four scores stratified by rates of in-hospital recurrent stroke events.
Predictive abilities of the ABCD series scores
The predictive abilities of the ABCD series scores were shown in Table 3. The threshold values for ABCD, ABCD2, ABCD2-I, and ABCD3 were 3, 4, 5, and 2, respectively. Compared with ABCD2-I score (AUC = 0.79 [95% CI 0.77–0.80]), other scores, including ABCD (AUC = 0.58 [95% CI 0.57–0.60]), ABCD2 (AUC = 0.58 [95% CI 0.56–0.59]), and ABCD3 (AUC = 0.58 [95% CI 0.56–0.59]) had lower short-term predictive utility for in-hospital stroke events (Figure 2). Other measures, including sensitivity, specificity, positive predictive value, and negative predictive value, indicated that ABCD2-I had the highest predictive ability as well (Table 3).
Comparison of four scores’ predictive ability for predicting in-hospital stroke events.
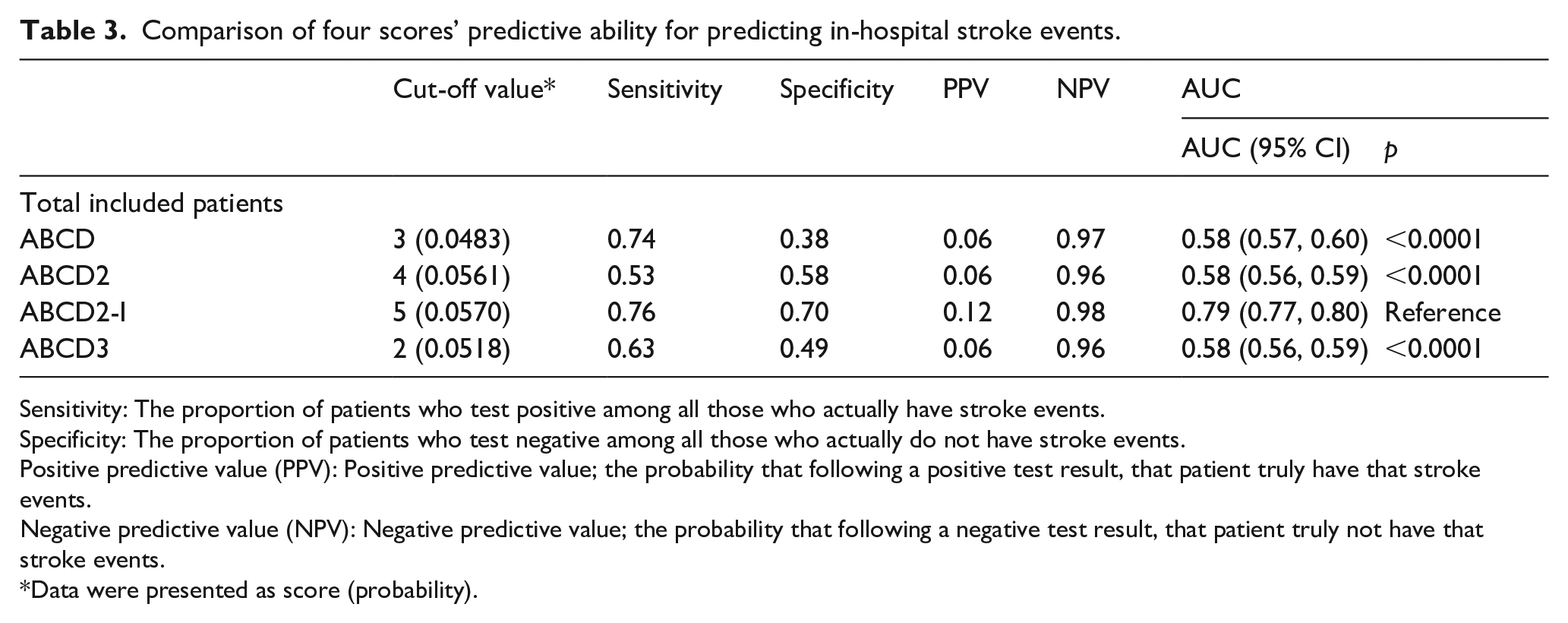
Sensitivity: The proportion of patients who test positive among all those who actually have stroke events.
Specificity: The proportion of patients who test negative among all those who actually do not have stroke events.
Positive predictive value (PPV): Positive predictive value; the probability that following a positive test result, that patient truly have that stroke events.
Negative predictive value (NPV): Negative predictive value; the probability that following a negative test result, that patient truly not have that stroke events.
Data were presented as score (probability).
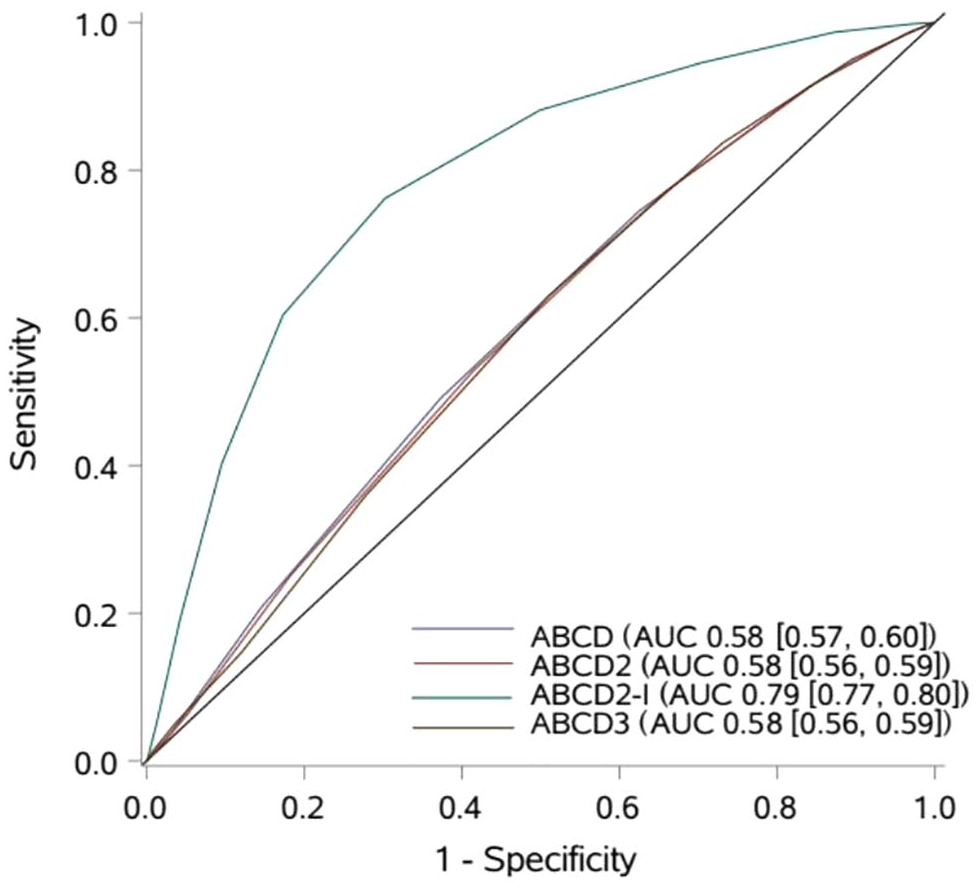
The receiver-operating characteristic curves (ROC) of four scores for prediction of in-hospital subsequent stroke events in TIA patients.
Incremental predictive values of added risk predictor
Table 4 demonstrates that after adding diabetes as a new predictor, the IDI and NRI of ABCD2 versus ABCD were negative values (IDI = −0.0005, NRI = −0.1466). No incremental value was observed after incorporating dual TIA as a component in ABCD3, compared with the ABCD2 score (IDI = −0.0002, NRI = −0.0018). However, after adding infarction on diffusion-weighted images in the ABCD2-I scores as a novel factor showed an incremental value for the predictive ability (IDI = 0.0597, NRI = 1.1036).
IDI, NRI after predictors added.
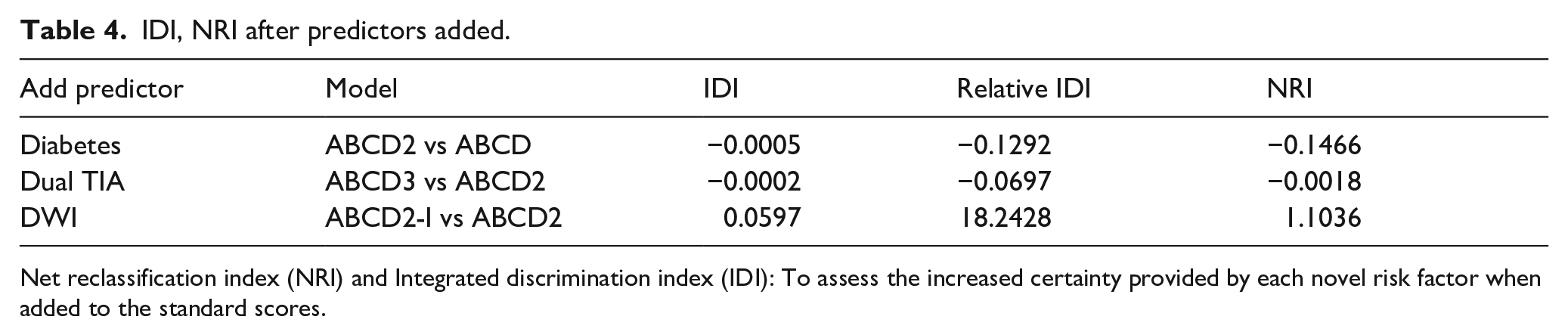
Net reclassification index (NRI) and Integrated discrimination index (IDI): To assess the increased certainty provided by each novel risk factor when added to the standard scores.
To further explore the predictive value of DWI, we also calculated the numbers and risk of stroke at each score stratified by DWI results. It indicated that DWI positive group had a much higher risk of stroke than DWI negative group at each score (Supplemental Table 4).
Discussion
Utilizing the data from a large nationwide registry, we assessed and compared the predictive ability of the ABCD series scoring systems. We found that the ABCD, ABCD2, ABCD3 scores showed sub-optimal predictive utility for predicting in-hospital subsequent stroke events in the context of modern guideline-based management. However, the ABCD2-I score, which added infarction on DWI as a novel risk component, showed an improving predictive ability.
The rate of stroke events after TIA during hospitalization was within the range reported by the previous studies, which was 2%–5.2% in 7 days after TIA.2,20,21 Patients who met the inclusion criteria were registered instead of whom considered to be at a higher risk of subsequent stroke events. The results from Table 2 showed that 58% were classified as low-risk by the ABCD2 score. In addition, the characteristics and the rates of target events in this study were similar to the whole Third China National Stroke Registry (CNSR-III), a large national multicenter, prospective cohort of ischemic cerebrovascular disease registry, which would minimize the selection bias of study population. 22 Patients who performed MRI were finally included. Whether a patient performs an MRI or not is mostly left to the clinical decisions made by the local neurologist and the patients. Excluding patients without MRI may introduce bias but no significant differences were found for most of the variables of baseline characteristics between the included patients and excluded patients lack of MRI (Supplemental Table 2).
The ABCD2-I score, which adds infarction on diffusion-weighted images as a risk component, has the highest AUC for predicting in-hospital stroke events. Compared with ABCD2 and ABCD3 scores, the ABCD and ABCD2-I scores improved the identification of the high-risk patients. ABCD2-I showed significant improvement in identifying the high-risk patients than ABCD score. In addition, we found that the ABCD2 score, which is the most commonly used predicting score in clinical practice, was not effective in stroke risk stratification as reported before. Of the patients who experienced stroke events, 1121 (76.5%) were DWI-positive and 345 (23.5%) were DWI-negative. This provided a piece of evidence that DWI can distinguish patients at higher risk of early stroke events after TIA, which is consistent with previous studies showing that DWI was positively associated with subsequent stroke events.20,21,23,24 IDI and NRI are two critical measures for scale assessment. No incremental value was observed after incorporating diabetes or dual TIA as components, but imaging component (DWI hyperintensity) is much more critical for subsequent stroke risk. Also, as seen in Supplemental Table 4, DWI positive group had a much higher risk of subsequent stroke events than DWI negative group at each score. The underline reasons may be that patients with positive DWI had more vascular risk factors than those negative (Supplemental Table 3)
In our study, prescription of aspirin alone and clopidogrel alone were higher in patients without stroke events, while prescription of aspirin and clopidogrel were higher in patients with stroke events, which could be misleading. Previous studies (The Clopidogrel in High-Risk Patients with Acute Nondisabling Cerebrovascular Events, CHANCE; Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke, POINT) have demonstrated that DAPT is superior to aspirin alone for reducing the risk of stroke in the first 90 days. 25 The underline reason may be that patients with more vascular risk factors were in more poor underlying vascular status therefore they were more likely to be treated with dual-antiplatelet therapy. Another possible reason is that stroke events occurred within 48 h of admission increased the use of early DAPT therapy, which may present a misleading conclusion. However, we cannot quantify how many stroke events occurred within 48 h, as the detailed time was not collected.
Our study has certain limitations. First, the hospitals were voluntarily enrolled and did not have any elaborately designed sampling frame. However, the large sample size helped improve the generalizability of the study. Second, our study was designed to validate the scores for predicting in-hospital stroke events because the onset time of target invents was not recorded, which could limit the comparisons. Third, we did not record the date and time of in-hospital stroke events; therefore, stroke events occurred within 48 h of admission may increase the use of early antithrombotics (especially dual antiplatelet therapy), which may present a misleading conclusion. Fourth, the long-term follow-up data of the stroke event was not recorded in this registry. However, as reported by the previous studies, TIA carries a high early risk of stroke especially in the first 2 weeks which is similar to the length of the hospital stay. In addition, short-term recurrence is consistent with the original purpose of the ABCD series scoring system, which is also predicting early stroke recurrence.
Conclusion
The traditional scales utilizing medical history (ABCD, ABCD2, and ABCD3 scores) show fair ability for predicting in-hospital stroke events after TIA, but the ABCD2-I score, which adds infarction on DWI, improves the predictive ability.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221113145 – Supplemental material for External validation of ABCD series scores for predicting early stroke events following transient ischemic attack in a large nationwide registry
Supplemental material, sj-docx-1-eso-10.1177_23969873221113145 for External validation of ABCD series scores for predicting early stroke events following transient ischemic attack in a large nationwide registry by Jia-Xu Weng, Hong-Qiu Gu, Shang Wang, Kai-Xuan Yang, Xin Yang, Chun-Juan Wang, Xia Meng, Xing-Quan Zhao, Yong-Jun Wang and Zi-Xiao Li in European Stroke Journal
Footnotes
Acknowledgements
We would like to thank all the participating centers in the CSCA program for their hard work on data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (72004146, 92046016), Beijing Hospitals Authority (PX2021024), Beijing Talents Project (4922018000021223ZK03), Beijing Municipal Science & Technology Commission (D171100003017002), CAMS Innovation Fund for Medical Sciences (2019-I2M-5-029), Beijing Natural Science Foundation (Z200016), and National Science and Technology Major Project (2017ZX09304018).
Ethical approval
The ethics committee of Beijing Tiantan Hospital approved this study (REC number: KY2018-061-02). All participating centers received both clinical quality assessment and research approval to collect data without requiring individual patient’s consent under the common rule or a waiver of authorization and exemption from their Institutional Review Boards.
Informed consent
All participating centers received both clinical quality assessment and research approval to collect data without requiring individual patient’s consent under the common rule or a waiver of authorization and exemption from their Institutional Review Boards.
Guarantor
Zi-Xiao Li.
Contributorship
Jia-Xu Weng, Hong-Qiu Gu and Shang Wang researched literature and conceived the study. Hong-Qiu Gu and Kai-Xuan Yang was involved in data analysis and interpretation. Jia-Xu Weng wrote the first draft of the manuscript. Zi-Xiao Li, Xia Meng, Hong-Qiu Gu and Shang Wang conceived the methodology. Zi-Xiao and Yong-Jun Wang involved in funding acquisition. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.