
Abstract
Abstract
The European Stroke Organisation (ESO) Simulation Committee was established in 2017 with the intent to promote simulation education and training in the stroke field. The application of simulation methodology in education and training improves healthcare professional performances in real clinical practice and patient outcomes. We evaluated the implementation of simulation training in stroke medicine, how it can significantly affect stroke pathways and quality of care. We herewith describe simulation techniques in the acute stroke setting. Simulation programs place the trainees in a safe environment, allowing both role-playings for decision making training and procedural simulation for technical skills improvement. This paper includes the position of the Committee on the key points, principles, and steps in order to set up and promote simulation programs in European stroke centers. Stroke is an emergency, and hyperacute phase management requires knowledge, expertise, optimal multidisciplinary team working, and timely actions in a very narrow time window. The ESO Simulation Committee promotes the implementation of simulation training in stroke care according to a specific and validated methodology.
Introduction
Despite acute therapies are constantly evolving, stroke remains a leading cause of death and disability worldwide. 1 Reperfusion therapies (i.e., intravenous thrombolysis and mechanical thrombectomy) largely proved effectiveness for the treatment of acute ischaemic stroke, and for intracerebral haemorrhages research indicates several potential options for the forthcoming future.2–4 Clinical outcomes, however, are highly time-dependent, with a reduction of treatment delays being one of the main targets for improvement of patient care.4,5
Moreover, stroke diagnosis and treatment are characterized by highly specific competencies that have to be applied in an emergency situation, and in a multidisciplinary setting. Stroke neurologists drive the diagnostic and therapeutic workup and have a substantial role in the coordination of the stroke team. However, time pressure plays a harmful role in team communication and on the decision-making process, with potential errors attributed to “human factor”.
Traditional methods of medical education for acute stroke settings are based on “knowledge”, often neglecting other non-technical skills. Simulation-based team training can improve team performance by improving communication, teamwork, and leadership.6,7 Moreover, simulation methodology in stroke care education, as in every other field, allows tailoring the educational goals to the trainees’ level and needs. The improvement in simulation performance is associated with significant changes in real-life patient management, as it has been demonstrated for several medical emergencies.8,9 Accordingly, in the ischaemic stroke setting, simulation training showed its efficacy in terms of improvement of knowledge, gain of time, teamwork, multidisciplinary exchange of competences, and confidence of health professionals in emergency situations.10–12 Notably, simulation training and the multidisciplinary approach to treatment can help deliver the highest quality of care, decrease in-hospital delays for treatment and improve patient’s outcome.6,13
The European Stroke Organisation Simulation Committee aims to promote and support the use of simulation in the stroke field across Europe for education, training, and research.
This opinion paper is the result of a consensus of experts. The aims are to facilitate the implementation of simulation techniques in the stroke field, providing insights to promote and support the systematic use of simulation training in stroke care medical education. We will focus on the goals, methods, and expected results of simulation training for acute stroke management.
Building simulation training in stroke medicine
First step: Analysis of the context
The healthcare systems show heterogeneity according to the political and regional healthcare administration. Differences in organizational aspects of education and training in Medical School, in post-graduate training and continuous medical education, would benefit including simulation methodology, complementary to the traditional ones, in order to target and tailor programs, according to local differences and specific needs. Each program should take into account the peculiarities and the Country and/or center-specific requirements. In order to efficiently address the local implementation of simulation training in stroke care, a preliminary analysis of the specific setting should be performed. It consists of identifying and describing the actual stroke care management and related issues focusing on areas of interest and critical local needs.
These elements include the following key points:
identification and description of the pre-hospital and in-hospital phase of the stroke pathway and its environment; Inventory equipment and tools relevant to stroke care available (for instance, type of available neuroimaging); identification and description of trainees, their professional profile and needs according to their allocated roles in the stroke team; review of local stroke care pathways and any potential pitfall; identification of institutional needs (if applicable); inventory of human resources and identification of tailored simulation programs (i.e., on-site or in situ simulation training).
In particular, in stroke care, the analysis should be focused on identifying the strengths and weaknesses of the local stroke pathway (pre- and intra-hospital, Figure 1). All members of the stroke team should be surveyed to before implementation in order to focus on what they would like to improve. This preliminary step is essential for designing the simulation program for local implementation.
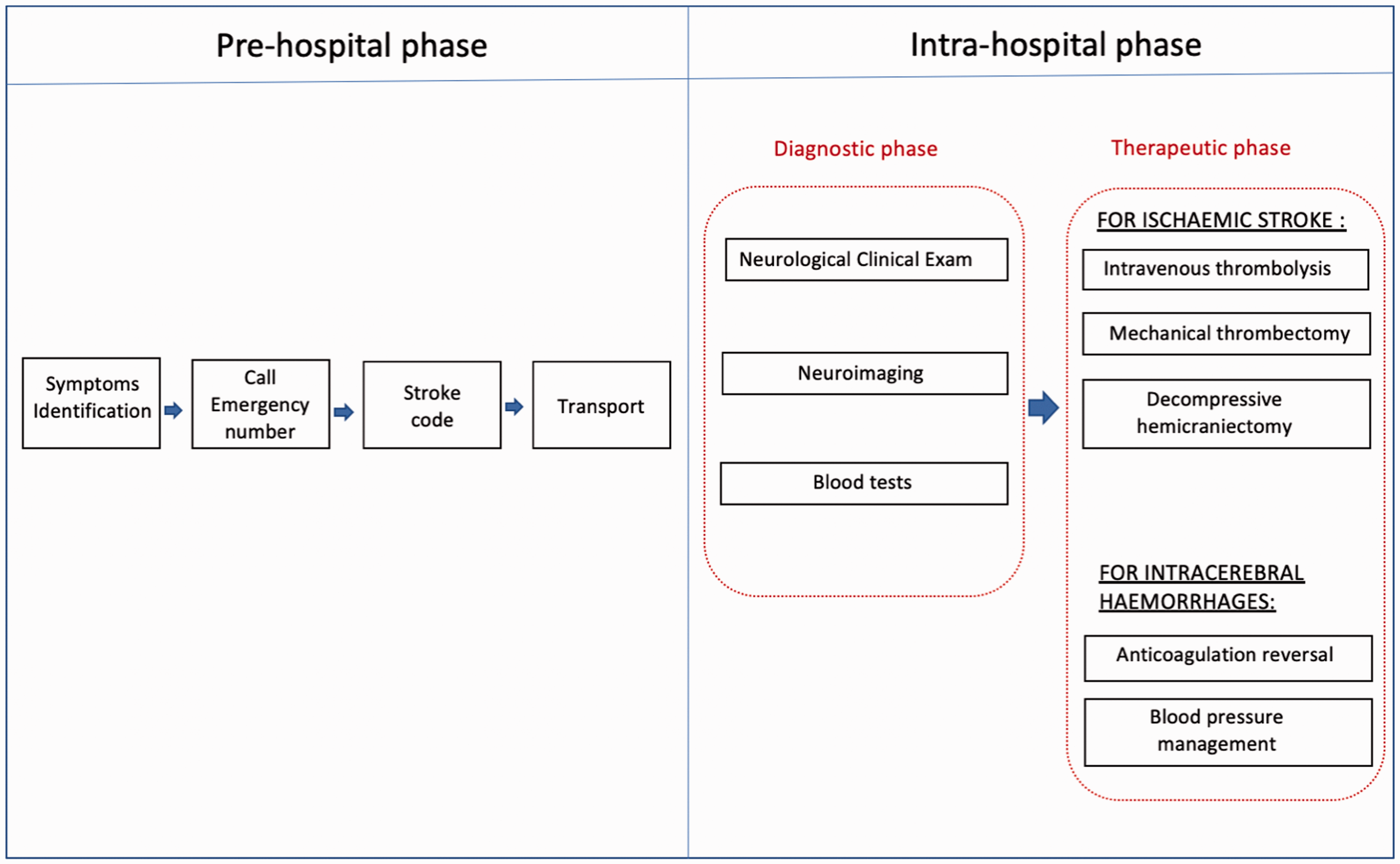
Stroke pathway.
Second step: Definition of the simulation training objectives
The second step for building a simulation training program is the definitions of the objectives, i.e., learning goals of the program.
General and educational objective(s) should be preliminary identified and clearly stated. A maximum of 2–3 goals for the program is highly recommended. For instance, improving technical skills, testing the communication attitudes, and the efficiency of the stroke pathway in a hospital setting are all worthy objectives. However, each of them requires a dedicated simulation pattern, with specific rules. Eventually, in an advanced simulation program, more than one aspect, behavioral, environmental, and technical, can be addressed in the simulation setting and reviewed in the debriefing sessions.
Some examples of objectives for simulation stroke programs are detailed in Box 1. These objectives can be applied in progressively more complex situations. Examples of objectives for stroke simulation programs.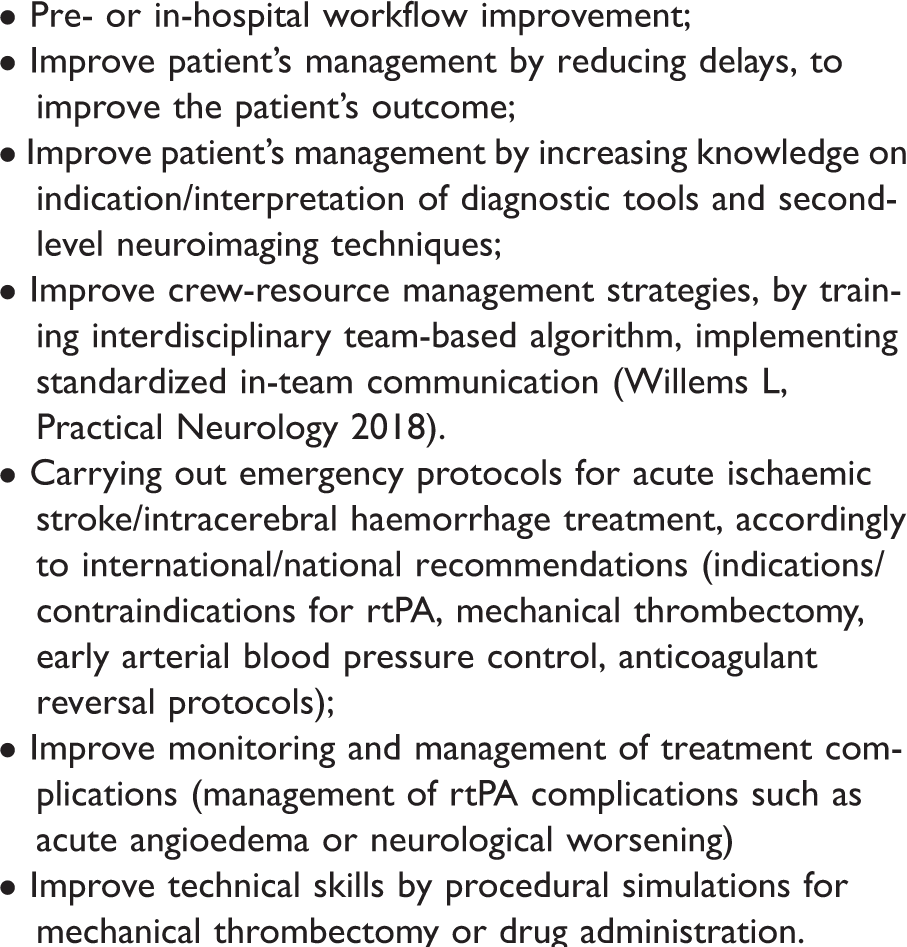
Third step: Definition of simulation training techniques and settings
Simulation stroke programs include different techniques of interventions, depending on the objectives of the training. All simulation techniques/settings have advantages and disadvantages, and they should be chosen accordingly to the objectives of the training.
Several approaches can be selected, either alone or combined, depending on the educational objectives and may be applied at different phases of the stroke pathway:
improving technical skills (i.e., mechanical thrombectomy, administration of rtPA); implementation of procedures (individual or collective, i.e., in-hospital stroke pathway, telemedicine expertise); clinical diagnostic and/or therapeutic reasoning (i.e., stroke diagnostic workflow); behavioral management (a professional situation, teamwork, communication, etc.);
The simulation techniques should be systematically adapted to the educational objectives and approaches. In particular, different simulation techniques can faithfully recreate both clinical scenarios for training purposes (i.e., role-playing simulation) and procedural “hands-on” training in performing time-critical procedures (i.e., procedural simulation), without exposing patients to harm during the learning process. 14
Descriptions of the simulation technique (or ‘dimensions’) can also be based on devices or places for simulation implementation. 15 For instance, high fidelity simulation refers to the simulation of case scenarios conducted on high fidelity mannequin, often in a simulation center. In stroke setting, this technique can be useful to train on the emergency situation, such as complications of intravenous thrombolysis (e.g., angioneurotic edema or neurological worsening), where the stroke team has to manage in frontline a specific, rare, medical emergency. In the simulation center, scenarios can also be played in high fidelity with environmental reality, such as the neuroimaging room for training on the diagnostic workflow of acute stroke diagnosis. Contrasting with simulation center simulation or on-site, the in-situ simulation technique is conducted in the real clinical context.
The benefits of performing simulation training in specialized simulation environments or centers are that trainers and equipment can be concentrated in one location, and the spaces allow the participants to focus on the learning tasks (for instance, dedicated debriefing rooms). However, simulation centers also have disadvantages. These protected spaces can represent a barrier for the transfer of skills and knowledge to every-day practice because trainees remain unfamiliar with the equipment, environments, procedures, and teams in the real-word. On the other hand, in-situ simulation training allows removal of these barriers and represents the “stress-test” for the real work context, thus showing any potential bias or system pitfall.16–21 In order to guide in the decision of what simulation technique is more suitable for a specific purpose, the specific objectives of the simulation training should be previously settled (Box 1).
Technique 1: Role-play simulation
Role-playing, both low- and high-fidelity simulation, provides the opportunity for training on case management and communication skills during a routine clinical scenario, based on direct observation and feedback. This technique can be applied to every health professional at all stages of training and practice. It has relevant interest across cognitive, communication, and teamwork domains. A role-play simulation scenario runs with a standard diagram composed of 3 phases: the briefing, the scenario, and the debriefing (Figure 2). The first is the briefing, which allows the instructor to specify the framework of the session and specific objectives. Therefore, the rules of the role-playing are clearly presented, such as the confidentiality of exchanges and the absence of judgment attitude. The duration of the scenario is established, with specific starting and ending points (e.g. “the scenario starts when the neurologist receives the call from the Emergency Department for a stroke code and it finishes when the neurologist takes its therapeutic decision”), in order to set the “fiction window”. Generally, the duration of the role-playing should be about 1/3 of the length of debriefing, leading to a reasonable duration for each scenario of about 20 minutes. During the simulation, the trainees are immersed in the situation in a totally safe environment. The instructor coordinates the scenario and observes the trainees focusing on the specific objectives of the simulation program. Using records and forms for the continuous evaluation of trainees helps to address the debriefing phase. Post simulation debriefing is one of the most effective components of simulation-based education: different techniques exist, but there are essential rules that should be followed in the debriefing arena, for the effectiveness of the simulation session. 22 Ensuring psychosocial safety and a supportive climate, by highlighting the need to ‘‘behave or perform without fear of negative consequences to self-image, social standing, or career trajectory”, is essential. Indeed, training facilitators in debriefing techniques are critical to ensure the effectiveness of the simulation program.
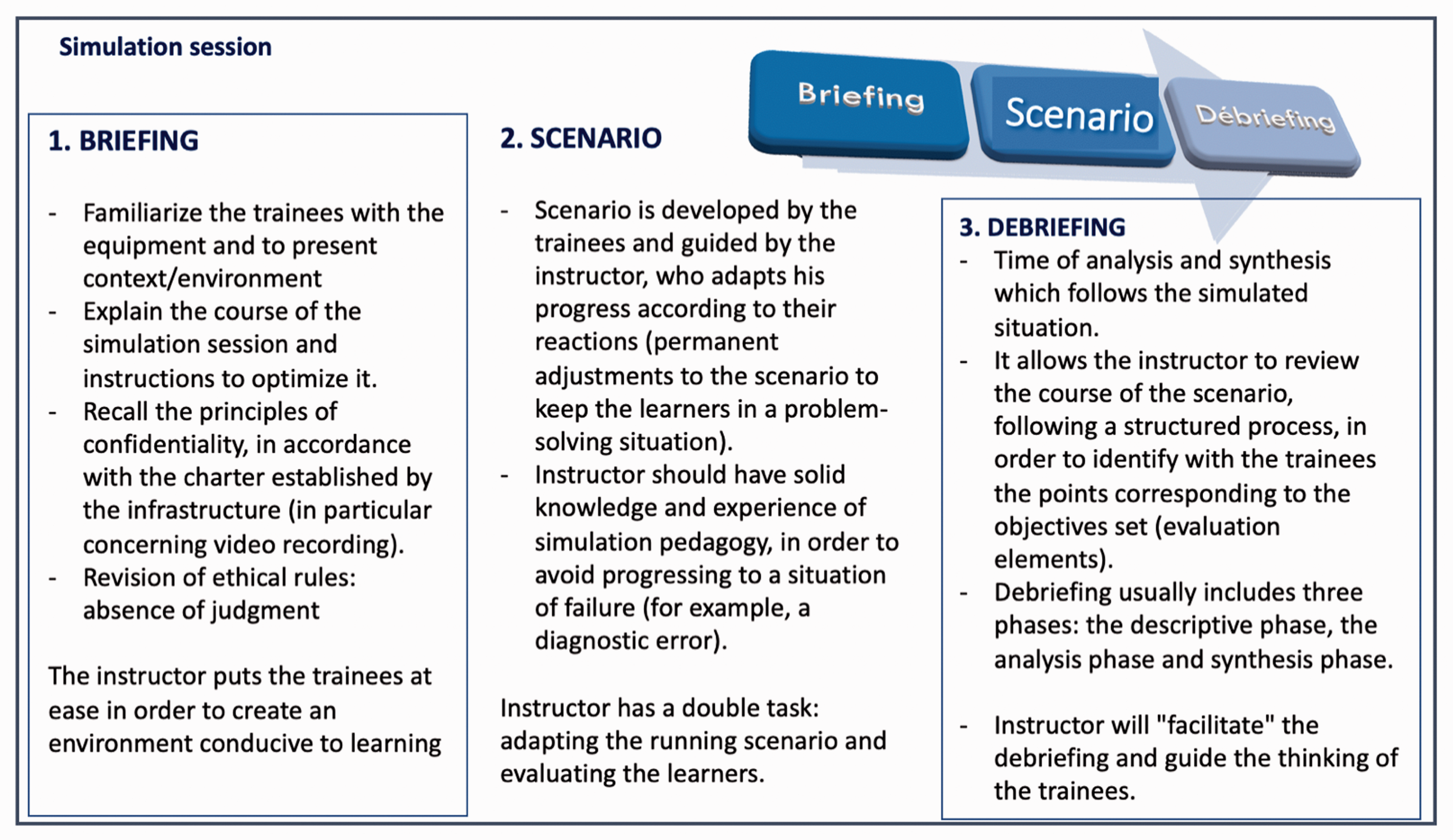
Schematic representation of the simulation session.
Technique 2: Procedural simulation
The significant evolution of the standard of care for stroke, with combined revascularization treatment, has brought the need to consider broadly applicable training standards and competences, as well as the credentialing requirements for practitioners.23,24 Traditionally, healthcare team members build up their expertise and skills on new procedures directly on patients, patients to potential risks during the learning curve process. 25
Moreover, the current traditional approach to training, based on numbers and volume of procedures done, does not guarantee that the trainee has acquired the ability to effectively and readily perform the procedure without tutoring. For technical skills, prospective, randomized, and blinded clinical studies have proved that trainees who acquired their skills on a simulator perform significantly better (40%–69% better) than their traditionally-trained colleagues. 26 Up to date, several neuro-simulators exist, enabling hands-on procedural training through different technologies using fully integrated systems.
For endovascular procedures, simulators of virtual reality allow the trainee to use a real endovascular device in a safe dimension and without any risk for the patient. A recent report demonstrated the feasibility and efficacy of the integration of a real stroke case scenario, with related neuroimaging, that allows transferring the real movements of the trainee to the virtual representation of the devices. 27 This simulation technology represents a new paradigm of procedural education, as allows the reproducibility of high-risk and high skilled procedures in a totally safe context. However, procedural simulations, in particular the ones with the new technologies, do have disadvantages. First, they depend on specific technological platforms that are expensive and need specific staff to be used and maintained.
Moreover, one procedural simulator can be used by only one trainee at times, making the training time-consuming. Last but not least, access to this technology is unavailable in remote areas. For the latter, a recent randomized study showed that the neuro-interventional training supported by a remote specialist with an online platform for live streaming of visual and audio data from an angiography suite provided similar technical results compared to training with local support. 28
Procedural simulation can be widely used in stroke treatment training, its implementation cannot entirely replace in vivo training, but it could be a primary delivery vehicle of abilities and standards, significantly accelerating the learning curve before taking care of real patients. It can ensure a standard benchmark of proficiency, allowing continuous performance evaluation and assessment.
Fourth step: Set up the simulation training – Description of case scenarios
The goal of simulation in the acute stroke setting is to reproduce scenarios for technical learning in a realistic environment with immediate feedback and learning goals assessment. Real-life clinical and/or professional situations, simple or complex, usual or exceptional, serve to support the construction of the clinical scenarios. The scenarios follow a plan to according to the objectives of the programs and to the experience of the instructors. They have one or two educational objectives and could carry on a different level of complexity. It is essential to test the scenarios before using them with learners in order to check out their feasibility and relevance. In addition, they must be fully understood by the trainers to ensure good interaction with the learners.
Each scenario should describe:
the target trainees; the educational objectives (technical and non-technical) and evaluation tools; the material resources; the necessary human resources (trainers, facilitators, standardized patients, etc.); the summary of the session:
duration; trainer/trainees ratio; the sequence of the simulation session: briefing, scenario development, debriefing; the main points of the debriefing; the methods for assessing learners,
The description of the scenario varies according to the simulation approaches and techniques used. A simulation training program can include one or more simulation sessions. Each simulation session takes place according to a pre-established standardized sequence and includes three distinct phases (Figure 2). The sequence has been described in the paragraph “technique 1: role-play simulation” and it is applied as well for other simulation techniques. The optimal number and time course of simulation sessions maximizing the learning curve should be anticipated, and decided accordingly to the type of simulation technique, the setting, the learning objectives, and the available human resources.
Evaluation of training in stroke medicine
Evaluation of simulation programs includes assessment of their impact on trainees and patient care and the quality of the simulation program itself.
For the evaluation of trainees, a four-level evaluation model has been extensively used. 29 This is common to other areas in healthcare training. The first level focuses on the satisfaction of the trainees on several aspects (such as objectives, content, simulation techniques, trainers, material) after the simulation session, which is evaluated by questionnaires. The second level is focused on knowledge, skills, and attitudes learning: have the educational objectives been achieved? Questionnaires, knowledge tests, exercises evaluating the translation of knowledge, observation, and interviews, if possible before and after the session, or self-evaluation by the trainee or between peers can be used. The third level assesses “behavioral changes” related to the simulation session and the transfer of learning. The aim is to evaluate whether the newly acquired knowledge, skills, and attitudes are used in professional practice. This measurement is, most of the time, carried out by questionnaires or interviews and can be carried out several times (at the beginning, at the end, and sometime after the simulation session). The fourth level makes it possible to assess the quality improvement of trainees on patient’s care, such as the impact treatment delays or the rate of correct diagnosis or treatment workout.
It is essential to evaluate the strengths and weaknesses of the simulation program continually. This evaluation is part of quality management and allows at identifying the difficulties encountered during its implementation, highlighting the points to be improved and to suggest solutions.
Conclusion
Considering that simulation is a useful tool for education and training in stroke medicine, the ESO Simulation Committee believes that simulation education should be made available and accessible to every European stroke professional. This consensus document provides insights into the simulation technique characteristics and strengths with the aim to fulfill the mission of the Committee within the ESO, which it to promote and support the development of simulation programs for stroke education in the stroke centers according to the principles and the methodology of the simulation technique. The implementation of the simulation programs in the European stroke centers will contribute to building up a safe and standardized high level of care.
Key points: General rules to set up a simulation training in stroke care
1–2 stroke expert simulationists as instructors in the simulation stroke program; Definition of objectives (Box 1) and measurement tools for trainee’s competence assessment; Definition of the target trainees, by promoting multidisciplinary participation in order to reflect real-life variety of healthcare professionals involved in stroke care (multidisciplinary programs with collaborative practice are strongly recommended); Definition of the timetable of the program (date of start and end of the program, number of sessions); Description of the number of expected trainees in order to ensure maximum interaction and hands-on practice wherever it applies; Preparation of a pre-specified plan for the session format (1 or more days or half a day sessions), by specifying the timetable of the session, always considering that debriefing should last at least 2/3 of the duration of simulation scenario*; Organization of the sessions with a correct proportion between instructors and trainees (1 instructor for maximum 5–6 trainees, depending on the experience of the instructor); Preparation of educational material for trainee’s participation in the simulation session (pre-required know-what and know-why); Development of evaluation sheet for trainee’s assessment according to the learning points and training goals; Preparation of the key points for the briefing based on the objectives of the simulation program; Preparation of the simulation scenarios adapted to the objectives of the simulation training program and tested them with a group of trainers before starting the program; Preparation of a survey for simulation training program ratings.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Not applicable.
Ethical approval
Not applicable.
Guarantor
BC.
Contributorship*
Barbara Casolla conceived the manuscript, the structure of the paper, literature search and writing of the manuscript. Maria Alonse de Lecinara, Raquel Neves, Waltraud Pfeilschifter, Veronika Svobodova, Simon Jung, Andre Kemmling, Robert Mikulik, Paola Santalucia critically reviewed, edited and finally approved the final version of the manuscript.