
Abstract
The safety and efficacy of mobile stroke units (MSUs) in prehospital stroke management has recently been investigated in different clinical studies. MSUs are ambulances equipped with a CT scanner, point-of-care lab, telemedicine and are staffed with a stroke specialised medical team. This European Stroke Organisation (ESO) guideline provides an up-to-date evidence-based recommendation to assist decision-makers in their choice on using MSUs for prehospital management of suspected stroke, which includes patients with acute ischaemic stroke (AIS), intracranial haemorrhage (ICH) and stroke mimics. The guidelines were developed according to the ESO standard operating procedure and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) methodology. The working group identified relevant clinical questions, performed systematic reviews and aggregated data meta-analyses of the literature, assessed the quality of the available evidence and made specific recommendations. Expert consensus statements are provided where sufficient evidence was not available to provide recommendations based on the GRADE approach. We found moderate evidence for suggesting MSU management for patients with suspected stroke. The patient group diagnosed with AIS shows an improvement of functional outcomes at 90 days, reduced onset to treatment times and increased proportion receiving IVT within 60 min from onset. MSU management might be beneficial for patients with ICH as MSU management was associated with a higher proportion of ICH patients being primarily transported to tertiary care stroke centres. No safety concerns (all-cause mortality, proportion of stroke mimics treated with IVT, symptomatic intracranial bleeding and major extracranial bleeding) could be identified for all patients managed with a MSU compared to conventional care. We suggest MSU management to improve prehospital management of suspected stroke patients.
Introduction
Despite many efforts to speed up and optimise acute stroke patient management, still only 0.8–1.3% of acute ischaemic stroke (AIS) patients receive their intravenous thrombolysis (IVT) within the so-called golden hour – the first 60 min after symptom onset, when chances of full recovery are highest.1,2 Many reports on stroke scales,3–7 emergency medical service (EMS) training and educational programmes,8–12 structured EMS pre-notification to hospital stroke teams,13–15 emergency department streamlining16–20 and different triage pathways (mothership vs drive the doctor vs drip and ship)21–31 have all demonstrated an improvement of treatment numbers and times, but timely delivery of the available and highly beneficial reperfusion therapies [IVT and mechanical thrombectomy (MT)] to AIS patients is still underachieved. Furthermore, delays in onset to treatment times correlate to longer bolus to reperfusion times in AIS patients with proximal intracranial occlusions treated with IVT. 32 Similarly, for patients with intracerebral haemorrhage (ICH), time to treatment and thus time to diagnosis is critical. 33 Large haematoma volumes and haematoma expansion are associated with poor clinical outcome 34 leading to a recommendation for early BP management. 35 Furthermore, given the fact that the use of anticoagulation has been associated with haemorrhage growth, anticoagulation reversal represents a key treatment option for ICH patients on anticoagulation therapy. 36
Many of these strategies depend on a quick differentiation of stroke patients from those with so-called stroke mimicking diseases 37 or different subtypes of stroke, which strongly depends on the training and expertise of the individual teams involved as well as brain imaging availability. To optimise access to treatments and the acute management of stroke patients, strategies crossing institutional boundaries are needed and have to also involve the prehospital stage.
Over the last 18 years, a new concept for acute stroke management using Mobile Stroke Unit (MSU) ambulances has emerged and evolved. 38 MSUs are emergency ambulances equipped with a computed tomography (CT) scanner for multimodal brain imaging (including CT angiography with or without CT perfusion), point-of-care blood analysis, telemedicine connection to stroke centres and dedicated and specialised teams on board, who if not part of their medical education, received additional training in stroke medicine. There are increasing numbers of stroke centres worldwide using MSUs to provide acute stroke care to their patients (world map with active centres on https://www.prestomsu.org).39,40 Reported results indicate an earlier treatment, increased numbers of patients receiving treatment and optimised triage to the individually required level of care.41–51 Most importantly, some studies have resulted in clinical benefits for patients treated with a MSU rather than conventional stroke care.49,50,52 In view of the former considerations and to address the current knowledge gap on this topic, we set out to provide the first guideline on the use of MSUs for stroke care. The current guideline aims to provide recommendations about whether MSU ambulances are of advantage for prehospital stroke management and to facilitate decision-making when considering MSU implementation as a service improvement. However, at the time of the emergency call a definite diagnosis is not clear and MSU ambulances will be involved in the assessment and treatment of patients with suspected stroke as well as those with confirmed ischaemic or haemorrhagic stroke. Therefore, to pay tribute to real-life practical aspects of the operation of a MSU within the EMS, these three different patient populations were considered in this guideline. To reflect this operational aspect, we combined all results to one recommendation only, which can be found at the end of the result section.
Methods
This guideline was initiated by the European Stroke Organisation (ESO) and prepared according to ESO standard operating procedures 53 , which are based on the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) system. 54 The ESO Guideline Board and Executive Committee reviewed the intellectual and financial disclosures of the module working group (MWG) members (Supplemental Table 1) and approved the composition of the group, which was co-chaired by the first (SW) and last (G Tsivgoulis) authors.
The MWG undertook the following steps: 1. Produced a list of topics of clinical interest to Guideline users that were agreed by all MWG members. 2. Three Patient Intervention Comparator Outcome (PICO) questions were developed and agreed upon within the MWG following a teleconference and e-mail correspondence. The three PICO questions were related to the following populations: patients with suspected stroke, patients with confirmed AIS & patients with confirmed acute ICH. The MWG formulated a list of PICO questions according to the ESO Guideline SOP, which were reviewed and subsequently approved by members of the ESO Guideline Board and Executive Committee. 3. Produced the following list of relevant outcomes and assessed their importance for which the MWG used the Delphi method (mean score from 8 respondents on a scale of 1 to 9; 7 to 9 – critical; 4 to 6 – important and 1 to 3 – of limited importance):
55
The list of outcomes in patients with suspected stroke was: • All-cause mortality (90 days) mean score: 7.9/9 • All-cause mortality (7 days) mean score: 7.6/9 • Symptomatic intracranial haemorrhage (sICH) mean score: 7.5/9 • Proportion of stroke mimics treated with IVT mean score: 6.4/9 • Major extracranial bleeding mean score: 6.1/9
Functional outcome was not included in the list of outcomes of suspected stroke patients because functional outcome using the modified Rankin Scale (mRS) score was not evaluated for stroke mimics.
The list of outcomes in the AIS subgroup was: • Excellent functional outcome, mRS 0–1 (90 days) mean score: 8.9/9 • Any better functional outcome (90 days) mean score: 8.8/9 • Good functional outcome, mRS 0–2 (90 days) mean score: 8.4/9 • All-cause mortality (90 days) mean score: 8.0/9 • Proportion receiving treatment with IVT/MT mean score: 7.5/9 • sICH mean score: 7.3/9 • Time between emergency call (alarm) and reperfusion therapy mean score: 7.3/9 • Treatment with IVT within the golden hour mean score: 7.1/9 • All-cause mortality (7 days) mean score: 7.0/9 • Proportion of large vessel occlusion (LVO) patients transported to a tertiary care stroke centre mean score: 6.8/9 • Major extracranial bleeding mean score: 6.0/9
Treatment with IVT within the golden hour was pre-specified for all patients with confirmed AIS included in the studies and for the subgroup of patients receiving IVT.
The list of outcomes in the ICH subgroup was: • Good functional outcome, mRS 0–2 (90 days) mean score: 8.5/9 • Any better functional outcome (90 days) mean score: 8.3/9 • All-cause mortality (90 days) mean score: 8.1/9 • Excellent functional outcome, mRS 0–1 (90 days) mean score: 7.6/9 • All-cause mortality (7 days) mean score: 7.5/9 • Proportion of ICH patients transported to a tertiary care centre mean score: 6.3/9 • Size of haematoma expansion mean score: 6.0/9
Based on voting scores, functional outcomes were allocated highest priority for confirmed AIS and ICH patients, while all-cause mortality was allocated the highest priority for suspected stroke patients. Unless specified otherwise, ‘excellent’ and ‘good’ functional outcomes were defined as 3-month mRS scores of 0–1 and 0–2, respectively.35,56,57 Unless specified otherwise, ‘any better’ functional outcome corresponded to an ordinal shift analysis of the mRS score (at least 1-point improvement across all mRS scores) at 3 months. 4. The recommendation was based on a systematic review of randomised trials and non-randomised studies evaluating the effect of MSU on the selected outcomes of the three populations of interest. Trials were categorised as randomised when randomisation was described in the trial protocol and in the publication of study results. All randomised studies used a cluster randomisation design. Non-randomised studies were subdivided into studies of intervention with experimental design, if their outcome was assessed in a blinded fashion. All other studies were categorised as non-interventional studies.
58
The literature search was completed on October 30, 2021. We conducted a systematic review for all PICOs resulting in 23 different sets of analyses (2 for suspected stroke, 18 for confirmed AIS, 3 for confirmed ICH). We also conducted a sensitivity analysis after removing the non-randomised studies without blinded endpoint assessment (3 sets of analyses). In case of unavailable or unclear data due to partially overlapping sets of participants, the corresponding authors of relevant studies were contacted to obtain unpublished, disentangled results collected but not reported in the original publication.
52
This was incorporated in the present analyses. 5. Six MWG members (SW, HA, KL, TS, SS and G.Turc) independently screened the titles and abstracts of the publications identified by the electronic search and assessed the full text of potentially relevant randomised and non-randomised studies. 6. Where appropriate, a random-effects meta-analysis was conducted by two MWG members (AHK, G. Tsivgoulis) who were not involved in any of the included studies using Stata software version 13.0 (Statacorp), with results summarised as odds ratios (ORs), common odds ratios (cORs) and 95% confidence intervals (CI). Crude ORs and cORs were abstracted or calculated from individual studies and all reported pooled associations of the meta-analysis are not adjusted for potential confounders. The DerSimonian and Laird method was used for all analyses.
59
Time metrics were evaluated using mean differences (MD) and corresponding standard deviations (SD) reported in individual studies. The pooled MD is reported with corresponding 95% CI. Any heterogeneity across studies was assessed using the I2 statistic, and heterogeneity was classified as moderate (I2 ≥ 30%), substantial (I2 ≥ 50%) or considerable (I2 ≥ 75%).
60
The updated Cochrane Collaboration risk of bias tool (RoB 2)
61
was used for the risk of bias assessment, in line with previous ESO guidelines.35,56,62 The assessment of the risk of bias in each study reporting data on excellent functional outcome (mRS 0–1 at 90 days; outcome allocated with the highest priority in our guideline manuscript) was summarised in a risk of bias chart (Supplemental Figure 1). The validity of the reported analyses was independently evaluated by all MWG members. 7. The results of data analysis were imported into the GRADEpro Guideline Development Tool (McMaster University, 2015; developed by Evidence Prime, Inc.). For each PICO question and each outcome, the risk of bias was assessed and quality of evidence rated as high, moderate, low or very low based on the type of available evidence [randomised or non-randomised studies (interventional with experimental design and non-interventional)] and considerations on inconsistency of results, indirectness of evidence, imprecision of results and risk of bias.53,54 GRADE evidence profiles/summary of findings tables were generated using GRADEpro. 8. Each PICO question was addressed separately in distinct sections. First, ‘Analysis of current evidence’ summarised current methodological considerations followed by a summary and discussion of the results of the identified randomised and non-randomised studies. Second, ‘Additional information’ was added when more details on the studies referred to in the first section were needed to provide information on key subgroup analyses of the included studies, on ongoing or future randomised-controlled clinical trials (RCTs) and potential implications on the organisation of MSU in healthcare systems. Third, an ‘Evidence-based Recommendation’ was provided, based on the GRADE methodology. The MWG has unanimously agreed to provide only one combined recommendation as at the time of MSU involvement in the patient’s assessment and treatment, the final diagnosis is unclear and, therefore, the MSU concept cannot be applied to patients with a specific diagnosis only. The MWG developed this decision in a group meeting after identifying that a single recommendation for patients with AIS would not consider modes of operation of an ambulance. The combined recommendation can be found at the end of the result section. The direction, strength and formulation of the recommendation was determined according to the GRADE evidence profiles and the ESO-SOP.53,54 The recommendation does not apply to planned or ongoing trials. Finally, according to the second ESO standard operating procedure
53
, Expert Consensus Statements were added whenever the guideline group considered that there was insufficient evidence available to provide evidence-based recommendations where practical guidance is needed for routine clinical practice. In that case, a pragmatic suggestion was provided, with the results of the votes of all MWG members presented in the supplemental material of this manuscript. Importantly, the suggestions provided in this paragraph should not be mistaken as evidence-based recommendations but rather as the opinion of the MWG members. The numerical results of the votes are provided in the Supplement (Supplemental Table 2). 9. The Guideline document was subsequently reviewed several times by all MWG members and revised until a consensus was reached. Finally, the Guideline document was reviewed and approved by external reviewers and members of the ESO Guideline Board and Executive Committee.
Results
PICO 1
In patients with suspected acute stroke, does prehospital management with a Mobile Stroke Unit (MSU) compared to conventional management improve clinical outcome?
Analysis of current evidence
GRADE evidence profile for PICO 1 on suspected acute stroke.
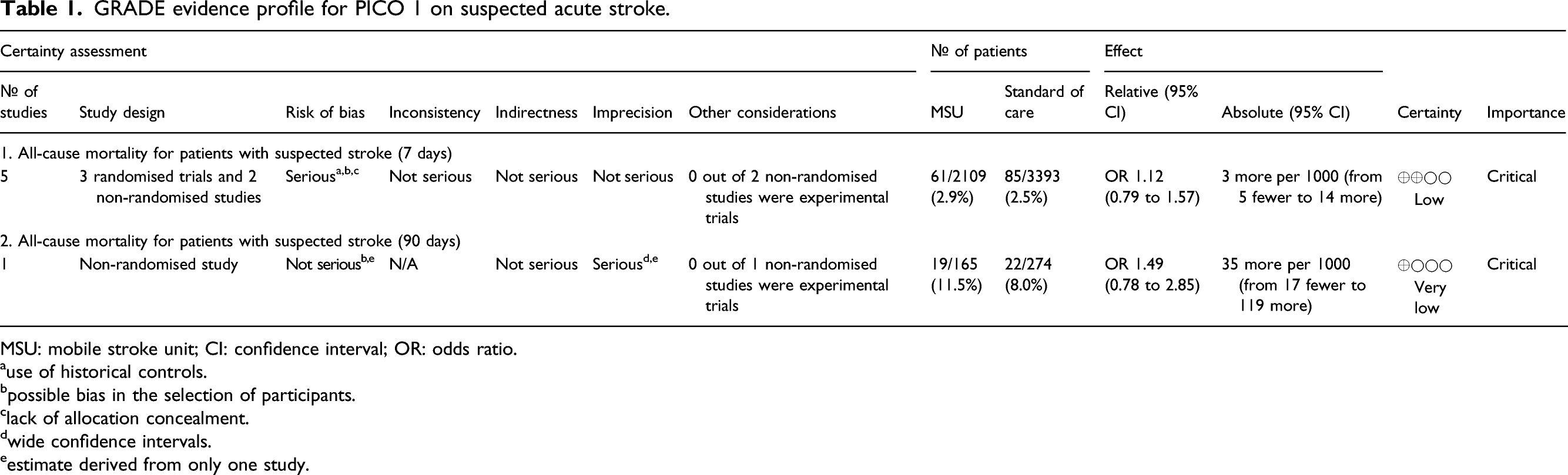
MSU: mobile stroke unit; CI: confidence interval; OR: odds ratio.
ause of historical controls.
bpossible bias in the selection of participants.
clack of allocation concealment.
dwide confidence intervals.
eestimate derived from only one study.
The first trial adding information to 7-day all-cause mortality of patients with suspected stroke was a RCT (Figure 1). The study PHANTOM-S published by Ebinger and co-authors in 2014 assigned 1804 participants to the MSU group and 2969 to conventional management. Participants were recruited between May 2011 and January 2013. The primary outcome of the trial focused on patients receiving IVT – time from emergency call-to-thrombolysis. The result showed a significant reduction of time to IVT for patients who received MSU care compared to those receiving conventional care (MSU: mean 51.8 min; 95% CI 49.0–54.6 vs control 76.3 min, 95% CI 73.2–79.3, p < 0.001).
42
Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with 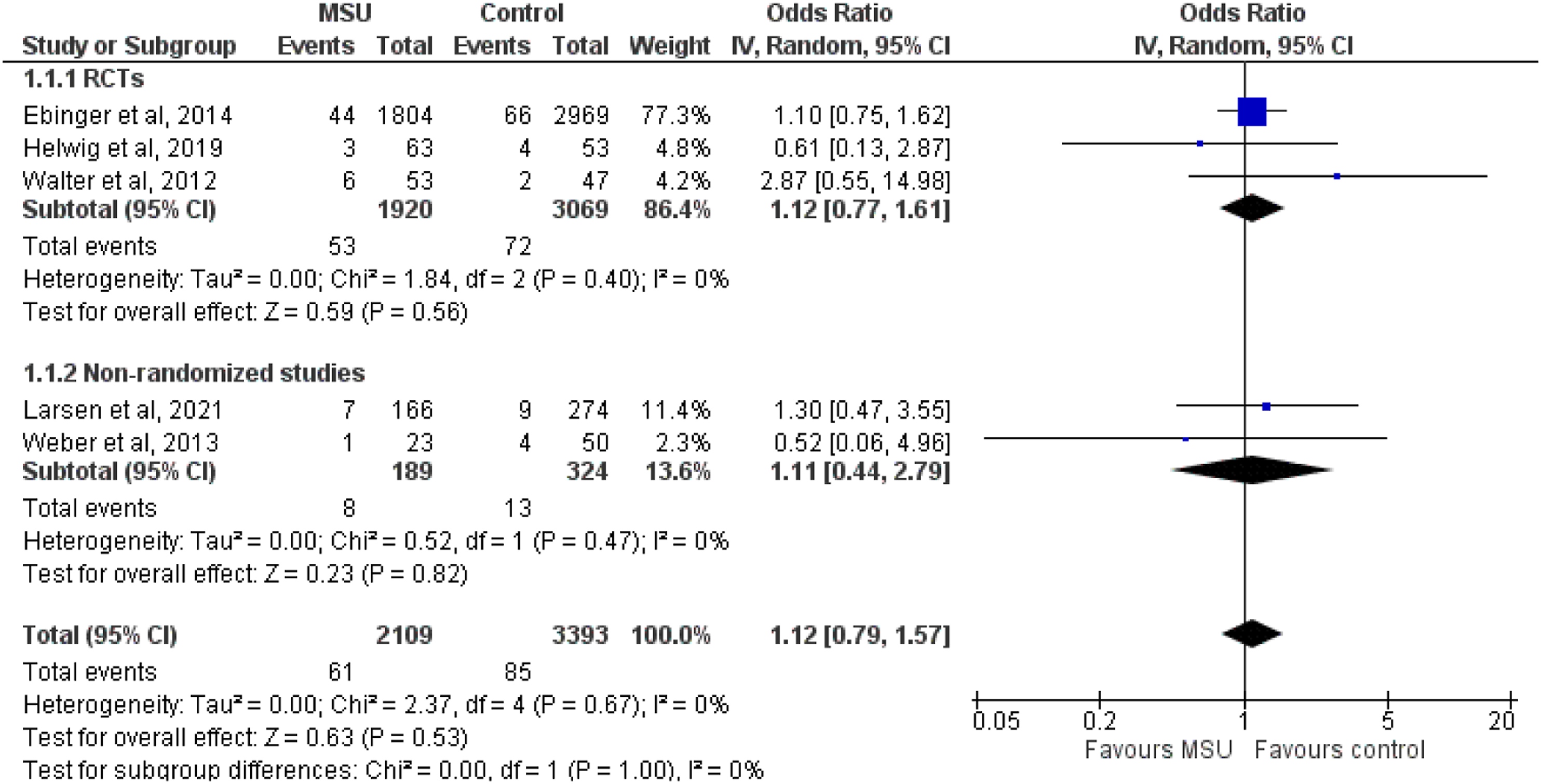
The second study performed by Helwig and colleagues in 2019 was a RCT with 63 participants receiving MSU management and 53 participants in the control group. The trial recruited patients between June 2015 and November 2017. The primary endpoint was the proportion of patients accurately triaged to either a comprehensive stroke centre (pre-specified for all LVO and ICH patients) or primary stroke centre (all others). The result showed a significant difference for both groups with correct triage for 100% of the MSU patients and 69.8% of the control patients (difference: 30.2%; 95% CI: 17.8%–42.5%; p < 0.001). 46 In the third RCT, published by Walter et al., in 2012, 53 participants were assigned to the MSU group and 47 to the conventional management group with a primary outcome parameter of emergency call to therapy decision. This trial recruited patients between November 2008 and July 2011. The result showed a significantly shorter time to therapy decision for patients treated by a MSU (median: MSU: 35 min (IQR 31–39) vs control 76 min (IQR 63–94), p < 0.0001). 41 All three RCTs were performed in Germany at two different centres.
The first non-randomised study published by Larsen and collaborators in 2021 recruited participants in Norway between May 2017 and March 2020. 51 One hundred sixty-six MSU patients were compared to 274 control patients. This study was the only providing information on 90-day all-cause mortality of suspected stroke patients. Importantly, the MSU ambulance used in this trial was the only MSU not staffed with a stroke specialist team. The MSU personnel consisted of anaesthetists trained in prehospital critical care with a 2-day CT brain scan analysis course and all personnel (doctors and paramedics) performed a 2-day stroke assessment course and NIHSS certification. Vascular Neurologists provided support via telemedicine. The primary endpoint of the study was the symptom onset to IVT treatment time. The result showed a significant time reduction for patients treated with a MSU (median: MSU 101 min (IQR 71–155) vs control care 118 min (IQR 90–176; p = 0.007). The second non-randomised study performed by Weber et al. 2013 adding data to 7-day all-cause mortality analysed 23 participants assigned to MSU management and 50 assigned to control pathway. The study was conducted in Germany and MSU patients were recruited between February and April 2011 and compared to standard care patients from 2010. The study was the pilot study to the PHANTOM-S trial by Ebinger and co-authors 42 and focussed on feasibility and safety of prehospital stroke management and time metrics to IVT. The result showed a mean call-to-needle time of 62 min, which compared favourably to 98 min of the control patients. No safety concern or relevant technical failures could be detected. 63
The random-effect meta-analysis revealed that there was no association between MSU (vs conventional management) and 7-day (OR: 1.12; 95% CI: 0.79–1.57; I2 = 0%; Figure 1) or 90-day (OR: 1.49; 95% CI: 0.78–2.85; Figure 2) mortality. There was no data available data to assess the impact of MSU for the remaining 3 selected outcomes (symptomatic intracranial haemorrhage, proportion of stroke mimics treated with IVT, major extracranial bleeding). However, information on the number of stroke mimics receiving IVT among all IVT-treated patients was available and results are described in PICO 2. Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with 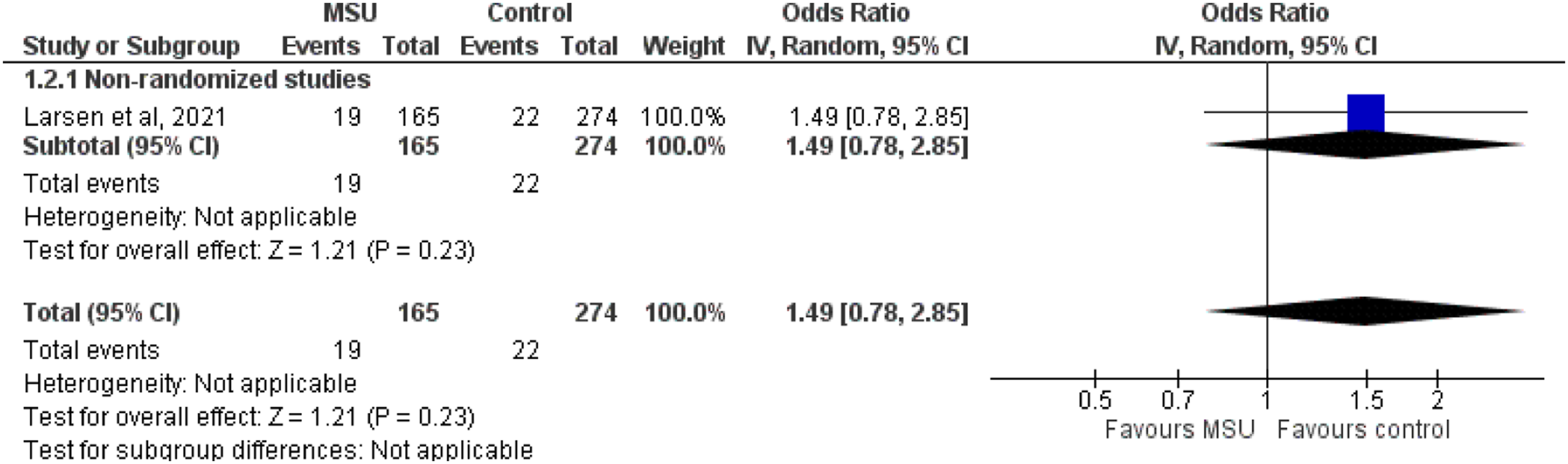
Table 1 provides details regarding the impact of MSU versus conventional management on 7-day and 90-day mortality in patients with suspected stroke.
PICO 2
In patients with confirmed AIS, does prehospital management with a MSU compared to conventional management improve clinical outcome?
Analysis of current evidence
GRADE evidence efficacy profile for PICO 2 (functional outcomes of AIS patients at 90 days).
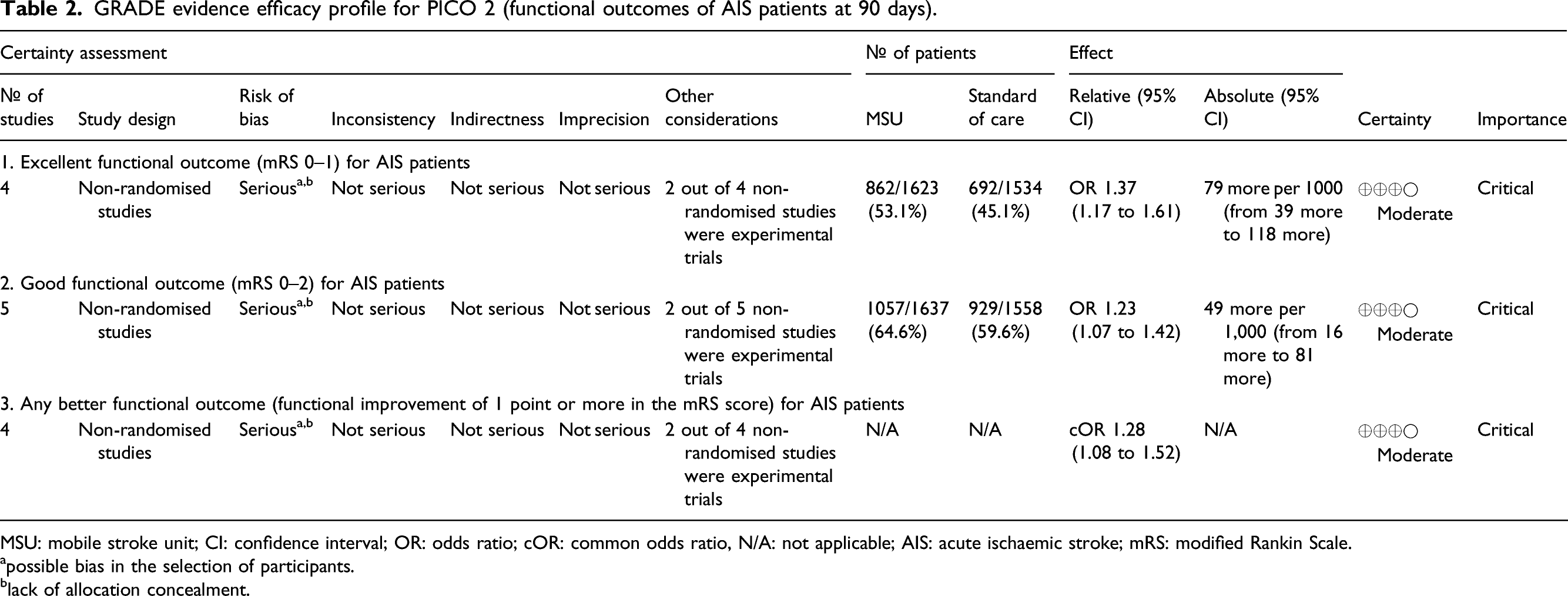
MSU: mobile stroke unit; CI: confidence interval; OR: odds ratio; cOR: common odds ratio, N/A: not applicable; AIS: acute ischaemic stroke; mRS: modified Rankin Scale.
apossible bias in the selection of participants.
black of allocation concealment.
GRADE evidence efficacy profile for PICO 2 (time metrics of intravenous thrombolysis, proportion of patients receiving intravenous thrombolysis and proportion of patients thrombolysed within the golden hour).
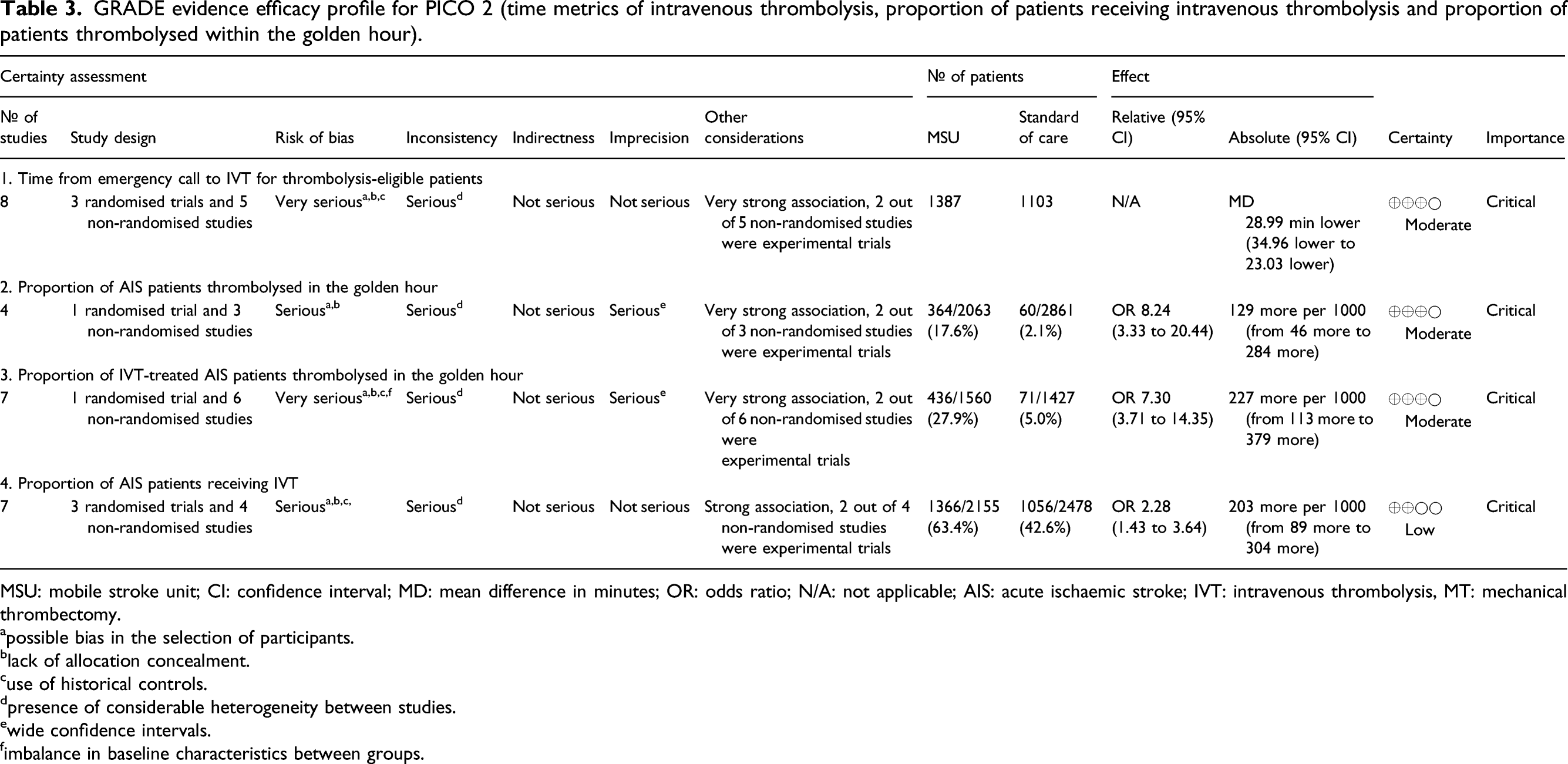
MSU: mobile stroke unit; CI: confidence interval; MD: mean difference in minutes; OR: odds ratio; N/A: not applicable; AIS: acute ischaemic stroke; IVT: intravenous thrombolysis, MT: mechanical thrombectomy.
apossible bias in the selection of participants.
black of allocation concealment.
cuse of historical controls.
dpresence of considerable heterogeneity between studies.
ewide confidence intervals.
fimbalance in baseline characteristics between groups.
GRADE evidence efficacy profile for PICO 2 (time metrics of mechanical thrombectomy, proportion of large vessel occlusion patients receiving mechanical thrombectomy and being primarily transported to tertiary stroke centres).
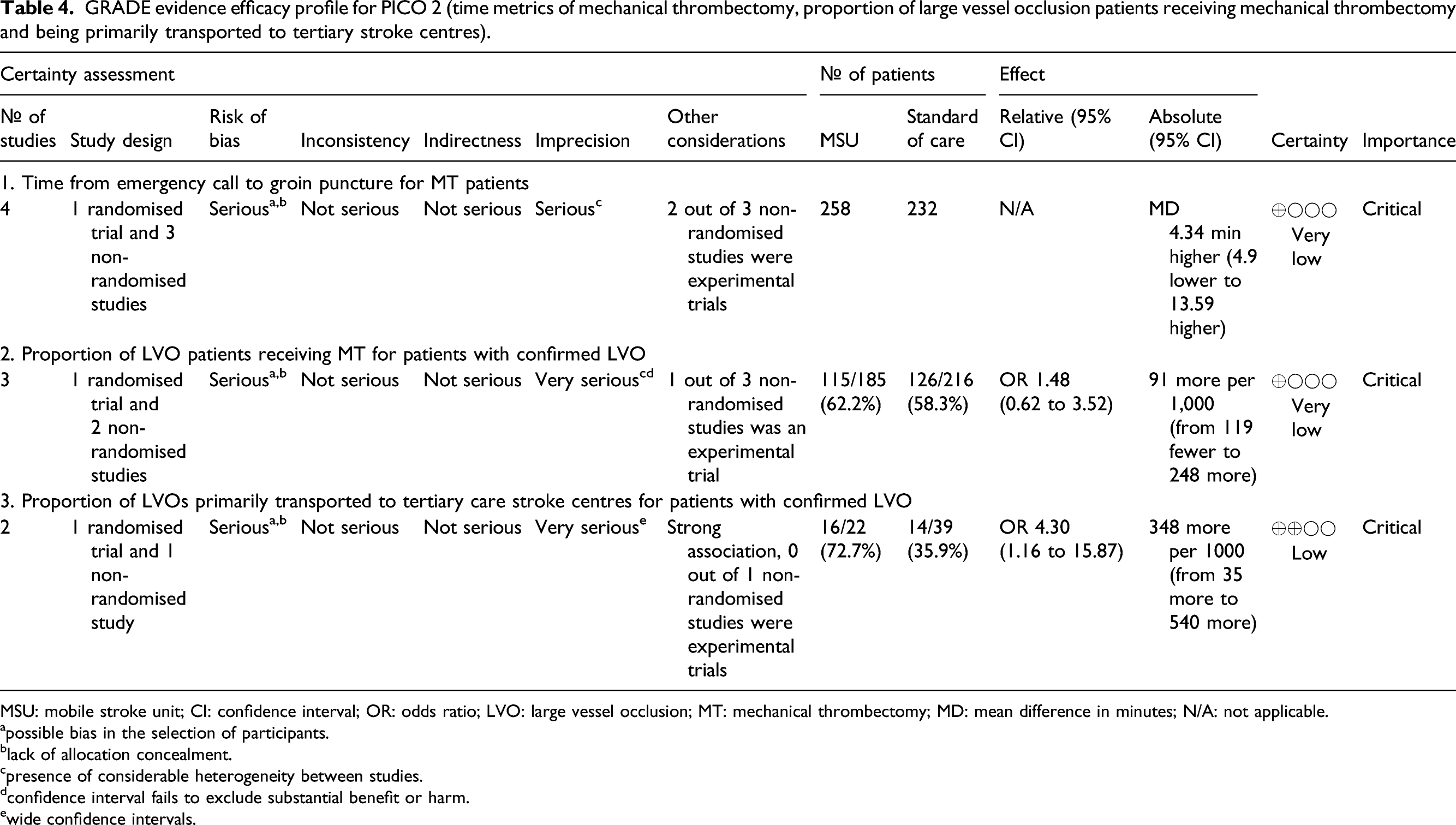
MSU: mobile stroke unit; CI: confidence interval; OR: odds ratio; LVO: large vessel occlusion; MT: mechanical thrombectomy; MD: mean difference in minutes; N/A: not applicable.
apossible bias in the selection of participants.
black of allocation concealment.
cpresence of considerable heterogeneity between studies.
dconfidence interval fails to exclude substantial benefit or harm.
ewide confidence intervals.
GRADE evidence safety profile for PICO 2 (all-cause mortality for patients with AIS).
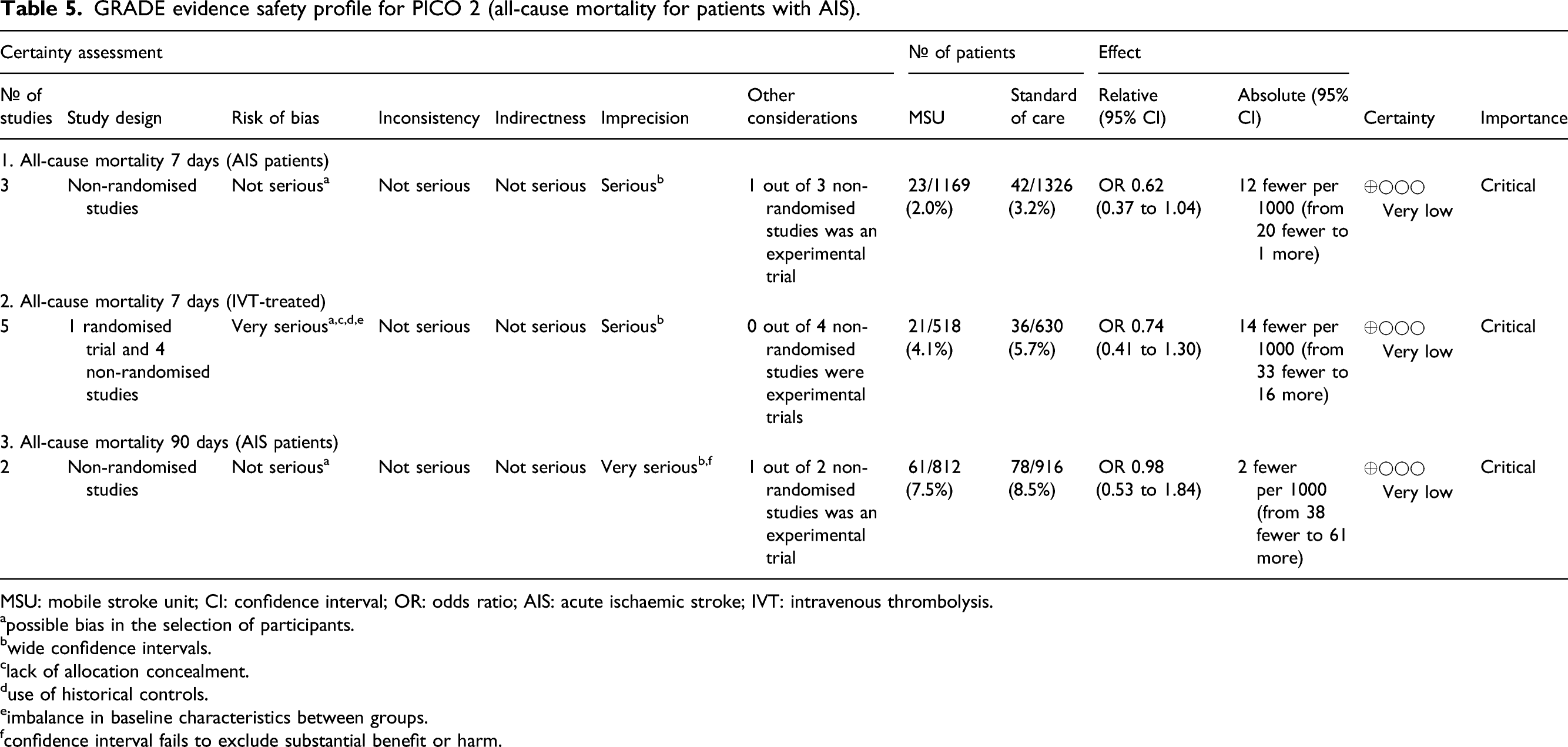
MSU: mobile stroke unit; CI: confidence interval; OR: odds ratio; AIS: acute ischaemic stroke; IVT: intravenous thrombolysis.
apossible bias in the selection of participants.
bwide confidence intervals.
clack of allocation concealment.
duse of historical controls.
eimbalance in baseline characteristics between groups.
fconfidence interval fails to exclude substantial benefit or harm.
GRADE evidence safety profile for PICO 2 (bleeding complications and proportion of stroke mimics receiving intravenous thrombolysis among acute ischaemic stroke patients).
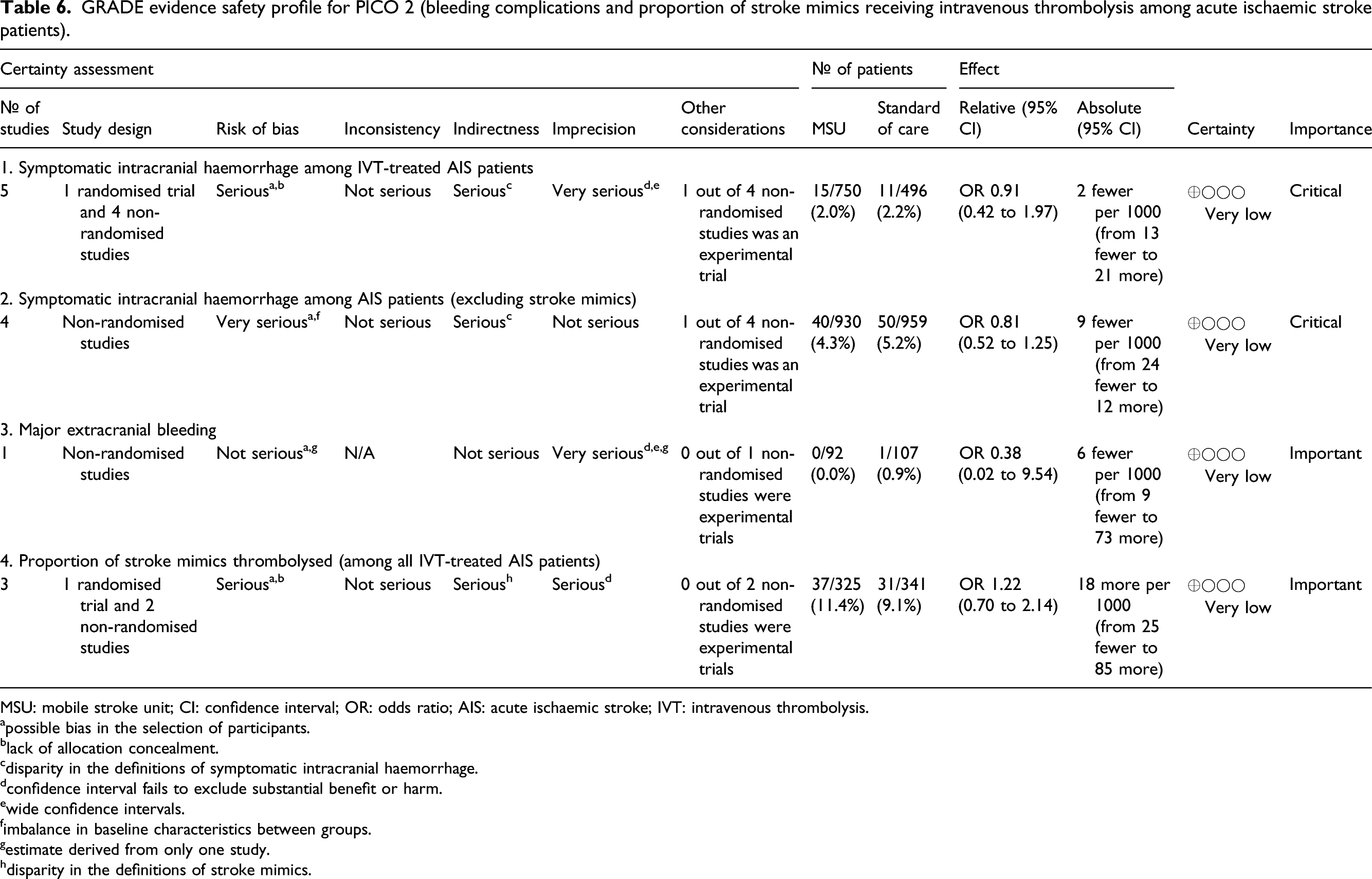
MSU: mobile stroke unit; CI: confidence interval; OR: odds ratio; AIS: acute ischaemic stroke; IVT: intravenous thrombolysis.
apossible bias in the selection of participants.
black of allocation concealment.
cdisparity in the definitions of symptomatic intracranial haemorrhage.
dconfidence interval fails to exclude substantial benefit or harm.
ewide confidence intervals.
fimbalance in baseline characteristics between groups.
gestimate derived from only one study.
hdisparity in the definitions of stroke mimics.
GRADE evidence efficacy profile of the sensitivity analysis for PICO 2 (functional outcomes of AIS patients at 90 days).
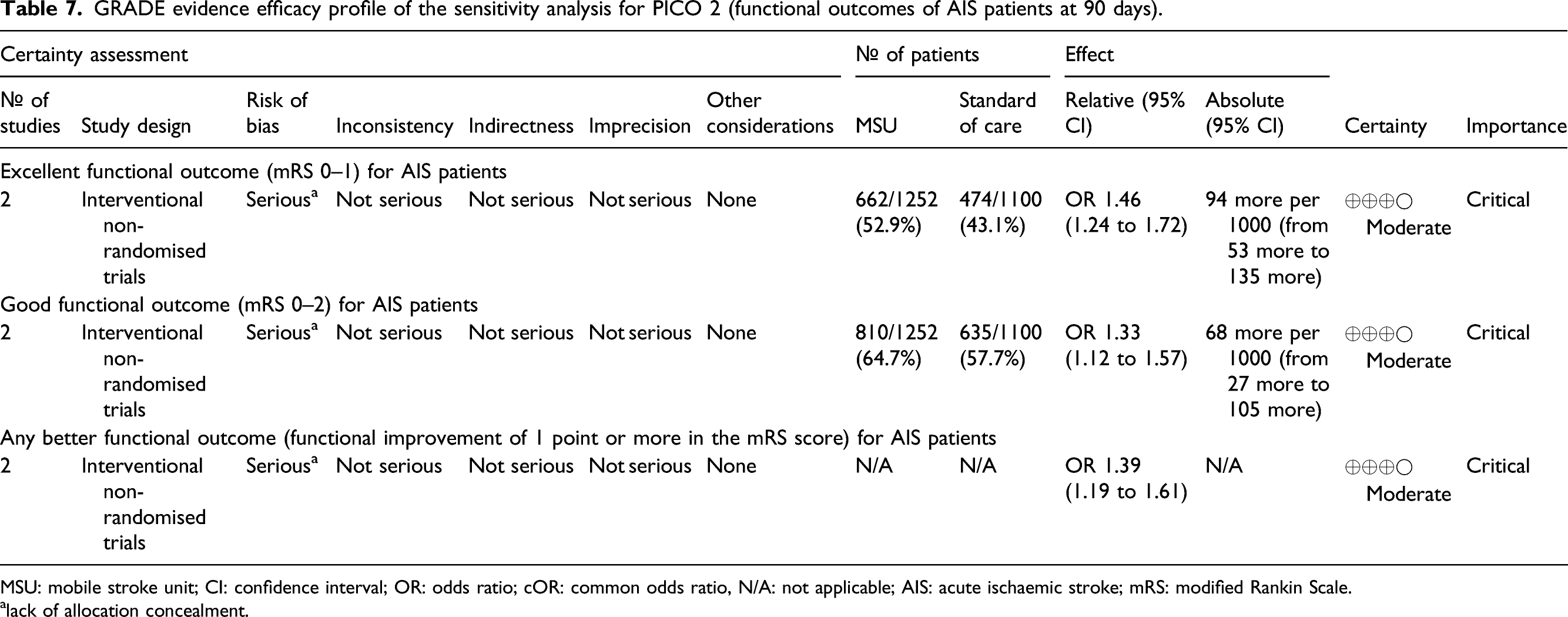
MSU: mobile stroke unit; CI: confidence interval; OR: odds ratio; cOR: common odds ratio, N/A: not applicable; AIS: acute ischaemic stroke; mRS: modified Rankin Scale.
alack of allocation concealment.
All RCTs were performed by two different centres in Germany. The RCT published by Ebinger and collaborators in 2014 (PHANTOM-S RCT, details described in PICO 1) recruited 614 participants with confirmed AIS to the MSU group and 1041 AIS patients to conventional management. 42 There was a second publication from the PHANTOM-S RCT that reported the findings of a substudy with random assignment of 614 AIS participants to the MSU pathway and 1497 to conventional management. This substudy aimed to identify the benefits of golden hour thrombolysis in patients with confirmed ischaemic stroke. The results showed a 6-fold increase in golden hour IVT (MSU: 31.0% vs control 4.9%; p < 0.01). 43
The RCT published by Helwig and collaborators in 2019, which is described in detail in PICO 1, recruited 32 participants with confirmed AIS to the MSU group and 39 to the control group. 46 In 2012, Walter et al., published another RCT (details described in PICO 1), in which 29 AIS participants in the MSU group and 25 in the conventional management group were analysed. 41
The first prospective, non-randomised, interventional study, B_PROUD, published by Ebinger and collaborators in 2021 assigned 749 participants to MSU and 794 participants to the conventional pathway. 49 The study was conducted between February 2017 and October 2019 in Berlin and included patients presenting with stroke symptoms at the time of ambulance arrival and with a final hospital-based diagnosis of AIS or Transient Ischaemic Attack (TIA). The control group included patients eligible for MSU dispatch but for whom a MSU was unavailable because it was already bound to another patient or in maintenance. A total of three MSU ambulances were used for this study. Six hundred fifty-four participants of the MSU group and 683 of the control group were included in the primary efficacy analysis. The primary endpoint of the study was the mRS distribution and a 3-tier disability scale (none to moderate disability; severe disability; death) at 3 months. The results showed a significantly lower mRS in patients treated with a MSU (MSU: 1, IQR: 0–3, control 2: IQR: 0–3; common OR for worse mRS: 0.71; 95% CI: 0.58–0.86; p < 0.001) and lower disability scores (none to moderate disability: MSU: 80.3%, control: 78.0%; severe disability: MSU: 12.6%, control: 13.3%; death: MSU: 7.1%, control: 8.8%; common OR for worse functional outcome: 0.73, 95% CI: 0.54–0.99; p = 0.04). The second prospective, non-randomised, interventional study, BEST-MSU, was conducted in multiple centres in the United States of America (USA) by Grotta and collaborators, 2021 and analysed 598 IVT-eligible patients in the MSU group and 417 in the conventional management group. 50 The study was conducted between August 2014 and August 2020. The MSUs were staffed with one or two paramedics, a CT technologist, a critical care nurse and an on-board or remote vascular neurologist. To reduce bias, IVT and trial eligibility were assessed after the intervention by a blinded neurologist. Alternating MSU or standard ambulance weeks were prospectively designated to the trial period. The primary outcome of the study was the utility-weighted mRS at 90 days, which was 0.72 in the MSU group and 0.66 in the EMS group (adjusted OR for a score of ≥0.91: 2.43; 95% CI: 1.75 to 3.36; p < 0.001). 55.0% of the MSU patients and 44.4% of the control patients had a mRS score of 0–1 after 3 months. Only the studies by Ebinger et al., 2021 and Grotta et al., 2021 had an experimental design with a blinded assessment of the functional outcome mRS at 90 days as their primary outcome parameter.49,50 Both studies were included in a sensitivity analysis.
The non-randomised study by Kunz et al. analysed data from 305 MSU participants and 353 AIS patients treated with a conventional approach. Participants were recruited between February 2011 and March 2015 64 and included patients who received MSU care during the PHANTOM-S pilot study 63 and the PHANTOM-S trial 42 until January 2013 (disentangled data by H.A.). All these patients had no pre-stroke dependency and were treated with IVT. The primary outcome of this study was the proportion of patients with a mRS score of 1 or lower after 3 months, which could be detected for 53% of MSU treated vs 47% of control patients (p = 0.14). The non-randomised study by Nolte and co-authors was a parallel analysis of 122 MSU and 142 conventional management patients treated with IVT between February 2011 and March 2015, who needed assistance already before their stroke, also including subjects of the PHANTOM-S pilot study 63 and the PHANTOM-S trial 42 until January 2013. The primary endpoint was the proportion of patients with a mRS of 0–3 after 90 days. In the MSU group, 39% of the patients reached the endpoint versus 25% of the control group (p = 0.01). 65
The results published by Weber et al., 2013 came from a pilot, non-randomised study to the randomised PHANTOM-S trial and have been described in detail in PICO 1. 63 All the latter non-randomised studies included only AIS patients who received IVT and were conducted in Berlin, Germany.63,64,65
The non-randomised, study performed in New York, USA by Kummer and co-investigators, published in 2019 analysed data from 66 MSU patients, of whom 29 were AIS patients with IVT treatment and 19 control patients, of whom 9 were AIS patients treated with IVT between October 2016 and September 2017. In this study, the MSU operated in two different areas following a biweekly schedule and patients treated with standard care in the MSU ‘off’ catchment area served as control group. The primary outcome was time between ambulance dispatch to IVT, which was significantly shorter for patients receiving MSU care (mean 61.2 min) than for those with conventional care (91.6 min, p = 0.001). 66
The Norwegian non-randomised study by Larsen and collaborators reported a total of 58 patients with hospital confirmed AIS in the MSU group and 101 confirmed AIS patients in their control group and details of the study have been described in PICO 1. 51 The non-randomised study performed by Taqui and collaborators, published in 2017, was conducted between July and November 2014 in Cleveland, USA. Recruited participants were identified as code stroke dispatches by the emergency medical dispatch centre. The Cleveland MSU operated with a vascular neurologist and radiologist via remote telemedical connection to the ambulance. The overall study population consisted of 100 MSU and 53 control patients. A total of 16 participants with AIS, who were treated with IVT were analysed after MSU treatment compared to 12 with conventional management. The aim of the study was to compare key management times. The result showed a significant reduction of all time metrics for patients treated with the MSU compared to control patients with time between emergency call-to-IVT (MSU: 55.5 min vs control: 94 min, p < 0.0001) and symptom onset to IVT (MSU: 97 min vs control: 122.5 min, p = 0.0485) as most important results. 45 A Chinese non-randomised study, published in 2021 by Zhou and collaborators, analysed data of 14 MSU AIS IVT-treated patients and 24 control patients, who were recruited if treated with IVT. The study was conducted in Xingyang, Henan Province in China between November 2018 and April 2019. The primary outcome was the time between emergency call-to-IVT, which was significantly shorter for patients receiving MSU care (median, MSU: 59.5 min, IQR 42–75 vs control: 89 min, IQR 32–164, p = 0.001). 67
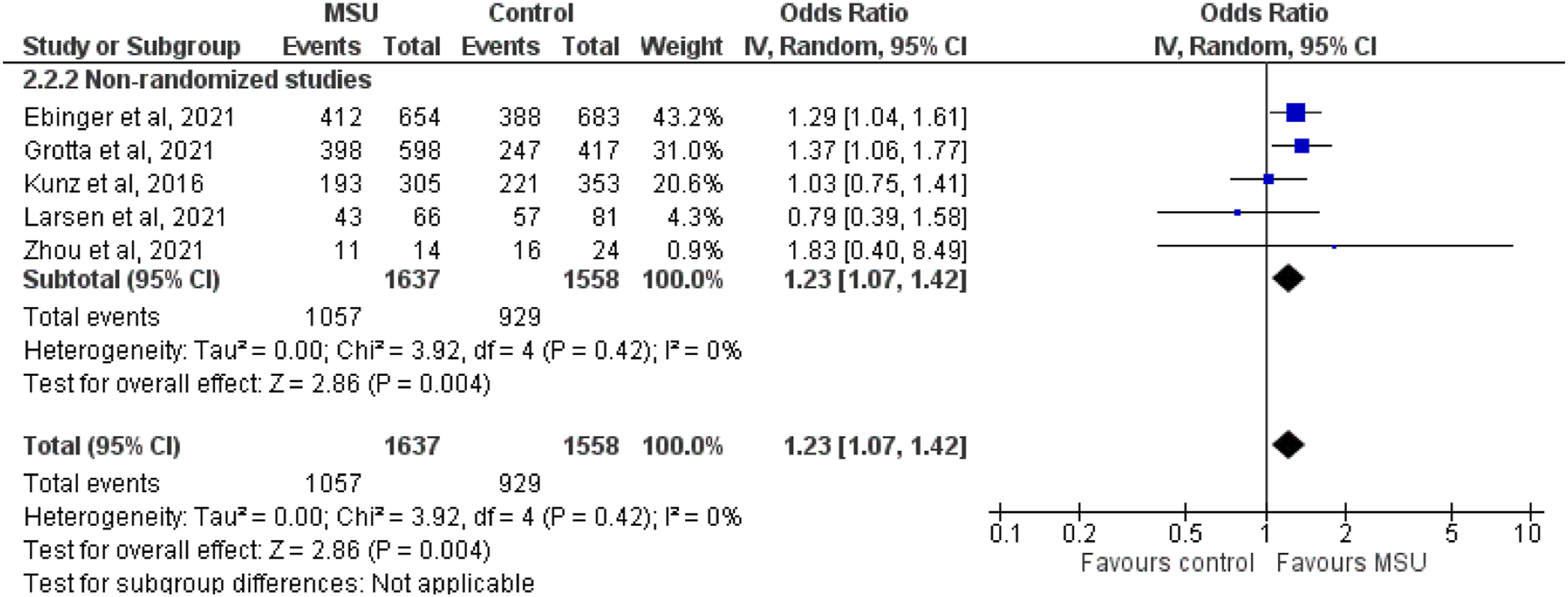
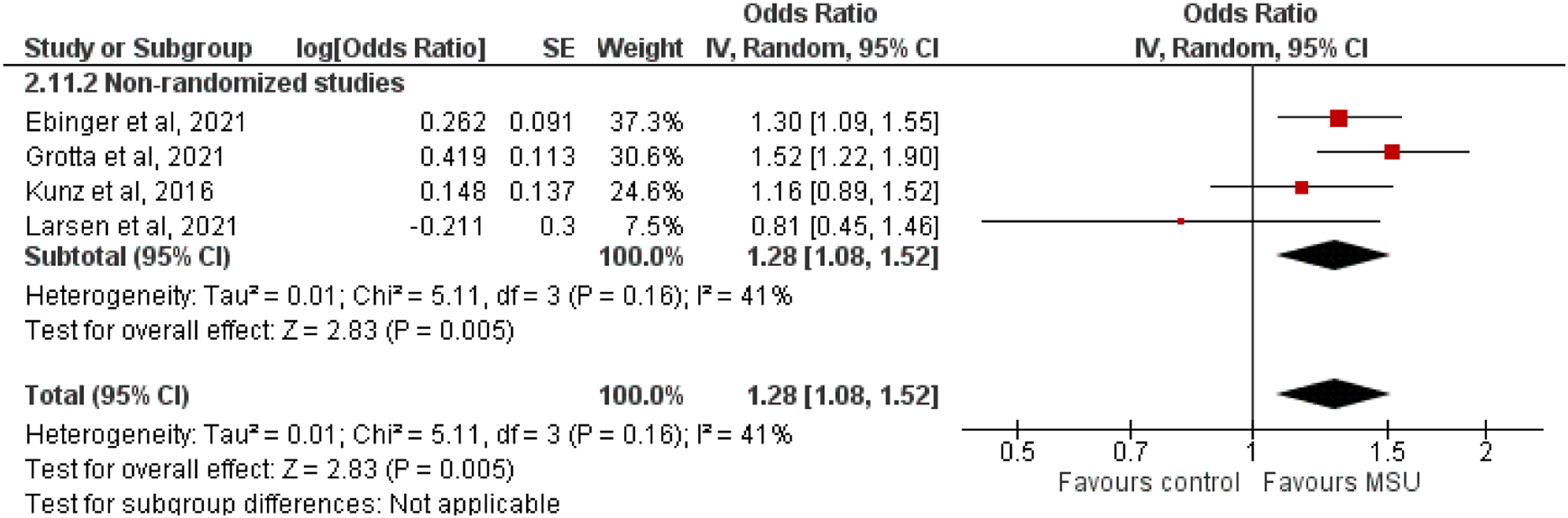
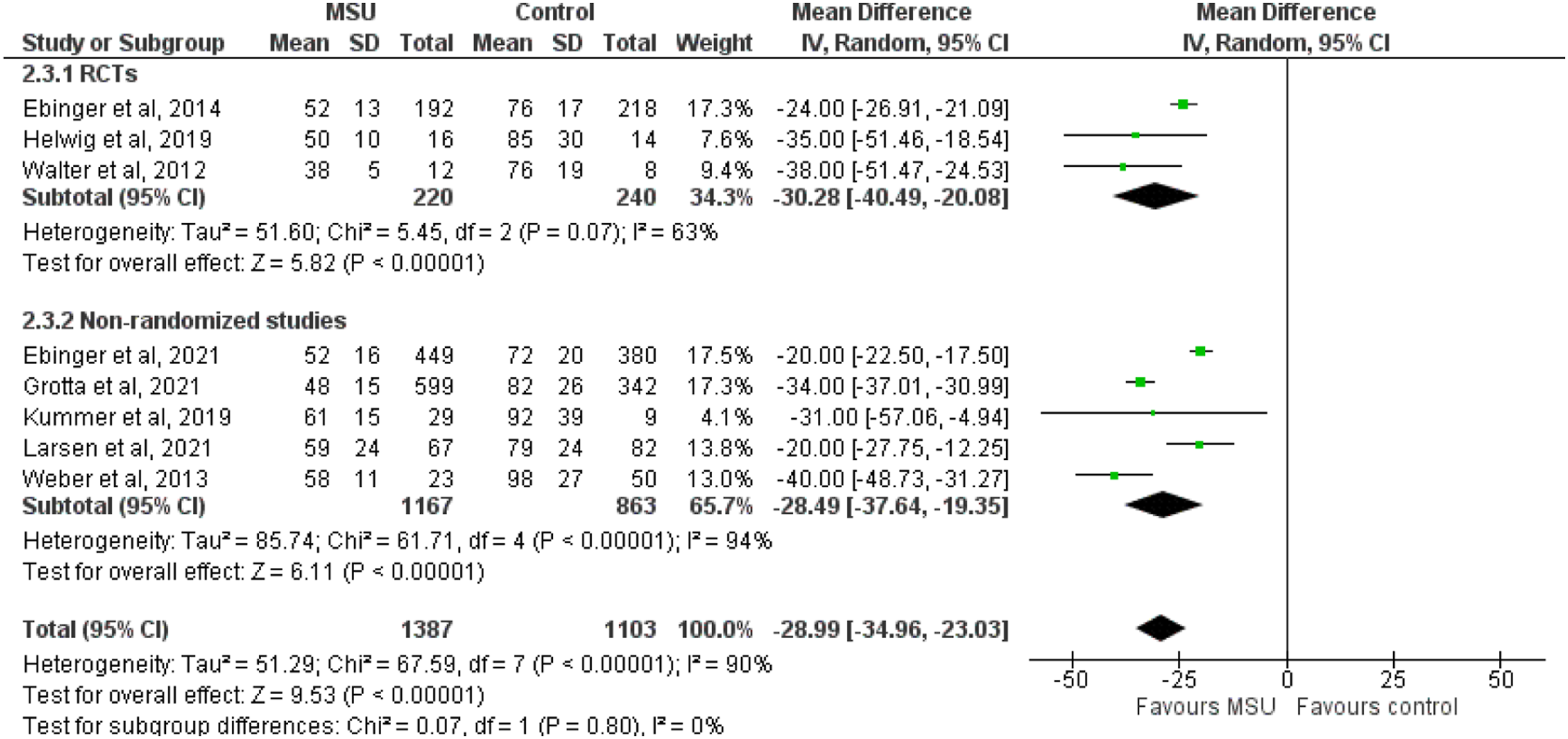
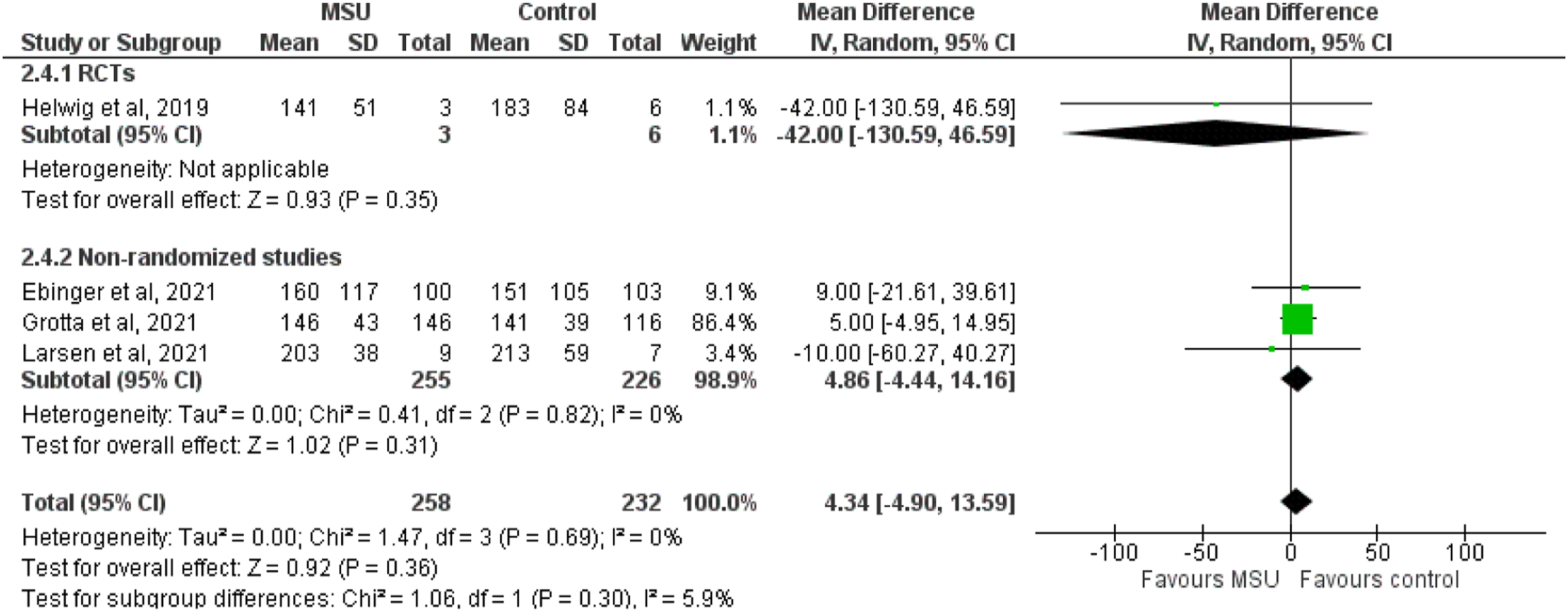
The random-effect meta-analysis revealed that MSU management compared to conventional management improved excellent (OR: 1.37; 95% CI: 1.17–1.61; I2 = 16%; Figure 3), good (OR: 1.23; 95% CI: 1.07–1.42; I2 = 0%; Figure 4) and any better (cOR: 1.28; 95% CI: 1.08–1.52; I2 = 41%; Figure 5) functional outcome in patients with AIS. MSU management was associated with a reduction in the elapsed time between stroke onset and tissue plasminogen activator bolus among AIS patients treated with IVT (pooled MD: −28.99 min; 95% CI: −34.96 to −23.03; I2 = 91%; Figure 6). There was no association between MSU management and elapsed time between symptom onset and groin puncture among AIS patients treated with MT (pooled MD: 4.34 min; 95% CI: −4.90 to 13.59; I2 = 0%; Figure 7). Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with 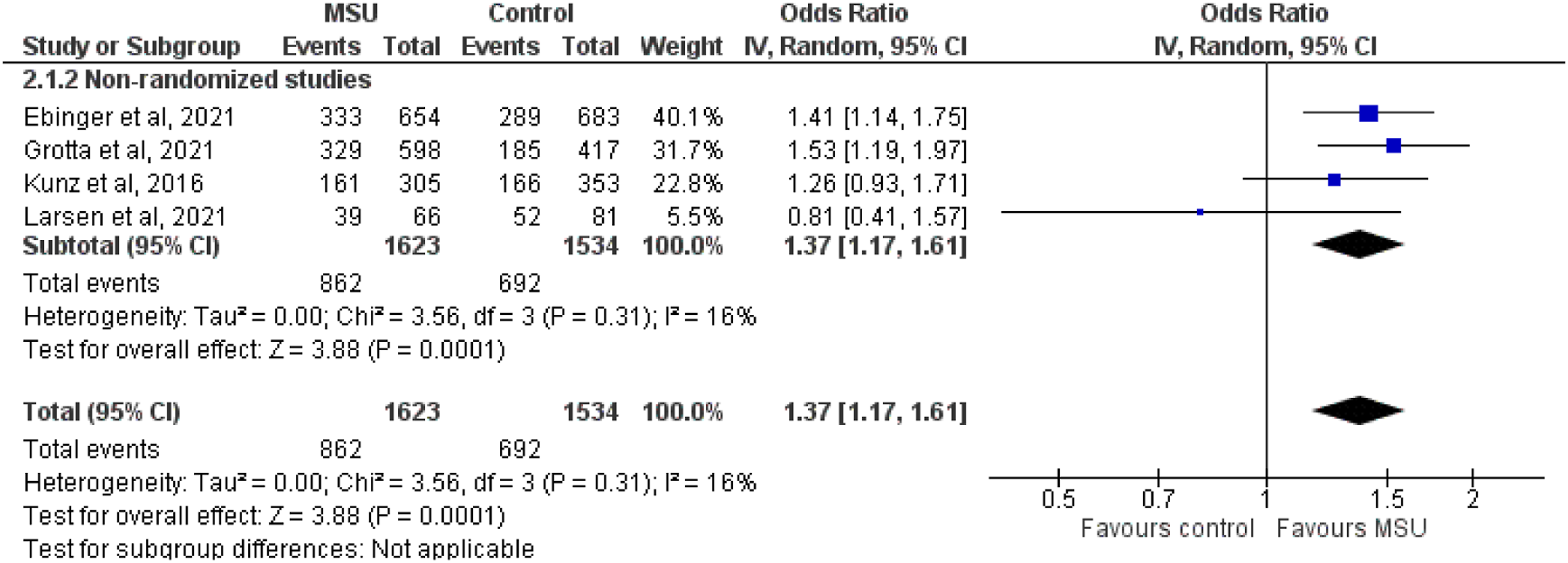
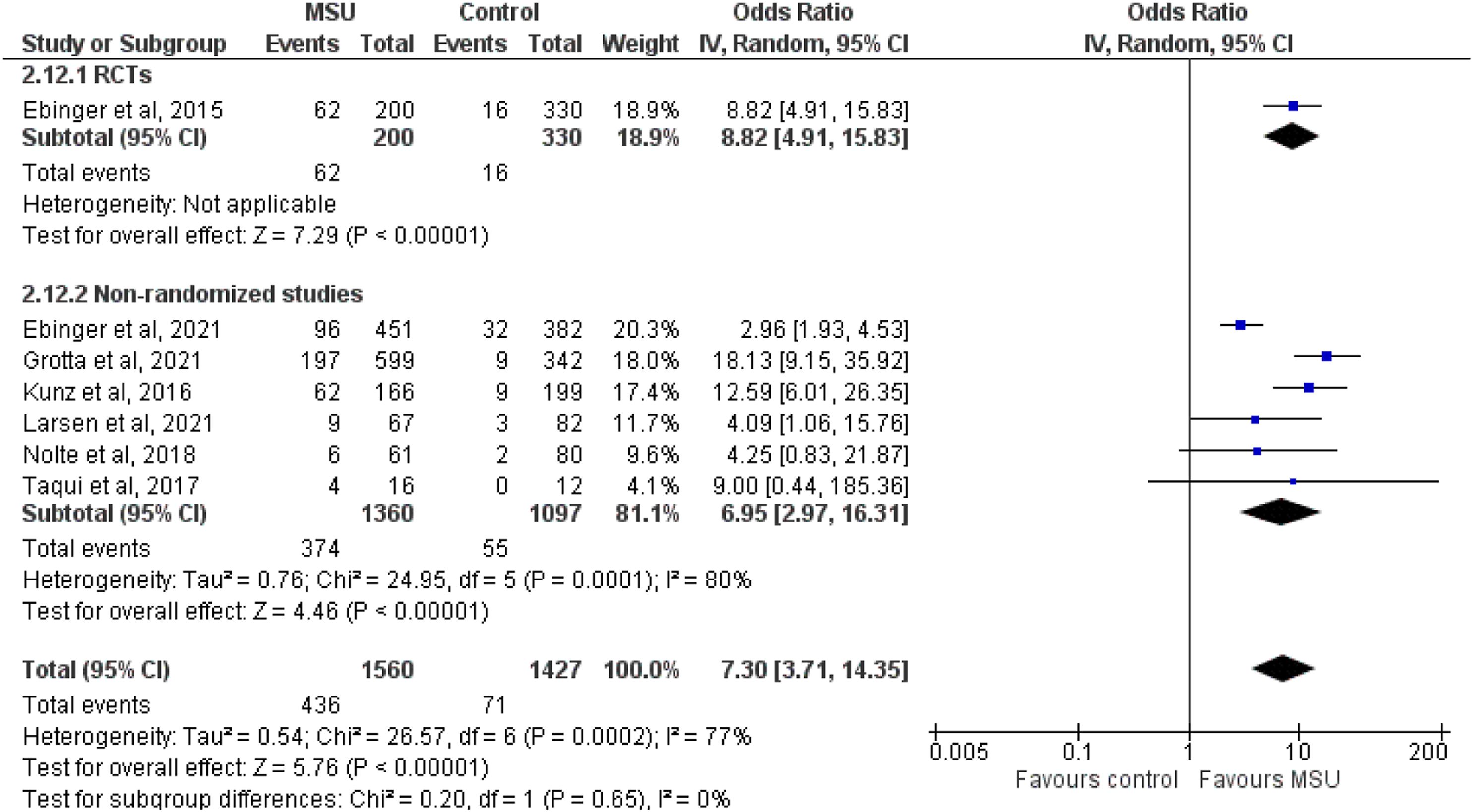
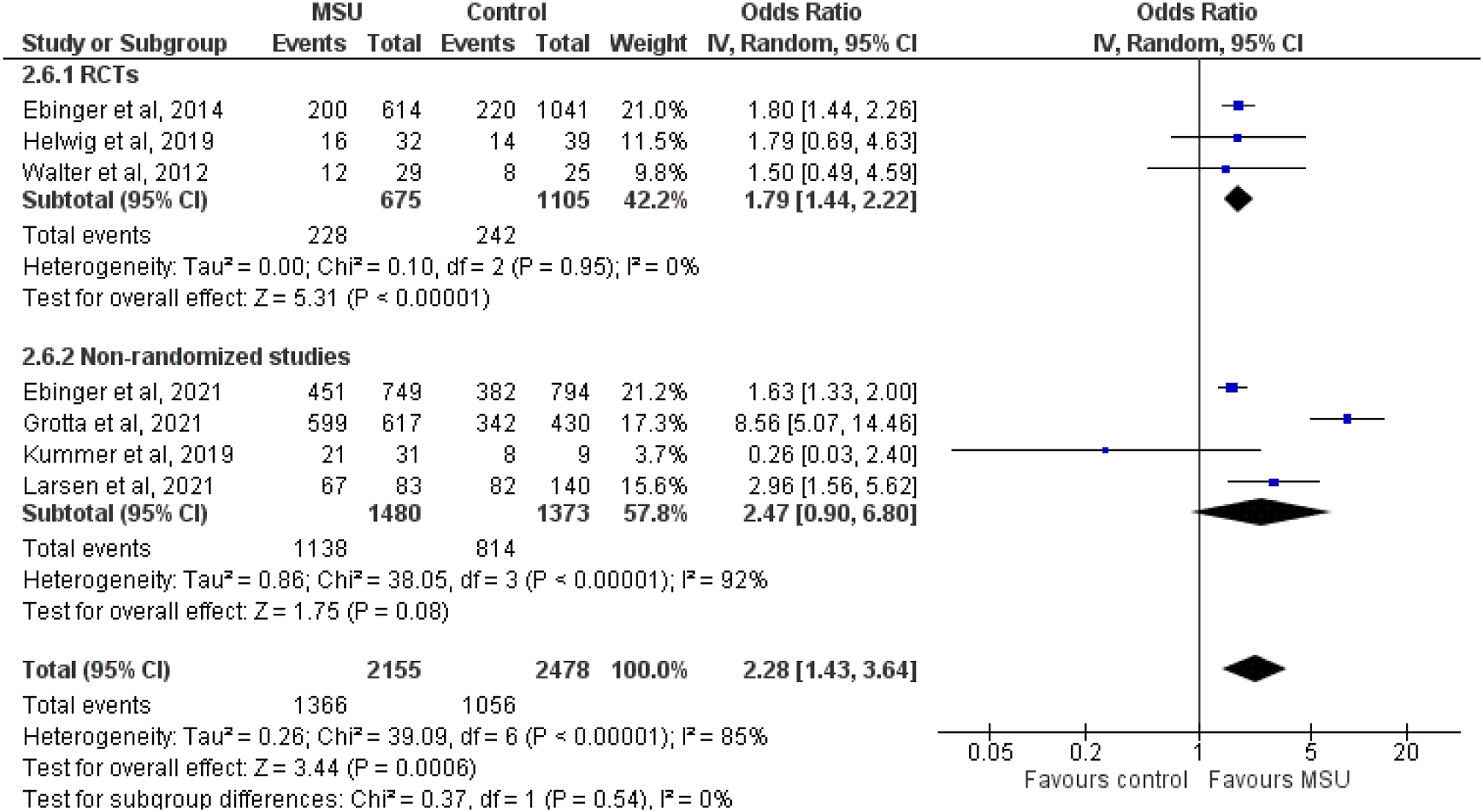
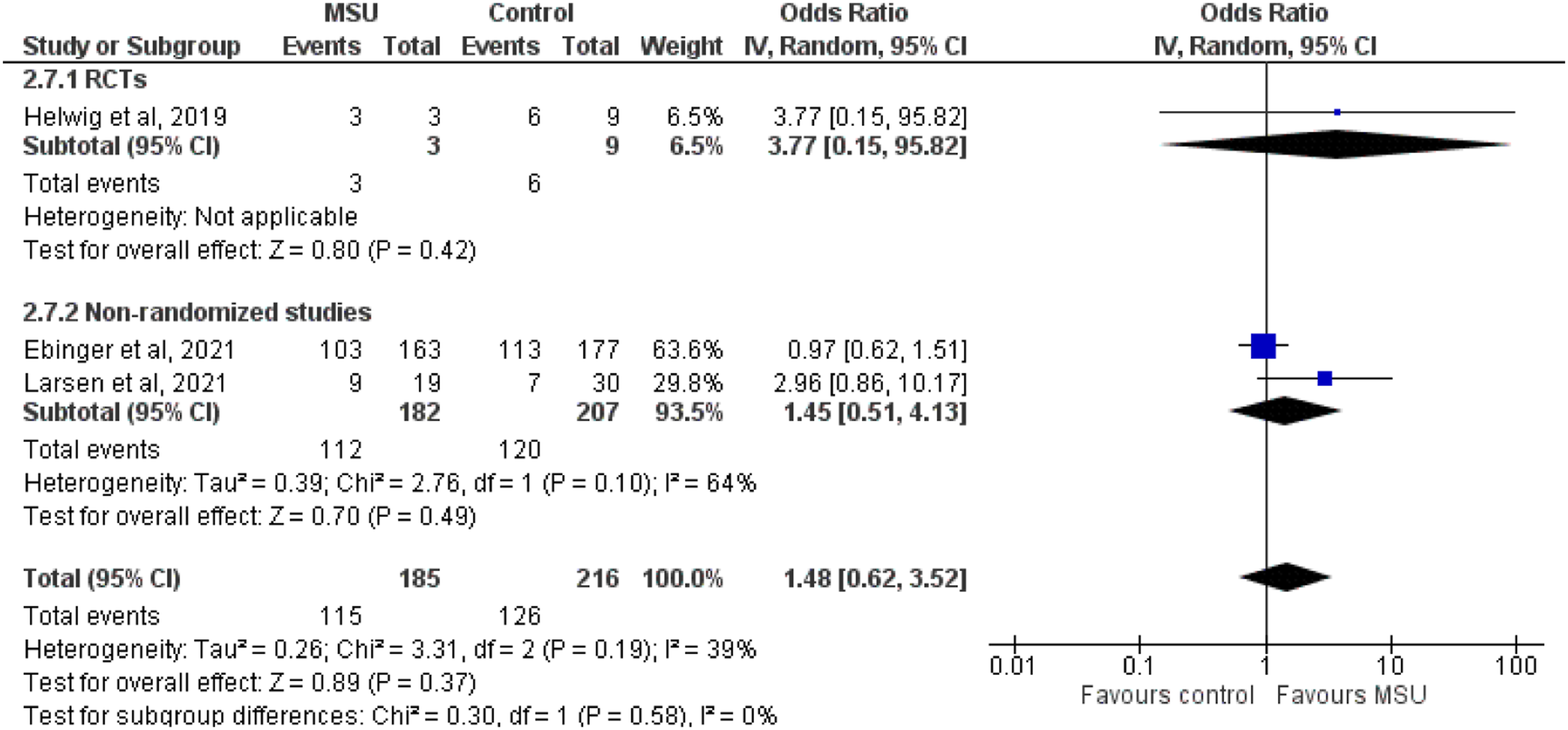
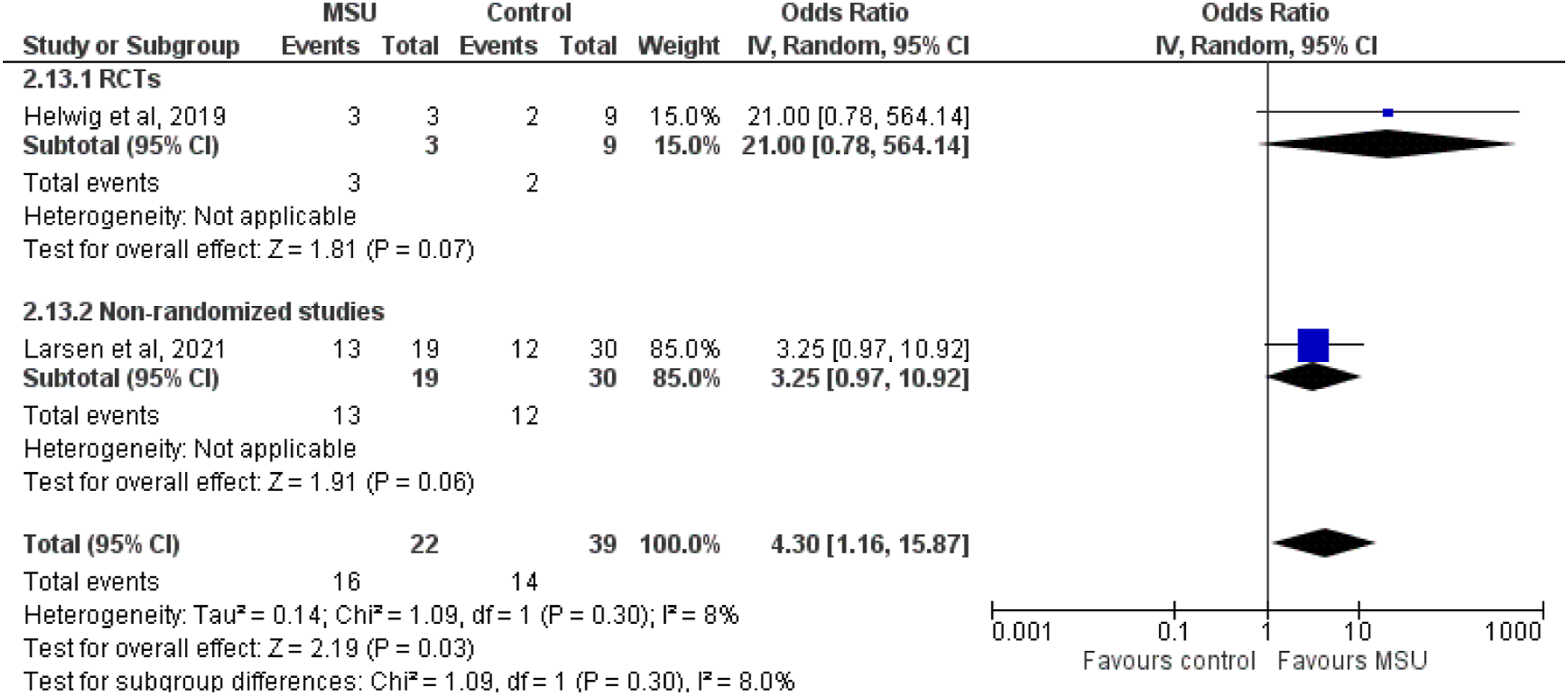
MSU management increased the rate of IVT within 60 min from symptom onset (‘golden hour’) among all AIS patients (OR: 8.24; 95% CI: 3.33–20.44; I2 = 87%; Figure 8) and among IVT-treated AIS patients (OR: 7.30; 95% CI: 3.71–14.35; I2 = 77%; Figure 9). MSU management also increased the proportion of AIS patients receiving IVT (OR: 2.28; 95% CI: 1.43–3.64; I2 = 85%; Figure 10). There was no association between MSU and the likelihood of receiving treatment with MT among all AIS patients (OR: 1.48; 95% CI: 0.62–3.52; I2 = 39%; Figure 11). MSU increased the rate of LVO patients that were primarily transported to thrombectomy-capable centres (OR: 4.30; 95% CI: 1.16–15.87; I2 = 8%; Figure 12). Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with 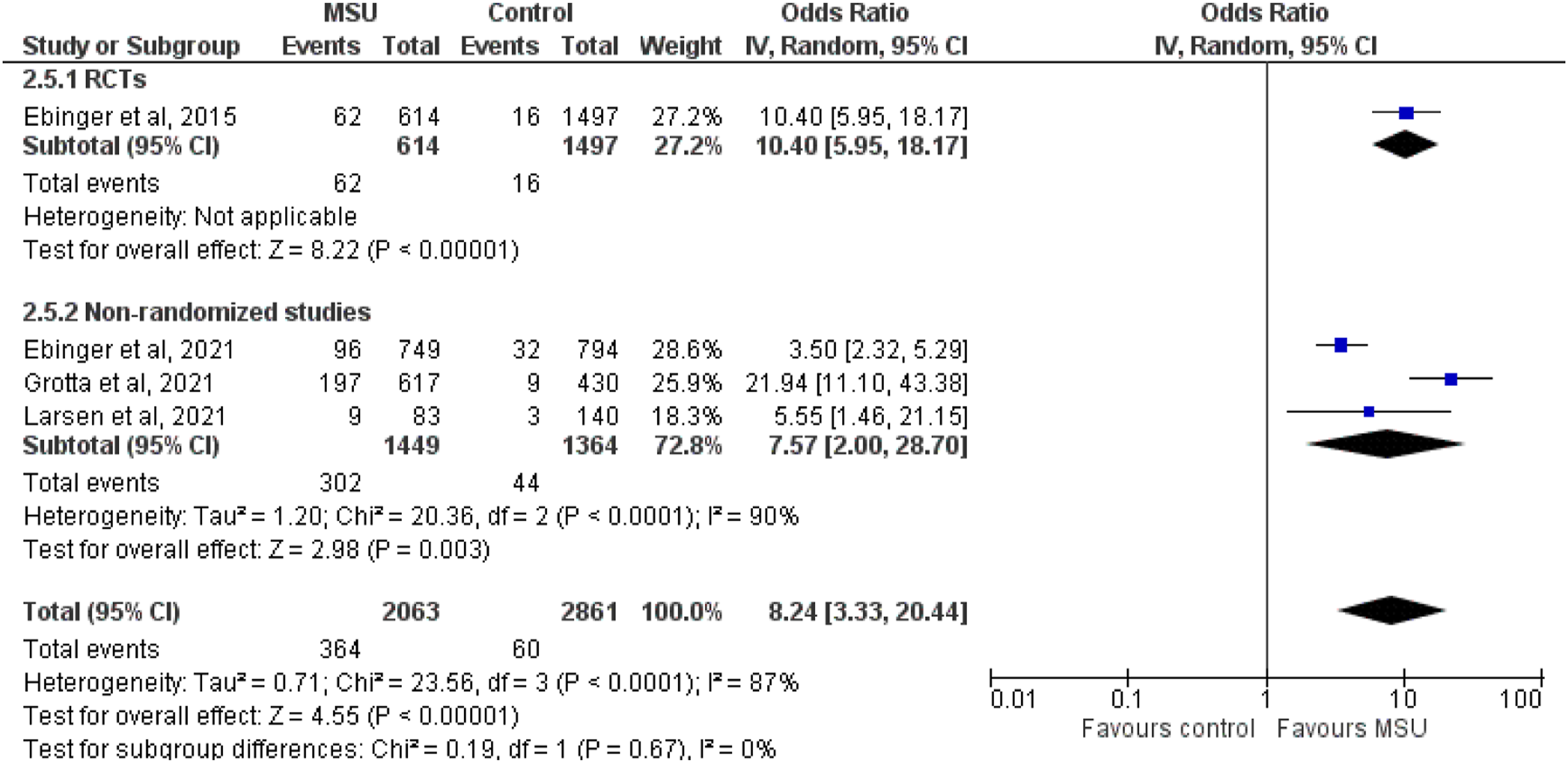
In summary, MSU compared with conventional management was associated with improved functional outcomes, swifter IVT delivery, higher rates of IVT within the golden hour, higher proportion of AIS patients receiving IVT and higher proportion of LVO patients being primarily transported to tertiary stroke centres (improvement in 8 out of 10 efficacy outcomes). MSU did not shorten the time between symptom onset to groin puncture and did not increase the rate of MT among AIS patients.
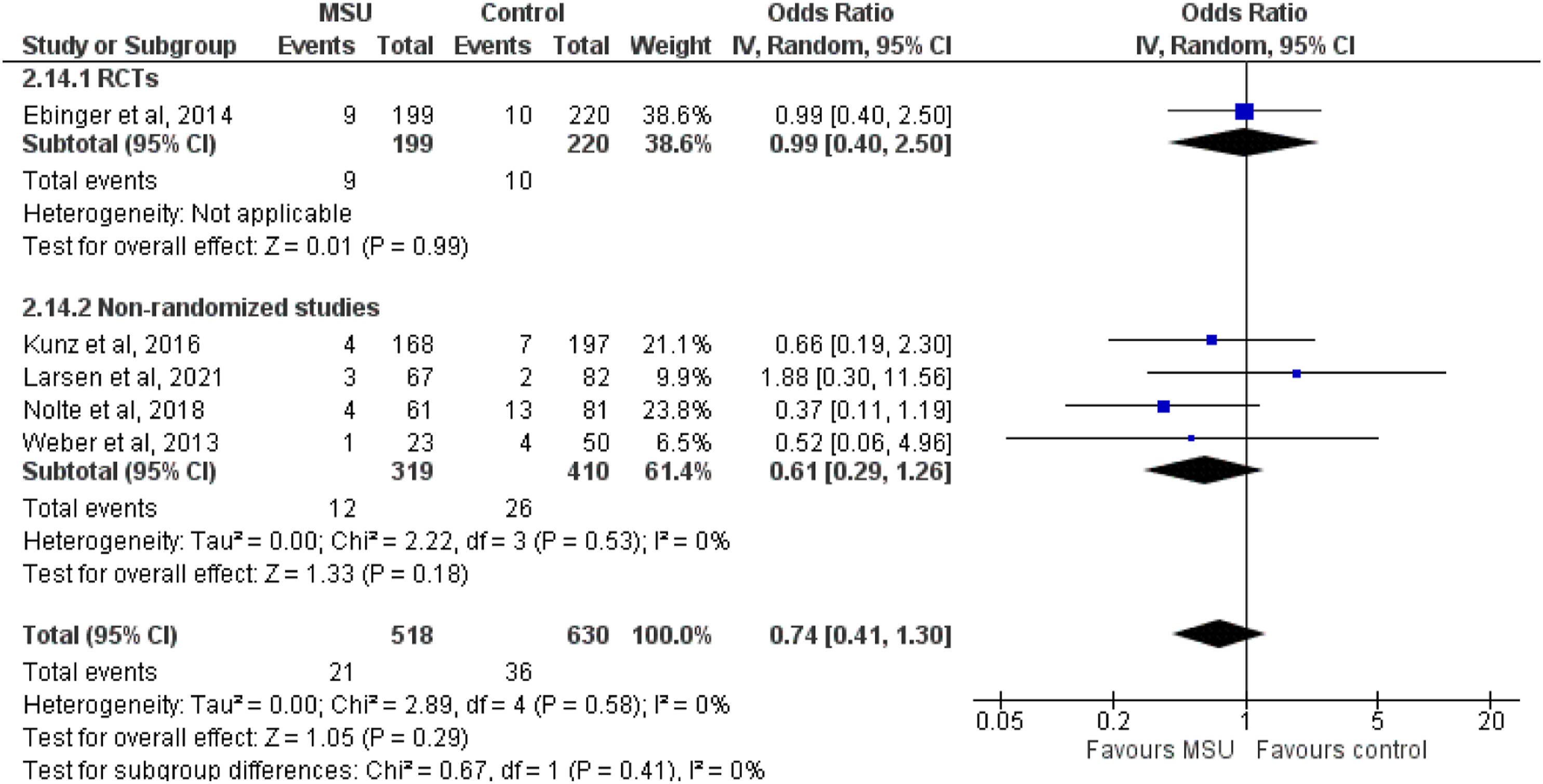
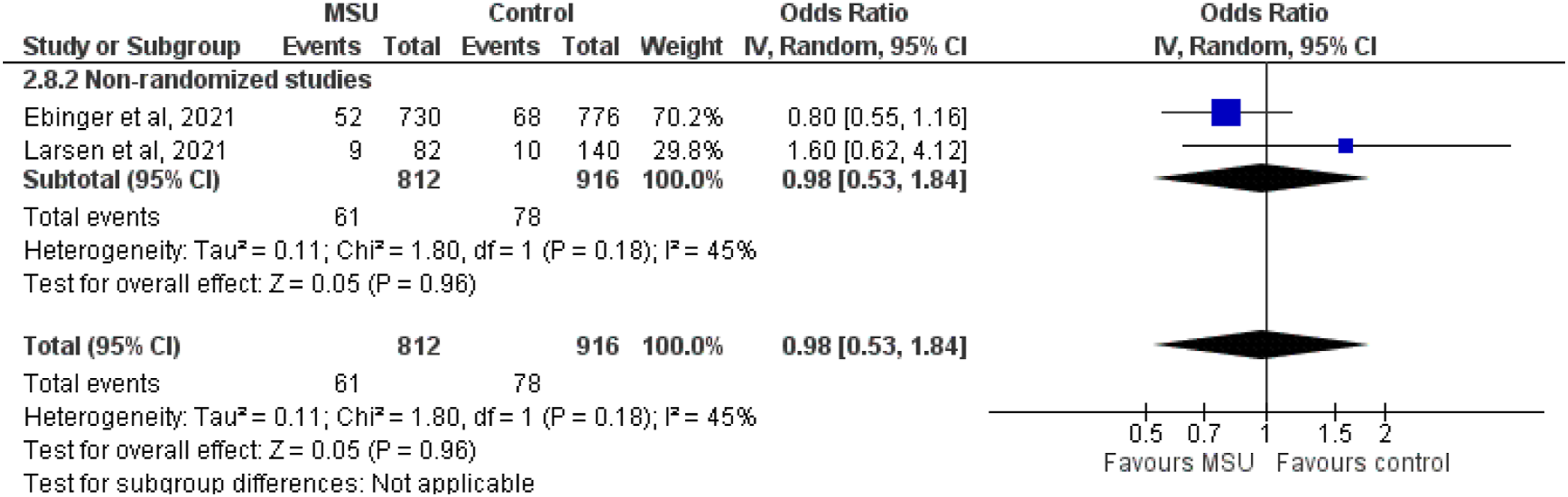
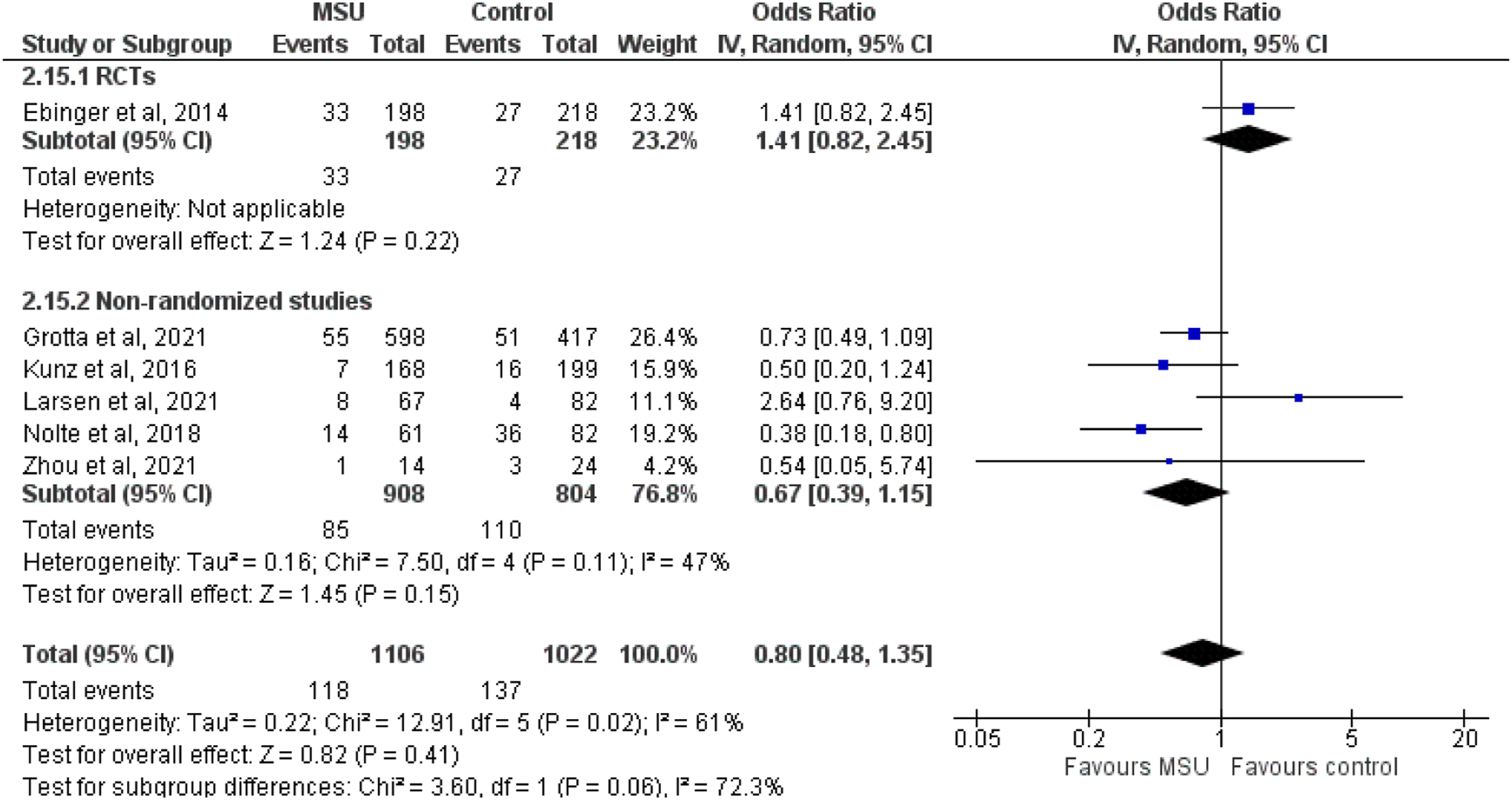
MSU was not associated with 7-day mortality among all AIS patients (OR: 0.62; 95% CI: 0.37–1.04; I2 = 0%; Figure 13) and among AIS patients treated with IVT (OR: 0.74; 95% CI: 0.41–1.30; I2 = 0%; Figure 14). There was no association of MSU with 90-day mortality among all AIS patients (OR: 0.98; 95% CI: 0.53–1.84; I2 = 45%; Figure 15) and among AIS patients treated with IVT (OR: 0.80; 95% CI: 0.48–1.35; I2 = 61%; Figure 16). Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with 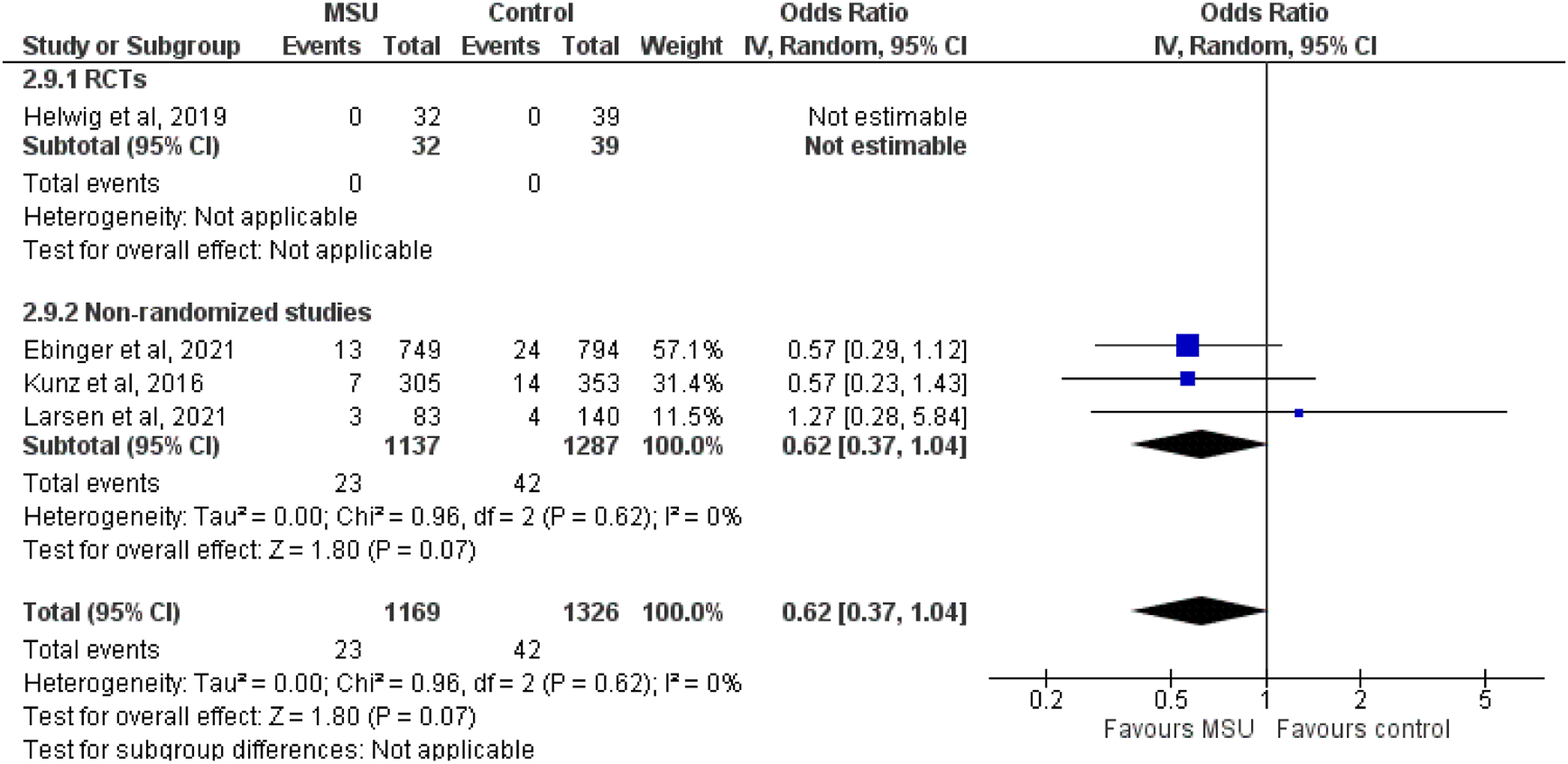
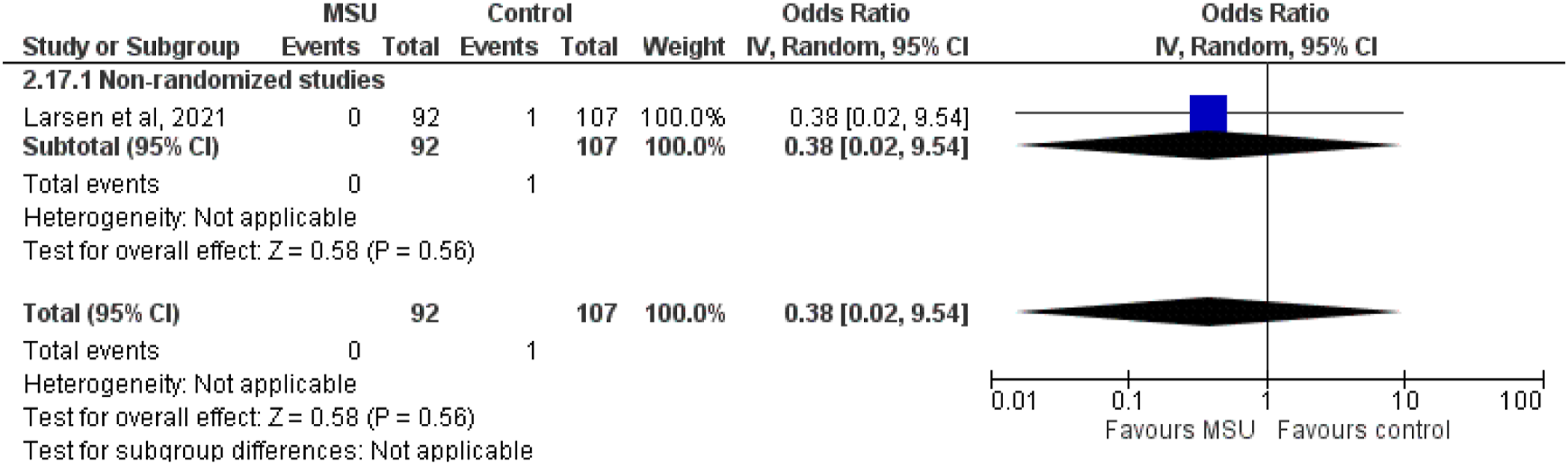
MSU was not associated with symptomatic intracranial haemorrhage (sICH) among all AIS patients (OR: 0.81; 95% CI: 0.52–1.25; I2 = 0%; Figure 17) and among AIS patients treated with IVT (OR: 0.91; 95% CI: 0.42–1.97; I2 = 0%; Figure 18). There was no association of MSU with major extracranial bleeding among AIS patients treated with IVT (OR: 0.38; 95% CI: 0.02–9.54; Figure 19). Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with 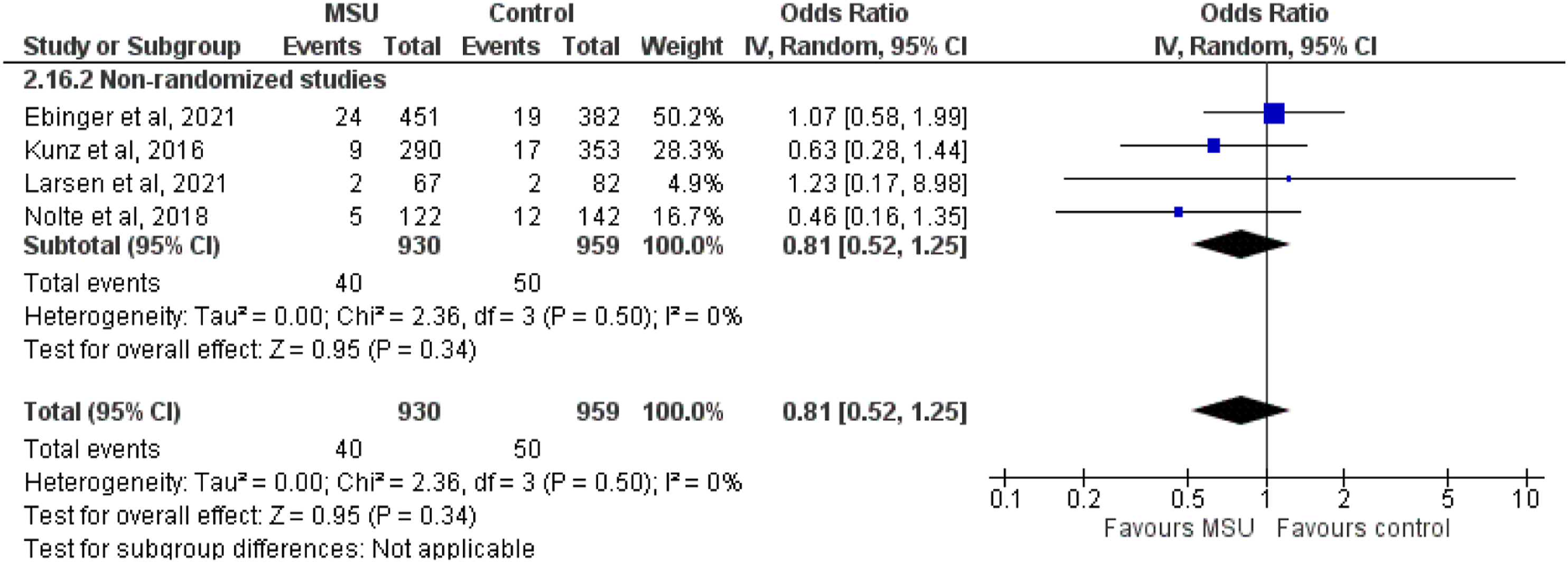
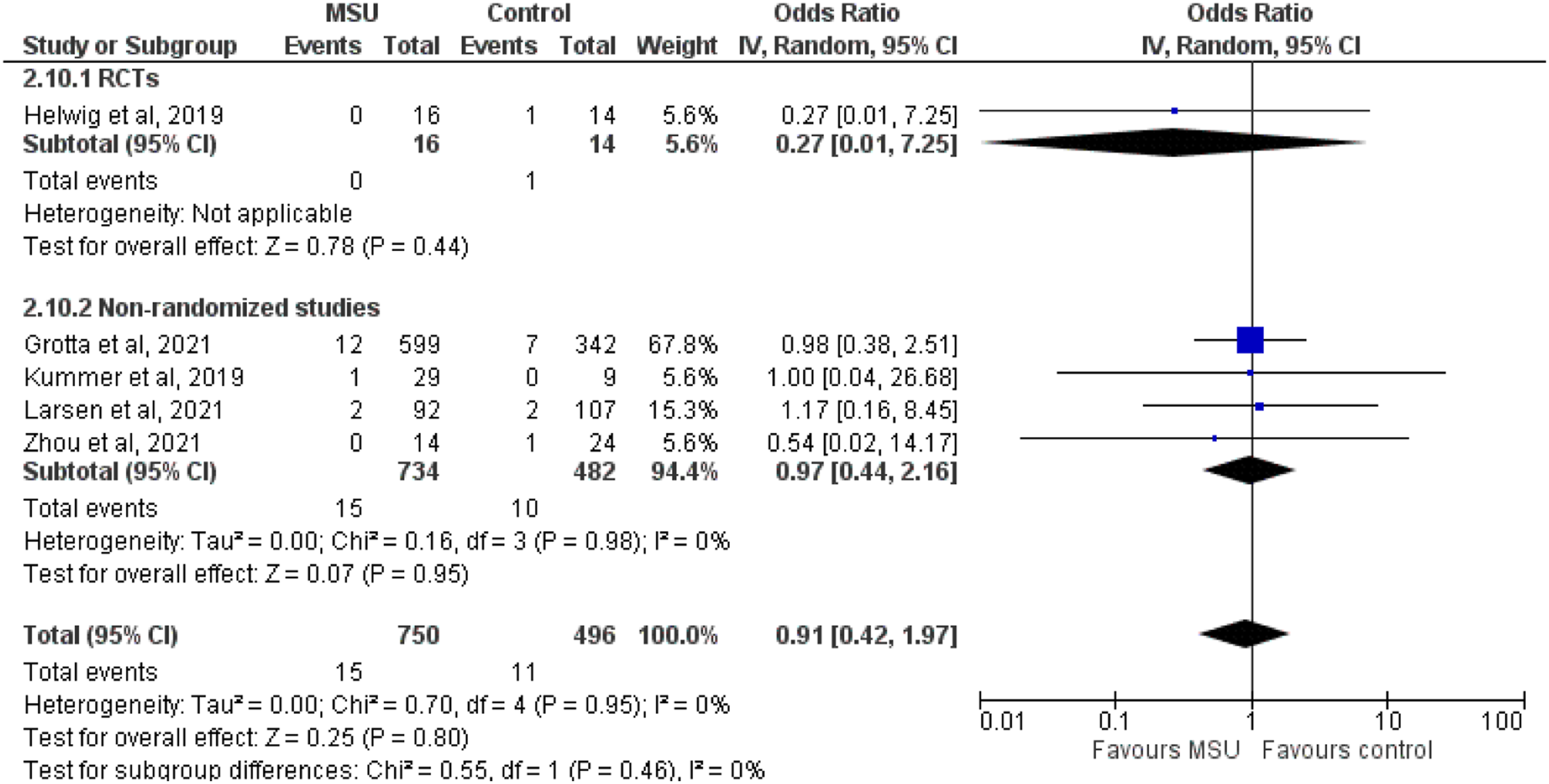
At the time of IVT delivery in the MSU the patient is considered as suffering from AIS and the confirmation of the diagnosis and diagnosis of stroke mimic is made afterwards during hospitalisation. Therefore, the outcome related to IVT in stroke mimics was analysed with the population of AIS patients. Among patients treated with IVT, MSU was not associated with the proportion of stroke mimics receiving IVT (OR: 1.22; 95% CI: 0.70–2.14; I2 = 0%; Figure 20). In brief, MSU was not associated with any of the 4 pre-specified safety outcomes. Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with 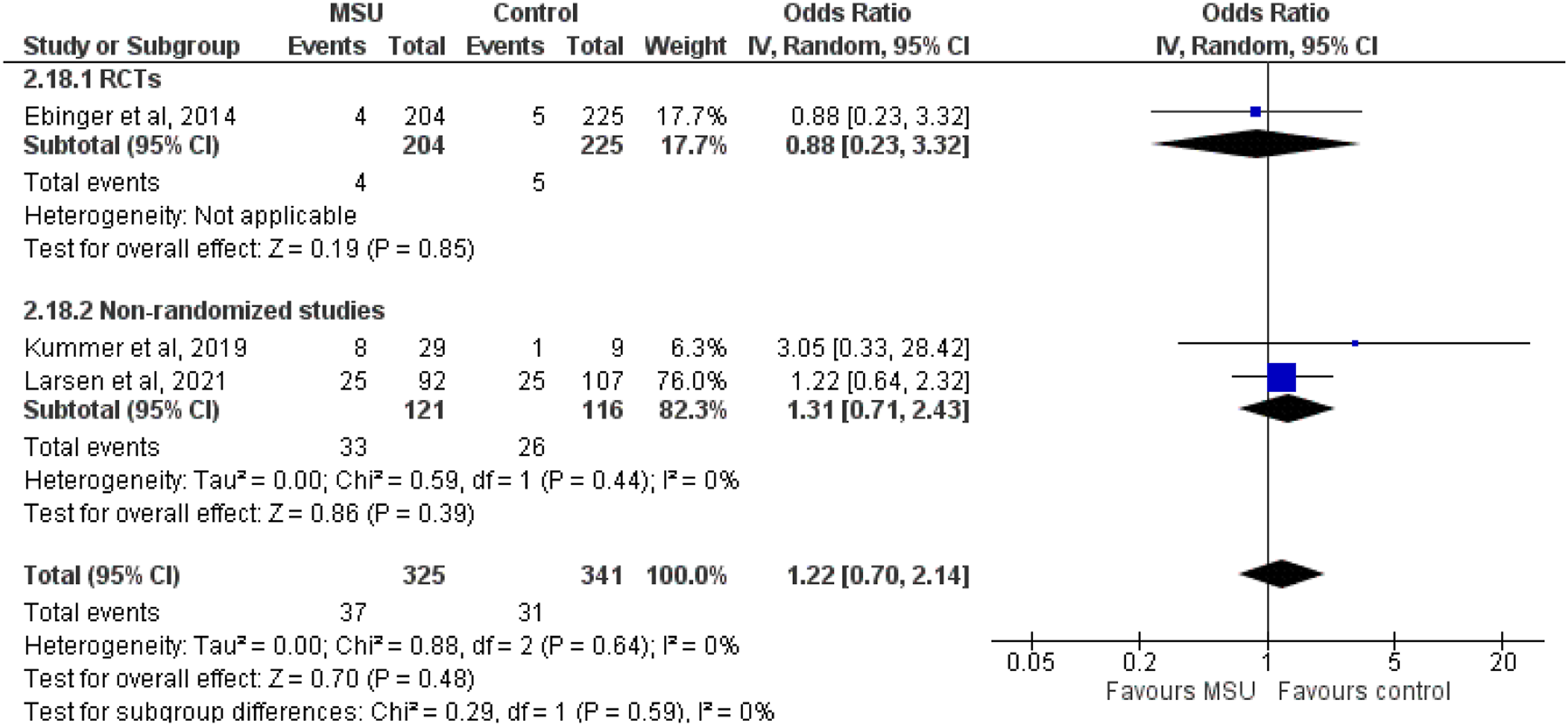
Table 2 provides details regarding the impact of MSU versus conventional management on 90-day functional outcomes among confirmed AIS patients. Table 3 provides details regarding the impact of MSU versus conventional management on time metrics and proportion of confirmed AIS patients receiving IVT. Table 4 provides details regarding the impact of MSU versus conventional management on time metrics, on proportion of patients receiving MT among confirmed AIS patients and on proportion of LVO patients primarily transported to tertiary stroke centres. Table 5 provides details regarding the impact of MSU versus conventional management on all-cause mortality. Table 6 provides details regarding the impact of MSU versus conventional management on bleeding complications.
Additional information
Considering the evidence by removing non-randomised, non-interventional studies
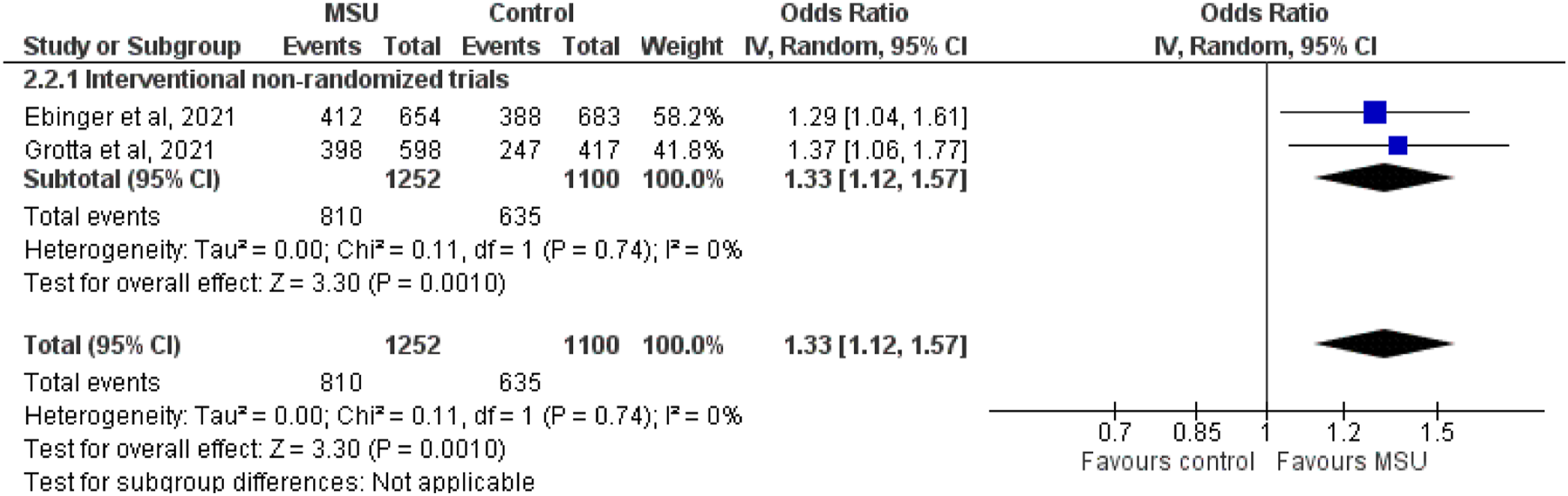
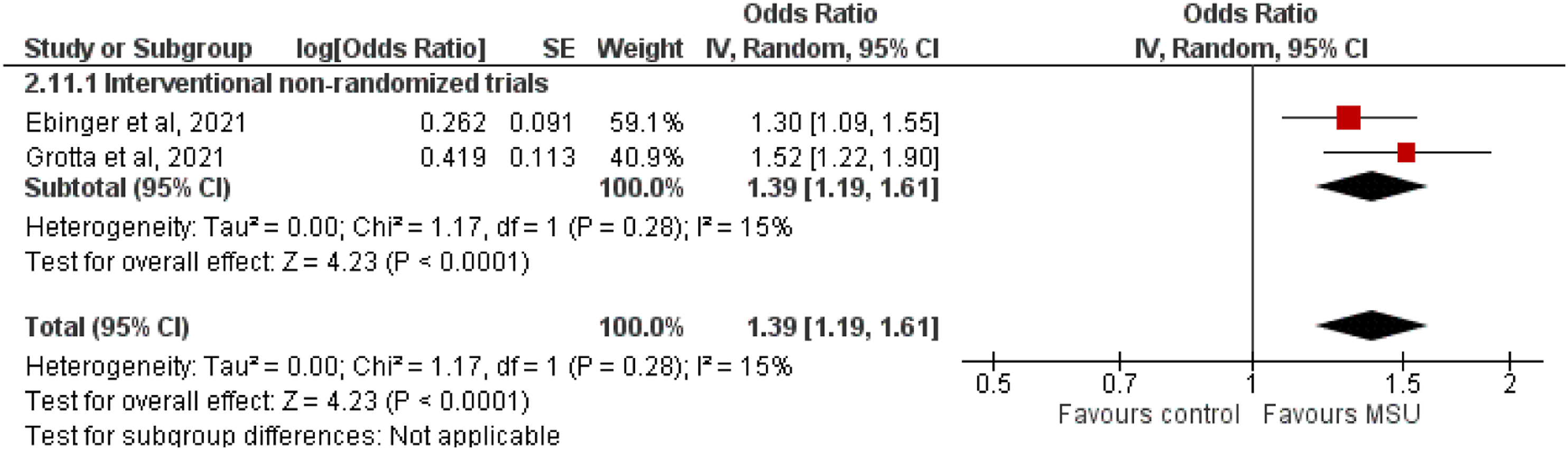
We also performed a sensitivity analysis evaluating the efficacy of MSU versus conventional management in AIS patients after excluding non-randomised studies, without blinded assessment of their primary endpoint. The random-effect meta-analysis included two non-randomised, interventional studies published by Ebinger and co-investigators (B_PROUD) and Grotta and collaborators (BEST-MSU) in 2021.49,50 The random-effect meta-analysis revealed that MSU compared to conventional management improved excellent (OR: 1.46; 95% CI: 1.24–1.72; I2 = 0%; Figure 21), good (OR: 1.33; 95% CI: 1.12–1.57; I2 = 0%; Figure 22) and any better (cOR: 1.39; 95% CI: 1.19–1.61; I2 = 15%; Figure 23) functional outcome in patients with AIS. Table 7 provides details of the sensitivity analysis regarding the impact of MSU versus conventional management on 90-day functional outcomes among confirmed AIS patients. Sensitivity (excluding non-interventional, non-randomised studies) random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Sensitivity (excluding non-interventional, non-randomised studies) random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Sensitivity (excluding non-interventional, non-randomised studies) random-effects meta-analysis comparing mobile stroke units and conventional management in patients with 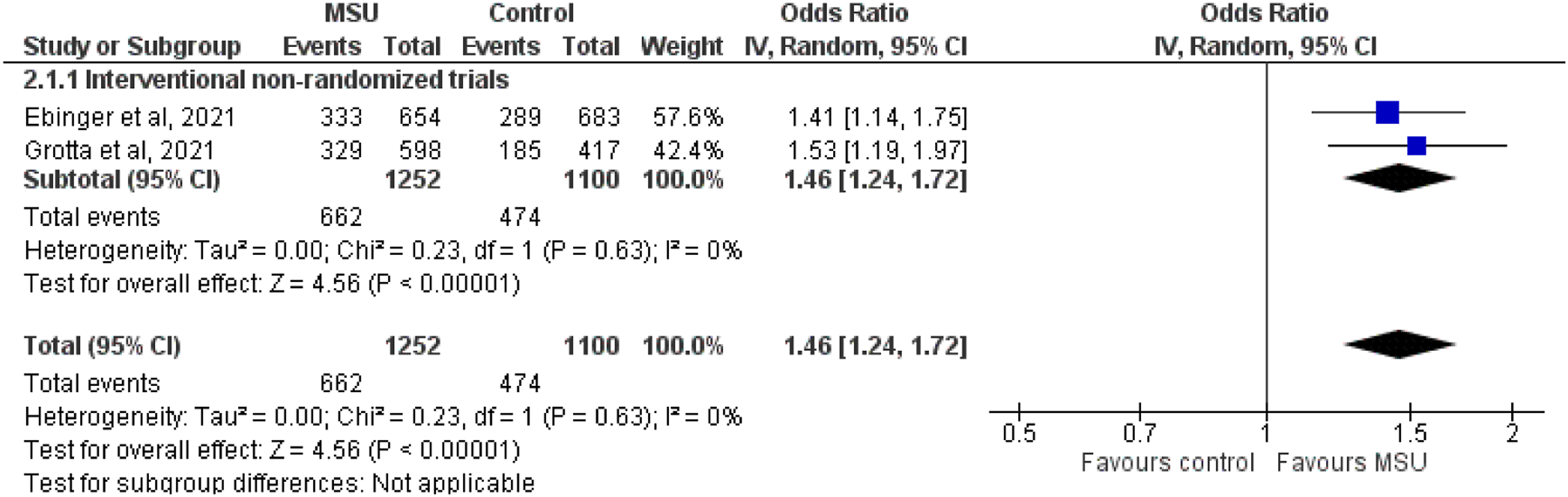
Considering expertise on MSU
MSU is an ambulance that contains a CT scanner, telemedicine equipment and a point-of-care system to determine platelet counts and international normalised ratio as a minumum, in addition to standard emergency equipment. Technology enables to also perform CT angiography and CT perfusion in the ambulance.
The MSU staff includes a paramedic, a radiology technician, depending on local regulations for operating CT scanner, and/or a specialist nurse.
In all the studies considered for the present guideline, radiology consultation was done by remote consultation or in presence with a (neuro)radiologist, if image analysis was not performed by the on-board or remote stroke specialist. In the studies considered for the present guideline, stroke expertise was either available in presence on the MSU or provided by teleconsultation. Only in a single study, published by Larsen and collaborators in 2021, the MSU was run by anaesthesiologists who received a short training in stroke assessment 51 but the final indication to treatment was agreed with a neurologist via remote teleconsultation.
To maintain the same benefits, which were found in the trials considered for the present guideline, it is necessary to guarantee the same level of stroke expertise, which was available in the included studies. MSU care not including neurological expertise on stroke may not have the same benefits as the interventions which have been tested so far. Additionally, it is important to mention that in all the studies there was a streamlined process to maximise efficiency in the evaluation of patients and in the initiation of the intervention. Structured and well-defined organisation will be essential to enable reproducibility of study findings in the routine clinical care.
PICO 3
In patients with confirmed acute intracranial haemorrhage, does prehospital management with a MSU compared to conventional management improve clinical outcomes?
Analysis of current evidence
The literature search identified three studies (two randomised and one non-randomised) that evaluated the effect of MSU versus conventional management on different outcomes in patients with ICH. One RCT and one non-randomised study added evidence to the outcome of the proportion of ICH patients primarily transported to tertiary care stroke centres. The data published by Wendt and co-authors in 2015 analysed a subgroup of the randomised PHANTOM-S trial 42 with 62 participants in the MSU group and 151 participants in the control group between May 2011 and January 2013 and was conducted in Germany. In the study, patients with intracranial haemorrhages, including spontaneous ICHs, traumatic ICHs, subdural haematoma, epidural haematoma and subarachnoid haemorrhages were analysed. The primary endpoint of the study was the proportion of patients transported to appropriate levels of stroke centres if needed. The overall result (all patients with code stroke dispatch) showed that MSU care significantly reduced the proportion of patients triaged to non-stroke centres (MSU: 5.5% vs control 11.6%, p < 0.01) and this was also significant for patients with intracranial haemorrhage (proportion triaged hospitals with neurosurgery department, MSU: 88.7%, control: 57%, p < 0.01). 44
In contrast, the non-randomised study conducted in Norway, published by Larsen and collaborators in 2021, focused on patients with ICH only and analysed 10 and 19 patients with either MSU or conventional management (for detailed description, please see PICO 1). 51 The latter study also adds evidence to the safety outcomes all-cause mortality on day 7 and day 90.
An additional RCT was conducted in Germany by Helwig and co-investigators and analysed eight patients per management groups. 46 This study adds additional information to 7-day all-cause mortality. This trial again included patients with the wider range of intracranial haemorrhages (detailed description PICO 1).
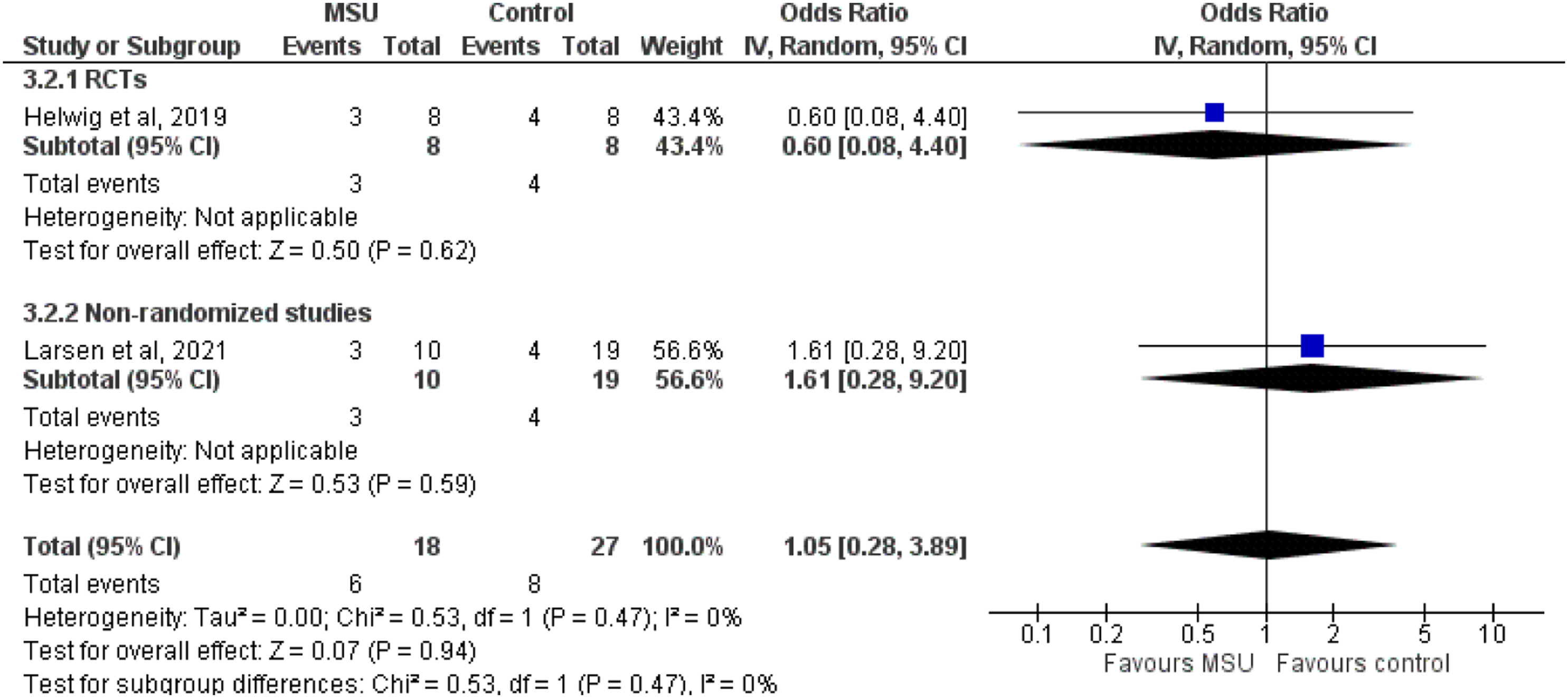
The random-effect meta-analysis revealed that MSU compared to conventional management increased the proportion of ICH patients primarily transported to tertiary care stroke centres, with neurosurgical treatment option (OR: 6.44; 95% CI: 2.96–14.01; I2 = 0%; Figure 24). There was no association between MSU (vs conventional management) and 7-day (OR: 1.05; 95% CI: 0.28–3.89; I2 = 0%; Figure 25) or 90-day (OR: 1.14; 95% CI: 0.24–5.50; Figure 26) mortality among ICH patients. Table 8 provides details regarding the impact of MSU versus conventional management on primary triage and all-cause mortality among patients with ICH. Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with Random-effects meta-analysis comparing mobile stroke units and conventional management in patients with GRADE evidence profile for PICO 3 on patients with ICH. MSU: mobile stroke unit; CI: confidence interval; OR: odds ratio; N/A: not applicable ICH: intracerebral haemorrhage. apossible bias in the selection of participants. bwide confidence intervals. clack of allocation concealment. dConfidence intervals fail to exclude substantial benefit or harm. eestimate derived from only one study.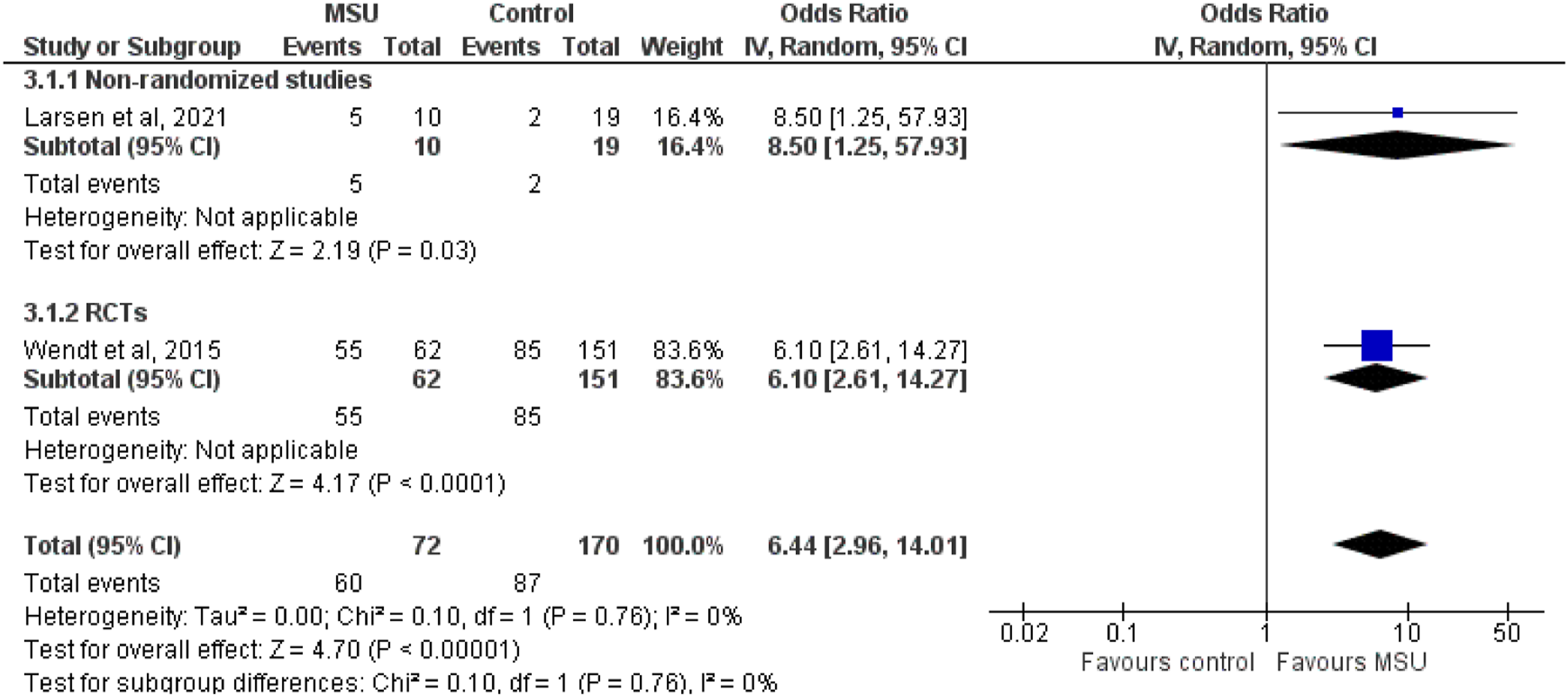

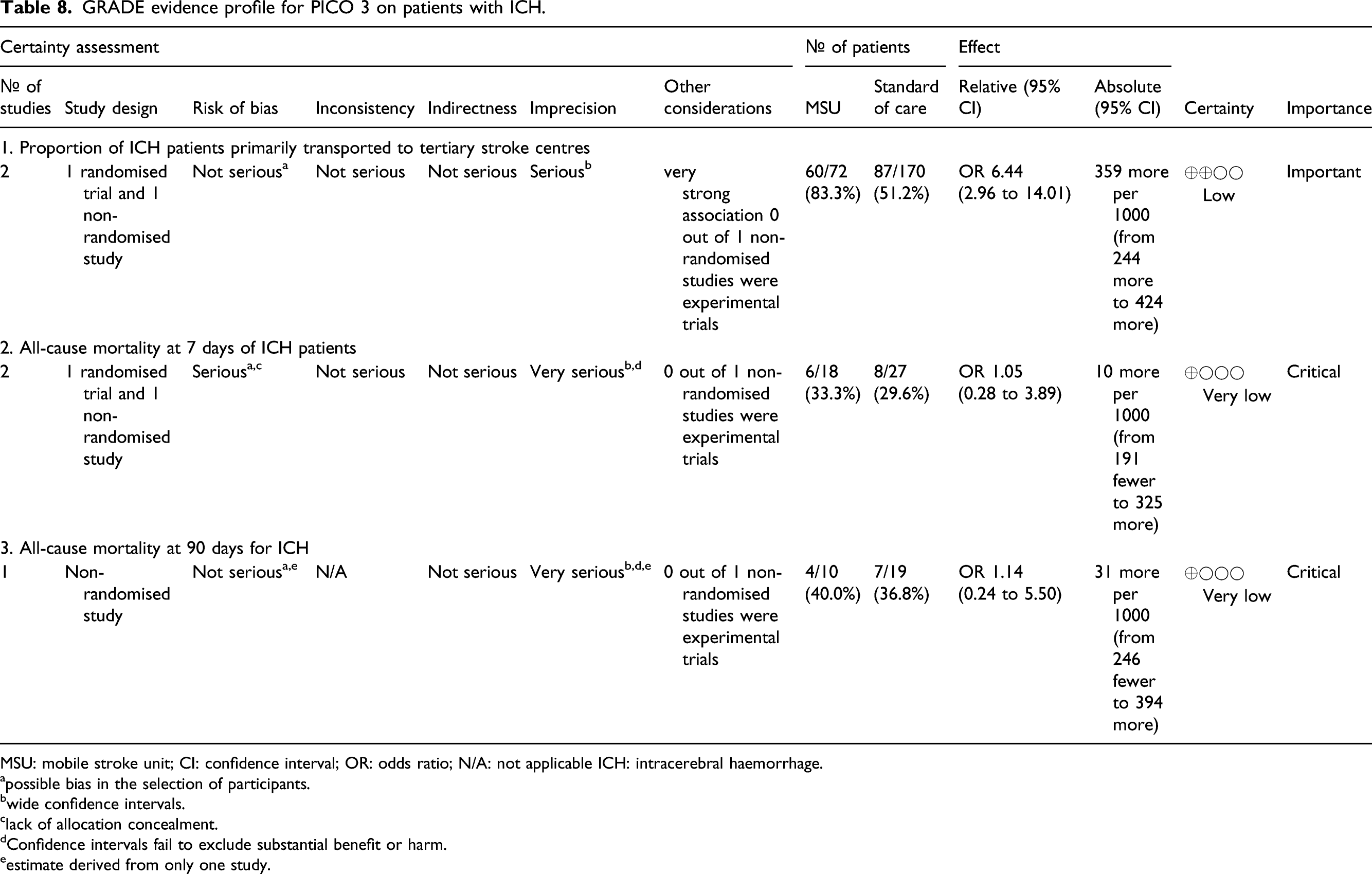
There was no data available to assess the impact of MSU in the remaining four selected outcomes (good functional outcome, any better functional outcome, excellent functional outcome and size of haematoma expansion).
Additional information
We consider the statements related to MSU staffing that have been displayed in the additional information of PICO 2 (patients with confirmed AIS) are also applicable to PICO 3 (patients with confirmed ICH). In confirmed acute ICH patients, we suggest prehospital management with MSUs over conventional management because the timely transport of these patients to tertiary stroke centres is crucial for optimal therapeutic management.Expert consensus statement
The numerical results of the votes for this Expert Consensus Statement are provided in Supplemental Table 2. We suggest the use of MSUs over conventional care for the prehospital management of patients with suspected stroke, for the following reasons: - In patients with AIS, prehospital management with a MSU improves functional outcomes, increases the rates of treatment with IVT, including the rates of thrombolysis within the golden hour and shortens onset to treatment time without any safety concerns. Quality of evidence: - In patients with intracranial haemorrhage, prehospital management with a MSU increases the proportion of patients primarily transported to tertiary care stroke centres, without concerns on short-term mortality. Quality of evidence: - In other patients (e.g. stroke mimics), no signal of safety concerns was identified. Quality of evidence:
When considering MSU care, to maintain the same benefits of clinical studies in routine practice and based on the current evidence, including specialist neurological expertise either by an in-person stroke expert or by remote consultation and a streamlined process of care are essential.Evidence-based Recommendation
Expert consensus statement
The numerical results of the votes for this Expert Consensus Statement are provided in Supplemental Table 2.
Discussion
Summary of PICO questions, evidence-based recommendation and expert consensus statements.
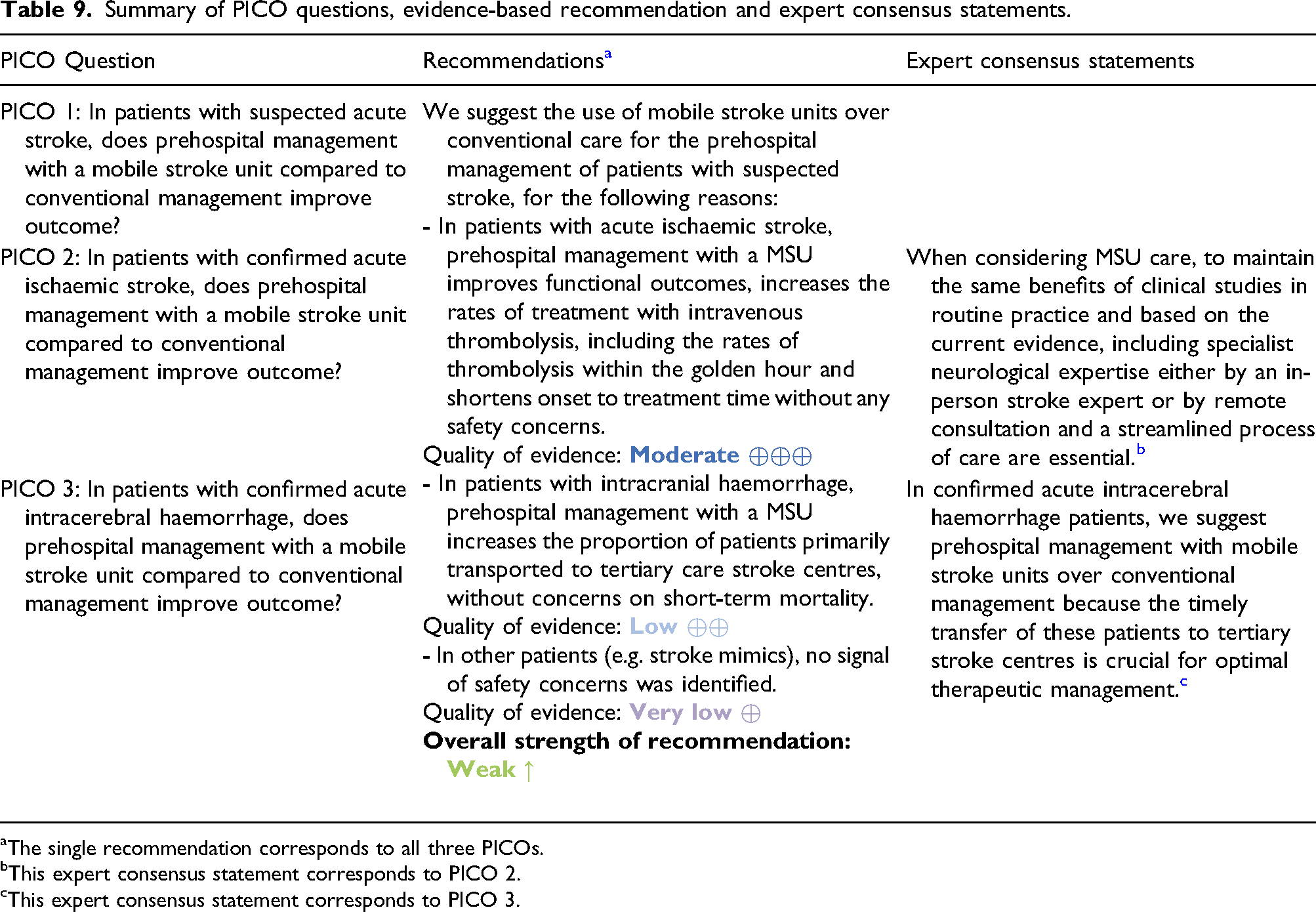
aThe single recommendation corresponds to all three PICOs.
bThis expert consensus statement corresponds to PICO 2.
cThis expert consensus statement corresponds to PICO 3.
We decided to provide only one combined recommendation, because MSU care applies a novel management pathway to patients with suspected stroke at the very first moment when patients contact the health care system. This is an unconventional approach, but at the time of the patients’ contact to the emergency medical dispatch centre, the definite diagnosis of the patients is unclear. With the currently available dispatch pathways, a pre-selection of patients and dispatch of MSUs to a selected subgroup of stroke patients (e.g. AIS) only, for whom enough evidence is available, is not possible.
The broad variety of patients seen when using a MSU pathway, is reflected by the different subsets of patients ranging from patients identified as suspected stroke patients by the emergency medical dispatch centre to patients eligible for IVT as identified by stroke specialists in the publications analysed for this guideline. This needs to be considered in the interpretation of the results.
We found that there is moderate evidence for suggesting MSU management over conventional management because at scene identification of patients with AIS and IVT treatment initiation leads to an improved functional outcome at 90 days, reduces onset to treatment times, increases the proportion of AIS patients receiving IVT and increases golden hour treatment, in which probability of full recovery is highest.1,68 In addition, in patients identified with an intracranial haemorrhage already at the emergency site, prehospital management with a MSU increases the proportion of patients who are primarily transported to tertiary care stroke centres with all treatment possibilities including advanced Blood pressure management and neurosurgery. There are no additional safety concerns for either stroke patients or patients presenting with stroke mimics when managed with a MSU in the prehospital setting.
The analysis performed for
Patients with
The analysed time from emergency call-to-IVT, which represents the prehospital phase plus the intrahospital door-to-needle times ranged between 72 to 98 min on average in the studies included in our analysis. Some studies reported door-to-needle times for their control groups with a median ranging from 29 to 58 min. This compares favourably to the mean door-to-needle time (without prehospital time) of 73 min with a median (interquartile range) of 67 (47–91) min described in the analysis of the Safe Implementation of Thrombolysis in Stroke registry. 70
The rationale for our specific recommendation was a consistent effect strongly favouring MSU management both in the primary and in the sensitivity analysis. Furthermore, in the B_PROUD study patients analysed for the primary clinical outcome were patients with MSU dispatch including those without IVT treatment. This confounding factor leads to an underestimation of the demonstrated effect on mRS as improved clinical outcome after AIS is strongly related to the administration of systemic or endovascular reperfusion therapies.56,71
We documented no benefit of MSU care in the proportion of LVO patients receiving MT or in time metrics of MT. However, even if MT was not demonstrated to be earlier in the two studies analysed, B_PROUD and BEST-MSU, LVO patients received earlier IVT treatment, which translates to a better outcome. 68 In both trials, patients with LVO had the same benefit in 90-day mRS compared to non-LVO patients (unpublished data from BEST-MSU and B_PROUD). It should be considered that in B_PROUD 49 and BEST-MSU 50 , CT angiography was not performed routinely and if done, it was repeated for most MSU patients with prehospital CTA after hospital arrival, which aligns in-hospital management of both groups and masks potential benefits of an early initial CTA. 72 Data from the Australian MSU programme, indicated a difference in median time to MT when referring to data from a historical control group. This result was mainly achieved by bypassing the local non-MT centres. 47 Future research will add more evidence for patients suffering from LVO and other strokes (e.g. acute ICH) and the MSU concept might facilitate the identification of novel diagnostic and therapeutic approaches that may provide benefit from ultra-early administration. We detected a significant difference favouring MSU treatment for the number of LVO patients directly transported to a tertiary, MT-capable stroke centre and data coming from the RCT by Helwig and collaborators published in 2019 emphasised that emergency site triage accuracy with a MSU was better than with the clinical Los Angeles Motor Scale (LAMS) for identification of LVO patients. 46 However, overall numbers analysed are low (22 MSU vs 39 control patients), which emphasises the need of further evaluations in larger cohorts.
It has been assumed that earlier management of suspected stroke patients with or without IVT in the MSU may increase the risk of sICH and extracranial bleeding complications or mortality due to potential mechanical distress during transport and compromised blood pressure management. We could not identify any significant difference in all-cause mortality of AIS patients treated with a MSU compared to standard care at 7 and 90 days. The MWG group unanimously agreed to upgrade the indirectness of the available data for sICH and proportion of stroke mimics receiving IVT from not serious to serious considering the wide CIs but also the disparity in sICH definitions of the studies analysed. However, a recent publication did not identify any difference in mortality and sICH of MSU golden hour treated patients and in-hospital golden hour treated AIS patients included in the SITS-EAST registry (Safe Implementation of Treatments in Stroke-East). 73
For patients with
The strengths of this guideline are its systematic approach to searching the literature and guidance by the GRADE methodology. We also performed a comprehensive set of analyses for the pre-specified outcomes selected by the Delphi approach. The most important question for stroke clinicians related to improved functional outcomes, swift access to IVT bolus and increased IVT rates in AIS patients could be answered with convincing evidence leading to a clear recommendation. Additionally, to mitigate the difference of published study populations and harmonise groups in the aggregate data meta-analysis, we included previously unpublished data obtained from the respective researchers in personal communication.
However, many questions posed by the MWG especially regarding the benefits for patients with ICH treated with a MSU need further research, especially with the option to administer acute treatments much earlier. The approach of MSU care will always involve patients with non-acute stroke or stroke mimics. While available data does not allow conclusions of additional beneficial effects for these patient groups, it does not suggest an increased risk or adverse outcome either. The certainty of this assertion is low or very low. Nevertheless, stroke unit care is also offered in stroke mimics or patients with non-acute stroke without increasing the risk of adverse outcomes but also without offering any additional benefit.
MSU care remained significantly associated with better functional outcomes at discharge when analysing all enrolled patients – including stroke mimics and patients with ICH – in the BEST-MSU study. Also, the B_PROUD study included 26% patients with MSU cancellation and still functional outcomes favoured MSU patients using this intention-to-treat approach. Finally, we should keep in mind that IVT in stroke mimics has not been associated with any safety concerns. 83
The benefits of a MSU pathway were all demonstrated in stroke systems of care with availability of specialist neurological expertise, which were already highly efficient as indicated by the short times to treatment and high IVT treatment numbers in the standard management groups. The set-up of an efficient stroke pathway is one of the major challenges every organisation faces and this may influence reproducibility of the results. Also, it is unclear whether results will show a similar outcome in different geographical areas e.g. rural settings as data available comes from urban or suburban regions. Travelling times will definitely vary between the different regions and even more between urban and non-urban areas. The travelling time relevant to all patients is the time to arrival at the patient’s site. However, this time does not differ between MSUs and conventional ambulances. Due to the possibility to diagnose and apply IVT treatment on board the MSU, longer travelling times to the stroke centres are unlikely to affect the patient’s outcome, if no further treatment is needed. Furthermore, once patients are diagnosed with AIS, then treatment with IVT is swiftly initiated. We identified no studies completely conducted in rural areas. This may represent another topic that deserves further research because cost-effectiveness of MSUs may vary in different geographic reasons given the fact that rural areas may have fewer patients with suspected stroke per day and might manage fewer cases per day due to the longer travelling times.
Evidence available for the different patient populations seen by a MSU differs and a high number of patients treated with a MSU, for whom evidence is weak likely impacts on the cost burden coming with the concept. To mitigate this, an increase of dispatch accuracy is needed, which will be more likely achieved with more real-life data of MSU operation.
The dispatch process of MSU centres included in this analysis varied from specially designed dispatch algorithms 69 and stroke scales 46 to being based on the standard medical priority dispatch system (MPDS), which reflects reality in the different prehospital medical settings.
MSU efficiency strongly depends on dispatch accuracy. However, dispatch is challenging, with a significant proportion of the dispatches being stroke mimics.
MSU management is associated with an increase in costs. Limited data is available indicating cost-effectiveness.84–87 The near future will bring further valuable information of the pre-specified cost-effectiveness analysis of the B_PROUD and BEST-MSU studies. However, stakeholders will eventually assess the cost-to-benefit ratio for their particular setting.
In conclusion, the current recommendation emphasises that optimisation of the prehospital phase of acute stroke care is crucial for getting the best out of the available acute stroke treatments. We suggest MSU management for suspected stroke patients, because it will improve the functional outcome of those with AIS without any signal of harm to patients with a final diagnosis of ICH or stroke mimics.
MSU may also offer the unique opportunity to further study additional interventions which can be rapidly delivered in both, AIS and ICH. Future research into MSUs will have to focus not only on the implementation of novel therapeutic strategies but also on the best setting for this prehospital acute stroke care approach including optimal dispatch organisation and cost-benefit analysis.
Plain language summary
Acute stroke is a treatable disease, but therapeutic success depends on administration of treatments rapidly after symptom onset. This is very well known for patients with a stroke caused by a blood clot (‘ischaemic stroke’), who benefit from a clot buster infusion (‘thrombolysis’) or treatment with wires navigating through brain arteries to pull out the blood clot (‘Mechanical thrombectomy, MT’). But also, some patients with bleeding in the brain (‘haemorrhagic stroke’) may benefit from very quick monitoring, stabilisation of their blood pressure, reversal of blood thinning therapies and care at a specialised stroke centre with a brain surgery treatment option. However, the main problem of current stroke patient management is that patients do not reach the hospital in time to achieve the best possible chances of disability-free survival. The new approach of taking the stroke team with all necessary diagnostic equipment to the patient rather than waiting for the patient in a hospital has shown to improve acute stroke patient management. This approach uses a specialised emergency ambulance, called MSU, which is equipped with a brain scanner, blood testing machines, telemedicine connection to the stroke centre and is staffed with a stroke specialist team. These ambulances are used in several centres worldwide to diagnose and treat stroke patients at the emergency site and to decide to which hospital the patients have to be transported. The guideline authors make recommendations about the benefits of these MSU ambulances for management of patients with suspected stroke, acute ischaemic or haemorrhagic stroke. The authors have based their recommendation and analysis on the available international literature.
The guideline makes one recommendation
MSU use is suggested for the prehospital assessment of patients with suspected stroke. If an ischaemic stroke is diagnosed MSUs can facilitate swift treatment initiation with clot buster infusion and transportation to an appropriate hospital that can provide potential clot removal through a procedure.
Potential benefits for patients with a brain bleed may be possible and no direct harm, especially to those not suffering from a stroke could be detected. Further research is needed to detect further benefits. Local EMS organisations should invest in optimising dispatch quality in order to make MSUs available to as many AIS patients as possible.
Supplemental Material
sj-pdf-1-eso-10.1177_23969873221079413 – Supplemental Material for European Stroke Organisation (ESO) guidelines on mobile stroke units for prehospital stroke management
Supplemental Material, sj-pdf-1-eso-10.1177_23969873221079413 for European Stroke Organisation (ESO) guidelines on mobile stroke units for prehospital stroke management by Silke Walter, Heinrich J Audebert, Aristeidis H Katsanos, Karianne Larsen, Simona Sacco, Thorsten Steiner, Guillaume Turc and Georgios Tsivgoulis in European Stroke Journal
Footnotes
Acknowledgements
We are grateful for all unpublished data received from Klaus Fassbender, James Grotta, Leonid Churilov and Jose-Miguel Yamal, which supported data analysis of our guideline. We thank Avtar Lal for his help with extraction and review of extracted data. Many thanks go to Brittany Wells for her English language review and editing. Finally, we are thankful for the unremitting administrative support of Sabrina Mutter and Yvonne Brüchert from the European Stroke Organisation head office.
Contributorship
SW and G. Tsivgoulis prepared the first draft of this manuscript. The remaining MWG members performed critical revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not necessary for the work described in this paper.
Informed consent
Not applicable.
Guarantor
A specific guarantor does not exist. The working group has jointly developed the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.