
Abstract
The aim of the present European Stroke Organisation guideline is to provide clinically useful evidence-based recommendations on the management of extracranial artery dissection (EAD) and intracranial artery dissection (IAD). EAD and IAD represent leading causes of stroke in the young, but are uncommon in the general population, thus making it challenging to conduct clinical trials and large observational studies. The guidelines were prepared following the Standard Operational Procedure for European Stroke Organisation guidelines and according to GRADE methodology. Our four recommendations result from a thorough analysis of the literature comprising two randomized clinical trials (RCTs) comparing anticoagulants to anti-platelets in the acute phase of ischemic stroke and twenty-six comparative observational studies. In EAD patients with acute ischemic stroke we recommend using intravenous thrombolysis (IVT) with alteplase within 4.5 hours of onset if standard inclusion/exclusion criteria are met, and mechanical thrombectomy in patients with large vessel occlusion of the anterior circulation. We further recommend early endovascular or surgical intervention for IAD patients with subarachnoid hemorrhage (SAH). Based on evidence from two phase 2 RCTs that have shown no difference between the benefits and risks of anticoagulants versus anti-platelets in the acute phase of symptomatic EAD, we strongly recommend that clinicians can prescribe either option. In post-acute EAD patients with residual stenosis or dissecting aneurysms and in symptomatic IAD patients with an intracranial dissecting aneurysm and isolated headache, there is insufficient data to provide a recommendation on the benefits and risks of endovascular/surgical treatment. Finally, nine expert consensus statements, adopted by 8 to 11 of the 11 experts involved, propose guidance for clinicians when the quality of evidence was too low to provide recommendations. Some of these pertain to the management of IAD (use of IVT, endovascular treatment, and antiplatelets versus anticoagulation in IAD with ischemic stroke and use of endovascular or surgical interventions for IAD with headache only). Other expert consensus statements address the use of direct anticoagulants and dual antiplatelet therapy in EAD-related cerebral ischemia, endovascular treatment of the EAD/IAD lesion and multidisciplinary assessment of the best therapeutic approaches in specific situations.
Keywords
Introduction
Cervico-cephalic artery dissections are defined by a hematoma in the wall of a cervical or intracranial artery and represent a leading cause of stroke in the young.1,2 While dissection of the extracranial cervical arteries (hereafter referred to as “extracranial artery dissection”, EAD) has been extensively studied and described in increasingly large observational studies,3-9 less data is available about isolated intracranial artery dissection (IAD). By contrast with cervical arteries, intracranial arteries are characterized by a paucity of elastic fibers in the media, little adventitial tissue, no external elastic lamina,10,11 and weaker supporting tissues. 12 In internal carotid arteries, the external elastic lamina is still present in the petrous portion of the temporal bone (C3 segment) and disappears in the horizontal segment of the cavernous portion (C5); hence, typical features of IAD are found for dissections occurring in the intradural portion of the internal carotid artery—i.e., starting in C6. 13 In vertebral arteries, the reduction of elastic fibers in the media and external elastic lamina is most pronounced in the last 0.5 cm before the intradural portion but is not complete until 0.5 cm after dural perforation (V4 segment). 13 While many characteristics and clinical manifestations are shared between EAD and IAD, there are also important differences. For example, the mean age of occurrence is younger (44 years) for EAD than for IAD (50 years). 13
The incidence of EAD is low in the general population, estimated around 2.6 to 3.0 / 100,000 inhabitants/year.14,15 The incidence of IAD is unknown, but probably lower than that of EAD in populations of European ancestry.14,15 The relative frequency of EAD versus IAD varies by study recruitment strategies and ascertainment methods 13 but is also highly variable according to geographic origin. For example, the proportion of IAD amongst all cervico-cephalic dissections is estimated around 11% in European populations, 16 around 27% in Latin America, 17 and up to 67–78% in East Asia.18,19 EAD/IAD are multifactorial conditions in the vast majority of cases, while they can rarely occur as part of an inherited connective tissue disorder or fibromuscular dysplasia.8,9 In EAD, hypertension and migraine are reported risk factors with common genetic risk variants in the PHACTR1 gene also associated with EAD.7,20 Frequently cervical trauma (most often minor) or recent infections are reported as triggers. Risk factors are less well characterized for IAD.
Clinically, EAD usually presents with “local” symptoms and signs partly due to compression of adjacent structures, including headache, cervical pain, Horner syndrome, and cranial nerve palsy. In about two thirds to three quarters of patients in published series, the EAD is complicated by cerebral ischemia (ischemic stroke or transient ischemic attack [TIA]), or more seldom retinal, or spinal cord ischemia, typically occurring several hours or days after the onset of local symptoms. Subarachnoid hemorrhage (SAH) exceptionally occurs in EAD when the dissection expands to the intradural portion of the artery. 9 The two main clinical manifestations of IAD are SAH (in about 50-60% of patients in published series), cerebral ischemia (30%-78%), and exceptionally both. About 80% of IAD patients have prodromal headache.21,22 Symptoms related to brainstem or cranial nerve compression can also occur. 13
From an imaging perspective, EAD/IAD can present as a segmental stenosis (most common presentation in EAD), an occlusion, or a dissecting aneurysm. Several features can be present at the same time, typically a dissecting aneurysm with a long tapering stenosis. In 15-20% of EAD patients, multiple cervical arteries are affected. 23 In EAD, stenosis resolution or recanalization occurs in 33–90% within 6 months;5,15,24-26 dissecting aneurysms are reported to resolve or decrease in size in 40–50% of patients but can also increase in size and develop anew.27,28 In the Cervical Artery Dissection in Stroke Study (CADISS) trial, dissecting aneurysms were present in 24 of 264 patients at baseline and in 36 of 248 patients with follow-up at 3 months: 12 of baseline dissecting aneurysms persisted and 24 new dissecting aneurysms had developed. 28 The timeframe of changes in imaging characteristics in IAD patients and the rates of recanalization are unknown. 13
The low incidence of EAD/IAD has proven a challenge to clinical trials conduction, and therefore guidelines have mostly relied on indirect evidence from observational studies and expert opinion. In addition, most guidelines have focused primarily on EAD management without discussion of the treatment of IAD.29-31 Recently, two randomized controlled trials (RCTs) have been published comparing anticoagulation to antiplatelet therapy in the acute phase of EAD,32-34 one of them while this guideline was being prepared. 34 Moreover, acute phase ischemic stroke management has undergone substantial developments in recent years which existing EAD/IAD guidelines have only partially included. To our knowledge, this is the first guideline taking a comprehensive approach to both EAD and IAD and the first to use the GRADE system (Grading of Recommendations Assessment, Development, and Evaluation), which allows clear separation of quality of evidence and strength of recommendation as well as a transparent process of literature search and analysis. 35
The aim of this guideline is to provide recommendations to guide physicians treating patients with EAD/IAD to reach therapeutic decisions when assessing patients with a suspected or confirmed EAD or IAD. It first addresses treatment in the first hours of ischemic stroke due to EAD/IAD and the question of recanalization, second the acute phase treatment of IAD for prevention of SAH and ischemic stroke, and third the prevention of longer term complications of EAD/IAD.
Methods
The guidelines for management of EAD and IAD follow the standard operations procedure (SOP) defined by the European Stroke Organisation (ESO) 36 and were developed using the GRADE methodology. 35 A Module Working Group (MWG) was established, consisting of 11 experts (SD, Chair; AP, MM, MA, PB, MK, HSM, STE, JK, AB, and JJM). The MWG was joined by five fellows during study screening (DS, KM, IC, PT, and JH) who assisted the experts with abstract and full text screening and drafting the text. The MWG included ten neurologists (of whom one is also a neurointerventionalist and one a neuroepidemiologist) and one neurosurgeon; all eleven are experts in cerebrovascular disease with a special interest in EAD and IAD or stroke in the young. Four of the fellows were trainee or early career neurologists and one was an early career neurosurgeon. Of the 16 MWG members, 12 were European, two were Japanese, and two from the United States; this wider geographical representation was important to account for differences in epidemiological characteristics and management strategies between continents. ESO guidelines board and ESO Executive committee approved the composition of the working group. All participants were asked to disclose any conflict of interest that could influence their participation. The group communicated using e-mail and teleconferences.
Diagnostic criteria
For cervical artery dissection, we used the term extracranial artery dissection (EAD) for clear differentiation from intracranial artery dissection (IAD). EAD refers to the dissection of a cervical carotid or vertebral artery radiologically confirmed by the presence of a mural hematoma, a dissecting aneurysm, a long tapering stenosis, an intimal flap, a double lumen, or an occlusion >2 cm above the carotid bifurcation revealing a dissecting aneurysm and/or a long tapering stenosis after recanalization. 23 The diagnosis of IAD is considered definite in presence of at least one of the following: 13 (i) a stenosis or occlusion of an intracranial artery secondarily developing towards a fusiform or irregular aneurysmal dilation at a non-branching site; (ii) an intramural hematoma, intimal flap, or double lumen; and (iii) pathological confirmation of IAD. Of note, given the dearth of data, we did not limit our review to studies strictly applying these diagnostic criteria. Indeed, especially for IAD, these diagnostic criteria are fairly recent, 13 and restricting our search to later studies only would have substantially reduced the number of available studies. We did not include studies on mycotic and blood blister-like aneurysms. Mycotic or oncological giant fusiform aneurysms are caused by the release of proteases by bacteria or tumor cells that break down the vessel wall but are non-dissecting. Blood blister-like aneurysms are located at non-branching sites of intracranial arteries and are caused by a degeneration of the internal elastic lamina and media without associated arterial dissection. 13
Selection of Population, Intervention, Comparator, and Outcome (PICO)
Regarding the population, the MWG decided to focus primarily on symptomatic EAD and IAD, with ischemia (ischemic stroke, TIA, or retinal ischemia), SAH, or headache.
Interventions and comparators addressed the early acute, acute, and post-acute phase of EAD/IAD. First, we addressed recanalization at the hyperacute phase of ischemic stroke caused by EAD/IAD using intravenous thrombolysis (PICO 1) and endovascular treatment (PICO2) (versus the absence of such treatment). Second, we tackled the acute phase of IAD without cerebral ischemia, encompassing IAD with SAH (PICO3) and IAD with only headache (PICO4) for which we each assessed endovascular or surgical intervention versus medical treatment. Third, we addressed the acute phase of EAD/IAD without SAH using anticoagulation versus antiplatelet agents (PICO5). Fourth, we considered endovascular or surgical intervention versus medical treatment for residual stenosis or dissecting aneurysm beyond the acute phase of EAD (PICO6).
We considered six separate outcomes: (i) death, (ii) functional outcome (good functional outcome defined as modified Rankin Scale [mRS] scores of 0–2 versus 3–6 and excellent functional outcome with mRS scores of 0–1 versus 2–6, or equivalent as defined in the individual studies), (iii) ischemic stroke, (iv) SAH, (v) intracerebral hemorrhage (ICH), and (vi) major bleeding, defined according to the International Society on Thrombosis and Haemostasis (ISTH). 37 We had initially also considered the following additional outcomes: new ischemic lesions on diffusion weighted imaging (DWI), recurrent dissection, and frequency of normalization or stability of vessel patency on imaging. Using the Delphi method, the MWG voted in a closed ballot to identify which outcomes were of highest priority, according to the GRADE methodology using a 9-point scale (7–9: critical; 4–6: important; 1–3: of limited importance). The final scores, based on the mean votes from all participants, were the following: death 8.8, functional outcome (good or excellent functional outcome) 8.7, ischemic stroke 8.0, ICH 7.6, SAH 7.5, new ischemic lesions on DWI 6.5, recurrent dissection 6.2, normalization or stability of vessel patency 5.5, major bleeding 5.0. Due to a large number of outcomes we decided to focus on the clinical outcomes only and discarded the imaging-based outcomes that had been rated by the MWG as important, but not critical for decision making.
PICO questions
The MWG formulated six main PICO (Population, Intervention, Comparator, Outcome) questions relevant for EAD and IAD management, each with several sub-questions relating to the six different outcomes defined above, different subpopulations, or intervention sub-types, as relevant to each PICO and described below in the PICO header questions (Supplementary Panel 1). These were refined following comments from the ESO Executive Committee and ESO Guidelines Board. Subsequently, ESO Executive Committee and ESO Guidelines Board approved them.
For each PICO question, search terms were identified, tested, refined, and agreed by the MWG with the ESO Guidelines methodologist (AL). Search terms are listed in the Supplementary Methods.
Identification and selection of relevant studies
A systematic review of literature was done to collect evidence to answer the PICO questions. This search was performed by the ESO Guidelines methodologist (AL). The following databases were searched: MEDLINE, EMBASE and CINAHL, from inception to April 5, 2021. We also searched reference lists of review articles, the authors’ personal reference libraries, and previous guidelines for additional relevant records. The search results were loaded into the web-based Covidence platform (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia) for assessment by the MWG. Two or more MWG members were assigned to independently screen the titles and abstracts of publications registered in Covidence and assess the full text of studies determined to be potentially relevant. All disagreements were resolved by discussion between the two authors or by a third MWG author. We prioritized RCTs, but due to the limited data, we also considered health registry data analyses, large observational studies (minimum size: 50 subjects for EAD, 20 subjects for IAD), and systematic reviews or individual patient data meta-analyses of observational studies. We chose a more liberal minimal sample size for IAD studies based on the dearth of published data on that disease. We considered only studies in human adults (>18 years) with the full article available in English. We excluded studies on penetrating injury of cervical or intracranial arteries and publications with only conference abstracts available.
Meta-analyses and assessment of quality and risk of bias
A random effects meta-analysis was conducted using the Review Manager (RevMan) 5.3 COCHRANE Collaboration software based on raw numbers extracted from the manuscripts. Results were presented as odds ratios (ORs) with 95% confidence intervals (CIs). Since there were very few RCTs and for some PICOs also few observational comparative studies, we also derived mean event rates from large single-arm observational studies using the metaprop function in the Meta package in R.
The risk of selection, performance, detection, attrition, and reporting biases in each RCT was assessed using the Cochrane Collaboration’s tool, 38 and heterogeneity across studies was assessed using Cochran’s Q (reported as a p value) and I2 statistics. The Cochrane Collaboration’s tool was used to perform the assessment of risk of bias of RCT. The various components of this tool, such as risk of selection (randomization, allocation concealment), performance (blinding of participants and personal), detection (blinding of outcome assessment), attrition (incomplete outcome data), and reporting (selective reporting) bias were assessed in each RCT. For non-RCTs, study conduct, subject selection, assessment, and statistical confounding were assessed using the Scottish Intercollegiate Guidelines Network (SIGN) checklist (https://www.sign.ac.uk/what-we-do/methodology/checklists/). Moreover, for each PICO question and each outcome, the quality of evidence was rated using the GRADEpro Guideline Development Tool (McMaster University, 2015; developed by Evidence Prime, Inc.) using guidelines for non-pooled data as necessary, 39 as high, moderate, low, or very low 36 by AL and verified by at least two members of the MWG and approved by the rest.
Data analysis, drafting of available evidence and recommendations
Each PICO writing group, comprising at least three MWG members, analyzed the available data and drafted two sections of text: “analysis of current evidence” which focused on relevant RCTs and/or observational studies and “additional information” to summarize indirect evidence from additional studies. Each PICO writing group formulated an “evidence-based recommendation” according to the GRADE evidence profiles and the ESO standard operating procedure, 36 and/or an “expert consensus statement” if the PICO group considered that not enough evidence was available for replacing an evidence-based recommendation to address specific situations. The expert consensus statements were then voted on by all expert MWG members (excluding the fellows and methodologists). These expert consensus statements should not be regarded as evidence-based recommendations, since they only reflect the opinions of the MWG.
The Guidelines document was reviewed by all MWG members and modified using a Delphi approach until consensus was reached. It was also reviewed by a member of the ESO Guidelines Board who served as External Advisor prior to submission. The document was reviewed and approved by five reviewers (2 members of the ESO Guidelines Board, 1 Executive Committee member, and 2 external reviewers).
Results
PICO 1: In extracranial artery dissection (EAD) or intracranial artery dissection (IAD) patients with acute ischemic stroke is intravenous thrombolysis (IVT) versus no intravenous thrombolysis associated with a reduced risk of death, a higher likelihood of favorable functional outcome (mRS 0–2 vs. 3–6, or 0–1 vs. 2–6, or equivalent), and no increased risk of ICH, subarachnoid hemorrhage (SAH), or any major bleeding?
Analysis of current evidence
Intravenous thrombolysis is effective and safe in acute ischemic stroke.31,40,41 EAD/IAD was not a specific exclusion criterion in RCTs of IVT versus placebo, but because dissection is uncommon the number of randomized patients with dissection is likely to be very low and no specific subgroup analysis has been published. 31 There is a theoretical concern that thrombolysis may increase the risk of enlargement of an intramural hematoma in the dissected artery and thus impair cerebral hemodynamics, or promote dissecting aneurysm formation or vessel rupture.42,43
Our systematic review identified no randomized data on the efficacy and safety of IVT in patients with EAD/IAD. Only 4 observational studies assessing the effect of IVT on clinical outcome in EAD/IAD patients met our inclusion criteria (Figure 1 and Table 1).44-47 Of note, all except one of the aforementioned studies (which was based on electronic health records with no indication on thrombolytic agent types
47
) consistently refer to alteplase, with no data available for other thrombolytic agents (e.g., tenecteplase). In total, these studies gather 593 EAD/IAD patients receiving IVT and 7573 EAD/IAD patients without IVT in the acute phase of EAD/IAD-related ischemic stroke. The vast majority of these patients were reported in a single study based on electronic health records from the Nationwide Inpatient Sample (NIS) in the United States (488 and 7374 EAD/IAD patients with IVT and without IVT, respectively),
47
where the diagnosis of dissection was based on International Classification of Diseases (ICD)-9 codes, thus not allowing a distinction between EAD and IAD. The other three studies focused exclusively on EAD patients.44-46 PRISMA flow chart of study selection for PICO1. “Wrong study design, patient population, intervention, comparator, and control group” in COVIDENCE corresponds to studies that do not match criteria for this PICO. Summary of observational studies findings relevant for PICO1. Values are mean ± SD or mean (range) unless otherwise specified; * median (IQR). aInternational Classification of Diseases (ICD)9 codes 443.2: other arterial dissection (excluding aortic and coronary dissection), 443.21: dissection of carotid artery, and 443.24: dissection of vertebral artery. bIn hospital mortality, which was approximated as 7 day mortality for the meta-analysis, based on the mean duration of hospital stays.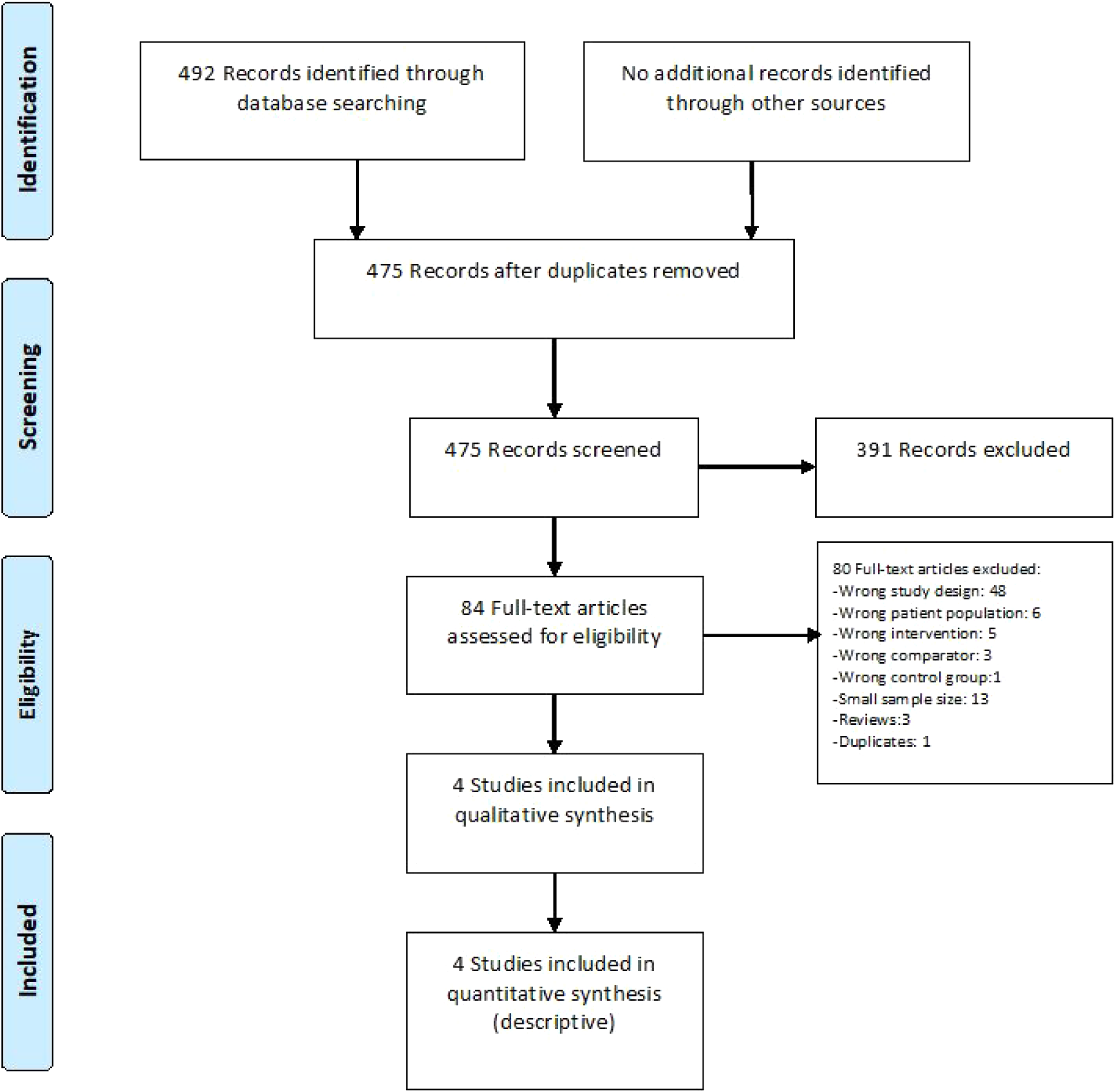
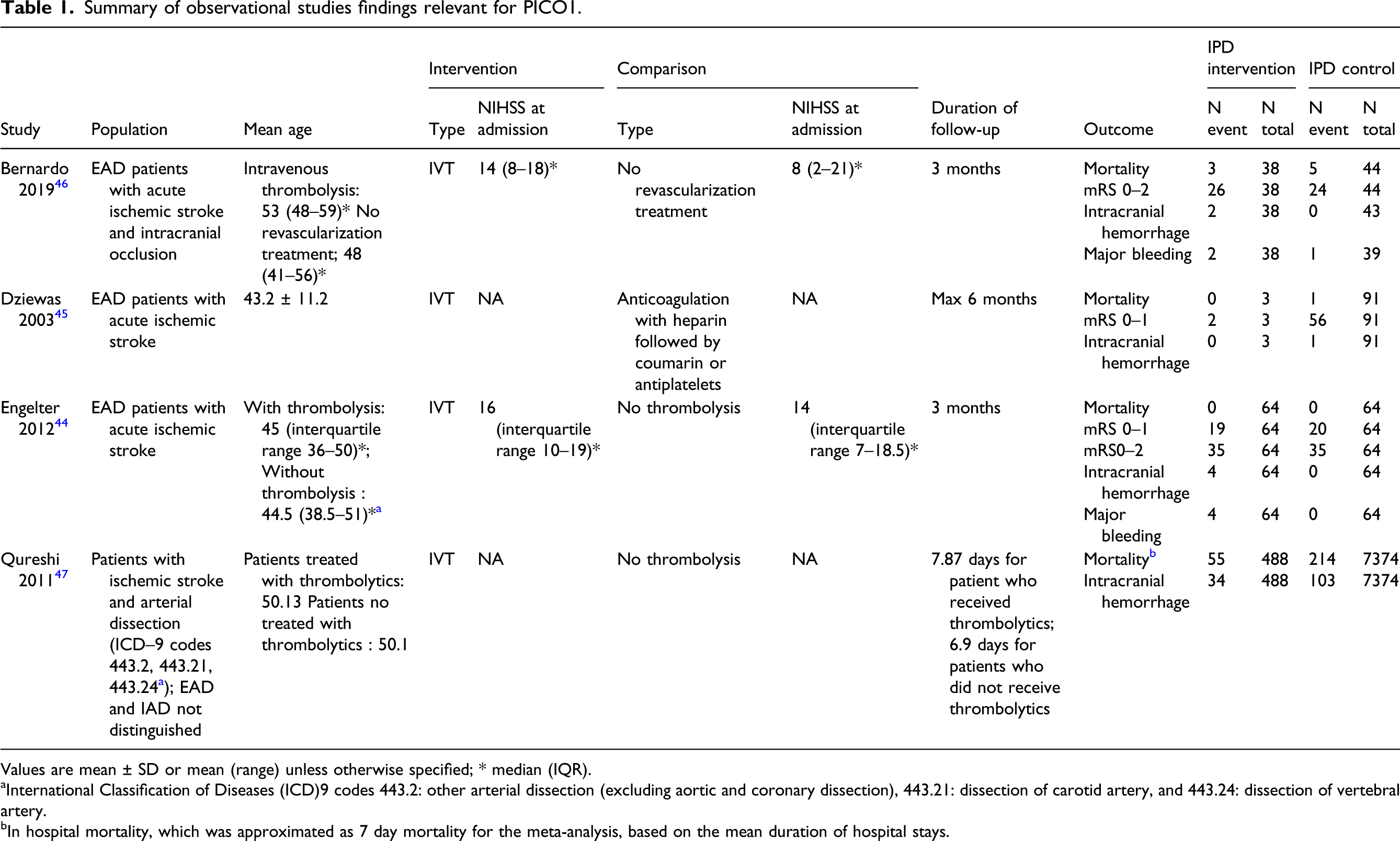
Mortality was assessed at 3 months for three studies,44-46 and seven days for two studies,45,47 of which three contributed to the meta-analysis, due to a lack of events in two studies: Overall, the meta-analysis showed no difference between the use of IVT compared to no-IVT treatment on mortality (OR, 1.95 [95% CI, 0.32–11.99]; p = 0.47; I2 = 83%; Figure 2(a)).45-48 At 7 days,47,49 mortality was significantly higher in EAD/IAD patients who received IVT compared to those who didn’t (OR, 4.16 [95% CI, 3.06–5.65]; p ≤ 0.001; I2 = 0%; Figure 2(b)). This result was largely driven by the NIS based on electronic health records.
47
In this study, patients with arterial dissections receiving IVT had a higher rate of medical co-morbidities, adjunctive procedures, and medical complications, compared to patients with dissection not receiving IVT. This study also included patients with ischemic stroke unrelated to arterial dissection, with (N = 47,411) and without IVT (N = 2,964,253) and, among all patients with ischemic stroke, there was no significant interaction between dissection and thrombolytic treatment for predicting in-hospital mortality (p = 0.78). (a) Meta-analysis of effects of intravenous thrombolysis in observational studies on mortality at 3 months. (b) Meta-analysis of effects of intravenous thrombolysis in observational studies on mortality at 7 days.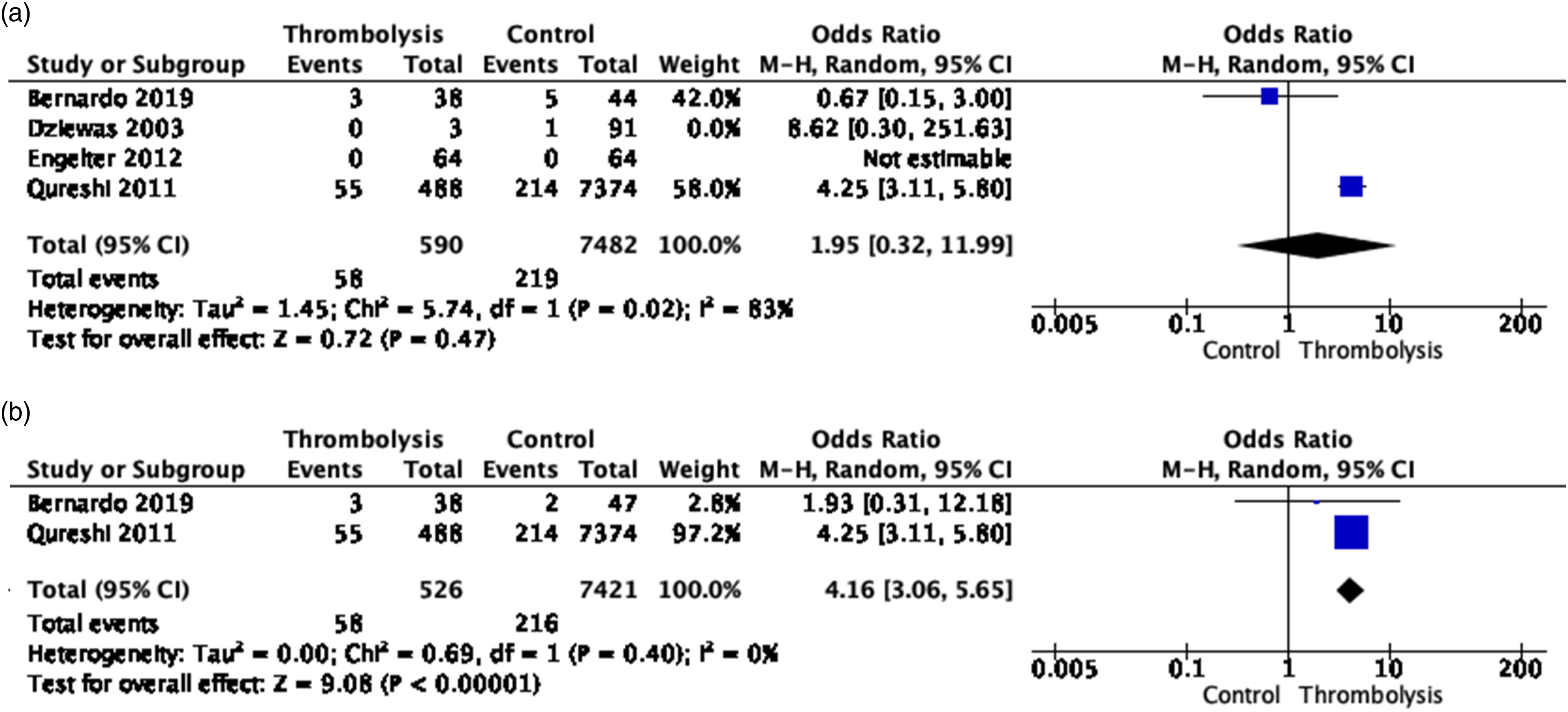
Regarding functional outcome (105 and 199 EAD patients with and without IVT),44-46 there were no differences between IVT and no-IVT patients, both using the endpoint excellent functional outcome (mRS 0–1 vs. 2–6; OR, 0.95 [95% CI, 0.46–1.96]; p = 0.90; I2 = 0%; Figure 3(a))44,45 and good functional outcome (mRS 0–2 vs. 3–6; OR, 1.19 [95% CI, 0.70–2.01]; p = 0.52; I2 = 0%; Figure 3(b))44,46,48 at 3 months. NIHSS at admission was higher in EAD patients with than those without IVT (Table 1).44,46 (a) Meta-analysis of effects of intravenous thrombolysis in observational studies on excellent functional outcome (mRS 0–1 vs. mRS 2–6) at 3–6 months. Functional outcome was assessed after a maximum of 6 months in Dziewas et al,
45
and at 3 months in Engelter et al.
44
. (b) Meta-analysis of effects of intravenous thrombolysis in observational studies on good functional outcome (mRS 0–2 vs. mRS 3–6) at 3 months.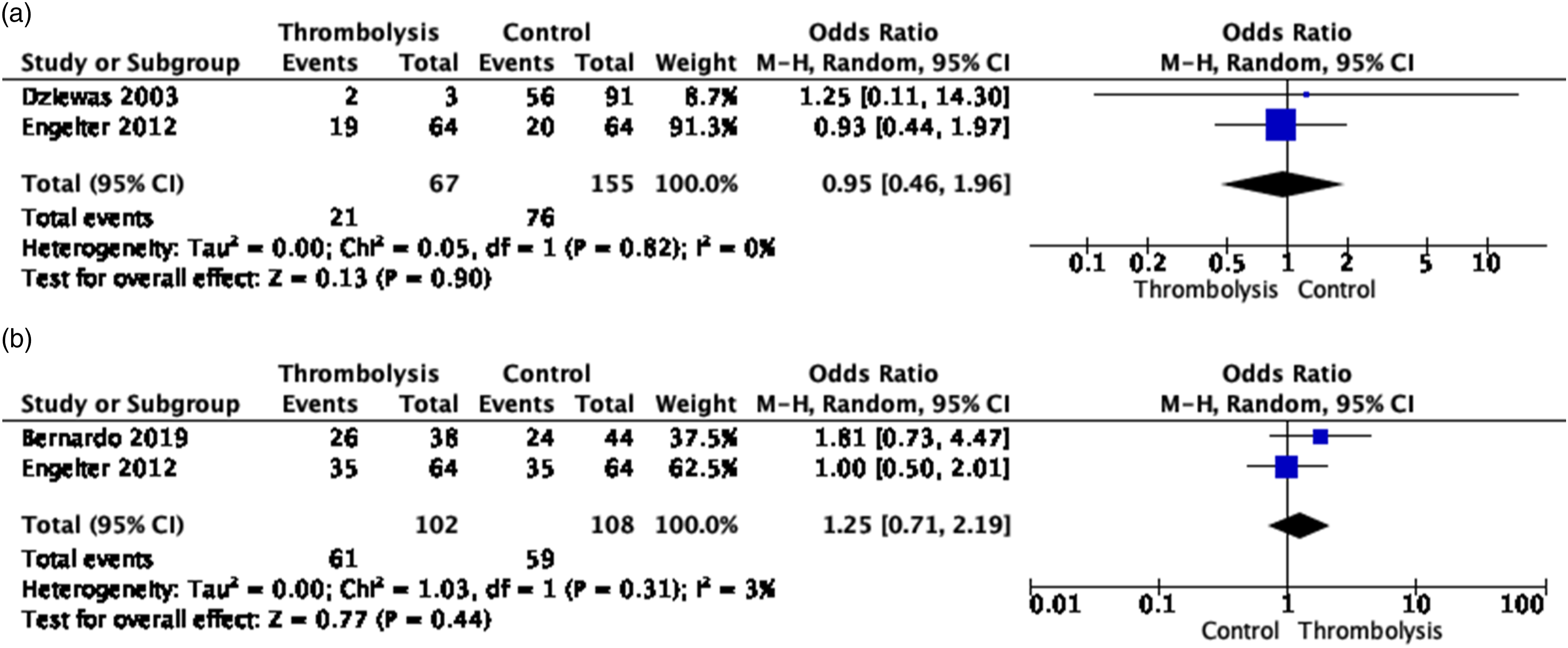
Finally, IVT with alteplase was found to increase the odds of intracranial hemorrhage (OR, 5.35 [95% CI, 6.62–7.92], p < 0.00001, I2 = 0%, Figure 4(a)), which became non-significant after removing the NIS study that likely included a mix of EAD and IAD cases and was based on electronic health records only (OR, 7.64 [95% CI, 0.91–63.86]; p = 0.08; I2 = 0%; Figure 4(b)).44-46,48 There was no significant association with major bleedings (OR, 3.92 [95% CI, 0.60–25.66]; p = 0.15; I2 = 0%; Figure 5).44,46 (a) Meta-analysis of effects of intravenous thrombolysis in observational studies on the risk of intracranial hemorrhage. (b) Meta-analysis of effects of intravenous thrombolysis in observational studies on the risk of intracranial hemorrhage, without the NIS study.
47
Meta-analysis of effects of intravenous thrombolysis in observational studies on the risk of major bleedings.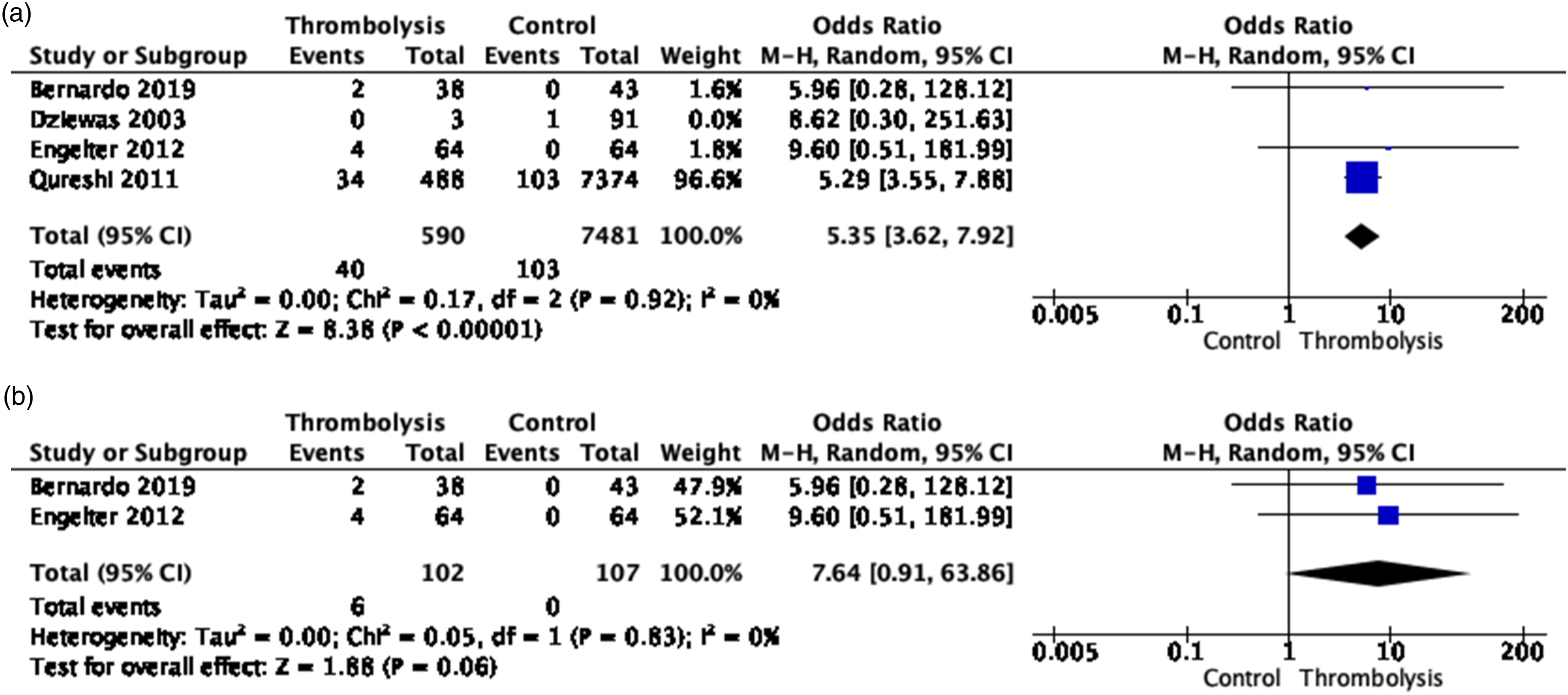

Quality of results in observational studies relevant for PICO1.
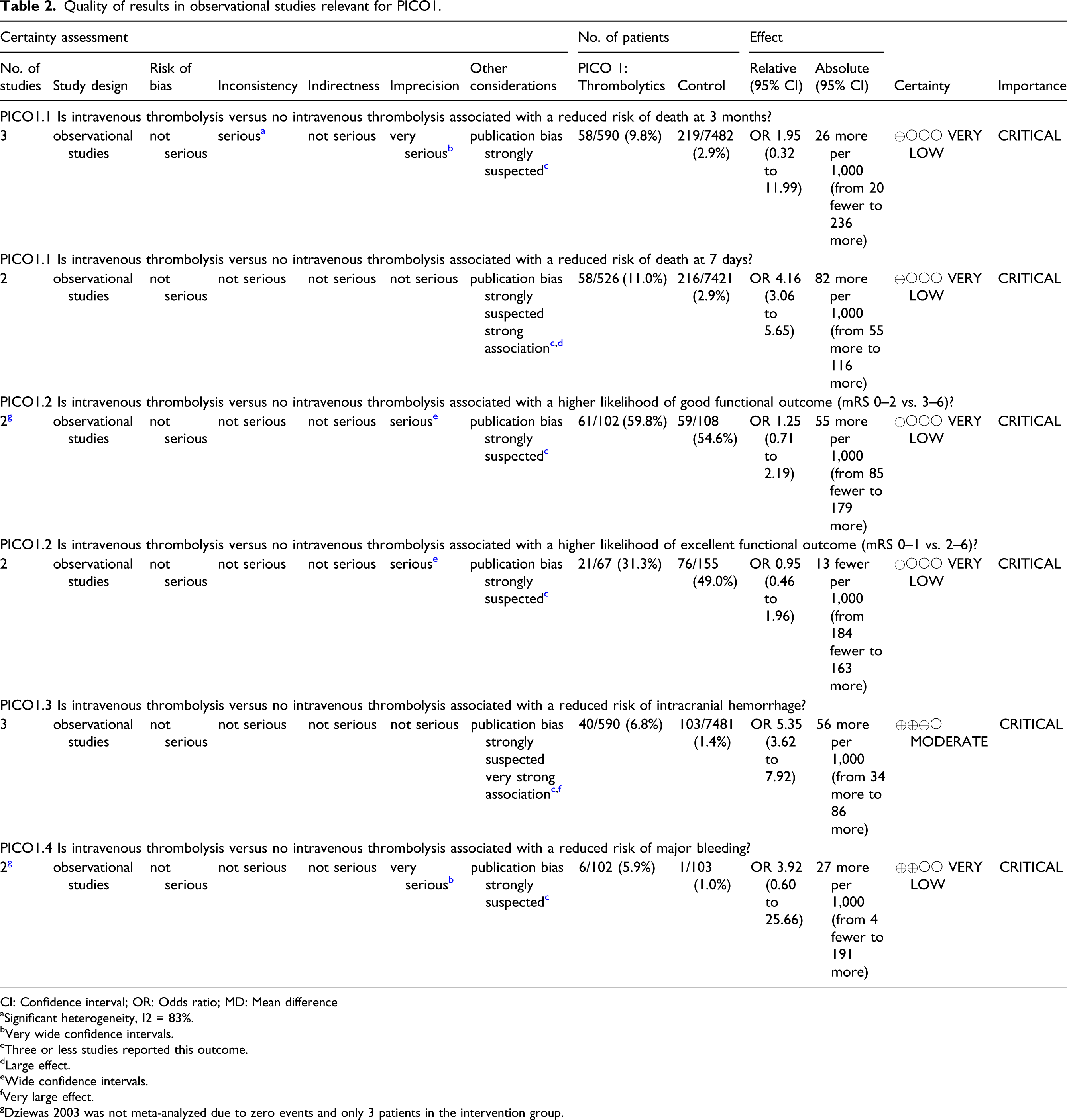
CI: Confidence interval; OR: Odds ratio; MD: Mean difference
aSignificant heterogeneity, I2 = 83%.
bVery wide confidence intervals.
cThree or less studies reported this outcome.
dLarge effect.
eWide confidence intervals.
fVery large effect.
gDziewas 2003 was not meta-analyzed due to zero events and only 3 patients in the intervention group.
The high rate of cervical internal carotid artery occlusions and associated supra-clinoid internal carotid artery (tandem) occlusions seen in patients with underlying dissection could potentially, partly, account for the apparent lack of benefit with IVT.44,46 However, the results are very difficult to interpret in this observational setting where EAD/IAD patients undergoing IVT were more severe than EAD/IAD patients not receiving IVT, as explained above.
In this context, it is important to consider studies that compared patients with EAD and ischemic stroke treated with IVT to patients with non-EAD ischemic stroke treated with IVT. In the Safe Implementation of Thrombolysis in Stroke International Stroke Thrombolysis Register (SITS-ISTR), compared with non-EAD ischemic stroke patients matched for age and stroke severity, EAD patients receiving thrombolytic therapies (180 patients of whom 67% received IVT and 33% intra-arterial thrombolysis) showed no significant differences in terms of safety and prognosis. 50 In particular, only one patient with an intramural hematoma expansion after IVT treatment was reported, who had an excellent outcome. In the NIS study, 47 no increase in the principal safety end point of post-thrombolytic intracranial hemorrhage was observed between EAD/IAD ischemic stroke patients and ischemic stroke patients without dissection. The lack of interaction between IVT and dissection on the risk of death and the absence of excessive rates of post-thrombolytic hemorrhages suggested the use of thrombolytic treatment in EAD/IAD patients was not subject to safety concerns. 47 This is in line with results from the Swiss IVT databank, 51 where 55 EAD patients undergoing IVT were compared with 1007 IVT-treated ischemic stroke patients without EAD. Intracranial hemorrhages were equally frequent in EAD (14%) and non-EAD patients (14%, p = 0.99), and recurrent ischemic strokes occurred in 1.8% of EAD patients and in 3.7% of non-EAD patients (p = 0.71). These findings are also supported by those of a recent prospective multicenter study and a meta-analysis of data from patients with dissection-related ischemic stroke treated with IVT, which confirmed that the risk of ICH in these patients is overall quite low (2% in the meta-analysis), while an excellent functional outcome (mRS 0–1 at hospital discharge) was observed in 41% of patients. 52
Thus, despite the low level of evidence and the limited data available, considering the overwhelming evidence of a benefit during the acute phase of ischemic stroke in general, and in line with a recent ESO guideline on IVT, 31 we believe that the treatment of EAD-induced acute ischemic stroke using IV alteplase within 4.5 hours of onset is safe.
Of note, in the previously published recent ESO IVT guideline, 31 the authors decided not to perform a meta-analysis of observational studies comparing EAD patients with IVT versus no IVT due to notable differences in study design, important risk of selection bias and confounding by indication. As study selection is specific to each ESO guideline, slightly different study inclusion criteria were used in the IVT and in the present dissection guideline. In the absence of RCTs for EAD/IAD except for PICO5, our MWG had indeed decided to analyze and critically interpret all available evidence, as described above. Importantly, our conclusion and evidence-based recommendation regarding use of IVT in EAD patients is the same as in the ESO IVT guideline. 31
Additional information
Even more than for EAD, the management of IAD is controversial because RCTs and large observational studies are not available. 13 Only anecdotal reports (case reports or small case series of fewer than 10 patients) have been published on the safety and efficacy of IVT in patients with IAD presenting with acute ischemic stroke.49,53,54 The scarce information available, therefore, does not allow conduction of a meta-analysis. In a consecutive single-center series of 181 EAD/IAD ischemic stroke patients, 49 10 were due to IAD and five of these received IVT. Among these, there were no cases of SAH nor symptomatic ICH after IVT. One patient had an asymptomatic hemorrhagic infarct type 1 and two patients died within 7 days from ischemic mass effect. The other three patients had favorable clinical outcomes at 3 months. 49
By contrast with extracranial arteries, intradural arteries are characterized by a well-developed internal elastic lamina, a paucity of elastic fibers in the media, little adventitial tissue, and no external elastic lamina. 11 These features, and weaker supporting tissues than cervical arteries, 12 may make intracranial arteries increasingly more prone to bleeding than extracranial arteries. Based on these observations, there is an obvious theoretical concern that IAD may result in sub-adventitial extension of the hematoma and increase the risk of SAH (especially when located in the posterior circulation) or that brain ischemia might progress to a hemorrhagic transformation as a consequence of thrombolysis, which has made many clinicians reluctant to use IVT in known or suspected IAD. 55 It should be noted, however, that the pathognomonic radiological findings of IAD (mural hematoma, intimal flap, and double lumen) are not easily detectable, especially in the hyperacute phase of the disease. In most cases, as described in the introduction, the definite diagnosis of IAD needs the combination of arterial wall and lumen imaging and also the comparison between baseline and follow-up imaging. This implies that, in clinical practice, the scenario in which the neurologist must decide whether or not to administer IVT in a patient with acute ischemic stroke because of a definite diagnosis of IAD is extremely uncommon.
The recent ESO guideline on IVT
31
suggested to refrain from IVT in IAD patients with acute ischemic stroke (approved by 6 of 9 group members). We believe that caution is warranted in patients with a suspected diagnosis of IAD. Indeed, IAD diagnosis is only very rarely confirmed in the time window for IVT in acute ischemic stroke patients. There is no evidence in the current literature that IVT in IAD patients without SAH is harmful and we fear that systematically refraining from IVT in patients with a suspicion of possible IAD may lessen the chances of ischemic stroke patients of benefiting from an efficient therapy. Therefore, we suggest that in patients with an acute ischemic stroke suspected to be caused by IAD, IVT should probably not be withheld after ruling out subtle signs of SAH on initial brain imaging. Our expert consensus statement is not in contradiction with the expert consensus statement of the IVT guideline that focused on the rare situation of patients with a confirmed diagnosis of IAD with 4.5 hours of ischemic stroke onset. Evidence-based recommendation In patients with symptomatic EAD with acute ischemic stroke within 4.5 hours of onset, we suggest using IVT with alteplase, if the standard inclusion / exclusion criteria are met. Quality of evidence: Low ⊕ ⊕ Strength of recommendation: Weak for an intervention ↑? In patients with symptomatic IAD with acute ischemic stroke within 4.5 hours of onset, there is insufficient data to provide a recommendation. Quality of evidence: Very low ⊕ Strength of recommendation: - Expert consensus statement In patients with an acute ischemic stroke suspected to be caused by IAD, all but one expert suggest that IVT should be considered, after ruling out standard contra-indications, including subtle signs of subarachnoid bleeding on brain imaging.
PICO 2: In extracranial artery dissection (EAD) & intracranial artery dissection (IAD) patients with acute ischemic stroke is endovascular treatment (stenting and/or thrombectomy) versus no endovascular treatment (with or without IV thrombolysis) associated with a reduced risk of death, a higher likelihood of favorable functional outcome (mRS 0–2 vs 3–6, or 0–1 vs 2–6, or equivalent), and no increased risk of ICH, or SAH?
Analysis of current evidence
No randomized controlled trial was available to address this PICO question. After exclusion of single-arm studies and systematic reviews, we identified five comparative observational studies including 463 EAD patients that met our inclusion criteria (190 patients with EVT and 373 with no EVT or [in 71 patients] without the primary EVT of interest [in that case carotid stenting]; Figure 6 and Table 3).46,48,56-58 No study on this question in IAD was identified. PRISMA flow chart of study selection for PICO2. “Wrong study design, setting, intervention, outcomes, and (patient) population” in COVIDENCE corresponds to studies that do not match criteria for this PICO Summary of findings from observational studies relevant for PICO2. * Several endovascular techniques were used, including intra-arterial thrombolysis (n = 1, 4.2%), thrombectomy with stent-retriever (n = 17, 70.8%), thromboaspiration (n = 8, 33.3%), angioplasty (n = 7, 29.2%), and cervical stent placement (n = 11, 45.8%). Most patients (n = 13, 54.2%) had more than one technique for EVT procedure. aSeveral endovascular techniques were used: the majority of patients had multiple IAT techniques, including thrombectomy (n = 19), IA thrombolysis (n = 17), stenting (n = 14), and angioplasty (n = 7); 11 patients were also treated with IVT. b. The comparison group here comprised patients with EAD not receiving intra-arterial thrombolysis (n = 137, of whom 11 received IVT)). cSeveral endovascular techniques were used, including mechanical thrombectomy with devices available 2007–2012 (stent retrievers), thrombus aspiration, or percutaneous transluminal angioplasty; intra-arterial application of urokinase or tissue plasminogen activator (tPA) as well as intracranial or extracranial stent placement was performed in selected patients.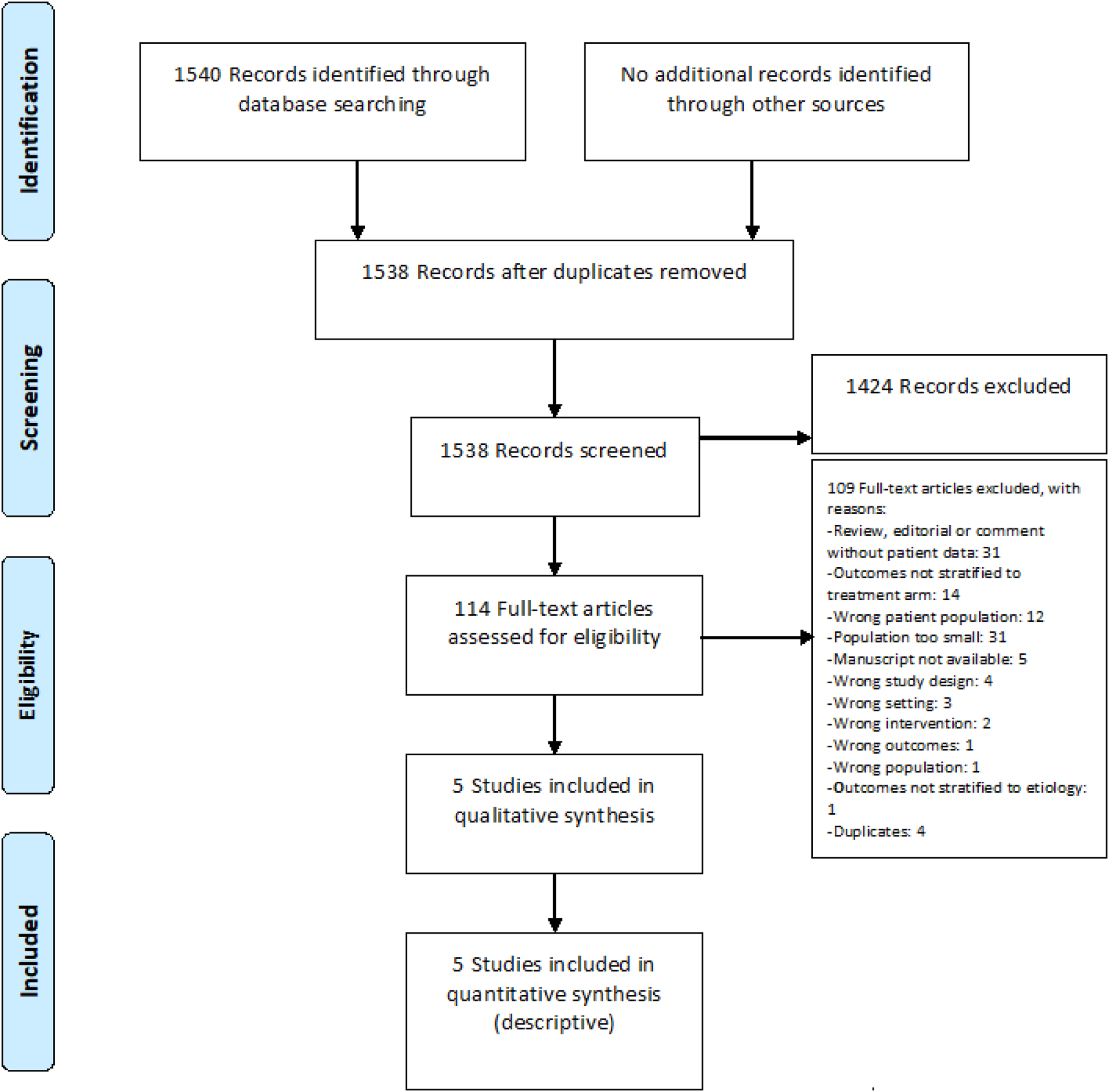
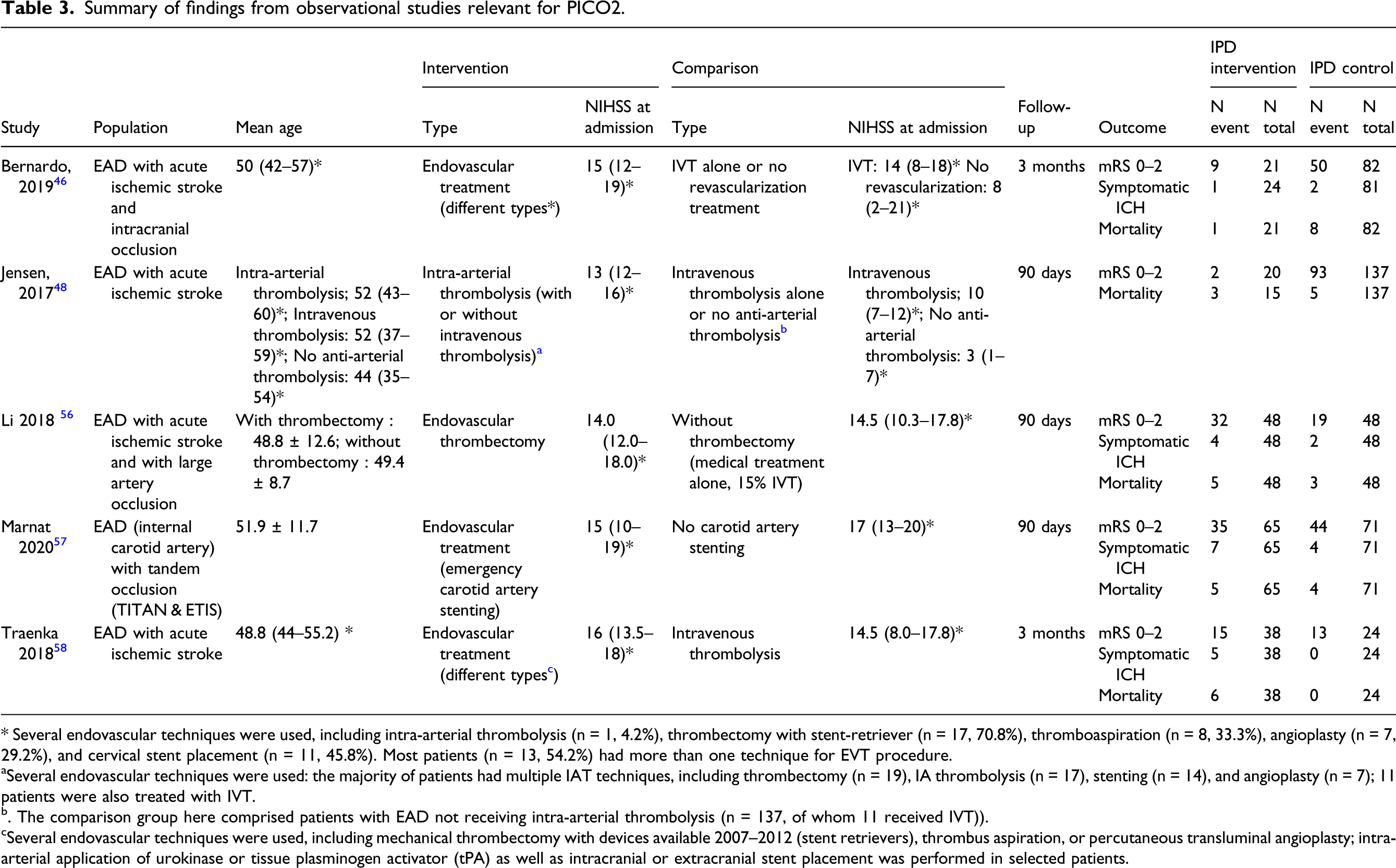
Of note, two steps in EVT need to be considered: intracranial clot removal (i.e., mechanical thrombectomy [MT]) and management of the EAD lesion and related stenosis. Most of the identified studies focused predominantly on the first step. Different types of EVT were used in the five identified observational studies. One study (48/48 EAD patients with/without intervention) focused on EVT with MT only compared with medical treatment and did not describe if adjunct procedures were used. 56 One study included only EAD patients undergoing EVT (the strategy of which was left to the discretion of the interventionist) and compared EAD patients in whom the EVT included carotid artery stenting to EAD patients undergoing EVT without carotid stenting (65/71). 57 Finally, three studies used mixed endovascular approaches,46,48,58 with mostly more than one technique per procedure (comparing in total 77/254 patients with/without EVT). A majority of patients in these studies underwent MT with stent retrievers, other interventions included intra-arterial thrombolysis, thrombus aspiration, percutaneous transluminal angioplasty, and cervical stent placement (45.8% of patients in one of the studies 46 ). In these studies, it was difficult to identify patients who only had one technique or a combination of these.
The meta-analysis conducted on these five EAD studies46,48,56-58 showed similar odds ratio (OR) for good functional outcome (mRS 0–2 or good recovery on Glasgow Outcome Scale), OR, 0.56 [95% CI, 0.19–1.59], I2 = 84%, p = 0.27, Figure 7) after EVT compared to no EVT. This finding is in accordance with a previous meta-analysis,
58
which included 8 studies and 212 patients (110 IVT and 102 EVT [including smaller studies than allowed in our inclusion criteria (Methods)]), showing no significant difference between the two therapeutic approaches (OR for good functional outcome, mRS 0–2, 0.97 [95% CI, 0.38–2.44]), despite the fact that EVT was associated with higher rates of recanalization (respectively, 84.2% for EVT vs. 66.7% for IVT; OR, 3.2 [95% CI, 0.9–11.38]) in that study.
58
Of note, the difference in NIHSS between patients treated with EVT and those who were not, in three of the five studies included in our meta-analysis,46,48,58 shows that EVT was performed in patients with more severe strokes and represents, therefore, an important selection bias (Table 3). The study by Li et al. that applied propensity score matching of 48 EAD patients undergoing EVT with 48 EAD patients without EVT, enabling a similar severity profile in both groups (Table 3), is the only study that showed a superiority of EVT, with 66.7% versus 39.6% of patients reaching a good functional outcome at 90 days (p = 0.008).
56
Meta-analysis of effects of endovascular treatment in observational studies on good functional outcome (mRS 0–2 vs. 3–6) at 3 months.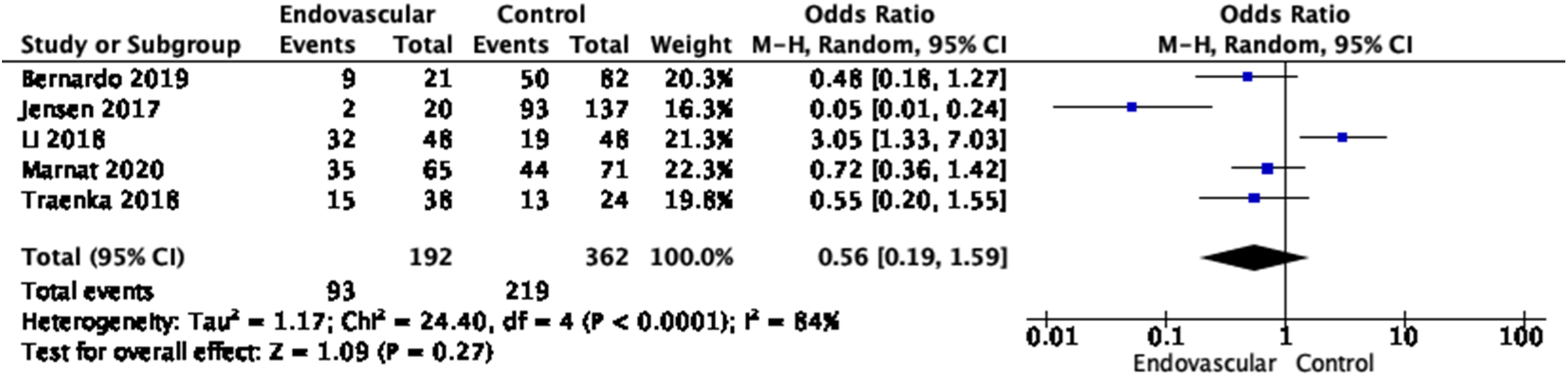
Of note, in the study by Marnat et al., 57 on the databases of Endovascular Treatment in Ischemic Stroke (ETIS) and Thrombectomy in Tandem Lesion (TITAN),59,60 including 65 EAD patients treated with emergency carotid stenting and 71 with EVT without stenting, EVT with EAD stenting was associated with greater rates of successful reperfusion (adjusted OR [aOR], 2.24 [95% CI, 1.33–2.77]). However, in sensitivity analyses restricted to patients with successful reperfusion, EVT with EAD stenting was not associated with improved rates of favorable outcome (aOR, 0.70 [95% CI, 0.45–1.08]), as in the overall group (Figure 7).
With respect to safety, EVT in EAD was associated with a non-significant increased risk of all symptomatic ICH (OR, 2.27 [95% CI, 0.92–5.61], I2 = 0%, p = 0.08, Figure 8). Previous lines of evidence showed a trend towards more ICH in the EVT group (20.5% vs. 5.3%, p = 0.072), but not symptomatic ICH (sICH, 4.2% vs. 5.3%, p = 0.669).
46
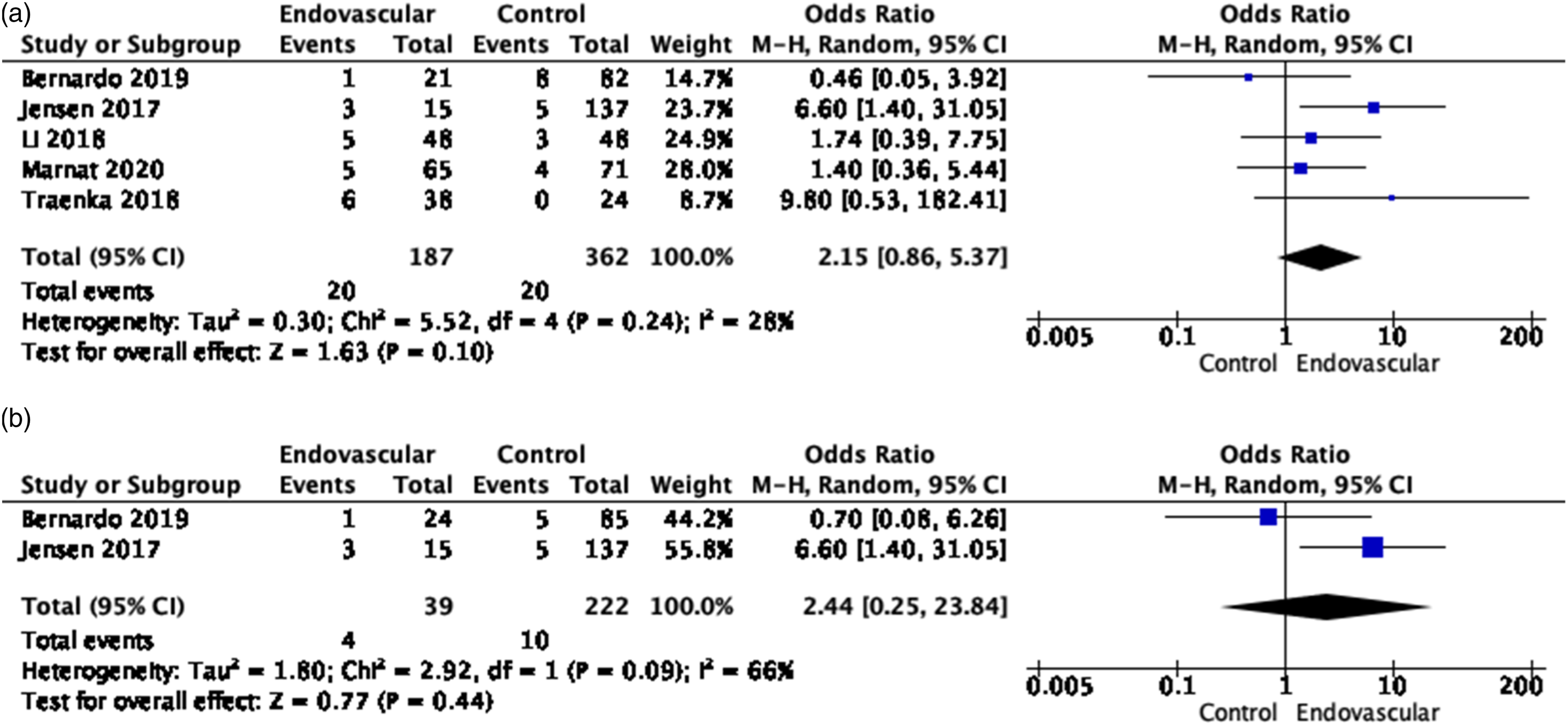
Of note, Traenka et al. and Bernardo et al. reported sICH nearly solely among EVT patients who had bridging therapy with IVT (80–100% of the cases).46,58 Mortality did not differ significantly between EVT and non EVT-treated patients overall (OR, 2.15 [95% CI, 0.86–5.37], I2 = 28%, p = 0.10, Figure 9), and at 7 days (OR, 2.44 [95% CI, 0.25–23.89], I2 = 66%, p = 0.44), Figure 9). Meta-analysis of effects of endovascular treatment in observational studies on risk of symptomatic ICH at 3 months. (a) Meta-analysis of effects of endovascular treatment in observational studies on mortality, at 3 months. (b) Meta-analysis of effects of endovascular treatment in observational studies on mortality at 7 days.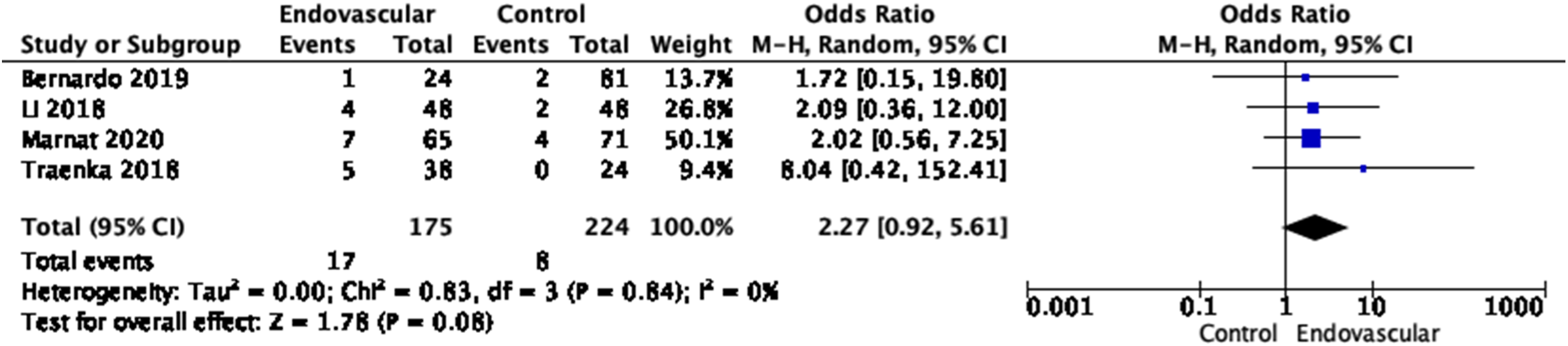
Quality of results in observational studies relevant for PICO2.
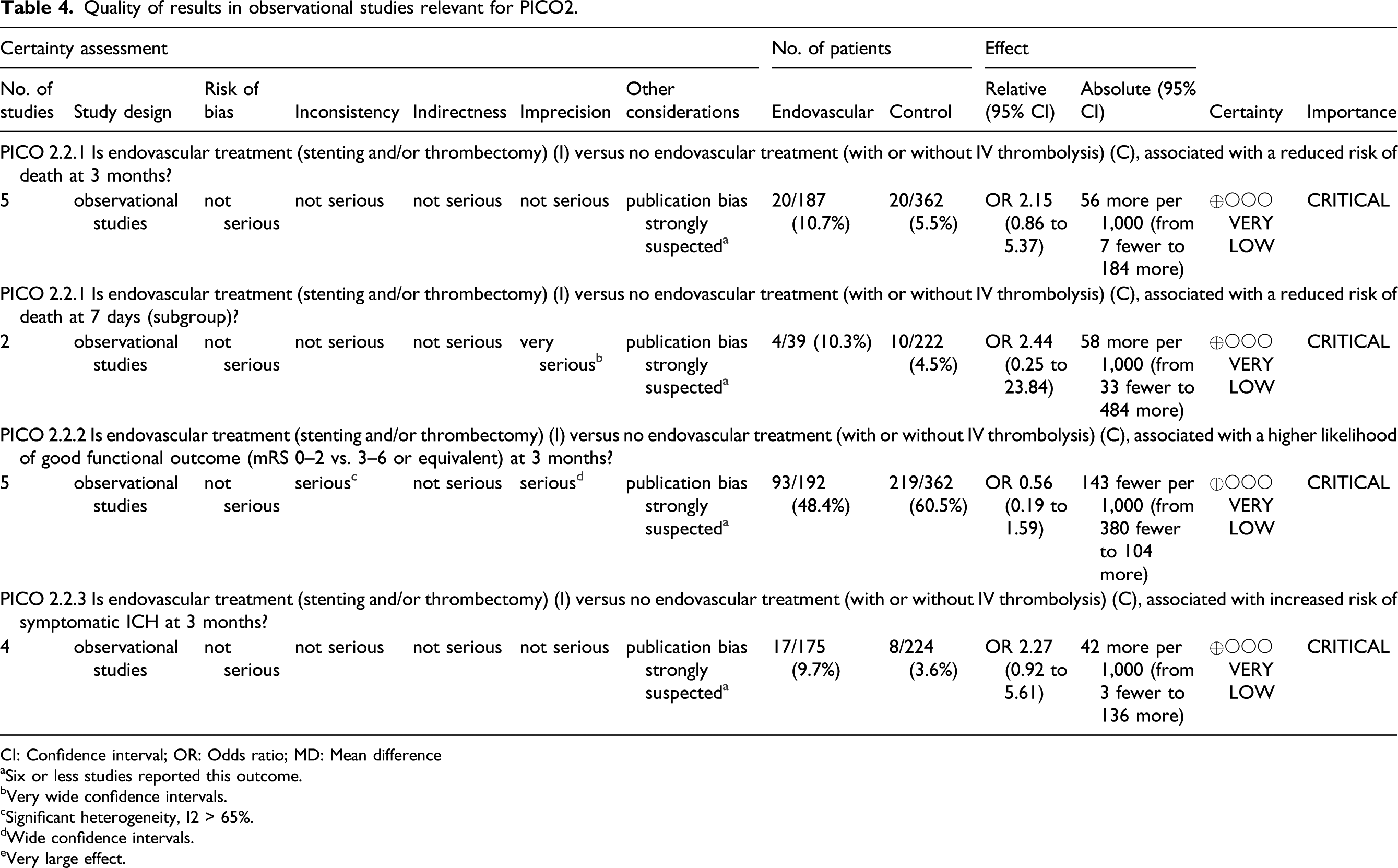
CI: Confidence interval; OR: Odds ratio; MD: Mean difference
aSix or less studies reported this outcome.
bVery wide confidence intervals.
cSignificant heterogeneity, I2 > 65%.
dWide confidence intervals.
eVery large effect.
EVT with MT plus best medical management over best medical management alone is recommended for clot extraction to improve functional outcome in adults with anterior circulation large vessel occlusion-related acute ischemic stroke, 61 irrespectively of the presence of a dissection. Previous ESO/ESMINT guidelines on MT have not addressed the specific situation of EAD/IAD patients. 61 Of note, based on a large single-center dataset of 445 consecutive patients receiving EVT (i.e., MT, IA thrombolysis, stent, and angioplasty), Jensen and collaborators compared the outcome between 24 EAD patients and 421 patients with another cause of acute ischemic stroke. 48 There was no significant difference in the odds of a good functional outcome (mRS 0–2) at 90 days between the two groups, accounting for differences in age and stroke severity. 48 Similarly, in the prospective, multicenter Prognostic Factors Related to Clinical Outcome Following Thrombectomy in Ischemic Stroke (RECOST) study, the rate of good functional outcome (mRS 0–2) was similar (as were recanalization rates) in 20 carotid EAD patients with tandem occlusion undergoing MT (±IVT) compared to 201 non-EAD patients with isolated intracranial large vessel occlusion. 62 In a more recent study, including the analysis of a database of 1422 acute ischemic stroke patients, with 43 EAD patients matched to 86 patients with other etiologies, safety and efficacy of EVT with MT were comparable in both groups: sICH and mortality rates were similar (OR, 0.85 [95% CI 0.21–3.49], p = 0.82; OR, 1.54 [95% CI 0.33–2.79], p = 0.58; OR, 0.18 [95% CI 0.02–1.46], p = 0.11, respectively), as well as rates of favorable functional outcome (OR, 1.26 [95% CI 0.61–2.64], p = 0.53). 63
Thus, despite the dearth and heterogeneity of (purely observational) data assessing EVT in EAD patients, considering the overwhelming benefit of MT in the setting of acute ischemic stroke with large vessel occlusion of the anterior circulation in general, we believe that the treatment of EAD-induced acute ischemic stroke with anterior circulation large vessel occlusion using MT is efficient and safe.
Additional information
The comparison between primary MT and bridging strategies of IVT immediately followed by MT in acute ischemic stroke patients with EAD is beyond the scope of this guideline but deserves special attention in future research and careful multidisciplinary assessment in current practice. As mentioned above, the few cases of sICH after MT were reported mostly among EVT patients who had bridging therapy with IVT and some authors have listed dissections as a factor potentially favoring primary MT. 64
Whether the EAD requires a specific EVT (e.g., angioplasty and stenting) before or after intracranial large vessel clot extraction remains to be determined. Treating the EAD lesion during the same procedure may be required in case of hemodynamic compromise (e.g., carotid occlusion with incomplete circle of Willis) or recurrent embolism during EVT. 65 Whenever possible, these complex cases should be discussed between the interventionalist and the neurologist, as the implantation of a stent requires a specific antithrombotic regimen (to prevent stent thrombosis that could cause ischemic stroke), with an increased bleeding risk in the setting of acute ischemic stroke.
For patients with IAD, beyond the bleeding risk inherent to the antiplatelet therapy needed by the stenting, the benefit-risk ratio of EVT (i.e., intracranial stenting) needs to be discussed also on the basis of the IAD location, considering anatomic specificities (e.g., occlusion risk of perforating arteries of the M1 segment of the middle cerebral artery). Evidence-based Recommendation In acute ischemic stroke patients with EAD and large vessel occlusion of the anterior circulation, we suggest using MT. Quality of evidence: Very low ⊕ Strength of recommendation: Weak for an intervention ↑? In acute ischemic stroke patients with IAD, there is insufficient data to provide a recommendation regarding the use of EVT. Quality of evidence: Very low ⊕ Strength of recommendation: - Expert consensus statement In acute ischemic stroke with EAD and large vessel occlusion of the anterior circulation, all but one expert suggest EVT (other than MT) for the treatment of the EAD lesion in case of carotid occlusion without patent circle of Willis or in case of recurrent embolism. In acute ischemic stroke with IAD and large vessel occlusion of the anterior circulation, all experts suggest EVT (other than MT) for the treatment of the IAD lesion at the hyperacute phase after assessing the risk/benefit ratio based on the location of the dissection and bleeding risk.
PICO 3: In patients with an intracranial dissecting aneurysm and a subarachnoid hemorrhage (SAH) does endovascular or surgical treatment of the aneurysm versus optimal medical treatment alone reduce the risk of SAH recurrence, ICH, death and increase the likelihood of favorable functional outcome (mRS 0–2 vs. 3–6, or 0–1 vs. 2–6, or equivalent)?
Analysis of current evidence
Summary of observational studies findings relevant for PICO3.
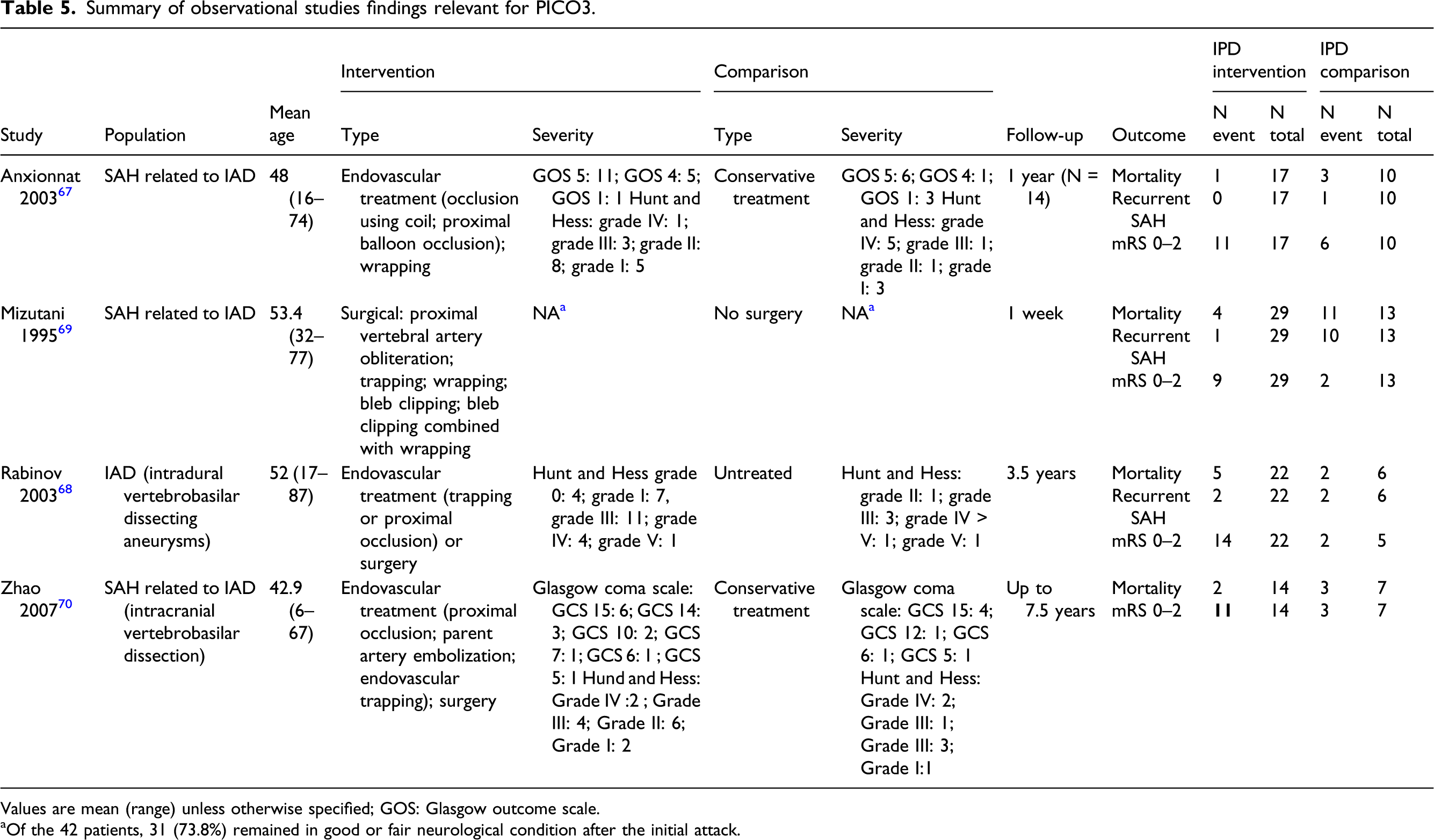
Values are mean (range) unless otherwise specified; GOS: Glasgow outcome scale.
aOf the 42 patients, 31 (73.8%) remained in good or fair neurological condition after the initial attack.
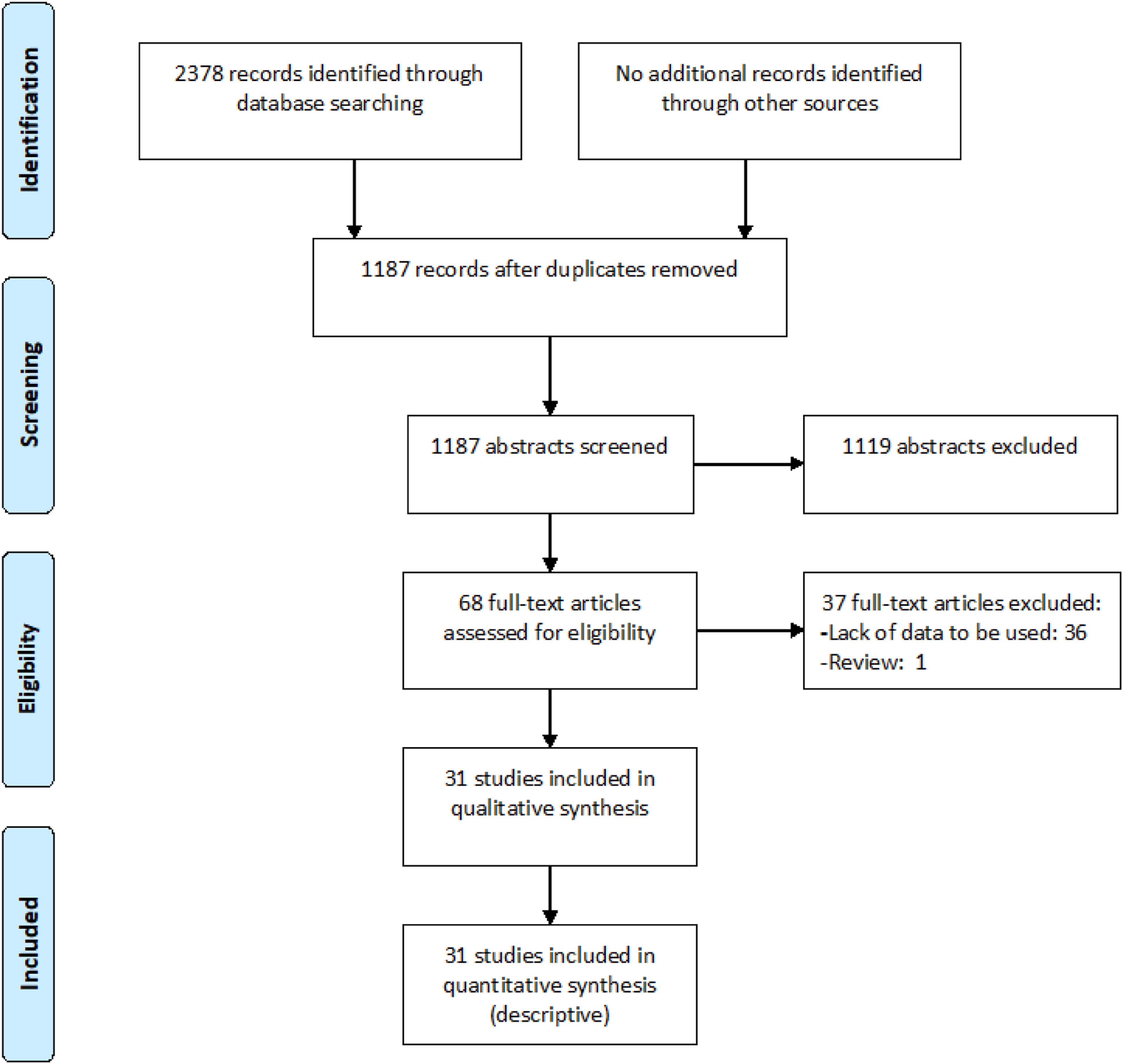
PRISMA flow chart of study selection for PICO3.
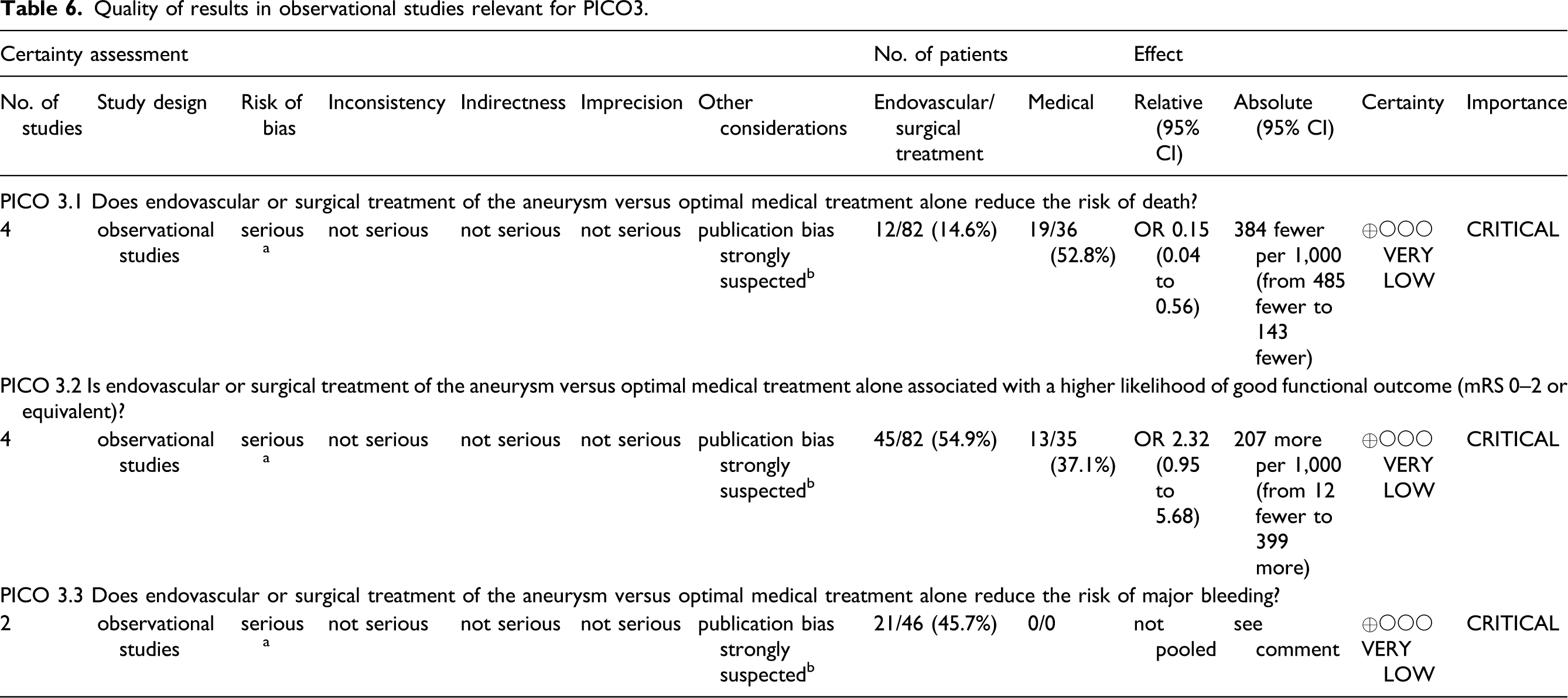
Quality of results in observational studies relevant for PICO3.

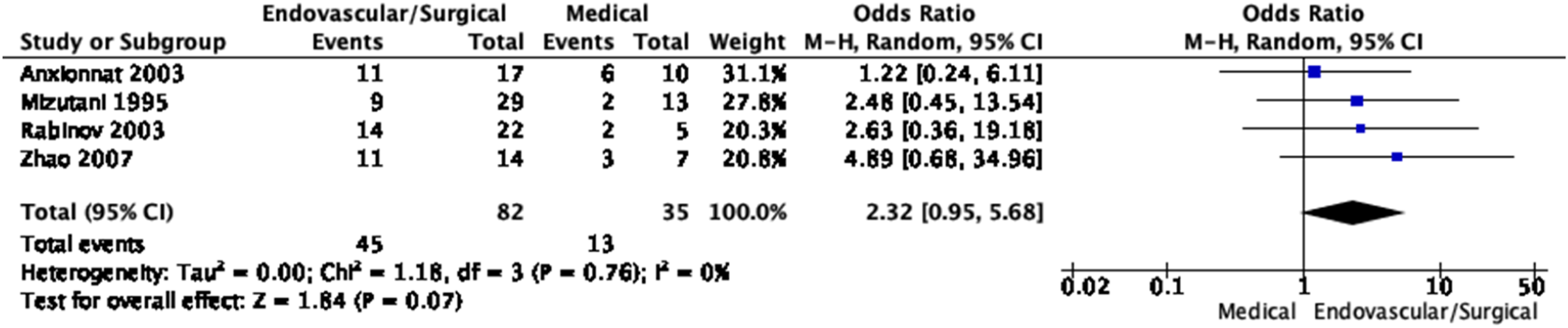
Meta-analysis of effects of endovascular or surgical treatment in observational studies on the risk of rebleeding (SAH recurrence).
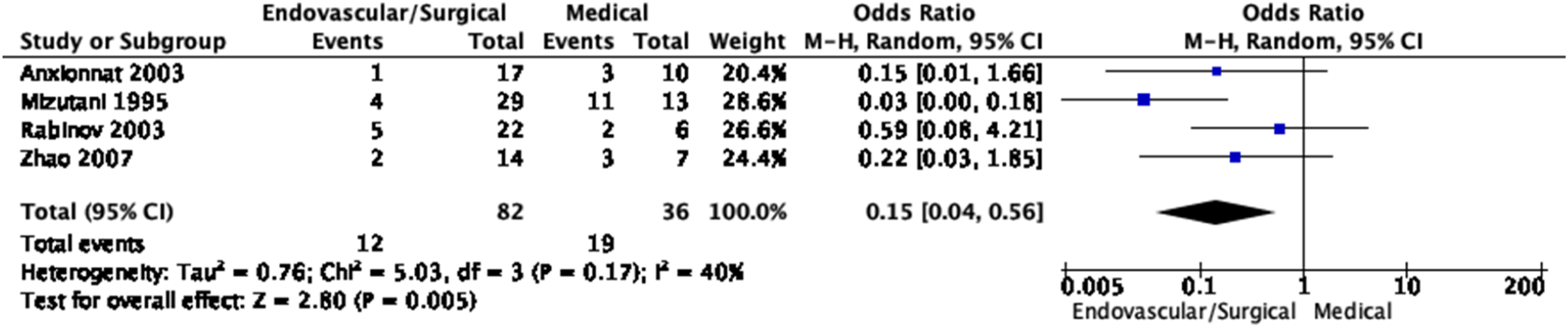
Meta-analysis of effects of endovascular or surgical treatment in observational studies on mortality. Anxionnat 2003 67 : deaths occurred in the acute or subacute phase; Mizutani 1995 69 : deaths occurred in the acute or subacute phase, the latest death occurred within a month; Rabinov 2003 68 : four of five deaths occurred in the initial hospital course, the last death occurred in a delayed fashion due to an unknown cause; Zhao 2007 70 : most deaths occurred in the acute or subacute phase, except one death that occurred at 16 months due to the rupture of another IAD.
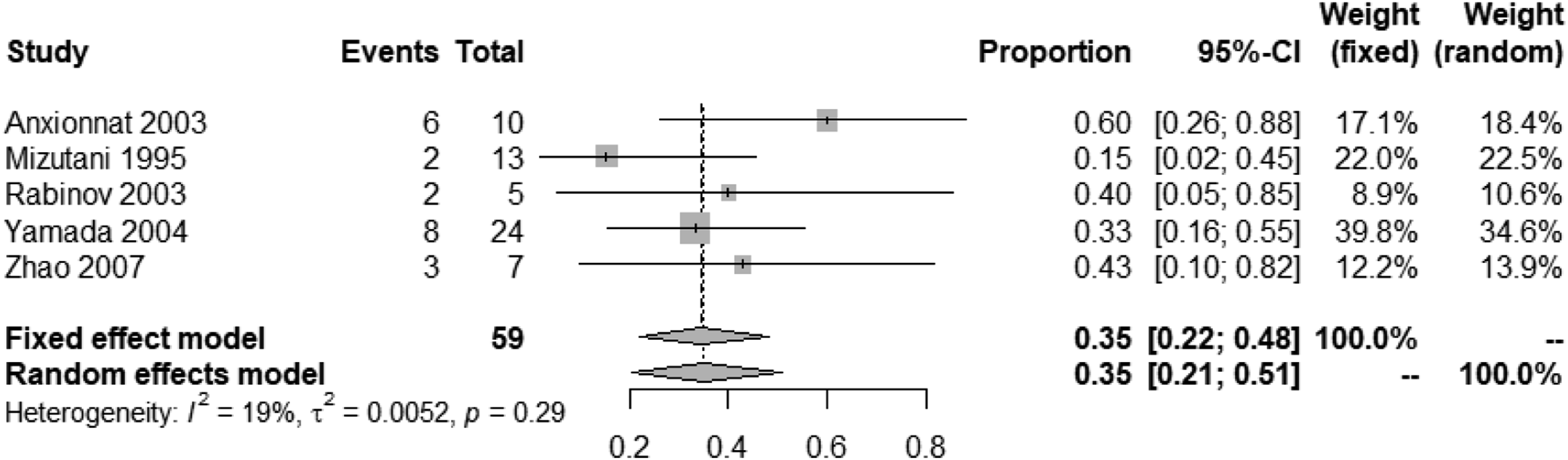
Meta-analysis of effects of endovascular or surgical treatment in observational studies on good functional outcome (mRS 0–2 vs. 3–6 or equivalent).
Additional information
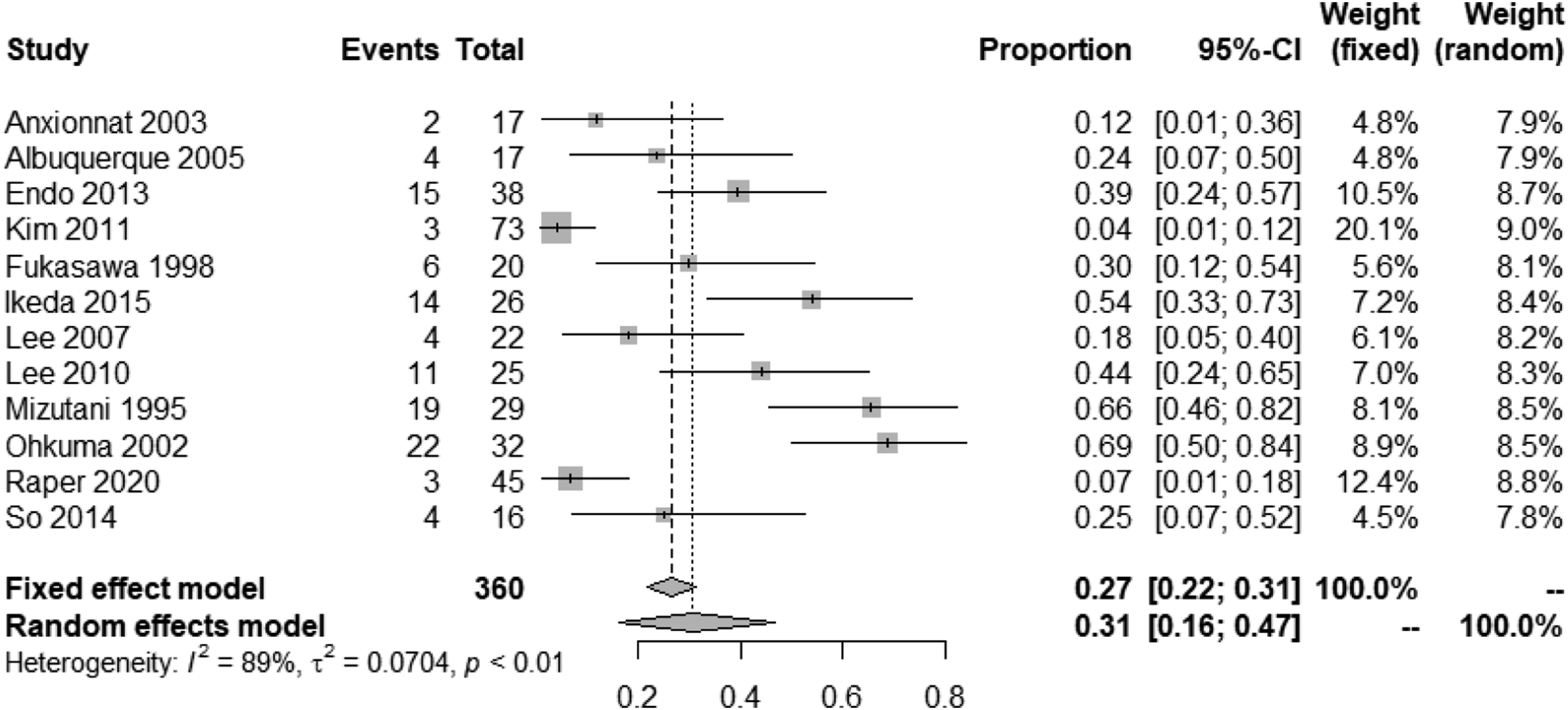
Due to the small number of comparative observational studies,67-70 we chose to also report the mean frequency of PICO3 outcomes across all identified observational studies (comparative and single-arm), by treatment group (endovascular/surgical or medical). In addition to the four comparative observational studies, twenty-three single-arm studies providing data regarding mortality, functional outcome, and SAH recurrence (rebleeding) rates were identified and included for descriptive analyses (one with medical treatment only 66 and all others with endovascular or surgical treatment only).66-92 In one study, medical and interventional management of cases was merged and both groups could not be unequivocally analyzed separately, this study was therefore only included in the analysis of the overall rebleeding rate. 93 Most studies were from Japan (11/27) followed by Korea (4/27), China (4/27), France (1/27), and USA (2/27). As there was important heterogeneity in the frequency of reported outcomes across studies, a random effects model was used to compute the mean frequencies.
The natural history and outcome of IAD-related SAH is similar to aneurysmal SAH. In identified studies, IAD with SAH was associated with a high mortality under medical treatment only, estimated on average at 55% (95% CI [34%–76%]) (Figure 14).66-70, 94,95 The strongest predictors of mortality are clinical condition on admission and rebleeding.
96
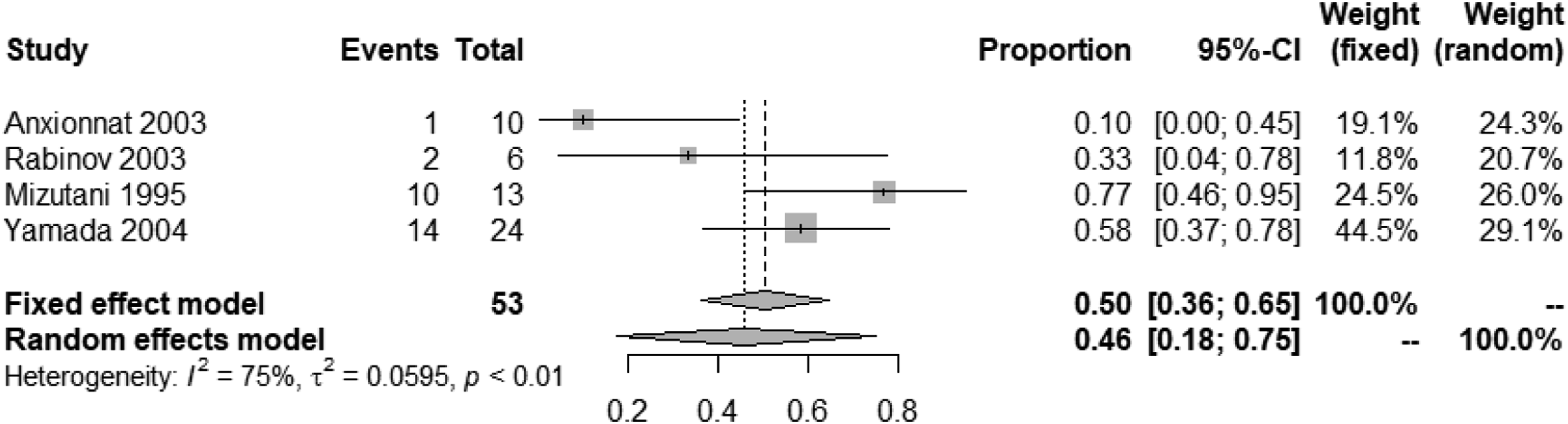
The rebleeding rate (SAH recurrence) was high (46%, 95% CI [18%–75%]) in the aforementioned studies (Figure 15).66-69 Most rebleedings occurred within the first hours to days after the initial event. In the unique study focusing on the outcome of patients managed conservatively by Yamada et al.,
66
most rebleeding occurred within the first 6 hours (10 out of 14) and the vast majority within the first 24 hours (13 out of 14). Eleven of the 14 patients who suffered rebleeding died.
66
In the study reported by Mizutani et al., 10 out of 13 patients treated conservatively suffered rebleeding and 6 died subsequently. Nineteen of 29 patients suffered rebleeding prior to intervention. Of the 30 patients with rebleeding, 17 occurred within the first 24 hours and 24 during the first week. Rebleeding was lethal in 47% of cases.
69
Mortality rate in IAD patients with SAH under medical treatment only. Rebleeding rate (SAH recurrence) in IAD patients with SAH under medical treatment only.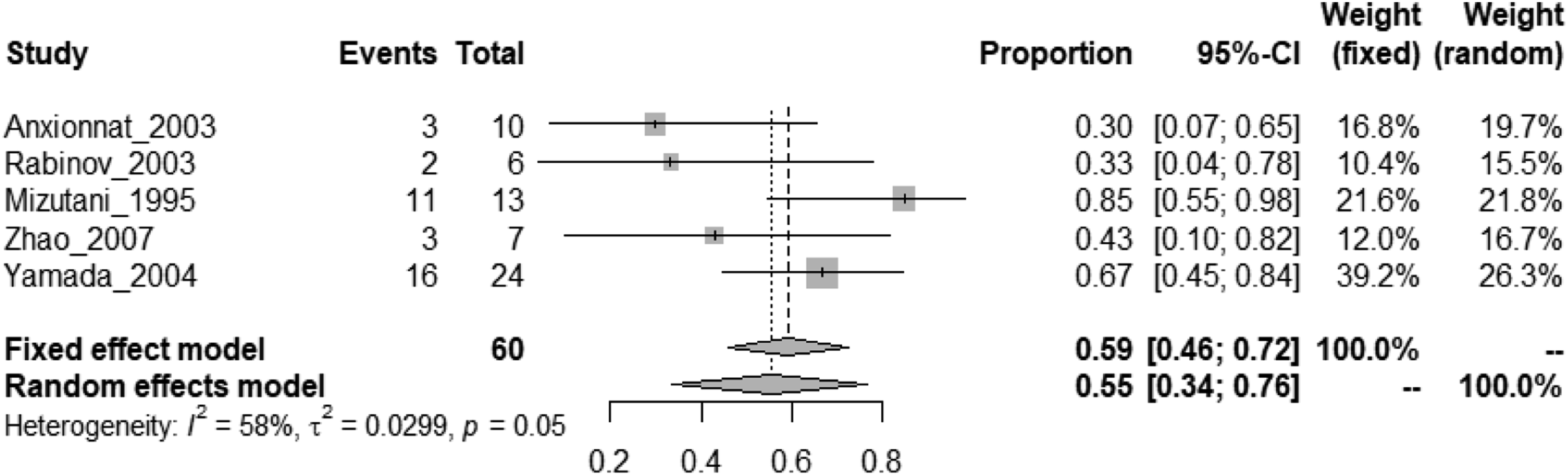
Management of patients with interventions reduced the rate of rebleeding to 32% (95% CI, 18%–48%) (Figure 16).67,69,71,72,74,77,81,84,87,91-93 Despite patients being allocated to interventions, 31% (95% CI, 16%–47%) of cases rebled prior to intervention (Figure 17),67,69,71,72,74,76,77,81,84,87,91,92 and only very few rebled after the lesion was secured (2%, 95% CI, 1%–4%) (Figure 18).67-69,71-75,77-79,81-92 Rebleeding rate (SAH recurrence) in IAD patients with SAH undergoing endovascular or surgical treatment. Rebleeding rate (SAH recurrence) in IAD patients with SAH undergoing endovascular or surgical treatment, prior to intervention. Rebleeding rate (SAH recurrence) in IAD patients with SAH undergoing endovascular or surgical treatment, after intervention.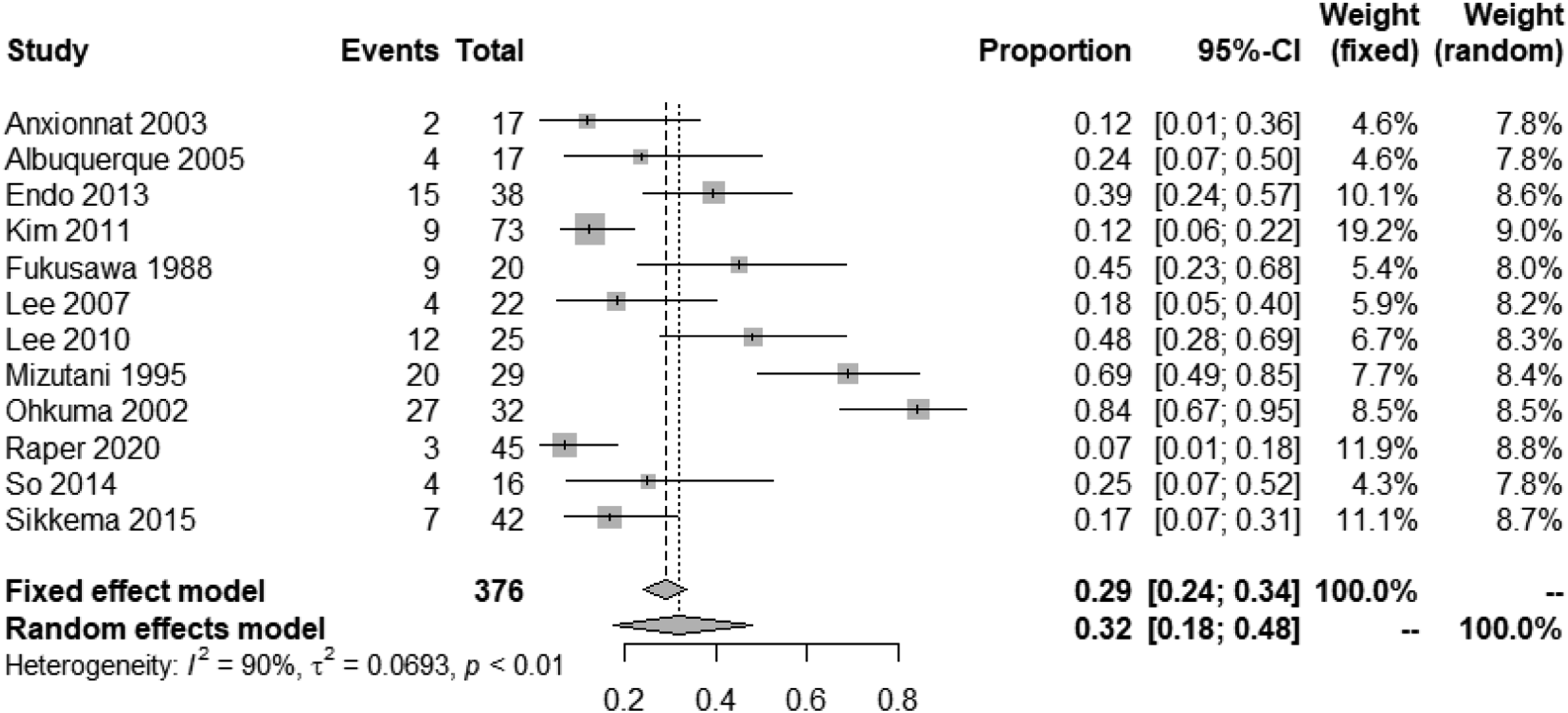
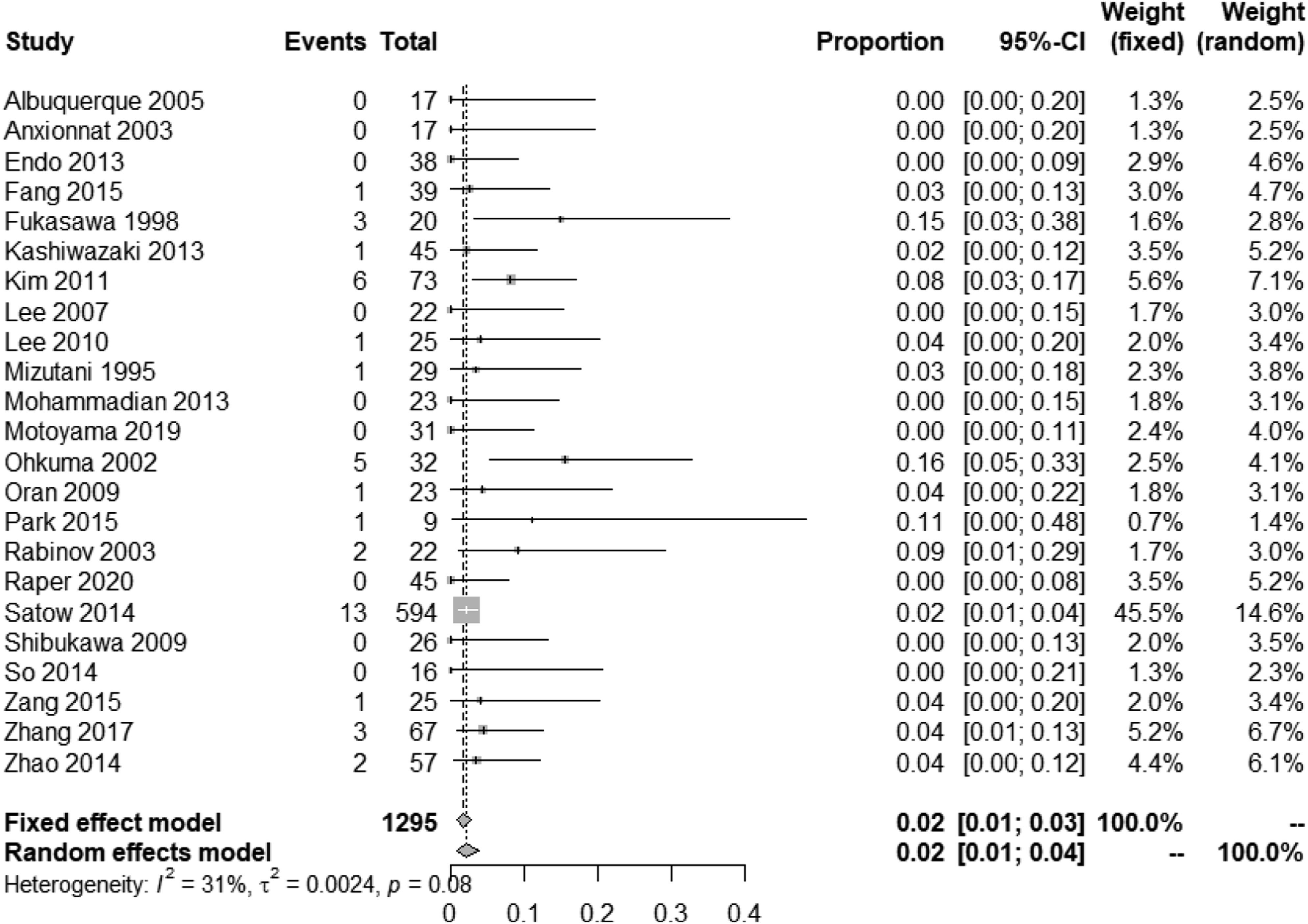
Twenty-six studies reported mortality rates in patients with SAH secondary to IAD.66-75,77-92 One study focused only on patients managed medically,
66
4 studies reported mortality for both patients managed medically or with interventions,67-70 while the remaining studies described survival rates only in patients undergoing intervention. The mortality of IAD with SAH, when treated by intervention, was 10% (95% CI, 7%–12%) (Figure 19) as compared to 55% (95% CI, 34%–76%) in absence of intervention (Figure 14). Mortality rate in IAD patients with SAH undergoing endovascular or surgical treatment.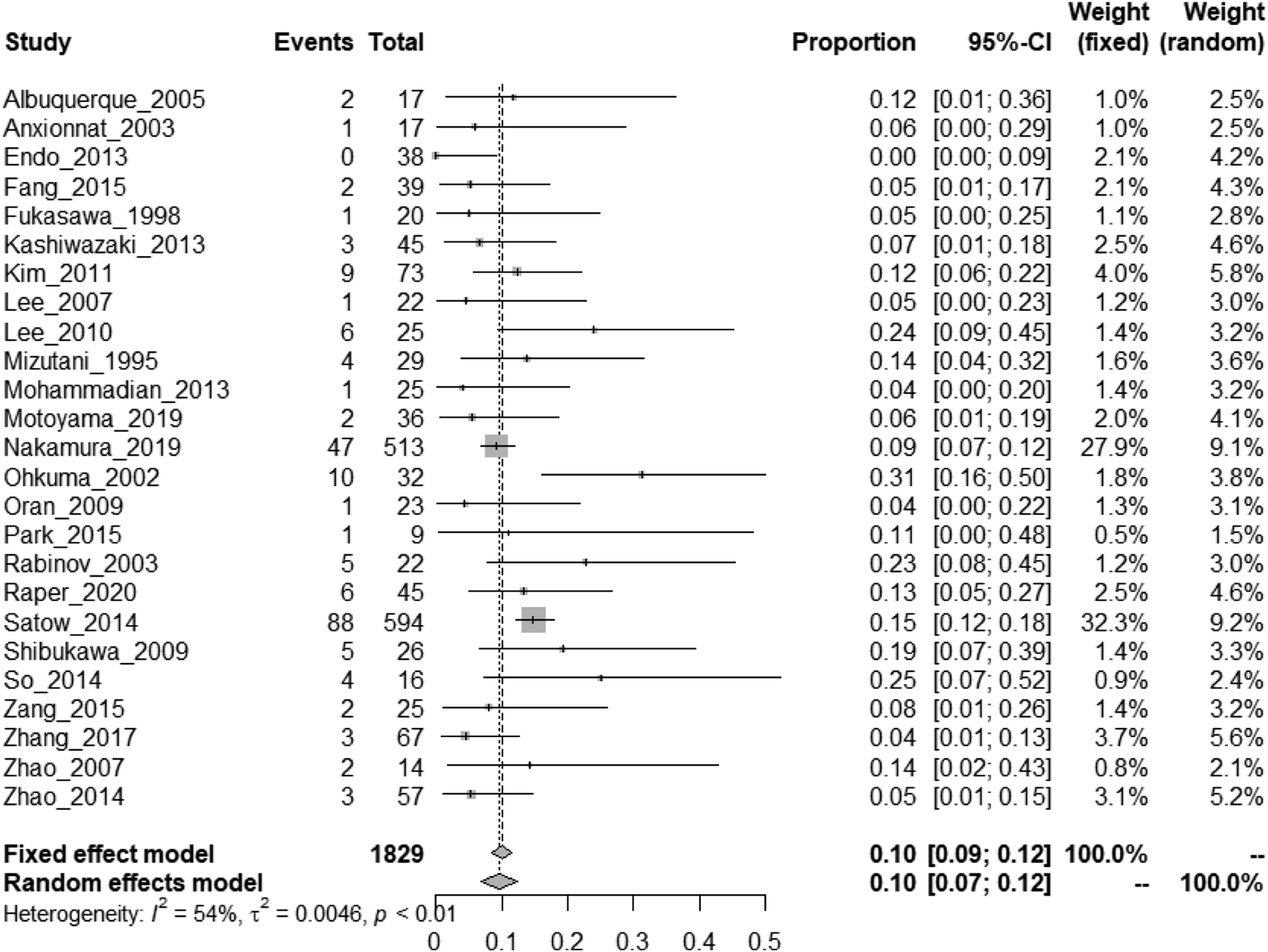
Twenty-five studies reported functional outcome associated with intervention,67-88,90-92 one study focusing only on cases managed medically
66
and 4 studies reporting outcomes for both cases managed medically and with intervention.67-70 The rate of good functional outcomes defined as mRS 0–2 was observed in 70% (95% CI, 64%–76%) of patients managed with an intervention (Figure 20) and 35% (95% CI, 21–51%) of patients managed medically (Figure 21). Rate of good functional outcome in IAD patients with SAH undergoing endovascular or surgical treatment. Rate of good functional outcome in IAD patients with SAH under medical treatment only.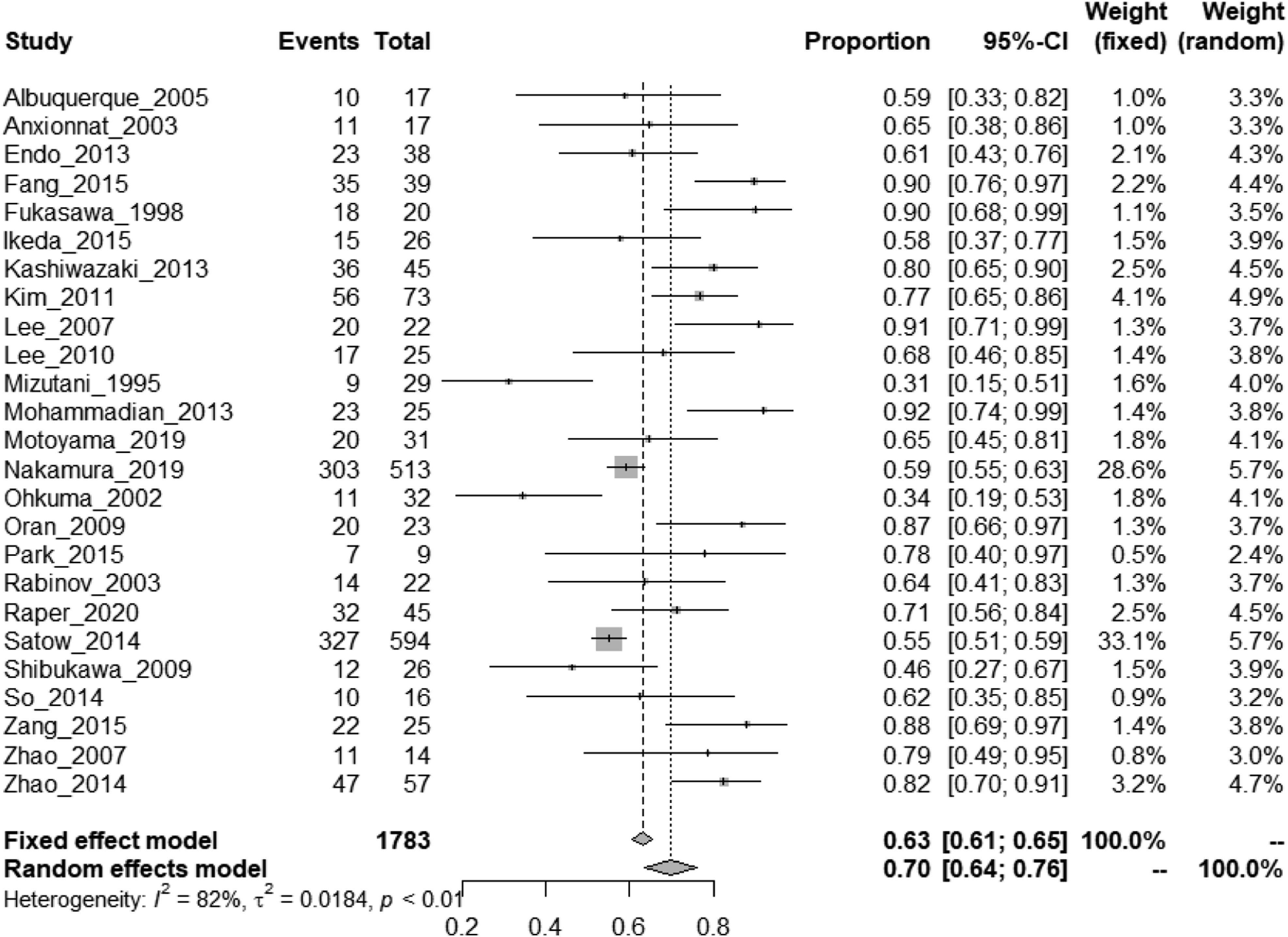
Overall, the very high rate of early rebleeding and subsequent fatality in the absence of intervention and the reduction of rebleeding and lower mortality associated with intervention (although based on limited small studies) are strong reasons for recommending early surgical or endovascular treatment in patients suffering IAD with SAH.
There are no RCTs and no observational studies systematically comparing different types of endovascular or surgical interventions. Those aiming at mechanically securing IAD consist most often in the trapping of the diseased vessel segment,67,84,96 with or without downstream revascularisation (e.g., selective aneurysmal sac occlusion through surgical clipping, surgical bypass, endovascular [stent-assisted] coiling or stent placement, including flow-diverter stents).83,89,90 Another possible intervention is occlusion of the vessel proximally to the disease segment. Vessel wrapping or side wall clipping offer only a limited protection against rebleeding and should be avoided.69,92,97 Interdisciplinary collaboration is essential to offer the best possible treatment adapted to each situation. Evidence-based Recommendation In patients suffering IAD with SAH, we suggest early surgical or endovascular intervention. There is insufficient data to provide a recommendation on the type of intervention to prioritize and the precise time window. Quality of evidence: Very low ⊕ Strength of recommendation: Weak for an intervention ↑? Expert consensus statement Different types of surgical and endovascular treatment methods can be used for treating IAD with SAH. In the absence of RCTs and considering the limited data from observational studies with high risk of bias, all experts suggest that the choice of intervention type in acute IAD-related SAH should ideally be the result of a multidisciplinary assessment.
PICO 4: In patients with an intracranial dissecting aneurysm and isolated headache (no transient ischemic attack [TIA], acute ischemic stroke, or subarachnoid hemorrhage [SAH]), does endovascular or surgical treatment of the aneurysm versus optimal medical treatment alone reduce the risk of ischemic stroke, SAH, intracerebral hemorrhage (ICH), death, and increase the likelihood of favorable functional outcome (mRS 0–2 vs. 3–6, or 0–1 vs. 2–6, or equivalent)?
Analysis of current evidence
We found no study matching our inclusion criteria to answer this question (Figure 22). The literature search did not find any randomized controlled trial of endovascular or surgical treatment in symptomatic IAD patients with an unruptured intracranial dissecting aneurysm and isolated headache or any observational studies meeting our minimal sample size criteria. The main reason for literature exclusion was small sample size (Methods) and that most studies on IAD focused on either patients with ischemic stroke, SAH, or mixed group of patients. PRISMA flow chart of study selection for PICO4. “Wrong patient population” in COVIDENCE corresponds to studies that do not match criteria for this PICO.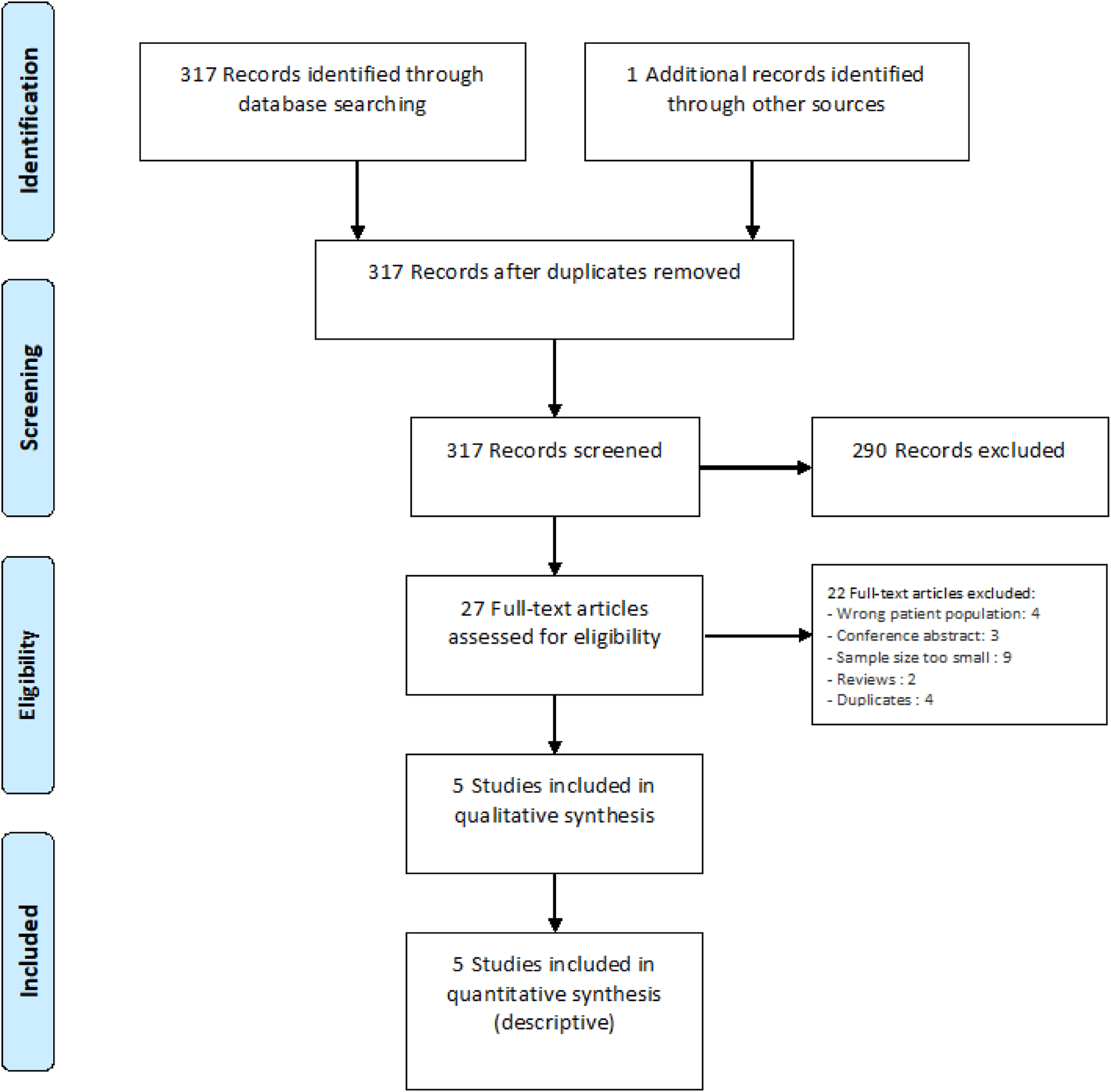
Additional information
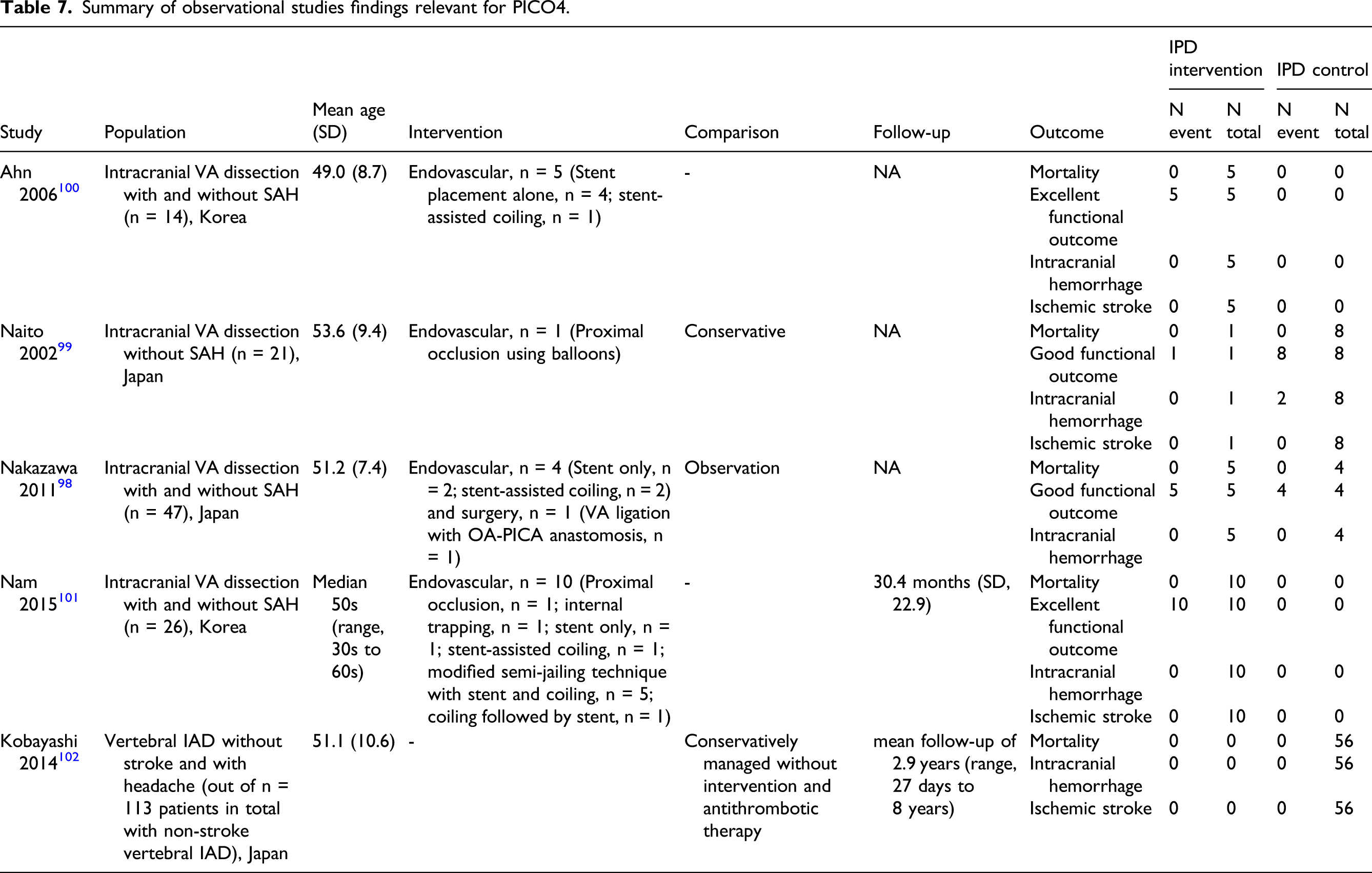
Summary of observational studies findings relevant for PICO4.
Supporting Information to the Expert consensus statement
Although data are scarce, in recent years most IAD patients with intracranial dissecting aneurysm and isolated headache are treated medically. Because the natural course of these patients is generally favorable, and because of the competing risks of both SAH and ischemic stroke, no antithrombotic treatment, but close monitoring has been proposed.13,102,103 Endovascular or surgical treatment might be considered if the dissecting aneurysm increases in size or signs of compression occur. Evidence-based Recommendation For symptomatic IAD patients with an intracranial dissecting aneurysm and isolated headache (no TIA, no acute ischemic stroke, no SAH), there is uncertainty over the benefits and risks of endovascular or surgical treatment and therefore it is not possible to make a recommendation. Quality of evidence: Very low ⊕ Strength of recommendation: - Expert consensus statement For symptomatic IAD patients with an intracranial aneurysm and isolated headache, all but one expert suggest against endovascular or surgical treatment unless the aneurysmal size increases significantly on follow-up imaging, or signs of compression occur.
PICO 5: In symptomatic extracranial artery dissection (EAD) and intracranial artery dissection (IAD) patients with ischemic stroke, transient ischemic attack (TIA), retinal ischemia, or local symptoms only, and without subarachnoid hemorrhage (SAH), is anticoagulant versus antiplatelet therapy in the acute phase associated with a reduced risk of ischemic stroke, death, higher likelihood of favorable functional outcome (mRS 0–2 vs. 3–6, or 0–1 vs. 2–6, or equivalent), and no increased risk of intracerebral hemorrhage (ICH), SAH, or other major bleeding?
Analysis of current evidence
We identified 2 completed RCTs addressing PICO5 (Figure 23, Table 8),32-34 both of which compared antiplatelets to vitamin K antagonists [VKA] in EAD, and of which one has two publications (with 3 months and 1 year follow-up),32,33 and no ongoing RCT. We found no RCT data on the use of direct acting oral anticoagulants (DOACs) in EAD nor any RCTs on the IAD population. PRISMA flow chart of study selection for PICO5. *these included 2 consecutive publications on the same trial (3 months and 1 year follow-up)32,33 and 4 observational studies on partly overlapping samples.16,17,108,113; “wrong population” in COVIDENCE corresponds to studies that do not match criteria for this PICO. Summary of RCT (per-protocol) findings relevant for PICO5. *presenting signs and symptoms. aPhenoprocoumon, acenocoumarol, or warfarin; target international normalized ratio [INR] 2·0–3·0 (heparin or LMWH recommended until target INR is reached); AC: anticoagulants; AP: antiplatelet; ASP: aspirin; ICH: intracerebral hemorrhage; IS: ischemic stroke; VKA: vitamin K antagonists.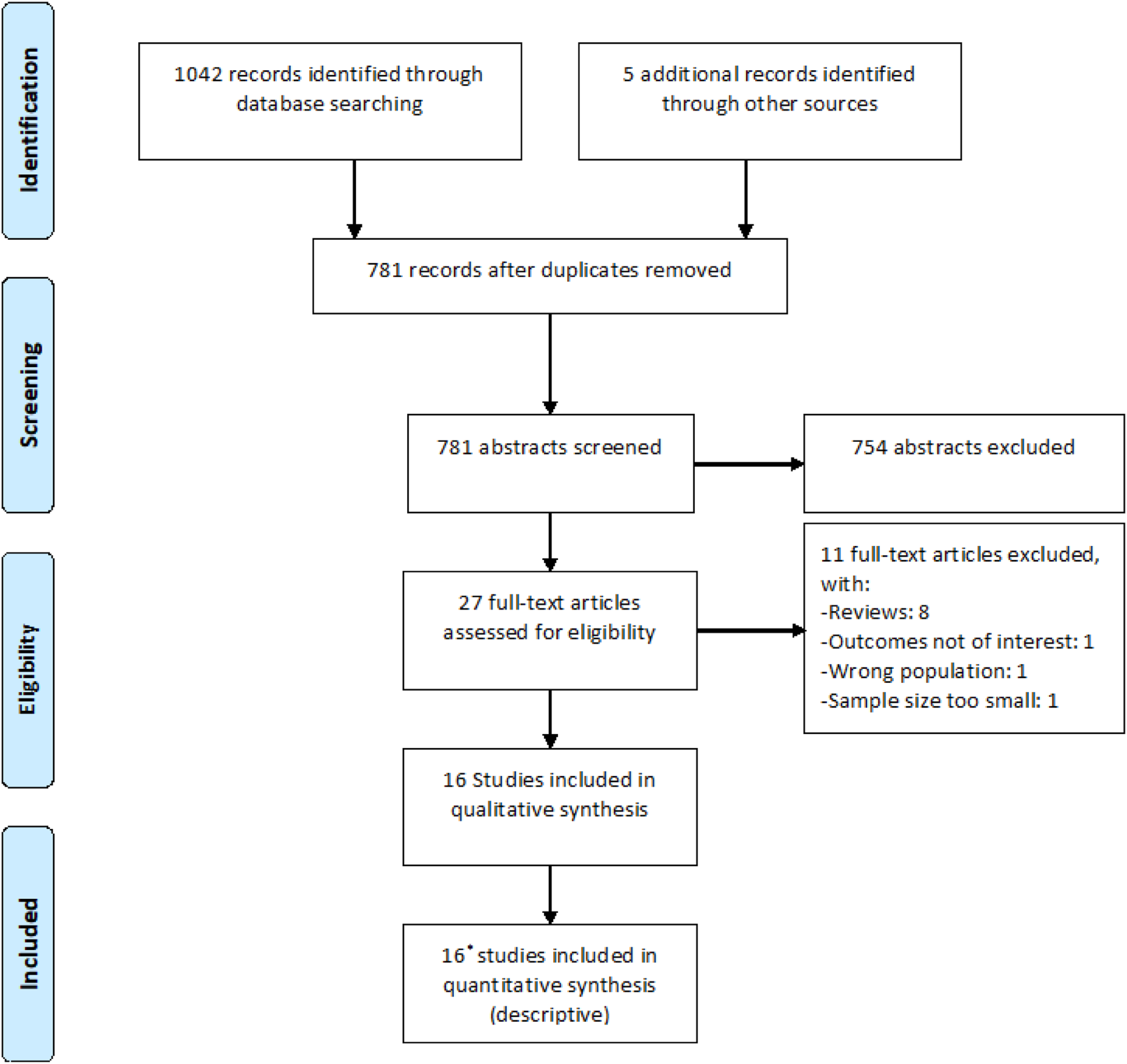
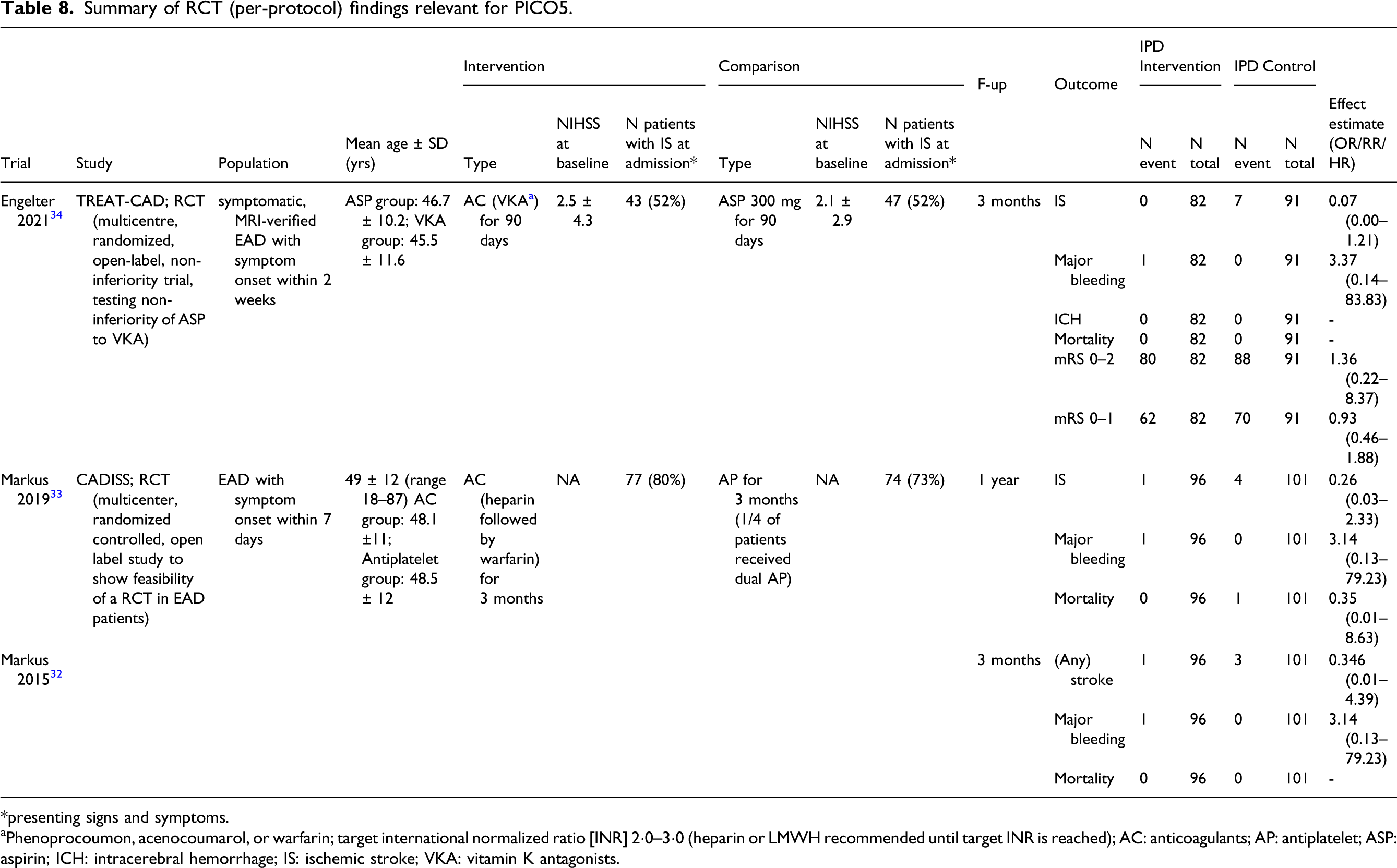
The CADISS study (Cervical Artery Dissection in Stroke Study) was a multicenter, randomized controlled, open label study designed to show feasibility of a RCT in EAD patients. CADISS included 250 EAD patients and randomly allocated participants to either antiplatelets or anticoagulant (VKA with or without bridging with unfractionated heparin [UFH] or low molecular weight heparin [LMWH]). 32 The specific choice of drug within either treatment arm was left to the discretion of the treating physicians. The intention-to-treat population comprised 126 patients in the antiplatelet group and 124 patients in the anticoagulation group. Antiplatelet treatment was heterogeneous with 22% of patients receiving aspirin alone, 33% receiving clopidogrel alone, 28% receiving both aspirin and clopidogrel, 16% receiving aspirin and dipyridamole, and one patient receiving dipyridamole only. In the anticoagulation group, 90% of patients received heparin and warfarin, whereas 10% received warfarin alone. Regarding the primary study endpoint (ipsilateral stroke or death), there was no statistically significant group difference. 32 Within the 3-month study period, ischemic stroke occurred in three (of 126) patients in the antiplatelet group and in one (of 124) patient in the anticoagulation group (OR, 0.335 [95% CI, 0.006–4.233], p = 0.63). There was one major hemorrhage (SAH) in the anticoagulation group. No major hemorrhage was observed in the antiplatelet group. 32 In the subsequent 12-month follow-up analysis, there were two additional ischemic strokes (one in each treatment arm) yielding again no statistically significant difference in the primary endpoint between groups. 33
In about 20% of the participants, the diagnosis of EAD was not confirmed by central adjudication either due to an alternative cause being identified or because imaging was not of sufficient quality to be confident of the diagnosis. However, per-protocol analysis excluding these subjects showed similar results.32,33 Although this is beyond the scope of PICO5, it can be noted that secondary analyses showed no association between treatment allocation (antiplatelets vs. anticoagulants) and whether dissecting aneurysms at baseline persisted at follow-up or whether new dissecting aneurysms developed, 28 or whether stenosis present at baseline showed recanalization. 33
Power calculations based on the per-protocol results from CADISS and the composite endpoint of stroke, death and major bleeding suggested a sample size of about 10000 (4876 per arm) would be required for a definitive phase 3 RCT. 32
TREAT-CAD was a multicenter randomized controlled therapy trial comparing aspirin to VKA in the treatment of EAD. Participants were randomly assigned to receive either aspirin (300mg/d) or VKA (with or without bridging with UFH or LMWH) for 3 months. To increase the number of endpoints and therefore power it included imaging marker events (new diffusion weighted imaging [DWI] or susceptibility weighted imaging [SWI]/T2*-lesions during follow-up as compared to baseline imaging), 104 as well as clinical endpoints (acute ischemic stroke, major intra- or extracranial hemorrhage, and death) in a composite study endpoint. The main results of TREAT-CAD were published in March 2021. 34 The primary analyses in TREAT-CAD were performed in the per-protocol population which comprised 173 patients (of 194 in the intention-to-treat population) of which 91 were allocated to aspirin and 82 were allocated to VKA. The primary composite endpoint occurred in 21 (23%) patients in the aspirin group and in 12 (15%) in the VKA group (absolute difference 8% [95% CI, –4 to 21], non-inferiority p = 0.55). 34 Accordingly, non-inferiority of aspirin was not shown. All ischemic strokes (n = 7) occurred in the ASA group, whereas the only major—though extracranial (gastrointestinal bleeding)—hemorrhage occurred in the VKA group. There were no deaths in either group. Five of the 7 ischemic strokes in the aspirin group occurred (or recurred) on day 1 after treatment onset, suggesting the importance of early initiation of antithrombotic treatment—whichever the clinician might choose.
As active treatment was stopped at 3 months in both trials, our meta-analyses combined the per-protocol results from CADISS and TREAT-CAD at 3 months follow-up32,34 for ischemic stroke (Figure 24), major bleeding (Figure 25), and the composite outcome of ischemic stroke, major bleeding, or death (Figure 26). There was no significant difference between the two treatment groups for the composite endpoint, ischemic stroke or major bleeding. In the anticoagulation group, the odds of developing the composite endpoint was OR, 0.35 (95% CI, 0.08–1.63), while that of developing ischemic stroke was OR, 0.18 (95% CI, 0.03–1.10), and that of major bleeding OR, 3.28 (95% CI, 0.34–31.80). There were no deaths at 3 months in either study. Information on functional outcome was available in TREAT-CAD only, where no difference was observed between both arms for excellent or good functional outcome.
34
It should be noted that both were phase 2 RCTs and underpowered to show small, but still important, differences between the two treatment regimens. Meta-analysis of effects on risk of ischemic stroke of anticoagulant versus antiplatelet treatment at the acute phase of EAD in RCTs (at 3 months). Meta-analysis of effects on risk of major bleeding of anticoagulant versus antiplatelet treatment at the acute phase of EAD in RCTs (at 3 months). Meta-analysis of effects on risk of ischemic stroke, major bleeding or death of anticoagulant versus antiplatelet treatment at the acute phase of EAD in RCTs (at 3 months).


We have based our grading recommendation on data from RCTs alone. The risk of bias is described in Figure 27, Table 9). The overall risk of bias was rated as not serious, inconsistency not serious, indirectness non-serious, imprecision mostly as serious to very serious due to small sample sizes in these phase 2 trials; the observation certainty was rated as moderate and the importance as critical. Risk of bias of RCTs for PICO5. Quality of results in RCTs relevant for PICO5. CI: Confidence interval; OR: Odds ratio. aWide confidence intervals. bOdds ratio not calculated because of zero events in the intervention and control arms. cVery wide confidence intervals.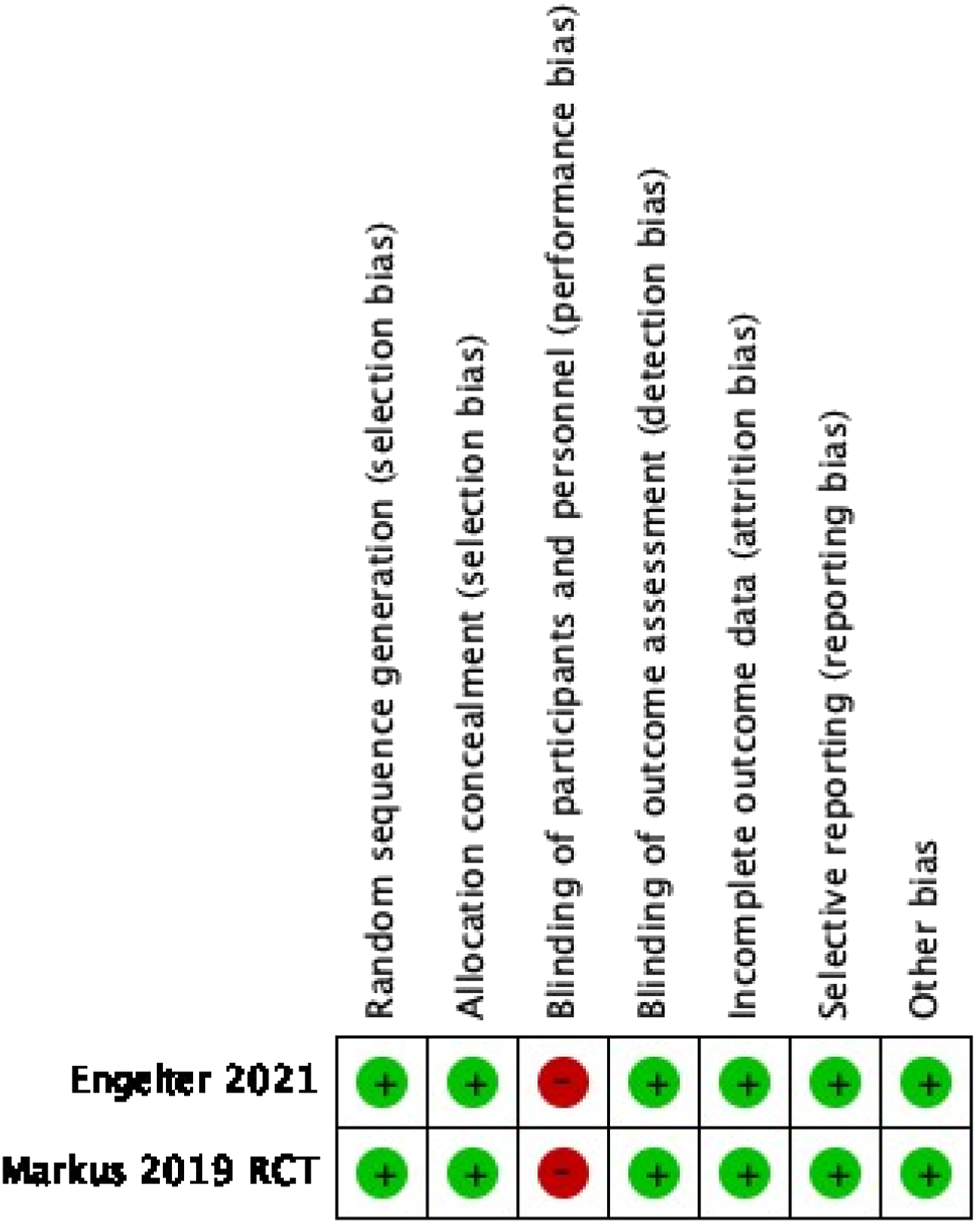
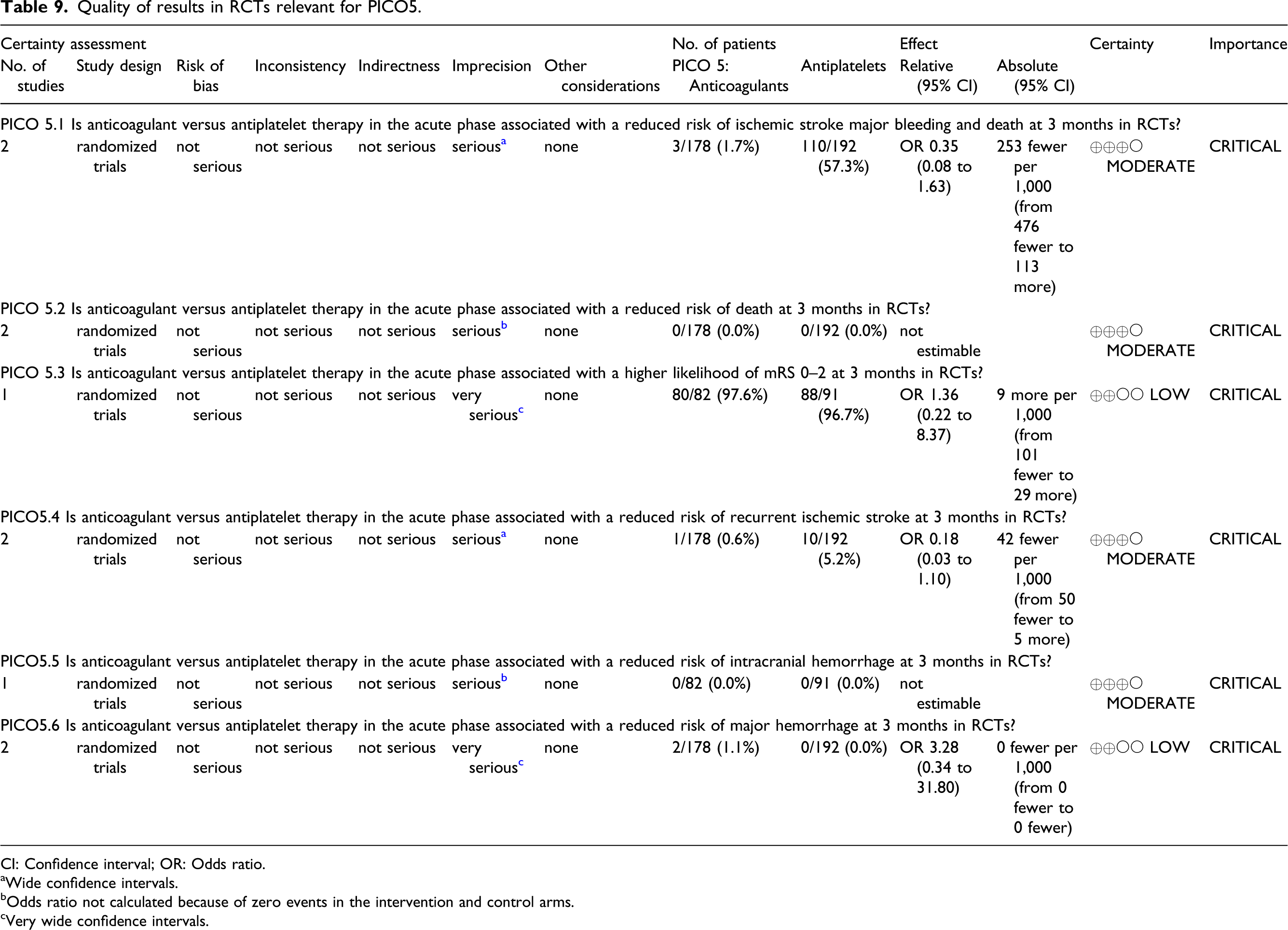
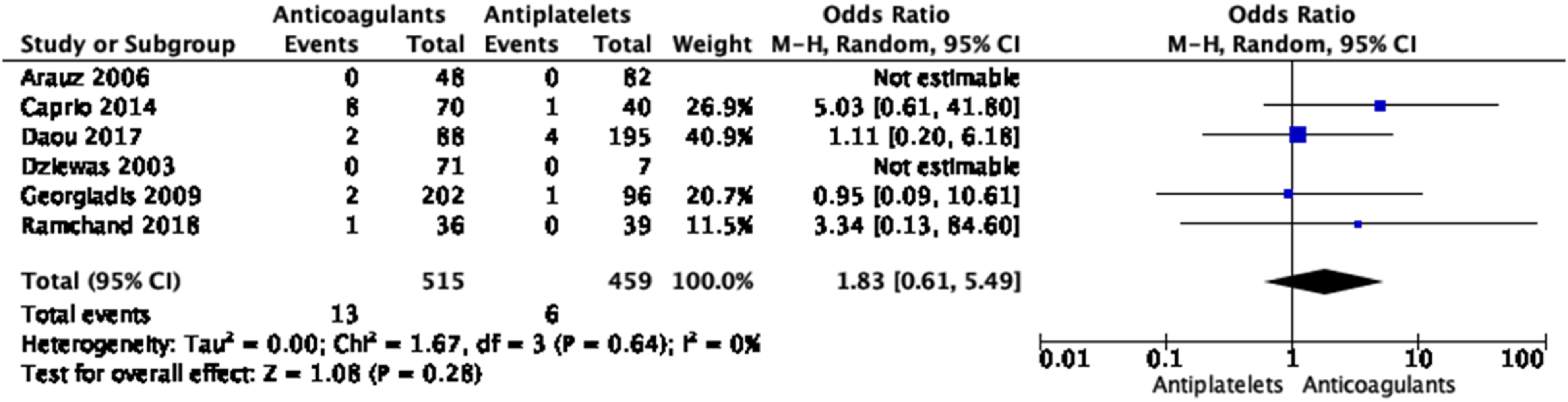
Overall, the two phase 2 RCTs have shown no difference between the benefits and risks of anticoagulants versus antiplatelets in the acute phase of symptomatic EAD. Although these were underpowered to show smaller differences in risks and benefits between the two approaches, they indicate that, based on current evidence, clinicians can prescribe either option.
It should be noted that, while there is no data demonstrating that antithrombotic treatment is better than no treatment in preventing stroke in EAD patients, as antiplatelets have been shown to be superior to placebo in preventing stroke after TIA or ischemic stroke in general,105,106 it wouldn’t be possible to carry out a trial on this in EAD patients with ischemic stroke or TIA. Prior to the CADISS trial, a survey of physicians was conducted on what they would use to treat EAD (with and without cerebral ischemia). 107 It shows that almost all would give either anticoagulants or antiplatelets emphasizing the fact that a trial would not be possible. Further adding to this evidence, a Cochrane review across observational case series of EAD showed that most patients with EAD of the internal carotid artery were treated with some type of antithrombotic treatment. 4 Although in an observational setting prone to bias, it is noteworthy that the small group of patients with no antithrombotic treatment had a much higher mortality rate (25%) than patients under antiplatelets or anticoagulants (each 1.8%).4
Additional information
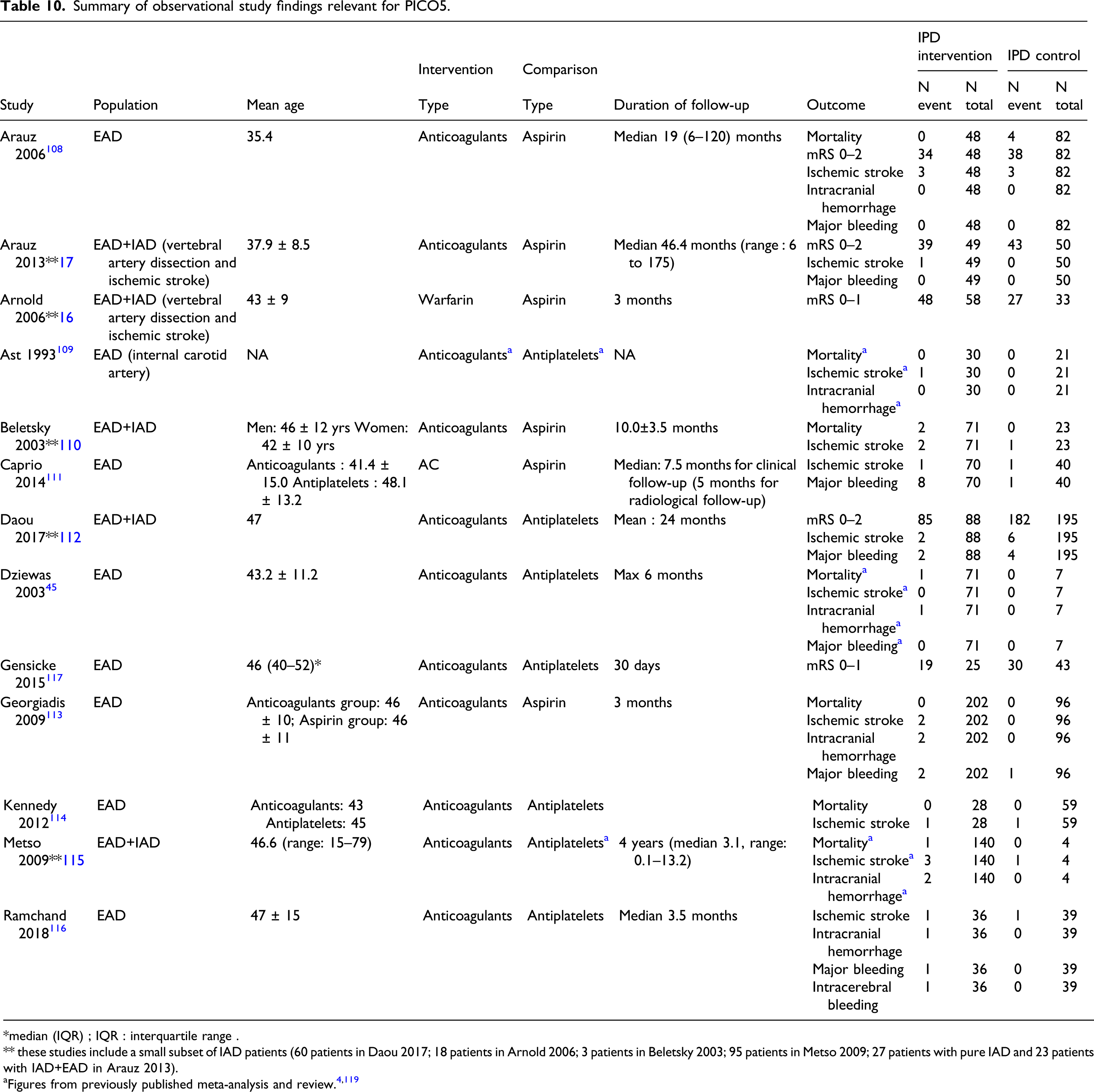
Summary of observational study findings relevant for PICO5.
*median (IQR) ; IQR : interquartile range .
** these studies include a small subset of IAD patients (60 patients in Daou 2017; 18 patients in Arnold 2006; 3 patients in Beletsky 2003; 95 patients in Metso 2009; 27 patients with pure IAD and 23 patients with IAD+EAD in Arauz 2013).
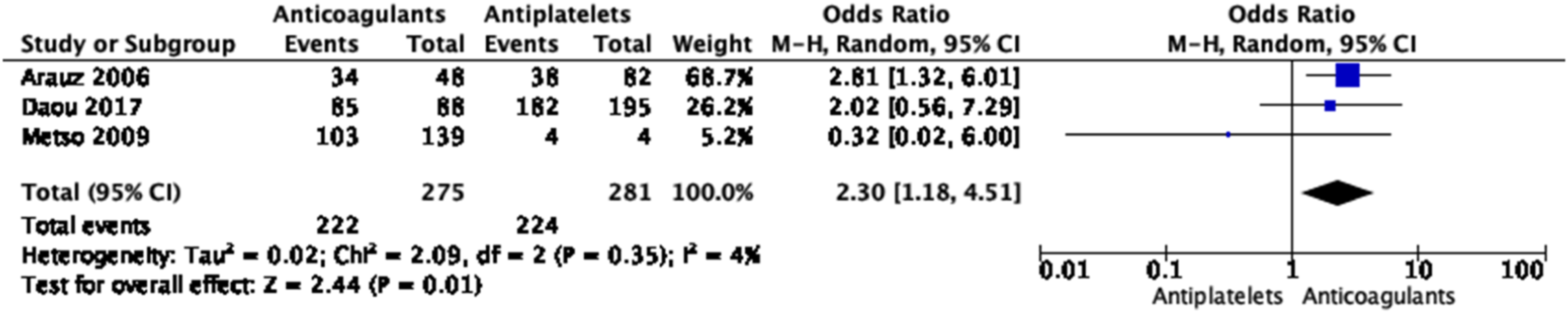
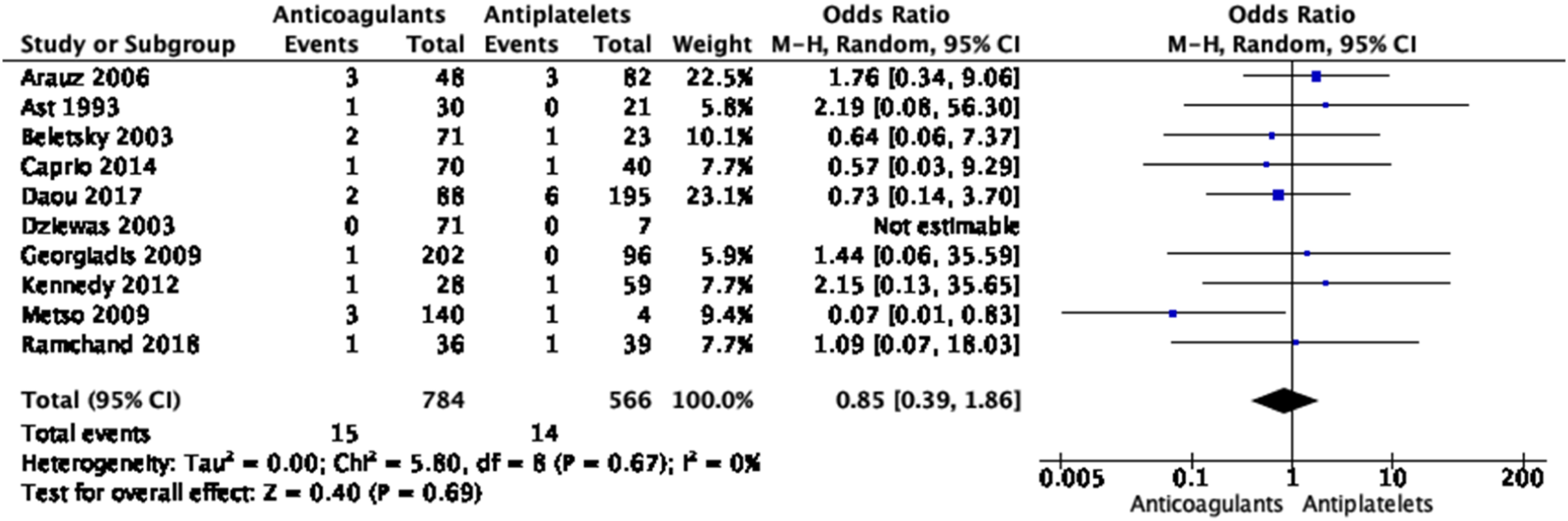
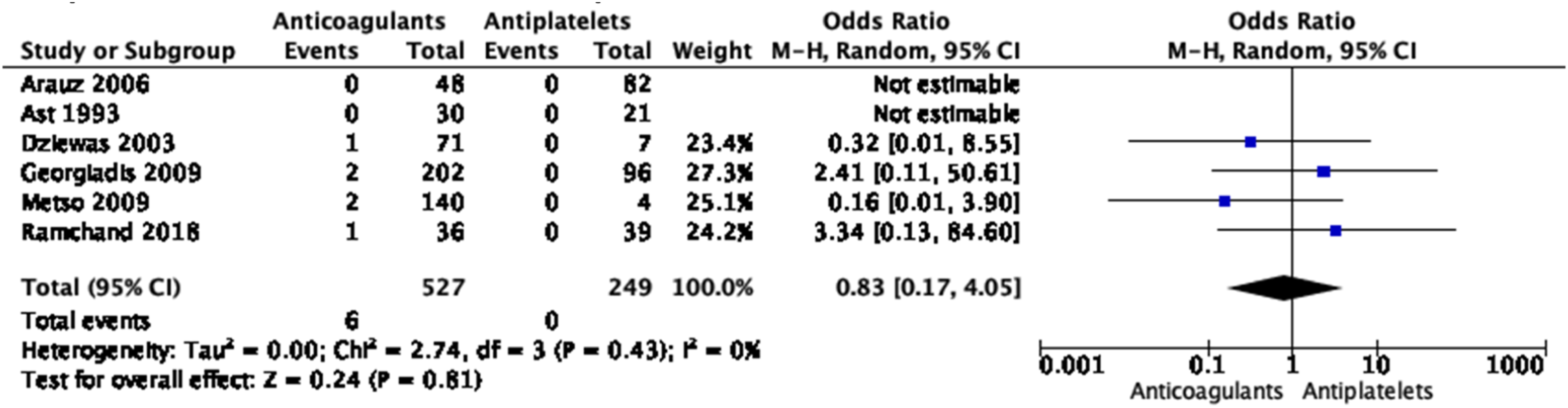
No significant differences in the treatment approaches were shown for any of the outcomes, except for a borderline significant higher rate of good functional outcome with anticoagulation based on three small studies (Figures 28–33 Meta-analysis of effects on mortality of anticoagulant versus antiplatelet treatment at the acute phase of EAD in observational studies. Meta-analysis of effects on good functional outcome (mRS 0–2) of anticoagulant versus antiplatelet treatment at the acute phase of EAD in observational studies. Meta-analysis of effects on excellent functional outcome (mRS 0–1) of anticoagulant versus antiplatelet treatment at the acute phase of EAD in observational studies. Meta-analysis of effects on ischemic stroke of anticoagulant versus antiplatelet treatment at the acute phase of EAD in observational studies. Meta-analysis of effects on intracranial hemorrhage of anticoagulant versus antiplatelet treatment at the acute phase of EAD in observational studies. Meta-analysis of effects on major bleedings of anticoagulant versus antiplatelet treatment at the acute phase of EAD in observational studies.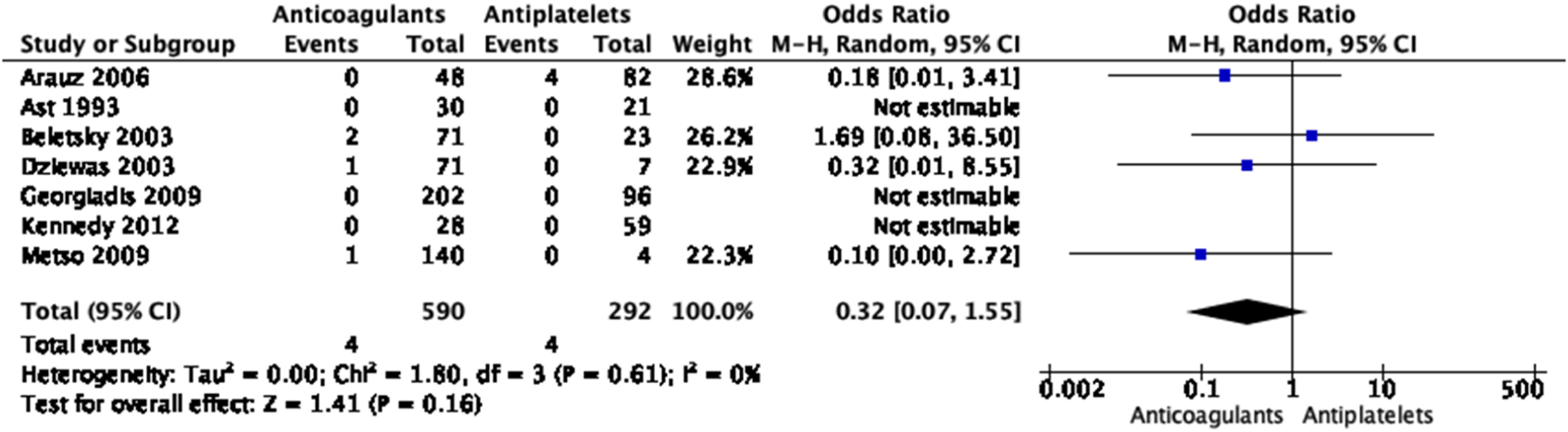

Only one retrospective observational study fulfilling our inclusion criteria compared use of DOACs to traditional anticoagulants (VKA or heparin) and antiplatelet agents in EAD patients. 111 Of the 149 included patients, 39, 70, and 40 were treated with a DOAC, traditional anticoagulant, and antiplatelet agent, respectively. There was no significant difference between the DOAC and other treatment groups for the risk of recurrent stroke (2 in the DOAC group vs. 1 in each of the other groups, p = 0.822). There were more major bleeding events in the traditional anticoagulant group (11.4%) compared to the DOAC (0.0%) and antiplatelet (2.5%) groups (p = 0.034). Three patients treated with DOAC and none in the other groups had a worsened degree of stenosis on follow-up imaging (8.6 vs. 0.0 vs. 0.0%, p = 0.019), but patients treated with DOAC more often had a severe stenosis or occlusion at baseline than patients in the other treatment groups. 111
Dual antiplatelet therapy with clopidogrel and aspirin has been shown to reduce the recurrent stroke rate in TIA and minor stroke in two large RCTs (CHANCE 121 and POINT 122 ) when given within 24 hours of symptom onset, compared to aspirin alone. These trials have shown a reduction the risk of stroke 121 or major ischemic events (ischemic stroke, myocardial infarction, or death from an ischemic vascular event) 122 at 3 months with a significant increase in the risk of major bleeding in the POINT trial. 122 Most stroke events, and the separation in stroke incidence curves between the aspirin plus clopidogrel arm and aspirin alone arm occurred within 10 days of randomization, while the separation in incidence of bleeding continued to increase throughout the treatment period and there was no net benefit from continuing treatment beyond 3 weeks.105,123 Similarly, the THALES trial showed that in patients with a mild to moderate acute non-cardioembolic ischemic stroke or TIA who were not undergoing thrombolysis, the risk of the composite outcome of stroke or death was lower with the combination of ticagrelor and aspirin than with aspirin alone within 30 days, although severe bleeding was more frequent with ticagrelor. 124 No subgroup information was available on patients with EAD/IAD in these trials. Recent ESO guidelines on TIA management recommend short term dual antiplatelet therapy with aspirin and clopidogrel over monotherapy, subsequently followed by monotherapy, in patients with acute non-cardioembolic high risk TIA. 105
There is no good information on the duration of antithrombotic treatment in EAD patients. The ESO-Karolinska guideline recommended (with a grade C) to pursue antithrombotic treatment for 6–12 months. 30 It was further suggested that in patients in whom full recanalization of the dissected artery has occurred and there have been no recurrent symptoms, stopping antithrombotic treatment may be considered. 30 In case of a residual dissecting aneurysm or stenosis, long-term antiplatelet treatment was recommended. 30 There is no new data justifying an update of this. Of note, in the two RCTs on EAD the randomized intervention (anticoagulants or antiplatelets) had a duration of 3 months.
Regarding IAD, there is no RCT comparing antiplatelet agents to anticoagulants at the acute phase. As proposed previously,
13
higher theoretical risk of SAH than EAD and the superiority of aspirin over anticoagulants in the acute phase of ischemic stroke in general are empirical arguments in favor of prescribing aspirin rather than anticoagulants in patients with IAD and cerebral ischemia. In case of recurrent thromboembolic events despite aspirin, dual antiplatelet treatment or anticoagulants could be considered. Before initiation of antithrombotic treatment in patients with IAD and cerebral ischemia, a lumbar puncture can be performed if neuroimaging cannot formally rule out minor SAH.
13
In IAD patients without SAH and cerebral ischemia, or in rare cases when both SAH and cerebral ischemia are present, close monitoring without antithrombotic treatment has been suggested.
103
Evidence-based Recommendation In the acute phase of symptomatic EAD, we recommend that clinicians can prescribe either anticoagulants or antiplatelet therapy. Quality of evidence: Moderate ⊕⊕⊕ Strength of recommendation: Strong for an intervention ↑↑ Expert consensus statement For symptomatic EAD patients treated with anticoagulants in the acute phase, all but three experts felt that DOACs could be used in place of vitamin K antagonists. For symptomatic EAD patients, all but one expert felt it was reasonable to use dual antiplatelet therapy with aspirin and clopidogrel in the acute phase in patients with TIA or minor stroke and restricted to a few weeks. For acute symptomatic IAD patients with ischemic stroke or TIA and no SAH, all but one expert felt antiplatelet agents had a better risk/benefit ratio than anticoagulants.
PICO 6: In extracranial artery dissection (EAD) patients and in intracranial artery dissection (IAD) patients without subarachnoid hemorrhage (SAH) does endovascular or surgical treatment of a stenosis or a dissecting aneurysm outside the acute phase versus optimal medical treatment alone reduce the risk of death, ischemic stroke, intracerebral hemorrhage (ICH), and SAH?
Analysis of current evidence
The literature search identified no RCT and no comparative observational studies meeting our sample size criteria (Figure 34). PRISMA flow chart of study selection for PICO6 “Wrong study design, language, setting, intervention, outcomes, and (patient) population” in COVIDENCE corresponds to studies that do not match criteria for this PICO.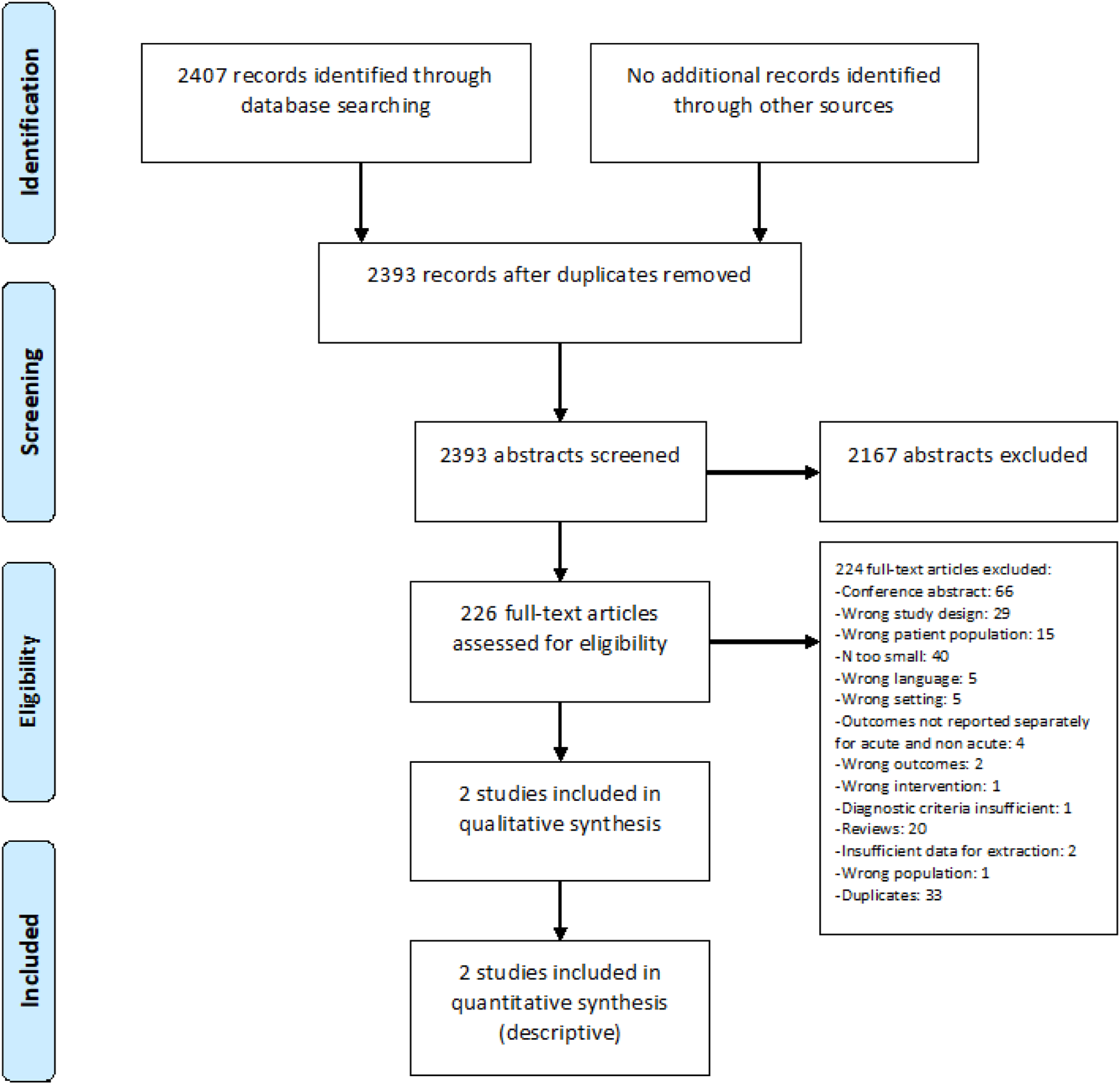
Importantly, there is overwhelming data on the very low rate of recurrent ischemic events in EAD patients.23,125 In the combined CADISP and French-Swiss EAD cohorts, out of 1,931 EAD patients, overall sixty patients (3.1%) had new-onset cerebral ischemia during follow-up at 3 to 6 months, of whom 33 patients (1.7%) an ischemic stroke, and 32 patients (1.7%) a TIA. 23 In the CADISS trial, comparing anticoagulation to antiplatelet therapy in 250 EAD patients, the rate of ischemic events during follow-up was 2% at 3 months and 2.4% at 1 year.28,33 The presence of dissecting aneurysms was not associated with a higher risk of stroke during follow-up: at 12 months, stroke occurred in 2.1% of patients with and 3.2% of patients without dissecting aneurysm (OR, 0.84 [95% CI, 0.10–7.31], p = 0.88). 28
Additional information
Summary of observational single-arm study findings relevant for PICO6.
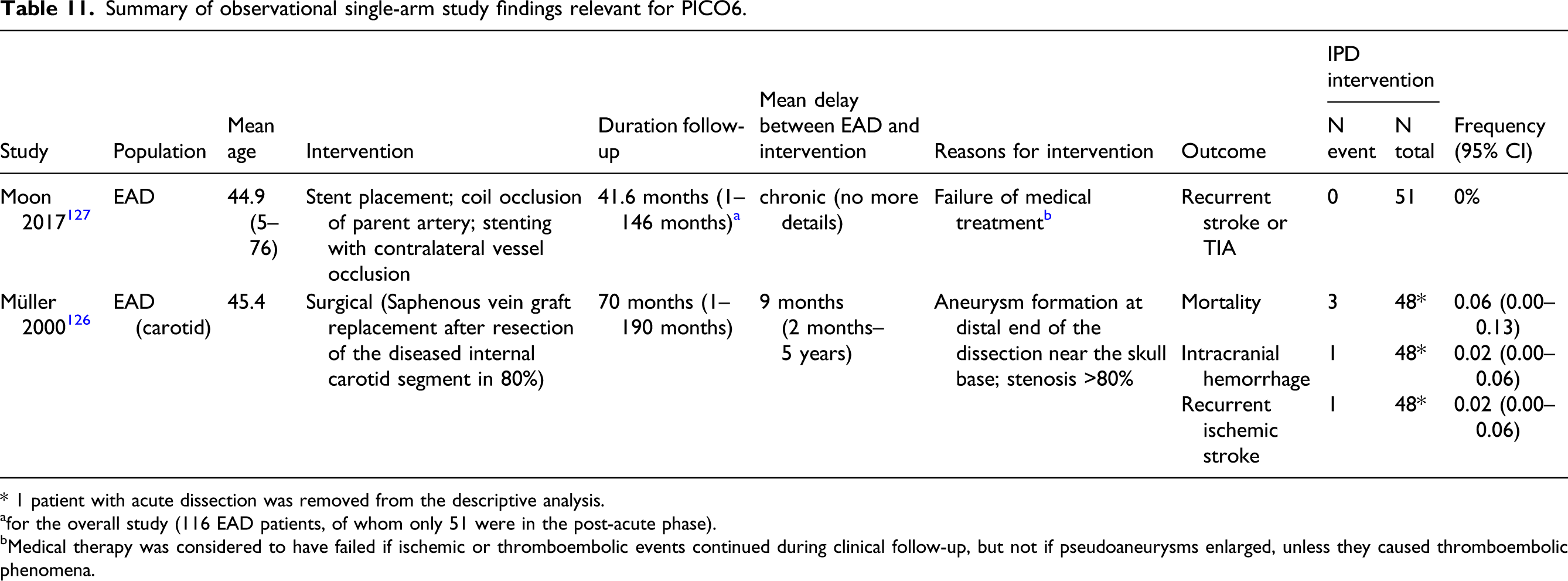
* 1 patient with acute dissection was removed from the descriptive analysis.
afor the overall study (116 EAD patients, of whom only 51 were in the post-acute phase).
bMedical therapy was considered to have failed if ischemic or thromboembolic events continued during clinical follow-up, but not if pseudoaneurysms enlarged, unless they caused thromboembolic phenomena.
In addition to the CADISS trial mentioned above, several observational studies add to the evidence that residual stenosis and dissecting aneurysms have a benign prognosis in EAD patients. In a long-term follow-up study of patients with carotid EAD and persistent (46 patients, 6.2 years) or transient (46 patients, 7.2 years) severe stenosis or occlusion, there was no relation between residual arterial pathology and stroke rate. 128 A systematic review gathering 166 EAD patients with internal carotid artery dissection (from 9 studies on <50 patients each) followed the evolution of dissecting aneurysms and reported that they rarely become symptomatic and rarely increase in size: 27 3% increased in size, 52% remained unchanged in diameter, 21% diminished in size, 19% completely resolved, 2% thrombosed, and 3% were repaired surgically; 2% underwent surgery 0.5–5.0 years later.
Much less data is available on IAD. In 52 IAD patients with asymptomatic vertebrobasilar dissecting aneurysms discovered incidentally (thus considered here as chronic, out of a total of 113 IAD patients followed up for 2.9 years [range, 27 days to 8 years]), Kobayashi et al. observed no stroke during follow-up and only one case of clinical deterioration due to mass effect.
102
Aneurysm size remained unchanged in 96% of the 52 patients during follow-up.
102
Evidence-based Recommendation In post-acute EAD patients with residual stenosis or dissecting aneurysm, there is uncertainty over the benefits and risks of endovascular or surgical treatment and therefore it is not possible to make a recommendation. Quality of evidence: Very low ⊕ Strength of recommendation: - Expert consensus statement Given the overwhelming evidence of a very low rate of recurrent ischemic events in post-acute EAD patients under medical treatment and the lack of evidence for an impact of residual stenosis or dissecting aneurysms on the rate of these events, all but one expert suggest against routine use of endovascular/surgical treatment in these patients: based on current limited evidence, endovascular/surgical treatment of post-acute EAD patients with residual stenosis or dissecting aneurysms may be carefully considered in exceptional situations, such as recurrent ischemic events despite optimal antithrombotic therapy or expanding dissecting aneurysms causing compression, after assessment by a multidisciplinary team (neurologist, neuroradiologist, neurosurgeon, and neurointerventionalist).
Discussion
Summary table of all evidence-based recommendations.
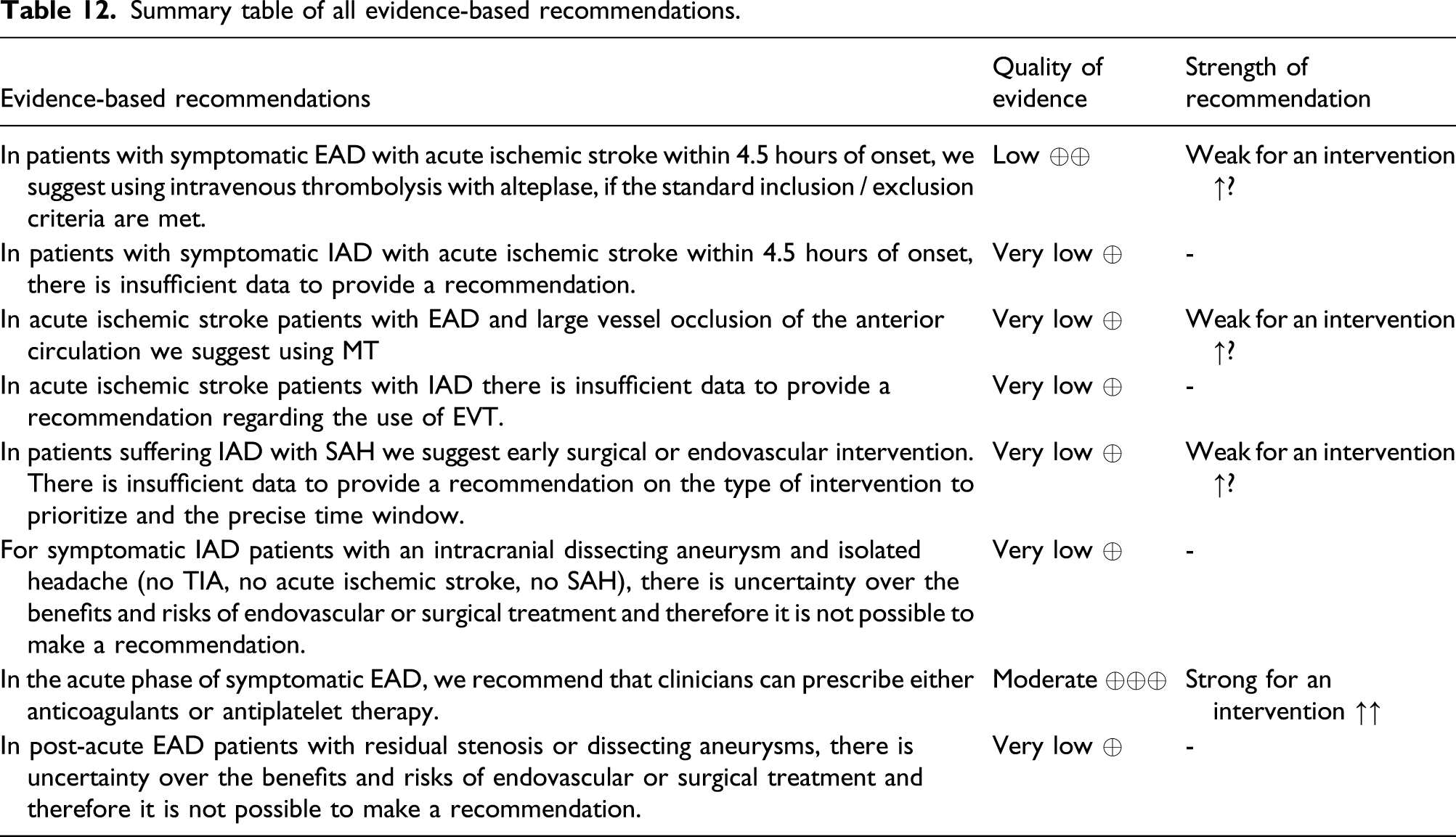
The three recommendations with low and very low quality of evidence were derived from observational studies: on IVT (PICO1) and EVT (PICO2) at the acute phase of EAD-related ischemic stroke, and on endovascular or surgical interventions in IAD with SAH (PICO3). Considering the nature of the evidence described in these observational studies, the very low incidence of EAD/IAD making it a major challenge to gather higher quality evidence, the strong benefit/risk ratio of some interventions in ischemic stroke overall, and information on the natural history of the disease, we nevertheless proposed recommendations for intervention (graded as weak because of the observational nature of the data), as we felt that running a clinical trial to more definitely answer these questions would be unethical. The recommendation with moderate quality of evidence was based on two phase 2 RCTs comparing anticoagulation and antiplatelet therapy in EAD (PICO5). While we acknowledge that additional trials may be warranted in the future to account for therapeutic innovations and novel antithrombotic regimens, we considered that it would be unrealistic to enroll the required number of patients to complete a phase 3 trial on an uncommon condition such as EAD. As results were consistent across the two published RCTs, we therefore also rated this recommendation as strong. For PICO4 and PICO6, addressing endovascular or surgical intervention in IAD with isolated headache, and in the post-acute phase of EAD, the quality of evidence was so low that no recommendation could be made.
Summary table of all expert consensus statements.
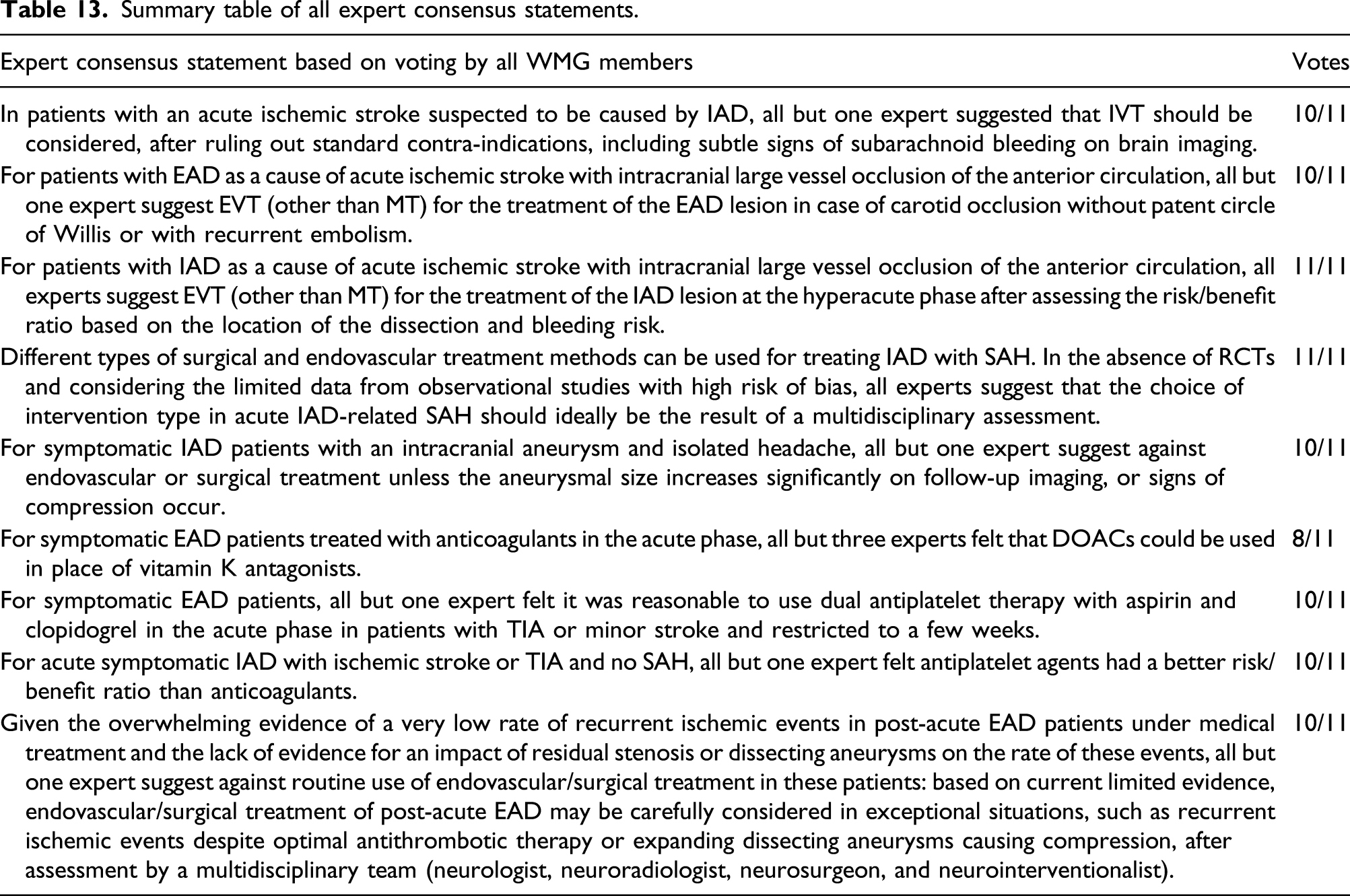
Many of these pertain to the management of IAD for which the quality of evidence was too low to provide recommendations, specifically for the use of IVT (PICO1) and EVT (PICO2) in the acute phase of IAD-related ischemic stroke, antiplatelet agents over anticoagulation in IAD with TIA or ischemic stroke (PICO5), and endovascular or surgical interventions when the IAD is associated with headache only (without SAH or cerebral ischemia, PICO4). Some expert consensus statements were aimed at sharing expert opinion on the implementation of certain recommendations, such as the use of direct anticoagulants in symptomatic EAD or of dual antiplatelet therapy in the first weeks after EAD-related TIA or minor stroke (PICO5), or the decision to conduct EVT for the treatment of the EAD/IAD lesion (PICO2). Finally, some expert consensus statements recommended in the absence of clear data to use complementary local expertise through multidisciplinary assessment on complex questions such as the choice of the type of intervention in IAD-related SAH (PICO3) or the decision to perform an intervention for post-acute EAD in the uncommon situation of recurrent ischemic events despite optimal antithrombotic therapy or expanding dissecting aneurysms causing compression (PICO6).
To our knowledge, this is the first comprehensive European guideline on the management of EAD and IAD, implementing GRADE methodology. 35 Recommendations and expert consensus statements are based on the work of a large group of experts with broad expertise relevant to the PICO questions, spanning across disciplines (neurology, neurointervention, neurosurgery, and neuroepidemiology), countries, and continents. The latter was specifically important for this guideline due to important differences in the epidemiology of EAD and IAD between European and East Asian ancestry populations and more extensive experience with IAD management in East Asia. While most of our PICOs relied on observational data only, we have applied very strict inclusion criteria, in contrast to previously published meta-analyses on this topic, most of which also included small case series. Importantly, this guideline also presents the first meta-analysis of the only two RCTs comparing anticoagulants and antiplatelets for the management of EAD.
We acknowledge limitations. The observational nature and small size of most of the studies described in this guideline is a major limitation. For some PICOs and outcomes, there was an important heterogeneity between included studies. Some studies combined EAD and IAD without providing the data that would enable a separate analysis of each. Not all studies used strict diagnostic criteria for dissection, especially older ones and for IAD. Important heterogeneity was noted in follow-up duration. For the two published RCTs, more elaborate individual level data meta-analysis could be warranted, but this was beyond the scope of the present study. Finally, the random effects meta-analyses included in this manuscript were based on raw data extracted from the publications. Secondary meta-analyses using adjusted ORs provided in the manuscripts or by contacting the authors could be of interest but are beyond the scope of the present work.
While conducting phase 3 RCTs on the management of EAD/IAD seems unrealistic based on power estimates from the CADISS trial, further prospective collection of data in the setting of international registries could provide important “real life” estimates of the impact of different therapeutic approaches on EAD/IAD-related outcomes. Some specific therapeutic questions, for which there is extremely limited data
Plain language summary
Extracranial artery dissection (EAD) and intracranial artery dissection (IAD) are characterized by bleeding in the wall of an artery in the neck or in the brain. They represent a leading cause of stroke in young and middle-aged adults, either due to clotting in the artery near the wall hematoma (for EAD and IAD) leading to vessel occlusion and causing an ischemic stroke, or due to rupture of the artery (for IAD) causing intracranial bleeding in the subarachnoid space surrounding the brain tissue (subarachnoid hemorrhage).
When patients with EAD present with an acute ischemic stroke, it is recommended that they receive the same acute phase treatments as other patients with ischemic stroke, which mainly aim at removing the blood clot from the vessel to restore normal blood flow. This can be done by using intravenous thrombolysis (i.e., injection of a product that dissolves the clot) and by retrieving the clot mechanically (mechanical thrombectomy). After these emergency treatments other medications are indicated for several months to avoid new clotting within the dissected artery. For this, it is recommended that physicians can choose between two types of blood thinning medications, antiplatelets (moderate blood thinning), or anticoagulants (intensive blood thinning). Indeed, two recent clinical trials where EAD patients were randomly assigned to receive either antiplatelets or anticoagulants found these two options to be equally efficient. For patients with IAD who suffer from a subarachnoid hemorrhage, an urgent intervention is recommended (either endovascular or surgical) as it is known to substantially reduce the risk of rebleeding and improve survival. Finally, for patients with IAD who present with headache only (without any ischemic stroke or subarachnoid hemorrhage) and in EAD patients with residual vessel narrowing or widening (so-called dissecting aneurysm) after the acute phase, there isn’t enough evidence to make recommendations on the use of endovascular treatment or surgery to improve the outcome of patients.
Supplemental Material
sj-pdf-1-eso-10.1177_23969873211046475 – Supplemental Material for ESO guideline for the management of extracranial and intracranial artery dissection
Supplemental Material, sj-pdf-1-eso-10.1177_23969873211046475 for ESO guideline for the management of extracranial and intracranial artery dissection by Stephanie Debette, Mikael Mazighi, Philippe Bijlenga, Alessandro Pezzini, Masatoshi Koga, Anna Bersano, Janika Kõrv, Julien Haemmerli, Isabella Canavero, Piotr Tekiela, Kaori Miwa, David J Seiffge, Sabrina Schilling, Avtar Lal, Marcel Arnold, Hugh S Markus, Stefan T Engelter and Jennifer J Majersik in European Stroke Journal