
Abstract
Background:
Monitoring and measuring different aspects of stroke care pathway is the cornerstone for improvement of quality. We aim to analyze and give an overview of improvements of stroke care quality in Estonia.
Patients and methods:
National stroke care quality indicators are collected and reported using reimbursement data and include all adult stroke cases. In Estonia, five stroke-ready hospitals are participating in Registry of Stroke Care Quality (RES-Q), providing data on all stroke patients 1 month every year. Data from the national quality indicators and RES-Q from 2015 to 2021 are presented.
Results:
The proportion of intravenous thrombolysis for all Estonian hospitalized ischemic stroke cases increased from 16% (95% Confidence Interval, CI 15%–18%) in 2015 to 28% (95% CI 27%–30%) in 2021. Mechanical thrombectomy was provided to 9% (95% CI 8%–10%) in 2021. The 30-day mortality rate has decreased from 21% (95% CI 20%–23%) to 19% (95% CI 18%–20%). More than 90% of patients with cardioembolic stroke are prescribed anticoagulants at discharge, but only 50% are on anticoagulant treatment 1 year after stroke. Also, the availability of inpatient rehabilitation needs improvement, being 21% (95% CI 20%–23%) in 2021. A total of 848 patients are included in the RES-Q. The proportion of patients receiving recanalization therapies was comparable to the national stroke care quality indicators. All stroke-ready hospitals show good onset-to-door times.
Conclusion:
The overall stroke care quality in Estonia is good, especially the availability of recanalization treatments. However, secondary prevention and the availability of rehabilitation services need improvement in the future.
Introduction
Globally, stroke is the second-leading cause of death and the third-leading cause of death and disability combined worldwide. 1 Appropriate management is crucial for reducing the burden of stroke. Several guidelines, both national and international have been prepared to guide clinicians in stroke care but the implementation of the results into clinical practice has proven to be challenging. 2 A recent survey based on expert opinion demonstrated that there are major inequalities in acute stroke treatment between and within 44 European countries in Europe. In many Eastern European countries, the access to and delivery of acute stroke care was more often insufficient or lacking. 3 The importance of voluntary registries on increased provision of evidence-based care has been reported earlier.4,5 In 2015, the European Stroke Organisation (ESO) initiated the ESO Enhancing and Accelerating Stroke Treatment (EAST) project aiming at improvement of stroke care quality, primarily in Eastern Europe. 2
Estonia is a tiny country at the Baltic Sea, near the Finnish and Russian border. The population of Estonia is 1,330,068. 6 After restoring its independence in 1991, the economy has dramatically improved and by the World Bank, Estonia is currently among high-income countries. 7 The life expectancy for men was 74 and for women 83 years in 2020. As most of the European countries, the share of persons at pension age has also increased over time. In 2021, 20% of the population were 65 years old and older. 6
The Estonian health care system is based on the solidarity principle of health insurance. All insured people have access to medical care which is covered by the Estonian Health Insurance Fund (EHIF). 8 However, the ambulance services and emergency assistance services in Estonia are provided free of charge to all persons, including persons without medical insurance. The management and supervision of health care system and development of health policy is under the scope of the Ministry of Social Affairs (MSA) and its agencies.
According to the EHIF reimbursement database, there are around 3500–3600 strokes annually. It is estimated that more than 90% of stroke patients are treated in hospitals. There are 18 acute care hospitals in Estonia. Intravenous thrombolysis (IVT) is provided in six stroke-ready hospitals and three of them are 24/7 ready for mechanical thrombectomy (MT).
The first patient with ischemic stroke was treated with IVT in 2003 in Tartu University Hospital which is the only academic hospital in Estonia. 9 During the following few years only single patients were given IVT, even in largest hospitals of Estonia. The possible reasons were short therapeutic window of 3 h, low awareness of stroke as medical emergency among medical personnel, and insufficient knowledge of stroke symptoms and action at onset of stroke among general population.
The Estonian Stroke Initiative (ESI) was founded as a subsociety under the Estonian L. Puusepp Society of Neurologists and Neurosurgeons (ENNS) in 2008. Increasing of stroke knowledge was set on the top of the priorities of activities of the ESI. An observational study over a 5 months period was designed to assess stroke awareness of the Estonian population in 2008–2009. With an original closed-ended questionnaire 355 randomly selected subjects were interviewed in public places in two largest cities. The overall knowledge about the stroke causes, risk factors, symptoms and behavior at the onset of stroke was better compared to many other studies but stressed the need for future awareness campaigns for younger subjects with lower education. 10 Starting from 2008, stroke awareness campaigns for general population were organized in three larger cities of Estonia on World Stroke Day in October, together with numerous media broadcasts, lectures in schools and workplaces all over the year. In parallel, educational events and lectures on modern management of stroke introducing the “time is brain” principles and stressing the importance of shortening the onset-to-door time (ODT) and door-to-needle time (DNT) were held by the members of the ESI to emergency medical services and hospitals.
The importance of quality of stroke care was also recognized by the EHIF and MSA in early 2000s. Three clinical audits were initiated by the EHIF and led by the ENNS in 2003, 2010, and 2013 with the aim to analyze acute care of stroke in 18 Estonian hospitals. The audits concluded that stroke management was better in large hospitals compared to small general hospitals. It was recommended that all stroke patients should be treated in stroke units and stroke units should be organized in all large hospitals. 11 Although the auditors stressed the need for defining stroke pathways, stroke-ready hospitals and the need for organizing stroke units, no specific changes were implemented into clinical practice.
However, after the publication of the results of the audits the ESI started actively collaborating with the EHIF and MSA of Estonia about the results of the audit and urgent need for reorganizations of stroke service and implementation of modern treatments into clinical practice. After years of negotiations with the stakeholders, it was finally agreed between the MSA, EHIF, Union of Estonian Medical Emergency and all acute care hospitals that (1) all patients from 1st of September 2019 with acute onset of stroke should be admitted straight to stroke-ready hospitals containing stroke units or stroke centers; (2) all stroke patients should be managed in stroke units or stroke centers; (3) access to post-stroke rehabilitation should be increased.
Estonia joined the Safe Implementation of Treatments in Stroke (SITS) International Stroke Treatment Registry (SITS-ISTR) in 2007 and since then several stroke-ready hospitals of Estonia have been using this platform for monitoring the trends and time logistics of IVT and MT. 12 However, as during the years the platform has been changed to more sophisticated one with several data not directly related to monitoring of stroke quality care, the interest has been lowered and currently three hospitals are participating.
Being aware of the importance of monitoring of the quality of care as a part of a process of quality improvement, a national health care quality indicators program was launched in Estonia in 2015. 13 This comprehensive project was initiated by the EHIF in collaboration with the Medical Faculty of the University of Tartu with the aim to improve the quality of health care in Estonia by selecting appropriate quality indicators which best assess the management of diseases causing the highest burden. Stroke care quality indicators were chosen among other indicators to be monitored and are annually reported.
Almost in parallel with the national program, the ESO-EAST project was initiated to improve stroke care at both hospital and national levels. 2 Estonia joined it from the very beginning in 2015. A national steering committee containing the representatives of all stroke-ready hospitals and members of the ESI was established. The Registry of Stroke Care Quality (RES-Q) platform was introduced to stroke-ready hospitals, and they were asked to join the initiative. 14
Herewith, the trends of stroke care in Estonia based on national quality indicators of stroke care and RES-Q indicators are presented.
Patients and methods
National indicators of quality of stroke care
In 2015, nine indicators of quality of care for stroke were chosen by the ESI. The prerequisite was that data should have been easily obtained from the EHIF reimbursement database. Some of the indicators were adopted from the Danish National Indicator Project but some of them were developed by the ESI originally. 15 These indicators are calculated every year including all stroke cases in Estonia.
The five quality indicators evaluated every year are:
Proportion of patients managed in central or regional hospitals (24/7 stroke-ready hospitals with acute stroke units and centers). Performance indicator (PI), goal 90%.
Proportion of patients receiving recanalization therapies (IVT, MT, or combined). PI, goal 30%.
Proportion of patients having received inpatients rehabilitation services within 30 days after admission with acute stroke. PI, goal 40%.
Proportion of patients with ischemic stroke and atrial fibrillation having a prescription for oral anticoagulants 12 months after hospitalization from the index stroke. PI, goal 75%.
Mortality of at 30 days after admission with acute stroke. Outcome indicator, goal <15%.
The annual reports are presented to the hospitals and are available to the public. 13
However, four of the proposed indicators are time dependant and currently not obtainable from the EHIF reimbursement database. The indicators never collected are: (1) Proportion of stroke patients in whom computer tomography (CT) or magnetic resonance imaging (MRI) is performed within an hour after admission to the hospital; (2) Proportion of stroke patients in whom imaging of carotid arteries is performed within 96 h of admission to the hospital; (3) Proportion of stroke patients in whom swallowing is tested within 24 h of admission to the hospital; and (4) Proportion of stroke patients evaluated by a physiotherapist within 48 h of admission to the hospital.
Hospitalized cases of acute stroke (ischemic stroke and intracerebral hemorrhage, International Classification of Diseases (ICD)-10 I63 and I61, respectively) including patients ⩾19 years of age are identified and analyzed. The EHIF reimbursement database is linked with the Estonian Prescription Registry and Death Registry for calculation of the results. If the patient is hospitalized repeatedly with the diagnosis of stroke during the same year, an acute stroke case is defined when occurring later than 30 days after the first admission. The oral anticoagulants (OAC) are warfarin, dabigatran, rivaroxaban, edoxaban, and apixaban and only cases of patients surviving the first 14 days after admission are analyzed. The patient must have an active prescription for an OAC 12 months + 1 day after cardioembolic stroke (ICD-10 codes I63 and I48).
RES-Q database
As the national quality indicators are reflecting only a small part of stroke care, the RES-Q database was included as a comprehensive tool for stroke care quality monitoring enabling measurement and analysis between hospitals, both nationally and internationally. Details of data composition, collection procedure, and the full collection form are reported elsewhere.2,14
The national steering committee has agreed to collect the data once a year in March since 2017. Five of six stroke-ready hospitals (Tartu University Hospital, North Estonia Medical Centre, West-Tallinn Central Hospital, East-Tallinn Central Hospital, and Pärnu Hospital) are actively participating with entering the data of all consecutive stroke patients discharged during 1 month period a year into the RES-Q electronic database.
The data acquired from the clinical RES-Q database and the EHIF are anonymous therefore the Ethics Committee license is not required.
Statistical analyses
Patient characteristics were described by relative frequencies for categorical data and means, standard deviations (SD), medians and interquartile ranges (IQR) for continuous data. Chi-squared test for trend was used to analyze changes of proportions over time. Time trend for DNT and DGT was tested with linear regression model. All statistical tests were conducted at a significance level of 0.05. The data analysis was performed by Microsoft® Excel® for Microsoft 365 MSO (Version 2202 Build 16.0.14931.20128) and statistical software R 1.4.1 (The R Foundation for Statistical Computing).
Data availability statement
All data generated or analyzed during this study are available from the corresponding author upon reasonable request.
Results
According to the EHIF reimbursement database, the number of hospitalized stroke cases (ischemic stroke and intracerebral hemorrhage) decreased between 2015 and 2021 from 3699 to 3351 (from 282 to 252 per 100,000 person-years, respectively) and the proportion of patients managed in stroke units/centers increased from 77% (95% Confidence Interval, CI 75%–78%) to 87% (95% CI 85%–88%). The 30 days’ case-fatality decreased from 21% (95% CI 20%–23%) to 19% (95% CI 18%–20%). The proportion of IVT for all Estonian hospitalized ischemic stroke cases increased from 16% (95% CI 15%–18%) in 2015 to 28% ( 95% CI 27%–30%) in 2021. Since 2017 MT was included into the analysis of stroke quality indicators. The proportion of patients receiving all recanalization therapies increased between 2017 and 2021 from 22% (95% CI 20%–23%) to 33% (95% CI 31%–35%) and MT alone or with combined IVT bridging from 3% (95% CI 3%–4%) to 9% (95% CI 8%–10%). The availability of inpatients’ rehabilitation within 30 days after admission increased between 2016 and 2019 from 17% (95% CI 16%–18%) to 23% (95% CI 22%–25%) but decreased to 18% (95% CI 16%–19%) in 2020 and increased again to 21% (95% CI 20%–23%) in 2021. The time trend analysis showed significant improvement for all these indicators (Figure 1). At 1 year after admission for cardioembolic stroke 52% (95% CI 49.0%–55.0%) and 53% (95% CI 50%–56%) of patients respectively discharged in 2015 and 2020 and surviving the first 14 days had prescription for OAC. No change was observed during the period (Figure 1).
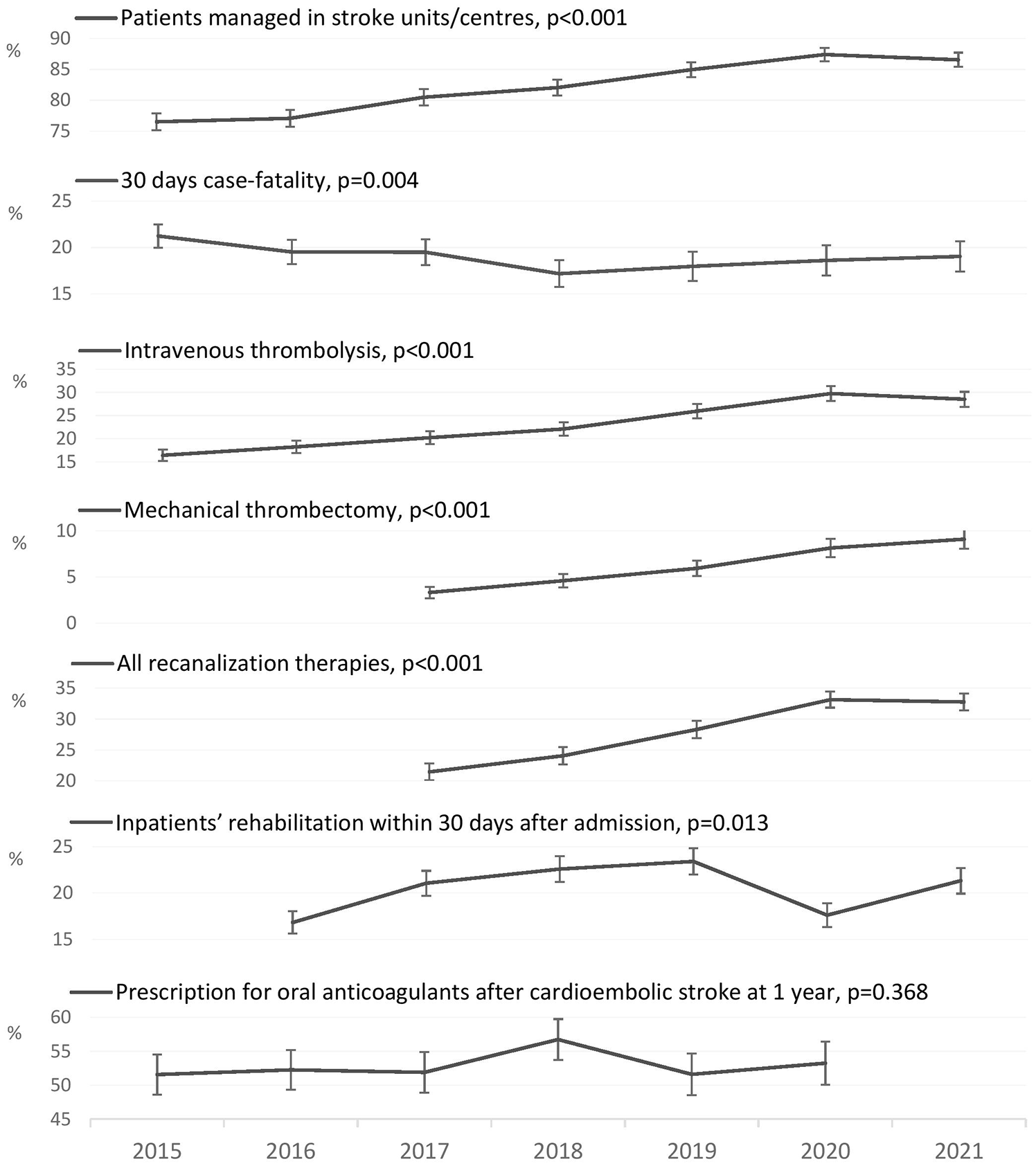
Time trends of stroke quality indicators according to the Estonian Health Insurance Fund reimbursement database.
According to the RES-Q database, 848 patients were discharged between 2017 and 2021 from five stroke-ready hospitals. The mean age was 73 (SD ± 13) years and 45% of them were men. The proportion of patients receiving recanalization therapies was comparable to the national stroke quality indicators and increased for combined bridging IVT and MT therapy (Figure 2). The time logistics for recanalization therapies is shown on Figure 3. The DNT has not changed over the years. The door-to-groin time (DGT) has somewhat improved over the study period from median of 100 min (IQR: 100–111) in 2017 to 64 (IQR: 57–84) min in 2021 but not statistically significant.
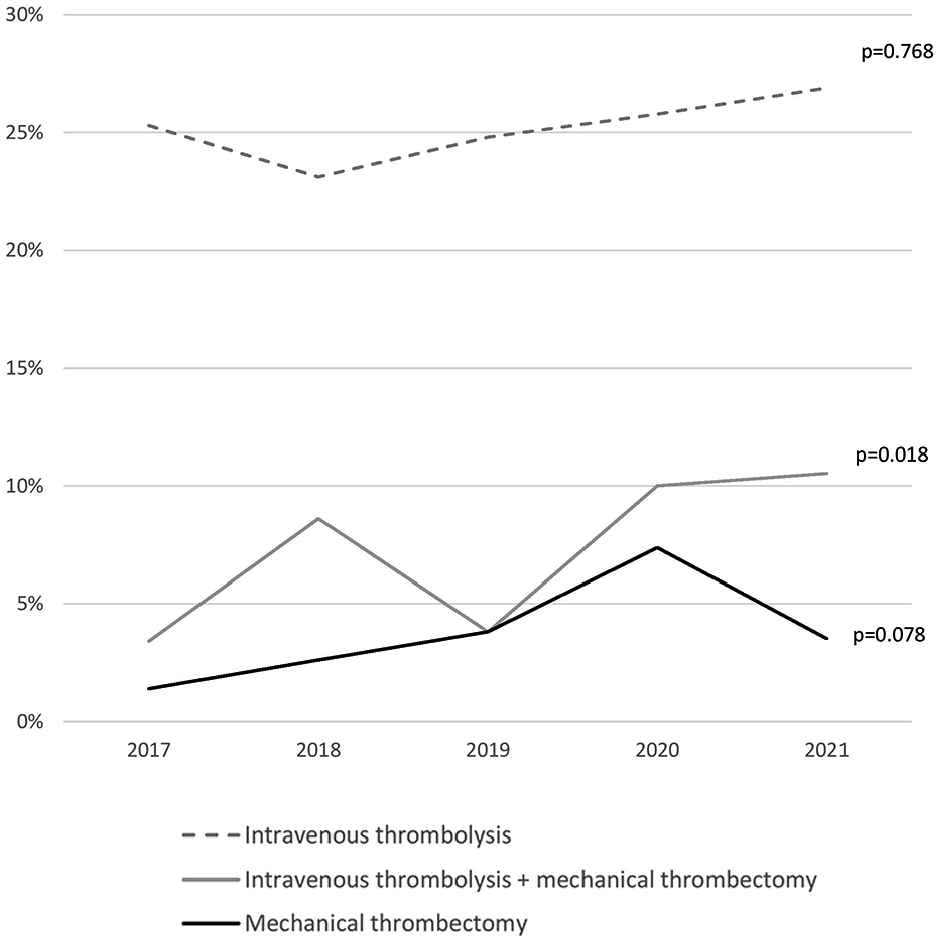
Proportion of patients with ischemic stroke receiving recanalization therapies in stroke-ready hospitals in Estonia from 2017 to 2021 according to the Registry of Stroke Care Quality data.
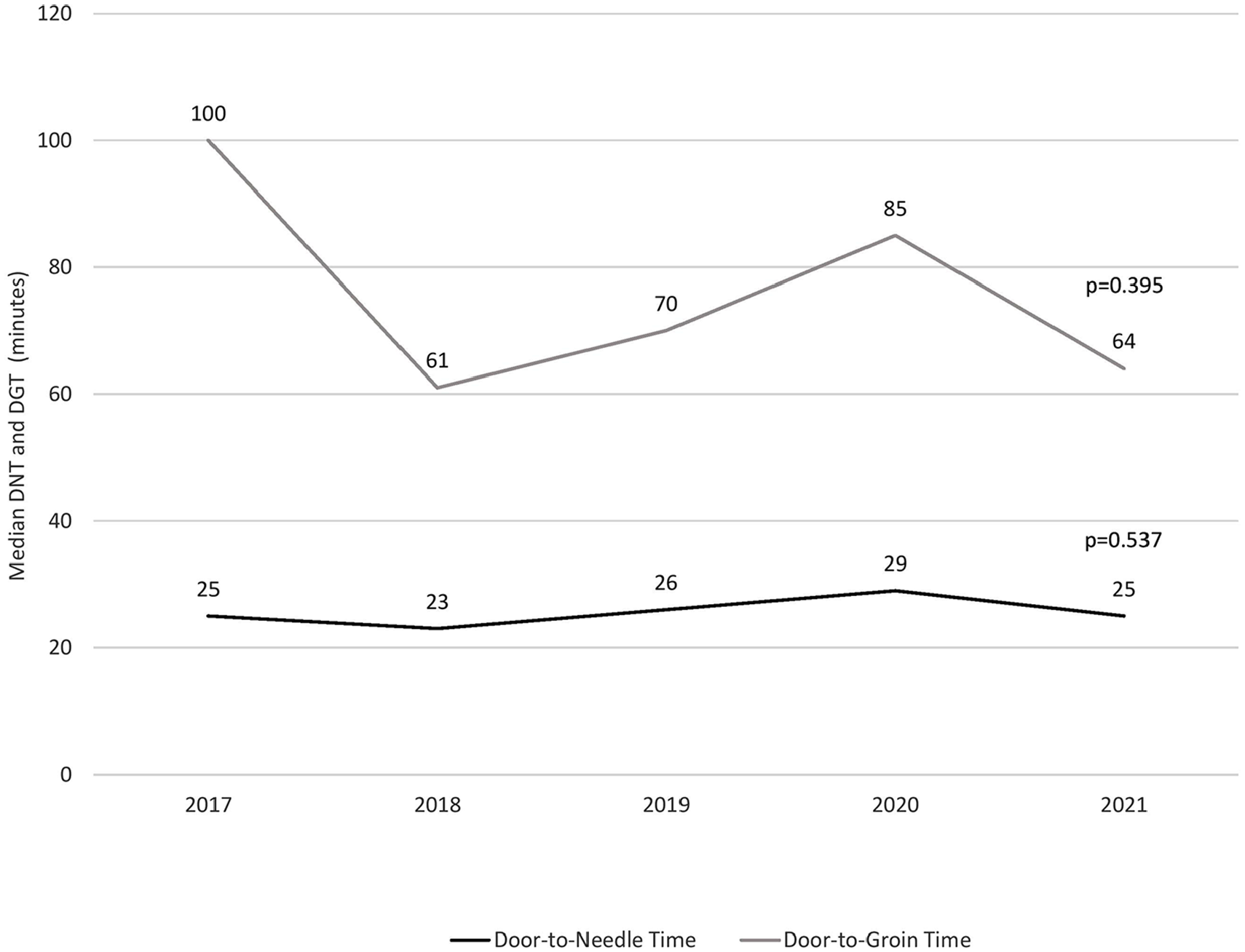
Median door-to-needle (DNT) and door-to-groin (DGT) times (in min) in stroke-ready hospitals in Estonia from 2017 to 2021 according to the Registry of Stroke Care Quality data.
The trend of indicators according to the ANGELS Initiative quality improvement program awards are shown on Figure 4. 16
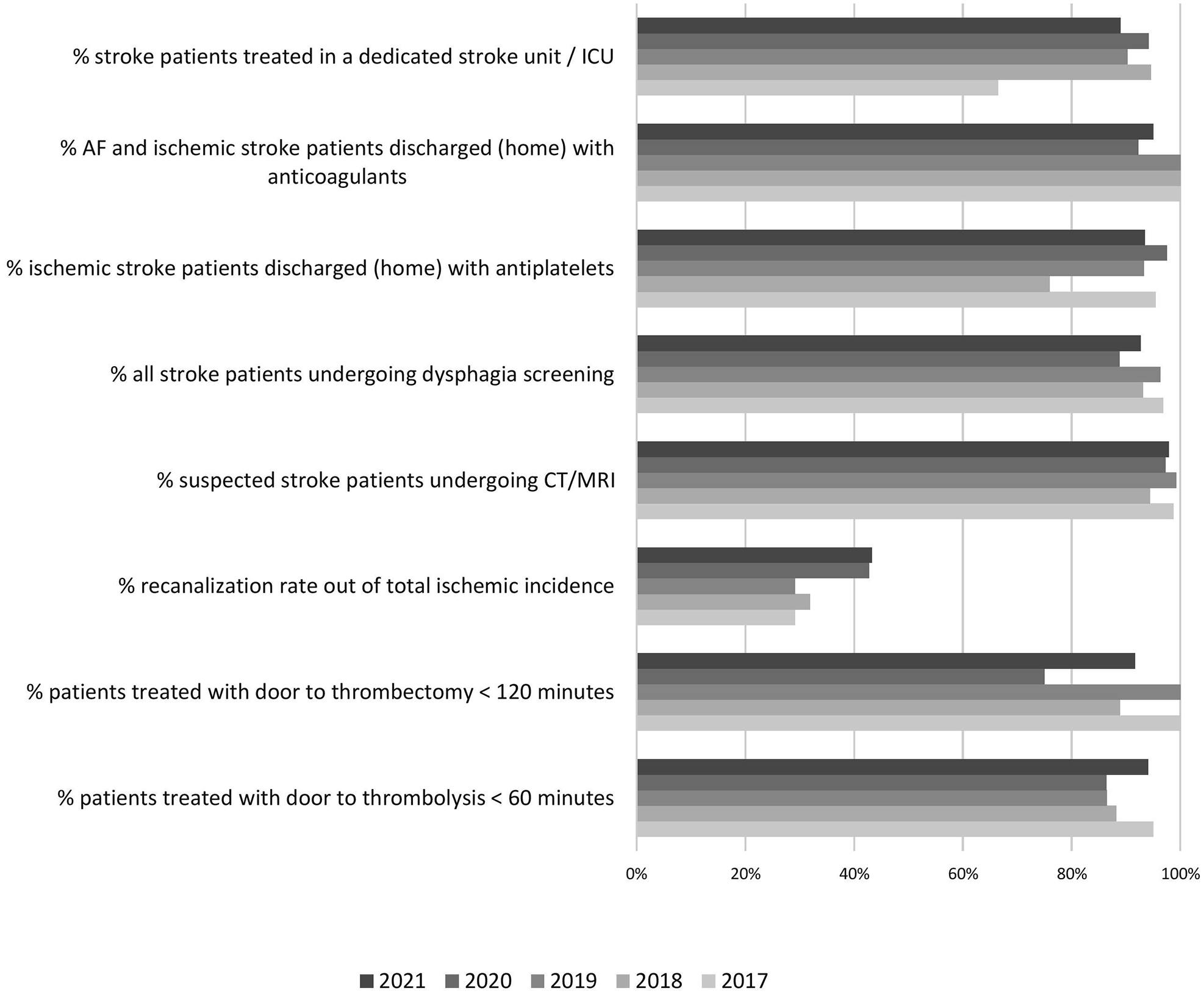
The trend of indicators according to the ANGELS Initiative quality improvement program in Estonia from 2017 to 2021 according to the Registry of Stroke Care Quality data (AF: atrial fibrillation; ICU: intensive care unit; CT: computer tomography; MRI: magnetic resonance imaging).
Discussion
Our results show that long-lasting efforts in stroke care quality improvement on a national level have led to equally good level of stroke care in stroke-ready hospitals in Estonia. Despite this, further contribution and collaboration of all stakeholders to continuous monitoring and measuring quality of care aiming at reduction of the implementation gap between evidence-based standards of care and current clinical practice cannot be overestimated. It is vital that all parties, hospitals, governmental authorities, and nongovernmental organizations participate actively in this process.
Acute stroke care
During the last 15 years the availability of revascularization therapies for ischemic stroke has increased and according to the current analysis as much as 33% from all hospitalized ischemic strokes in Estonia receiving the treatment. This is confirmed also by a recent survey from European countries were the rate of IVT per million population in Estonia was the highest in Europe. 3
The aim is to treat at least 90% of patients in stroke units/centers. According to the quality indicators of stroke care and data from RES-Q, this target is quite close. It has been achieved by the help of governmental-level decision in 2019 which demands that all stroke patients are transported straight to stroke-ready hospitals. However, there are no certified stroke units in Estonia as this is not required by the payor and the government. One of the obstacles is the fact that Estonia as a very small country cannot afford separate stroke units even in large hospitals. Stroke patients are treated in neurological departments usually by general neurologists. However, approximately 80% of all hospitalized neurological patients have stroke. Future plans include ESO certification for all stroke-ready hospitals in Estonia, however the very strict criteria might become an obstacle. 17
It is important to mention, that DNT-s are good in all stroke-ready hospitals and somewhat better than the goal of 30 min set by the RES-Q. The time logistics has probably been affected by COVID-19 pandemic and by the implementation of extended time window for IVT and MT since 2019 with the help of CT perfusion Rapid AI in three and emergency MRI in one hospital. 18 On the other hand, this has provided the access for recanalization therapies for a larger number of patients. The need for improvement of the ODT has been recognized and all hospitals work on defining the gaps and solutions for improvement.
The 30 days mortality is slowly decreasing. This may be related to better primary prevention and stroke unit care. The results of the indicators according to the Angles award program are not yet ideal and show that educational activities for the whole staff are needed for implementation of the results of evidence-based medicine into clinical practice. 16
The importance of teamwork in improving stroke care quality cannot be underestimated. Tartu University Hospital participated at the Quality in Acute Stroke Care Europe Project and the results show that more attention should be paid to the improvement of nursing care by training and using uniform protocols in all stroke-ready hospitals. 19 The registering of fever, blood sugar, swallowing data has also been incorporated into the new collection form of RES-Q and thereby enabling monitoring and analysing these basic principles of stroke unit care.
Rehabilitation and secondary prevention
The availability of inpatient post-stroke rehabilitation after stroke has been a general problem in Estonia. Although the proportion of patients receiving rehabilitation is slowly increasing, it has somewhat decreased during the COVID-19 pandemic. However, after the recognition of the shortcoming by the stakeholders, there have been some improvements also on the availability of outpatient rehabilitation and the early supported discharge will be the main focus in the future.
The proportion of patients receiving antiplatelets in secondary stroke prevention is good according to the RES-Q data. However, as aspirin is purchased without prescription, the adherence to treatment cannot be monitored after the ischemic stroke.
At discharge, nearly all patients are prescribed anticoagulants according to RES-Q data, but after 1 year following stroke approximately 50% receive the treatment. This could reflect a treatment adherence issue. All direct OACs are available and are reimbursed to the patients by 75%–90%. However, part of the low proportion could be related to data collection methodology. The RES-Q evaluates the time of discharge from the hospital and the national quality indicator is evaluated 1 year after stroke. Moreover, the national indicators reflect the proportion from all patients having the prescription not only surviving patients.
Life after stroke
In 2020, an innovation project funded by the EHIF focusing on improving life after stroke – rehabilitation, social support, returning to work, and patient’s quality of life was initiated and is ongoing in four hospitals. 20
The aim of the project is to improve patients’ quality of life through developing more integrated care pathway from the patient’s perspective. The project contains three activities: (1) The development projects at the hospitals. The development projects in 4/6 hospitals providing acute stroke care get extra funding from the EHIF’s innovation and the participating hospitals use different solutions and collaboration with the aim to improve stroke pathway and life after stroke. The patients’ representatives are also a member of the steering committee; (2) Collecting outcomes to understand the patients’ wellbeing and to improve their health outcomes using stroke standard set including patient-reported outcome measures. 21 Benchmarking enables to detect and learn from best practices. After the pilot the measuring can be extended to other hospitals and conditions; (3) Changing the payment into a bundled payment model: testing a new, bundled payment model for the whole stroke care pathway.
While data collection and monitoring mostly show the level of stroke care, there are several important aspects that lead to these results and contribute to the constant improvement in care quality (Figure 5).

The timeline of developments of stroke care quality in Estonia from 2003 to 2021 (ESO-EAST: European Stroke Organisation – Enhancing and Accelerating Stroke Treatments project; IVT: intravenous thrombolysis; MT: mechanical thrombectomy; RES-Q: Registry of Stroke Care Quality; SITS: Safe Implementation of Treatments in Stroke).
Estonian Stroke Initiative (ESI)
For 13 years, ESI has contributed to the education of stroke neurologists in Estonia and it has helped to achieve equal quality results at a national level. Educating also other members of the stroke care team will be given more attention in the future. ESI and ENNS have also been the primary partners for collaborations with governmental authorities and have continuously enhanced the improvement of stroke care quality in Estonia.
Stroke action plan
Estonia is actively participating in the Stroke Action Plan in Europe initiative. 22 We have compiled a comprehensive group of different organizations (societies of medical professionals, patient organization, governmental institutions) actively involved in the project. The joint Declaration for Action on Stroke is signed by all participants and the goals for the first year have been made.
Strengths and limitations of the study
The data from the RES-Q database are collected only once a year and thereby the number of cases is small with only limited power to be used for comparisons. However, as other data resources are available for the whole country, we can confirm, that the RES-Q data are in line with data from national quality indicators. One limitation of the RES-Q is manual and voluntary data entry with insufficient quality control. These limitations can be overcome by auditing and stricter definition of the collected variables, and this should be addressed in the future. 2
RES-Q data are collected in an unblinded manner during 1 month annually causing possibly performance bias. Most of the indicators rely on a comprehensive collaboration between pre-hospital and hospital staff on a pre-specified standard operating procedure implemented in the hospitals. We think that it is unlikely that the quality of care can be improved for 1 month only deriving from the fact that the quality is being monitored. Therefore, in addition to the RES-Q database, we presented the data of the national quality indicators in which all stroke cases in Estonia are included. As these variables are collected from the EHIF reimbursement database, those may therefore contain errors due to retrospective nature. However, the temporal trend can be analyzed as the methodology is unchanged.
Future perspectives
The continuous work on the stroke quality care over the past decades in Estonia has created a good basis for further developments. The Action Plan for Stroke in Europe has just begun and will hopefully add significant improvements in many areas of stroke care. Our priorities include continuous monitoring of quality indicators (including expanding the data collection into the RES-Q database, continuing with SITS registry, and national quality indicators), development of a digitalized platform for modern data collection (i.e. establishing Estonian Stroke Registry), continuous educational programs for stroke neurologists and other members of the stroke care team, improvement of secondary prevention strategies and ESO certification of stroke units in our country.
Conclusions
The trends of quality of acute stroke care in Estonia show improvement, however more emphasis should be paid on rehabilitation and secondary prevention. Together with the national quality indicators the RES-Q provide an excellent opportunity for monitoring the trends of stroke care and comparisons both national and international level.
Footnotes
Acknowledgements
The authors acknowledge the colleagues from five departments who contributed to the RES-Q, and the Irene Cost Action CA18118 for non-financial support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
No signed informed consent was obtained because of analysis of anonymous data from the Estonian Health Insurance Fund and the RES-Q.
Ethical approval
No ethical approval was obtained because of analysis of anonymous data from the Estonian Health Insurance Fund and the RES-Q.
Guarantor
Janika Kõrv.
Author contributions
JK and RV contributed to conception and study design. JK, RV, IK, KGP, AK, AL, and KA contributed to acquisition and analysis of data. JK and RV contributed to drafting of the manuscript and figures. IK, KGP, AK, AL, and KA contributed with critical comments during manuscript revision. All authors approved the submitted manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author (JK), upon reasonable request.