
Abstract
Introduction:
The COVID19 pandemic collapsed intensive care units (ICUs) all around the world, conditioning systems of care (SOC) for other critical conditions such as severe ischemic stroke requiring endovascular treatment (EVT). Our aim was to evaluate the impact of an adaptive Stroke Unit (SU) based SOC on functional outcomes, with the goal of avoiding both general anesthesia (GA) and ICU admission in stroke patients treated with EVT.
Material and methods:
We performed an observational study comparing data from our traditional ICU-GA based SOC and the adaptive SU-Conscious Sedation (CS) based SOC (consecutive patients undergoing EVT 1 year prior and after onset of the pandemic). Primary outcome was 90-days modified Rankin Scale (mRS), and secondary outcomes included, among others, in-hospital complications, and hospital length of stay (LOS).
Results:
A total of 210 EVT were performed during the study period (107 under the traditional-SOC and 103 under the adaptive-SOC). A significantly greater proportion of patient was treated under CS (15.9% vs 57.3%; p < 0.001) and admitted for post-procedural care at SU (15% vs 66%; p < 0.001) in the adaptive SOC. Rates of in-hospital complications were similar in both periods, with reduced hospital LOS in the adaptive SOC (10 (7–15) vs 8 (6–12); p = 0.005). The adaptive SOC was associated with higher odds for 90 days favorable outcome (mRS 0–2) (aOR 3.15 (1.34–7.39); p = 0.008).
Conclusion:
In our case, an adaptive SOC that combined both preference for CS and postprocedural care in SU was associated with better functional outcomes and reduced healthcare resource use for patients undergoing EVT.
Keywords
Introduction
Endovascular treatment (EVT) represents one of the two effective reperfusion therapies for acute ischemic stroke (AIS), and it has been proven effective in improving functional outcome of these patients. 1 This therapy is only delivered in stroke centers with enough resources and under complex systems of care that condition peri-procedural care. 2 Currently, there is no clear indication concerning where these patients should be admitted nor which level of care they require. Current guidelines recommend that patients with AIS should be admitted to stroke units (SU), 3 and recommendations regarding peri-procedural care for patients undergoing EVT include admission to neurologic intensive care units. 4 To our knowledge, there is no comparative literature concerning admissions to intermediate level of care SU versus Intensive Care Units (ICUs). Furthermore, there is no consensus regarding the best anesthesia protocol for patients undergoing EVT. Observational studies including large numbers of patients suggest that general anesthesia (GA) is associated with worse functional outcome, 5 whereas meta-analysis from randomized clinical trials may indicate a better functional outcome for these patients. A recent meta-analysis of these randomized clinical trials demonstrates that GA is associated with better functional outcomes, 6 in contrast to the HERMES collaboration, that demonstrated that patients undergoing EVT under conscious sedation (CS) have better functional outcomes. 7 As mentioned above, due to the lack of consensus regarding the previous facts, that indeed conditions the system of care for patients undergoing EVT, institutions usually develop protocols based on their own experience and availabilities.
The COVID-19 pandemic has collapsed the ICUs all around the world because of the severely affected patients requiring invasive mechanical ventilation. This fact has conditioned the systems of care for other disorders potentially requiring ICU beds like myocardial infarction, major trauma, and stroke. In the case of stroke, this especially affects the systems of care for patients undergoing EVT.8,9 These patients might require invasive mechanical ventilation as well as GA, and, depending on clinical severity, admission at the ICU. Most of the acute stroke services have seen significant reorganization or some have even been closed, and the ability to offer endovascular treatment has been reduced in many units. 9 Several reports indicate a negative impact in the outcomes of patients suffering from stroke and undergoing EVT derived from the pandemic 10 and the consequent adaptive protocols. 11
Our center’s traditional system of care involved a preference for GA and posterior admission at the ICU for post-procedural care, with the length of stay in ICU depending on clinical evolution. In order to decrease the need for mechanical ventilation and reduce admissions to the ICU, so as to maintain the ability to offer EVT for patients suffering from acute ischemic stroke in spite of the impact of the pandemic, this protocol was adapted with preference for CS and an adaptive SU-based system of care was established (Supplemental Figure S1).
Our primary objective is to assess the impact of this adaptive SU based system of care on 90-day functional outcome for patients undergoing EVT, compared to the previous traditional ICU based system of care. Our secondary objectives are to assess the impact of this system of care regarding healthcare resource use (hospital length of stay (LOS), LOS at ICU, and need for institutional care after the acute phase of stroke), procedural metrics, and in-hospital complications.
Methods
We retrospectively reviewed data from a prospective registry of consecutive patients with AIS undergoing EVT that were admitted to our center, which covers a population of approximately 715.000 people with an average of 105 EVT performed per year. Our center represents a tertiary hospital, reference for acute ischemic stroke care in the region of Gipuzkoa in northern Spain. Therefore, patients requiring acute reperfusion therapies are transferred to our center directly. We included AIS patients receiving EVT from the immediate pre-pandemic 1-year period (March 2019–February 2020) under our traditional system of care and patients receiving EVT during the first year of the pandemic period (March 2020–February 2021) under an adaptive system of care.
All patients were evaluated by a multidisciplinary team including emergency-physicians and neurologists prior to EVT, as well as anesthesiologists and neurointerventional radiologists during the procedure. Neurointerventional staff composition was the same during the study period. Patients treated under our traditional system of care were usually treated under GA (only exceptionally using CS), and subsequently admitted at the ICU for post-procedural care provided by intensive care physicians. Patients treated under the adaptive system of care underwent an individualized decision concerning the anesthesia protocol (with avoidance of GA if possible) and preference for post-procedural care at a specialized intermediate level of care SU provided by neurologists (with support from anesthesiologists and/or intensive care physicians when needed), depending on bed availability in both units (Supplemental Figure S1). Post procedural care for all patients included non-invasive monitoring (and invasive monitoring if needed at the ICU/Post Anesthesia Care Unit) and follow-up CT at 24 h before starting antithrombotic treatment. As for blood-pressure management, threshold for the use of antihypertensive medications was done following current AHA guidelines, 3 although final decisions were made under in-charge physicians’ discretion in each unit. Patients were transferred to the neurology ward after clinical stabilization and were discharged from the hospital following the same procedures during the study period.
We collected baseline demographic characteristics, medical history, including baseline modified Rankin scale (mRS), as well as clinical and radiological characteristics of the stroke: National Institutes of Health Stroke Scale (NIHSS) score, site of vessel occlusion, Alberta Stroke Program Early CT Score (ASPECTS) in anterior circulation strokes and posterior circulation ASPECTS (PC-ASPECTS) in posterior circulation strokes, presence of hyperdense artery sign and presence of target-mismatch profile. We also collected data from the modality of reperfusion therapy (pretreatment with intravenous thrombolysis or direct EVT), stroke management metrics (onset-to-hospital presentation, onset-to-needle, onset-to-puncture, onset-to-recanalization, door-to-needle, door-to-puncture, door-to-recanalization, and puncture-to-recanalization delays), technique of EVT (stent retriever, thromboaspiration, combined technique, intraarterial alteplase or angioplasty), number of device passes, final angiographic recanalization modified Thrombolysis In Cerebral Infarction (mTICI) scale, anesthetic method, ventilation time, both local and intracranial procedural complications, and destination after EVT (SU or ICU).
In-hospital complications included symptomatic hemorrhagic transformation, in-hospital recurrence, acute symptomatic seizures, respiratory and urinary tract infections, and congestive heart failure. Hospital LOS, LOS at ICU, need for chronic disease and rehabilitation inpatient hospital services after the acute phase of stroke and 3-month mortality were also collected. Clinical outcome evaluation (90-day modified Rankin Scale, mRS) was assessed at out-patient neurovascular clinic or by a standardized telephone interview performed by the same trained neurovascular specialist nurse. Favorable clinical outcome was defined as a mRS score <3.
We first compared both cohorts (traditional and adaptive system of care) for all variables by univariate analysis, and we then performed a univariate analysis to evaluate variables associated with favorable clinical outcome. Qualitative variables were expressed as number of patients (percentage) and compared with the chi-squared or Fisher’s exact tests, as appropriate. Quantitative variables were expressed as median (interquartile range) or mean (standard deviation, SD) and compared using the Mann–Whitney or student’s t-test, as appropriate. Multivariate logistic regression model was used to determine the association between the system of care and functional outcome adjusted for clinically relevant variables associated with functional outcome from univariate analyses (p < 0.05). The analyses were performed using IBM-SPSS Statistics version 21.0. The project was approved by our institution’s Clinical Research Ethics Committee (PI2020122).
Results
A total of 210 EVT were performed during the whole study period, with a similar number of procedures performed during the pre-pandemic (n = 107) and pandemic periods (n = 103). Baseline characteristics of patients were similar in both cohorts, although previous treatment with antiplatelet therapy was significantly more frequent in the traditional system of care group (30 (28%) vs 11 (10.7%); p = 0.002) and there was a trend toward more frequent prior anticoagulation treatment in the adaptive system of care group (22 (20.6%) vs 33 (32%); p = 0.062). However, the proportion of patients with previous atrial fibrillation was similar in both cohorts (32 (29.9%) vs 31 (30.1%); p = 0.976). Stroke with known onset time was more frequent in the adaptive system of care group (57.9% vs 70.9%; p = 0.051). Clinical severity, site of vessel occlusion and ASPECTS/PC-ASPECTS scores were similar in both groups. Information concerning baseline characteristics, clinical severity, and radiological characteristics of the stroke is detailed in Table 1. Only two patients infected by SARS-CoV2 underwent EVT during the study period.
Baseline characteristics of patients, clinical, and radiological characteristics of the stroke in both cohorts.
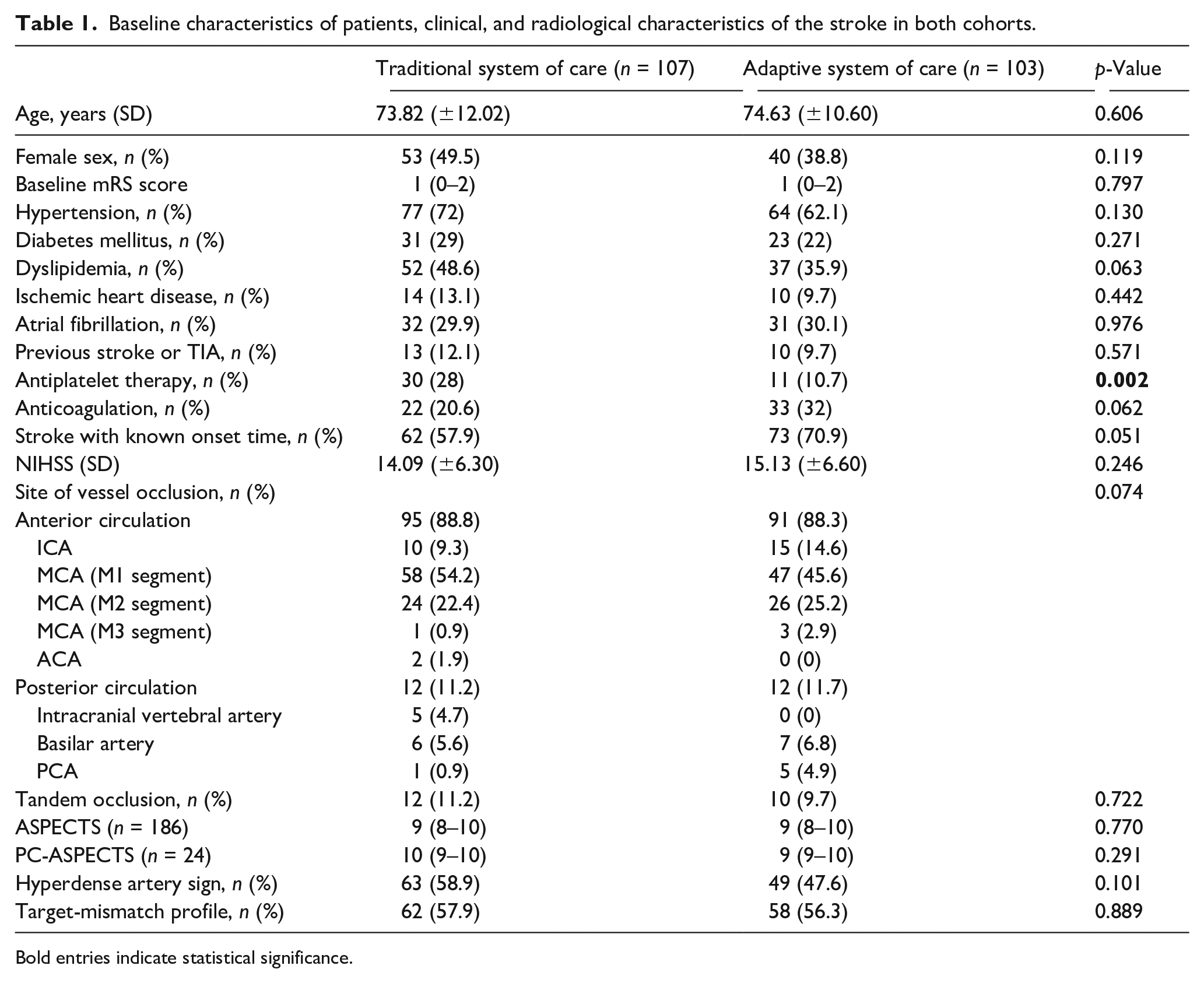
Bold entries indicate statistical significance.
Regarding stroke treatment, there were no differences in time window and time metrics except for a decreased median time from puncture to recanalization in the adaptive system of care group (50 (28–57) vs 41.5 (20–68.5) min; p = 0.014). Previous administration of intravenous thrombolysis and technique of EVT were similar in both groups, with a slight trend to fewer number of devices passes (2 (1–3) vs 1 (1–2.7); p = 0.063). An increased proportion of final TICI 3 scale (51 (47.7%) vs 68 (70%); p = 0.013) was observed in the adaptive system of care group, although the rates of successful reperfusion TICI2B/3 were similar between the two groups (95 (88.8%) vs 92 (89.3%); p = 0.901). As a result of to the changes implemented in the adaptive system of care, a significantly greater proportion of patients were treated under CS (15.9% vs 57.3%; p < 0.001) in this cohort. Local inguinal procedural complications were infrequent in both groups (4 (3.7%) vs 4 (3.9%); p = 1.000), and there was only one clinically relevant complication of the procedure at the intracranial circulation level in the whole study period (1 distal embolization (0.9%) in the traditional system of care group).
Due to the implementation of the adaptive pandemic system of care, an increased proportion of patients were transferred to the SU after the EVT, compared to the previous period (16 (15%) vs 68 (66%); p < 0.001). Most of these patients were transferred immediately to the SU and a small proportion were transferred to the SU after a short post-anesthesia care unit stay (nine patients, 13.2%). In relation to transfers between units during the whole study period, on the one hand, only three patients (3.68%) needed to be transferred to the ICU after initial admission at the SU because of clinical deterioration (one because of hydrocephalus, one because of symptomatic hemorrhagic transformation, and one because of severe acute respiratory failure). On the other hand, three patients (2.4%) initially admitted at the ICU were transferred to the SU (one because of in-hospital stroke recurrence and two because patients required intermediate level of care before transferring to the general ward).
There were no significant differences regarding in hospital complications in both groups. Both ICU and total hospital LOS were shorter during the pandemic period (LOS at ICU: 2 (1–3) vs 0 (0–1); p < 0.001; total hospital LOS: 10 (7–15) vs 8 (6–12); p = 0.005). There was a trend to an increased proportion of patients discharged home, and, therefore, not requiring institutional care after acute phase (46 (43%) vs 58 (56.6%); p = 0.054). On the 90-day evaluation, there was a significant increase in the proportion of patients achieving a favorable clinical outcome in the adaptive system of care group (38 (35.5%) vs 62 (60.2%); p < 0.001) (Figure 1) and a trend toward a reduction of the patients requiring institutional care (14 (13.3%) vs 6 (5.8%); p = 0.066). This significant increase in the proportion of patients achieving a favorable clinical outcome in the adaptive system of care was also seen in patient that achieved complete recanalization (TICI3) (21 (41.2%) vs 48 (68,6%); p = 0.003). Full information regarding Stroke treatment metrics, in-hospital stay, complications, mortality and functional outcome can be found in Table 2.
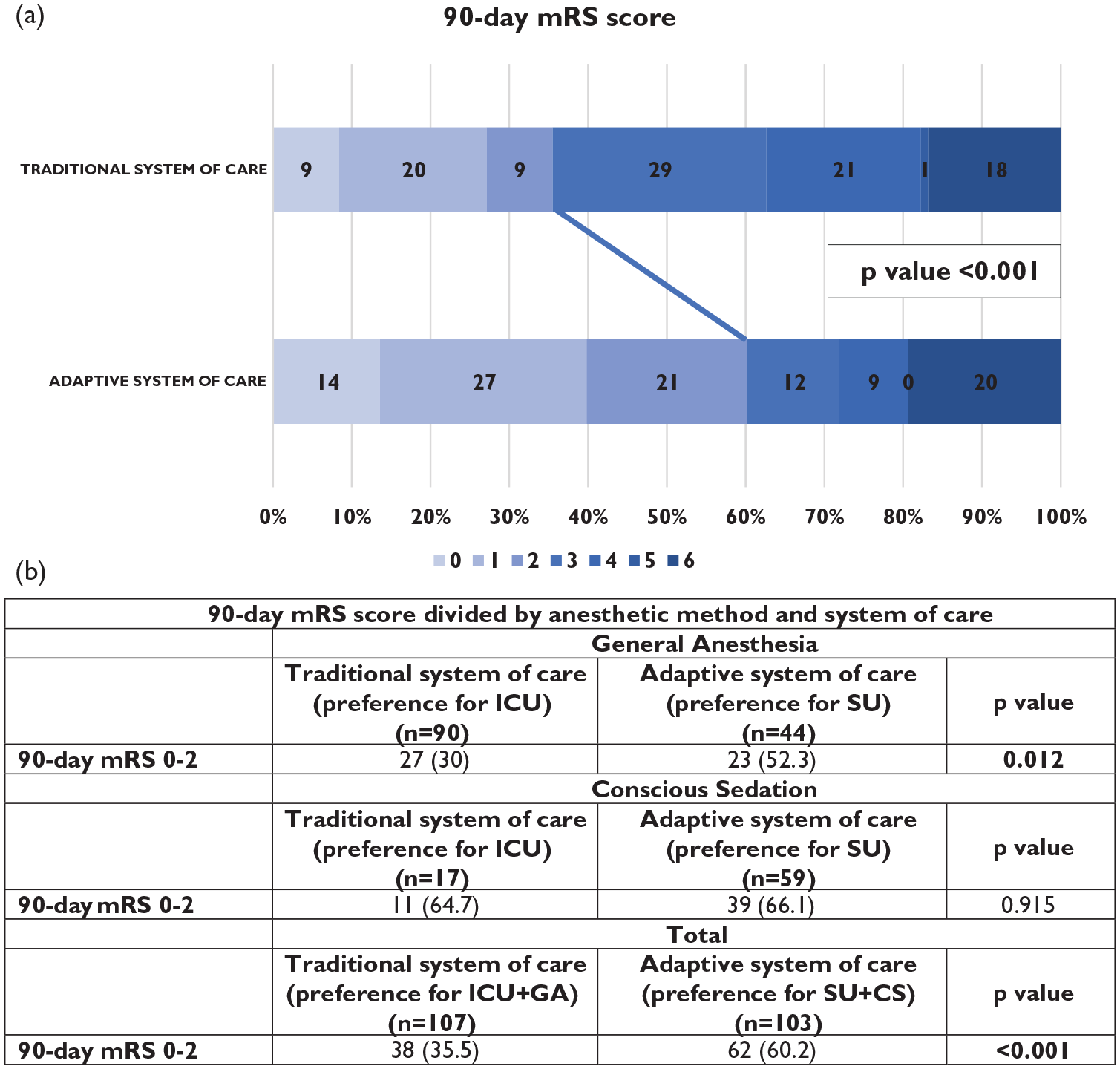
(a) Distribution of 90-day mRS score of patients in both cohorts. (b) Ninety-day favorable outcomes (mRS 0–2) split based on the anesthetic method.
Stroke treatment metrics, in-hospital stay, complications, and clinical outcome of patients in both cohorts.
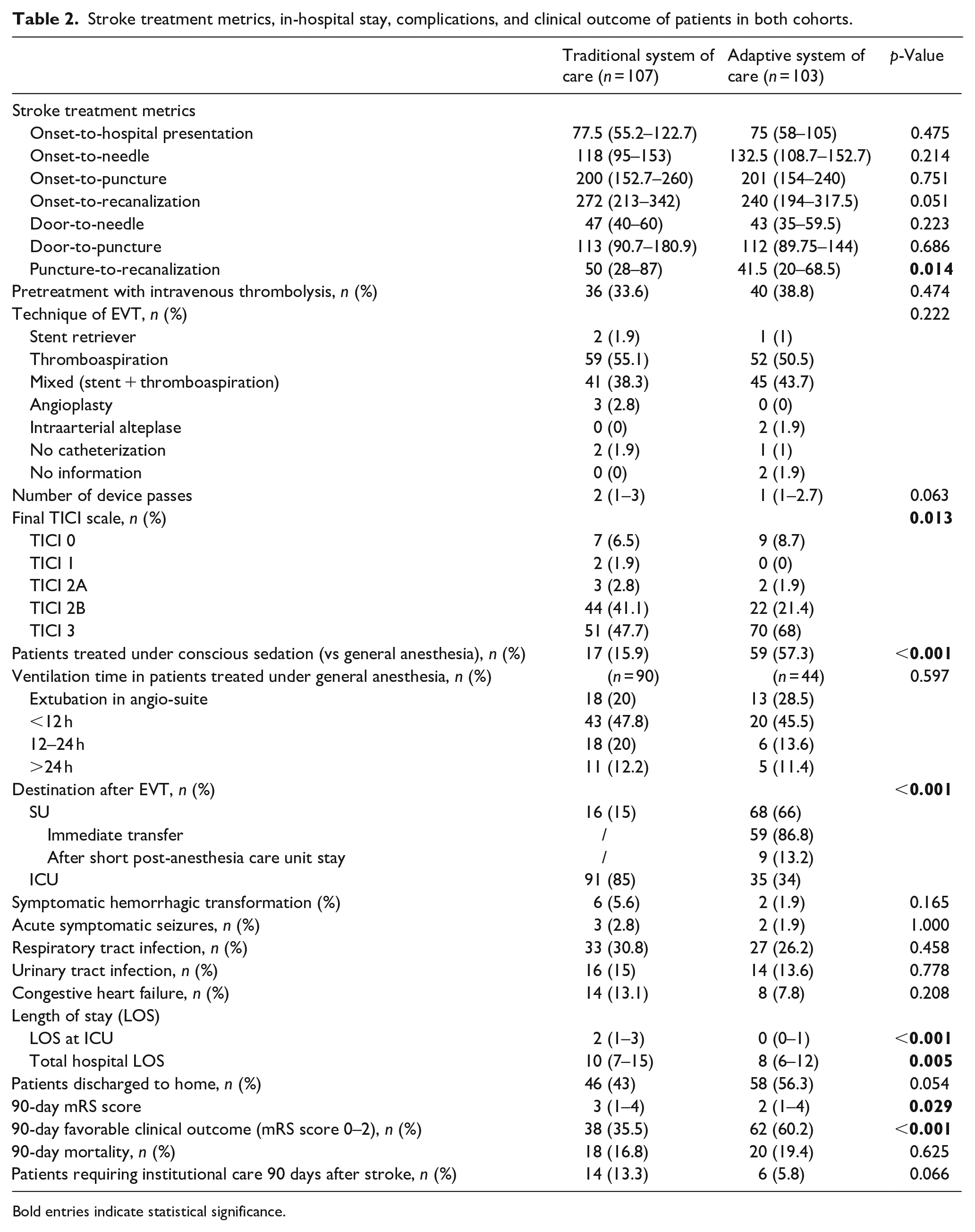
Bold entries indicate statistical significance.
The evolution of the implementation of the adaptive system of care led to a constantly increased proportion of patients treated under CS and admitted to the SU, as seen in Figure 2. The evolution of these two variables during the whole study period in relation to the proportion of patients achieving a favorable outcome at 90 days is also shown in Figure 2.
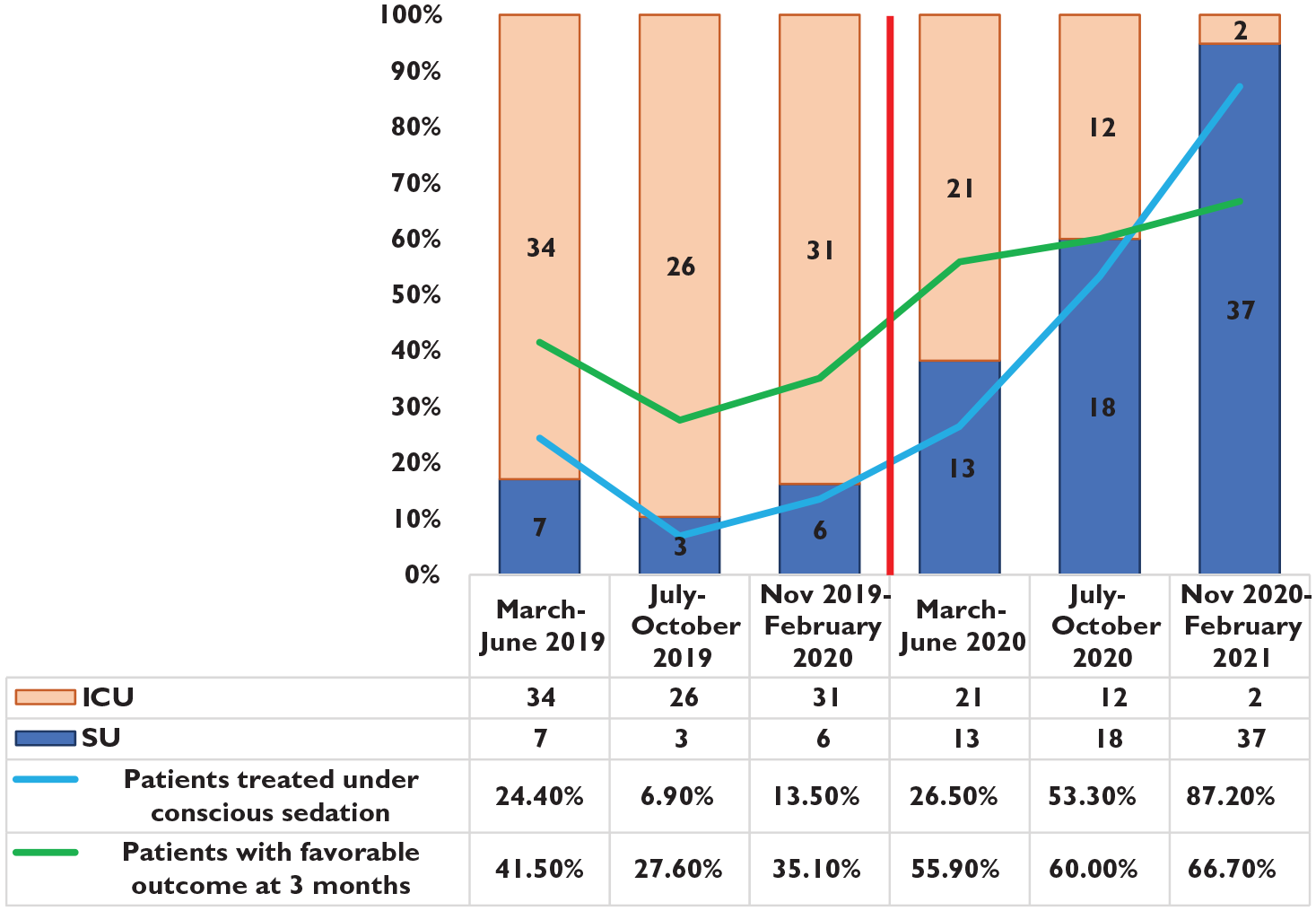
Evolution and relation between proportion of patients admitted to ICU/SU (columns), patients treated under conscious sedation (blue line), and patients with favorable outcome at 90 days (green line). Vertical red line represents the beginning of the COVID19 pandemic and the implementation of an adaptive system of care.
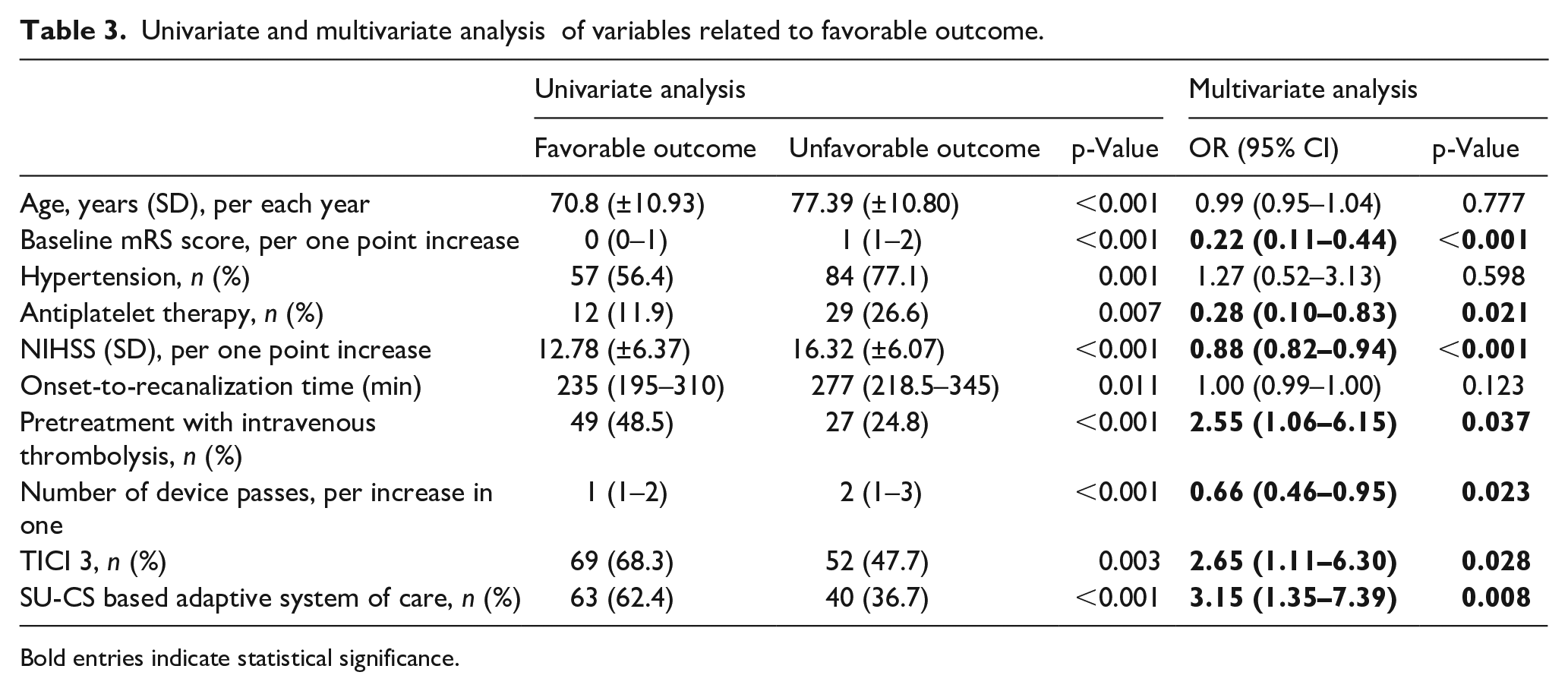
As presented in the multivariate analysis including the variables selected from the univariate analysis (Supplemental Table S2), the adaptive pandemic system of care was independently associated with a favorable 90-day clinical outcome (OR 3.15 (1.35–7.39); p = 0.008), along with baseline mRS score (OR 0.22 (0.11–0.44); p < 0.001), antiplatelet therapy (OR 0.28 (0.1–0.83); p = 0.021), NIHSS (OR 0.88 (0.82–0.94); p < 0.001), pretreatment with intravenous thrombolysis (OR 2.55 (1.06–6.15); p = 0.037), number of device passes (OR 0.66 (0.46–0.95); p = 0.023), and TICI 3 (OR 2.65 (1.11–6.30); p = 0.028) (Table 3).
Univariate and multivariate analysis of variables related to favorable outcome.
Bold entries indicate statistical significance.
Discussion
The aim of this study was to assess the consequences of the implementation of an adaptive SU based system of care in the context of the COVID19 pandemic. Although there were concerns of a probable reduction in the ability to offer endovascular treatments because of the pandemic, as outlined in previous reports, 9 in our center, the adaptive system of care helped to maintain a similar number of patients receiving EVT, compared to the previous period. There were also no differences in the criteria for the selection of patients: age, baseline mRS, site of vessel occlusion, and clinical severity were similar to the previous cohort.
This adaptive system of care significantly increased the used of CS in patients undergoing EVT (15.9% vs 57.3%; p < 0.001), contrary to some initial recommendations in regard to the selection of the anesthetic method in the context of the pandemic. The Society for Neuroscience in Anesthesiology and Critical Care suggested that in the context of the pandemic, a lower threshold to use GA should be followed, and that CS was suitable for experienced centers with low rates of conversion. 12 This trend toward an increased use of GA was followed in some adaptive protocols, leading to an increased proportion of patients being discharged with an unfavorable outcome. 11 However, other centers that maintained a traditional protocol that uses CS as first choice, reserving GA for airway, respiratory or hemodynamic compromise, did not suffer an impact of the pandemic in functional outcome among EVT treated patients. 13
In our case, despite not being an experienced center in treating patients under CS, neurointerventionalists and anesthesiologists rapidly adapted to the intraprocedural changes, with 87.20% of the patients being treated under CS during the last 4 months of the study period, as seen in Figure 2. One of the theorical advantages of GA includes less risk for patient movement, with improved neurointerventionalist comfort and a possible reduction of intraprocedural complications. However, in our case, the increased use of CS led to a shorter puncture-to-recanalization time (50 (28–57) vs 41.5 (20–68.5) min; p = 0.014), with similar rates of intraprocedural complications. Another theorical advantage of GA includes secure airway with consequent reduced risk of aspiration, which was not confirmed in our case, with similar rates of respiratory tract infections in both systems of care. In addition to reducing the need for GA, we also tried to reduce ventilation time in patients that required from it, with a trend toward more patients being extubated in the angio-suite (18 (20%) vs 13 (28.5%); p = 0.597). A shorter ventilation time has also been related with a better prognosis after EVT for stroke. 14
As mentioned previously, the ongoing discussion concerning the studies comparing anesthetic methods have not concluded which is the best option for patients undergoing EVT.5–7 We suggest that this debate may not be answered in absolute terms (GA vs CS), and that an individualized protocol that uses CS as first choice, reserving GA for patients with airway, respiratory or hemodynamic compromise might be the optimal response to answer this question, although this should be evaluated in larger prospective trials in which individualized protocols are compared.
The other major change we implemented was the preference for post-procedural care of patients in intermediate level of care SU, with support from anesthesiologists and intensive care physicians if needed. The benefits of implementing organized SUs for treating patients suffering from stroke are well known, as patients are more likely to be alive, independent, and living at home 1 year after the stroke. 15 Factors as interventions with the goal of preventing complications, being treated by physicians and nurses specialized in stroke and optimal antithrombotic therapy management might explain the better outcomes of these patients.16,17 Even though these benefits have not been specifically studied for patients undergoing EVT, the relevance of the systems of care in the positive trials that demonstrated the benefits of EVT has been outlined. 18
Currently, there are no studies available comparing outcomes between ICUs and SUs for patients suffering from ischemic stroke and undergoing EVT. As seen in Table 2 and Figure 2, the progressive implementation of the adaptive system of care led to a significant reduction in the need for ICU admission of patients, with only 5.12% of the patients being admitted for critical care in the last 4 months. The consequences not only included better patient outcomes, but also variables with economic implications such as days of ICU admission, total LOS, and need for institutional care improved considerably. Benefits from the admission of non-comatose patients with other types of potentially severe strokes in SUs, such as aneurysmal subarachnoid hemorrhage and intracerebral hemorrhage, have also been suggested in recent observational studies that compare admission to ICUs and SUs.19,20 The fact that the preference for postprocedural care at the SU accompanied the change of anesthetic method in our case might be the reason for the larger benefit observed in the present study, compared to other recent observational studies that supported the superiority of CS over GA. 21
It is essential to outline that the implementation of this adaptive system of care was made in a forced way, due to an unpredictable event like COVID-19 pandemic, with no previous planning or designing. Despite difficulties, as mentioned above, professionals from all the disciplines involved in the care of these patients rapidly adapted, with an unexpected consequent significant improvement in functional outcome and a significant reduction in the use of in- and out-of-hospital resources.
Limitations of this study include the retrospective observational design, relatively small sample size, and that both cohorts are not simultaneous in time. Differences in baseline characteristics of patients in regard to previous antiplatelet therapy should also be noticed. Moreover, the association of both measures adopted in the adaptive system of care (preference for CS and preference for admission to SU) does not allow to analyze the relevance of each variable on its own in the observed improvement in patient outcomes.
In conclusion, in our case, the pandemic has meant a change toward a more effective system of care for patients suffering from acute ischemic stroke and undergoing EVT. A multidisciplinary system of care that combines both preference for CS and postprocedural care in SU, in patients who do not require from critical care, was associated with better functional outcomes and reduced healthcare resource use, including reduced hospital LOS and need for institutional care.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221098269 – Supplemental material for Impact on functional outcome of an adaptive Stroke Unit based system of care for patients undergoing endovascular treatment during pandemic times
Supplemental material, sj-docx-1-eso-10.1177_23969873221098269 for Impact on functional outcome of an adaptive Stroke Unit based system of care for patients undergoing endovascular treatment during pandemic times by Jon Equiza, Patricia de la Riva, José Angel Larrea, Juan Marta-Enguita, Inés Albájar, Alex Lüttich, Eñaut Garmendia, Maitane Alonso, Ana de Arce, Noemí Díez, Félix Gonzalez, Pablo Iruzubieta, Naroa Sulibarria, Josep Puig and Maite Martínez-Zabaleta in European Stroke Journal
Supplemental Material
sj-docx-2-eso-10.1177_23969873221098269 – Supplemental material for Impact on functional outcome of an adaptive Stroke Unit based system of care for patients undergoing endovascular treatment during pandemic times
Supplemental material, sj-docx-2-eso-10.1177_23969873221098269 for Impact on functional outcome of an adaptive Stroke Unit based system of care for patients undergoing endovascular treatment during pandemic times by Jon Equiza, Patricia de la Riva, José Angel Larrea, Juan Marta-Enguita, Inés Albájar, Alex Lüttich, Eñaut Garmendia, Maitane Alonso, Ana de Arce, Noemí Díezz, Félix Gonzalez, Pablo Iruzubieta, Naroa Sulibarria, Josep Puig and Maite Martínez-Zabaleta in European Stroke Journal
Footnotes
Acknowledgements
Part of this work has been previously presented at the Annual Meeting of the Spanish Academy of Neurology (November 2021).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not required as the manuscript does not include individual patient data or patient images.
Ethical approval
The project was approved by the Basque Government’s Clinical & Drug Research Ethics Committee
Guarantor
MMZ is the guarantor of this manuscript and takes full responsibility for the article, including for the accuracy and appropriateness of the reference list.
Author contributions
All authors of this work met the International Committee of Medical Journal Editors criteria for authorship and made substantial contributions to the conception and design, acquisition of data, analysis and interpretation of data, drafting, critical revising, and final approval of this manuscript.
Data sharing
All data relevant to the study are included in the article or uploaded as Supplemental Information.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.