
Abstract
Introduction:
The objective of the study was to assess use and persistence of secondary preventive treatment after ischemic stroke comparing immigrants and Danish-born residents.
Patients and methods:
A cohort of patients discharged with ischemic stroke (IS) diagnosis (n = 106,224) by immigration status was identified from the Danish Stroke Registry between 2005 and 2018. We investigated use (claiming at least one prescription in 180 days post-discharge according to information from the Register of Medicinal Products Statistics) and persistence of treatment within 180 days thereafter using multivariable logistic regression and Fine and Gray models.
Results:
Overall, 82,078 Danish-born residents (80.6%) and 3589 (80.7%) immigrants with IS used at least one of the recommended preventive medications post-discharge. Immigrants had lower odds of use of anticoagulants and angiotensin-converting enzyme (ACE) inhibitors/angiotensin II receptor blockers (ARB) (odds ratio (OR), 0.66; 95% confidence interval (CI), 0.53–0.82 and OR, 0.87; 95% CI, 0.75–0.98, respectively) but had higher odds of use of beta-blockers (OR, 1.25; 95% CI, 1.02–1.53) than Danish-born residents after adjustment for age at stroke, sex, sociodemographic factors, duration of residence, stroke severity, and comorbidities. The odds were most evident among immigrants originating from non-Western countries. Persistence of medication use did not differ between immigrants and Danish-born residents after adjustment for sociodemographic factors and comorbidities.
Conclusion:
Modest disparities in use of standard guideline recommended secondary preventive medications were observed when comparing immigrants and Danish-born residents with ischemic stroke. Furthermore, no differences in persistence of medication therapy were observed.
Introduction
Stroke is considered a leading cause of death and disability worldwide. 1 Stroke incidence, stroke care, and outcomes have been demonstrated to vary across various ethnic groups.2,3 The majority of strokes including recurrent strokes can be prevented through proper assessment and control of risk factors. 4 In Denmark, recent studies have documented a higher incidence of all stroke types and a significantly lower chances of reperfusion therapy among immigrants than among local-born population.5,6 Given that the risk of stroke recurrence within the first-year is common, 7 immigrants’ higher incidence of stroke calls for attention to the poststroke care need for this population. However, evidence on uptake of secondary stroke prevention among immigrants is limited.
Current stroke guidelines recommend several classes of medications such as anticoagulants, antiplatelets, antihypertensives, and statins for both primary and secondary stroke prevention.8–10 These preventive medications have been demonstrated to reduce the risk of stroke recurrence and subsequent mortality.11–15 Despite the clinical benefits, a Danish study has previously reported lower utilization of secondary preventive treatment in immigrants than in Danish-born residents following acute coronary syndrome. 16 One study conducted in the United States found no ethnic differences in preventive treatment adherence poststroke. 17 However, this study used self-reported data and it had included population that was predominantly non-immigrant. Overall, studies investigating use and persistence of the recommended preventive medications in immigrants with stroke using electronic pharmacy claims data are scarce.
Differences in utilization of secondary preventive treatment among ethnic minorities and immigrants may be ascribed to factors related to country of origin and migration like duration of residence and socioeconomic status.18–21 These factors have, however, not been considered in the earlier studies.17,22 Therefore, the present study sought to address this gap by using Danish nationwide registers and examined whether immigrants based on the region of origin compared to Danish-born residents have lower chances of use of secondary preventive treatment after ischemic stroke. Furthermore, we compared treatment persistence between immigrants and Danish-born residents according to use of each preventive medication.
Patients and methods
Data sources and study population
The Danish healthcare system is tax-funded, allowing free access to hospital care, general practitioners, and partial reimbursement of medication costs for all residents including immigrants. All residents are automatically entitled to various reimbursement thresholds for medicines at 0%, 25%, 50%, 75%, and 100% depending on the annual expenditure on reimbursable medicines.23,24 We conducted a nationwide register-based cohort study using data from the Danish Stroke Registry (DSR), Register of Medicinal Products Statistics, National Health Services Register, Danish Register of Causes of Death, and Statistics Denmark. In Denmark, all residents are assigned a unique personal identification number, which enables linkage between the registers. The DSR contributed information on patient demographics, stroke type, lifestyle risk factors, comorbidities, admission date, and discharge date. 25 The Register of Medicinal Products Statistics provided individual-level data on all prescription drugs in Denmark. 26 The National Health Services Register contributed data on contact with a general practitioner that includes email and telephone consultations. 27 We retrieved the date of death from the Danish Register of Causes of Death. 28 Statistics Denmark contributed information on immigration status (country of origin), date of birth, date of immigration, highest attained education, family income, and occupation. We identified all diagnoses in the registers in accordance with World Health Organization’s (WHO) International Classification of Diseases (ICD) system, 10th revision (ICD 10).
We created a cohort of all Danish residents, who were admitted with ischemic stroke (ICD 10, I63) starting from January 1, 2005 to December 31, 2018. We included patients who were ⩾18 years of age and discharged alive during the study period. Excluded were inhospital deaths. The DSR has been reported to have a sensitivity and a positive predictive value of stroke diagnoses of more than 90%. 29 All prescribed medications among ischemic stroke cases were identified based on WHO’s anatomical therapeutic chemical (ATC) codes. Included medications and their average prices per pack are displayed in Supplemental Table 1 and Supplemental Figure 1.
Exposure and outcomes
Immigration status was the exposure of interest and the derived determinants were based on the country of origin or birth in accordance with Statistics Denmark. 30 The study population was categorized as immigrants and Danish-born residents. Furthermore, we classified immigrants as originating from Western and non-Western countries as this group classification has been linked with various challenges in accessing healthcare in Denmark.19,30 Western countries included all 28 European Union countries and Andorra, Iceland, Liechtenstein, Monaco, Norway, San Marino, Switzerland, Vatican State, Australia, New Zealand, Canada, and United States. Non-Western group were all other countries. 30 Because of the large proportion of Turkish, Polish, Pakistani, and Iraqi among the population of immigrants in Denmark, we presented these immigrant subgroups as individual categories. Danish-born residents constituted the reference group.
The primary outcome was use of preventive treatment: anticoagulants, antiplatelets, angiotensin-converting enzyme (ACE) inhibitors/angiotensin II receptor blockers (ARB), beta-blockers, calcium channel blockers, diuretics, and statins. We defined use of secondary preventive treatment as claiming at least one prescription within 180 days after the date of stroke discharge. Use of medications included both new and old users of the assessed medications. The use of diuretics was small and we therefore excluded diuretics from further analyses. Secondary outcome was persistence of preventive treatment, defined as claiming a new prescription within 180 days after the index prescription. Subjects were followed up from the first prescription until an outcome of interest, emigration, death, or study end (December 31, 2018), whichever came first.
Variables
For use and persistence of secondary preventive medications, the following variables were used: country of origin, age, sex, marital status, education, occupation, income, and duration of residence, smoking, stroke severity, hypertension, diabetes, myocardial infarction, atrial fibrillation, history of stroke or transient ischemic attack (TIA), date of discharge, and date of death. Detailed information about categorization of variables in the analysis is provided in the Supplemental Material.
Statistical analyses
We used odds ratios (ORs) and 95% confidence intervals (CI) to investigate association between immigration status (immigrants vs Danish-born residents) and use of secondary preventive treatment adjusting for age at stroke, sex, sociodemographic factors (marital status, income, occupation, education, and duration of residence) and clinical factors (stroke severity, history of stroke or TIA, smoking, myocardial infarction, atrial fibrillation, diabetes, and hypertension) in multivariable logistic regression analysis. First, we assessed use of preventive medications by immigration status: overall immigrants and Danish-born residents. Second, we assessed use of preventive medications by region of origin: Western immigrants, Non-Western immigrants and Danish-born residents. Third, use of preventive medications was assessed by country of origin: Polish, Turkish, Pakistani, Iraqi, Other and Danish-born residents. In all models, Danish-born residents were the reference group. In addition, we performed subgroup analyses in which use of preventive medications was compared between immigrants and Danish-born residents based on (i) education (four groups: immigrants high education level, Danish-born high education level, immigrants low education level vs Danish-born low education level, (ii) income (four groups: immigrants high income, Danish-born high income, immigrants low income vs Danish-born low income, (iii) marital status (four groups: immigrants cohabiting, Danish-born cohabiting, immigrants living alone vs Danish-born living alone), and (iv) stroke severity (four groups: immigrants severe stroke, Danish-born severe stroke, immigrants less severe stroke vs Danish-born less severe stroke). We considered death as a competing event when computing unadjusted curves of absolute risk for treatment persistence. We used Aalen-Johansen estimator to calculate cumulative incidence curves of treatment persistence. Gray’s test was used to test differences in cumulative incidence curves. Furthermore, we employed Fine and Gray (FG) model for competing risk 31 and estimated subhazard ratios (SHRs) and 95% CI for the association between immigration status and treatment persistence adjusting for relevant confounders. The FG model was adjusted for the same set of variables used for estimating odds of use of preventive treatment. The models were assessed for proportionality of hazard assumptions and linearity.
We further evaluated use and persistence of anticoagulants in subgroup of patients with atrial fibrillation by immigration status because of long-term recommendation of anticoagulants for this population. Finally, we assessed whether use and persistence of the secondary preventive medications differed by immigrants’ duration of residence (<10 years and ⩾10 years of residence in Denmark) compared with Danish-born residents. We reported estimates as unadjusted and fully adjusted stratified by immigration status, region of origin, country of origin, and medication class.
All analyses were performed in R statistical software (version 4.0.5 and 4.1.1).
Data availability
Data access may be granted upon approval from the relevant data custodians.
Results
Between January 2005 and December 2018, 110,926 ischemic stroke cases were identified, of which 4702 were inhospital deaths and 106,224 were discharged alive. We included patients who were discharged alive, of whom 4447 were immigrants and 101,777 were Danish-born residents. Among the discharged ischemic stroke cases, 85,667 patients used at least one of the included medications, of which 3589 (80.7%) were immigrants and 82,078 (80.6%) were Danish-born residents (Figure 1). Of those using the treatment, 74,690 (87.2%) claimed the second prescription, 6059 (7.1%) died, and 4918 (5.7%) failed to claim the second prescription within 180 days follow-up. The proportions of immigrants and Danish-born residents who had made contact with a general practitioner after ischemic stroke were relatively similar (85.2% vs 85.1%, p = 0.760). Immigrants were in general younger than Danish-born residents at the time of their stroke diagnosis, were more likely to have a low income, and were more likely to be unemployed and cohabiting (Table 1). Low educational level was most common among Turks. Diabetes and hypertension were most prevalent in Pakistanis (Table 2).
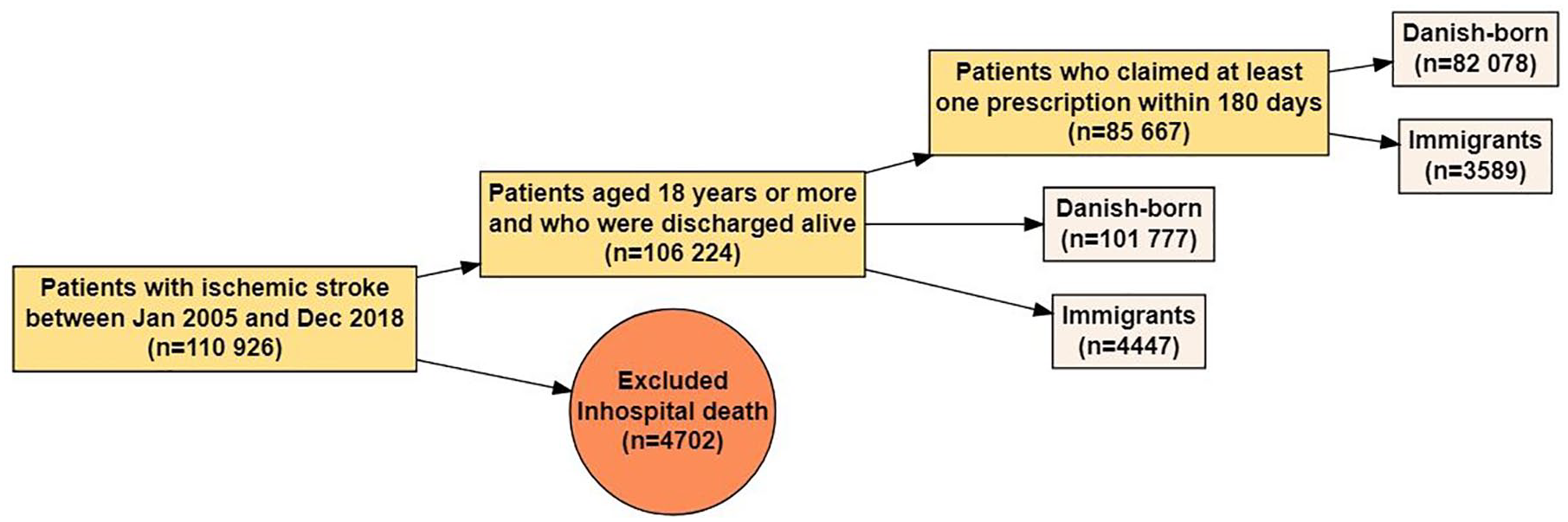
Flowchart.
Characteristics of population discharged with ischemic stroke diagnosis by immigration status.
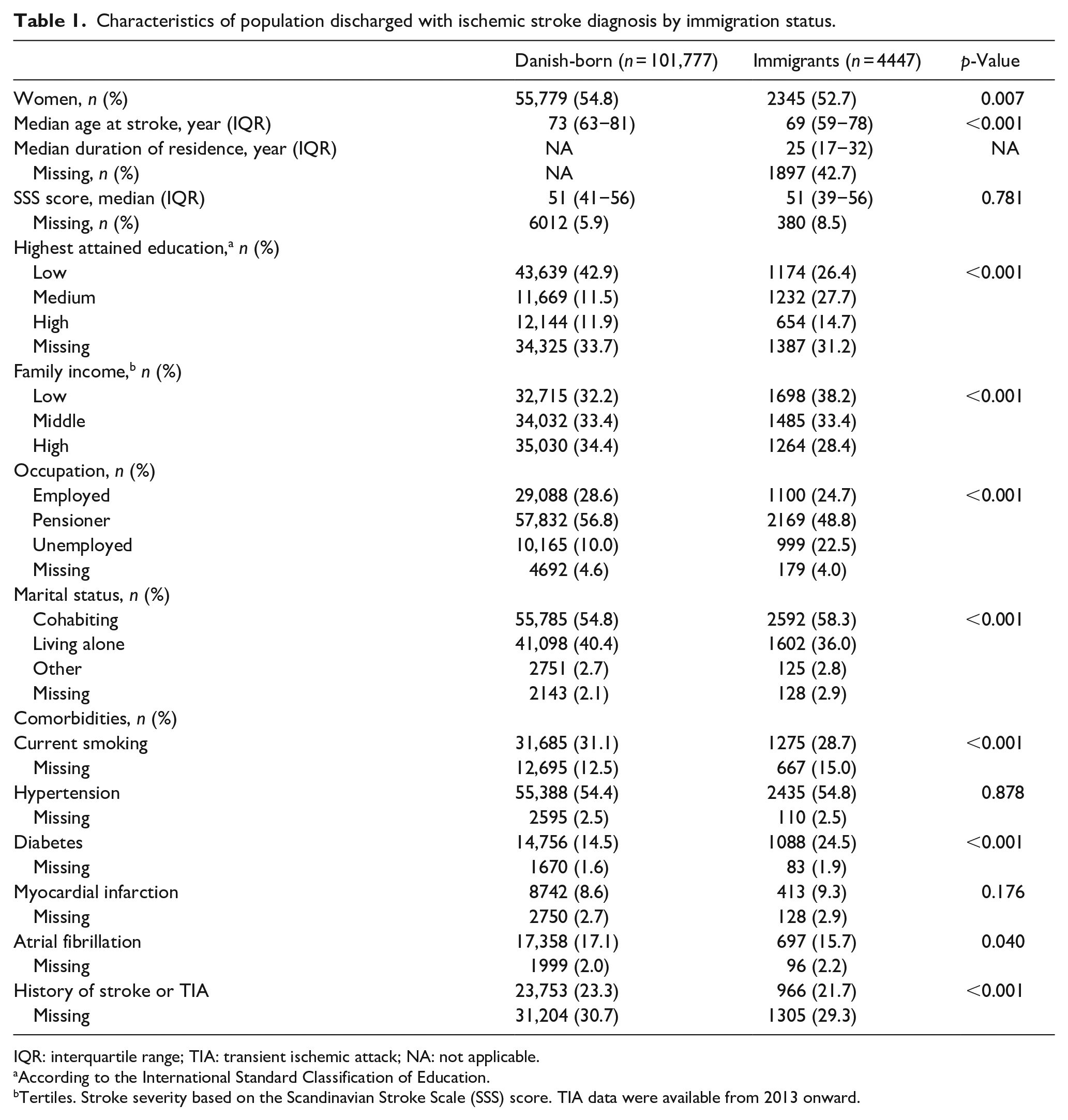
IQR: interquartile range; TIA: transient ischemic attack; NA: not applicable.
According to the International Standard Classification of Education.
Tertiles. Stroke severity based on the Scandinavian Stroke Scale (SSS) score. TIA data were available from 2013 onward.
Characteristics of population of immigrants discharged with ischemic stroke diagnosis by region and country of origin.
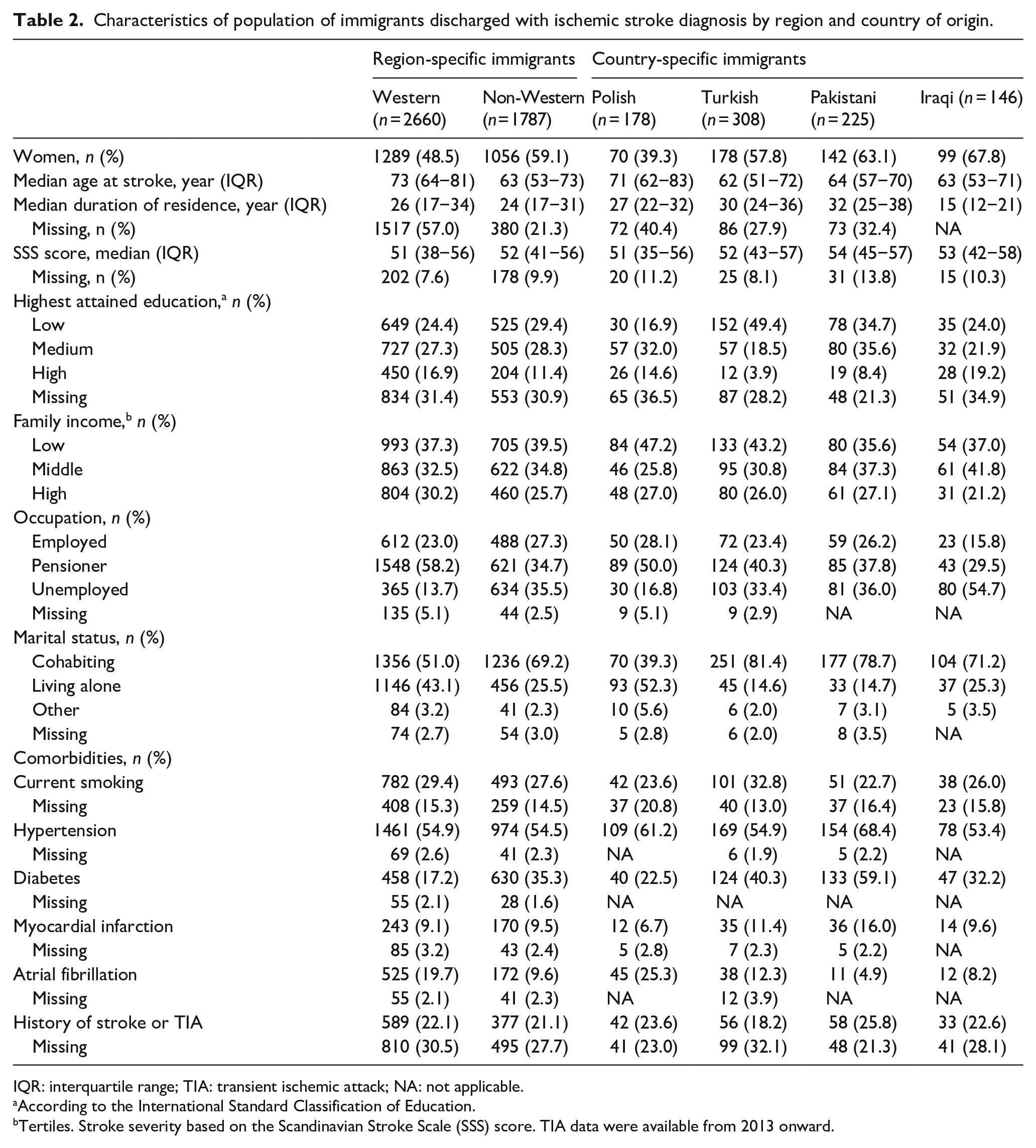
IQR: interquartile range; TIA: transient ischemic attack; NA: not applicable.
According to the International Standard Classification of Education.
Tertiles. Stroke severity based on the Scandinavian Stroke Scale (SSS) score. TIA data were available from 2013 onward.
Use of secondary preventive treatment
Among patients using preventive treatment after stroke discharge, 11.0% were new users and 89.0% were old users (before the index stroke) of at least one of the preventive medications. The majority of patients were using preventive medications within the first 10 days poststroke discharge (49,943 (58.3%) vs 35,724 (41.7%)) (Supplemental Figure 2). The unadjusted ORs of use of each medication class did not differ between immigrants and Danish-born residents, except for anticoagulants (OR, 0.88; 95% CI, 0.82–0.96) (Supplemental Table 2). In the fully adjusted model for age at stroke, sex, sociodemographic factors, duration of residence, stroke severity, and comorbidities, the odds ratio of use of anticoagulants was significantly lower among immigrants than among Danish-born residents (OR, 0.66; 95% CI, 0.53–0.82) (Figure 2). The lower odds of use of anticoagulants were more pronounced in non-Western immigrants (adjusted OR, 0.58; 95% CI, 0.43–0.79) followed by Western immigrants (adjusted OR, 0.72; 95% CI, 0.55–0.95) relative to Danish-born residents. A similar pattern was observed in odds of use of ACE inhibitors/ARB among immigrants than among Danish-born residents (adjusted OR, 0.87; 95% CI, 0.75–0.98). However, non-Western immigrants (adjusted OR, 0.74; 95% CI, 0.61–0.90) only had lower odds of use of ACE inhibitors/ARB than Danish-born residents. In the country-specific estimates, Turks in particular had the lowest odds of use of anticoagulants and ACE inhibitors/ARB.
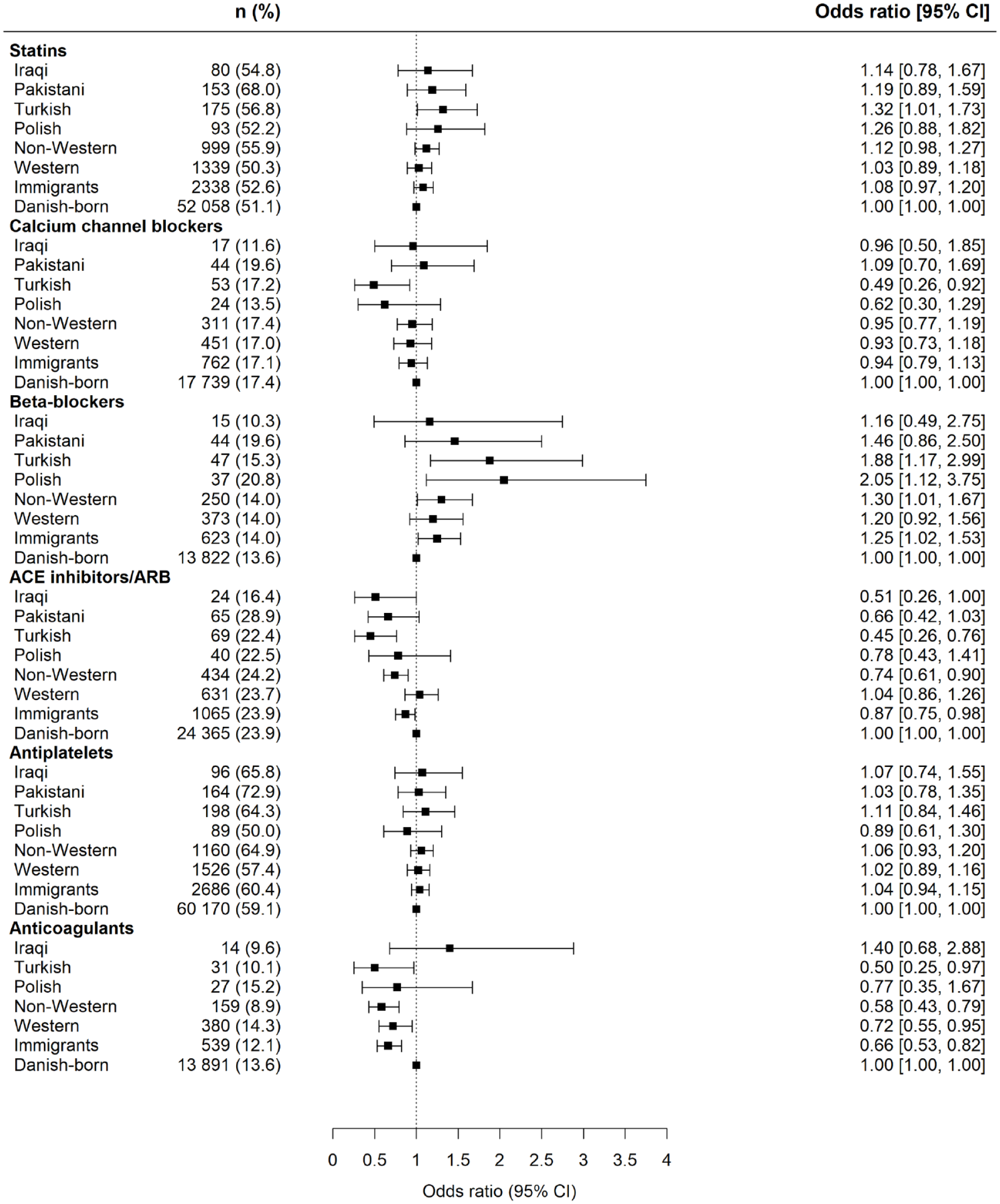
Fully adjusted odds ratios showing use of preventive medications within 180 days after stroke discharge among immigrants compared with Danish-born residents. The fully adjusted model composed age at stroke, sex, income, occupation, education, marital status, duration of residence, stroke severity, history of stroke or transient ischemic attack, smoking, myocardial infarction, atrial fibrillation, diabetes, and hypertension. The first model contained two levels: overall immigrants and Danish-born residents. The second model contained three levels: Western immigrants, Non-Western immigrants and Danish-born residents. The third model contained country of origin: Polish, Turkish, Pakistani, Iraqi, Other and Danish-born residents. CI: confidence interval; ACE: angiotensin-converting enzyme; ARB: angiotensin II receptor blockers.
In contrast, we found immigrants had higher odds of use of beta-blockers than Danish-born residents (adjusted OR, 1.25; 95% CI, 1.02–1.53). The higher odds of use of beta-blockers were evident for non-Western immigrants compared to Danish-born residents. While in the country-specific estimates, we observed highest odds of use of beta-blockers in Polish, followed by Turkish immigrants. The results on use of antiplatelets, calcium channel blockers, and statins did not differ in overall estimates between immigrants and Danish-born residents. However, we found significant lower odds of use of calcium channels blockers and higher odds of use of statins in Turks than in Danish-born residents after adjustment for sociodemographic factors and comorbidities.
Fully adjusted estimates showing factors associated with use of anticoagulants are displayed in Figure 3. We observed that low educational level and less severe stroke (>30 SSS score points) were associated with lower odds of use of anticoagulants in immigrants than in Danish-born residents (Figure 3). However, regardless of income level, immigrants were found to have lower odds of use of anticoagulants than Danish-born residents. In addition, low educational level was associated with significantly lower odds of use of ACE inhibitors/ARB among immigrants than among Danish-born residents. While less severe stroke for immigrants was associated with higher odds of use of beta-blockers than Danish-born residents (Supplemental Table 3).
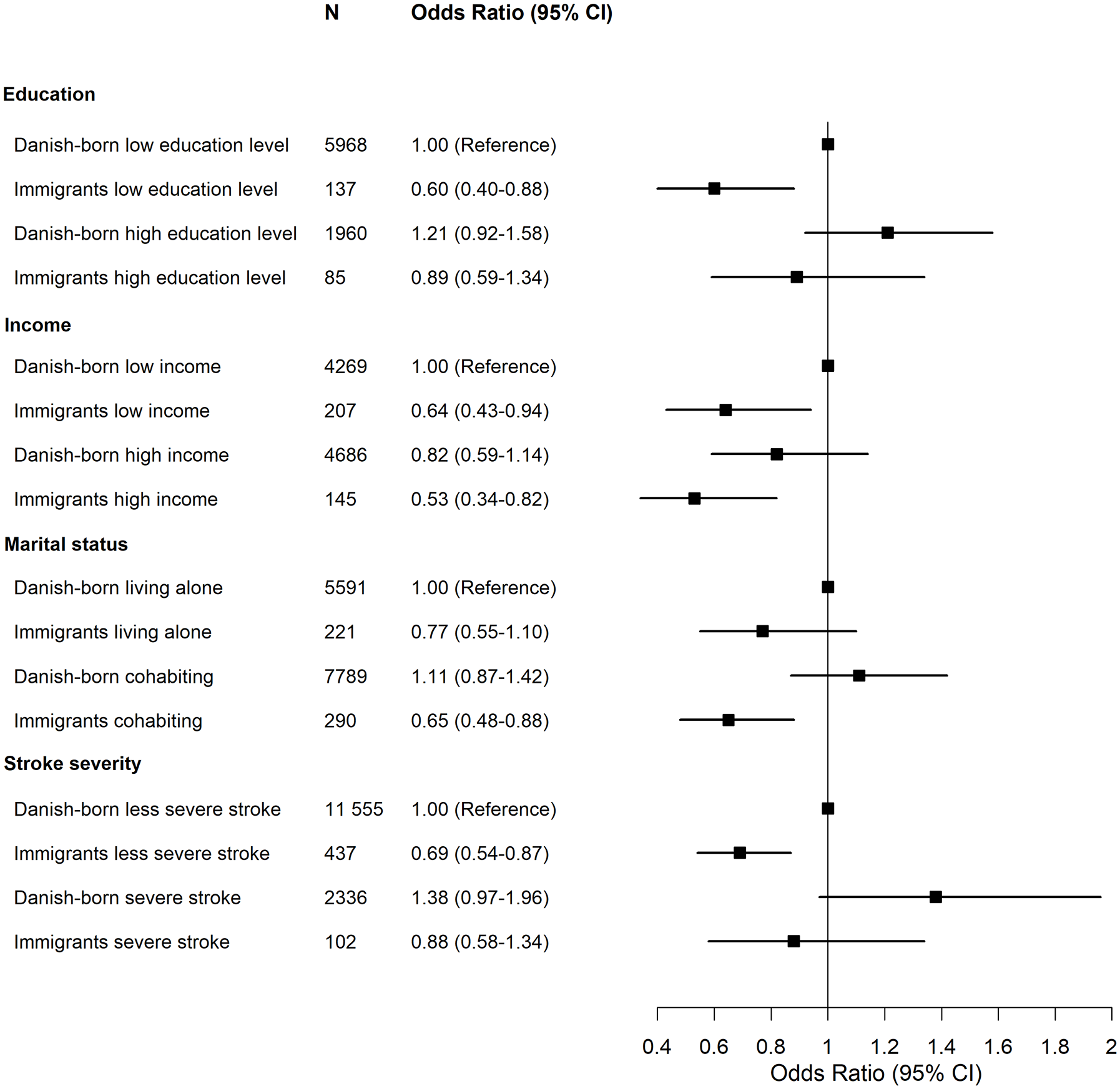
Fully adjusted odds ratios showing factors associated with use of anticoagulants in patients with ischemic stroke. CI: confidence interval. Odds ratios were extracted from the fully adjusted model for the relationship between predictors and use of anticoagulants. Stroke severity measured by the Scandinavian Stroke Scale score and 0–30 points was classified as “severe stroke” and >30 as “less severe stroke.”
Persistence of secondary preventive treatment
Figure 4 shows unadjusted curves of absolute treatment persistence comparing immigrants and Danish-born residents. Unadjusted estimates showed higher persistence of antiplatelets in immigrants than in Danish-born residents (SHR, 1.07; 95% CI, 1.03–1.12), whereas no differences were found in other preventive medications. After adjustment for age at stroke, sex, sociodemographic factors, duration of residence, stroke severity, and comorbidities, we found no difference in persistence of all included preventive medications between immigrants and Danish-born residents (SHR, 1.21; 95% CI, 0.97–1.51 for anticoagulants, SHR, 1.01; 95% CI, 0.86–1.20 for ACE inhibitors/ARB; Supplemental Table 4).
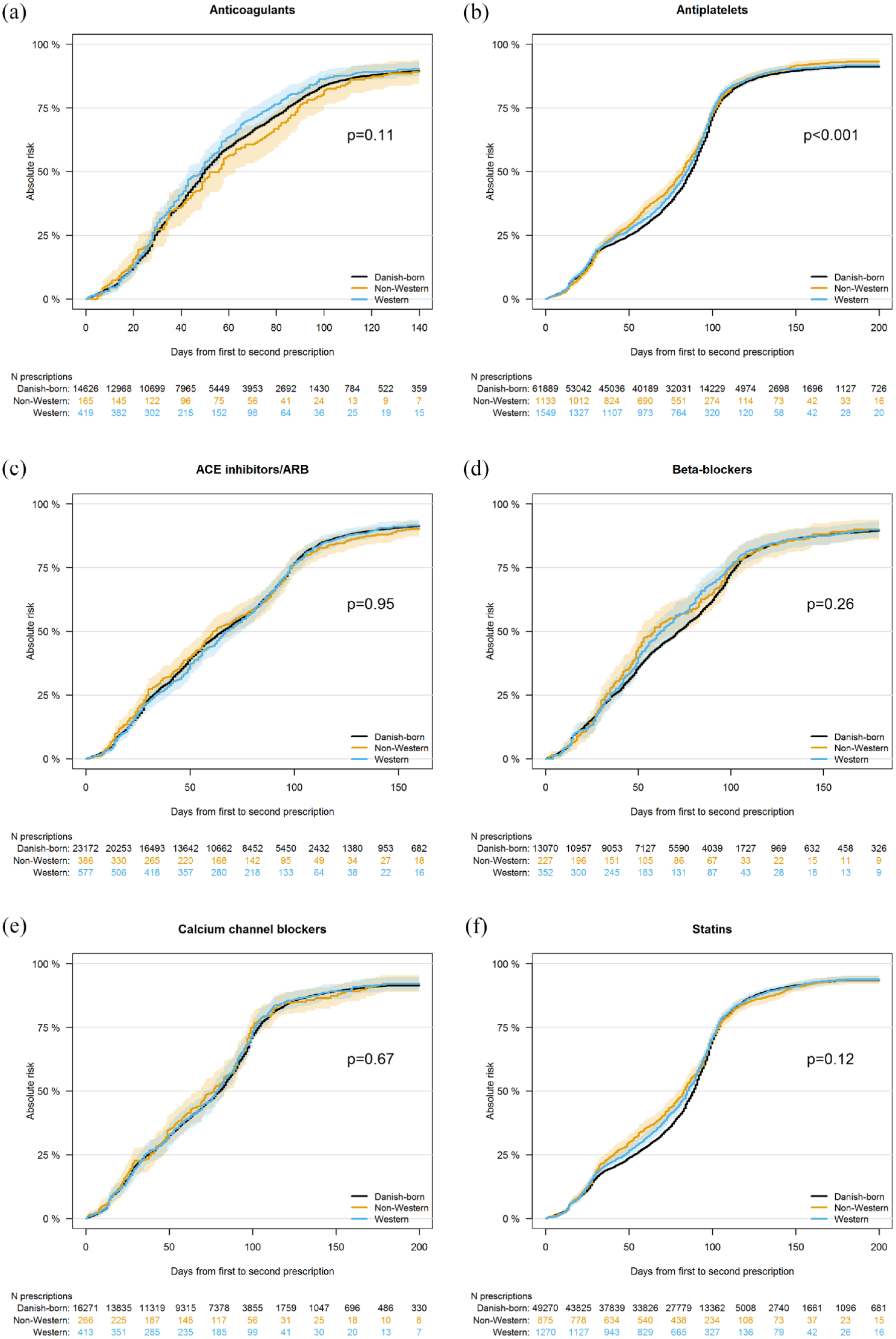
Unadjusted curves of absolute treatment persistence comparing immigrants with Danish-born residents. p value based on Gray’s test. Colored spectrums indicate confidence intervals. ACE: angiotensin-converting enzyme; ARB: angiotensin II receptor blockers.
Further analysis showed no significant difference in use or persistence of anticoagulants between immigrants and Danish-born residents in patients with ischemic stroke and atrial fibrillation in both unadjusted and adjusted models (Supplemental Table 5). In general, we found no differences in use or persistence of secondary preventive medications according to duration of residency of immigrants in Denmark (<10 years and ⩾10 years of residence vs Danish-born residents) after adjustment for covariates (Supplemental Table 6).
Discussion
This nationwide cohort study demonstrated no disparities in the rates of use of various guideline recommended secondary preventive medications between immigrants and Danish-born residents, except for anticoagulants. However, after adjustment for clinical and sociodemographic factors, immigrants had significantly lower chances of use of anticoagulants and ACE inhibitors/ARB than Danish-born residents following ischemic stroke. In contrast, we observed higher chances of use of beta-blockers in immigrants than in Danish-born residents poststroke. Regarding treatment persistence, our study found a significant higher persistence of antiplatelets among immigrants than in Danish-born residents, but this difference disappeared after adjustment for relevant confounders. Furthermore, no differences in persistence of other preventive medications (anticoagulants, ACE inhibitors/ARB, beta-blockers, calcium channel blockers, and statins) were observed when comparing immigrants and Danish-born residents in both unadjusted and adjusted models. Similarly, no evidence was found that use or persistence of anticoagulants differed between immigrants and Danish-born residents in patients with ischemic stroke and atrial fibrillation before and after adjustment for confounders.
The present study adds knowledge on use and persistence of secondary preventive treatment among immigrants with stroke. Our findings on use of secondary preventive treatment clearly corroborate the previous study conducted in Denmark, which found lower use of ACE inhibitors in immigrants than in Danish-born residents after acute coronary syndrome. 16 However, this Danish study observed a higher discontinuation of ACE inhibitors among immigrants than among Danish-born residents, which was not in agreement with our findings. Two studies conducted in the United States investigating medication adherence across various ethnic groups after stroke reported conflicting results.17,22 For example, the first study by Lank et al. reported no ethnic difference in adherence of five medication classes poststroke, which is consistent with our results. This study used self-reported data, which may have introduced recall bias in comparison to our electronic pharmacy claims data. The second study by Albright et al. found that black ethnicity more likely than white was associated with statins nonadherence following hospitalization for ischemic stroke. Overall, the population included in these studies was mainly non-immigrant, and there is significant variability in measurement of treatment adherence and persistence, thus challenging the comparison.
The lower use of some secondary preventive medications in immigrants in Denmark may be explained by differences in socioeconomic status, or health-seeking behaviors, or acculturation factors such as language barriers. Consistent with previous research, 18 we identified low educational level was associated with lower chances of use of anticoagulants and ACE inhibitors/ARB among immigrants than among Danish-born residents of the similar education level. Turks in particular had large proportion of patients with low educational level, which may contribute to explaining why they had the lowest chances of use of anticoagulants, ACE inhibitors/ARB, and calcium channel blockers. Patient education level may indicate one’s cognitive ability to obtain, process, and understand health information and hence sustain treatment after stroke discharge. This study identified less severe stroke as another important factor associated with lower chances of use of anticoagulants among immigrants. This finding may reflect that immigrants consider a minor stroke as less serious and thus lack motivation for use of this preventive treatment. Low educational level, less severe stroke, and low income may be acting together resulting in underutilization of anticoagulants among immigrants. Additionally, our results showed higher chances of use of beta-blockers among immigrants than among Danish-born residents, notably for immigrants with less severe stroke. It is unclear how less severe stroke was associated with higher utilization of beta-blockers among immigrants, despite this finding not being explained by differences in income and educational level. We speculate that this might be due to indications prior to stroke admission as the majority of patients were using these preventive medications before the stroke onset. We did not observe a large difference in the prices of antihypertensive medications (beta-blockers vs ACE inhibitors vs calcium channel blockers) as illustrated in the Supplemental Material. Like Danish citizens, immigrants in Denmark are automatically entitled to free access to a general practitioner and to various reimbursement thresholds for medicines depending on the annual expenditure on reimbursable medicines. For example, a patient gets 50% reimbursement if the annual expenditure on medicines is between 1020 DKK (~137 EUR) and 1705 DKK (~229 EUR). Furthermore, a full reimbursement for medicines (100%) can be offered to a patient if his/her annual expenditure on medicines is above 20,091 DKK (~2700 EUR) with a copayment of 4320 DKK (~580 EUR). 23 Therefore, it is less likely that the differences detected in utilization of some secondary preventive medications are due to the reimbursement strategy used. While insurance status is associated with higher chances of receiving outpatient medical care in countries like the United States. 32 Although a broad range of clinical and sociodemographic factors were considered, other unmeasured covariates such as language barriers, stroke education, cultural norms, and behavioral factors may also explain some ethnic differences seen in medication use in the Danish setting. 19
Our findings have some clinical implications. The lower chances detected in use of anticoagulants and ACE inhibitors/ARB may have an impact in the risk of stroke recurrence, readmissions, and long-term outcomes among immigrants as previously reported in minorities compared with the majority population. 33 The lack of association between immigration status and persistence of the secondary preventive medications is an encouraging finding in the fight for reducing disparities in care poststroke. In addition, the association between immigration status and anticoagulants use and persistence was nonsignificant in patients with ischemic stroke and atrial fibrillation. This finding is appealing as it demonstrates effort by the Danish healthcare system in providing equal access to outpatient medical care regardless of immigration status. After stroke discharge, patients are usually referred back to their own general practitioner for outpatient medical care. Hence, better patient education including emphasis on the importance of secondary preventive treatment involving patient’s general practitioner and family members could be a feasible way of reducing disparities in medical care poststroke. We believe that providing patient education is essential considering that the follow-up care available in Denmark for most patients will not include in-depth follow-up with a stroke specialist.
A major strength of our study was the use of electronic pharmacy claims data for estimating use and persistence of secondary preventive treatment by immigration status, which is a more reliable method than using self-reported data. Data on dispensed medications were available during the entire study period between 2005 and 2018. We were able to investigate the association between immigration status and medications use and persistence taking into account a wide range of clinical and sociodemographic factors. Our study has several limitations. We acknowledge that our country-specific estimates might be chance occurrences due to small sample size. Therefore, the results for immigrant subgroups should be interpreted with caution. We could not ascertain if lack of use or persistence was due to a lack of prescribing by the treating physician or to lack of filling the prescription at the pharmacy by the patient. Furthermore, it was not possible to assess whether patients actually used the medications following dispensation at the pharmacy. Our registers lack data on inhospital prescriptions, which can determine the duration of the prescribed medications by clinicians. Lastly, acetyl salicylic acid (ASA) can be bought over the counter without prescription; this may have led to underestimation of patients using this medication.
Conclusion
This cohort study from 2005 to 2018 observed some differences between immigrants and Danish-born residents with respect to use of secondary preventive medications but found no difference in medication persistence after ischemic stroke.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221111870 – Supplemental material for Immigration status and utilization of secondary preventive treatment after ischemic stroke
Supplemental material, sj-docx-1-eso-10.1177_23969873221111870 for Immigration status and utilization of secondary preventive treatment after ischemic stroke by George F Mkoma, Søren P Johnsen, Helle K Iversen, Grethe Andersen and Marie Norredam in European Stroke Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The TrygFonden supported this work (ID: 126642). The funders had no role in the study design, data analysis, or writing of the manuscript.
Ethical approval
This study was approved by the Danish Data Protection Agency, reference number 514-0457/20-3000.
Guarantor
SPJ
Contributorship
GFM, SPJ, HKI, GA, and MN designed the study and analytical strategy. GFM performed the literature review and analyzed cohort data. GFM, SPJ, HKI, GA and MN contributed to the interpretation of results. GFM wrote the first draft of the report. All authors commented on the report draft and approved the final text.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.