
Abstract

E-Poster Discussion-Reperfusion Treatment I
AS02-074
THROMBECTOMY IN ACUTE ISCHEMIC STROKE PATIENTS WITH NIHSS 5 OR LOWER.
1Oslo university Hospital, Neurology, Oslo, Norway
2Oslo University Hospital Rikshospitalet, Neurology, Oslo, Norway
3Oslo University Hospital, Neuroradiology, Oslo, Norway
Background and aims
It remains unclear whether patients presenting with large vessel occlusion strokes and mild symptoms benefit from mechanical thrombectomy (MT). The purpose of the present study was to compare outcomes in acute ischemic stroke patients with intracranial vessel occlusions and minor stroke symptoms (NIHSS 5 or lower) treated with MT with those who treated with intravenous thrombolysis (IVT) alone.
Methods
In a prospective observational study at Oslo University Hospital, we assessed the outcome in patients admitted with minor stroke (NIHSS 5 or lower), premorbid modified Rankin Scale 0–2, middle cerebral-M1/M2, intracranial carotid, anterior cerebral or basilar artery occlusions. Groups receiving MT and IVT only were compared. Clinical outcome with improvement of NIHSS from baseline to 24 hours and modified Rankin Scale at 3 months were compared as well as MT safety.
Results
Among 323 consecutive patients treated with EVT in 2017–18 48 (15.1%) had mild strokes with NIHSS 5 or lower at admission. All patients were assessed with perfusion imaging before MT. Median NIHSS was 1 after 24 hours and median mRS after three months was 0 (range 0–3) in patients with NIHSS 5 or lower who were treated with MT. In the group of consecutive patients with NIHSS 5 or lower who were treated with IVT, median NIHSS after 24 hours was 1 (range 0–5) and median mRS 0 (range 0–3).
Conclusion
Thrombectomy in selected patients with low NIHSS is safe and can increase the chance of excellent clinical outcome after 3 months. Larger prospective studies are needed.
Trial registration number
N/A
AS02-008
CLINICAL EFFECT OF SUCCESSFUL REPERFUSION IN PATIENTS PRESENTING WITH POSTERIOR CIRCULATION LARGE VESSEL OCCLUSION: DATA FROM A MULTICENTER REGISTRY
1Inselspital Bern, Neurology, Bern, Switzerland
2University Hospital Bern- Inselspital- University of Bern, University Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland
3University Hospital Bern- Inselspital- University of Bern, Department of Neurology, Bern, Switzerland
Background and Aims
Mechanical thrombectomy (MT) in patients with acute large vessel occlusions (LVO) in the posterior circulation (PC) is currently not evidence-based. Aims of this study were (1) to assess the safety of MT in this setting compared to MT of LVO in the anterior circulation (AC) and (2) to evaluate the clinical effect of reperfusion.
Methods
In the multicenter BEYOND-SWIFT registry (NCT03496064), the effect of successful reperfusion was evaluated using multivariable logistic regression analyses (adjusted Odds Ratios, aOR and 95% confidence intervals, 95%-CI). The primary outcome was a favorable outcome at 90 days (modified Rankin Scale (mRS) 0–3). Safety outcomes (mortality, symptomatic intracranial hemorrhage (sICH) and non-hemorrhagic clinical worsening) and efficacy, as measured by long-term functional outcomes, in MT patients with LVO in the PC (N = 207) were compared to patients presenting with LVO in the AC (N = 1832).
Results
Patients with successful reperfusion of LVO in the PC had higher rates of favorable outcome (mRS 0–3, 51.2% vs 23.8%, P = 0.021), but this effect was not significant after adjusting for confounding variables (aOR 2.652, 95%-CI 0.841–8.363). However, successful reperfusion was significantly correlated with lower mortality (aOR 0.169, 95%-CI 0.055–0.517) and reduced the risk of sICH (aOR 0.092, 95%-CI 0.018–0.467). On mRS shift analysis, successful reperfusion significantly increased the odds of reaching a lower mRS category (aOR 4.158, 95%-CI 1.525 – 11.336).
Conclusions
Successful reperfusion seems beneficial in patients presenting with LVO in the PC by reducing mortality and the incidence of sICH. Randomized controlled trials comparing patient selection strategies and concomitant medical treatment are warranted.
Trial registration number
NCT03496064
AS02-038
RISK OF BRAIN TISSUE INFARCTION IN PATIENTS WITH ACUTE ISCHEMIC STROKE TREATED WITH THEOPHYLLINE AS AN ADD-ON TO THROMBOLYTIC THERAPY
1Aalborg University Hospital, Neurology, Aalborg, Denmark
2Aarhus University Hospital, Neurology, Aarhus, Denmark
3Aarhus University, Centre of Functional Integrative Neuroscience, Aarhus, Denmark
Background and Aims
The vasoactive agent theophylline has shown neuroprotective effect with reduced brain tissue edema, brain damage and mortality in animal stroke models but the results were controversial in case series and previous randomized clinical trials. Recently we have shown significant early clinical improvement after theophylline but the tissue effect remains unclear.
Hypothesis: Theophylline as add-on to standard thrombolytic therapy reduce the risk of brain tissue infarction
Methods
The TEA-Stroke Trial is a two-center, proof of concept phase II clinical study with a randomized, double-blinded, placebo-controlled design. Patients with acute ischemic stroke verified by MRI and NIHSS≥4 were randomized 1:1 to either theophylline or placebo as an add-on to standard thrombolytic therapy. We will use logistic regression at voxel level to examine reduction in tissue risk of infarction predicted by imaging markers. Assuming a better predictive accuracy, a deep convolutional neural network was trained on data only from the placebo group to predict tissue outcome based on imaging. Actual and predicted outcome lesion volumes were compared to assess the effect of theophylline.
Results
The trial was stopped because of slow recruitment after randomization of 64 patients. The baseline characteristics were balanced and there were no safety concerns. A detailed analysis of risk of brain tissue infarction is ongoing and the results will be presented.
Conclusions
The TEA-Stroke Trial is the first study to evaluate whether the addition of theophylline to thrombolytic therapy reduces the risk of brain tissue infarction in patients with acute ischemic stroke.
Trial registration number
Trial Registration: EudraCT number 2013–001989-42
AS02-067
WAKE-UP: AGE AND TREATMENT RESPONSE AFTER THROMBOLYSIS IN STROKE PATIENTS WITH UNKNOWN ONSET
1Center for Stroke Research Berlin CSB, Neurology, Berlin, Germany
2DZHK German Center for Cardiovascular Research, Partner Site- Berlin, Berlin, Germany
3Berlin Institute of Health BIH, Neurology, Berlin, Germany
4Charité – Universitätsmedizin Berlin, Klinik und Hochschulambulanz für Neurologie, Berlin, Germany
5Hospices Civils de Lyon, Service de Biostatistique, Lyon, France
6Centre National de la Recherche Scientifique- UMR 5558, Laboratoire de Biométrie et Biologie Evolutive- Equipe Biostatistique-Santé, Villeurbanne, France
7University Hospitals Leuven, Department of Neurology, Leuven, Belgium
8VIB-KU Leuven Center for Brain Disease Research, Laboratory of Neurobiology, Leuven, Belgium
9KU Leuven–University of Leuven, Department of Neurosciences- Experimental Neurology, Leuven, Belgium
10University of Glasgow, Institute of Neuroscience and Psychology, Glasgow, United Kingdom
11Université Claude Bernard Lyon 1, Department of Stroke Medicine, Lyon, France
12Hospices Civils de Lyon, Neurology, Lyon, France
13Institut d’Investigació Biomèdica de Girona, Department of Radiology- Hospital Universitari Doctor Josep Trueta, Girona, Spain
14University of Glasgow, Robertson Centre for Biostatistics, Glasgow, United Kingdom
15Aarhus University Hospital, Department of Neurology-, Aarhus, Denmark
16Universitätsklinikum Hamburg–Eppendorf, Klinik und Poliklinik für Neurologie- Kopf- und Neurozentrum, Hamburg, Germany
17DZNE German Center for Neurodegenerative Diseases, Partner Site- Berlin, Berlin, Germany
18Medical Park Humboldtmühle, Department of Neurology, Berlin, Germany
Background and Aims
The influence of age on the treatment effect of thrombolysis is unknown in patients with wake-up stroke.
Methods
All patients screened in the WAKE-UP trial and with a visible lesion on diffusion-weighted imaging (DWI) were eligible for this pre-specified substudy. Clinical characteristics were compared between young (<55 years) vs. old (≥55 years) patients and among age quartiles. Among randomized patients, the treatment effect of thrombolysis was compared between young vs. old patients and across quartiles of age using logistic regression analyses.
Results
Overall, 1,101 patients included in WAKE-UP had a DWI lesion on MRI of which 181 patients (16.4%) were <55 years old. Older patients were more likely to have arterial hypertension (20.4% vs. 60.4%), atrial fibrillation (3.3% vs. 9.7%), hypercholesterolemia (13.8% vs. 36.3%), and diabetes mellitus (7.2% vs. 18.4%, all p < 0.01). Younger patients demonstrated a higher proportion of current smokers (55.4% vs. 26.4%, p < 0.01) and larger mean DWI lesion volumes (20.8 vs. 13.1 ml, p = 0.01). Among randomized patients (n = 490), age had no effect on the treatment effect of thrombolysis neither when comparing young vs. old patients nor using quartiles of age (p for interaction: 0.96 and 0.80, respectively).
Conclusions
In stroke patients with unknown onset enrolled in WAKE-UP, risk factors differed by age. Age had no significant effect on the treatment effect of thrombolysis. Therefore, our data do not support age as a criterion for therapeutic decision making in this stroke Population.
Trial registration number
NCT01525290
AS02-045
EVALUATION OF HEMORRHAGIC TRANSFORMATION RATES WITH NEUROPROTECTION (3K3A-APC) CO-ADMINISTRATION
1Cedars Sinai Medical Center, Neurology, Los Angeles, USA
2University of California Los Angeles, Psychiatry and Biobehavioral Sciences, Los Angeles, USA
Background and Aims
Activated protein C (APC) mediates activation of protease-activated receptor 1 (PAR1), whose agonism has been shown in preclinical models to have neuroprotective effects in central nervous system disorders. Using 3K3A-APC, we evaluated the effects in patients with acute ischemic stroke when co-administered with conventional recanalization treatments (intravenous tissue plasminogen activator or thrombectomy) in reduction of post-treatment hemorrhage.
Methods
Utilizing the NeuroNEXT trial NN104 (RHAPSODY) database, susceptibility weighted and gradient echo images were graded for intracerebral hemorrhage size according to radiographic criteria described in ECASS (Hemorrhagic infarction type 1 and 2 and parenchymal hematoma type 1 and 2) at four time points post-treatment (Day 0, 7, 30, and 90). Images were graded by two individuals blinded to treatment, with an expert providing consensus reads. Analysis was performed for the presence of any bleed at any time using a logistic regression model and controlled for both patient demographics and treatment (placebo versus drug).
Results
Overall, 101 patients were evaluated and patients who received the placebo were more likely to have hemorrhage at any time compared with those that received any amount of drug (p < 0.05; OR = 2.73,1.08–7.54). There was no significant difference in patient demographics (age, gender, diabetes, or time to treatment/thrombectomy) in the predilection for hemorrhage.
Conclusions
When grading hemorrhagic transformation using ECASS definitions, the neuroprotectant 3K3A-APC showed to have significant effects in prevention of hemorrhage when co-administered with conventional treatment.
Trial registration number
NeuroNEXT trial NN104 (RHAPSODY)
E-Poster Discussion-Prevention and Risk Factors
AS22-031
ALBUMINURIA AND STROKE RISK: A SYSTEMATIC REVIEW AND META-ANALYSIS
1Centre for the Prevention of Stroke and Dementia- University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
Albuminuria has been proposed as a sensitive biomarker of systemic endothelial dysfunction. A previous meta-analysis of 10 observational cohort studies demonstrated that participants with albuminuria had a 71% greater risk of stroke compared with those without.
Methods
We did a systematic review to February 2018 (MEDLINE/EMBASE) for cohort studies or randomized controlled trials that reported stroke incidence in adults according to baseline albuminuria +/− glomerular filtration rate (eGFR). Study and participant characteristics and relative risks (RR) were extracted. Estimates were combined using a random effects model. Heterogeneity was assessed by x2 statistics and I2, and by subgroup strata and meta-regression, with a particular focus on the impact of more complete adjustment for blood pressure (BP) on the association.
Results
We identified 36 studies comprising 1,728,135 participants with 26,994 stroke events. Overall, the presence of any level of albuminuria was associated with greater stroke risk (RR 2.12, 95%CI 1.75–2.58; p < 0.001) even after adjustment for established cardiovascular risk factors (RR 1.72, 1.51–1.95; p < 0.001). The association with albuminuria also remained after adjustment for multiple blood pressure measurements over previous months to years (RR 1.59, 1.29–1.94; p < 0.001), whereas the association of eGFR with stroke risk was much diminished (RR = 1.10, 1.04–1.18; p = 0.01).
Conclusions
Even after extensive adjustment, albuminuria is strongly and independently associated with incident stroke risk, possibly indicating a shared renal and cerebral susceptibility to vascular injury that is not fully explained by vascular risk factors.
Trial registration number
N/A
AS22-057
RISK FACTORS FOR INTIMAL AND MEDIAL CALCIFICATION OF THE INTRACRANIAL INTERNAL CAROTID ARTERY IN PATIENTS WITH HISTORY OF CARDIOVASCULAR DISEASE
1UMC Utrecht, Neuroradiology, Utrecht, The Netherlands
2UMC Utrecht, Radiology, Utrecht, The Netherlands
3UMC Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, The Netherlands
Background and Aims
Intracranial carotid artery calcification (ICAC) is an independent risk factor for stroke. ICAC occurring in the tunica intima is related to atherosclerotic disease, while when affecting the tunica media is a manifestation of Mönckeberg’s disease. In this study we aimed to identify the risk profiles associated with the type of calcification in patients with manifest arterial disease or increased cardiovascular risk factors.
Methods
We searched among participants of the Second Manifestations of Arterial Disease (SMART) study those that had undergone a non-contrast CT of the head. The pattern (predominantly intimal or predominantly medial) of ICAC was assessed by 2 raters on thin-slice reconstructed images using a previously histology-validated method. Association between common cardiovascular risk factors (age, sex, body mass index, hyperlipidemia, diabetes mellitus, hypertension, smoking status, HsCRP levels, MDRD) and type of calcification was assessed with adjusted Poisson regression analysis.
Results
475 patients (57% men, median age 58 years [range 24 - 79]) were assessed. 40.8% (n = 194), 26.5% (n = 126) and 32.6% (n = 155) had predominantly intimal, predominantly medial and absent or indistinguishable ICAC respectively. Older age was associated with both calcification types. Being male (RR 1.23; 95%CI 1.03–1.47) and a current smoker (RR 1.28; 95%CI 1.08–1.51) was associated with predominantly intimal calcification, while hyperlipidemia (RR 2.15; 95%CI 1.23–3.76) and lower levels of HsCRP (RR 0.97; 95%CI 0.95–1.00) were correlated to predominantly medial calcification.
Conclusions
Medial and intimal ICAC show different risk profiles. Our results may provide a starting point for more targeted therapy in the context of stroke prevention.
Trial registration number
N/A
AS09-018
PREVIOUS USE OF ASPIRIN AND BASELINE SEVERITY OF ISCHAEMIC STROKE: DATA FROM THE THIRD INTERNATIONAL STROKE TRIAL
William Whiteley Geoffrey Cohen Chiara Padiglioni Sara Mastrocola David Giannandrea Silvia Cenciarelli Peter Sandercock Stefano Ricci
1Città di Castello Hospital, Neurology, Città di Castello PG, Italy
2Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom
Background and Aims
Several reports have suggested a lower clinical severity in patients who were on aspirin when the stroke occurred, whereas others have indicated either no effect or even an increase of severity. We investigated this by analysing the IST-3 baseline data.
Methods
IST-3 was a large scale randomised trial of i.v. alteplase versus open control in 3035 patients with acute ischaemic stroke within 6 hours of onset. We extracted data on previous use of antiplatelet drugs (mostly aspirin) from the baseline and 7 day forms and compared stroke severity measured at randomisation in those who were already on aspirin and those who were not.
Results
Slightly more than half of the patients (51.5%) reported taking aspirin prior to stroke onset in the 2 days before randomisation. Aspirin users compared with non-users were significantly older (mean age 79 vs 75, p < 0.0001), and had a higher prevalence of atrial fibrillation (35.5% vs 24.4%, p < 0.0001), but had a similar gender distribution (female 49.9%). When we compared the NIHSS score at randomization, we found that patients who had received aspirin before randomisation had slightly more severe strokes than those who did not (median 11 vs 10, Wilcoxon test, p = 0,004). However, after adjusting for age, atrial fibrillation and delay from stroke to randomisation there was no significant effect of previous aspirin use on stroke severity at onset (p = 0.49).
Conclusions
In this large data set aspirin users had similar stroke severity to non users, after taking into account confounding variables.
Trial registration number
N/A
AS03-034
CHONIC CORTICAL CEREBRAL MICROINFARCTS SLOW DOWN COGNITIVE RECOVERY AFTER ACUTE ISCHEMIC STROKE
1Bordeaux University Hospital, Stroke unit, Bordeaux, France
2Kyoto university, Radiology, Kyoto, Japan
3Bordeaux university hospital, Neuroradiology, Bordeaux, France
Background and Aims
Cortical cerebral microinfarcts (CMI) have been associated with vascular dementia and Alzheimer’s disease. The aim of the present study was to evaluate the role of cortical CMI detected on 3T MRI, on the evolution of cognition during the year following an acute ischemic stroke.
Methods
We conducted a prospective and monocentric study, including patients diagnosed for a supra-tentorial ischemic stroke with a NIHSS ≥ 1, without pre-stroke dementia or neurological disability. Cortical CMI were assessed on a brain 3T MRI realized at baseline, as well as markers of small vessel disease (SVD), stroke and cortical volumes. Cognitive assessment was performed at three time-points (baseline, three months and one-year) using the Montreal Cognitive Assessment (MoCA), the Isaacs set test (IST), and the Zazzo’s cancellation task (ZCT). Generalized linear mixed models were performed to evaluate the relationships between the number of cortical CMI and changes in cognitive scores over one-year.
Results
Among 199 patients (65 ± 13 years old, 68% men), 88 (44%) had at least one cortical CMI. Hypertension was the main predictor of a higher cortical CMI load (B = 0.7, p < .001). The number of cortical CMI was associated with an increase time at the ZCT over one-year (B = 4.31, p = 0.007), regardless of the other MRI markers, stroke severity and demographic factors.
Conclusions
Cortical CMI are additional MRI markers of poorer processing speed after ischemic stroke and can be considered as a cerebral frailty condition which counteracts to the recovery process, suggesting a reduced brain plasticity.
Trial registration number
N/A
AS03-004
THE ROLE OF LEFT ATRIAL ENLARGEMENT ON DETECTION OF ATRIAL FIBRILLATION WITH INSERTABLE CARDIAC MONITORS: INSIGHTS FROM THE CRYSTAL AF STUDY
1Medtronic, Diagnostics and Monitoring Research, Mounds View, USA
2Università Cattolica del Sacro Cuore, Cardiology, Rome, Italy
3Medtronic, Cardiac Rhythm and Heart Failure, Mounda View, USA
4National & Kapodistrian University of Athens, Neurology, Athens, Greece
Background and Aims
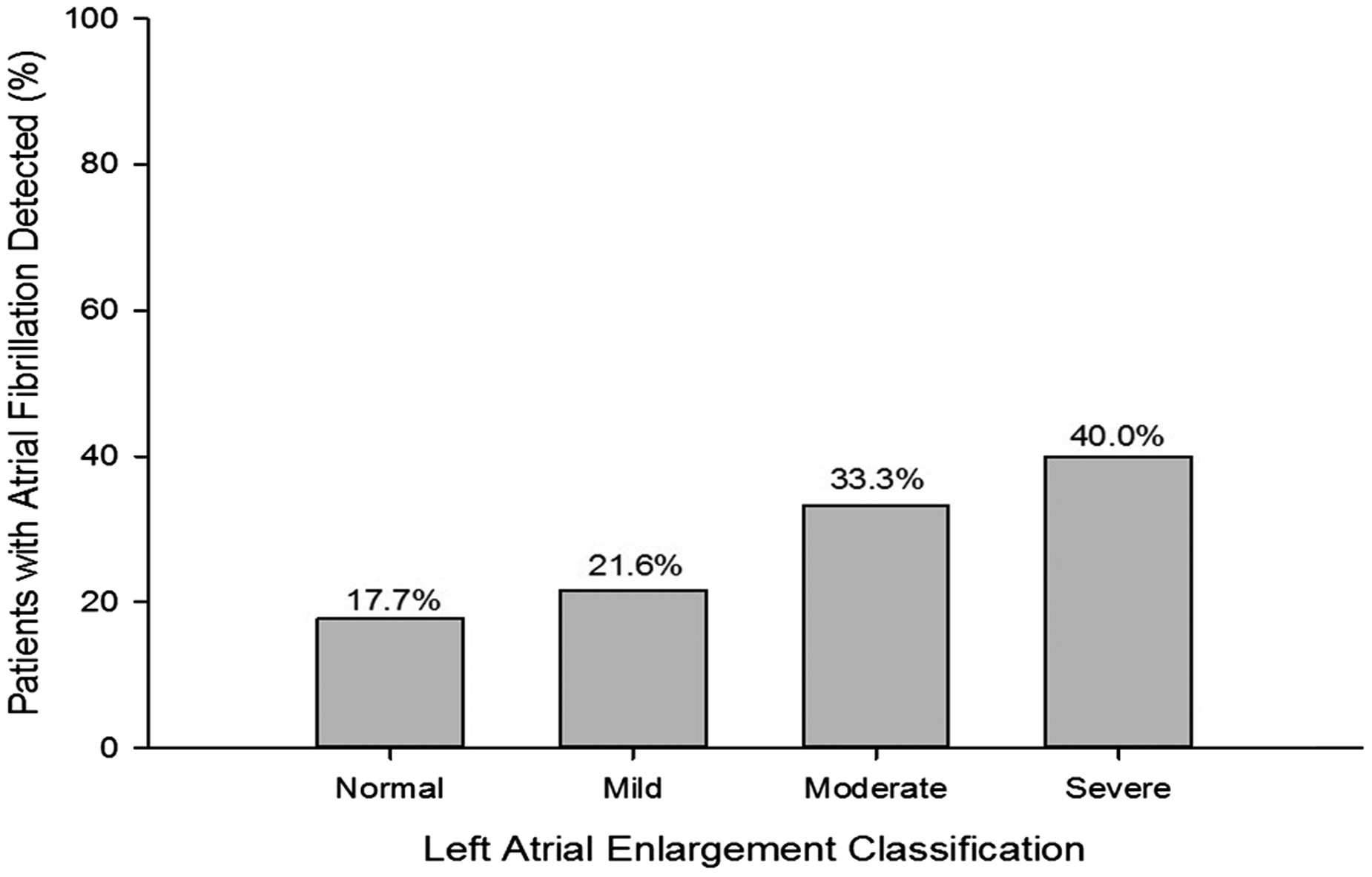
Trials are underway to investigate whether prophylactic oral anticoagulation (OAC) is superior to aspirin for recurrent stroke prevention among patients with cryptogenic stroke and atrial cardiopathies, such as left atrial enlargement (LAE). We investigated the relationship between LAE and atrial fibrillation (AF) detected by insertable cardiac monitors (ICM).
Methods
Cryptogenic stroke patients with ICMs from the CRYSTAL AF study were included. LAE was classified as normal, mild, moderate, or severe based on gender and left atrial diameter measurements. We assessed the percentage of patients with AF detected who had normal/mild vs. moderate/severe LAE and analyzed the incidence of AF according to LAE classification.
Results
A total of 116 ICM patients (60.8 ± 11.4 years, 68% male) with LAE data available were included and followed for 21.3 ± 8.5 months. LAE was defined as normal, mild, moderate, and severe in 53.4%, 31.9%, 10.3%, and 4.3% of patients, respectively. Among the 25 patients with AF detected, 76% had normal/mild LAE and 24% had moderate/severe LAE. AF incidence increased with LAE severity (p = 0.13, Cochran-Armitage Trend Test - Figure) but never reached a majority of patients.
Conclusions
Most cryptogenic stroke patients with AF did not have appreciable LAE. Although AF incidence increased with LAE severity, only a minority with even the most severe LAE had AF detected. Therefore, prophylactic OAC in patients with LAE may not be an effective stroke prevention strategy.
Trial registration number
NCT00924638
E-Poster Discussion-Outcome Complications and Prognosis I
AS17-161
POST-STROKE FATIGUE: A SEVEN-YEAR FOLLOW-UP STUDY (RESULTS FROM THE SAHLGRENSKA ACADEMY STUDY ON ISCHEMIC STROKE)
1Institute of Biomedicine, Department of Laboratory Medicine, Gothenburg, Sweden
2Department of Clinical Genetics and Genomics, Sahlgrenska University Hospital, Gothenburg, Sweden
3Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Gothenburg, Sweden
4Department of Neurology, Sahlgrenska University Hospital, Gothenburg, Sweden
5Institute of Psychology, University of Gothenburg, Gothenburg, Sweden
Background and Aims
Post-stroke fatigue (PSF) is a common, yet often overlooked, consequence after stroke with impact on quality of life. We aimed to identify features associated with PSF in the long-term after stroke.
Methods
This study comprises 432 patients, aged 18–69 years at index ischemic stroke, with follow-up after seven years. Vascular risk factors and inflammatory biomarkers hsCRP and interleukin 6 were determined at baseline. At follow-up, PSF was assessed by the Daily Fatigue Impact Scale, cognitive function by the Barrow Neurological Institute Screen for Higher Cerebral Functions, affective symptoms by Hospital Anxiety and Depression Scale, nocturnal insomnia by the Karolinska Sleep Questionnaire, neurologic deficit by the National Institutes of Health Stroke Scale, pain by 36-Item Short Form Survey and physical activity by a questionnaire. Associations between PSF and baseline and 7-year variables were analysed with Pearson’s correlation or Student’s t-test, and we also performed analyses stratified by sex.
Results
PSF was significantly associated with female sex and stroke severity (baseline NIHSS), but not with vascular risk factors or inflammatory biomarkers. Among 7-year variables, PSF was strongest correlated with poor functional outcome (modified Rankin Scale), level of physical activity, depressive symptoms, anxiety, insomnia, and pain (Table 1). The association with insomnia was stronger in women than in men (two-way ANOVA interaction analysis p = 0.036).

Conclusions
Our results indicate a complex interplay between PSF, gender and long-term post-stroke outcomes, but no association between vascular risk factors or inflammatory biomarkers and PSF the in long-term was found. Future studies examining predictors of PSF are warranted.
Trial registration number
N/A
AS17-089
LIFE SATISFACTION AFTER STROKE IN UK BIOBANK PARTICIPANTS
1University of Cologne- Faculty of Medicine and University Hospital Cologne, Department of Neurology, Cologne, Germany
2University College London, Queen Square Institute of Neurology, London, United Kingdom
Background and Aims
We investigated the relationship between focal brain injury in stroke and life satisfaction in UK Biobank.
Methods
We examined data from 502 642 British UK Biobank participants, contrasting neuropsychological measures of 2 529 stroke patients with presumed focal brain injury and a healthy comparison group of 168 829 participants by means of chi-2-tests (level of significance: p < 0.001). In ancillary analyses, we focused on subgroups of stroke patients with diagnosed paresis or speech impairments and those unable to work due to their illness.
Results
Statistically significant differences were observed for happiness, family, health and financial satisfaction measures, originating from only minor percentage decreases (1-2%) in case of the former and considerable ones (5-19%) in case of the latter two. Friendship satisfaction did not yield significant differences. While stroke participants unable to work differed significantly in all of the categories evaluated here, no differences emerged in case of paresis or speech impairments other than for health satisfaction (c.f. Table 1).

Conclusions
While focal brain injury in stroke degrades life satisfaction, it does so most prominently when it inhibits return to employment. Neither motor paresis nor language impairment lead to any measurable differences in the evaluated categories other than health satisfaction. Friendship satisfaction seems to be sustained particularly well.
Trial registration number
N/A
AS17-173
LONG-TERM HEALTH-RELATED QUALITY OF LIFE IN PATIENTS WITH INTRACEREBRAL HEMORRHAGE AND INTRAVENTRICULAR HEMORRHAGE
1Johns Hopkins Hospital, Anesthesiology and Critical Care Medicine, Baltimore, USA
2Johns Hopkins University, Neurology, Baltimore, USA
3Johns Hopkins University, Neurology- Anesthesiology and Critical Care Medicine, Baltimore, USA
Background and Aims
Although functional recovery in Intracerebral Hemorrhage (ICH) and Intraventricular Hemorrhage (IVH) has been described, little is known regarding the long-term health-related quality of life (HR-QoL) of survivors.
Methods
We studied survivors (N = 732) enrolled in the MISTIE III and CLEAR III trials, and compared EuroQoL (EQ) visual analog scale (VAS) scores by dichotomized “good” (modified Rankin Scale [mRS] score 0–3) versus “poor” (mRS score 4–5) functional outcome at day 30 (D30), 180 (D180) and 365 (D365); and evaluated the percentage of patients by functional outcome after dichotomizing responses, “no problems” versus “problems,” to EQ dimensions at D30 and D365.
Results
Median (interquartile range [IQR]) EQ VAS score for “good” versus “poor” functional outcome participants: D30 (70 [60-80] v. 40 [20-55]), D180 (77 [60-90] v. 50 [35-70]) and D365 (80 [65-90] v. 50 [40-70]). The median increase for EQ VAS score between D30 to D180 was 20 (IQR 5–40), and 16.5 (IQR 0–35) for D30 to D365. At D30 and D365, good functional outcome participants performed best (“no problems”) in self-care (68.8% and 69.1%) and performed worst (“problems”) in usual activities (73% and 66.6%). Poor functional outcome participants performed best in pain/discomfort (40.5%) at D30 and anxiety/depression (44.4%) at D365. This group performed worst in mobility (99.2%) and usual activities (98.5%) at both time points.
Conclusions
EQ VAS increases substantially between D30 and D180, but not significantly from D180 to D365. QoL impairments vary with functional level (mRS). Nearly 40% of patients with poor functional outcome reported “no problems” with pain/discomfort and anxiety/depression.
Trial registration number
N/A
AS17-132
CLINICAL FRAILTY INDEPENDENTLY PREDICTS EARLY MORTALITY AFTER ISCHAEMIC STROKE
1University of Cambridge, Department of Medicine, Cambridge, United Kingdom
2Cambridge University Hospitals NHS Foundation Trust, Department of Medicine for the Elderly, Cambridge, United Kingdom
3University of Cambridge, Department of Clinical Neurociences, Cambridge, United Kingdom
Background and Aims
Clinical frailty has emerged as an important syndrome for clinical care and research; independently predicting morbidity and mortality across a range of medical conditions. However, there has been little research into the role of frailty in stroke. This study investigates the effect of frailty on both 28-day mortality following ischaemic stroke and outcomes after stroke thrombolysis.
Methods
Frailty was measured at the time of admission using the Clinical Frailty Scale (CFS) for all ischaemic stroke admissions aged ≥75 years. Co-morbidities and clinical outcomes were collected retrospectively, blinded to CFS score.
Results
In 433 individuals with ischaemic stroke, each one-point increase in the CFS was independently associated with increased 28-day mortality after adjustment for age, sex, cardiovascular risk factors, and stroke severity (OR 1.03 (1.01–1.05), p < 0.01). In 63 thrombolysed individuals, whilst there was no difference in presentation stroke severity between ’non-frail and ’frail’ individuals (median NIHSS (IQR): 12.5 (9.25) versus 15 (11.5), p = 0.17), after thrombolysis ‘non-frail’ individuals had a significantly lower median NIHSS than ’frail’ individuals (5 (10.5) versus 16 (16.5), p < 0.01). On multivariable analysis, CFS remained independently associated with poorer neurological recovery (each one-point increase in CFS was associated with a one-point decrease in NIHSS improvement after thrombolysis: linear regression coefficient 1.07, p = 0.03) and 28-day mortality (OR 1.05 (1.001–1.09), p = 0.048).
Conclusions
Clinical frailty is independently associated with 28-day mortality after ischaemic stroke, and poorer neurological recovery for individuals receiving thrombolysis. This has important practical implications for clinical prognostication, service organisation, and future research into reducing the impact of frailty on stroke recovery.
Trial registration number
N/A
AS17-142
HISPANIC YOUNG STROKE PATIENTS HAVE A HIGHER RISK OF MORTALITY THAN CAUCASIAN AND ASIAN PATIENTS: THE GLOBAL OUTCOME AFTER STROKE AT YOUNG AGE (GOAL)-INITIATIVE
1Radboud University Medical Centre- Donders Institute for Brain- Cognition and Behaviour, Department of Neurology, Nijmegen, The Netherlands
2Helsinki University Hospital, Department of Neurology, Helsinki, Finland
3North Tees and Hartlepool, NHS Foundation trust, Stockton on Tees, United Kingdom
4National Institute of Neurology and Neurosurgery of Mexico, Manuel Velasco Suárez, Mexico city, Mexico
5Inselspital University Hospital- University of Bern, Department of Neurology, Bern, Switzerland
6Hospital Dr. Rafael A. Calderon Guardia, Neurosciences Department, San Jose, Costa Rica
7Lucerne Cantonal Hospital, Neurocenter- Department of Neurology and Neurorehabilitation, Luzern, Switzerland
8Vrije Universiteit Brussel, The Faculty of Medicine and Pharmacy, Jette, Belgium
9Mongolian National Univeristy of Medical Sciences, International School of Traditional Medicine, Uluunbaatar, Mongolia
10Taipei Medical University, Depatrment of Global Health and Development, Taipei, Taiwan R.O.C
11Inserm, Bordeaux Population Health Research Centre, Bordeaux, France
12Tel Aviv University, School of Medicine- Sackler Faculty of Medicine, Tel Aviv, Israel
13Medical University of Graz, Department of Neurology- Department of Radiology- division of neuroradiology, Graz, Austria
14Istanbul University- Faculty of Medicine, Department of Neurology, Istanbul, Turkey
15Medical University of Graz, Department of Neurology, Graz, Austria
16Haukeland University Hospital, Centre for Neurovascular Diseases- Department of Neurology, Bergen, Norway
17Ashford and St Peter’s Hospitals, Department of Stroke Medicine, Chertsey, United Kingdom
18University of Central Florida, Stroke Center- Orlando VA Medical Center, Orlando, USA
19SARAH Hospital of Rehabilitation, Department of Neurology, Brasilia, Brazil
20University of Gothenburg, Insitute of Biomedicine- the Sahlgrenska Academy, Gothenburg, Sweden
21University of Gothenburg, Institute of Neuroscience and physiology- the Sahlgrenska Academy, Gothenburg, Sweden
22Kyushu University, Department of Health Care Administration and Management- Center for Cohort Studies- Graduate School of Medical Sciences, Fukuola, Japan
23Hanyang University, Department of Neurology- College of Medicine, Seoul, Republic of Korea
24Kyushu University, Department of Medicine and Clinical Science- Graduate School of Medical Sciences- Center for Cohort Studies, Fukuola, Japan
25University of Maryland School of Medicine, Department of Neurology- Veterans Affairs Maryland Health Care System, Baltimore, USA
26Royal Adelaide Hospital, Department of Neurology, Adelaide, Australia
27University of Tartu, Department of Neurology and Neurosurgery, Tartu, Estonia
28Chang Gung Memorial Hospital- Linkou Medical Center- and College of Medicine- Chang Gung University, Department of Neurology, Taoyuan, Taiwan R.O.C
29University of Lille, Department of Neurology, Lille, France
30Universidade Nova de Lisboa, Department of Neurology- Hospital Egas Moniz- Centro Hospitalar Lisboa Ocidental and CEDOC- Nova Medical School, Lisbon, Portugal
31G.B. Pant Hospital, Department of Neurology, New Delhi, India
32Cleveland Clinic Abu Dhabi, Neurological Institute, Abu Dhabi, United Arab Emirates
33University of Ibadan, Department of Medicine- College of Medicine, Ibadan, Nigeria
34Inkosi Albert Luthuli Central Hospital, Department of Neurology- Nelson R. Mandela School of Medicine, Mayville, South Africa
35Waikato Hospital, Department of Neurology, Hamilton, New Zealand
36University of Toronto, Department of Medicine Neurology- University Health Network, Toronto, Canada
37Hospital Civil de Guadalajara Fray Antonio Alcalde, Department of Neurology, Guadalajara, Mexico
38University Medicine, Department of Neurology, Greifswald, Germany
39Hospital Civil de Guadalajara Fray Antonio Alcalde, Department of Neurology, Guadalajara, Mexico
40Sunnybrook Health Sciences Centre, Department of Medicine Neurology, Toronto, Canada
41University of Malaya, Department of Medicine, Kuala Lumpur, Malaysia
42Tel Aviv University, Department of Epidemiology and Preventive Medicine, School of Public Health, Sackler Faculty of Medicine, Tel-Hashomer, Israel
43Christchurch Hospital, Department of Neurology, Christchurch, New-Zealand
44University of Brescia, Department of Clinical and Experimental Sciences, Neurology Clinic, Brescia, Italy
Background and Aims
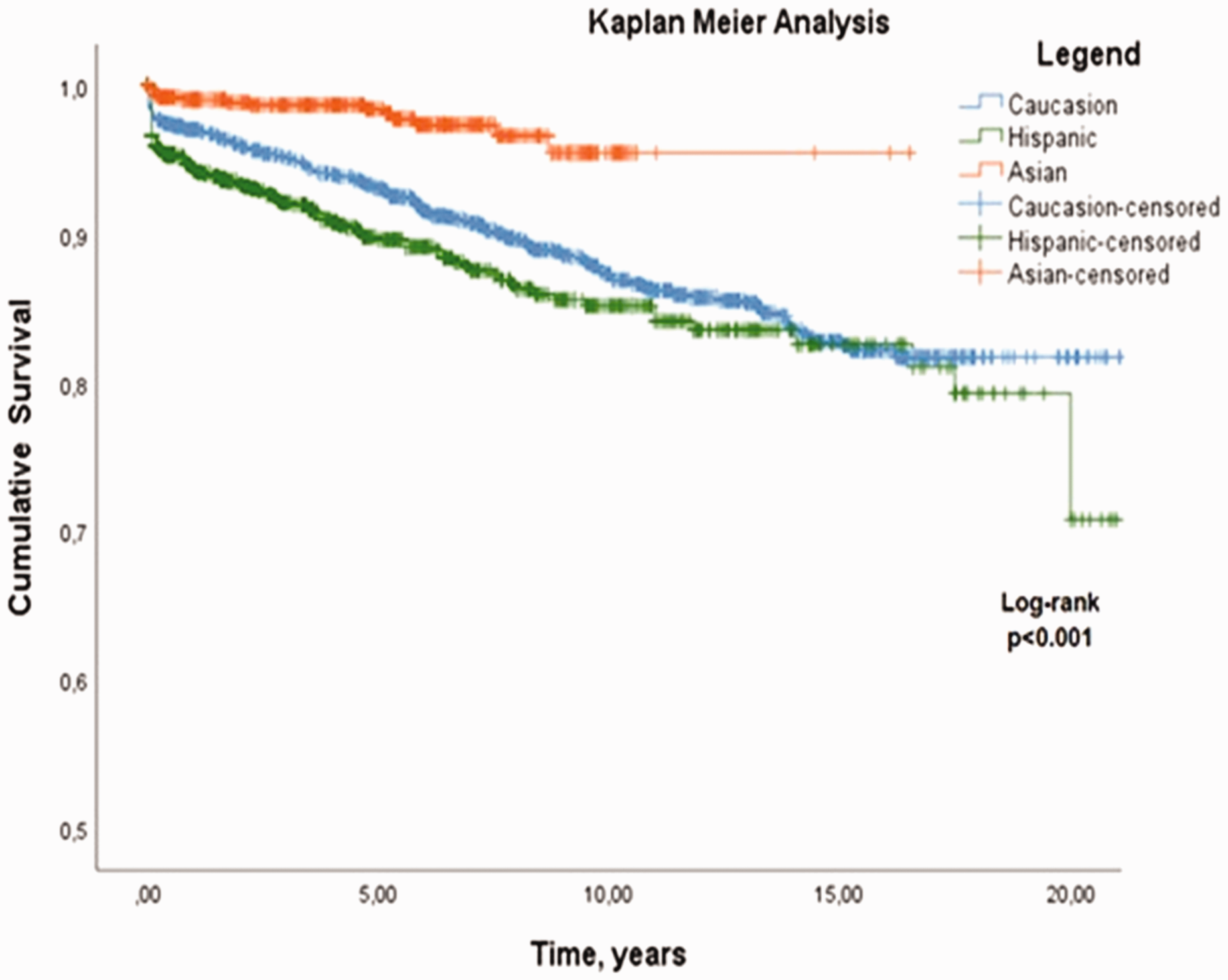
Young stroke patients have an increased long-term mortality, with high variability between studies. Exploring these differences may identify, possible modifiable, determinants of mortality. Therefore, we investigated the risk of mortality after young stroke between ethnicities worldwide.
Methods
Patients were participants in the GOAL study, a worldwide multicenter individual patient meta-analysis based on existing young stroke cohorts. We included all ischemic stroke patients aged 18–50 years old. Outcomes were all-cause mortality during follow-up in mortality rates and through Kaplan-Meier analysis, stratified for age, sex and ethnicity.
Results
Follow-up data was available for 3785 patients (mean age 39.8 ± 8.3 years; 56.6% men), 1593 (42.1%) Hispanic, 1446 (38.2%) Caucasian- and 746 (19.7%) Asian patients. During a median of 5.0 (IQR 1.4–9.6) years, 333 (8.8%) patients died. The mortality-rate of Hispanic patients was 22.3 per 1000 person-years, which was 1.8 (95%CI 1.4–2.2; p < 0.0001) times higher than the 12.7 per 1000 person-years for Caucasian patients. Asian patients had a mortality-rate of 4.5 per 1000 person-years, which was 0.4 (95%CI 0.2–0.6; p < 0.0001) times higher than Caucasian patients.
Conclusions
Risk of mortality varied five-fold between ethnicities. This could be due to differences in genetic profiles, but also due to modifiable risk-factors such as the prevalence of co-morbidities and cardiovascular risk-factors, as well as varying stroke-etiologies.
Trial registration number
N/A.
E-Poster Discussion-Epidemiology I
AS16-047
UNSPECIFIED STROKE: CHARACTERISTICS AND TIME-TRENDS ACROSS THREE DECADES IN THE POPULATION-BASED ROTTERDAM STUDY
1Erasmus MC University Medical Center, Epidemiology and Neurology, Rotterdam, The Netherlands
2Erasmus MC University Medical Center, Epidemiology, Rotterdam, The Netherlands
3Erasmus MC University Medical Center, Neurology, Rotterdam, The Netherlands
Background and Aims
Neuroimaging is required to determine the subtype (ischemic and hemorrhagic) of a clinically diagnosed stroke. However, patients suffering from a stroke may not be referred to a hospital, may die before reaching an imaging unit, or may decline further clinical care. In such instances, a stroke will remain unspecified. In this study, we determined trends, patient characteristics and prognosis of unspecified stroke over the last three decades.
Methods
We included 1,546 stroke-free participants from the population-based Rotterdam Study who suffered a stroke during follow-up between 1990 and 2016. We calculated the frequency of stroke subtypes for every year and patient characteristics between stroke subtypes. Furthermore, we estimated event-free survival (for recurrent stroke or death) using unadjusted (Kaplan-Meier) and age and sex adjusted survival curves.
Results
The percentage of unspecified stroke decreased from 63% in 1990 to 16% in 2016. Compared to specified strokes, patients with unspecified stroke were on average older (85.7 vs. 78.5 years) and had more often multimorbidity such as physical impairment and dementia. These patients with unspecified strokes were more often diagnosed by the nursery home physician (23.5% vs 1.1%) and were less often hospitalized (77.3% vs. 17.7%). Furthermore, patients with unspecified stroke had a higher probability of stroke recurrence or death immediately and years after stroke than those with ischemic stroke in both unadjusted and adjusted survival curves.
Conclusions
The burden of unspecified stroke has decreased in the last decades. However, patients with unspecified stroke are older and represent a frail patient group with a poor outcome.
Trial registration number
N/A
AS16-004
SURVEILLANCE OF TREND AND DISTRIBUTION OF STROKE MORTALITY BY SUBTYPE, AGE, GENDER, AND GEOGRAPHIC AREAS IN TIANJIN, CHINA, 1999–2016
1Tianjin center for disease control and prevention, Department of non-communicable disease prevention and control, Tianjin, China
Background and Aims
Analyze epidemiological transition trend and distribution of stroke mortality in Tianjin, China. Provide evidence for the control of stroke mortality and morbidity.
Methods
The study was based on 267511 stroke cases in Tianjin between 1999 and 2016. The cause of death was coded according to the ICD-10 into stroke subtypes. Standardized mortality rates were calculated for stroke and its subtypes, adjusted by age and gender using the year 2000 world standard population. The age, gender, and geographic distribution of stroke and subtype mortality were analyzed. χ2 -tests were used to determine the statistical significance of differences in mortality trends.
Results
The stroke mortality rate in Tianjin declined from151.30/100 000 (1999) to 86.58/100 000 (2016). The stroke mortality rate for males was higher than females. Stroke mortality rates increased with age. The subtypes of stroke have changed considerably in Tianjin. Hemorrhagic was major during 1999–2001, while cerebral infarction attained the first rank and accounted for more than 50% of stroke mortality in 2002–2016. The proportion of ischemic stroke was 66.66% in urban and over 13.33% higher than that in rural. Stroke in the suburban area was mainly hemorrhagic stroke, up to 66.11%.
Conclusions
There are significant differences in the distribution of stroke mortality by subtype, age, gender, and geographic area in Tianjin. The subtypes of stroke are associated with different risk factors and therefore require different public health prevention and control measures, as well as medical treatment. This study provides pertinent information for formulation of measures for the prevention and control of stroke.
Trial registration number
N/A
AS16-088
PREVALENCE AND IMPACT OF SEIZURES AT STROKE ONSET IN A POPULATION-BASED REGISTRY
1University of L’Aquila, Department of Neurology, L’Aquila, Italy
Background and Aims
We aimed to assess the prevalence and early prognostic impact of seizures at the onset (SaO) of a first-ever stroke (FES).
Methods
Prospective population-based registry including all the residents with a FES in 2011–2013 followed up to 5 years. SaO were defined as seizures within the first 24 hours from stroke onset.
Results
We included 1,280 patients with a FES, 52.6% women, mean age 76.1 ± 12.6 years; 919 (71.8%) patients had an ischemic and 361 (28.2%) a hemorrhagic stroke. SaO occurred in 44 (3.4%) patients and were generalized in 38 (86.4%) and focal in 6 (13.6%). Age and sex distribution, stroke type and stroke severity at onset (NIHSS score) were similar in patients with and without SaO. The 7- (P = 0.309) and 30-day case-fatality rates (P = 0.613) and the distribution of modified Rankin Scale scores at hospital discharge (P = 0.542) did not differ in patients with SaO compared with those without. The Cox analysis including age, sex, stroke type, stroke severity at onset, and vascular risk factors showed that stroke severity (hazard ratio [HR] 1.10, 95% confidence interval [CI] 1.08–1.12, P<0.001; HR 1.09, 95% CI 1.07–1.11, P<0.001) and hemorrhagic stroke (HR 2.34, 95% CI 1.56–3.52, P<0.001; HR 2.41, 95% CI 1.75–3.31, P<0.001) were the only predictors of 7- and 30-day case-fatality.
Conclusions
According to our population-based data, SaO are not a predictor of poor prognosis in patients with a FES, suggesting that the management of seizures in stroke patients should not interfere with the hyperacute therapeutic measures.
Trial registration number
N/A
AS16-076
TRENDS IN INCIDENCE RATES OF ACUTE STROKE AND 30-DAY CASE FATALITY RATES IN ENGLAND, 1999–2011: A RECORD-LINKAGE STUDY OF OVER 1 MILLION INCIDENT STROKES
Lucy Wright
1University of Oxford, Big Data Institute- Nuffield Department of Population Health, Oxford, United Kingdom
Background and Aims
Incidence rates of acute stroke have declined in high-income countries, but at a slower rate than mortality. There is only limited information on trends in stroke incidence rates in England, and on trends in short-term case-fatality in hospitalised individuals.
Methods
A linked dataset of national routine hospital statistics and mortality was analysed to calculate trends in stroke incidence rates and 30-day case fatality rates (CFR) between 1999 and 2011. In calculations of incidence rates, the numerators were the total number of hospital admissions plus out-of-hospital deaths, and the denominators were the mid-year population estimates for relevant calendar years, expressed per 100 000. To calculate CFR we divided the total number of deaths from any cause in people admitted with stroke by the total number of stroke admissions.
Results
There were 1,030,319 acute strokes, 55% in women. Between 1999 and 2011 age-standardised incidence rates decreased in men from 320.7 per 100 000 to 220.0, and in women from 263.2 to 178.7 (Figures 1,2). The reporting of stroke type in electronic patient records has improved: in 2011 only 15% were not classified as haemorrhagic or ischaemic stroke. There was a reduction in short-term mortality from 27% to 13% in men and from 28% to 17% in women at 30 days after hospitalisation for stroke (Figure3).
Conclusions
Hospitalised incidence rates from stroke fell by a third. Trends differed depending on stroke type, due to changes in reporting of stroke type, and by age and sex. 30-day case-fatality following stroke fell in men and women.
Trial registration number
N/A
AS16-081
QUALITY OF CARE AND MORTALITY FOLLOWING STROKE IN INDIVIDUALS WITH SCHIZOPHRENIA
1University of Toronto- University Health Network, Department of Psychiatry, Toronto, Canada
2Institute for Clinical and Evaluative Sciences, Cardiovascular Research Group, Toronto, Canada
3Institute for Clinical and Evaluative Science, Cardiovascular Research Group, Toronto, Canada
4University of Toronto- University Health Network, Faculty of Medicine, Toronto, Canada
5University of Toronto-Centre for Addiction and Mental Health, Department of Psychiatry, Toronto, Canada
Background and Aims
Individuals with schizophrenia appear to have a greater risk of death following stroke, compared to the general population. However, the reasons for this are not well understood. We used data from the province of Ontario, Canada, to compare stroke care and outcomes in people with and without schizophrenia.
Methods
We used the Ontario Stroke Registry to identify patients hospitalized with stroke between April 1, 2002 and March 31, 2013, and identified those with schizophrenia using validated algorithms. We compared processes of acute stroke care delivery in those with and without schizophrenia and used Cox proportional hazards models to examine the association between schizophrenia and mortality, adjusting for demographics, stroke severity, and processes of care.
Results
The study sample included 52,473 people, 612 (1.2%) of whom had schizophrenia. Individuals with compared to without schizophrenia were younger (median age 66 vs. 74 years) and more likely to arrive by ambulance (79.9% vs. 72.2%), but had longer median time between symptom onset and arrival at hospital (7.74 vs. 5.78 hours). The use of thrombolysis, stroke unit care, rehabilitation, and antiplatelet therapy was similar in those with and without schizophrenia; however, those with schizophrenia were less likely to undergo carotid imaging and to be treated with antihypertensive, lipid-lowering or anticoagulant medications. One year mortality was greater in those with compared to without schizophrenia (adjusted hazard ratio 1.32, 95% CI 1.14–1.54), even after adjustment for age, sex, and other factors.
Conclusions
Conclusion
Schizophrenia is associated with increased mortality after stroke, despite similar acute stroke care quality.
Trial registration number
N/A
E-Poster Discussion-Rehabilitation and Recovery
AS08-048
STROKE IN YOUNG ADULTS: WALKING SPEED AS AN INDICATOR FOR RETURN TO WORK
1Manchester Metropolitan University, Research Centre for Musculoskeletal Science and Sports Medicine, Manchester, United Kingdom
2Powys Teaching Health Board, Community Neuro Service- Newtown Hospital, Newtown, United Kingdom
3Cardiff and Vale University Health Board, Stroke Rehabilitation Centre- University Hospital Llandough, Cardiff, United Kingdom
4Betsi Cadwaladr University Health Board, Physiotherapy Department- Ysybyty Gwynedd, Bangor, United Kingdom
5Hywell Dda University Health Board, Neuro-Physiotherapy- South Pembrokeshire Hospital, Pembroke Dock, United Kingdom
6Cwm Taf University Health Board, Neuro-Physiotherapy Department- Keir Hardie University Health Park, Merthyr Tydfil, United Kingdom
7Abertawe Bro Morgannwg University Health Board, Physiotherapy Department- Morriston Hospital, Swansea, United Kingdom
Background and Aims
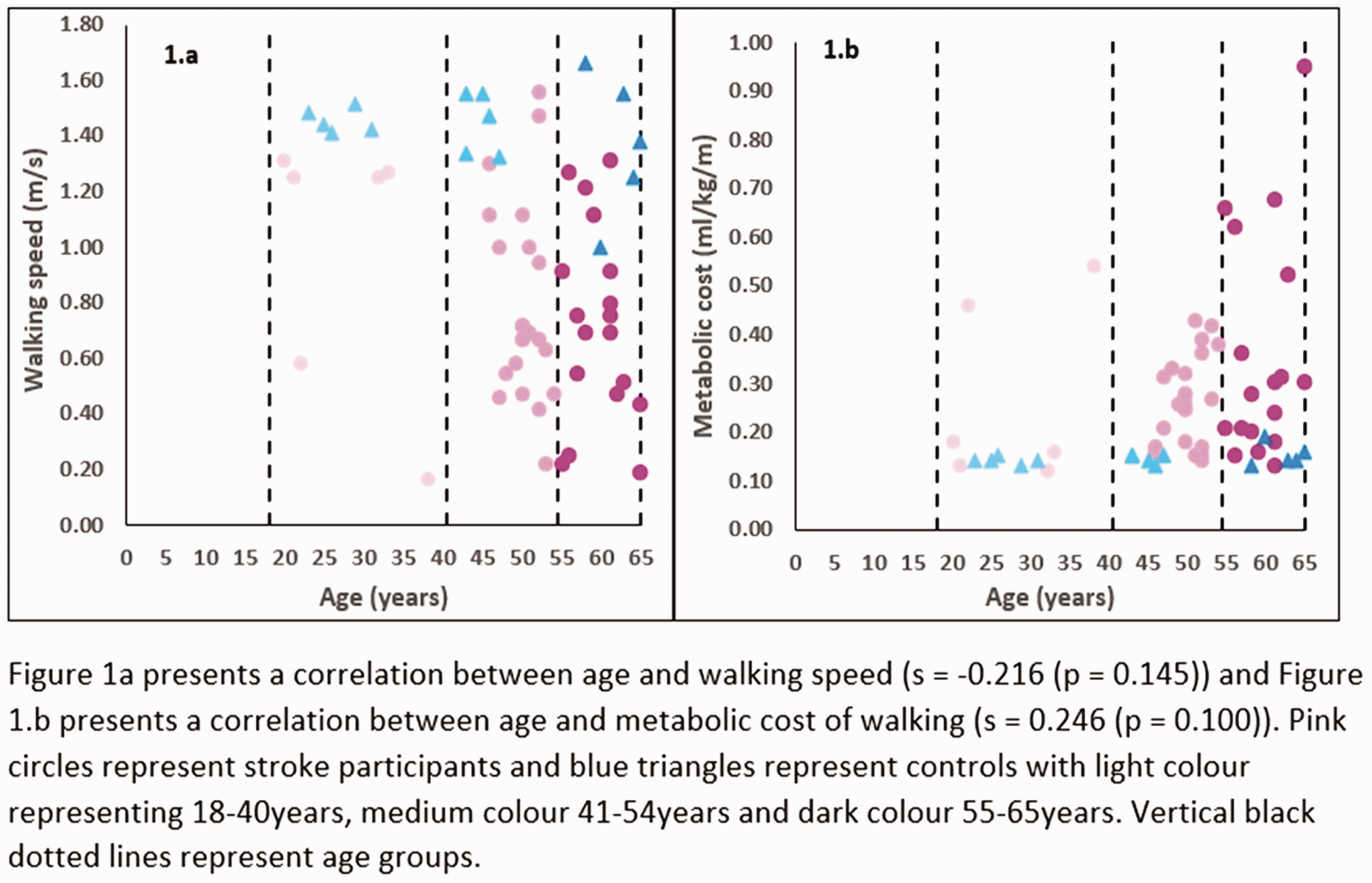
One in ten adults who experience a stroke are under the age of fifty years. Most are unable to return to employment or participate in social activities from their difficulties walking. No research study has comprehensively analysed how a stroke affects walking performance or efficiency in young adults. This study aimed to investigate how a stroke in young adults affects walking performance and energy cost during walking compared to healthy age-matched controls.
Methods
Participants who had experienced a stroke (18-40years: n = 6, 41–54years: n = 20, 55–65years: n = 15) and controls (n = 15) were recruited from six health boards in Wales, UK. Type, location and cause of stroke, occupation and smoking status were recorded. Walking performance was measured using three-dimensional gait analysis and energy cost through measurement of energy expenditure during three minutes of walking.
Results
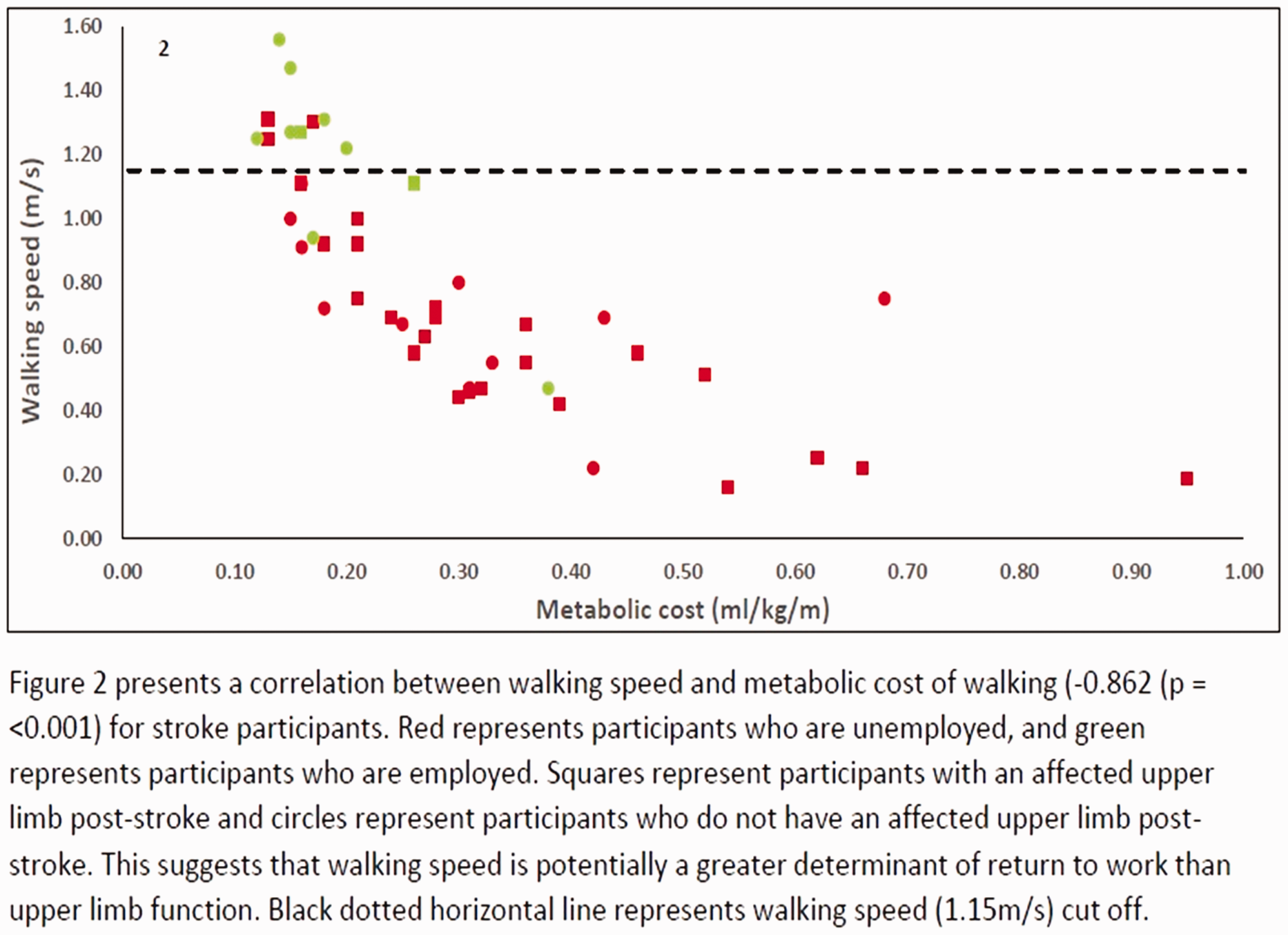
Stroke participants walked slower and had a higher energy cost of walking than control (Figure 1a and 1b). 96% were in full-time employment pre-stroke, but only 22% returned to employment post-stroke. Those who returned to employment post-stroke walked significantly faster, with lower energy cost and with greater walking symmetry than those who did not return to employment (Figure 2).
Conclusions
Young adults who have had a stroke and are unable to walk faster than ∼1.15m/s post stroke are unlikely to return to work post-stroke. It is recommended that walking speed is used as an indicator of performance post stroke. Rehabilitation for return to work should be aimed at increasing walking speed and reducing energy cost.
Trial registration number
N/A
AS08-054
PREDICTION OF PHYSICAL ACTIVITY LEVEL AFTER MILD STROKE: A 6-MONTH FOLLOW-UP OF 215 PATIENTS IN THE FALL STUDY OF GOTHENBURG (FALLSGOT)
1Institute of Neuroscience and Physiology, Department of Clinical Neuroscience- Rehabilitation Medicine- Sahlgrenska Academy- University of Gothenburg, Gothenburg, Sweden
2Institute of Medicine, Department of Molecular and Clinical Medicine- Sahlgrenska Academy- University of Gothenburg, Gothenburg, Sweden
Background and Aims
Physical activity after stroke is inadequately studied. The aim was to identify factors in acute stroke that are associated with low physical activity level six months after onset in mild stroke.
Methods
In this substudy of The Fall Study of Gothenburg, physical activity level was assessed using the Saltin Grimby Physical Activity Scale (SGPALS) in 215 patients with mild stroke. Mild stroke was defined as a National Institutes of Health Stroke Scale (NHISS) score of 4 or less. Associations between characteristics prior and during the acute phase after a stroke and low physical activity level (defined as a SGPALS score of 1) six months after mild stroke were identified using univariable and multivariable logistic regression analyzes.
Results
At six months after stroke, low physical activity level was reported by 81 individuals (37.7%). In the multivariable analysis, stroke severity (NIHSS) odds ratio (OR) 1.32 (95% confidence interval (CI) 1.02–1.71) p 0.029, physical inactivity prior stroke onset OR 4.13 (95% CI 2.06–8.30) p < 0.0001, fear of falling OR 2.53 (95% CI 1.23–5.20) p 0.012 and impaired ability in tandem standing acute after stroke OR 4.87 (95% CI 1.22–17.91) p 0.017 were associated with low physical activity level six months after onset in mild stroke.
Conclusions
Almost four out of ten individuals with mild stroke are sedentary first half after stroke onset. Of the determinants of low physical activity, particularly physical activity level prior the stroke, but also poor postural control and fear of falling acute after stroke, seem to be modifiable.
Trial registration number
N/A
AS08-028
SEMI-AUTOMATIC ANALYSIS OF SPONTANEOUS SPEECH IN HISTORY INTAKE FROM APHASIA-RELATED STROKE PATIENTS TO RANK AND CATEGORIZE FAST SYMPTOMS
1Aristotle University of Thessaloniki, Department of Informatics, Thessaloniki, Greece
2University of Macedonia, Department of Educational and Social Policy, Thessaloniki, Greece
Background and Aims
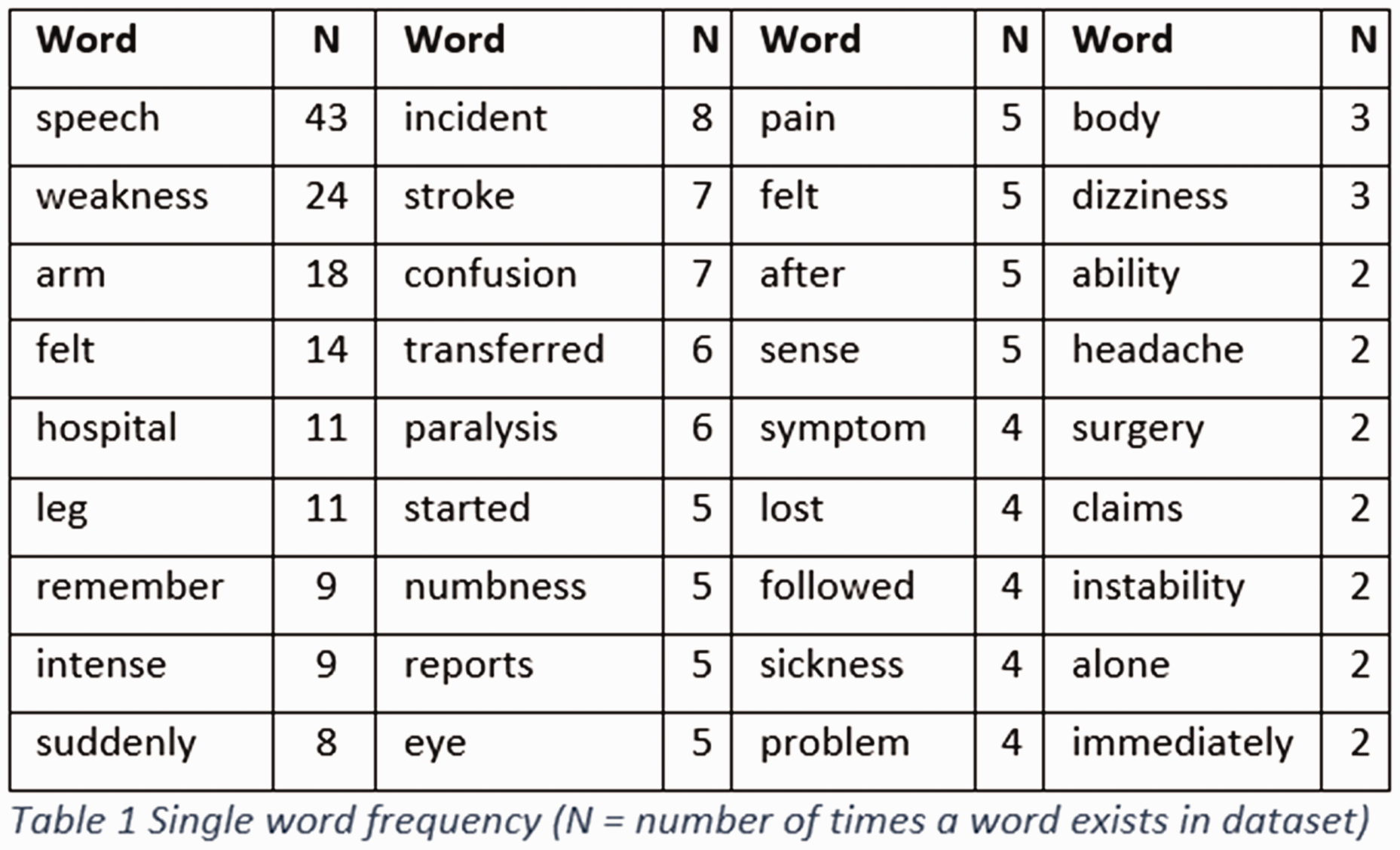
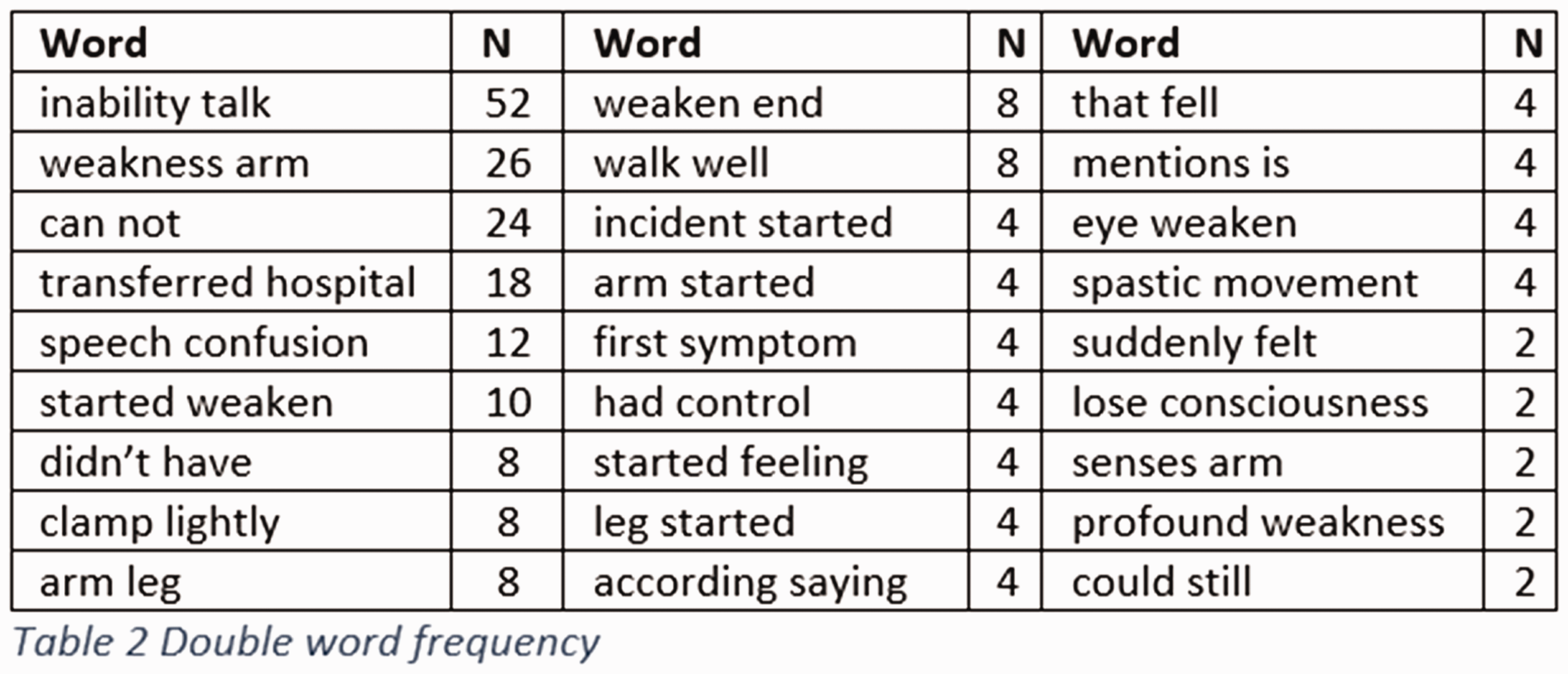
Spontaneous speech analysis from aphasia-related stroke patients during a history intake is often compromised due to either syntactic, morphological or semantic difficulties. Statistics and machine learning techniques were used to analyze spontaneous responses to the question “why are you here today?” from patients with stroke-related aphasia. We aim to rank and categorize Face, Arm, Speech, Time (FAST) symptoms.
Methods
We use a dataset consisting of 58 participants, 68.96% male and 31.04% female, aged between 26 and 78 with mean 58.29 and median 61, the majority having suffered an ischemic stroke. All participants have responded orally, and audio recordings had been transcribed for subsequent analysis of the text. We used two standard natural language processing techniques, namely term frequency (tf) which shows the number of times a word occurs in a document and latent Dirichlet allocation (LDA) which distinguishes topics within documents.
Results
Regarding tf, we rank single and double- word sequences (Tables 1–2) and we observe that “speech” and “arm” appear frequently, while words related to face, or other conditions also exist. Regarding LDA, we selected 3 topics which are clearly distinguished from each other and we observe that “speech” and “arm” (Figure 1) are categorized in two of them, while the third one is vaguer as it contains words related to the general condition of the patients.

Conclusions
Overall, we aim to use this work as a proof of concept that Artificial Intelligence techniques such as machine learning can be efficient in analyzing, categorizing and comprehending text of aphasic patients.
Trial registration number
N/A
AS04-061
A PROSPECTIVE, RANDOMISED, DOUBLE-BLIND STUDY EFFECT OF LEVODOPA IN COMBINATION WITH PHYSIOTHERAPY ON FUNCTIONAL MOTOR RECOVERY AFTER STROKE
1Tashkent Medical Academy, Neurology, Tashkent, Uzbekistan
Background and Aims
Functional disability is generally caused by hemiplegia after stroke. Physiotherapy used to be the only way of improving motor function in such patients. However, administration of amphetamines in addition to exercise improves motor recovery in animals, probably by increasing the concentration of norepinephrine in the central nervous system. Our aim was to ascertain whether levodopa could enhance the efficacy of physiotherapy after hemiplegia.
Methods
We did a prospective, randomised, placebo-controlled, double-blind study in which we enrolled 49 primary stroke patients. For the first 3 weeks patients received single doses of levodopa 100 mg or placebo daily in combination with physiotherapy. For the second 3 weeks patients had only physiotherapy. We quantitatively assessed motor function every week with Rivermead motor assessment (RMA).
Results
FINDINGS:Six patients were excluded from analyses because of non-neurological complications. Motor recovery was significantly improved after 3 weeks of drug intervention in those on levodopa (RMA improved by 6.4 points) compared with placebo (4.1), and the result was independent of initial degree of impairment (p < 0.004). The advantage of the levodopa group was maintained at study endpoint 3 weeks after levodopa was stopped. At the end of the study the total RMA score gain for the levodopa group was 8.2 points compared with 5.7 in the placebo group (p = 0.020).
Conclusions
A single dose of levodopa is well tolerated and, when given in combination with physiotherapy, enhances motor recovery in patients with hemiplegia. In view of its minimal side-effects, levodopa will be a possible add- on during stroke rehabilitation.
Trial registration number
N/A
WITHDRAWN
E-Poster Discussion-Acute Management I
AS06-110
PRACTICE PATTERNS AND OUTCOMES OF ENDOVASCULAR THERAPY IN MILD STROKE: A FLORIDA-PUERTO RICO COLLABORATION
1University of Miami, Miller School of medicine, Miami, USA
2Delray Medical Center, Neurology, Delray, USA
3Emory University/Grady Memorial Hospital, Neurology, Atlanta, USA
4Baptist Med Ctr, Neurosurgery, Jacksonville, USA
5HIMA San Pablo Hosp-, Neurology, Caguas, Puerto Rico
6Florida Intl University, Neurology, Miami, USA
Background and Aims
To evaluate the current practice patterns, safety and outcomes of patients who receive endovascular therapy (EVT) and have mild neurological symptoms.
Methods
From Jan 2010 to Jan 2018, 127,794 ischemic stroke patients were enrolled in the Florida-Puerto Rico Registry. Patients presenting within 24 hours of symptoms who received EVT were classified into mild (NIHSS ≤ 5) or moderate/severe categories. Differences in clinical characteristics and outcomes were evaluated using multivariable logistic regression.
Results
Among 3,786 EVT patients, median age 73 (IQR = 20), 50% women, 446 (12%) had NIHSS≤5. Compared to NIHSS>5, mild patients arrived later to the hospital (median 138 vs. 101 min), were less likely to receive IV tPA (30% vs. 43%), had a longer door to puncture time (median 167 vs. 115 min) and more likely treated in South Florida (64% vs. 53%). In multivariable analysis younger age, private insurance (vs. Medicare), history of Hypertension, prior independent ambulation and hospital size were independently associated with NIHSS ≤5. Amongst EVT patients with NIHSS≤5, 76% were discharged home/rehabilitation and 64% were able to ambulate independently at discharge as compared to 53% and 32% of patients with NIHSS>5. Symptomatic ICH occurred in 4% of mild EVT patients and 6.4% in those with NIHSS>5.
Conclusions
Despite lack of evidence-based recommendations, 12% of patients receiving EVT in clinical practice have mild neurological presentations. Individual, hospital and geographical disparities are observed amongst EVT patients based on the severity of clinical symptoms. Our data suggest safety and overall favorable outcomes for EVT patients with mild stroke.
Trial registration number
N/A
AS06-028
ACUTE ISCHEMIC STROKE, ATRIAL FIBRILLATION AND EARLY DOAC-TREATMENT: 30-DAY RISK OF RECURRENT ISCHEMIC STROKE, INTRACRANIAL HAEMORRHAGE IN A MULTI-CENTRE INDIVIDUAL PATIENT DATA META-ANALYSIS
1University Hospital Basel & University of Basel, Neurology & Stroke Center, Basel, Switzerland
2University Hospital Basel & University of Basel, Clinical Trial Unit, Basel, Switzerland
3UCL, Institute of Neurology, London, United Kingdom
4University of Perugia, Stroke Unit and Division of Cardiovascular Medicine, Perugia, Italy
5National & Kapodistrian University of Athens School of Medicine, Second Department of Neurology, Athens, Greece
6National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Osaka, Japan
7Azienda Ospedaliera Universitaria Integrata Verona, Department of Neuroscience, Verona, Italy
8University of Erlangen-Nuremberg, Department of Neurology, Erlangen, Germany
9Neurocentro della Svizzera Italiana, Neurologia, Lugano, Switzerland
10Santa Maria della Misericordia Hospital- University of Perugia, Stroke Unit, Perugia, Italy
11University Hospital Basel & University of Basel & Felix Platter Hospital, Neurology & Stroke Center, Basel, Switzerland
Background and Aims
We aimed to investigate recurrent ischaemic stroke (IS) and symptomatic intracranial haemorrhage (ICH) early after a recent cerebral ischaemia in patients with atrial fibrillation (AF) and their time course in relation to the initiation of direct oral anticoagulants (DOACs).
Methods
International, individual patient data meta-analysis from 8 cohort studies. We included patients with acute IS or TIA, non-valvular AF, and a DOAC within 30 days. We excluded patients with symptomatic intracranial haemorrhage (ICH) within 24 hours of endovascular recanalization therapy (n = 2), or not started on a DOAC within 30 days. The endpoints were recurrent IS (re-IS) and ICH within 30 days.
Results
We included 2555 patients (median age: 77 years, IQR 70–84), of which 2460 had IS (96.5%). The median NIHSS was 5 (IQR 2–10). DOAC were started after a median of 5 days (IQR 2–10). Re-IS occurred, after a median of 6 days (IQR 2–15), in 37 patients (1.4%); 16 of these re-IS (43%) occurred prior to DOAC-start. ICH occurred, after a median of 10 days (IQR 7.5–14), in 11 patients (0.4%); 6 of these ICH (55%) occurred after DOAC-start.
Conclusions
Among patients with acute IS and AF, nearly half of the re-IS occurred prior to DOAC-start, i.e. were potentially preventable. The number of ICH potentially attributable to early start of DOAC was very low. Ongoing randomized clinical trials will show whether an earlier DOAC-start can further reduce the risk of re-IS while keeping the risk of ICH low.
Trial registration number
N/A
AS06-049
SAFETY AND EFFICACY OF MECHANICAL THROMBECTOMY AND R-TPA VERSUS PRIMARY THROMBECTOMY IN THE TREATMENT OF ISCHEMIC STROKE: RESULTS OF THE ANDALUSIAN REGISTRY
1Hospital Universitario Virgen Macarena. Neurovascular research laboratory Intituto Biomedicina de Sevilla., Neurology, Sevilla, Spain
2Hospital Universitario Virgen del Rocío. Neurovascular research laboratory Intituto Biomedicina de Sevilla., Interventional Neuroradiology, Sevilla, Spain
3Instituto de Biomedicina de Sevilla, Neurovascular research laboratory, Sevilla, Spain
4Hospital Universitario Virgen del Rocío. Neurovascular research laboratory Intituto Biomedicina de Sevilla., Neurology, Sevilla, Spain
5Área de Gestión Sanitaria Sur de Sevilla- Hospital de Valme., Unidad de Gestión Clínica de Salud Pública- Prevención y Promoción de la Salud-, Sevilla, Spain
6Hospital Universitario Juan Ramón Jiménez, Neurology, Huelva, Spain
7Hospital Universitario Virgen Macarena. Neurovascular research laboratory Intituto Biomedicina de Sevilla, Neurology, Sevilla, Spain
8Hospital Universitario Virgen del Rocio. Neurovascular research laboratory Intituto Biomedicina de Sevilla, Interventional Neuroradiology, Sevilla, Spain
Background and Aims
Currently, treatment of acute ischemic stroke combines the administration of r-TPa with mechanical thrombectomy but there are situations in which the administration of r-TPa is contraindicated and primary thrombectomy (PT) can be performed. We compared safety and efficacy of these two treatment modalities in our region.
Methods
Prospective study including patients treated with mechanical thrombectomy in a comprehensive stroke center in Andalucía between August 2016 and December 2018. Baseline characteristics, safety (complications) and efficacy data (NIHSS, 90-day mRS, TICI) between those previously treated with rTPa and those undergoing PT are compared.
Results
527 patients, 43% treated with r-TPa and thrombectomy, 57% with PT. PT patients were older (71.4 vs 68.5 years, p = 0.01), with higher baseline mRS (75th percentile 1 vs 0, p = 0.04), more arterial hypertension (77.3% vs 66.2%, p = 0.005), previous stroke/TIA (22.4% vs 10.8%, p = 0.001) and cardioembolic etiology (55.6% vs 41.4%, p = 0.003). Median NIHSS pre-procedure 16 in both groups. Regarding safety, both hemorrhagic and procedure-related complications, were similar in both groups and also recanalization rates TICI 2B-3, 91.5% in r-TPa group vs. 89.4% in PT (n.s.). Start-to-door time was shorter in r-TPa patients (109 vs 264 min, p < 0.001). r-TPA patients needed less passes for recanalization (1.9 vs 2.5, p = 0.001). 90-day mRS was better in the r-TPa group (mRS 0–2; 62.0% vs 54.1%, p = 0.05).
Conclusions
In our sample, we found no differences in safety in patients treated with r-TPa and thrombectomy versus those treated with thrombectomy alone. Patients treated with r-TPa arrive earlier at the hospital and have better functional outcome.
Trial registration number
N/A
AS06-044
INFARCT IN NEW TERRITORY AFTER ENDOVASCULAR STROKE TREATMENT: A DIFFUSION-WEIGHTED IMAGING STUDY
1Inselspital- University of Bern, Neuroradiology, Bern, Switzerland
2Inselspital- University of Bern, Neurology, Bern, Switzerland
3Inselspital- University of Bern, Radiology & Neuroradiology, Bern, Switzerland
4Inselspital- University of Bern, Supportive Center of Advanved Neuroimaging, Bern, Switzerland
5University of Calgary- Calgary- Alberta- Canada., Diagnostic Imaging, Calgary, Canada
Background and Aims
To assess the prevalence and associated factors of infarcts in new territory (INT) in patients undergoing endovascular stroke treatment for an acute large-vessel occlusion.
Methods
All patients of a single center prospective registry who underwent endovascular stroke treatment and received pre- and post-interventional diffusion weighted imaging were included (N = 259). Using an established scoring system, INT were classified according to size (I-III, ≤2mm, >2mm-≤20mm, >20mm) and likelihood of being related to the intervention (A, high likelihood; B, low likelihood). Additionally, a new type of infarct was defined, occurring in a territory distal to the occlusion but in a territory without initial hypoperfusion (IINHT).
Results
A total of 180 INTs and 38 INHTs were observed in 32.8% (N = 85/259) of patients. In most patients, INTs were angiographically occult (90.2%), and 12 patients had INT/IINHTs greater than 2cm (type III). No protection during stent-retrieval showed a trend towards higher incidence of INTs/INHTs, while pretreatment with IV tPA showed no association, also when considering bolus timing. INT/IINHTs were clinically relevant with respect to their size and were associated with lower rates of functional independence after adjusting for confounders (adjusted Odds Ratio per size group increase 0.64, 95% confidence interval 0.47–0.87).
Conclusions
INTs and IINHT are not rare, often angiographically occult, and may serve as a surrogate endpoint for safety evaluation of new devices and endovascular techniques. Treatment with IV tPA before or during the intervention does not seem to affect the occurrence of INTs or IINHTs, and further research on associated factors is warranted.
Trial registration number
N/A
AS06-038
PRIOR ANTIPLATELET USE IN PATIENTS UNDERGOING ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE: RESULTS FROM THE MR CLEAN REGISTRY
1Erasmus MC, Radiology & Nuclear Medicine, Rotterdam, The Netherlands
2Erasmus MC, Neurology, Rotterdam, The Netherlands
3Onze Lieve Vrouwe Gasthuis, Neurology, Amsterdam, The Netherlands
4Erasmus MC, Public Health, Rotterdam, The Netherlands
5Cardiovascular Research Institute Maastricht- Maastricht University Medical Center, Neurology, Maastricht, The Netherlands
6Amsterdam UMC- location AMC, Radiology & Nuclear Medicine, Amsterdam, The Netherlands
7Amsterdam UMC- location AMC, Neurology, Amsterdam, The Netherlands
Background and Aims
Antiplatelet agents may improve functional outcome after endovascular treatment (EVT) for ischemic stroke, despite the potentially increased risk of symptomatic intracranial hemorrhage (sICH). A large proportion of patients are on antiplatelets prior to occurrence of stroke, which risks and benefits have not been addressed in large cohorts. We aimed to compare outcomes of patients undergoing EVT in patients with and without prior antiplatelet use.
Methods
We analyzed patients registered in the MR CLEAN Registry between March 2014 and June 2016, for whom data on antiplatelet use was available. We used multivariable regression analyses to compare prior to no prior antiplatelet use, adjusted for baseline prognostic factors. Primary outcome was symptomatic intracranial hemorrhage (sICH). Secondary outcomes were 90-day functional outcome (modified Rankin Scale), successful recanalization (extended-thrombolysis-in-cerebral-infarction ≥ 2B) and 90-day mortality.
Results
1469 Patients were analyzed, of which 493 (34%) patients were on prior antiplatelets. The risk of sICH was increased for patients on prior antiplatelets (9% vs. 4%; adjusted odds ratio (aOR) 2.05, 95%confidence interval (CI) 1.17–3.58). No significant associations were found between prior antiplatelet use and functional outcome (adjusted common OR 0.89, 95%CI 0.68–1.17), successful recanalization (aOR 0.96, 95%CI 0.71–1.29), or mortality (aOR 1.21, 95%CI 0.82–1.77).
Conclusions
Although prior antiplatelet use seems to increase the risk of sICH after EVT, no effect on functional outcome, recanalization or mortality was observed. However, these results might be hampered by residual confounding.
Trial registration number
N/A
E-Poster Discussion-Embolic Stroke
AS25-018
EFFECTIVENESS AND SAFETY OF RIVAROXABAN VERSUS WARFARIN IN NONVALVULAR ATRIAL FIBRILLATION PATIENTS WITH SEVERE KIDNEY DISEASE OR UNDERGOING HEMODIALYSIS
1University of Connecticut School of Pharmacy, Pharmacy Practice, Storrs, USA
2Charité – Universitätsmedizin Berlin, Pharmacology and Toxicology, Berlin, Germany
3New England Health Analytics LLC, Pharmacoepidemiology, Granby, USA
4Southcoast Health, Cardiac Arrhythmia Services, Fall River, USA
5Bayer AG, Real-World Evidence Generation, Berlin, Germany
Background and Aims
Nonvalvular atrial fibrillation (NVAF) patients with stage 4 or 5 chronic kidney disease (CKD) or undergoing hemodialysis were excluded from trials of non-vitamin K antagonist oral anticoagulants (OACs). We sought to evaluate the effectiveness and safety of rivaroxaban versus warfarin in NVAF patients with stage 4 or 5 CKD or undergoing hemodialysis.
Methods
Using MarketScan data from 1/2012-12/2017, we identified OAC-naïve NVAF patients with ≥1 claim for stage 4 or 5 CKD or hemodialysis and ≥12-months of insurance coverage before OAC initiation. Differences in baseline covariates between cohorts were adjusted using inverse probability-of-treatment weights based on propensity-scores (standardized differences <0.1 achieved for all covariates after adjustment). Patients were followed until a thrombotic or major bleeding event, OAC discontinuation/switch, insurance disenrollment or end-of-data availability. Hazard ratios (HRs) and 95% confidence intervals (CIs) comparing the cohorts were calculated using Cox regression.
Results
We identified 1896 rivaroxaban and 4848 warfarin users. Median (25-75% range) age = 72 (63-80), CHA2DS2-VASc = 4 (2-5) and duration of available follow-up = 1.4 (0.6–2.7) years and 88% of patients had stage 5 CKD and/or were undergoing hemodialysis. Rivaroxaban did not significantly reduce stroke/systemic embolism or ischemic stroke, but was associated with a 32% reduction in major bleeding risk versus warfarin (Figure).

Conclusions
In NVAF patients with CKD stages 4, 5 or on dialysis, rivaroxaban appears associated with less major bleeding.
Trial registration number
N/A
AS21-022
SYMPTOMATIC CAROTID NEAR-OCCLUSION CAUSES A HIGH RISK OF RECURRENT IPSILATERAL ISCHEMIC STROKE
1Department of Pharmacology and Clinical Neuroscience, Department of Neurology- Norrland University Hospital, Umea, Sweden
2Department of Medical Imaging, Department of Medical Imaging- Sunnybrook Health Science Center, Toronto, Canada
Background and Aims
Carotid near-occlusion (CNO) is a severe carotid stenosis causing distal artery size collapse. Large clinical trials suggested a low risk of recurrent ipsilateral ischemic stroke (RIIS) for symptomatic CNO. These trials often included patients after several weeks delay since last event and included mostly CNO with partial distal collapse, few with full collapse. The short-term risk of RIIS has been suggested to be high for CNO with full collapse. The aim of this study was to compare the risk of RIIS in patients with symptomatic conventional ≥50% stenosis, CNO with partial and full collapse.
Methods
We retrospectively re-examined 4403 consecutive computed tomography angiographies. We included patients with symptomatic ≥50% carotid stenosis eligible for carotid endarterectomy. We compared the risk of preoperative RIIS within 90 days after the presenting event between conventional ≥50% stenosis (n = 266), CNO with partial collapse (n = 55) and CNO with full collapse (n = 31).
Results
The risk of RIIS was 14.9% (95%CI 9.2–24.1%) for ≥50% conventional carotid stenosis, 24.0% (95% CI 6.0–30.0%) for CNO with partial collapse and 25.3% (95%CI 8.4–33.7%) for CNO with full collapse (p = 0.15, log-rank test). Mean age was lower for CNO (69 years) than conventional ≥50% stenosis (73 years, p = 0.001). Adjusting for age and other confounders, the risk of RIIS was significantly higher for CNO than ≥50% conventional carotid stenosis (adjusted HR 2.0; 95%CI 1.1–3.9, p = 0.03).
Conclusions
Symptomatic CNO causes a high short-term risk of RIIS with no apparent difference between partial and full collapse. A randomized controlled trial is warranted
Trial registration number
N/A
AS25-042
SETTING UP AN AF-STROKE PREVENTION SERVICE IN SECONDARY CARE: THE SCREENING AND OPTIMISING STROKE PREVENTION IN ATRIAL FIBRILLATION (SOS-AF) SERVICE
1Cambridge University Hospitals NHS Foundation Trust, Stroke, Cambridge, United Kingdom
2Eastern Academic Health Sciences Network, Eahsn, Cambridge, United Kingdom
Background and Aims
Our work in 2015 showed the burden of AF in acute medical admissions is 15%, a stark contrast to previous literature estimates of 3–6%. Medical inpatients are older with multiple comorbidities and a high stroke-risk (median CHA2DS2VASc score = 4.4). 50% of AF patients weren’t on anticoagulation on admission and only 38% of newly-diagnosed AF were discharged anticoagulated.
Methods
SOS-AF was set up as a secondary-care stroke prevention service at Cambridge University Hospital, UK in October 2017. It provides in-hospital AF screening of all medical admissions, by 2 specialist nurses and 4 stroke clinicians using electronic notes and 12-lead ECG.
Every AF patient not on anticoagulation is holistically risk-stratified. Patients/families are involved and educated, and anticoagulation is started where appropriate. We accept referrals from inpatient teams and primary care to our clinic and multidisciplinary meeting.
Results
In our first year we screened 14979 patients, identifying 393 new AF cases. The AF prevalence was 22.1% in medical admissions. We advised not to anticoagulate 158 patients, where the risks outweighed the benefits. Clinicians followed our advice 82% of the time and 402 patients were appropriately anticoagulated. We have increased local anticoagulation rates by 15% and prevented an estimated 16 cardioembolic strokes and 8 deaths, saving £94,600/year on bed-days and the NHS £352,000/year.
Conclusions
Secondary-care must play an active role in stroke prevention in AF. By cost-effective screening in a high-risk population and providing specialist advice to primary and secondary care, SOS-AF delivers individualised patient care and significant financial savings to the health economy.
Trial registration number
N/A
AS21-033
DEVELOPMENT OF A BASIC RISK SCORE FOR NEW PROGRESSION OF CAROTID PLAQUE: THE SUITA STUDY
1National Cerebral and Cardiovascular Center, Preventive Cardiology, Suita, Japan
2National Cerebral and Cardiovascular Center, Preventive Medicine and Epidemiologic Informatics, Suita, Japan
Background and Aims
We first showed that the new progression of carotid plaque (Prog-PQ) is a risk factor for cardiovascular disease (CVD), but the Prog-PQ risk score has not been established.
Methods
We studied 4,724 Japanese (mean age 59.7 years) without CVD whose intima-media thickness (IMT) was measured with carotid ultrasonography on both sides of the entire carotid artery areas (April 1994 to August 2001). Carotid plaque was defined as a maximum IMT of the common carotid artery >1.1mm. We excluded subjects with carotid plaque at baseline (n = 1,044), lost to follow-up (n = 167), and missing data (n = 2). For 3,511 subjects carotid ultrasonographic follow-ups were performed every two years until March 2016. Cox proportional hazard ratios were analyzed after adjusting for cardiovascular risk factors. We used the area under the receiver operating characteristic curve to evaluate the model’s discrimination.
Results
During 38,454 person-years of follow-up, 1,771 instances of Prog-PQ occurred. We developed a scoring system for each risk factor as follows: 0/2/4/6/9/11 points for age 30’s to 80’s, respectively; -1 point for women; 0/1/2 points for systolic blood pressure (<120/120-159/≥160mmHg); 0/1/2/3 points for total cholesterol (<160/160-239/240-279/≥280mg/dL); 2/0/-1 points for HDL cholesterol (<35/35-59/≥60mg/dL); 1 point for overweight or current smoking; and 2 points for diabetes (C-statistic 0.647; 95%CI, 0.629–0.665). Individuals with 2 or 10 points had 27% or 62% observed probability of Prog-PQ in 10 years, respectively.
Conclusions
We have developed a 10-year risk score for Prog-PQ, that can easily predict atherosclerosis in routine clinic/health examinations without carotid ultrasonography.
Trial registration number
n/a
AS21-030
BASELINE COGNITIVE FUNCTION AMONG 1,000 PARTICIPANTS IN THE CAROTID REVASCULARIZATION AND MEDICAL MANAGEMENT FOR ASYMPTOMATIC CAROTID STENOSIS TRIAL (CREST-2)
1The University of Alabama at Birmingham, Department of Neurology, Birmingham, USA
2Columbia University Medical Center, Neurology, New York, USA
3The University of Alabama at Birmingham, Department of Biostatistics, Birmingham, USA
4The University of Alabama at Birmingham, School of Public Health, Birmingham, USA
5Medical University of South Carolina, Neurology, Charleston, USA
6Unversity of Maryland, Vascular Surgery, Baltimore, USA
7Mayo Clinic, Department of Neurology, Jacksonville, USA
Background and Aims
We wanted to determine baseline cognition via telephone assessment among individuals in CREST-2 (clinicaltrials.gov NCT02089217), which enrolls cognitively competent individuals with asymptomatic carotid artery occlusive disease or remotely symptomatic atherosclerotic stenosis. Participants undergo baseline cognitive assessment before revascularization or starting medical management alone, and at periodic follow-up. To minimize assessment variability of cognition across >120 CREST-2 centers, we employ centrally-administered telephone assessments, based on the population-based REGARDS cohort study.
Methods
Data came from the first 1,000 patients . We used the REGARDS protocol of CERAD Word List Learning (WL-L) and Delayed Recall (WL-Delay), and Word Fluency for the letter “F” and Animal Names. Using the general population norms from REGARD (N>23,000), we calculated Z-scores for each CREST-2 test, based on the mean score for age-sex-education matched REGARDS participants.
Results
The mean age was 69 yrs, 59%M, and 47% left-sided stenosis. Among our tests, the burden of impairment was found in WL-L (p < 0.0001) and WL-Delay (p < 0.0001), with relatively little impact on Word Fluency measures. For WL-Delay, the 50th and 25th percentiles in CREST-2 were at the 25th and 8th percentiles in REGARDS, respectively.
Conclusions
Patients with high-grade asymptomatic carotid stenosis had significantly lower baseline learning and memory scores than the general population. These data justify the use of a telephone-based test battery for testing cognitive change in CREST-2 and relevance for testing reversibility in the CREST-H (hemodynamics) subset with cerebral hypoperfusion.
Trial registration number
NS080168
E-Poster Discussion-Reperfusion Treatment II
AS05-015
SAFETY AND OUTCOME OF INTRAVENOUS THROMBOLYSIS IN ACUTE ISCHAEMIC STROKE PATIENTS ON PROPHYLACTIC DOSES OF LOW-MOLECULAR-WEIGHT HEPARINS
1Department of Clinical Neurosciences, Department of Neurology, Stockholm, Sweden
2International Clinical Research Center, Neurology Department- St. Anne’s University Hospital in Brno and Masaryk University, Brno, Czech Republic
3Neurocentre- Regional Hospital Liberec, Neurocentre- Regional Hospital Liberec, Liberec, Czech Republic
4Faculty Hospital Nitra- Constantine Philosopher University, Faculty Hospital Nitra- Constantine Philosopher University, Nitra, Slovak Republic
5Department of Neurology- Heidelberg University Hospital, Department of Neurology- Heidelberg University Hospital, Heidelberg, Germany
6University of Newcastle upon Tyne and Newcastle upon Tyne Hospitals NHS Foundation Trust, University of Newcastle upon Tyne and Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle, United Kingdom
7Emergency Department Stroke Unit- Hospital Policlinico Umberto I, Department of Neurology and Psychiatry- Sapienza University, Rome, Italy
Background and Aims
There are limited data on intravenous thrombolysis (IVT) treatment in ischemic stroke patients who have received prophylactic doses of low-molecular-weight heparins (LMWH). We aimed to evaluate safety and outcomes of IVT treatment in stroke patients taking thromboprophylactic doses of LMWH.
Methods
We analyzed 109291patients treated with IVT, recorded in the SITS International Thrombolysis Register between 2003 and 2017, not taking oral anticoagulants or therapeutic doses of heparin at stroke onset. 1411 patients (1.3%) were on prophylactic LMWH for deep venous thrombosis prevention. Outcome measures were symptomatic intracerebral haemorrhage (SICH), parenchymal hematoma, death within 7 days and 3 months, and functional dependency at 3 months.
Results
Patients on LMWH were older, had more severe strokes, more pre-stroke disability and comorbidities than patients without LMWH. There was no significant increase in adjusted odds ratios (aOR) for SICH (aOR 1.02 [95% CI 0.48–2.17] as per SITS-MOST, aOR 0.95 [0.59–1.53]per ECASS II]), nor for 7-day mortality (aOR 1.14, [0.82–1.59]), in the prophylactic LMWH group. The LMWH group had a higher aOR for 3-month mortality (aOR 1.94 [1.49–2.53]) and functional dependency, aOR 1.44 (1.10–1.90). Propensity score analysis matching patients on baseline characteristics removed differences between groups on all outcomes except 3-month mortality.
Conclusions
IVT in acute ischemic stroke patients on treatment with prophylactic doses of LMWH at stroke-onset is not associated with an increased risk of SICH or early death.
Trial registration number
N/A
AS05-018
SAFETY AND OUTCOMES OF IV THROMBOLYSIS IN POSTERIOR VERSUS ANTERIOR CIRCULATION ACUTE ISCHEMIC STROKE. RESULTS FROM THE SITS INTERNATIONAL STROKE THROMBOLYSIS REGISTER (SITS-ISTR) AND META-ANALYSIS
1Karolinska University Hospital, Department of Neurology, Stockholm, Sweden
2Karolinska Institute, Department of Clinical Neuroscience, Stockholm, Sweden
3Pavol Jozef Šafárik University, Department of Neurology, Košice, Slovak Republic
4Vilnius University, Institute of Clinical Medicine, Vilnius, Lithuania
5Vilnius University Hospital Santaros Klinikos, Centre of Neurology, Vilnius, Lithuania
6Santa Maria Hospital, Department of Neurology, Lisbon, Portugal
7Vilnius University, Faculty of Medicine, Vilnius, Lithuania
8Ospedale San Giovanni Bosco, Neurology and Stroke Unit, Torino, Italy
9University Medical Center Ljubljana, Department of Vascular Neurology and Neurological Intensive Care, Ljubljana, Slovenia
10Regional Hospital Liberec, Neurocentre, Liberec, Czech Republic
11Memorial Hizmet Hospital, Acute Stroke Center, Istanbul, Turkey
12Centro Hospitalar Lisboa Central, Stroke Unit, Lisbon, Portugal
13AO Cosenza, Department of Neurology, Cosenza, Italy
14University of Glasgow, School of Medicine- Dentistry and Nursing, Glasgow, United Kingdom
Background and Aims
Posterior circulation stroke (PCS) accounts for 8–12% of acute stroke patients receiving intravenous thrombolysis (IVT). We aimed to compare safety and outcomes following IVT between patients with PCS and anterior circulation stroke (ACS), and incorporate the results in a meta-analysis.
Methods
We included patients in the SITS Thrombolysis Registry 2013–2017 with CT/MR angiographic occlusion data. Outcomes were parenchymal hematoma (PH), symptomatic ICH (SICH) per SITS-MOST, ECASS-II and NINDS, 3-month modified Rankin Scale score, and death. Matching for SICH risk factors (age, sex, NIHSS, blood pressure, glucose, atrial fibrillation) was done using inverse probability weighting. Meta-analysis of studies comparing outcomes in PCS vs ACS after IVT was conducted.
Results
Of 5146 patients, 753 had PCS (14.6%). PCS patients had lower median NIHSS: 7 (IQR 4–13) vs 13 (7-18), p < 0.001, and less frequent cerebrovascular risk factors. PH occurred in 3.2% PCS patients versus 7.9% in ACS. After matching, bleeding complications and mortality were lower in PCS vs ACS (95% CI for group difference): PH 3.1% vs 7.7% (3.0%-6.3%); SICH SITS-MOST 0.5% vs 1.9% (2.4%-0.8%); 3-month death (69% data availability) 12.8% vs 19.3% (1.1%-12.1%). Differences in rates of SICH NINDS, SICH ECASS-II and 3-month mRS 0–2 were non-significant. Meta-analysis including 13 studies showed relative risk for SICH in PCS versus ACS being 0.49, (95% CI 0.32–0.75).

Conclusions
Posterior circulation stroke carries approximately half the risk of bleeding complications after IVT compared to ACS and has similar functional outcomes, acknowledging limitations of the NIHSS for stroke severity or infarct size adjustment.
Trial registration number
N/A
AS05-013
OUTCOME OF ENDOVASCULAR THERAPY IN STROKE PATIENTS WITH LARGE VESSEL OCCLUSION AND MILD SYMPTOMS
1Stroke Center- Department of Neurology, Neurocenter EOC of Southern Switzerland, Lugano, Switzerland
2Lausanne University Hospital and University of Lausanne, Department of Neurology, Lausanne, Switzerland
3University Hospital Bern and University of Bern- Inselspital, Department of Neurology, Bern, Switzerland
4University Hospital Bern and University of Bern- Inselspital, Department of Neuroradiology, Bern, Switzerland
5University Hospital of Basel, Department of Neurology and Stroke Center, Basel, Switzerland
6Hôpitaux Universitaires de Genève, Stroke Center- Service de Neurologie, Geneva, Switzerland
7Cantonal Hospital Aarau, Department of Neurology, Aarau, Switzerland
8Cantonal Hospital, Department of Neurology, St. Gallen, Switzerland
Background and Aims
Endovascular therapy (EVT) is the most effective method to obtain recanalization and functional independence in acute ischemic stroke (AIS) patients with an emergent large vessel occlusion (ELVO) and NIHSS ≥ 6.
We compared outcomes after EVT and intravenous thrombolysis (IVT) in stroke patients with ELVO and mild neurological deficits.
Methods
We retrospectively compared AIS patients from the Swiss Stroke Registry with ELVO and NIHSS ≤5 treated by EVT (+/- IVT) versus IVT alone, matched by propensity scores.
Primary endpoint was favourable functional outcome (modified Rankin Scale [mRS] 0–1) at 3 months.
Secondary outcomes were mRS (shift analysis) and survival with high disability (mRS 4–5). Safety endpoints were mortality and symptomatic haemorrhage (sICH).
Results
Out of 11.356 patients, 339 met the inclusion criteria, and 126 were matched per group. A comparably large proportion of EVT and IVT patients had favourable outcome (56% and 67% respectively; OR = 0.65, 95% CI 0.36–1.17, p = 0.15).
EVT patients had slightly higher mRS score at 3 months (p = 0.04), while the proportion of patients with high disability was comparably low (p = 0.16). Mortality was higher among EVT subjects (10% vs 3%; p = 0.04) and sICH was rare (n = 6 vs n = 1, p = 0.14).
Conclusions
EVT and IVT appear similarly effective in achieving a favourable outcome in AIS patients with ELVO and mild neurological symptoms, despite signs of poorer results with EVT regarding outcome across all levels of disability and mortality.
Further studies are required to determine whether and which subgroups of patients with ELVO and mild symptoms may particularly benefit from EVT.
Trial registration number
N/A
AS05-025
IS INTRAVENOUS THROMBOLYSIS GETTING ANY QUICKER IN THE UK? DATA FROM THE NATIONAL STROKE REGISTRY
1King’s College London, School of Population Health and Environmental Sciences, London, United Kingdom
2Royal Devon and Exeter NHS Foundation Trust, Royal Devon and Exeter Hospital, Exeter, United Kingdom
3King’s College London, Division of Health and Social Care Research, London, United Kingdom
Background and Aims
Intravenous thrombolysis (IVT) for acute ischaemic stroke is recommended within 4.5 hours of symptom onset, but within this time frame there is a steep decline in the odds of a good outcome with the passage of time.
Methods
Patient-level data from the Sentinel Stroke National Audit Program (SSNAP), the national stroke registry for England, Wales and Northern Ireland, were analysed for patients who received thrombolysis between July 2013 and September 2018.
Results
Of the 427,645 patients admitted to 142 stroke units over 5 years, 49,550 (11.6%) were thrombolysed. Median door-to-needle time has decreased by approximately 2 minutes per year, from 59 minutes in 2013 to 50 minutes in 2018. Of those thrombolysed, 29,605 patients received IVT within one hour of symptom onset (59.75%). The proportion of patients thrombolysed within one hour increased from 52% in July 2013 to 63% in September 2018. Quarterly medians and interquartile ranges are shown in the figure.

Conclusions
Door-to-needle time has steadily reduced in the UK over the last 5 years, with an increase in the proportion of patients thrombolysed within one hour of hospital arrival. However, progress is slow and further significant quality improvements are needed in order to maximise the population benefit from alteplase for acute ischaemic stroke.
Trial registration number
N/A
AS05-036
INTRAVENOUS THROMBOLYSIS FOR SUSPECTED ISCHEMIC STROKE WITH SEIZURE AT ONSET
1University Hospital Basel and University of Basel, Department of Neurology and Stroke Center, Basel, Switzerland
2Helsinki University Hospital, Department of Neurology, Helsinki, Finland
3Charité-Universitätsmedizin Berlin, Department of Neurology, Berlin, Germany
4University Hospital Heidelberg, Department of Neurology, Heidelberg, Germany
5Inselspital- Bern University Hospital, Department of Neurology, Bern, Switzerland
6Academic Medical Centre- Amsterdam, Department of Neurology, Amsterdam, The Netherlands
7Nuovo Ospedale Civile S. Agostino-Estense- Modena University Hospital, Stroke Unit- Department of Neuroscience, Modena, Italy
8University Hospital and Medical School of Dijon- University of Burgundy, Department of Neurology, Dijon, France
9University Hospital Zurich and University of Zurich, Department of Neurology, Zurich, Switzerland
10Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
11University of Basel and University Center for Medicine of Aging and Rehabilitation- Felix Platter Hospital, Neurorehabilitation Unit, Basel, Switzerland
Background and Aims
Seizure at onset (SaO) has been considered a relative contraindication for intravenous thrombolysis (IVT) in patients with acute ischemic stroke, although this appraisal is not evidence-based. Here, we investigated the prognostic significance of SaO in patients treated with IVT for suspected ischemic stroke.
Methods
In this multicenter, registry-based study on IVT-treated patients with suspected ischemic stroke we assessed the association between SaO and (i) symptomatic intracranial hemorrhage (sICH; European-Cooperative-Acute-Stroke-Study-II [ECASS-II] criteria), (ii) mortality and (iii) functional outcome on the modified Rankin Scale (mRS) at 3 months using (a) unadjusted and (b) adjusted logistic regression, (c) coarsened exact matching and (d) inverse probability weighted analyses.
Results
We included 10,074 patients (mean age 70.2 ± 13.8 years, 44.7% female). The 146 patients with SaO (1.5%) had higher NIHSS on admission (median [IQR] 13 [7-21] vs 9 [5-15]), more often history of prior stroke (25.7% vs 16.5%) and more often stroke mimics (39% vs 2%) than non-SaO patients. In unadjusted regression analyses, patients with SaO had generally less favorable outcomes than non-SaO patients. After covariate adjustment, as well as in matched and weighted analyses, all associations between SaO and any of the outcome measures disappeared (graph). These results were consistent in the patient subgroup with verified ischemic stroke after exclusion of the stroke mimics.

Conclusions
Among patients treated with IVT for suspected ischemic stroke, SaO was not an independent predictor of poor prognosis. Withholding IVT from otherwise eligible patients with assumed ischemic stroke presenting with SaO may not be justified.
Trial registration number
N/A
AS15-045
E-Poster Discussion-Etiological Diagnosis
IS THE EMBOLIC STROKE OF UNDETERMINED SOURCE DEFINITION GOOD ENOUGH FOR YOUNG ADULT STROKE PATIENTS?
1These authors contributed to this abstract equally- Hospital Egas Moniz- Centro Hospitalar Lisboa Ocidental, Neurology, Lisboa, Portugal
2Hospital Egas Moniz- Centro Hospitalar Lisboa Ocidental, Neurology, Lisboa, Portugal
Background and Aims
In young adult stroke patients, up to 25% meet the embolic stroke of undetermined source (ESUS) criteria. Although the transesophageal echocardiography (TEE) is considered the gold-standard study to exclude some embolic sources, it is not deemed necessary for the ESUS definition. Our aim is to evaluate the diagnostic yield and therapeutic impact of the TEE in young adults with ESUS.
Methods
Retrospective analysis of a single-center cohort of consecutive young adult ischemic stroke patients (18-55 years), admitted between 2010–2018, satisfying ESUS criteria. In these patients, TEE findings and consequent diagnostic and therapeutic implications were characterized. The following findings were considered possible stroke etiologies: intracavitary/aortic thrombus, vegetation, patent foramen oval (PFO) with interatrial septum aneurysm (ASIA) and/or large shunt and Risk of Paradoxical Embolism (RoPE) score ≥7, atrial/ventricular septum defect and complex aortic arch atheroma.
Results
Among 293 young adult stroke patients, 116 (39.6%) fulfilled the ESUS criteria. 113 (97.4%) underwent TEE, which allowed to disclose the stroke etiology in 32 (28.3%): intracavitary/aortic thrombus in 1.8% (n = 2), vegetation in 0.9% (n = 1), PFO with ASIA and/or large shunt and RoPE score ≥7 in 19.5% (n = 22), atrial/ventricular septum defect in 1,8% (n = 2) and complex aortic arch atheroma in 4,4% (n = 5). TEE findings modified the secondary prevention strategy in 30.1% (n = 34): anticoagulation in 15% (n = 17), PFO/septum defect closure in 23% (n = 26) and antibiotic treatment in 0.9% (n = 1).
Conclusions
The diagnostic yield of TEE in young adults with ischemic stroke may question the defined ESUS criteria in this age group.
Trial registration number
N/A
AS15-060
E-Poster Discussion-Etiological Diagnosis
STROKE MIMICS AND CHAMELEONS WHEN ACTIVATING STROKE CODE
1Seoul National University Hospital, Department of Neurology, Seoul, Republic of Korea
Background and Aims
When encountering a suspected stroke patient, it is challenging to distinguish patients with acute stroke (AS) in a short time in an emergency. We aimed to determine the frequency and characteristics of stroke mimics (false positive cases) and stroke chameleons (false negative cases), and identify the key clinical features.
Methods
All consecutive patients admitted in the emergency room with stroke code between 2016 and 2017 were included for the analysis. Patients with a sudden onset of neurological deficit in a time window less than 8 hours were accepted in the stroke code pathway. Stroke mimics were determined by an expert neurologist after brain MRI imaging. Stroke chameleons were defined as failure to suspect stroke or incorrect exclusion of stroke at the emergency department.
Results
Among the all included patients (mean 65.7 years, 57.1% male), 443 patients were correctly diagnosed as AS, 205 patients were stroke mimics, and 37 patients were stroke chameleons at the initial screening. The positive predictive value of stroke code activation was 68.4%, and the sensitivity was 92.3%. In the stroke mimics, the most frequent discharge diagnosis was epilepsy (19.5%), brain tumor (10.2%), drug-related encephalopathy (9.8%), and metabolic encephalopathy (8.3%). In the stroke chameleons, the initial diagnosis was mistaken for non-stroke for the following reasons: only dizziness symptoms (32.4%), visual symptoms (13.5%), and headache (8.1%).
Conclusions
This study demonstrated that the frequency and characteristics of stroke mimics and chameleons. These findings may be used to raise awareness in emergent setting to recognize and treat such patients appropriately.
Trial registration number
N/A
AS15-014
NONFOCAL TRANSIENT NEUROLOGICAL ATTACKS ARE ASSOCIATED WITH CEREBRAL SMALL VESSEL DISEASE
1University Medical Center Utrecht, Department of Neurology, Utrecht, The Netherlands
2OLVG west, Department of Neurology, Amsterdam, The Netherlands
3University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, The Netherlands
4Erasmus Medical Center, Department of Biomedical Imaging, Rotterdam, The Netherlands
5Leiden University Medical Center, Department of Radiology, Leiden, The Netherlands
Background and Aims
Nonfocal transient neurological attacks (TNAs) are associated with an increased risk of stroke and dementia. Cerebral ischemia probably plays a role in their etiology, but the precise mechanisms are unknown. We hypothesized that TNAs are related to manifestations of cerebral small vessel disease on MRI.
Methods
We included participants with no history of stroke or TIA from the Heart Brain Connection Study. The presence of lacunes and WMHs of presumed vascular origin was evaluated on brain MRI according to the STRIVE criteria. WMHs were scored according to the Fazekas score (grade 0–3), and further dichotomized into ≤1 (none to multiple punctate lesions) versus ≥2 (early confluent or confluent lesions). We assessed the following TNAs with a standardized interview: unsteadiness, lightheadedness, unconsciousness, confusion, amnesia, blurred vision, paresthesias and bilateral weakness. We calculated odds ratios (ORs) with 95% confidence intervals (CIs) for the presence of lacunes and early confluent or confluent WMHs, adjusted for age, sex and hypertension.
Results
Of 304 participants (60% male; mean age 67 ± 9 years), 63 participants (21%) experienced ≥1 TNAs. In participants with TNAs the presence of lacunes and early confluent or confluent WMHs was more common than in participants without TNAs (35% versus 20%; adjusted OR 2.32, 95% CI 1.22–4.40 and 48% versus 27%; adjusted OR 2.65, 95% CI 1.44–4.90, respectively).
Conclusions
TNAs are associated with the presence of lacunes and early confluent or confluent WMHs of presumed vascular origin, which indicates that cerebral small vessel disease might play a role in the etiology of TNAs.
Trial registration number
N/A
AS15-004
PROGNOSTIC PERFORMANCE OF DIFFERENT THRESHOLDS OF LEFT ATRIAL DIAMETER TO PREDICT ATRIAL FIBRILLATION AFTER EMBOLIC STROKE OF UNDETERMINED SOURCE
1University of Thessaly, Department of Medicine, Larissa, Greece
2Centre Hospitalier Universitaire Vaudois and University of Lausanne, Stroke Center and Neurology Service- Department of Clinical Neurosciences, Lausanne, Switzerland
3Medical School of Athens- Alexandra Hospital, Department of Clinical Therapeutics, Athens, Greece
Background and Aims
We analyzed consecutive patients with embolic stroke of undetermined source (ESUS) from three prospective stroke registries to compare the prognostic performance of different left atrial diameter (LAD) thresholds for the prediction of detection of atrial fibrillation (AF).
Methods
We calculated the sensitivity, specificity, positive prognostic value (PPV), negative prognostic value (NPV) and Youden’s J-statistic of different LAD thresholds to predict AF detection. We performed multivariate stepwise regression with forward selection of covariates to assess the association between the LAD threshold with the highest Youden’s J-statistic and AF detection.
Results
Among 675 patients followed for 2437 patient-years, the mean LAD was 38.5 ± 6.8mm. AF was detected in 115 (17.0%) patients. The LAD threshold of 40mm yielded the highest Youden’s J-statistic of 0.35 with sensitivity 0.69, specificity 0.66, PPV 0.27 and NPV 0.92. The likelihood of AF detection was nearly twice in patients with LAD>40mm compared to LAD≤40mm (HR:1.92, 95%CI:1.24–2.97, p = 0.004). The 10-year cumulative probability of AF detection was higher in patients with LAD>40mm compared to LAD≤40mm (53.5% and 22.4% respectively, log-rank-test:28.2, p < 0.001). The annualized rate of stroke recurrence of 4.0% in the overall population did not differ significantly in patient above vs. below this LAD threshold (HR:0.96, 95%CI:0.62–1.48, p = 0.85).
Conclusions
The LAD threshold of 40mm has the best prognostic performance among other LAD values to predict AF detection after ESUS. In ESUS patients with LAD≤40mm, the probability that AF will not be detected during a follow-up of 3.6 years is 92%.
Trial registration number
N/A
AS15-028
LONG TERM SURVEILLANCE RESULTS FOR ATRIAL FIBRILLATION DETECTION IN A COHORT OF CRYPTOGENIC STROKE PATIENTS IN A COMMUNITY HOSPITAL SETTING
1Cone health, stroke center, Greensboro, USA
2Cone Health stroke center, neurology, greensboro, USA
3Cone Health, cardiology, Greensboro, USA
Background and Aims
Atrial fibrillation (AF) detection rates of 30% have been shown in a large clinical trial but real world detection rates for AF on long term follow up are not well described. We present long term follow up results for AF detection in our cohort of cryptogenic stroke patients with implantable loop recorders (ILR) at our community hospital.
Methods
We reviewed electronic medical charts of our prospective cohort of cryptogenic stroke patients who underwent ILR insertion. All patients met ESUS criteria for cryptogenic strokes and had remote structured follow up in cardiology device clinic.
Results
432 patients underwent ILR implantation from March 2014 to December 2018. 116 (26.85%) developed atrial fibrillation and were not followed further. In patients without AF median device follow up time was 1013 days (range 81–1736).median time from index event to device insertion was 4.5 days and AF detection was 141.5 days (range 0–1074). All patients had AF duration more than 6 minutes.111 patients were started on anticoagulation (95%) and 5 patients refused. Median time from AF detection and starting anticoagulation was 1 day. Average CHAD2vasc score was 5. There were no significant differences in age, sex, race amongst patients with and without AF detected.
Conclusions
On long term follow up. (median 1013 days) we found atrial fibrillation in 116 out of 432 patients (26.85%) Our median time to AF detection of 141 days suggests benefits of long term continuous monitoring in cryptogenic stroke patients . Detecting AF changed management to anticoagulation in majority of our patients soon after AF detection.
Trial registration number
N/A
E-Poster Discussion-Outcome Complications and Prognosis II
AS18-044
FOREIGN BODIES IN MECHANICALLY EXTRACTED THROMBI IN ACUTE ISCHEMIC STROKE PATIENTS WHO UNDERWENT ENDOVASCULAR TREATMENT
1Erasmus MC- University Medical Center Rotterdam, Experimental Cardiology, Rotterdam, The Netherlands
2Haaglanden Medical Center, Radiology, The Hague, The Netherlands
3Erasmus MC- University Medical Center Rotterdam, Neurology, Rotterdam, The Netherlands
4Erasmus MC- University Medical Center Rotterdam, Radiology, Rotterdam, The Netherlands
Background and Aims
During endovascular treatment procedures for acute ischemic stroke (AIS), stent-retrievers may be re-introduced as multiple attempts are often needed to achieve complete reperfusion. In this paper we describe the occurrence of foreign bodies in retrieved thrombi.
Methods
Thrombi (n = 281) were collected directly after thrombectomy from MR CLEAN registry hospitals in the Netherlands. Of these, 16 thrombi were still entrapped within in the stent-retriever. Regular thrombi were sectioned and prepared for cross-sectional light microscopy (LM). Thrombi still entrapped in their stent-retriever were prepared as a whole for scanning electron microscopy (SEM). All thrombi were systematically inspected for the presence of foreign body’s with either LM or SEM. For LM, a thrombus was considered positive if the foreign body was found within the thrombus. For SEM, a thrombus was considered positive if the foreign body was entwined within the thrombus, not merely adherent to the surface.
Results
Foreign bodies, some consisting of thread- (Fig 1) or sheet-like structures (Fig 2) were found in 19 of 281 thrombi (7%). Of these, 4 were found in the 16 SEM specimens (25%).

Figure 1: Thread-like foreign body with SEM at 30x (A). Magnification of red box in (A) at 150x (B).

Figure 2. Sheet like foreign body’s with LM (examples marked by black arrows).
Conclusions
Foreign bodies are found in a substantial proportion of thrombi retrieved by mechanical thrombectomy for AIS. Neuro-interventionalists should be aware of the possibility of inadvertently introducing foreign bodies during thrombectomy procedures.
Trial registration number
N/A
AS17-051
THE EPIDEMIOLOGY OF FRACTURE IN PATIENTS WITH ACUTE ISCHEMIC STROKE IN KOREA
1Soonchunhyang University Hospital, Neurology, Seoul, Republic of Korea
2Seoul National University Bundang Hospital, Neurology and Cerebrovascular Center, Seongnam, Republic of Korea
3Nowon Eulji Medical Center- Eulji University, Neurology, Seoul, Republic of Korea
4Ilsan Paik Hospital- Inje University, Neurology, Goyang, Republic of Korea
5Seoul Medical Center, Neurology, Seoul, Republic of Korea
6Eulji University Hospital- Eulji University, Neurology, Daejeon, Republic of Korea
7Hallym University Sacred Heart Hospital, Neurology, Anyang, Republic of Korea
8Korea University College of Medicine, Biostatistics, Seoul, Republic of Korea
9Asan Medical Center, Clinical Research Center, Seoul, Republic of Korea
Background and Aims
Patients who survive an acute phase of stroke are at risk of falls and fractures afterwards. However, it is largely unknown how frequent fractures occur in Asian stroke population.
Methods
Patients with acute (<7 days) ischemic stroke who were hospitalized between January 2011 and November 2013 were identified from a prospective multicenter stroke registry in Korea, and were linked to the National Health Insurance Service claim database. The incidences of fractures were investigated up to 4 years after index stroke. The cumulative incidence was estimated by the Kaplan-Meier product-limit method. Cox proportional hazards regression models were applied for exploring risk factors of post-stroke fractures.
Results
Among a total of 11,522 patients, 1,616 fracture events were identified: 712 spine fractures, 397 hip fractures and 714 other fractures. The cumulative incidence of any fractures was 2.72% at 6 months, 4.69% at 1 year, 8.87% at 2 years and 9.97% at 4 years. Those of spine/hip fractures were 1.15%/0.63%, 1.99%/1.08%, 3.60%/2.04% and 6.71%/3.64%, respectively. Age by a 10-year increment (hazard ratio, 1.33; 95% confidence interval, 1.26 to 1.40), female (1.69; 1.49 to 1.91), previous fracture (1.76; 1.58 to 1.97), osteoporosis (1.41; 1.25 to 1.60) and serum creatinine by a 1mg/dL increment (1.09; 1.03 to 1.14) were independent risk factors of fractures after stroke.
Conclusions
The cumulative incidence of fractures was about 5% at 1 year and 10% at 4 years after acute ischemic stroke in Korea. Older age, female, pre-stroke fracture, osteoporosis and increased serum creatinine raised the risk of post-stroke fractures.
Trial registration number
N/A
AS18-026
SERUM URIC ACID AND RISK OF HEMORRHAGIC TRANSFORMATION IN PATIENTS WITH ISCHEMIC STROKE
1Center of Cerebrovascular Disease- Department of Neurology- West China Hospital- Sichuan University- Chengdu- P.R. China, Center of Cerebrovascular Disease- Department of Neurology, Chengdu, China
Background and Aims
Uric acid is an antioxidant with neuroprotective effects in experimental stroke models. Whether serum uric acid (UA) plays a role in hemorrhage transformation (HT) remains unclear. We sought to explore the association between serum UA and HT in patients with acute ischemic stroke (AIS) taking into consideration potential sex-related differences.
Methods
AIS patients within 7 days after stroke onset were prospectively and consecutively enrolled between January 2016 and October 2017. Patients were categorized into three groups according to serum UA tertiles by sex (Males: tertile1: ≤305.0, tertile2: 305.1–382.0 and tertile3: ≥382.1; Females: tertile1: ≤248.5, tertile2: 248.6–316.0 and tertile3: ≥316.1 umol/L). HT was detected by follow-up computed tomography (CT) or Magnetic Resonance Imaging (MRI). The multivariate logistic analysis was performed to assess the association of serum UA with HT.
Results
1025 AIS patients (mean age 62.6 years, 65.3% males) were finally included. 108 (10.5%) patients experienced HT. After adjustment for potential confounders, the highest UA tertile in male patients showed a significant decrease in HT compared with the lowest UA tertile (OR0.035, 95% CI 0.008–0.163). Similar results were observed for female patients, and the highest UA tertile in females was independently inversely associated with HT compared with the lowest UA tertile (OR 0.188, 95% CI 0.070–0.507).
Conclusions
Higher serum UA was associated with lower risk of HT. Admission serum UA might be used as one of the predictors for HT. More studies are needed to elucidate the potential neuroprotective mechanism of serum UA and its link to HT.
Trial registration number
N/A
AS18-059
UPTAKE OF EVIDENCE-BASED PREVENTION FOR DEEP VEIN THROMBOSIS AND PULMONARY EMBOLISM IN STROKE UNITS IN ENGLAND, WALES AND NORTHERN IRELAND
1King’s College London, School of Population Health and Environmental Sciences, London, United Kingdom
2Royal Devon and Exeter NHS Foundation Trust, Royal Devon and Exeter NHS Foundation Trust, Exeter, United Kingdom
Background and Aims
Intermittent pneumatic compression (IPC) reduces the risk of deep vein thrombosis (DVT) after stroke (CLOTS3 2013). In 2013, the NHS provided funding in England to encourage IPC uptake. The Welsh Government funded the provision of IPC sleeves in all Welsh stroke units in 2016. We report IPC usage in England, Wales and Northern Ireland (NI) over time.
Methods
Data were extracted from the national register of stroke in England, Wales and NI (SSNAP). The percentage of hospitals applying IPC to patients between April 2014 and July 2018 in the 3 countries are reported.
Results
Since April 2014, the percentage of hospitals using IPC has increased in England (24% to 93%) and Wales and NI (0% to 75%). The proportion of English hospitals applying IPC to more than 40% of patients rose from 2.7% to 25.5%. Comparatively, uptake of IPC was slower in Wales and NI with no hospitals applying IPC to >40% of patients until October 2015. The proportion of hospitals reporting IPC application >40% of patients has remained relatively stable since January 2017.

Conclusions
IPC is an inexpensive and effective treatment, however uptake has been slow. Compared to Wales and NI, more hospitals in England use IPC and have for longer, which may be due to the earlier provision of funding for IPC sleeves. The percentage of hospitals treating >40% of patients has remained low and stable since January 2017 in all three countries. Efforts focussed on education, and increasing availability should be made.
Trial registration number
N/A
AS17-074
ARTERY OCCLUSION INDEPENDENTLY PREDICTS UNFAVORABLE OUTCOME IN PATIENTS WITH CERVICAL ARTERY DISSECTION
1University Hospital Basel, Neurology and Stroke Center, Basel, Switzerland
Background and Aims
To assess the impact of dissected artery occlusion (DAO) on functional outcome and complications in patients with cervical artery dissection (CeAD).
Methods
We analyzed combined individual patient data from three multicenter cohorts of consecutive CeAD patients (the CADISP-Plus consortium dataset). Patients with data on DAO and functional outcome were included. We compared patients with DAO to those without DAO. Primary outcome was favorable functional outcome (i.e. Modified Rankin Scale (mRS) score 0–1) measured 3–6 months from baseline. Secondary outcomes included the occurrence of delayed cerebral ischemia, major hemorrhage, recurrent CeAD and death. We performed univariate and multivariable binary logistic regression analyses and calculated odds ratios (OR) with 95% Confidence intervals (CI), with adjustment for potential confounders.
Results
Of 2148 patients (median age 45 years (IQR 38–52), 43.6% women), 728 (33.9%) had DAO. Patients with DAO more frequently presented with cerebral ischemia (84.6% vs 58.5%, p < 0.001). DAO-patients were less likely to have favorable outcome when compared to non-DAO patients (mRS 0–1: 59.6% vs 80.1%, punadjusted<0.001). After adjustment for age, sex, and initial stroke severity, DAO was independently associated with less favorable outcome (OR 0.65, CI 0.50–0.84, p = 0.001). Delayed cerebral ischemia numerically occurred more frequently in patients with DAO than in non-DAO patients (4.5% vs 2.9%, p = 0.059). The remaining secondary outcomes did not differ.
Conclusions
DAO independently predicts less favorable functional outcome in CeAD patients. Further research on vessel patency, collateral status and effects of revascularization therapies particularly in DAO patients is warranted.
Trial registration number
N/A
E-Poster Discussion-Epidemiology II
AS30-041
GENDER INEQUITIES IN STROKE, DOES THROMBECTOMY CHANGE THE DEAL?
1Hospices Civils de Lyon- Public Health Department- F-69003 Lyon- France, Public Health Department, LYON, France
2Hospices Civils de Lyon- Pierre Wertheimer neurologic hospital F-69003 Lyon- France, Stroke Unit, Lyon, France
Background and Aims
Implementation of mechanical thrombectomy leads to new stroke care organization challenges. It is necessary to ensure that this won’t increase inequities in access to reperfusion therapies at acute phase. We aimed to study gender inequities in access to thrombectomy in a French prospective population-based cohort study.
Methods
All patients managed for confirmed ischemic stroke (IS) from November 2015 to December 2016 in the Rhône French county were prospectively included in the STROKE69 cohort. We studied patients and stroke characteristics, management times, access to thrombectomy and 3-Month outcome (good for mRS = 0-2) according to gender.
Results
The 1543 included IS patients comprised 766 (49.6%) women and 777 (50.4%) men. Women were older (mean age+/-SD 78+/-14.5 versus 70.5+/-14.3, p < 0.001), and more severe at admission (NIHSS> = 15 22% versus 16%, p = 0.005) than men. They less frequently called emergency medical services (54% versus 64%, p < 0.001) and were less managed in stroke unit (54% versus 68%, p < 0.001) than men. Prehospital times were not significantly different but door-to-imaging time was longer for women than men (2h40 versus 2h27, p = 0.01). Finally, for women versus men respectively, 9% versus 11% were treated with thrombectomy (adjusted OR* = 0.9 (0.6–1.3), p = 0.627), 22% versus 26% were treated with thrombectomy and/or thrombolysis (adjusted OR* = 0.9 (0.7–1.2), p = 0.537) and 51.7% versus 68.5% had good 3-month outcome (adjusted OR* = 1.3 (0.9–1.9), p = 0.093).
*adjusted on age and NIHSS at admission.
Conclusions
Disparities in stroke features and acute care pathway observed between gender do to not translate in differences in reperfusion strategies access or 3-month outcome in our cohort after adjustment.
Trial registration number
NCT02596607
AS29-013
DIAGNOSTIC ACCURACY OF EXPLICIT DIAGNOSTIC CRITERIA FOR TIA: A VALIDATION STUDY
1the Ural State Medical University, Neurology, Ekaterinburg, Russia
2Julius Center for Health Sciences and Primary Care- University Medical Center Utrecht- Utrecht University, Neurology, Utrecht, The Netherlands
3Rigshospitalet Glostrup- University of Copenhagen, Neurology, Copenhagen, Denmark
4University Medical Center Utrecht- Utrecht University, Neurology, Utrecht, The Netherlands
Background and Aims
The diagnosis of transient ischemic attack (TIA) can be difficult. Explicit diagnostic criteria for TIA (EDCT) were recently proposed by us. The aim of this study was to test the EDCT for sensitivity and specificity in a material from general practice.
Methods
We used data from 206 patients in whom the general practitioner suspected a TIA. All patients participated in the ‘Markers in the Diagnosis of TIA’ (MIND-TIA) study. Clinical information was collected within 72 hours after onset using standardized questionnaire. Subsequently, all patients were evaluated at a TIA service. A panel of three experienced neurologists ultimately determined the definite diagnosis based on all available diagnostic information. Sensitivity, specificity, predictive values, and c-statistic of the EDCT were calculated. A secondary analysis was performed with adjusted sub-criteria of the EDCT.
Results
Of the 206 patients, 126 (61%) had an actual TIA (n = 104) or minor stroke (n = 22), and 80 (39%) an alternative diagnosis. Most common alternative diagnoses were migraine with aura (n = 24, 30.0%), stress related or somatoform symptoms (n = 16, 20.0%), and syncope (n = 9, 11.3%). The original EDCT had a sensitivity of 98.4% (94.4 – 99.8), and a specificity of 61.3% (49.7 – 71.9). The c-statistic was 0.80 (0.73 – 0.87). The adjusted EDCT showed a specificity of 73.8% (62.7 – 83.0) and the same sensitivity, with a c-statistic of 0.86 (0.80 – 0.92).
Conclusions
Explicit diagnostic criteria for TIA had an excellent sensitivity and good specificity and can be a valuable diagnostic tool for the diagnosis of TIA, especially in the primary care setting.
Trial registration number
N/A
AS16-048
BEYOND A SINGULAR ODDS RATIO FROM ORDINAL OUTCOME SCALES: INTRODUCING THE NET BENEFIT PROFILE
1charité universitätsmedizin, center for stroke research, berlin, Germany
2Amsterdam UMC, dept of Neurology, Amsterdam, The Netherlands
3hospital Sainte Anne, dept Neurology, Paris, France
Background and Aims
Most acute stroke trials assess functional outcome on the modified Rankin Scale (mRS) as their primary endpoint. Stacked bar charts show the mRS distributions in the treatment arms, but do not quantify the treatment effect. To do so, a common odds ratio (cOR) can be calculated to estimate the odds of any clinical improvement due to treatment. This approach, however, still fails to quantify the extent of the improvement whilst relying on problematic statistical assumptions. Our aim was to find a more intuitive way to quantify and visualize the expected shift on the mRS due to treatment.
Methods
We describe the net benefit profile, which visualizes the expected shift on the mRS in 100 treated patients. We use multiple Mann-Whitney-U tests to calculate absolute risk differences between treatment groups, from which we derive the number-needed-to-treat and subsequently construct the profile. As an example, we applied our concept to the effect of mechanical thrombectomy on the mRS, using pooled data from the HERMES collaboration (figure). mRS scores can be replaced by corresponding health-utilities, which results in a profile of expected shift in various amounts of health-utility.
Results

Conclusions
Our method is free of ordinal logistic regression assumptions, and helps to translate ordinal trial results into clinical practice as it quantifies the extent of the treatment benefit. Adding (country specific) utilities incorporates the relevant patient perspective, and may be useful for more detailed cost-utility analyses.
Trial registration number
N/A
AS16-042
COME FLY WITH ME!
1Our Lady of Lourdes Hospital, Stroke and Geriatric Medicine, Drogheda, Ireland
Background and Aims
Following a stroke, medical professionals are frequently asked by patients when is it safe to fly? Currently, there are no official European guidelines on flying after a stroke. Timeline recommendations vary between 10 days to 21 days and up to 3 months depending on clinician opinion, severity of stroke, travel insurance status and individual airline carriers. We reviewed current advice given by European airlines on flying after a stroke.
Methods
An internet review of European airlines’ websites was performed in December 2018. Data was collected on information available: 1) On website 2) By direct contact via email or telephone 3) Advice given 4)Timeline recommendations.
Results
58 European airline websites were reviewed. 48 (83%) commercial airlines have no information available on their website on flying after a stroke. After contact by email, telephone or webchat, 27 (47%) airlines could give recommendations, but only 7 (12%) airlines could advise about specific timelines. Responses included 3 days, 10 days, 10 days with doctor’s clearance, 11–21 days, 2 weeks, 1 month, 3 months and 6 months. 39 (67%) airlines advised to contact their treating doctor on flying and 13 (22%) airlines have a doctor attached to their company to advise.
Conclusions
To date, there is no timeline guideline consensus on flying following a stroke. Most airlines recommend a medical clearance certificate from their treating doctor, however doctors do not have formal guidelines to base their decisions on. A stroke advisory group to standardise when flying after stroke is safe may be beneficial in guiding treating doctors.
Trial registration number
N/A
AS30-007
SEX DIFFERENCES IN ISCHEMIC STROKE SUBTYPES, STROKE CARE AND OUTCOMES: THE SOUTH LONDON STROKE REGISTER
1Beijing University Health Science Center, School of Public Health, Beijing, China
2King’s College London, School of Population Health & Environmental Sciences, London, United Kingdom
Background and Aims
To identify sex differences in ischemic stroke subtypes, stroke care and outcomes.
Methods
From 1999 to 2016, 2684 first-ever ischemic stroke patients were recorded in the South London Stroke Register (SLSR). The SLSR data includes stroke subtypes (modified TOAST), sociodemographic factors, case mix, stroke care and pre-stroke risk factors, together with functional and survival outcome. Sex differences in poor outcomes (BI<15 or death) among subtypes wereexamined throughmultiple logistic regression analysis. Sex differences in survival outcomes among subtypes were examined using Kaplan-Meier curves and multivariate Cox proportional hazard models.
Results
The mean age for stroke onset in women is 6 years higher than for men (74 vs. 68, P<0.001). Women are more likely to experience a poorer case mix (P<0.001). Cardioembolism (CE) stroke is more common in women (29.15% vs. 24.11%, P = 0.003) and Small vessel occlusion (SVO) stroke is more common in men (28.27% vs. 23.71%, P = 0.006). There was no difference between men and women with regard to the rates of stroke unit admission and secondary prevention management. After adjusting for confounding factors, there were no sex differences in poor outcomes identified; however, being female had a lower risk of death for ischemic stroke (Hazard Ratio (HR) = 0.882, [95%CI: 0.790,0.984]).
Conclusions
CE subtype is more common in women while SVO is more common in men. There were no significant sex differences in stroke care. After adjusting for potential confounding factors, women had a lower risk of death, however, there were no sex differences in poor outcomes.
Trial registration number
N/A
E-Poster Discussion-Outcomes after Stroke
AS17-033
WHITE MATTER HYPER-INTENSITY BURDEN AND OUTCOME IN ISCHEMIC STROKE PATIENTS TREATED WITH MECHANICAL THROMBECTOMY: FINDINGS FROM THE THRACE TRIAL AND MULTICENTER STUDY
1Centre Hospitalier Sainte Anne, Interventional Neuroradiology, Paris, France
2CHRU Lille, Neuroradiology, Lille, France
3CHRU Lille, Neurology, Lille, France
4Centre Hospitalier Sainte Anne, Neurology, Paris, France
5Centre Hospitalier Sainte Anne, Neuroradiology, Paris, France
6Massachusetts General Hospital- Harvard Medical School, Stroke Research Center, Boston, USA
7CHRU Nancy, Neuroradiology, Nancy, France
Background and Aims
We aimed to determine the influence of WMH burden on clinical outcome, rate of symptomatic intracranial hemorrhage (ICH) and procedural success in AIS patients treated by MT with current stentriever/aspiration devices.
Methods
Patients with AIS due to LVO from THRACE trial, and prospective cohorts from two academic comprehensive stroke centers treated with MT, were pooled and retrospectively analyzed. WMH volumes were obtained by semi-automated planimetric segmentation and tested in association with the rate of favourable outcome (90 days functional-independence), successful recanalization after MT, and symptomatic ICH.
Results
A total of 535 subjects were included between 2015 and 2018 (49% female, mean age 68.0 years ± 15.0). Overall, 458(85.6%) patients presented with detectable WMH (median:5.7cc IQR[2.8–12.7]). Patients demonstrated increasingly worse outcomes with increasing WMH volumes, with 57% of patients in the 1st quartile of WMH volume vs 27% in the 4th demonstrating favourable outcome (p < 0.001), aOR:1,04 for unfavourable outcome 95%CI [1,01-1,07], p = 0,021 as a linear variable). WMH severity was not associated with sICH rate (aOR: 1,08 [0.53–1,64], p = 0,80) nor did it influence recanalization success (aOR:1.04 [0.84–1.29], p = 0.67).
Conclusions
Our study provides evidence that patients with AIS due to LVO and severe WMH as assessed by pretreatment MRI, are at higher risk for less favourable outcome following MT, despite similar rates of sICH and procedural success. . Since over a quarter of patients with severe WMH in our sample experienced favorable 3 months outcome, WMH may not be a good argument to deny MT.
Trial registration number
ClinicalTrials.gov Identifier: NCT01062698
AS17-110
WHITE MATTER HYPERINTENSITIES IN ISCHEMIC STROKE PREDICT LEVELS OF NEUROFILAMENT LIGHT CHAIN PROTEIN IN SERUM AFTER SEVEN YEARS
1University of Gothenburg- Institute of neuroscience and physiology, Department of clinical neuroscience, Gothenburg, Sweden
2University of Gothenburg- Institute of Biomedicine, Department of Clinical Pathology and Genetics, Gothenburg, Sweden
3University of Gothenburg- Institute of Neuroscience and Physiology, Department of Psychiatry and Neurochemistry, Gothenburg, Sweden
Background and Aims
A high burden of white matter hyperintensities (WMH) predicts further progression of WMH but the time course is unknown. Serum neurofilament light chain protein (sNfL) levels provide a measure of white matter axonal damage during the months prior to blood sampling. We hypothesized that increased sNfL at seven years post stroke reflect continuing WMH progression at this time point.
Methods
Participants in the Sahlgrenska Academy Study on Ischemic Stroke examined with MRI at baseline and after seven years (n = 188, mean age 53 years, females 35%) were included. From visual ratings according to the Fazekas scale, three groups with different development stages of WMH were defined; early (without marked WMH at both time points), intermediate (marked WMH at follow-up only), and late stages (marked WMH at both time points). Levels of sNfL at seven years were measured by a single-molecule array assay.
Results
WMH in early, intermediate, and late stages were found in 123 (65%), 31 (16%), and 34 (18%) of the patients and mean levels of sNfL were 19 (95% CI: 16 -21), 31 (95% CI: 23–40), and 43 (95% CI: 33–57) pg/mL, respectively. Age and late stages of WMH were independently associated with sNfL in multivariable analysis, whereas no associations were found for subtype (TOAST) of index stroke, hypertension or recurrent stroke.
Conclusions
sNfL at seven years post stroke is associated with the development stage of WMH but not with etiologic subtype. Our results suggest that progression of WMH continues in the very long-term post-stroke.
Trial registration number
N/A
WITHDRAWN
AS20-007
TIME COURSE OF GRAPH-THEORETICAL PROPERTIES OF STRUCTURAL BRAIN NETWORKS AFTER STROKE IN RELATION TO CLINICAL RECOVERY
1Universitätsklinikum Hamburg-Eppendorf, Neurology, Hamburg, Germany
Background and Aims
Motor recovery after stroke relates to the degree of strategically located damage to brain structures such as the corticospinal tract. Impact of stroke lesions on the global integrity and topology of structural brain networks is less well described. We quantified longitudinal changes of structural brain network properties using graph-theoretical parameters in a prospective study of stroke patients with impaired motor functions.
Methods
Stroke patients with upper extremity motor deficits were prospectively enrolled and investigated by advanced structural MRI and clinical testing (grip strength, UEFM) at four time points (day 3–5 to 1 year after after stroke). Structural brain networks were reconstructed, numerical and topological measures of network integrity computed. Changes in network characteristics were assessed for association with clinical recovery using linear regressions.
Results
34 patients were included in the study. Network connectivity declined exponentially in ipsilesional hemispheres with steepest declines in patients with poor clinical recovery. Both ipsi- and contralesional hemispheres demonstrated disturbed network topology characterized by impaired structural integration and modulated by lesion volume.
Conclusions
Changes in structural brain networks occur predominantly during the early months after stroke and are modulated by lesion volume. In ipsilesional hemispheres, dynamic of connectional disintegration is related to the degree of recovery of motor function.
Trial registration number
N/A
AS17-065
CEREBRAL MICROBLEEDS AND LONG-TERM CLINICAL EVENTS OF ACUTE STROKE/TIA PATIENTS WITH NON-VALVULAR ATRIAL FIBRILLATION: THE SAMURAI-NVAF STUDY
1National Cerebral and Cardiovascular Center, Cerebrovascular medicine, Suita, Japan
2National Cerebral and Cardiovascular Center, Neurology, Suita, Japan
3National Cerebral and Cardiovascular Center, Stroke Care Unit, Suita, Japan
Background and Aims
Cerebral microbleeds (CMBs) have been reported to be a potential risk of intracranial hemorrhage and ischemic stroke. Limited data exist about the association of CMBs and clinical outcomes among patients with non-valvular atrial fibrillation (NVAF), most of whom need anticoagulants relating to a risk of intracranial hemorrhage.
Methods
Of 1,192 patients who participated in the SAMURAI-NVAF study (a prospective, multicenter, observational study), 1,099 patients (77.6 ± 10.0 years old, 620 men) surveyed the number of CMBs during the index ischemic stroke/TIA hospitalization. We assessed the association of CMBs with the long-term composite outcomes of all ischemic or hemorrhagic events and all-cause death after acute hospital discharge.
Results
CMBs were detected in 233 patients (23.4%); single CMB in 85, 2–4 CMBs in 96, and ≥5 CMBs in 52. The median follow-up period was 1.9 (interquartile range, 1.0–2.0) years. Ischemic stroke or systemic embolism was occurred in 74 patients, intracranial hemorrhage in 19, all ischemic events in 96, major bleeding in 45, and all-cause death in 183. The composite endpoint rate in patients without CMBs was 158.8 per 1000 patients-years, 173.6 in patients with single CMB, 225.6 in patients with 2–4 CMBs, and 289.5 in patients with ≥5 CMBs, respectively. According to the Cox regression analyses, ≥5 CMBs were associated with the composite outcome (adjusted hazard ratio 1.57; 95% CI 1.00–2.47) and major bleeding (2.61; 1.04–6.55).
Conclusions
Among NVAF patients with stroke/TIA, ≥5 CMBs were an independent risk factor of future vascular events or death, and major bleeding.
Trial registration number
N/A
E-Poster Discussion-Acute Management II
AS06-036
ADVANCED IMAGING ON A MOBILE STROKE UNIT DETECTS HIGH RATE OF LARGE VESSEL OCCLUSIONS IN THE FIELD
1University of Tennessee Health Science Center at Memphis, Department of Neurology- Mobile Stroke Unit, Memphis, USA
2University of Athens, Department of Neurology, Athens, Greece
Background and Aims
Mobile Stroke Units (MSU) traditionally utilize 8-slice CT for field diagnosis. We sought to implement a 16-slice, ultra-fast CT with auto-injection, aortic arch/neck/circle of Willis CTA on a first-of-its-kind MSU.
Methods
Our MSU was equipped with a Somatom Scope™ CT and multiphasic CTA (ESCAPE protocol). Field CT/CTA interpretation was by on-board stroke fellowship-trained clinicians. Operation began July 2016, averaging 12 days/month.
Results
During the first 365 days of service, 1031 MSU emergency activations occurred; of these, 629 (61%) were disregarded with unrelated diagnoses, and 402 patients transported: 245 (61%) stroke, 17 (4%) TIA, 140 (35%) other neurologic emergencies. Stroke/TIA patients were 59% female, 72% African American, 66 + 15 (median 65) years; median NIHSS score 6 (IQR 3–12) with 24 (10%) having hemorrhagic stroke (basal ganglia 15; thalamic 4; brainstem 1; aneurysmal SAH 3; hemorrhagic transformation of infarction 1); of 20 intraparenchymal hemorrhages, median ICH score was 2 (IQR 1–3) and 4 (20%) were spot sign positive. Among ischemic strokes, CTA revealed 62 (28%) LVO of which 9 (15%) were extracranial. A total of 73 (33%) received field tPA (1 sICH at 18 hours; 31.5% treated within golden hour). Total time from start, to images ready for viewing for combined non-contrast CT with CTA was 4.0 (IQR 3.5–4.5) minutes. No imaging needed to be repeated for image quality and all patients were triaged correctly.
Conclusions
MSU use of advanced imaging including multiphasic head and neck CTA is feasible, offers high yield of LVO detection and supports rapid diagnosis and appropriate triage from the field.
Trial registration number
N/A
AS06-108
PREHOSPITAL IDENTIFICATION OF LARGE VESSEL OCCLUSION BY PRESS (PREHOSPITAL STROKE SCORE) – A NEW COMBINED SYMPTOM SCORE
1Prehospital Emergency Medical services- Central Denmark Region, Research and development, Aarhus N, Denmark
2Aarhus University Hospital, Dept. of Neurology, Aarhus, Denmark
3Aarhus University Hospital, Dept. of Radiology, Aarhus, Denmark
4Aalborg University Hospital, Department of Clinical Medicine, Aalborg, Denmark
Background and Aims
The success of effective acute stroke treatment relies on fast recognition and short delay to treatment. Prehospital identification might optimize visitation. Early identification of a suspected large vessel occlusion (LVO) can facilitate direct transfer to a comprehensive stroke center (CSC).
The Prehospital Stroke Score (PreSS) is a simple two-part symptom-based stroke score which has been implemented in the ambulance services in the Central Denmark Region. PreSS 1 aims at identifying stroke. (1 point in either face weakness, arm weakness or slurred speech.) PreSS 2 aims at identifying LVO. (2 points in arm weakness, gaze palsy, incorrect month and/or age.)
We aimed to investigate the ability of PreSS 2 to identify LVO prehospitally.
Methods
PreSS positive patients admitted to a stroke center were prospectively included (June-December 2018). The PreSS score was compared with neuroimaging determining LVO status. Initial NIHSS in LVO patients who were either PreSS positive or negative were compared.
Results
Among 832 patients evaluated for stroke, 63 had LVO (7.6%). We found a PreSS 2 sensitivity of 57.1% and a specificity of 90.2%. Median NIHSS was significantly higher in LVO patients identified with PreSS part2 (19 vs.14, p = 0.007.)
Conclusions
The high specificity ensures that very few patients with non-LVO risk a longer transfer to a CSC that could delay thrombolysis. PreSS 2 does not identify all patients with LVO, but the patients that are missed scores markedly lower on NIHSS. It seems that PreSS 2 identifies patients with high NIHSS where the evidence for thrombectomy is strongest.
Trial registration number
N/A
AS06-109
IS IT POSSIBLE TO DETECT LARGE-VESSEL OCCLUSIONS IN ACUTE ISCHEMIC STROKE USING CLINICAL SCREENING SCALES?
1Akershus University Hospital, Department of Neurology, Lørenskog, Norway
2University of Oslo, Department of General Practice, Oslo, Norway
3University of Oslo, Institute of Clinical Medicine- Campus Akershus, Nordbyhagen, Norway
Background and Aims
Since endovascular thrombectomy is only performed in specialized centers, successful prehospital screening for large-vessel occlusion (LVO) would be of great importance. A vast majority of screening tools developed for this purpose have been tested retrospectively in patients with an established stroke diagnosis. Hence, these tools may have limited value calculating LVO in a prehospital setting. The aim of this study was to investigate the predictive values in patients presenting with acute stroke symptoms.
Methods
The Stroke Unit at Akershus University Hospital is the largest in Norway with a catchment area of about 10% of the population in Norway. Since 2012, we have had a stroke fast track with direct access to neurologist on call, for patients with acute stroke symptoms considered as prehospital candidates for intervention. All patients included in the stroke fast track 2015–2017 have been reviewed in order to validate existing LVO screening tools in a population with acute stroke symptoms of <4.5 hours.
Results
1310 patients were admitted as thrombolysis candidates, 383 received an intervention. About 10% of the total population had LVO detected by CT angiography at admission. 15 existing screening scales were tested with sensitivity ranging from 31–81, specificity 70–96, positive predictive values 26–54 and negative predictive values 93–97.
Conclusions
Screening tools for LVO performed suboptimal in this large unselected population of patients with acute stroke symptoms <4.5 hours. No scale predicted LVO with both high sensitivity and high specificity. Health care systems that use LVO prediction instruments for triage will miss some patients with LVO.
Trial registration number
N/A
AS06-119
DOES SECONDARY TRANSFER FOR THROMBECTOMY IMPACT SIGNIFICANTLY THE OUTCOME OF PATIENTS? RESULTS OF A RETROSPECTIVE OBSERVATIONAL STUDY OF 622 CONSECUTIVE PATIENTS FROM BEGIAN HOSPITALS NETWORKS
1Cliniques Universitaires Saint-Luc, Neurology, Bruxelles, Belgium
2AZGroeninge, Neurology, Kortrijk, Belgium
3UZLeuven, Neurology, Leuven, Belgium
4C.H.U. - Hôpital Civil Marie Curie, Neurology, Charleroi, Belgium
5Université de Liège, Unité de Recherche de Psychologie et Neurosciences Cognitives PsyNCog, Liège, Belgium
6Centre Hospitalier Chrétien, Neurology, Liège, Belgium
Background and Aims
Endovascular thrombectomy in acute ischaemic stroke with proximal occlusion is recognized as the best treatment. It is not known if the patients should be referred directly to the Comprehensive Stroke Center (CSC) or to the nearest Primary Stroke Center (PSC) first.
Methods
We reviewed 622 consecutive acute stroke patients treated by thrombectomy between 2015 and 2017. Each network consists in a CSC and several PSC far of less than 100 kilometers. We considered 6 predictive factors: age, NIHSS on admission, transfer, delay between stroke onset to emergency admission, IV thrombolysis before thrombectomy, delay between symptoms and to recanalization time.
Results
There was a mean delay of 42 minutes between admission to emergencies and recanalization for patients who bypass the PSC (CSC = 107 min, PSC = 149 min; p < 0.001). Good outcome (modified Rankin Score less or equal to 2) did not differ significantly at 3 month of follow up (44,6% in the group from CSC and 53,4% in the group from PSC, p = 0.12). Stepwise logistic regression analysis revealed that iv thrombolysis before thrombectomy is a good predictive factor (p < 0.001).
Conclusions
In hospitals networks where the distances between PSC and CSC are less than 100 km and the delay of thrombectomy does not exceed 45 min, drip & ship has no negative impact on the mRS at 3 months. The only predictive factor of good outcome was iv thrombolysis performed before thrombectomy, which may suggest the usefulness of sending patients to the nearest PSC first.
Trial registration number
N/A
AS06-074
PREDICTORS OF CLINICAL OUTCOME IN BASILAR ARTERY OCCLUSION TREATED BY MECHANICAL THROMBECTOMY, INFLUENCE OF PREVIOUS INTRAVENOUS RECOMBINANT TISSUE-TYPE PLASMINOGEN ACTIVATOR ADMINISTRATION
1Lille University Hospital- INSERM- U1171–Degenerative and Vascular Cognitive Disorders, Department of Neurology- Stroke unit, Lille, France
2Lille University Hospital, Department of Neuroradiology, Lille, France
Background and Aims
Whether previous administration of intravenous r-tPA (IVT) before mechanical thrombectomy (MT) improves clinical course of basilar artery occlusion (BAO) patients is unkown. We aimed to define prognosis factors, including previous IVT, in a cohort of BAO patients treated with MT.
Methods
We prospectively included BAO patients treated by MT who were admitted to Lille University Hospital from 2011 to 2018 and who underwent cerebral MRI as first-line imaging. Multivariate logistic regressions were used to assess the independent influence of IVT and other potential predictors (baseline characteristics and procedural data) on favorable outcome (defined as a modified Rankin scale score 0–2 or similar to the pre-stroke’s one) and on mortality after 3-months.
Results
We included 119 patients (mean age, 62.13 years; 59% had previous IVT before MT). Favorable outcome, successful recanalization and mortality were reached in 33.6%, 64% and 44.5% respectively. IVT prior to MT was independently associated with a 12.7-fold increase chance of favorable outcome and a 78% reduction of mortality rate. Additionally, DWI pc-ASPECTS, smoking and diabetes status were significant predictors of favorable outcome. Mortality predictors were age, weight, clinical severity, systolic blood pressure, time to treatment, absence of complete recanalization and proximal occlusion.
Conclusions
Previous IVT improved functional outcome and survival in BAO patients treated by MT. While waiting for RCT, this result encourages not to avoid IVT before MT. In addition, clinical severity, vascular risk factors, time to treatment, clot location and extent of ischemic lesion were associated with clinical outcome and should be considered for future RCT patients’selection.
Trial registration number
N/A
E-Poster Discussion-Neurointervention I
AS07-083
DIRECT ASPIRATION FIRST PASS TECHNIQUE IS ASSOCIATED WITH SHORTER PROCEDURAL TIMES AND IMPROVED OUTCOMES IN COMPARISON WITH STENT-RETRIEVER THROMBECTOMY IN BASILAR ARTERY OCCLUSION
1Royal Melbourne Hospital- University of Melbourne, Department of Neurology, Parkville, Australia
2University Hospital of “Tor Vergata”, Stroke Unit- Department of Neuroscience, Rome, Italy
3The Florey Institute of Neuroscience and Mental Health- University of Melbourne, The Florey Institute of Neuroscience and Mental Health, Parkville, Australia
4University of Technology, Department of Neurology and Dresden Neurovascular Center, Dresden, Germany
5Sainte-Anne -Hospital, Department of Interventional Neuroradiology, Paris, France
6Royal Adelaide Hospital, Department of Neurology, Adelaide, Australia
7Princess Alexandra Hospital, Division of Medicine, Brisbane, Australia
8Careggi University Hospital- University of Florence, Department of Neurology, Florence, Italy
9IRCCS Neurological Institute C. Mondino and S. Policlinico Matteo, Department of Neurology, Pavia, Italy
10Mount Sinai Hospital, Neurosurgery, New York, USA
11Austin Health, Department of Neurology, Melbourne, Australia
12Royal Melbourne Hospital- University of Melbourne, Department of Radiology, Melbourne, Australia
Background and Aims
The optimal endovascular approach for basilar artery occlusion (BAO) is uncertain. We compared reperfusion and clinical outcomes between the direct aspiration first pass technique (ADAPT) and stent retriever thrombectomy (SRT) in BAO.
Methods
Clinical and procedural data of consecutive endovascular-treated BAO patients from the Basilar Artery Treatment and MANagement (BATMAN) collaboration were retrospectively analysed. Functional independence was defined as modified Rankin Scale (mRS)≤2, excellent outcome as mRS 0–1 at 3 months; successful reperfusion as mTICI 2b-3. Binary and ordinal logistic regression analyses adjusted for age and baseline NIHSS were performed.
Results
We included 200 BAO patients [93 treated with first-line ADAPT and 107 with SRT or combined approach (“Solumbra technique”)]. Mean age was 68y (SD 14), median NIHSS 19 (IQR 7–32) and median procedural time 73min (IQR 38–106). An additional stent retriever was used in 6/93 (6.5%) patients in the ADAPT group. Although a greater proportion of patients achieved successful reperfusion (ADAPT 87% vs SRT 76%, p = 0.07), this was not statistically significant. Procedural times were shorter in the ADAPT group [47min (IQR 30–73) vs SRT 94min (IQR 65–131);p < 0.001)]. Excellent outcomes were more frequent in ADAPT-treated patients (34% vs 20%, adjusted OR = 2.8, 95%CI 1.3–6.3, p = 0.01). Functional independence occurred in 56% ADAPT vs 44% SRT, adjusted OR = 2.3, 95%CI 1.1–4.7;p = 0.03 and outcomes in ordinal shift were improved in the ADAPT group (common-OR = 2.0, 95%CI 1.1–3.5;p = 0.01).
Conclusions
ADAPT is associated with shorter procedural times and improved outcomes in comparison with SRT in BAO. Randomized controlled trials to determine the optimal endovascular technique are warranted.
Trial registration number
N/A
AS07-082
CLINICAL OUTCOME OF ACUTE ISCHEMIC STROKE PATIENTS WITH ARTERIAL TANDEM OCCLUSIONS BY EMERGENT CERVICAL CAROTID APPROACH OF REVASCULARIZATION
1Hospital Universitari Germans Trias i Pujol, Neurosciences, Badalona, Spain
2Hospital Universitari Germans Trias i Pujol, Neurointerventional Unit- Neurosciences, Badalona, Spain
Background and Aims
Carotid stenting in patients with tandem occlusions (cervical internal carotid artery (ICA) and middle cerebral artery), who undergo endovascular treatment (EVT) for acute ischemic stroke (AIS), may have higher risk of symptomatic intracranial haemorrhage (SICH) whereas isolated angioplasty may result in acute reocclusion of residual stenosis.
Methods
We retrospectively reviewed a prospective registry of AIS patients undergoing EVT for tandem occlusions over a 10-year period. We compared clinical [early neurological deterioration (END) as a decline of ≥4 points in NIHSS at 24h and poor outome as a mRS >2 at 3m] and neuroimaging outcomes [ICA reocclusion and SICH at 24 hours] between patients with and without acute carotid stenting.
Results
Out of 641 patients with anterior large artery occlusions who received EVT, 107 had tandem occlusions, of which 95 underwent intracranial thrombectomy. Two groups of patients were defined according to cervical carotid type of revascularization: (1) carotid stenting group (CS): emergent stenting+/-angioplasty (30/95, 31.6%) (2) non-carotid stenting group (NCS): angioplasty, aspiration or nothing (65/95, 68.4%). Emergent stenting was independently associated with a lower risk of early ICA reocclusion (OR 0.11 95%IC [0.02–0.54]) and higher risk of SICH (OR 20.76 95%IC [1.38–312.61]) compared to NCS group. No differences were observed on END (OR 2.00 95%IC [0.37–10.63]) or poor outcome (OR 0.34 95%IC [0.12–1.14]) between groups.
Conclusions
Reocclusion of cervical ICA was lower and SICH higher after EVT for tandem occlusion when thrombectomy was combined with ICA stenting. However, this did not result in significantly poorer early or late clinical outcome.
Trial registration number
NA
AS07-051
INFLUENCE OF THE EXPERIENCE OF THE STROKE CENTER ON RECANALIZATION AND PROGNOSIS OF ANTERIOR CIRCULATION STROKE PATIENTS UNDERGOING MECHANICAL THROMBECTOMY. DATA FROM THE NORDICTUS REGISTRY
1INIBIC/CHUAC, Department of Neurology, A Coruña, Spain
2Hospital Marqués de Valdecilla, Department of Neurology, Santander, Spain
3Hospital Clínico Valladolid, Department of Neurology, Valladolid, Spain
4Hospital de Donostia, Department of Neurology, Donostia, Spain
5Hospital Central de Asturias, Department of Neurology, Oviedo, Spain
6Hospital de Vitoria, Department of Neurology, Vitoria, Spain
7University Hospital Santiago de Compostela, Department of Neurology, Santiago de Compostela, Spain
8Hospital de Galdakao, Department of Neurology, Vizcaya, Spain
9Hospital de Burgos, Departmen of Neurology, Burgos, Spain
10Hospital Universitario Miguel Servet, Department of Neurology, Zaragoza, Spain
11Hospital de Cruces, Department of Neurology, Bilbao, Spain
12Hospital de León, Department of Neurology, León, Spain
13Complejo Hospitalario de Vigo, Department of Neurology, Vigo, Spain
14Hospital Clínico Universitario Valladolid, Department of Neurology, Valladolid, Spain
Background and Aims
The minimal number of acute ischemic stroke patients needed to be treated in order to be accredited as an interventional neuroradiologist differ among different training programs. We evaluated whether the experience of the tertiary stroke center (TSC) may influence recanalization and prognosis of patients treated with mechanical thrombectomy (MT).
Methods
We retrospectively analyzed data from patients with anterior circulation stroke undergoing MT over a period of 2 years in 13 TSC belonging to the NORDICTUS Spanish stroke network. We collected the total number of MT performed in each center during the first year of data inclusion and analyzed their influence on recanalization (TICI2b/3 vs TICI 0/1/2a), hemorrhagic transformation, good functional outcome (modified Rankin scale ≤2) and mortality at 3 months.
Results
A total of 601 patients (71 ± 13 years, 46% men) were included. TICI2b/3 recanalization rates depended on the number of procedures performed during the first year, so that the greater the number of MTs, the higher the recanalization rates. Percentages of complete recanalization >70% were achieved when centers have performed at least 30 procedures. Performing procedure times, functional dependence and mortality were significantly higher in centers with fewer thrombectomies. A number of MT <30 was independently associated with worse functional prognosis (OR 2.6; 95% CI 1.03–6.56, p = 0.043)
Conclusions
Our data show that the experience of the TSC is an independent prognostic factor in patients undergoing MT. A minimum experience of 30 procedures results in better functional prognosis, so we consider that this number should be taken into account in the accreditation programs.
Trial registration number
N/A
AS07-014
ENDOVASCULAR THROMBECTOMY WITH AND WITHOUT PRIOR INTRAVENOUS THROMBOLYSIS IN ACUTE ISCHEMIC STROKE CAUSED BY BASILAR ARTERY OCCLUSION. RESULTS FROM THE SITS INTERNATIONAL THROMBECTOMY REGISTER
1Karolinska University Hospital, Department of Neurology, Stockholm, Sweden
2Karolinska Institutet, Department of Clinical Neuroscience, Stockholm, Sweden
3Hospital Santo António, Department of Neuroradiology, Porto, Portugal
4Hospital Universitari Germans Trias i Pujol, Stroke Unit, Barcelona, Spain
5Universitat Autònoma de Barcelona, Department of Neurosciences, Badalona, Spain
6Hospital Clínico San Carlos, Stroke Unit. Neurology Department, Madrid, Spain
7Karolinska University Hospital, Department of Neuroradiology, Stockholm, Sweden
8Faculty Hospital Trnava, Department of Neurology, Trnava, Slovak Republic
9Centro Hospitalar Universitário de Lisboa Centra, Stroke Unit, Lisbon, Portugal
10Tampere University Hospital, Department of Neurology, Tampere, Finland
11North Estonia Medical Centre, Department of Neurology, Tallinn, Estonia
12Ospedale Civile S. Agostino Estense- Modena University Hospital, Stroke Unit- Neurology Clinic, Modena, Italy
13University of Modena and Reggio Emilia, Department of Neuroscience, Modena, Italy
14IRCCS Istituto delle Scienze Neurologiche di Bologna, Department of Neurology and Stroke Center- Maggiore Hospital, Bologna, Italy
15Keele University, Institute for Science and Technology in Medicine, Staffordshire, United Kingdom
16Helsinki University Hospital, Department of Neurology, Helsinki, Finland
17Sapienza University of Rome, Department of Human Neurosciences, Rome, Italy
Background and Aims
Evidence is lacking on the safety and outcomes of endovascular thrombectomy (EVT) with and without prior intravenous thrombolysis (IVT) in patients with basilar artery occlusion (BAO). We aimed to compare characteristics, and report outcomes, in BAO patients treated with IVT+EVT and EVT alone.
Methods
We included patients registered in the SITS Thrombectomy Registry 2014–2017, recruited from 40 centers (15 countries) performing routine three months outcome assessment. Clinical, radiological, and workflow characteristics were compared between BAO patients treated with IVT+EVT and EVT alone. Outcomes were SICH, mRS, and death at three months. Outcome differences were not subjected to significance testing due to strongly suspected confounding by indication.
Results
Of 462 BAO patients, 240 (52%) received IVT+EVT, and 222 (48%) EVT alone. Age (69 vs 71 years) and baseline NIHSS (19 vs 15) did not differ significantly. Previous stroke (22.5% vs 8.9%), atrial fibrillation (31.5% vs 18.0%) and baseline OAC use (22.3% vs 5.5%) were significantly more common in EVTonly patients. Onset-to-door (153 vs 78 min), onset-to-groin (330 vs 252 min) and onset-to-recanalisation (418 vs 310 min) times were longer in EVTonly, all p < 0.001. The door-to-groin time was 139 vs 141 min. Outcomes were similar between IVT+EVT and EVTonly: modified SICH SITS-MOST 2.4% vs 2.1%; mRS 0–2 33.9% vs 32.5%; death 35.1% vs 39.5%.
Conclusions
Despite major differences in baseline characteristics, and time to groin puncture and recanalisation, outcomes are similar between patients with BAO receiving EVT+IVT and EVT alone. Efforts to improve workflow for patients with BAO are strongly encouraged.
Trial registration number
N/A
AS07-029
RESTENOSIS AFTER CAROTID ANGIOPLASTY AND STENTING (RECAST) REGISTRY: PREDICTORS AND CLINICAL SIGNIFICANCE
1Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBIS, Interventional Neurorradiology, Seville, Spain
2Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBI, Neurology, Seville, Spain
3Instituto de investigación Biomédica de Sevilla IBiS, Laboratorio de Investigación Neurovascular, Seville, Spain
4Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBI, Interventional Neurorradiology, Seville, Spain
5Hospital Universitario Reina Sofía, Interventional Neurorradiology, Córdoba, Spain
6Hospital Universitario Reina Sofía, Neurology, Córdoba, Spain
7Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
8Hospital Universitario Central de Asturias, Interventional Neurorradiology, Oviedo, Spain
9Hospital Universitario Virgen Macarena/Instituto de Biomedicina de Sevilla IBiS, Neurology, Seville, Spain
Background and Aims
Carotid angioplasty and stenting (CAS) long term benefit, can be reduced by complications related to intra-stent restenosis. Our aim was to identify independent risk factors and clinical significance of restenosis ≥ 70%.
Methods
A national prospective multicenter registry was carried out between January-2015/December-2017. Patients with symptomatic or asymptomatic carotid stenosis who underwent carotid angioplasty with/without stent were included. Minimum required follow-up (performed by ultrasonography) was 6 months. Maximum residual post-procedure stenosis was 40%. Demographic, clinical and radiological data were collected.
Results
Three hundred and eighty five patients were included (75.8% Male, 70 years old median age). Most of them were symptomatic (70.6%). Stent was employed in 94% (360). Restenosis ≥ 70% rate was 9.9% (38). In the univariate analysis, peripheral vasculopathy (p < 0.001), chronic kidney disease (p = 0.042), asymptomatic patients (p = 0.035), absence of anterior communicating artery (ACoA) (p = 0.018), existence of pial collateral circulation (p = 0.06), right internal carotid artery treatment (p = 0.042), no stent use (p < 0.001), impaired vasoreactivity (p = 0.002) and prior 50% restenosis (p < 0.001) were related to the development of ≥ 70% restenosis. Peripheral vasculopathy [HR 3.4(95% CI 1.6–7.2);p = 0.001] and existence of pial collateral circulation [HR 3.2(95% CI 1.3–7.7);p = 0.009] were identified as independent predictors of ≥ 70% restenosis respectively. ≥ 70% restenosis was related to ipsilateral stroke within first 12 months after procedure (22.2% vs 1.9%;p < 0.001).
Conclusions
Carotid restenosis after CAS is associated with ipsilateral stroke occurrence. In our sample, Peripheral vasculopathy and existence of pial collateral circulation identify patients at high risk of restenosis.
Trial registration number
N/A
E-Poster Discussion-Imaging
AS11-021
THE DEGREE TO WHICH ISCHEMIC STROKE AFFECTS NETWORK HUBS PREDICTS COGNITIVE RECOVERY
1Elisabeth Tweesteden Hospital, Department of Neurology, Tilburg, The Netherlands
2University Medical Center Utrecht, Department of Neurology and Neurosurgery, Utrecht, The Netherlands
3Unversity Medical Center Groningen, Department of Clinical and Experimental Neuropsychology, Groningen, The Netherlands
4University Medical Center Utrecht, Department of Rehabilitation- Physical Therapy Science & Sports, Utrecht, The Netherlands
Background and Aims
It is uncertain what determines the potential for cognitive recovery after ischemic stroke. The extent to which strategic areas of the brain network, so-called hubs, are affected could be a key factor. We developed a ‘lesion impact score’, which estimates damage to network hubs by integrating information on the stroke lesion with the topology of healthy brain networks. We verified whether the lesion impact score indeed reflects global network disturbances in patients, and hypothesized that it could predict cognitive recovery.
Methods
Seventy-five ischemic stroke patients with cognitive dysfunction during hospitalization were included. A brain MRI and neuropsychological assessment were performed 3–6 weeks after stroke. Neuropsychological testing was repeated after one year to assess cognitive recovery. Brain networks were reconstructed from diffusion-weighted data. Each network consisted of 90 grey matter regions (i.e. network nodes).
The lesion impact score of each node was defined as the product of the ‘hub-score’ and the percentage of node volume affected by the infarct. This percentage was calculated using segmentation of the lesions. The ‘hub-score’ was defined as the average betweenness centrality of each node in a control sample.
Results
A higher lesion impact score was independently related to lower global network efficiency (β = -0.53[-0.78:-0.28], P<0.001). Moreover, the lesion impact score was an independent predictor of cognitive recovery one year after stroke (OR = 0.62[0.39:0.99], P = 0.044).
Conclusions
We introduced a lesion impact score that combines information on lesion size and network topology to predict long-term recovery after stroke. This score can be used in a clinical setting, also without availability of high-resolution diffusion-weighted MRI.
Trial registration number
N/A
AS11-024
BRUSH SIGN IS ASSOCIATED WITH INCREASED SEVERITY IN CEREBRAL VENOUS THROMBOSIS
1Hospital Santa Maria - CHLN- University of Lisbon, Department of Neurosciences and Mental Health Neurology, Lisbon, Portugal
2Hospital Santa Maria - CHLN- University of Lisbon, Department of Neuroradiology, Lisbon, Portugal
3Bern University Hospital Inselspital- University of Bern, Department of Neurology, Bern, Switzerland
4Faculty of Medicine- University of Lisbon, Institute of Anatomy, Lisbon, Portugal
5Bern University Hospital- Inselspital- University of Bern, University Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland
Background and Aims
The “brush sign” (BS) is an abnormally accentuated signal drop of the subependymal and deep medullary veins in paramagnetic-sensitive MR sequences, previously described in acute ischemic stroke. We aimed to describe the BS in patients with thrombosis of the cerebral veins and sinuses (CVT) and explore its association with clinical severity, thrombosis extent, parenchymal brain lesion and prognosis.
Methods
We assessed consecutive adult patients admitted to two university hospitals with diagnosis of acute CVT and imaging assessment with MRI, including paramagnetic-sensitive sequences. Demographics, imaging findings, clinical presentation and functional outcomes were compared between patients with and without BS.
Results
In the 118 patients included, BS was observed in gradient-echo T2*-weighted (T2*WI) in 16% and susceptibility-weighted imaging (SWI) in 13% of cases. All patients with BS had thrombosis of the superior sagittal sinus, the straight sinus or the deep venous system. BS was associated with ipsilateral parenchymal lesion (odds ratio [OR] 6.4, 95%CI 1.9–21.1; p = 0.002) and higher thrombus load (median [IQR] 5 (4-6) versus 2 (2-4); p < 0.0001). BS was also associated with focal neurological signs (OR 4.2; 95%CI 1.4–12.7, p = 0.01). The functional outcome at 3 months was not significantly different in patients with BS.
Conclusions
BS in T2*WI and SWI was observed in approximately one in seven acute CVT patients. BS was significantly associated with ipsilateral parenchymal brain lesion, extent of thrombosis and focal neurological signs related with CVT. This suggests that BS can represent a marker of severity in CVT.
Trial registration number
N/A
AS10-063
BLOOD-BRAIN-BARRIER LEAKAGE AND REPERFUSION INJURY: RESULTS FROM THE REPERFUSION INJURY IN ISCHEMIC STROKE (RISK) STUDY
1AOU Careggi, Stroke Unit, Florence, Italy
2University of Florence, Department of Neuroradiology, Florence, Italy
3AOU Careggi, Neuroradiology, Florence, Italy
4University of Florence, NEUROFARBA Department, Florence, Italy
5University of Florence, Atherothrombotic disease Center, Florence, Italy
6University of Florence, Neurovascular Interventional Unit, Neurovascular Interventional Unit, Italy
7AOU Careggi, Neurovascular Interventional Unit, Florence, Italy
8AOU Careggi, Emergency Department, Florence, Italy
Background and Aims
In patients with acute ischaemic stroke treated with acute therapy, we aimed to evaluate whether pre-treatment blood-brain-barrier (BBB) leakage is associated with reperfusion injury (RI).
Methods
We prospectively enrolled patients with acute ischaemic stroke treated with intravenous thrombolysis and/or endovascular treatment. Before acute treatment, each patient received Computed Tomography (CT), angio-CT, and CT perfusion. We assessed pre-treatment BBB leakage within the ischaemic area with CT perfusion by using Ktrans. RI was defined as haemorrhagic infarction type 2 or parenchymal haemorrhage type 1 or 2. We evaluated independent associations between BBB leakage and RI with logistic regression adjusting for age, sex, baseline stroke severity and onset to treatment time.
Results
We enrolled 166 patients with available assessment of BBB leakage, mean ( ± SD) age 74.9 ( ± 12.4) years, 84 (51%) males, and median (IQR) National Institutes of Health Stroke Scale of 18 (12-23). A total of 29 (17%) patients received intravenous thrombolysis, 101 (61%) underwent endovascular treatment, 36 (22%) both. RI occurred in 28 (17%) patients, mean BBB leakage was higher in patients with RI (0.81 vs 0.60; p = 0.011). After adjustment in the logistic regression model, we found that BBB leakage was independently associated with RI (OR = 2.93; 95% CI = 1.13–7-62).
Conclusions
Higher BBB leakage was associated with reperfusion injury after acute stroke treatment. Our results need external validation, but suggest that assessment of pre-treatment BBB leakage may help to identify patients at risk of haemorrhagic transformation.
Trial registration number
N/A
AS11-042
PREDICTING OUTCOMES FROM INFARCT LOCATION: VOXEL-BASED LESION SYMPTOM MAPPING VS. MACHINE LEARNING METHODS
1Methinks, Medical Imaging, Barcelona, Spain
2Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
Background and Aims
In addition to infarct volume, the lesion of specific brain areas may have greater prognostic consequences after stroke. We compared the prognostic value of three different advanced imaging methods that analyze the lesion distribution in stroke patients.
Methods
In a cohort of patients with ischemic stroke studied with MRI (n = 195), we studied the prognostic consequences (poor outcome defined as mRS>2 at three months) of lesion location. We used voxel-based lesion-symptom mapping (VLSM) and two machine learning-based methods to extract features for a random forest classifier: 1/Clustering of regions in the brain with the K-means method; 2/Deep learning autoencoder. We compared the anatomic distribution in VLSM maps and the k-means regions, and we analyzed the predictive value of the three methods.
Results
Several brain areas (mainly in the left hemisphere) were associated with poor functional outcome in VLSM. The clustering method resulted in 10 distinct brain areas with different prognostic value. The majority (83%) of the voxels identified by VLSM were located within the cluster with the highest capacity to predict poor outcome. The predictive capacity (AUC) of the five random forest analyses were in increasing order: clinical variables (0.75), lesion volume (0.83), VLSM (0.83), clustering (0.85), and deep learning method (0.89).
Conclusions
The similarities between VLSM and machine learning methods in the study of the prognostic consequences of specific brain areas suggest that image-based tools may offer reliable prognostic information. Deep-learning methods may increase the predictive capacity of these tools.
Trial registration number
N/A
AS11-052
INTRACRANIAL VESSEL WALL MR IMAGING TO IDENTIFY THE ETIOLOGY OF ISCHEMIC STROKE IN THE YOUNG – A PROSPECTIVE STUDY
1University Health Network - University of Toronto, Medicine - Div. of Neurology - Stroke Program, Toronto, Canada
2University Health Network - University of Toronto, Department of Medical Imaging - Div. of Neuroradiology, Toronto, Canada
Background and Aims
To determine the additional diagnostic yield of intracranial vessel wall MRI (VW-MRI) compared with standard work-up for identifying stroke etiology in young patients.
Methods
For this prospective single-center observational study, we recruited consecutive patients presenting with ischemic stroke, under age 55 years, between 2015 and 2018. In addition to the standard-of-care stroke work-up, we performed 3-Tesla contrast-enhanced VW-MRI. A multidisciplinary panel of stroke experts reviewed the conventional investigations (parenchymal and vascular imaging, laboratory results, and cardiac work-up) to reach consensus on stroke etiology and optimal treatment. The panel then reviewed the VW-MRI and reached consensus on whether this altered stroke etiology and/or treatment. We compared the proportions of patients for each stroke etiology before and after VW-MRI using two-sided McNemar’s test.
Results
We recruited 102 patients: 44/102 (43%) women, median age 48 (IQR: 42–54). Stroke etiology based on conventional work-up was changed after reviewing VW-MRI in 36/102 patients (35%, 95%CI:27-45%). In 17/29 patients (59%) with undetermined stroke etiology on standard work-up, a cause was identified on VW-MRI (p < 0.001). In 16/17 patients, suspected intracranial atherosclerosis on conventional imaging was confirmed with VW-MRI though 18 additional patients were diagnosed with intracranial atherosclerosis on VW-MRI (p < 0.0001). The decision on treatment was changed in 18/102 patients after reviewing VW-MRI (18%, 95%CI:11-26%).
Conclusions
In unselected young ischemic stroke patients, the suspected stroke etiology and subsequent treatment may be modified based on VW-MRI in up to a third of cases. This has diagnostic and therapeutic implications for institutes choosing to implement this newer technique.
Trial registration number
N/A
E-Poster Discussion-Rare Causes and Case Reports I
AS23-050
WHAT CAN HEALTH-ADMINISTRATIVE DATASETS TELL US ABOUT PAEDIATRIC STROKE?
1Agency for Health Quality and Assessment of Catalonia, Stroke Programme, Barcelona, Spain
2Agency for Health Quality and Assessment of Catalonia, Public Data Analysis for Health Research and Innovation Program PADRIS, Barcelona, Spain
Background and Aims
Paediatric stroke is a great unknown due to its low frequency and lack of high-quality registry data. Health-administrative datasets (HAD) may be an alternative source of information. Objective: To describe frequency, subtypes and outcomes after paediatric stroke using HAD.
Methods
Based on a selection of ICD9 diagnostic codes, we identified a cohort of paediatric (<18y) strokes (ischaemic, haemorrhagic and non-symptomatic vascular lesions) using the Minimum Basic Dataset of acute-care hospital admissions (Catalonia, 2007–2017). We defined index and recurrent events (>30d from index admission), and readmissions (≤30d of index event). Retrieved data includes date of admission/discharge, age, sex, discharge facility, therapeutic and diagnostic procedures. Survival was obtained from the Central Registry of Insured Persons (7.5M) as of December 2018.
Results
788 strokes (58.1% men) were identified (index events: 553, recurrent strokes: 235) of which 203 cerebral bleedings, 279 ischaemic strokes, and 306 non-symptomatic vascular lesions. Overall incidence ranged from 2–4/100,000 paediatric inhabitant-years. Median age was 9 years (range: 4–14). A peak of incidence is seen in <12 months-old babies, particularly among cerebral bleedings. Overall, 3.1% died during hospitalisation (7.4% among bleedings), and 90% were discharged home. Kaplan-Meier curves show significant differences by diagnosis, with bleedings showing poorest survival by time. Half of deaths occur during long-term follow-up. No information on functional status could be retrieved.
Conclusions
HAD offer valid, population-based data that confirm previously published incidence in other European settings. However, long-term functional status is typically absent making enrichment with granular data from other sources necessary.
Trial registration number
N/A
AS23-010
ABDOMINAL OBESITY INCREASES THE RISK OF CRYPTOGENIC ISCHEMIC STROKE IN YOUNG ADULTS: THE SECRETO STUDY
1Helsinki University Hospital, Department of Neurology, Helsinki, Finland
2Kuopio University Hospital, Neuro Center, Kuopio, Finland
3Turku University Hospital- University of Turku, Division of Clinical Neurosciences, Turku, Finland
4University Medicine, Department of Neurology, Greifswald, Germany
5Haukeland University Hospital- Istanbul University, Department of Neurology, Bergen, Norway
6Istanbul Faculty of Medicine, Department of Neurology, Istanbul, Turkey
7Azienda Unità Sanitaria Locale - IRCCS di Reggio Emilia, Neurology Unit, Reggio Emilia, Italy
8Oulu University Hospital, Department of Neurology, Oulu, Finland
9Tampere University Hospital, Department of Neuroscience and Rehabilitation, Tampere, Finland
10Hospital de Santa Maria- University of Lisbon, Department of Neurosciences Neurology, Lisbon, Portugal
11The Sahlgrenska Academy at University of Gothenburg- Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
12Radboud University Medical Center, Neurology, Nijmegen, The Netherlands
Background and Aims
Recent epidemiologic studies suggest concomitant increase in the prevalence of obesity and incidence of ischemic stroke at younger ages. The contribution of obesity in these early-onset strokes is not well established. We studied the association of different obesity metrics with acute cryptogenic ischemic stroke (CIS).
Methods
Ongoing prospective multi-center case-control study enrolling patients aged 18–49 with imaging-positive acute CIS and age- and sex-matched stroke-free controls (NCT01934725). Obesity metrics included body-mass index (BMI) as well as waist circumference (WC) and waist-to-hip ratio (WHR). We used conditional logistic regression, analyzed obesity metrics in tertiles, and adjusted for cigarette smoking, excessive alcohol consumption, low physical activity, diabetes, hypertension, and combined oral contraceptive use.
Results
A total of 213 patient-control pairs were analyzed. WC and WHR were higher in stroke patients compared with healthy controls, emphasized by the difference in upper tertiles (WC, 42.3% vs 30.0%; WHR, 39.0% vs 33.3%). No difference in BMI emerged between the groups. Abdominal obesity was an independent risk factor for CIS in a multivariate analysis: WC (odds ratio 3th tertile vs 1st tertile, 2.01, 95% confidence interval 1.05–3.88) and WHR (3th tertile vs 1st tertile, 2.20, 1.10–4.39; 2nd tertile vs 1st tertile, 2.03, 1.10–3.74).
Conclusions
An increased WC and even a moderately increased WHR were associated with CIS in young adults, independent of comorbid conditions. Mechanisms of this association deserve in-depth studies.
Trial registration number
N/A
AS23-006
FREQUENCY OF FABRY DISEASE AND RISK FACTORS OF YOUNG ADULT STROKE IN JAPAN
1Fuji City General Hospital, Neurology, Fuji- Shizuoka, Japan
2The Jikei University School of Medicine, Neurology, Minato- Tokyo, Japan
3Nippon Medical School, Neurology, Bunkyo- Tokyo, Japan
4Institute of Brain and Blood Vessels- Mihara Memorial Hospital, Stroke Medicine, Isesaki- Gunma, Japan
5Yokohama Rosai Hospital, Neurology, Yokohama- Kanagawa, Japan
6Tokyo Metropolitan Tama Medical Center, Neurology and Stroke Medicine, Fuchu- Tokyo, Japan
7Japanese Red Cross Okayama Hospital, Stroke Medicine, Okayama, Japan
8Kobe City Medical Center General Hospital, Neurology, Kobe- Hyogo, Japan
9Juntendo University School of Medicine, Neurology, Bunkyo- Tokyo, Japan
10NTT Medical Center Tokyo, Cerebrovascular Medicine, Shinagawa- Tokyo, Japan
Background and Aims
Young adult stroke has different risk factors and causes compared to elderly populations. Fabry disease (FD) is one of important causes for ischemic stroke (IS) in young adult, but the frequency of FD among IS is still debated. Herein, we aimed to clarify the frequency of FD and risk factors of young adult stroke in Japan patients.
Methods
We prospectively enrolled patients age 16 to 55 with IS from 37 clinical stroke centers in Japan. Participants were categorized by age into younger-aged group (ages 16–44 years), middle-aged group (ages 45–50 years), and elder-aged group (ages 51–55 years). The clinical characteristics of the 3 groups were compared. FD screening was conducted by measuring alpha-galactosidase A (α-Gal A) activity and the concentration of globotriaosylsphingosine (Lyso-Gb3) in plasma.
Results
We enrolled 520 patients (383 men, median age of onset: 48 years). FD screening was conducted in 318 patients in this study. The frequency of hypertension (HT), diabetes mellitus (DM) and dyslipidemia (DL) were significantly higher in the elder-aged group (n = 180), the middle-aged group (n = 180) than that in the younger-aged group (n = 160) (HT 62%, 58% versus 41%, P < .001; DM 29%, 20% versus 10%, P = 0.01; DL 54%, 47% versus 36%, P = 0.03). Only one male patient (0.3%) had low α-Gal A activity and high level of Lyso-Gb3.
Conclusions
Our study showed the frequency of FD was 0.3% in young adult stroke patients with IS. Risk factors for stroke tended to significantly elevate in accordance with ages.
Trial registration number
N/A
AS23-064
ASPIRIN IS EQUIVALENT TO ANTICOAGULANTS FOR PREVENTING RECURRENT EVENTS IN PATIENTS WITH ANTIPHOSPHOLIPID ANTIBODIES FOLLOWING AN INITIAL STROKE/ARTERIAL THROMBOEMBOLIC EVENT: SYSTEMATIC REVIEW/META-ANALYSIS
1SUNY Downstate Medical Center, Neurology, Brooklyn, USA
2RTI International, Biostatistics and Epidemiology, Research Triangle Park, USA
3McMaster University, Medicine, Hamilton, Canada
4Barbara Volcker Center for Women and Rheumatic Diseases, Rheumatology, New York, USA
5Centre de recherche du CHU de Quebec - Universite Laval, Medicine - Rheumatology, Quebec CIty, Canada
6University of Washington Medical Center, Medicine - Hematology, Seattle, USA
7Duke University Medical Center & Duke Clinical Research Institute, Biostatistics and Bioinformatics, Durham, USA
8Duke University Medical Center, Medicine Hematology and Pathology, Durham, USA
Background and Aims
Patients with thromboembolic events (TE) and elevated antiphospholipid antibody (aPL+) have a high risk for recurrent TE. Optimal treatment after a first arterial TE (ATE) is unknown. Aim: Determine in aPL+ patients and initial ATE (predominantly stroke) the recurrent TE risk on antiplatelet (AP) or anticoagulant (AC) therapy.
Methods
Search in PubMed, CINAHL, Cochrane, and EMBASE using terms for the condition, outcomes of interest and therapies (Jan 1990 - Aug 2018). Inclusion criteria: prospective trials or cohort studies investigating patient with initial ATE and aPL+. Excluded studies: no estimated recurrence rates, no specification if incident event was ATE or venous, or included patients with multiple events, case studies/small series. We used systematic review methodology (Cochrane, Evidence-based Practice Centers). Two-year summary rates were estimated using a random effects model. Risk of bias was assessed. High risk of bias studies were excluded.
Results
Five studies were included. The two-year proportion for recurrent TE (including TIAs) in patients on AC = 0.231 (95% CI: 0.162, 0.318) with 108 events in 430 patients; the two-year proportion for patients on AP = 0.216 (95% CI: 0.177, 0.261) with 80 events in 370 patients. Data was similar excluding TIA outcome.
Conclusions
aPL+ patients with initial stroke/ATE have a risk of recurrent TE on AC similar but slightly higher than the risk on AP. Our data do not support the recommendation for AC to prevent recurrent TE in aPL+ patients with an initial stroke/ATE. A phase 3 randomized trial, Anticoagulation Discontinuation in Patients with Antiphospholipid Syndrome (ADAPS), is planned.
Trial registration number
N/A
AS23-009
RISK OF RECURRENT ISCHEMIC STROKE IN YOUNG CRYPTOGENIC PATIENTS WITH EMBOLIC STROKE OF UNDETERMINED SOURCE
1Palacký University Hospital, Comprehensive Stroke Center- Department of Neurology, Olomouc, Czech Republic
2Palacký University Hospital, Department of Cardiology, Olomouc, Czech Republic
3Palacký University Medical School, Department of Biophysics and Statistics, Olomouc, Czech Republic
Background and Aims
In young patients, cause of ischemic stroke (IS) remains very often cryptogenic and thus effectiveness of secondary prevention may be uncertain. Elderly cryptogenic IS patients (CIS) with ESUS (Embolic Stroke of Undetermined Source) have higher risk of recurrent IS (RIS). The aim was to compare risk of RIS between ESUS and other CIS patients < 50 years.
Methods
The study set consisted of young acute IS patients < 50 years enrolled in the prospective HISTORY (Heart and Ischemic STrOke Relationship studY) study registered on ClinicalTrials.gov (NCT01541163). In all patients, brain ischemia was confirmed on CT or MRI. Admission ECG, serum specific cardiac and thrombophilia markers, neurosonology, TEE, 24-hour and 3-week ECG-Holter were performed to assess cause of IS according to the ASCOD classification.
Results
Of 279 enrolled patients < 50 years (153 males, mean age 41.1 ± 7.8 years), 199 (71%) were identified as cryptogenic and 106 (59 males, mean age 40.7 ± 7.5 years) fulfilled ESUS criteria. During the follow-up with median of 17 months, two (2%) ESUS and 4 (4%) other CIS patients suffered from RIS (p = 0.421). The mean time to RIS did not differ between both groups (14 vs. 27 months, p = 0.248). One-year risk of RIS was 0 for ESUS and 0.025 (95% CI: 0–0.059) for other CIS patients (p = 0.248).
Conclusions
The risk of RIS was very low and did not differ between ESUS and other CIS patients. Acknowledgment: Supported by the grant of Ministry of Health of Czech Republic n. 17–30101A, and by the grant IGA LF UP_008_2019.
Trial registration number
N/A
E-Poster Discussion-Haemorrhagic Stroke I
AS24-017
VARIATION OVER TIME IN RISK FACTORS ASSOCIATED WITH DEATH AFTER INTRACEREBRAL HAEMORRHAGE: PROSPECTIVE COHORT STUDY
1UCL Queen Square Institute of Neurology, Stroke Research Centre- Department of Brain Repair and Rehabilitation, London, United Kingdom
2University College London, Department of Statistical Science, London, United Kingdom
3University College London, Haemostasis Research Unit- Department of Haematology, London, United Kingdom
4UCL Queen Square Institute of Neurology, Lysholm Department of Neuroradiology and the Neuroradiological Academic Unit- Department of Brain Repair and Rehabilitation, London, United Kingdom
5University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
6University of Liverpool, Liverpool Centre for Cardiovascular Science, Liverpool, United Kingdom
7UCL Queen Square Institute of Neurology, Department of Molecular Neuroscience, London, United Kingdom
8University of Glasgow, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
Background and Aims
The risk of death and other outcomes in the short term (6 months) following intracerebral haemorrhage are well known, but less is known about the longer term (beyond 6 months). Our aim was to evaluate whether the impact of different factors associated with death after intracerebral haemorrhage vary with time.
Methods
We included patients recruited to the multicentre prospective observational CROMIS-2 ICH study. Death data were collected from patient and general practitioner questionnaires (first 6 months) and official death registrations (thereafter). Death was defined as “early” if occurring within 6 months of study entry, and “later” if occurring after this time point.
Results
We included 1094 patients, and there were 306 deaths (absolute event rate 11.7 per 100 patient-years, 95% CI 10.5 to 13.1 per 100 patient-years; Figure). Early and later death were associated with different baseline factors (Table). In multivariable analyses, early death was independently associated with age at study entry, history of hypertension, pre-event mRS, admission NIHSS, and haemorrhage volume > 60ml, whereas later death showed independent associations with age, pre-event mRS, anticoagulant use prior to ICH and the presence of intraventricular extension (Table). Hazard ratios for APOE ε2, GCS, NIHSS, and haemorrhage volume > 60ml showed significant change between early and later periods (Table).

Conclusions
We provide new evidence that the factors associated with mortality after intracerebral haemorrhage vary with time; this information could help design better prognostic scores for later death and identify modifiable risk factors that could improve long term outcomes for these patients.
Trial registration number
https://clinicaltrials.gov; NCT02513316
AS24-050
ORAL ANTICOAGULANT RELATED INTRACEREBRAL HEMORRHAGES (ICH) AND TRENDS IN SALE OF ORAL ANTICOAGULANTS (OAC) – RESULTS FROM THE COOL-ICH STUDY
1Bispebjerg Hospital, Department of Neurology, Copenhagen, Denmark
2Nordsjællands Hospital, Department of Neurology, Hillerød, Denmark
3Herlev and Gentofte Hospital, Department of Neurology, Herlev, Denmark
4Rigshospitalet, Department of Neurology, Copenhagen, Denmark
5Rigshospitalet, Department of Neurosurgery, Copenhagen, Denmark
6Bispebjerg Hospital, Department of Radiology, Copenhagen, Denmark
7Klinikum Frankfurt Höchst, Department of Neurology, Frankfurt, Germany
8Heidelberg University Hospital, Department of Neurology, Heidelberg, Germany
Background and Aims
Non-vitamin-K oral anticoagulants (NOAC) have become first choice in OAC instead of Vitamin-K antagonists (VKA) especially based on lower risk of ICH related to NOACs in clinical trials. We aimed to determine the annual use of OAC based on sale of individual drugs and incidence of ICH related to NOAC or VKA in a population-based cohort since NOACs were introduced.
Methods
The study was based on the population in the Capital Region of Denmark (1.8 million inhabitants). All patients presenting with a non-traumatic ICH while on an OAC from 2010–17 were included into this consecutive cohort. All patient data was validated through medical charts. Sold defined daily dosis (DDD) of OAC was retrieved through the Registry of Medicinal Product Statistics (www. Medstat.dk). R version 3.5.1 was used in data analysis. The study was approved by the Danish Data Protection Agency (2012-58-0004) and by the Danish Patient Safety Authority (3-3013-2102/1).
Results
A total of 453 patients with OAC-ICH was identified. Incidence rate of OAC-ICH increased from 2.79 to 4.47 per 100,000 person-years from 2010 to 2017. Sale of OAC increased from 7.7 to 17 DDD/1,000 inhabitants/day from 2010 to 2017.
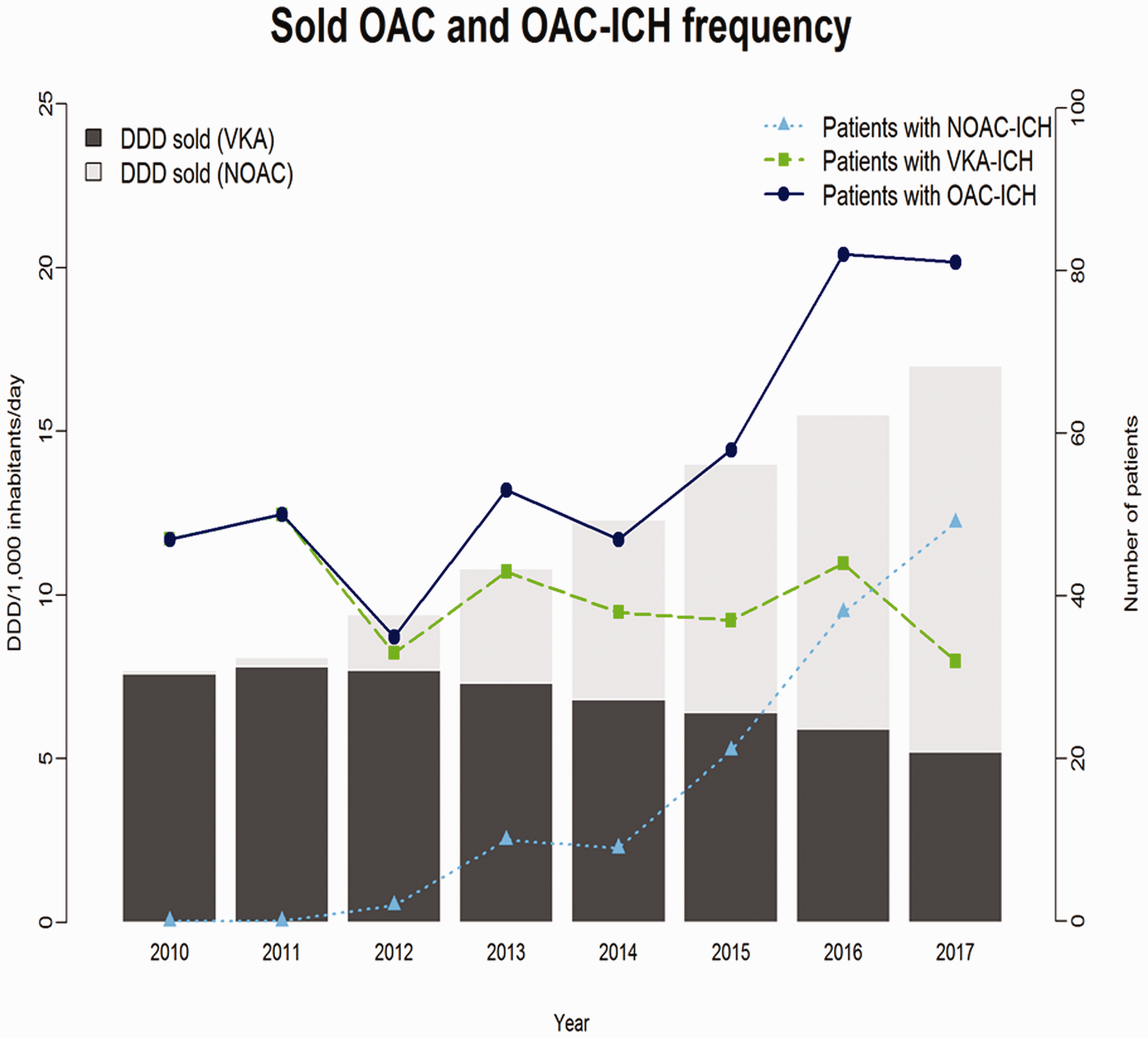
Conclusions
Incidence of OAC-ICH has increased by about 1/3 but use of OAC has more than doubled. NOAC is now the most sold OAC as well as related to more ICH-events than VKA.
Trial registration number
N/A
AS24-041
BASELINE IL-6 LEVELS ARE ASSOCIATED WITH MIDLINE SHIFT AND FUNCTIONAL OUTCOME IN SPONTANEOUS INTRACEREBRAL HEMORRHAGE: AN EXPLORATORY ANALYSIS OF THE FAST TRIAL
1Yale University School of Medicine, Neurology, New Haven, USA
2Brigham and Women’s Hospital, Neurology, Boston, USA
3Massachusetts General Hospital, Neurology, Boston, USA
4Barrow Neurological Institute, Neurobiology, Phoenix, USA
5Henry Ford Hospital, Neurology, Detroit, USA
6Klinikum Frankfurt Höchst, Neurology, Frankfurt, Germany
Background and Aims
Interleukin-6 (IL-6), a proinflammatory cytokine, is an established biomarker in acute brain injury, but the clinical significance of IL-6 in spontaneous intracerebral hemorrhage (ICH) has not been well studied. We aim to determine whether IL-6 levels are associated with secondary injury and functional outcome after ICH in a clinical trial cohort.
Methods
We performed an exploratory analysis of the recombinant activated factor VII for acute ICH (FAST) trial. Patients with baseline serum IL-6 levels were included. Regression analyses were used to assess the associations between IL-6, 24-hour midline shift, and 90-day modified Rankin scale (mRS).
Results
Of 841 enrolled patients, 557 (66%) had baseline IL-6 levels (mean age 64 [SD 13], female sex 203 [37%) and were included. ICH location was deep in 437 (78%) patients and lobar in 78 (22%). IL-6 levels were associated with ICH volume (b 0.26; 95% CI 0.17- 0.35; p < 0.001) and were higher in patients with lobar versus deep ICH (7.4 ng/L [IQR 10.1] vs 4.0 ng/L [IQR 5.1]; p = 0.004). IL-6 was associated with midline shift (b 0.40; 95%CI 0.10–0.69; p = 0.009) after adjustment for ICH volume. IL-6 was associated with worse mRS (OR 1.43; 95% CI 1.22–1.69; p = 0.001) after adjustment for age, sex, ICH volume, GCS, intraventricular hemorrhage, hematoma expansion, location, and treatment. Treatment was not associated with IL-6 or outcome.
Conclusions
In the FAST trial population, baseline IL-6 levels were associated with 24-hour midline shift and functional outcome. These results warrant further investigation of IL-6 as a biomarker for secondary injury and outcome after ICH.
Trial registration number
N/A
AS24-043
RISK OF NON-LOBAR INTRACEREBRAL HEMORRHAGE IS GREATEST AT AN EARLY AGE
1University of Cincinnati, Neurology and Rehabilitation Medicine, Cincinnati, USA
Background and Aims
The risk of intracerebral hemorrhage (ICH) due to hypertension (HTN) is well documented. In lacunar stroke, the risk from HTN is highest at an early age. This suggests the first exposure to HTN may be a high risk period for stroke, however this relationship is not clear in ICH. We sought to evaluate if the odds ratio (OR) for non-lobar ICH from HTN was higher in the youngest compared with oldest patients in each race.
Methods
The Ethnic/Racial Variations of ICH (ERICH) study is a prospective multicenter case-control study of ICH among whites, blacks, and Hispanics. Controls matched to cases 1:1 by age ( ± 5 years), sex, ethnicity/race, and metropolitan area were identified by random-digit dialing. Participants were interviewed to determine history of HTN and use of anti-HTN medications. Participants divided into age groups based on ethnicity-specific quartiles (i.e., each ethnicity was divided into quartiles independent of others). Cases in each ethnic/age group were compared to controls using logistic regression (i.e., cases/controls unmatched).
Results
2039 non-lobar ICH cases and 2066 controls were included. ORs were highest in the youngest age quartile for blacks and Hispanics (10.0 for blacks, and 9.60 for Hispanics). Whites had the highest OR (6.8) in the second quartile (58-68). HTN produced a statistically significant (p < .05) elevation in OR in all age groups for Hispanics.
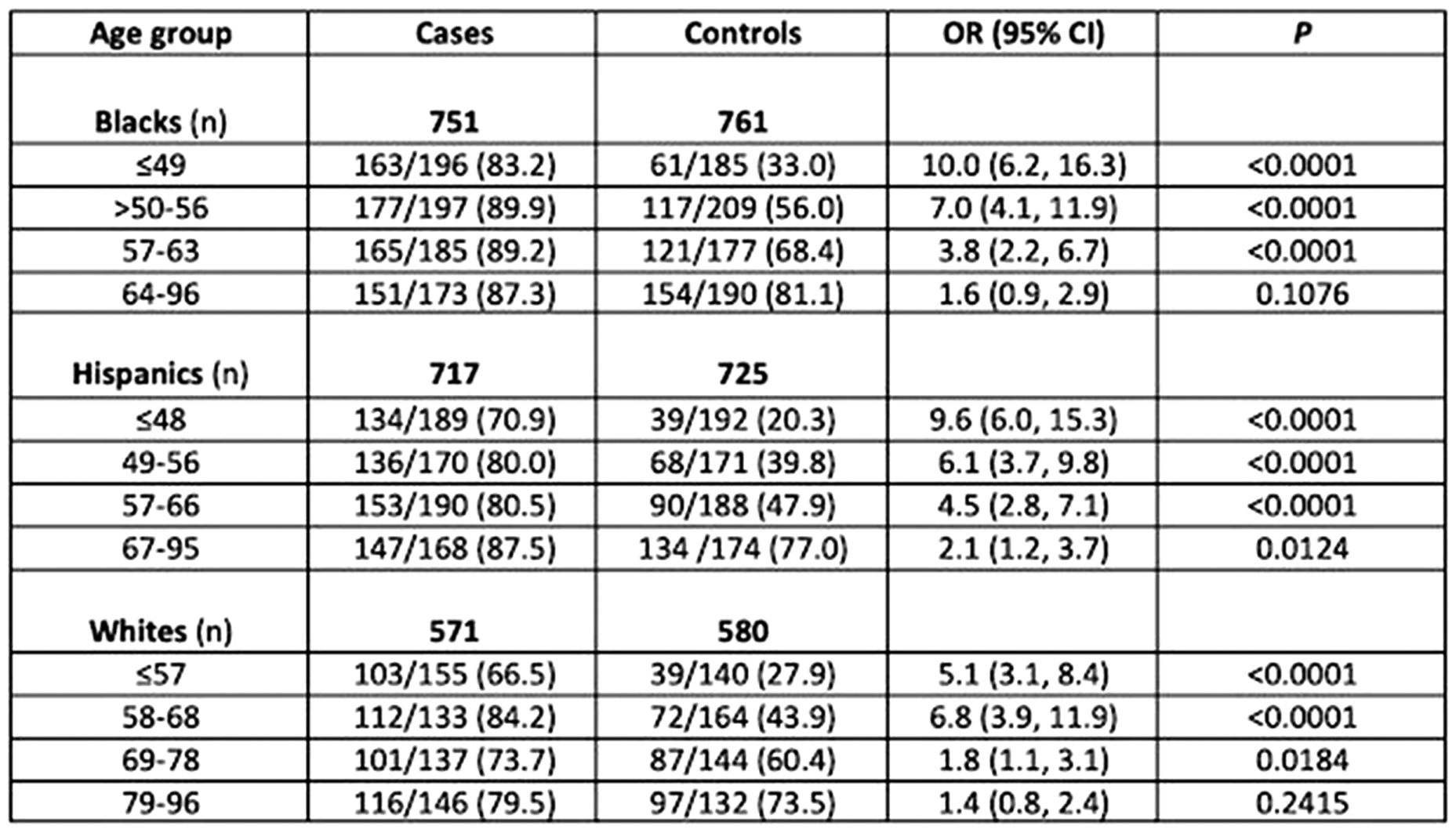
Conclusions
Hypertensive patients are at a higher risk of developing non-lobar, HTN-related ICH at a younger age, which is consistent with the hypothesis that first exposure to HTN is a particularly sensitive time.
Trial registration number
N/A
AS24-023
OPTIMUM PROGNOSTIC CUT-POINT OF BASELINE AND EARLY CHANGE IN NIHSS AND GCS SCORES IN INTRACEREBRAL HEMORRHAGE: INTERACT1 + 2 STUDIES
1The Second Affiliated Hospital of Soochow University, Department of Neurology, Suzhou, China
2The George Institute for Global Health, The George Institute for Global Health, Sydney, Australia
3Royal Prince Alfred Hospital, Department of Neurology, Sydney, Australia
4National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Osaka, Japan
5University of Leicester, Department of Cardiovascular Sciences and NIHR Leicester Biomedical Research Centre, Leicester, United Kingdom
Background and Aims
To determine the optimal cut-point of baseline and early change in National Institutes of Health Stroke Scale (NIHSS) and Glasgow Coma Scale (GCS) scores for outcome prediction in acute intracerebral hemorrhage (ICH).
Methods
Data from participants of the INTERACT trials, where early change in NIHSS and GCS scores were from baseline to 24 hrs. The optimal cut-points for predicting 90-day clinical outcomes (death and dependency on the modified Rankin scale [mRS]) were determined using Youden’s Index and multivariable logistic regression.
Results
In the INTERACT2 trial, baseline NIHSS with a cut-point of 10 was superior to baseline GCS score and early change in GCS and NIHSS scores for predicting death or major disability (sensitivity 77.5%, specificity 69.1%, positive predictive value [PPV] 74.6%, negative predictive value [NPV] 72.4%) within 90-days (aOR, 95%CI 6.4 [5.25–7.81], P<0.001) as well as major disability (sensitivity 74.9%, specificity 42.4%, PPV 55.9%, NPV 76.1%) alone (aOR, 95%CI 4.29 [3.56–5.17]). Early increase in NIHSS score with a cut-point of 1 point optimally predicted death (sensitivity 63.8%, specificity 80.2%, PPV 26.8%, NPV 95.1%) within 90-days (aOR, 95%CI 5.44 [4.05–7.31], P<0.001). Results were consistent in the INTERACT1 database.
Conclusions
In ICH patients, a baseline NIHSS score ≥10 is optimal for predicting bad outcome (death or major disability; major disability), whereas any early increase in NIHSS score predicts death better than baseline NIHSS and GCS scores.
Trial registration number
URL: http://www.clinicaltrials.gov. Unique identifier: (NCT00716079)
E-Poster Discussion-Genetics in Stroke
AS33-030
CIRCULATING MONOCYTE CHEMOATTRACTANT PROTEIN-1 AS A NOVEL RISK FACTOR OF STROKE
1LMU Munich/University Hospital, Institute for Stroke and Dementia Research, Munich, Germany
2Imperial College London, Department of Biostatistics and Epidemiology- School of Public Health, London, United Kingdom
3The University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
4University of Cambridge, Department of Clinical Neurosciences, Cambridge, United Kingdom
5Massachusetts General Hospital MGH, Center for Genomic Medicine, Boston, USA
6Washington University School of Medicine, Department of Neurology- Radiology- and Biomedical Engineering, St. Louis, USA
7RIKEN Center for Integrative Medical Sciences, Laboratory for Statistical Analysis, Yokohama, Japan
8University of Oxford, Clinical Trial Service Unit and Epidemiological Studies Unit- Nuffield Department of Population Health, Oxford, United Kingdom
9University of Virginia School of Medicine, Departments of Neurology and Public Health Sciences, Charlottesville, USA
10Helmholtz Zentrum München - German Research Center for Environmental Health, Institute of Epidemiology, Munich, Germany
11University of Ulm Medical Center, Department of Internal Medicine II-Cardiology, Ulm, Germany
Background and Aims
Circulating cytokines have been implicated in the pathogenesis of vascular disease. We explored whether genetically determined circulating levels of specific cytokines are associated with stroke.
Methods
We selected genetic instruments for 41 cytokines from a genome-wide association study of 8,293 healthy adults and evaluated their associations with stroke and stroke subtypes in MEGASTROKE (67,162 cases; 454,450 controls) applying two-sample Mendelian randomization (MR). UK Biobank was used for validation (4,985 cases; 364,434 controls). Genetic instruments for monocyte chemoattractant protein-1 (MCP-1) were further tested for association with coronary artery disease and myocardial infarction. We used observational data from the longitudinal population-based MONICA/KORA cohort (2,110 individuals; 15.7 years of follow-up) to examine associations between baseline MCP-1 levels and incident stroke.
Results
Genetic predisposition to higher MCP-1 levels was associated with higher risk of any stroke (OR [95%CI] per 1-SD increase = 1.06, [1.02–1.09]), any ischemic stroke (OR = 1.06, [1.02–1.10]), large artery stroke (OR = 1.19, [1.09–1.30]) and cardioembolic stroke (OR = 1.14, [1.06–1.23]). Analyses in the UK Biobank showed similar associations for available phenotypes. Genetically determined MCP-1 levels further associated with coronary artery disease and myocardial infarction. In MONICA/KORA, following adjustments for major vascular risk factors subjects with higher baseline MCP-1 levels were at increased risk of incident ischemic stroke (99 events; highest vs. lowest quartile HR = 2.08, [1.14–3.82]) over a mean 16-year follow-up.
Conclusions
Converging evidence from genetic and observational data supports circulating levels of the chemokine MCP-1 to be associated with risk of ischemic stroke. Whether targeting MCP-1 or its receptors can lower stroke incidence requires further study.
Trial registration number
N/A
WITHDRAWN
AS33-042
DIAGNOSTIC YIELD OF COL4A1 AND COL4A2 ANALYSIS IN A STROKE COHORT
1Ghent University Hospital, Department of Neurology, Ghent, Belgium
2Ghent University Hospital, Center for Medical Genetics, Ghent, Belgium
Background and Aims
Mutations in the genes encoding the α-1 chain of collagen type 4 - COL4A1 and COL4A2 have been associated with a broad phenotypic spectrum involving familial porencephaly, hemorrhagic and ischemic cerebrovascular disease, ocular, muscular and renal symptoms. Disease severity is variable and penetrance age-dependent and incomplete. Thus far, only limited genotype-phenotype correlations were established. We aimed to evaluate the diagnostic yield of COL4A1 and COL4A2 analysis in a cohort of stroke patients.
Methods
Molecular analysis of the whole coding region of COL4A1 and COL4A2 was performed in 267 consecutive patients. Variants were evaluated according to the ACMG guidelines and the Sherloc protocol.
Results
Twenty-three patients were identified, harbouring 15 COL4A1 and 11 COL4A2 variants. Seven were considered (likely) pathogenic, including 4 glycine substitutions and 2 frameshift mutations. All other variants were class 3 variants of undetermined significance All patients with a (likely) pathogenic mutation presented with ischemic stroke or extensive cerebral white matter lesions. Three patients had a family history of stroke. In 3 patients, additional features of the COL4A-spectrum were found, adding to the interpretation of the identified variant. Two patients showed tortuosity or dissection of the cervical arteries.
Conclusions
Molecular analysis of COL4A1 and COL4A2 detects a relatively high number of variants in stroke patients. Considering the (likely) pathogenic variants, mutation uptake in our study cohort is 2.6%. The interpretation of class 3 variants remains however challenging. Further analysis is needed to clarify genotype-phenotype correlations in stroke patients with COL4A variants.
Trial registration number
N/A
AS33-021
A GENOME-WIDE ASSOCIATION STUDY FOUND A NEW LOCUS IN A MANNOSIDASE GENE ASSOCIATED WITH LACUNAR ISCHEMIC STROKE
1Sant Pau Research Institute - Vall d’Hebron Institute of Research VHIR, Stroke Pharmacogenomics and Genetics Lab- Neurology Research Laboratory, Barcelona, Spain
2Sant Pau Research Institute, Stroke Pharmacogenomics and Genetics Lab, Barcelona, Spain
3Fundació Docència i Recerca Mútua Terrassa- Sant Pau Research Institute, Stroke Pharmacogenomics and Genetics Lab, Terrassa- Barcelona, Spain
4Hospital Universitari Vall d’Hebron, Stroke Unit- Department of Neurology, Barcelona, Spain
5IMIM-Hospital del Mar, Department of Neurology, Barcelona, Spain
6Health Research Institute of Santiago de Compostela IDIS, Clinical Neuroscience Research Laboratory, Santiago de Compostela, Spain
7Hospital Germans Trias I Pujol- Universitat Autònoma de Barcelona, Department of Neurosciences, Badalona, Spain
8Hospital Universitari Son Espases- Institut d’Investigació Sanitaria de Palma IdISPa, Neurobiology Laboratory- Research Unit, Palma de Mallorca, Spain
9University Hospital of Albacete, Department of Neurology, Albacete, Spain
10Hospital Universitari Mútua Terrassa, Neurology Service, Terrassa, Spain
11Hospital de la Santa Creu i Sant Pau, Stroke Unit- Department of Neurology, Barcelona, Spain
12MEGASTROKE consortium- International Stroke Genetics Consortium ISGC- University of Bordeaux, INSERM U1219 Bordeaux Population Health Research Center, Bordeaux, France
13MEGASTROKE consortium- International Stroke Genetics Consortium ISGC- University Hospital- LUM Munich, Institute for Stroke and Dementia Research ISD, Munich, Germany
14Germans Trias I Oujol Research Institute IGTP, GenomesForLife-GCAT Lab Group- Program of Predictive and Personalized Medicine of Cancer PMPPC, Badalona, Spain
15Washington University School of Medicine, Department of Psychiatry, Saint Louis- MO, USA
16Washington University School of Medicine, Department of Neurology, Saint Louis- MO, USA
17Virgen del Rocío & Macarena Hospitals- IBIS, Department of Neurology, Sevilla, Spain
18MEGASTROKE consortium- International Stroke Genetics Consortium ISGC- Sant Pau Research Institute, Stroke Pharmacogenomics and Genetics Lab, Barcelona, Spain
Background and Aims
Currently, more than 20 loci have been found associated with ischemic stroke (IS) risk. However, these genetic risk factors did not explain all heritability associated with IS. We aim to explore whether new stroke genetic risk factors can be found in specific homogeneous populations.
Methods
We performed a GWAS (Genome-Wide Association Study) analysis in a Spanish cohort of IS cases and controls (n = 6,235). Etiological classification was performed following TOAST criteria. For replication analysis we used MEGASTROKE data (n = 521,612) and a second Spanish cohort (n = 1,720). Moreover, we performed in silico analysis on GTEx portal, RT-PCR with 66 blood cDNA samples, and enzymatic activity assays on 34 plasma samples. For genetic quality controls we followed previous published recommendations. Genotype imputation was performed by Michigan Imputation Server. R and SPSS software were used for statistical analysis.
Results
We found 3 independent GWAS-significant SNPs (SNP1-p = 3.66x10e-08; SNP2-p = 2.04x10e-08; SNP3-p = 4.20x10e-08) on a Mannosidase gene region. In MEGASTROKE replication, all SNPs showed a significant p-value in lacunar subtype analysis (Trans-ethnical analysis, SNP1-p = 3.12x10e-02; SNP2-p = 4.48x10e-02; SNP3-p = 5.89x10e-03). In the second replication, SNP3 also presented a significant p-value on lacunar strokes (p-value = 4.70x10e-02). Allele risks were associated in silico with higher expression of Mannosidase gene. RT-PCR experiments confirmed this association (p-value = 4.40x10e-02). Lacunar strokes showed higher mannosidase activity compared to other IS subtypes (p-value = 3.60x10e-02) and to controls (p-value = 9.00x10e-03).
Conclusions
We found a new locus associated with lacunar stroke risk in a specific population and confirmed in an international cohort of patients. The candidate gene/protein could be a potential biomarker for lacunar stroke diagnosis.
Trial registration number
N/A
E-Poster Discussion-Systematic Review and Meta Analysis
AS34-037
EFFECT OF GLYCERYL TRINITRATE ON OUTCOME AFTER ACUTE STROKE: UPDATE OF A SYSTEMATIC REVIEW AND META-ANALYSIS OF INDIVIDUAL PATIENT DATA
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
Glyceryl trinitrate (GTN) is a candidate reperfusion and hypotensive treatment for acute stroke. We assessed the safety and efficacy of GTN using individual patient data (IPD) from completed trials.
Methods
Randomised controlled trials of GTN in patients with acute stroke were identified and IPD sought from the trialists. The effect of GTN versus control on functional outcome, assessed using the modified Rankin Scale (mRS), and death was studied overall and by time to randomisation. Secondary outcomes included measures of disability, cognition, mood and quality of life.
Results
Six trials of GTN (GTN-1/2/3, RIGHT, ENOS and RIGHT-2) were identified. Two of these were ambulance-based trials; the others recruited in-hospital. Overall, individual patient data was available for 5,005 participants; mean age 71.1 (SD 12.3) years; female 43.7%; time onset to randomisation 22.8 [7.6–34.3] hours; final diagnosis of qualifying event: ischaemic stroke 81.9%, primary intracerebral haemorrhage 15.8%, stroke type unknown 0.1% and transient ischaemic attack 2.2%. Compared with control, GTN lowered blood pressure by 7.0/3.2mmHg. At day 90, GTN did not alter any clinical or functional outcome measures (Table 1). However, in 440 patients recruited within 2–6 hours post stroke, GTN was associated with reductions in death, dependency and disability (mRS and Barthel Index; Table 1).

Conclusions
Overall, GTN did not alter outcome in patients with acute stroke. However, when administered within 2–6 hours GTN appears to improve outcome.
Trial registration number
N/A
AS34-034
SLEEP AND CIRCADIAN RHYTHM DYSFUNCTION IN HUMAN ISCHEMIC STROKE: A SYSTEMATIC REVIEW
1University of Melbourne, Florey Institute of Neuroscience & Mental Health, Melbourne, Australia
2Austin Hospital, Austin Health, Heidelberg, Australia
3Institute for Breathing and Sleep, Austin Health, Heidelberg, Australia
Background and Aims
Sleep and circadian rhythm pathologies are potentially modifiable risk factors and consequences of ischemic stroke (IS). Experimental sleep and endogenous circadian-rhythm disruption activate deleterious pathophysiological mechanisms which contribute to the pathogenesis and evolution of IS. Sleep and stroke research in humans has primarily focused on obstructive sleep apnea. We conducted a systematic review to assess the bidirectional relationship of non-apnea sleep disorders, sleep architecture, and endogenous circadian-rhythm dysfunction in patients with IS.
Methods
Systematic searches in MEDLINE, Embase, and PsycINFO were conducted in accordance with PRISMA guidelines. Extracted variables were chosen based on the STROBE guidelines and appraisal of methodological quality was assessed using the Newcastle-Ottawa scale.
Results
A systematic search yielded 5192 unique citations, of which 67 observational studies met inclusion criteria. Study quality was generally moderate (n = 39) to high (n = 27). Thirty-one studies included relevant neuroimaging outcomes. Long-sleep duration (≥8 hours) and non-apnea sleep disorders significantly increase the risk of IS after adjusting for cerebrovascular covariates. Inversely, IS was associated with suppressed sleep architecture and endogenous circadian-rhythms relative to controls which was associated with worse post-stroke severity and recovery.
Conclusions
Prolonged sleep duration and non-apnea sleep disorders increase the risk of IS, while sleep architecture and endogenous circadian-rhythms are disrupted after IS and associated with worse post-stroke outcome. However, study methodology (e.g., stroke to sleep and circadian assessment times) and stroke topography were heterogenous thereby limiting generalizable conclusions. Homogenous neuroimaging-driven prospective studies are warranted to elucidate the bidirectionally neuroprotective role of normalized sleep and circadian-rhythms in IS.
Trial registration number
N/A
AS34-041
CARDIAC CT-ANGIOGRAPHY VERSUS ECHOCARDIOGRAPHY FOR DETECTION OF CARDIAC THROMBI IN ISCHEMIC STROKE: A SYSTEMATIC REVIEW
1Amsterdam UMC- University of Amsterdam, Neurology, Amsterdam, The Netherlands
2Amsterdam UMC- University of Amsterdam, Radiology and Nuclear Medicine, Amsterdam, The Netherlands
3Amsterdam UMC- University of Amsterdam, Clinical Epidemiology and Public Health, Amsterdam, The Netherlands
Background and Aims
Approximately half of cardioembolic strokes are due to left atrial appendage thrombi secondary to (paroxysmal) atrial fibrillation. Echocardiography is currently the first-line method for imaging of the heart in ischemic stroke patients. We performed a systematic review of literature on cardiac CT-angiography (CTA) compared to echocardiography for detection of cardiac thrombi in ischemic stroke patients.
Methods
We searched Medline and EMBASE databases for relevant publications up to June 2018. We included studies reporting on both CTA (index test) and echocardiography (reference test), and providing data on the cardiac thrombus cases. Results were stratified for type of echocardiography: transesophageal (TEE)/transthoracic (TTE).
Results
Out of 1428 publications identified in the initial search, 14 studies (all single-center cohort) with data of 1568 patients were included. Mean age varied between 52–69 years and proportion of men between 53%-83%. Time interval between stroke and first test ranged between 0–21 days (reported in 9/14 studies). Time interval between tests ranged between 0–199 days (reported in 13/14 studies). In comparison with TEE, sensitivity and specificity of CTA for cardiac thrombus ranged from 0%-100% and 91%-100%, respectively (Figure). Four studies evaluated CTA against TTE, sensitivity was estimable for 2 (0% and 50%) and specificity varied between 67% and 100% (Figure).

Conclusions
Studies were heterogeneous in terms of timing since stroke and order of the investigations, CT-scanner, and scan protocol, which complicates interpretation of diagnostic accuracy. Large studies focusing on diagnostic yield (and correlation with clinical outcome) of cardiac CTA in the acute phase of ischemic stroke versus echocardiography are warranted.
Trial registration number
N/A
AS34-019
IS THE ASSOCIATION BETWEEN CHRONIC KIDNEY DISEASE AND STROKE RISK TRULY INDEPENDENT?
1Centre for the Prevention of Stroke and Dementia- University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
Chronic kidney disease (CKD) appears to be an independent risk factor for stroke, with various purported mechanisms and treatments proposed. Low glomerular filtration rate (eGFR) is a risk factor for stroke independent of cardiovascular risk factors in epidemiological studies, but there has been no systematic assessment of the impact of more complete adjustment for blood pressure (BP) on the association.
Methods
We did a systematic review to February 2018 (MEDLINE/EMBASE) for cohort studies or randomized controlled trials that reported stroke incidence in adults according to baseline eGFR. Study and participant characteristics and relative risks (RR) were extracted. Estimates were combined using a random effects model. Heterogeneity was assessed by x2 statistics and I2, and by subgroup strata and meta-regression.
Results
We identified 203 studies reporting data on 5,567,768 participants with 118,851 stroke outcomes. 85 studies (3,417,098 participants; 72,996 strokes) provided adequate data for meta-analysis of eGFR and stroke risk. Incident stroke risk was increased among participants with eGFR <60 ml/min/1.73m2 (RR = 1.73, 95% CI 1.57–1.90; p < 0.001), although there was quantitative heterogeneity between studies (x2 – p < 0.0001; I2 - 78.5%). Moreover, the association was reduced after adjustment for cardiovascular risk factors, with progressive attenuation on more thorough adjustment for hypertension: single baseline BP measure (RR = 1.63, 1.34–1.99; p < 0.001); history or treated hypertension (RR = 1.35, 1.24–1.46, p < 0.001); multiple BP measurements over months to years (RR = 1.10, 1.02–1.18; p = 0.01).
Conclusions
The apparently independent relationship between CKD and stroke may be confounded by their shared association with long-term prior blood pressure, rendering other proposed mechanisms and related treatments unnecessary.
Trial registration number
N/A
AS34-020
DO ACUTE STROKE PATIENTS DEVELOP HYPOCAPNIA? A SYSTEMATIC REVIEW AND META-ANALYSIS
1Department of Cardiovascular Sciences, University of Leicester, Leicester, United Kingdom
2Neurology Department, University of Sao Paulo, Sao Paulo, Brazil
3Biomedical Engineering- Modelling and Applied Social Sciences Centre, Federal ABC University, Sao Bernardo do Campo, Brazil
4National Institute for Health Research Biomedical Research Centre, University of Leicester, Leicester, United Kingdom
Background and Aims
Carbon dioxide (CO2) is a potent cerebral vasomotor agent. Despite reduction in CO2 levels (hypocapnia) being described in several acute diseases, there is no clear data on baseline CO2 values in acute stroke. This systematic review and meta-analysis aims for the first time to determine if acute stroke patients tend to be hypocapnic, by assessment of studies incorporating carbon dioxide measurements in the acute stroke setting.
Methods
Four online databases, Web of Science, MEDLINE, EMBASE and CENTRAL, were searched for articles that described either partial pressure of arterial CO2 (PaCO2) and end-tidal CO2 (EtCO2) in acute stroke.
Results
After screening, based on predefined inclusion and exclusion criteria, 18 studies were retained. There were 5 studies in intracerebral haemorrhage and 13 in ischaemic stroke, totalling 685 stroke participants. In 11 studies (306 patients) detailing carbon dioxide values (EtCO2 or PaCO2) for acute stroke patients and controls, acute stroke was associated with a significant decrease in CO2 levels compared to controls (-0.90 mmHg [95% CI -1.69 to -0.12]; P = 0.0005, I2 = 68%) (Figure). Data obtained from cerebral haemodynamics suggest a significant reduction in cerebral blood flow velocities and cerebral autoregulation in acute stroke patients.
Figure. Forest plot with random-effects for differences in EtCO2 levels between acute stroke and healthy controls.

Conclusions
The evidence from this review suggests that acute stroke patients are significantly more likely than controls to be hypocapnic, supporting the value of routine CO2 assessment in the acute stroke setting. Further studies are required in order to evaluate the clinical impact of these findings.
Trial registration number
N/A
E-Poster Discussion-Multidisciplinary Care I
AS14-022
FAMILIAL CAREGIVING FOLLOWING STROKE: FINDINGS FROM THE COMPREHENSIVE POST-ACUTE STROKE SERVICES (COMPASS) STUDY
1University of North Carolina-Wilmington, School of Nursing, Wilmington- NC, USA
2University of North Carolina at Chapel Hill- Gillings School of Global Public Health, Department of Epidemiology, Chapel Hill- NC, USA
3University of North Carolina at Chapel Hill, Department of Biostatistics- Collaborative Studies Coordinating Center, Chapel Hill- NC, USA
4Wake Forest School of Medicine, Social Sciences and Health Policy- Division of Public Health Sciences, Winston-Salem- NC, USA
5Wake Forest School of Medicine, Department of Neurology, Winston-Salem- NC, USA
6Duke University, School of Medicine, Durham- NC, USA
Background and Aims
In this cluster-randomized pragmatic trial we characterized caregiving types and intensity, and the effect of stroke transitional care (COMPASS-TC) on caregiver strain.
Methods
Of 5882 patients enrolled in the COMPASS study, 4208 (71%) identified a familial caregiver. Caregiver questionnaires, including the Modified Caregiver Strain Index (MCSI), were administered 3 months post-discharge. Demographics and caregiving frequency, duration, and tasks were characterized. MCSI (standardized to 0–100) was compared by group (COMPASS-TC vs. usual care).
Results
Median patient NIHSS was 1 (range 0–39, IQR 0–3). Most caregivers were women (68%) and spouses (53%). Only 1228 caregivers (29%) completed the MCSI. Ascertainment was associated with older patient age, white race, and spousal relationship. 10% of caregivers reported excellent health. 79% provided care ≥9 weeks. 33% provided ≥30 hours of care per week, assisting with an average of 1.0 (SD 1.5) activities of daily living (ADL) and 6.3 (SD 3.3) instrumental ADL (IADL). Average standardized caregiver strain was 21.9 (SD: 23.3), increasing with higher stroke severity and multiple comorbidities. Female caregivers reported higher strain. Of 1722 patient-caregiver dyads enrolled in intervention, 40% completed all intervention components. In intention-to-treat (ITT) analysis, treatment group was not associated with decreased caregiver strain (mean difference 0.65 (95% CI -1.99, 3.29)).
Conclusions
Mild-to-moderate stroke patients received significant assistance. However, caregiver strain was relatively low. In this study, 40% received COMPASS-TC inclusive of caregiver support. In ITT analysis, treatment group was not associated with reduced caregiver strain. Future research needs to identify best ways to reach caregivers and implement interventions to reduce strain.
Trial registration number
NCT02588664
AS14-001
DOES MODE OF ARRIVAL TO THE HOSPITAL IN ACUTE STROKE AFFECT DISCHARGE DISPOSITION?
1Providence Holy Cross Medical Center, Stroke Care, Valencia, USA
2Providence Holy Cross Medical Center, Stroke Care, Mission Hills, USA
3Providence Holy Cross Medical Center, Data Science, Mission Hills, USA
Background and Aims
Prehospital delay in acute stroke (AS) is problematic since disability reducing treatments are time limited. We examined if mode of arrival to the hospital in AS predicted treatment time (TT) or discharge disposition (DD). We also looked at presenting symptoms (PS) triggering initiation of emergency medical services (EMS).
Methods
Using a stroke registry, 1172 records were retrospectively reviewed for patients diagnosed with stroke or transient ischemic attack (TIA) arriving to a community hospital between 2015 and 2018. TIA was omitted from the DD analysis. A uni-variable analysis was completed for all variable candidates for the logistic regression model to evaluate if the mode of arrival was associated with DD while controlling for other covariates.
Results
Weakness/Paresis (WP) was the most frequent PS. Sixty-six percent of patients arrived by EMS versus 33.7% by private transportation (PT), with 61% arriving via PT discharging to home. Statistically significant findings (p < 0.0001) included; patients with WP were more likely to discharge to an acute rehabilitation unit (ARU) versus home, time from arrival to triage was a predictor of DD, patients presenting with altered level of consciousness were more likely discharged to a skilled nursing facility or hospice. Patients arriving via EMS were treated 13.2 minutes faster (p = 0.0014). There was no difference in DD for patients presenting with aphasia (p = 0.087).
Conclusions
Patients experiencing WP triggered initiation of EMS more than any other symptom. Those arriving via EMS were treated faster and were more likely to be discharged to an ARU warranting more community education.
Trial registration number
N/A
AS14-017
INCIDENCE AND IDENTIFICATION OF DEHYDRATION IN ACUTE STROKE: AN OBSERVATIONAL STUDY
1University of Central Lancashire, The Stroke Research Unit- Faculty of Health & Wellbeing, PRESTON, United Kingdom
2Lancashire Teaching Hospiyals NHS Foundation Trust, Research Department, Preston, United Kingdom
Background and Aims
Achieving adequate hydration post-stroke may prevent neurological deterioration by reducing the ischaemic penumbra and maintaining cerebral perfusion, and may reduce the risk of complications such as infection, constipation, delirium and venous thromboembolism. However, there is little evidence that any single symptom, sign or test - including many that clinicians customarily rely on – has diagnostic utility for dehydration. This study aimed to identify how dehydration was diagnosed, how frequently dehydration occurred, and in whom, after acute stroke.
Methods
A consecutive sample of patients (>18yrs), admitted to one hospital trust with a final diagnosis of stroke between March and June 2017. Clinical characteristics were collated using case-note review for the first 72 hours after admission. Blood plasma osmolarity was calculated from routinely collected admission blood tests.
Results
50 patients, mean age 75 years (range 48–100), 25 (50%) female, were included. None of the case-notes included documentation of clinical assessment of dehydration. One or both of the routine blood tests (urea and electrolytes; blood glucose) needed to perform the osmolarity calculation were not requested for 9 (18%) patients. Of the remaining patients, 18 (44%) were hydrated, 14 (34%) had impending dehydration, 9 (22%) were dehydrated. Impending or frank dehydration more commonly occurred in the presence of upper-limb, lower-limb, or facial weakness, although these were non-significant.
Conclusions
Dehydration or impending dehydration may occur in over half of hospitalised stroke patients, but assessment and diagnosis of dehydration is not routinely documented. Some blood tests required to inform osmolarity calculations are not routinely collected on admission.
Trial registration number
N/A
E-Poster Discussion-Multidisciplinary Care I
AS14-022
FAMILIAL CAREGIVING FOLLOWING STROKE: FINDINGS FROM THE COMPREHENSIVE POST-ACUTE STROKE SERVICES (COMPASS) STUDY
1University of North Carolina-Wilmington, School of Nursing, Wilmington- NC, USA
2University of North Carolina at Chapel Hill- Gillings School of Global Public Health, Department of Epidemiology, Chapel Hill- NC, USA
3University of North Carolina at Chapel Hill, Department of Biostatistics- Collaborative Studies Coordinating Center, Chapel Hill- NC, USA
4Wake Forest School of Medicine, Social Sciences and Health Policy- Division of Public Health Sciences, Winston-Salem- NC, USA
5Wake Forest School of Medicine, Department of Neurology, Winston-Salem- NC, USA
6Duke University, School of Medicine, Durham- NC, USA
Background and Aims
In this cluster-randomized pragmatic trial we characterized caregiving types and intensity, and the effect of stroke transitional care (COMPASS-TC) on caregiver strain.
Methods
Of 5882 patients enrolled in the COMPASS study, 4208 (71%) identified a familial caregiver. Caregiver questionnaires, including the Modified Caregiver Strain Index (MCSI), were administered 3 months post-discharge. Demographics and caregiving frequency, duration, and tasks were characterized. MCSI (standardized to 0–100) was compared by group (COMPASS-TC vs. usual care).
Results
Median patient NIHSS was 1 (range 0–39, IQR 0–3). Most caregivers were women (68%) and spouses (53%). Only 1228 caregivers (29%) completed the MCSI. Ascertainment was associated with older patient age, white race, and spousal relationship. 10% of caregivers reported excellent health. 79% provided care ≥9 weeks. 33% provided ≥30 hours of care per week, assisting with an average of 1.0 (SD 1.5) activities of daily living (ADL) and 6.3 (SD 3.3) instrumental ADL (IADL). Average standardized caregiver strain was 21.9 (SD: 23.3), increasing with higher stroke severity and multiple comorbidities. Female caregivers reported higher strain. Of 1722 patient-caregiver dyads enrolled in intervention, 40% completed all intervention components. In intention-to-treat (ITT) analysis, treatment group was not associated with decreased caregiver strain (mean difference 0.65 (95% CI -1.99, 3.29)).
Conclusions
Mild-to-moderate stroke patients received significant assistance. However, caregiver strain was relatively low. In this study, 40% received COMPASS-TC inclusive of caregiver support. In ITT analysis, treatment group was not associated with reduced caregiver strain. Future research needs to identify best ways to reach caregivers and implement interventions to reduce strain.
Trial registration number
NCT02588664
E-Poster Discussion-Neurointervention II
AS07-092
REDUCTION OF TIME TO REPERFUSION LEADS TO BETTER OUTCOMES OF ENDOVASCULAR TREATMENT FOR ISCHEMIC STROKE IN ROUTINE CLINICAL PRACTICE: RESULTS OF THE MR CLEAN REGISTRY
1Erasmus University Medical Center, Radiology, Rotterdam, The Netherlands
2Amsterdam UMC, Radiology, Amsterdam, The Netherlands
3Maastricht UMC, Neurology, Maastricht, The Netherlands
4Amsterdam UMC, Neurology, Amsterdam, The Netherlands
5Maastricht UMC, Radiology, Maastricht, The Netherlands
6Haaglanden MC, Radiology, The Hague, The Netherlands
7Haaglanden MC, Neurology, The Hague, The Netherlands
8St. Antonius Ziekenhuis, Neurology, Nieuwegein, The Netherlands
9St. Antonius Ziekenhuis, Radiology, Nieuwegein, The Netherlands
10UMC Groningen, Neurology, Groningen, The Netherlands
11UMC Groningen, Radiology, Groningen, The Netherlands
12Rijnstate, Radiology, Arnhem, The Netherlands
13Rijnstate, Neurology, Arnhem, The Netherlands
14UMC Utrecht, Neurology, Utrecht, The Netherlands
15UMC Utrecht, Radiology, Utrecht, The Netherlands
16Erasmus University Medical Center, Neurology, Rotterdam, The Netherlands
Background and Aims
Outcome after endovascular treatment (EVT) seem highly time dependent, but whether active reduction of time to treatment leads to better outcomes has not been demonstrated. We analyzed the data of the MR CLEAN registry, which comprises all patients in the Netherlands who had EVT for acute ischemic stroke, for a trend in time to treatment, and its association with outcome.
Methods
We compared workflow, neurological deficit (NIHSS) at 24h, functional outcome (mRS) at 90-days, occurrence of symptomatic intracranial hemorrhage (sICH) and mortality in patients with ischemic stroke and a proximal intracranial occlusion in the anterior circulation included in the second cohort of the Registry (June 2016-November 2017; n = 1779) to patients included in the first cohort (March 2014-June 2016; n = 1526) using logistic regression.
Results
Baseline NIHSS was 16 in both cohorts. Times from onset-to-groin and onset-to-reperfusion were shorter in the second cohort than in the first (185 versus 210 minutes;p < 0.001 and 239 versus 270 minutes; p < 0.001, respectively). Rates of sICH and mortality did not differ between the cohorts (5.8% versus 5.7%;p = 0.89 and 29% versus 29%;p = 0.60). However, follow-up NIHSS was lower (median 9 versus 11;p < 0.001) and more patients achieved functional independence at 90 days (42.3% versus 38.9%;p = 0.017) in the second cohort. In a logistic regression model, the difference in good outcome between the two cohorts (aOR 1.27;95%CI 1.08–1.50) was reduced after additional adjustment for time to reperfusion (aOR 1.16;95%CI 0.98–1.37).
Conclusions
The MR CLEAN Registry data indicate that improving workflow indeed leads to better functional outcome after EVT in routine clinical practice.
Trial registration number
N/A
AS07-057
PERIINTERVENTIONAL MEAN ARTERIAL BLOOD PRESSURE BELOW 60 MMHG PREDICTS POOR OUTCOME AFTER STROKE THROMBECTOMY
1Medical University of Graz, Department of Neurology, Graz, Austria
2Medical University of Graz, Department of Anaesthesiology and Intensive Care Medicine, Graz, Austria
3Medical University of Graz, Department of Radiology- Division of Neuroradiology- Vascular and Interventional Radiology, Graz, Austria
4Medical University of Graz, Institute for Medical Informatics- Statistics and Documentation, Graz, Austria
Background and Aims
We aimed to investigate the influence of periprocedural blood pressure values on three-months functional outcome in stroke patients undergoing mechanical thrombectomy (MT) under general anaesthesia (GA).
Methods
We screened all patients ≥18 years with anterior circulation large vessel occlusion who were treated with MT under GA at our centre from January 2011 to June 2016. Clinical and radiological data were prospectively collected as part of an ongoing cohort study. All included patients had continuous invasive periinterventional blood monitoring, these data were extracted from electronic anaesthesia records. We used multivariate regression and receiver operating characteristic (ROC) curves to investigate effects of blood pressure values on unfavourable outcome, defined as modified Rankin Scale (mRS) scores 3–6 three months post-stroke.
Results
A total of 115 patients were included in this study (mean age: 65 ± 13 years, 56% male). Average periinterventional systolic and mean arterial blood pressure (MAP) had no effect on long-term outcome. However, single severe blood pressure drops were related to unfavourable outcome, with absolute MAP drops showing the highest association to it, compared to both systolic and relative drops (with reference to pre-interventional values). ROC curve analysis identified the strongest predictive blood pressure value for unfavourable outcome as a MAP ever ≤60 mmHg (OR 2.72, p = 0.01). A MAP ≤60mmHg remained an independent predictor for poor functional outcome after multivariate analysis (p = 0.04).
Conclusions
For patients undergoing MT under GA, single MAP drops ≤60mmHg are associated with unfavourable long-term outcome. Therefore, every effort should be made to prevent hypotensive episodes below this threshold.
Trial registration number
N/A
AS07-058
ORAL ANTICOAGULANT USE PRIOR TO ENDOVASCULAR TREATMENT OF ACUTE ISCHEMIC STROKE: RESULTS FROM THE MR CLEAN REGISTRY
1Maastricht University Medical Center plus, Neurology, Maastricht, The Netherlands
2Erasmus MC- University Medical Center, Neurology, Rotterdam, The Netherlands
3Erasmus MC- University Medical Center, Radiology & Nuclear Medicine, Rotterdam, The Netherlands
4Erasmus MC- University Medical Center, Public Health, Rotterdam, The Netherlands
5Maastricht University Medical Center plus, Radiology, Maastricht, The Netherlands
Background and Aims
Prior oral anticoagulation (OAC) use is a risk factor for complications after intravenous thrombolysis for acute ischemic stroke. However, limited evidence exists on outcomes after endovascular treatment (EVT). We aim to compare outcomes after EVT between patients with and without prior use of OACs in clinical practice.
Methods
Data of ischemic stroke patients with an intracranial anterior circulation occlusion, included in the nationwide, prospective, multicentre MR CLEAN Registry between March 2014 and November 2017, were analyzed. Primary outcome was functional outcome on the modified Rankin Scale score at 90 days. We compared outcomes between groups with ordinal and binary logistic regression, adjusted for baseline prognostic factors. Symptomatic intracranial hemorrhage (sICH) was a secondary outcome. We performed a subgroup analysis according to OAC type.
Results
3175 patients were included in this study, of whom 503 (16%) used OACs. Use of OACs was associated with worse functional outcome (cOR 0.57; 95% CI 0.48–0.69). However, there was no difference after adjustment for baseline characteristics (acOR 0.98; 95% CI 0.77–1.25). Further, OAC use was not associated with higher incidence of sICH (aOR 0.63; 95% CI 0.35–1.13). Outcomes in a subgroup analysis according to OAC type were not significantly different.
Conclusions
In clinical practice, prior OAC use was associated with similar functional outcome and sICH rate after EVT for acute stroke. Therefore, patients on OACs should not be routinely excluded from EVT.
Trial registration number
N/A
AS07-120
PREVALENCE AND OUTCOME OF PATIENTS WITH MULTIVESSEL OCCLUSIONS IN THE MR CLEAN REGISTRY
1Amsterdam UMC- location AMC, Neurology, Amsterdam, The Netherlands
2Amsterdam UMC- location AMC, Radiology & Nuclear Medicine, Amsterdam, The Netherlands
Background and Aims
Little is known about the occurence and implications of multivessel occlusions (MVO) in patients who present with an intracranial large vessel occlusion and are candidate for endovascular treatment (EVT).
Methods
We report data from the MR CLEAN Registry, a prospective, observational study on all EVT patients in the Netherlands. MVO was defined as an MCA occlusion (M1/M2) or intracranial ICA/ICA-T occlusion, with a concurrent second occlusion in the ACA or PCA territory on initial DSA and confirmed on baseline CTA, as assessed by a core laboratory. Scores on the mRS at 90days were compared between MVO and single vessel occlusion patients with ordinal logistic regression after 1:1 propensity score matching based on age, occlusion location, baseline NIHSS and pre-stroke mRS.
Results
Of 1526 patients with proximal occlusions of the anterior circulation, 35 (2.3%) had an MVO. Thirty out of thirty-five (86%) had a concurrent ACA occlusion. After matching with 35 single vessel occlusion patients, baseline characteristics were well-balanced. However, worse collateral grades were observed in MVO patients (23% vs 3% absent collaterals, p = 0.02). Six percent of MVO patients regained functional independence (mRS 0–2) at 90 days, compared to 31% of single vessel occlusion patients (p < 0.01). Mortality at 90 days was 58% vs 44% for MVO and single vessel occlusion patients, respectively (p = 0.27). A similar, though non-significant association of MVO and worse outcome was observed in mRS shift analysis (cOR 0.42, 95%CI 0.16–1.10).
Conclusions
MVO in EVT patients on baseline imaging may be associated with worse functional outcome.
Trial registration number
N/A
AS07-133
HYPOPERFUSION INTENSITY RATIO IS A POOR DISCRIMINATOR OF INFARCT GROWTH IN PATIENTS UNDERGOING THROMBECTOMY
1Emory University, Neurology, Atlanta, USA
Background and Aims
The hypoperfusion intensity ratio (HIR) is a perfusion-weighted imaging parameter defined as the ratio of Tmax>10 seconds: Tmax>6 seconds volume, correlateing with poor collaterals and infarct growth during transfer of patients to comprehensive stroke centers (CSC). We aim to assess the utility of HIR in stratifying successfully-reperfused patients as fast versus slow progressors.
Methods
Consecutive acute ischemic stroke patients transferred to our CSC from 09/10-10/18 were included if the following criteria were met: 1) computed tomography perfusion (CTP) imaging 2) follow-up neuroimaging for assessment of final infarct volumes and 3) achievement of Thrombolysis In Cerebral Infarction scale (TICI) 2b or greater post-thrombectomy (defined as incompletely [TICI2b] or fully reperfused [TICI2c/3]). Infarct growth rate was calculated as difference between infarct volume on follow-up imaging and acute DWI lesion volume, divided by time from CTP to reperfusion (hrs).
Results
A total of 578 patients (179 females, median age 65(55-75)) were eligible for this analysis, comprising 208 TICI 2b and 370 TICI 2c/3 patients. Median infarct growth rate was significantly lower in the TICI 2c/3 vs 2b cohorts (11.2 ml/hr vs 18.3 ml/hr, p < 0.001 Mann-Whitney U test). Median HIR did not differ between TICI 2c/3 and 2b cohorts (0.39 vs 0.42, p = 0.20, Mann-Whitney U test). A linear regression established that HIR was a poor discriminator for IG (R2 0.05 vs 0.08, respectively) and IG rate (R2 0.043 vs 0.067) in both cohorts.

Conclusions
HIR is a poor discriminator of infarct growth in successfully reperfused patients who undergo perfusion imaging at a CSC.
Trial registration number
N/A
E-Poster Discussion-CSVD + VCI
AS27-029
GENOTYPE AND PHENOTYPE CORRELATION IN PATIENTS WITH CADASIL: A RETROSPECTIVE STUDY
1University of Glasgow, Institute of Neuroscience and Psychology, Glasgow, United Kingdom
Background and Aims
CADASIL is the most common monogenic cerebral small vessel disorder, caused by distinctive cysteine-altering mutations affecting the 34 EGFr domains of the NOTCH3 protein. A recent report suggests that mutations outside EGFr domains 1–6 are mainly paucisymptomatic and have lower MRI lesion loads. We investigated the genotype-phenotype correlation in a CADASIL cohort.
Methods
We reviewed clinical and imaging features of CADASIL patients who attended a Neurovascular Genetics Clinic, between January 2001 and October 2018. The cohort was divided into two groups: proximal-genotype (EGFr domains 1–6) and distal-genotype (EGFr domains 7–34). Leukoaraiosis, microbleeds and lacunes were manually measured using MANGO software. The relationships between genotype, clinical phenotype and imaging phenotypes were explored by linear regression, co-varying for age, sex and risk factors. Log-rank tests were performed for time to event analysis for clinical end-points.
Results
We included 165 CADASIL patients with cysteine missense mutations, 140 of whom were proximal-genotype and 25 distal-genotype. Compared to proximal-genotype cases, distal-genotype patients experienced their first stroke 6 years later (mean 52.1, SD 12.13; p = 0.05); onset of cognitive impairment (5 years later, mean 53.6, SD 14.3) and neuropsychiatric disorders (3 years later, mean 48.4, SD 15.2) was not significantly different between genotypes. Volumes of subcortical white matter hyperintensities (mean 112 ml, SD 37), lacune counts (mean 2.5, SD 3.5) and microbleeds (0) were significantly less in the distal genotype patients.
Conclusions
We confirmed a genotype-phenotype correlation in CADASIL, mutations outside the classic EGFr domains 1–6 being associated with later onset of symptoms and lower MRI structural lesion loads.
Trial registration number
N/A
AS27-039
STRUCTURAL NETWORK CONNECTIVITY AND HYPERTENSION IN CEREBRAL SMALL VESSEL DISEASE
1Donders Institute for Brain Cognition and Behaviour - Radboudumc, Center for Cognitive Neuroimaging, Nijmegen, The Netherlands
Background and Aims
Recent studies have shown that white matter disruption, indicated by network efficiency, plays an important role in the development of cognitive impairment in cerebral small vessel disease (SVD). As wide range of network measures now exist, we investigated which network measure is the most biologically informative in explaining the cognitive deficits and we assessed the effect of hypertension on this network measure.
Methods
410 non-demented participants with SVD on neuroimaging were included (mean age 64.9 years [SD: 8.7], 46% female) (table 1). Weighted connectivity matrices from diffusion tensor imaging and graph-theoretical measures were calculated. To identify the most influential network measure, we performed elastic net method. We performed linear regression models and mediation analysis to assess the association between hypertension, SVD markers and network measure, adjusted for age, sex, education and other cardiovascular risk factors.
Results
Global efficiency showed the strongest association with psychomotor speed and cognitive index among all network measures in SVD. Hypertension was significantly associated with lower global efficiency (β = -0.16, P = 0.001) and higher white matter hypertensities (WMH) volume (β = 0.16, P = 0.002) (table 2). Mediation analysis showed that hypertension was directly related to global efficiency (β = -0.19, P = 0.03 ). However the effect of indirect pathway through WMH is stronger (β = -0.24, P <0.001).
Conclusions
We demonstrated that global efficiency is the strongest predictor for cognitive deficits in SVD among all network measures and seems to be most suitable as surrogate marker of SVD. Hypertension negatively influences the structural network in SVD through direct and indirect pathway via WMH.
Trial registration number
N/A
AS26-018
THE INTERACTION EFFECT OF LACUNES AND SUBCLINICAL CAROTID ATHEROSCLEROSIS ON COGNITIVE DECLINE
1Huashan Hospital, Neurology, Shanghai, China
2Fudan University, School of Life Sciences, Shanghai, China
Background and Aims
Lacune, as an important imaging marker of cerebral small vessel diseases (CSVDs), is considered to be a significant risk factor for cognitive decline in many studies. The underlying mechanism by which lacunes induce cognitive impairment remains unclear. We investigated the association between lacunes at different locations, subclinical carotid atherosclerosis (CA) and global cognitive decline in a rural Han Chinese population.
Methods
In the longitudinal population-based Taizhou Imaging Study, 562 participants free of neurological disorders underwent brain MRI, neuropsychological testing and carotid B ultrasound at baseline. A total of 456 participants were followed up for cognitive performance for a mean (SD) of 4.6 (0.6) years. Linear logistic regression was used to estimate the interaction effect of lacunes and subclinical CA (increased intima media thickness or plague) on global cognitive decline.
Results
Lacunes were detected in 150 individuals (26.7%) at baseline in our study and most of them were located in bilateral basal ganglia. We found only subcortical anterior circulation lacunes were associated with global cognitive decline (β: -0.115; 95% CI -0.054 to -0.003), whereas subclinical CA were not (β: -0.059; 95% CI -0.026 to 0.007). In linear regression model, increased common carotid artery or internal carotid artery IMT strengthened the association between lacunes and cognitive decline (β: -0.138; 95% CI -0.273 to -0.045; β: -0.112; 95% CI -0.404 to -0.014, respectively).
Conclusions
Lacunes increased the risk of global cognitive decline in this Chinese longitudinal cohort study. Subclinical carotid atherosclerosis and lacunes had an interaction effect on cognitive decline.
Trial registration number
N/A
AS27-054
PREDICTION OF COGNITIVE DECLINE AFTER INTRACEREBRAL HAEMORRHAGE USING TOTAL SMALL VESSEL DISEASE SCORE
1Centre Hospitalier Universitaire de Lille, Department of Neurology, Lille, France
2Massachusetts General Hospital, Department of Neurology, Boston, USA
3Université Paris-Descartes, Department of Neuroradiology, Paris, France
Background and Aims
We aimed to determine whether a validated total cerebral small vessel disease (SVD) score could predict cognitive decline after intracerebral haemorrhage (ICH).
Methods
We analyzed data from first-time ICH survivors with no history of prior cognitive impairment, enrolled in a single-center prospective study. We reviewed MRI scans to compute a validated 6-point score for SVD burden and cortical atrophy. The cognitive performance was quantified by: 1) administering the telephone interview for cognitive status (TICS) test; 2) identifying diagnosis of dementia based on medical records. Linear mixed model analyses were utilized to identify predictors of changes in TICS score, and Cox regression to identify predictors of new-onset dementia. We calculated SVD score cut-offs to maximize sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for diagnosis of dementia.
Results
We enrolled 612 spontaneous ICH survivors with a median follow-up of 46.3 months [interquartile range 35.5–58.7]. Out of all participants, 214 (35%) developed dementia. Increasing SVD scores were associated with faster cognitive decline (coeff -0.25, standard error 0.02) and dementia diagnosis (hazard ratio 1.33, 95% CI 1.08–1.64). Age, atrophy and lower TICS score at baseline were also independently associated with cognitive decline and new-onset dementia (all p < 0.001). A SVD score cut-off of ≥ 2 had highest sensitivity (83%) and specificity (91%) for dementia diagnosis with PPV of 84% and NPV of 91%, respectively.
Conclusions
Total SVD score is associated with cognitive decline after ICH. Replication of our results in an independent cohort is ongoing to further support its implementation in clinical care.
Trial registration number
N/A
AS27-016
WHITE MATTER HYPERINTENSITIES PREFERENTIALLY AFFECT LONG AND INTERHEMISPHERIC BRAIN CONNECTIONS
1University Medical Center Hamburg Eppendorf, Department of Neurology, Hamburg, Germany
Background and Aims
White matter hyperintensities (WMH) are a common finding in healthy elderly adults. While mostly incidental, they are also linked to cognitive decline, an association which is hypothesised to result from the reduction of brain network efficiency, raising the question of how this reduction is caused. In this study we tested the hypothesis that WMH reduce global brain network efficiency by preferentially disturbing long-range connections in the brain.
Methods
We analysed MRI data from 930 subjects of the Hamburg City Health Study – a single center, prospective cohort study. WMH were segmented on FLAIR images, and the structural connectome was constructed based on diffusion imaging. Connectome edges were subdivided (Figure 1) based on streamline course (interhemispheric, left intrahemispheric and right intrahemispheric) and streamline length (long and short). The relative connectivity of these subgroups of connections, i.e. fraction of the sum of all edge weights in a particular subgroup of the total summed edge weights, were related to the WMH load in a linear regression analysis.

Results
Mean WMH volume was 1.416 ml (SD = 2.009). Increasing WMH load was significantly associated with a relative connectivity decrease in long (<0.001) and interhemispheric (p = 0.005) connection subgroups and an increase in short (p < 0.001) and left intrahemispheric (p = 0.01) connection subgroups.
Conclusions
WMH are associated with decreased connectivity of long and interhemispheric connections in the brain as compared to short and intrahemispheric connections. This pattern of preferential affection of long-range and interhemispheric connections may help understand the association of WMH with reduced global brain network efficiency and cognitive decline.
Trial registration number
N/A
E-Poster Discussion-Rare Causes and Case Reports II
AS35-103
HISTOPATHOLOGICAL ANALYSIS OF CEREBRAL THROMBUS IS PIVOTAL AND CAN REVEAL ISCHEMIC STROKE ETIOLOGY
1San Raffaele Scientific Institute, Department of Neurology - Stroke Unit- Institute of Experimental Neurology INSPE - Neuroimmunology Unit, Milan, Italy
2San Raffaele Scientific Institute, Department of Neuroradiology, Milan, Italy
3San Raffaele Scientific Institute, Department of Pathology, Milan, Italy
4San Raffaele Scientific Institute, Department of Neurology - Stroke Unit, Milan, Italy
Background and Aims
Histopathological analysis of cerebral thrombi retrieved from mechanical thrombectomy is emerging as an important tool in the diagnostic work-up to unravel stroke etiology and, accordingly, to optimize secondary prevention strategy. However, up to day, no clear thrombus signature has been defined and quantitative analysis of thrombus components is not able to clearly categorize thrombus origin. We here report a case of acute stroke treated with endovascular procedure, in which histopathological analysis allowed an etiological categorization.
Methods
After retrieval, thrombus material was fixed in formalin and subsequently embedded in paraffin; stainings with Hematoxylin and Eosin, Masson’s trichrome, Alcian blue and immunohistochemistry with anti-CD34 antibody (for endothelial cells) were perfomed.
Results
An 86-year-old man admitted to our emergency room with an occlusion of distal right M1 segment was subjected to mechanical thrombectomy achieving complete recanalization (Figure1). A single fragment, with cylindrical morphology and stiff texture, was retrieved. Histopathological analysis showed a thickened intima layer with accumulation of smooth muscle cells and proteoglycans embedded within extracellular matrix; infiltrating foamy macrophages and scattered lymphocytes as well as cholesterol clefts were also identified (Figure2). The findings were compatible with an atheromatous plaque, thus defining stroke as atherosclerotic, and antiplatelet therapy was started.
Conclusions
Qualitative histopathological analysis of retrieved thrombus allowed to define the atherosclerotic origin of stroke. A local thrombosis superimposed on an intracranial atherosclerotic plaque likely represents the stroke mechanism in our patient. The analysis of retrieved clots should be part of ordinary clinical work-up as adjuvant to determine stroke etiology.
Trial registration number
N/A
WITHDRAWN
AS23-008
POSTERIOR ARTERIAL ISCHEMIC STROKE IN CHILDHOOD: CLINICAL FEATURES AND NEUROIMAGING CHARACTERISTICS
1University Children’s Hospital Bern, Department of Pediatrics- Division of Child Neurology, Bern, Switzerland
2University Children’s Hospital Bern, Department of Neuroradiology, Bern, Switzerland
Background and Aims
Literature regarding the clinical manifestation and neuroradiological findings of pediatric posterior circulation arterial ischemic stroke (PCAIS) is scarce. This study aims to describe epidemiological features, clinical characteristics and neuroimaging data of pediatric PCAIS in Switzerland using the populations based Swiss Neuropediatric Stroke Registry (SNPSR).
Methods
Children aged 1 month to 16 years presenting with a purely PCAIS between 2000 and 2016 were included. Epidemiology, clinical manifestation, stroke aetiology and neuroradiological features were summarized using descriptive statistics. Stroke severity was assessed using the Pediatric NIHSS. Correlation analysis was performed using Spearman correlation coefficient.
Results
Forty-three children with PCAIS were included (27 boys (62.8%), median (IQR) age 7.9y (5-11.7)). The incidence of PCAIS is Switzerland was 0.183/100 000 and represented 16% of all childhood AIS. Most patients presented with unspecific neurological complaints such as headache (58.1%) and nausea/vomiting (46.5%). The most frequent clinical manifestations were ataxia (58.1%) and motoric/sensory hemisyndrome (53.5%/51.2%). Unilateral focal cerebral arteriopathy (FCA) was the most common aetiology (11 children, 25.6%). The majority of infarcts were located in the cerebellum (46.5%) and thalamus (39.5%). A shorter diagnostic delay correlated with more severe stroke symptoms at presentation (rho = .-0.365, p = 0.016).
Conclusions
Pediatric PCAIS is due to FCA in one quarter of the patients in our cohort. The frequently reported unspecific clinical symptoms, especially when associated with mild neurological findings, carry the risk for a delayed stroke diagnosis. A high index of suspicion and increased awareness are required for a timely diagnosis and treatment initiation.
Trial registration number
N/A
WITHDRAWN
AS23-023
PREVALENCE AND CLINICAL PROFILE OF MIGRAINE WITH AURA IN A COHORT OF YOUNG PATIENTS WITH STROKE: A RETROSPECTIVE ANALYSIS
1Policlinico Universitario Campus Bio-Medico di Roma, Neurology, roma, Italy
2ASST Bergamo est, UOC Neurologia, Bergamo, Italy
3Università Politecnica delle Marche, Neurology, Ancona, Italy
4Università Campus Bio-Medico di Roma, Neurology, Rome, Italy
Background and Aims
Subjects with Migraine with Aura (MA) have an increased risk for stroke. We aimed at exploring if MA patients suffering from stroke display peculiar clinical stroke profiles and aura characteristics.
Methods
We retrospectively searched our hospital clinical electronic dossiers for patients younger than 60-year-old diagnosed an acute stroke at discharge and for MA patients who had undergone testing for patent foramen ovale (PFO). We defined three groups: stroke without MA history (S+MA-), stroke with MA history (S+MA+), MA patients (S-MA+). We collected vascular risk factors, the results of PFO detection tests, thrombophilic screening, stroke severity (NIHSS), and etiology. In S+MA+ and S-MA+ patients, onset age, type of aura, attack frequency, aura duration were also recorded.
Results
We found 175 stroke patients (6.3% were S+MA+ patients) and 105 S-MA+ subjects. S+MA+ patients were younger (p = .01), more frequently female (p = .026), and less frequently hypertensive (p = .049) than S+MA- patients. Moreover, S+MA+ patients presented a higher prevalence of PFO than (p < .0001) S+MA- patients and than (p = .034) S-MA+ subjects. S+MA+ patients were also characterized by a visual type of aura (p = .019). We found no difference with regard to MA frequency, duration or onset age.
Conclusions
Our study suggests that PFO represents a relevant pathogenetic mechanism subtending the increase in stroke risk in MA patients. No clinical phenotype of MA can help physicians to individuate patients at risk. Although the screening for PFO detection is not advisable in all MA patients, future studies are warranted to circumstantiate patients where it can have clinical value.
Trial registration number
N/A
E-Poster Discussion-Haemorrhagic Stroke II
AS24-033
AMYLOID LOAD AND STRUCTURAL BRAIN ALTERATIONS IN LOBAR MICROBLEED-ONLY PATIENTS AND CEREBRAL AMYLOID ANGIOPATHY RELATED LOBAR INTRACEREBRAL HEMORRHAGE
11, Massachusetts General Hospital- Stroke Research Center, Boston, USA
22, Massachusetts General Hospital- Department of Radiology, Boston, USA
33, Massachusetts General Hospital- Department of Emergency Medicine, Boston, USA
Background and Aims
The aim of this study was to compare the measures of structural brain damage and amyloid load between patients who presented with lobar microbleeds on MRI but no ICH (LMB-only) and cerebral amyloid angiopathy related lobar intracerebral hemorrhage (CAA-ICH).
Methods
Standard MRI markers (LMB counts, cortical superficial siderosis, enlarged perivascular spaces) and Freesurfer-based volumetric analysis (Gray Matter Volume[GMV], White Matter Volume[WMV], and White Matter Hyperintensity volume[WMHv]) were obtained in 37 LMB-only, 78 CAA-ICH patients and 78 age-matched healthy controls (HC). Pittsburgh Compound B-Positron Emission Tomography (PiB-PET) measures of amyloid deposition were also compared between LMB-only and CAA-ICH patients.
Results
Age, vascular risk factors and standard MRI markers of CAA were not different between LMB-only and CAA-ICH patients (all p>0.2). WMHv was higher in LMB-only and CAA-ICH when compared to HC (both p < 0.001) but lower in LMB-only compared to CAA-ICH patients (p = 0.026). WMV and GMV were significantly lower (p < 0.001, p = 0.003, respectively) in CAA-ICH patients compared to HC. WMV was significantly lower in LMB-only patients (p = 0.001) while GMV was not different from HC. Global amyloid load was similar between LMB-only (1.34 ± 0.18) and CAA-ICH (1.34 ± 0.23) patients (p = 0.958).
Conclusions
Similar distribution of amyloid load and hemorrhagic markers between LMB-only and CAA-ICH suggest that vascular amyloid is the predominant microangiopathy in LMB-only patients. The lower WMHv and relatively higher GMV in LMB-only suggest that this condition represents an earlier stage of CAA, that might preferentially benefit from therapeutic interventions such as amyloid lowering.
Trial registration number
N/A
AS24-042
LOBAR LACUNES ARE ASSOCIATED WITH FUTURE INTRACEREBRAL HEMORRHAGE RISK IN CEREBRAL AMYLOID ANGIOPATHY
1Massachusetts General Hospital, Stroke Research Center, Boston, USA
2Massachusetts General Hospital, Department of Emergency Medicine, Boston, USA
Background and Aims
Recent studies have reported the association of lacunar infarcts located in subcortical regions (lobar, as opposed to deep lacunes) with Cerebral Amyloid Angiopathy (CAA). We aimed to investigate whether the presence of lobar lacunes (LL) predicts future symptomatic lobar intracerebral hemorrhage (L-ICH) in patients with CAA.
Methods
The study included 108 prospectively enrolled patients diagnosed with probable CAA, who had multimodality neuroimaging and long-term biannual follow up. Demographics, vascular risk factors, standard MRI markers (lacunar infarcts, microbleeds, cortical superficial siderosis, leukoaraiosis) and follow-up data for L-ICH were reviewed. Adjusted Cox regression models were used to investigate the associations between the LL and the risk of future L-ICH.
Results
Twenty-five patients (23.1%) had LL whereas only 1 patient had a deep lacune. Nineteen patients (17.6%) experienced L-ICH during a median follow-up of 30 months [IQR 14–55 months]. In univariate analyses, age and presence of LL were associated with occurrence of L-ICH during follow-up (p = 0.033, p = 0.016 respectively). In a Cox regression model, the presence of LL was independently associated with increased ICH risk, after adjusting for age, hypertension, presence of cortical superficial siderosis, lobar microbleed count, and presence of ICH before the index event (hazard ratio: 2.94; 95% CI: 1.05–8.25; p = 0.040).
Conclusions
Our findings not only confirm the previously reported high prevalence of LL in CAA patients but also indicate that LL is associated with an increased risk of future symptomatic ICH in this population. These results have implications both for current clinical practice and future research.
Trial registration number
N/A
AS24-040
INITIATION OF ANTIPLATELET THERAPY AFTER SPONTANEOUS INTRACEREBRAL HEMORRHAGE
1Weill Cornell Medicine, Neurology, New York, USA
2Massachusetts General Hospital, Neurology, Boston, USA
3Yale University School of Medicine, Neurology, New Haven, USA
4Johns Hopkins University, Brain Injury Outcomes Center, Baltimore, USA
5Columbia University College of Physicians and Surgeons, Neurology, New York, USA
Background and Aims
Antiplatelet therapy (APT) after intracerebral hemorrhage (ICH) alleviates the thromboembolic risk without increasing the risk of recurrent ICH. Given the paucity of data on the relationship between initiation of APT after ICH and functional outcomes, we sought to study this association in a multicenter cohort.
Methods
We meta-analyzed individual patient data from: (1) the Massachusetts General Hospital (MGH) ICH registry (n = 1,854), (2) the Virtual International Stroke Trials Archive (VISTA-ICH) database (n = 762), and (3) the Yale stroke registry (n = 185). Our time varying exposure was initiation of antiplatelet therapy after ICH. Our outcomes, assessed at 90 days, were all-cause mortality and major disability or death (modified Rankin Score 4–6). We used Cox regression analyses adjusting for age, sex, admission ICH volume, hematoma location, presence of intraventricular hemorrhage, prior antiplatelet therapy, and pre-morbid mRS.
Results
We included a total of 2,801 ICH patients of whom antiplatelet therapy was initiated in 288 (10.3%) patients. The median times to initiation of APT were 11 days (interquartile range, [IQR], 7–15), 39 days (IQR, 11–66), and 7 days (IQR, 5–15) in the MGH, VISTA-ICH and Yale cohorts, respectively. In Cox models adjusted for confounders, APT after ICH was not associated with 90-day mortality (hazard ratio [HR], 0.85; 95% confidence interval [CI], 0.66–1.10) or 90-day death or major disability (HR, 0.83; 95% CI, 0.59- 1.16).
Conclusions
Initiation of APT after ICH was not associated with mortality or major disability at 90 days. The variation in clinical practice regarding timing of APT after ICH supports the need for randomized controlled trials.
Trial registration number
N/A
AS24-088
BURDEN OF HYPERTENSION-RELATED GENETIC RISK ALLELES INFLUENCES AGE-OF-ONSET IN SPONTANEOUS INTRACEREBRAL HEMORRHAGE
1Yale School of Medicine, Department of Neurology, New Haven, USA
2Beth Israel Deaconess Medical Center, Department of Neurology, Boston, USA
3Mayo Clinic, Department of Neurology, Jacksonville, USA
4University of Michigan Medical School, Department of Neurology, Ann Arbor, USA
5University of Virginia School of Medicine, Department of Neurology, Charlottesville, USA
6University of Washington School of Medicine, Department of Neurology, Seattle, USA
7Krakow University Hospital, Department of Neurology, Krakow, Poland
8Medical University of Graz, Department of Molecular Biology and Biochemistry, Graz, Austria
9Institut Hospital del Mar d’Investigacions Mèdiques, Neurovascular, Barcelona, Spain
10Neurovascular Research Laboratory, Neurovascular Genetics, Barcelona, Spain
11Lund University, Department of Neurology, Lund, Sweden
12Jagiellonian University, Department of Neurology, Krakow, Poland
13University of Cincinnati College of Medicine, Department of Neurology, Cincinnati, USA
14Harvard Medical School, Department of Neurology, Boston, USA
15Massachusetts General Hospital, Department of Neurology, Boston, USA
16Wake Forest School of Medicine, Department of Biostatistical Sciences, Winston-Salem, USA
17Yale School of Medicine, Department of Internal Medicine, New Haven, USA
Background and Aims
Genetically determined high blood pressure influences risk of intracerebral hemorrhage (ICH). We hypothesize that higher numbers of hypertension-related genetic risk variants lead to ICH at a younger age.
Methods
We performed a case-only study utilizing publicly available individual-level data from European-ancestry ICH cases enrolled in three genetics studies. We used independent single nucleotide polymorphisms (SNPs) shown in prior studies to associate with high blood pressure at p < 5x10−5 to create polygenic risk scores (PRSs), calculated as the sum of the alleles of interest multiplied by each allele’s effect on systolic (SBP) or diastolic (DBP) blood pressure. We used these PRSs as independent variables in linear regression models for ICH age-of-onset.
Results
A total of 1,282 ICH cases (mean age 71 [SD 13], 589 females [46%]) were included in the study. We used 234 SNPs for SBP and 214 SNPs for DBP to construct separate PRSs. Each standard deviation increase of the PRS was associated with a 0.76 year decrease in age-of-onset when considering SBP (beta -0.76, SE 0.33; p = 0.02) and with a 0.90 year decrease when considering DBP (beta -0.90, SE 0.33; p = 0.006). After stratifying by ICH location, the association remained significant for deep hemorrhages when considering both SBP (beta -0.92, SE 0.47; p = 0.05) and DBP (beta -1.13, SE 0.46; p = 0.02).
Conclusions
The genetic load of hypertension-related risk alleles is negatively correlated with age-of-onset of ICH, especially in deep ICH locations. This genetic information could be used to identify young individuals at risk of stroke who may benefit from more aggressive preventive interventions.
Trial registration number
N/A
AS24-084
QUANTIFICATION OF THE LEAK RATE OF THE SPOT SIGN IN MULTI-PHASE CT ANGIOGRAM STRONGLY PREDICTS INTRACRANIAL HEMORRHAGE GROWTH
1University of Calgary, Department of Clinical Neurosciences, Calgary, Canada
2University of Calgary, Department of Clinical Neurosciences- Community Medicine, Calgary, Canada
3University Ostrava, Department of Neurology, Ostrava, Czech Republic
4National Institute of Mental Health and Neurosciences, Department of Neurology, Bengaluru, India
5Hospital Universitari Vall d’Hebron, Department of Neurology, Barcelona, Spain
6University of Calgary, Department of Radiology, Calgary, Canada
Background and Aims
CTA spot signs are imaging predictors of ICH expansion. They vary in timing of appearance and may enlarge over time. Multiphase CTA (mCTA) identifies spot sign growth through 3 time resolved images. We sought to quantitate spot sign growth over 3 phases of mCTA and determine if it is associated with total hematoma expansion.
Methods
Data was from a single center (2012-2018) and included patients with CT confirmed intracerebral hemorrhage (ICH). In-house software (Quantomo) was used to measure spot sign of the spot sign (microliter) in 3 mCTA phases each mCTA phase blinded to measurement volumetric analysis of total (ICH+IVH) hematoma volume (ml) at baseline CT and follow-up CT/MRI.
Results
164 patients [60% male, mean age 67 yrs NIHSS 7, median onset-to-CT 4.48 hrs were included. Median baseline ICH volume was 17.34 ml (IQR 5.25, 29.9). Amongst all subjects spot sign detected by mCTA phase in 17% 1st, 23.2% 2nd, and 22.6% 3rd. Median ICH growth was 14.2 ml with phase 1 spot vs. 10. ml with phase 2 or 3 spots vs. 0 ml with no spot. Figure 1 shows spot sign leak rate (microL/s) between phase 1 vs. 2 by hematoma growth. Phase 2 vs 3 graph was bimodal pattern.
Conclusions
Measurement of spot sign growth (“leak rate” in microl/s) on mCTA is a novel predictor of ICH growth and may identify an ICH subpopulation at risk for dramatic hematoma expansion ideal for STAT hemostatic treatment.
Trial registration number
N/A

E-Poster Discussion-Pathophysiology and Experimental Stroke
AS19-019
USE OF ARTIFICIAL INTELLIGENCE TO PREDICT VOLUME OF BRAIN AND INFARCTION GROWTH RATE; A STEP TOWARDS PRECISION MEDICINE
1Hamad Medical Corporation, Neuroscience, Doha, Qatar
2HAMAD MEDICAL CORPORATION, NEUROCIENCE, DOHA, Qatar
3University of Alberta, Neuroscience, Edmonton, Qatar
4Qatar University, KINDI Center for Computing Research, Doha, Qatar
Background and Aims
The final human brain infarction volume [IV] and infarction growth rate [IGR] are strong predictors of outcome. IGR is dynamic with varying speed of growth. The conventional mathematical techniques are unable to predict IV and IGR.
Methods
We prospectively collected data on acute ischemic stroke (AIS) patients treated by thrombolysis and/or mechanical thrombectomy between January 2014 and December 2016. IGR and IV were measured at baseline and 24-hour CT. For IGR, we assumed the stroke volume to be zero at stroke onset. IGR1 [Δvolume (IVCT1–0)/Δtime (timeCT1- stroke onset time)] and IGR2 [IGR2 = Δvolume/Δtime = (IVCT2- IVCT1)/(timeCT2- timeCT1)]. To quantify the difference between estimated IGR and actual IGR mean square error (MSE) was used
Results
134 consecutive patients with AIS following middle cerebral artery occlusion were treated. Mean time-to-treatment was 213.27 ± 227.12 minutes. Clot burden score [p = 0.003], time-to-treatment [p = 0.78] was inversely correlated with IGR, while IGR1 positively correlated with IGR2 [p = 0.067]. IGR2 was significantly higher with low collateral score [p = 0.001]. An unfavorable modified treatment in cerebral infarction score was significantly higher IGR2 compared to favorable score [p = 0.035]. ANFIS training and testing showed significant difference with better collateral score [p = 0.024] in testing group with lower IGR2 [p = 0.03]. ANFIS-based model was able to predict IGR2 and IV, calculated from predicted IGR 2, without any significant difference compared to original data [p = 0.001]. MSE was 8.95% with 91.05% accuracy.
Conclusions
We showed the potential to predict outcome and more effective patient selection for extended hours thrombectomy and hemicraniectomy in malignant strokes, a step towards precision medicine.
Trial registration number
N/A
AS19-004
WHOLE BRAIN FUNCTIONAL ULTRASOUND IMAGING MAPPING DURING STROKE OFFERS NEW INSIGHTS INTO THE LINKS BETWEEN SPREADING DEPOLARIZATION AND TISSUE INFARCTION
1Neuro-Electronics Research Flanders NERF- A Research Initiative by IMEC- VIB and KU Leuven, Laboratory of Neural Circuits, Leuven, Belgium
Background and Aims
Complex hemodynamic events such as spreading depolarizations (SD) occur during the acute phase of stroke and increase the damage of the brain tissue. SDs are poorly considered for prognosis while they may improve stroke outcome.A better understanding of ultra-early hemodynamic events remains critical to improve stroke outcome.
Methods
Functional ultrasound imaging continuously mapped entire rat brains subjected to mild or severe ischemia. Real-time imaging at high resolution (100µm, 400ms) provided a voxel-based cerebral blood volume analysis of stroke induced-hemodynamic changes covering 800 brain regions. Postmortem assessment was performed 24 hours after stroke and compared to imaging data.
Results
Within peri-ischemic territories, SDs have been detected spreading around the ischemic core. Their rising point was mostly located in normally perfused tissue at the front of the ischemic region. Later comparison of fUSi and tissue staining has enlightened a marked mismatch between the ischemic and infarcted territories where SDs were initially detected.
Conclusions
The comparison between fUSi data and postmortem assessment of the infarcted tissue using standard histological approach confirms the critical role of early SD-like events in the prediction of the size and the location of the late infarcted tissue. Modulating or even inhibiting SDs by targeting the region where they rise could protect the healthy tissue from infarction and so reduce infarct size and associated deficits. Finally, fUSi is a promising technology for high precision stroke mapping in preclinical studies that may lead to more relevant data for understanding the effect of neuroprotective therapies while reducing the number of animals.
Trial registration number
N/A
AS19-003
ARYL HYDROCARBON RECEPTOR MODULATES STROKE-INDUCED NEUROINFLAMMATION AND NEUROGENESIS IN THE ADULT MOUSE BRAIN
1National Yang-Ming University, Department and Institute of Physiology, Taipei, Taiwan R.O.C
2Taipei Veterans General Hospital- Taipei, Neurology, Taipei, Taiwan R.O.C
Background and Aims
The aryl hydrocarbon receptor (AhR) is a ligand-dependent transcription factor activated by environmental toxicants and endogenous tryptophan metabolites. Emerging evidence suggests that AhR activation may play a role in brain damage after acute stroke. However, its actions in poststroke neuroinflammation and neurogenesis remain unknown.
Methods
Conditional knockout of AhR from nestin-expressing neural stem/progenitor cells (AhRcKO) and wild-type (WT) mice were subjected topermanent middle cerebral artery occlusion (MCAO). WT mice were treated with either vehicle or the AhR antagonist 6,2’,4’-trimethoxyflavone (TMF, 5 mg/kg/day) intraperitoneally. The animals were examined at 2 and 7 days after MCAO.
Results
The AhR signaling pathway was significantly upregulated after stroke. Both TMF-treated WT and AhRcKO mice showed significantly decreased infarct volume, as well as improved sensorimotor and nonspatial working memory functions compared with their respective controls. Immunohistochemistry revealed that AhR was increased predominantly in activated microglia and astrocytes after MCAO compared with the normal controls. The TMF-treated WT and AhRcKO mice demonstrated significant amelioration of microgliosis and astrogliosis. Interestingly, these mice also showed augmentation of neural progenitor cell proliferation at the ipsilesional neurogenic subventricular zone (SVZ) and the hippocampal subgranular zone. In the peri-infarct cortex, the ipsilesional SVZ/striatum and the hippocampus, both the TMF-treated and AhRcKO mice demonstrated downregulated IL-1β, IL-6, IFN-γ, CXCL1, and S100β and concomitantly upregulated Neurogenin 2 and Neurogenin 1.
Conclusions
AhR activation following acute ischemic stroke modulates, at least partly, neuroinflammation and neurogenesis, and AhR inhibition may potentially benefit functional outcomes in association with anti-inflammatory and neurogenic effects.
Trial registration number
N/A
AS19-015
RELATIONSHIP BETWEEN ‘ON-TREATMENT PLATELET REACTIVITY’ STATUS, SHEAR STRESS AND CEREBRAL MICRO-EMBOLIC SIGNALS IN ASYMPTOMATIC AND SYMPTOMATIC CAROTID STENOSIS: THE HAEMOSTASIS IN CAROTID STENOSIS STUDY
1The Adelaide and Meath Hospital, Neurology, Dublin, Ireland
2St Vincent’s University Hospital, Neurology, Dublin, Ireland
3The Adelaide and Meath Hospital, Vascular Surgery, Dublin, Ireland
4The Adelaide and Meath Hospital, Medicine for the Elderly/Stroke Service, Dublin, Ireland
5St James Hospital, Medicine for the Elderly/Stroke Service, Dublin, Ireland
6St James Hospital, Vascular Surgery, Dublin, Ireland
7Royal College of Surgeons in Ireland, Molecular and Cellular Therapeutics, Dublin, Ireland
8Royal Free Hampstead NHS Trust, University Department of Surgery, London, United Kingdom
9St James Hospital, Centre for Advanced Medical Imaging, Dublin, Ireland
10The Adelaide and Meath Hospital, Vascular Neurology Research Foundation and Department of Neurology, Dublin, Ireland
Background and Aims
Background
Assessing ‘high on-treatment platelet reactivity’ (HTPR) status could enhance understanding of the pathogenesis of vascular events in carotid stenosis patients on antiplatelet therapy.
Methods
This prospective, multicentre study assessed aspirin-HTPR status and its relationship with micro-emboli signals (MES) in asymptomatic versus symptomatic ≥50-99% carotid stenosis patients on aspirin monotherapy or combination therapy. Platelet function/reactivity was assessed under ‘moderately-high shear stress’ with the PFA-100® and ‘low shear stress’ with VerifyNow® and Multiplate® analysers. Bilateral 1-hour transcranial Doppler ultrasound of the middle cerebral arteries classified patients as MES+ve or MES-ve.
Results
Data from 30 asymptomatic patients were compared with 42 symptomatic patients in the ‘early phase’ (≤4 weeks) and 36 of these patients in the ‘late phase’ (≥3 months) after TIA/ischaemic stroke. Median daily aspirin doses were higher in early symptomatic (225mg;P<0.001) but not late symptomatic (75mg;P = 0.62) vs. asymptomatic patients (75mg). There was a lower prevalence of aspirin-HTPR in early (28.6%;P = 0.028) but not late symptomatic (38.9%;P = 0.22) compared with asymptomatic patients (56.7%) on the PFA-100®, but not on the VerifyNow® or Multiplate® (P≤0.53). Early symptomatic patients had a higher prevalence of aspirin-HTPR on the PFA-100® (28.6%) vs. VerifyNow® (9.5%;P = 0.049) but not Multiplate® assays (11.9%, P = 0.10). There were no differences in aspirin-HTPR prevalences between early or late symptomatic vs. asymptomatic MES+ve or MES-ve subgroups.
Conclusions
Recently symptomatic moderate-severe carotid stenosis patients had a lower prevalence of aspirin-HTPR than their asymptomatic counterparts on the PFA-100®, likely related to higher aspirin doses. Aspirin-HTPR prevalence was positively influenced by higher shear stress rates, but not MES status.
Trial registration number
N/A
AS19-012
ATHEROSCLEROTIC PLAQUE LOCATION MAY BE RELATED TO GEOMETRY OF CAROTID ARTERY AND DIFFERENT PATTERN OF ISCHEMIC LESION
1Ewha Womans University College of Medicine, Department of Neurology, Seoul, Republic of Korea
2Kyung Hee University College of Medicine, Department of Neurology, Seoul, Republic of Korea
3Kyung Hee University College of Medicine, Department of Radiology, Seoul, Republic of Korea
Background and Aims
Atherosclerotic plaque of internal carotid artery (ICA) is an important cause of anterior circulation infarction. We hypothesized that the geometry of ICA and the lesion pattern of cerebral infarction would be associated with the location of carotid plaque.
Methods
From January 2013 through December 2017, acute ischemic stroke patients with symptomatic proximal ICA disease were enrolled. The location of carotid plaque was divided to high-apical and low-body type. The geometric parameters of carotid artery were measured and ischemic lesion patterns were classified according to the number, location, and size of lesion. Clinical, geometric parameters, and ischemic lesion patterns were compared between the high-apical and low-body type plaques.
Results
One hundred patients (36 patients with high-apical type and 64 patients with low-body type) were studied. Distal ICA-external carotid artery (ECA) angle was narrower in patients with low-body type than high-apical type plaques (22.8 ± 10.0 vs. 31.3 ± 16.0, p = 0.005). Small scattered lesion was more frequently observed in low-body type plaque (p = 0.029), whereas confluent plus additional lesion were frequently observed in high-apical type plaque (p = 0.002). Low-body type plaques were independently associated with single or multiple small lesions (p = 0.017).
Conclusions
The narrow ICA-ECA angle is associated with low-body type plaque of carotid artery. A stroke with high-apical type plaque more appears with a large (diameter > 15mm) lesion, whereas low-body type plaque more appears with small sized lesions.
Trial registration number
N/A
E-Poster Discussion-Service Organisation
AS12-010
AGE DIFFERENCES IN THE USE OF HEALTH CARE RESOURCES FOR ACUTE ISCHEMIC STROKE- RESULTS FROM THE FEDERAL GERMAN DRG STATISTICS
1Klinikum Dortmund, Neurology, Dortmund, Germany
2Alfried Krupp Krankenhaus, Neurology, Essen, Germany
3drg-market, na, Osnabrück, Germany
4Katholische Kliniken Ruhrhalbinsel, Neurology, Essen, Germany
5University of Perugia, Neurology, Perugia, Italy
6University of Heidelberg, Neurology, Heidelberg, Germany
7Universityhospital St. Josef-Hospital, Neurology, Bochum, Germany
Background and Aims
The federal database of DRG statistics contains over 1.25 million hospitalized strokes for the years 2013–2017.
Methods
Here, the temporal evolution of access to stroke unit care (SU), intravenous thrombolysis (IVT), mechanical thrombectomy (MT), early rehabilitation, and in-hospital mortality were analyzed. Additionally, age related differences of access to stroke care were analyzed for 2017 (<80y vs ≥80y and within predefined cohorts). P-values of <0.001 were considered as statistically significant.
Results
From 2013 to 2017, SU access increased significantly from 66.8% to 73.5%, as did rates of IVT (12.4% to 15.9%) and MT (2.4% to 5.8%). Access to early rehabilitation and mortality rates did not differ significantly. SU access was significantly lower in older age (75.2%<80y vs 70.6%≥80y), whereas transfer to early rehabilitation was significantly more frequent in older age (11.7%<80y vs 22.2%≥80y). Moreover, recanalizing therapies were significantly higher in younger age (IVT 16.2%<80y vs 15.4%≥80y; MT 6.0%<80 y vs 5.5%≥80y). Finally, there was a significant increase of in-hospital mortality with increasing age.
Conclusions
Access to SU care, IVT, MT, and early rehabilitation were increasing in Germany from 2013 to 2017. SU admissions were lower in higher age, still remaining on a fairly high level (>70% in ≥80y). In contrast, older patients were significantly more frequent transferred to early rehabilitation. Despite significant differences in recanalizing treatment rates, an overall high access rate to IVT of > 15% and to MT of >5.5% was documented in both age groups in 2017. In house mortality after stroke increased with age.
Trial registration number
N/A
AS12-011
THE STOCKHOLM STROKE TRIAGE STUDY – MODELLING OUTCOMES FOLLOWING THE IMPLEMENTATION OF A NOVEL PREHOSPITAL TRIAGE SYSTEM
1Karolinska University Hospital, Department of Neurology, Stockholm, Sweden
2Karolinska Institutet, Departent of Clinical Neuroscience, Stockholm, Sweden
3University of Calgary, Department of Community Health Sciences, Calgary, Canada
4University of Calgary, Hotchkiss Brain Institute, Calgary, Canada
5Dalhousie University, Department of Industrial Engineering, Halifax, Canada
6University of Calgary, Department of Clinical Neurosciences, Calgary, Canada
Background and Aims
The Stockholm region (2.3M population, 6519 km2) is served by one comprehensive and six primary stroke centres (CSC, PSC). In 2017–2018 we accelerated delivery of endovascular thrombectomy (EVT) by 66 minutes by implementing the novel prehospital Stockholm Stroke Triage System (SSTS) for PSC bypass, based on symptom severity and ambulance-hospital teleconsultation. We modelled its effects on clinical outcomes and compared with the validated Ambulance Clinical Triage-For Acute Stroke Treatment (ACT-FAST) algorithm.
Methods
Conditional probability modelling was used to predict the probability of excellent outcome (mRS 0–1) for mothership and drip-and-ship strategies, before and after SSTS implementation, comparing with ACT-FAST. Predictive values for large artery occlusion (LAO) and non-LAO stroke, intracerebral hemorrhage, and stroke mimics, were combined with efficacy decay of thrombolysis and EVT, real-life proportions of EVT- and IVT-treated patients, and pre-, intra-, and inter-hospital workflow time metrics for Stockholm ambulances and hospitals, before and after SSTS implementation.
Results
The mothership approach is predicted to produce superior outcomes compared to drip-and-ship in the largest part of the Stockholm Region. The area of mothership superiority has increased following a 2017–2018 shortening of onset-to-groin time for EVT patients from 203 min (n = 108) to 137 min (n = 119). ACT-FAST was predicted to give nearly identical results for geographic superiority of mothership over drip-and-ship.

Conclusions
The 2017–2018 implementation of a novel prehospital stroke triage system combining symptom severity and teleconsultation, is predicted to result in superior outcomes using the mothership approach in all but the most remote parts of the Stockholm Region.
Trial registration number
N/A
AS12-007
MACHINE LEARNING OF SENTIMENTS EXPRESSED IN YOUTUBE PUBLIC AWARENESS CAMPAIGNS -STROKE
1Monash Health, Neurosciences, Clayton, Australia
2Peninsula Health, Medicine, Frankston, Australia
3Monash University, Medicine, Clayton, Australia
Background and Aims
Public education campaigns to recognise the signs and symptoms of stroke are necessary as treatments are time dependent. Social media (YouTube) has been used for this purpose. In this study we use machine learning approach to examine these Australian campaigns against exemplar 2006 campaign in North America (Stroke Heroes Act Fast). Further we explore the sentiment in the North American campaign to evaluate social media responses.
Methods
The number of views and comments on these videos were extracted from YouTube application programming interface (API). Natural language processing steps consisted of stripping number, punctuations, stop words and parsing comments into separate sentences. Sentiment analysis of the words were performed using National Research Council (NRC) word emotion association lexicon.
Results
Over 5 campaigns (2009-2015), there were 14895 views (0.06360597% of the Australian population) and 1 comment on videos (xK1Qf0MTIRU [re-enactment of a stroke], RBaMgsSKzCc [title: Know the warning signs], MmoGeCXov [title: Join the Fight Stroke], 7pbdKLOHNU [title: Fire in the Brain] and xA-P5voEik8 [title: FAST Train]). The exemplar campaign from North America (YHzz2cXBlGk) has 406,253 views (0.12% of North American population) and 123 comments. Sentiment expressed include trust (25.7%), fear (22.4%), joy (20.2%), sadness (20.8%), surprise (7.1%), anticipation (21.3%), disgust (4.9%), anger (4.4%), negative (30.1%) and positive (44.8%).
Conclusions
The Australian social media campaigns have not garnered as many views or comments compared to Exemplar campaign. The overwhelming positive sentiment in the North American campaign provides clue for developing material on social media for education.
Trial registration number
n/a
AS12-044
LARGE VESSEL OCCLUSION PATIENTS WITH MILDER BASELINE SYMPTOMS HAVE BETTER COLLATERALS AND LESS HARM FROM TRANSFER DELAYS
1Royal Melbourne Hospital, Neurology, Melbourne, Australia
2Royal Adelaide Hospital, Neurology, Adelaide, Australia
3Royal Melbourne Hospital, Radiology, Melbourne, Australia
4Leiden University Medical Centre, Neurology, Leiden, The Netherlands
Background and Aims
Severity-based clinical triage tools, aimed to allocate suspected large vessel occlusion (LVO) patients at risk of requiring thrombectomy to comprehensive stroke centers, miss a proportion of patients with milder symptoms. Our hypothesis was that LVO patients with milder symptoms have better collateral quality and less impact of delayed thrombectomy due to inter-hospital transfer on functional outcome, as compared to patients with more severe symptoms.
Methods
We compared pre-thrombectomy CT-perfusion markers of collateral circulation, including cerebral blood flow (CBF)<30% volume and hypoperfusion intensity ratio (HIR) between patients with National Institutes of Health Stroke Scale (NIHSS)<10 and ≥10 in thrombectomy patients admitted to the Royal Melbourne Hospital 2007–2018. The association between transfer and functional outcome (90-day modified Rankin Scale, mRS) adjusted for age, sex, site of occlusion and reperfusion, was compared between patients with NIHSS<10 and ≥10 using logistic regression.
Results
Of 607 patients, 111(18.3%) had NIHSS<10. Patients with NIHSS<10 had smaller baseline CBF<30% volume (median 5.5 vs 17mL, p < 0.001) and lower HIR (0.33 vs 0.49, p < 0.001), indicating better collaterals. For mRS/0/1/return-to-baseline, there was a significant transfer-by-NIHSS (<10/≥10) interaction (p = 0.0001), NIHSS≥10 patients: adjusted odds ratio, aOR = 0.647 (95% CI, 0.40 – 1.06); NIHSS<10 patients: aOR = 0.896 (0.32 – 2.53); Ordinal logistic regression analysis demonstrated a shift towards higher mRS score for transfer patients with NIHSS≥10 (p = 0.02), but not for transfer patients with NIHSS<10 (p = 0.95).

Conclusions
Thrombectomy patients with lower baseline NIHSS have better collateral circulation. Delays due to inter-hospital transfer were not significantly associated with worse outcome for these patients, mitigating the reduced sensitivity of triage tools in milder patients.
Trial registration number
N/A
AS12-078
DIRECT PRESENTATION VERSUS TRANSFER FROM A PRIMARY STROKE CENTER OF PATIENTS WITH A CONTRAINDICATION FOR IV THROMBOLYSIS
1Amsterdam University Medical Centers- location AMC, Department of Neurology, Amsterdam, The Netherlands
2Erasmus MC University Medical Center, Department of Neurology and Department of Public Health, Rotterdam, The Netherlands
3Amsterdam University Medical Centers- location AMC, Department of Radiology and Nuclear Medicine, Amsterdam, The Netherlands
4Emergency Medical Services, North-Holland North, Alkmaar, The Netherlands
5Sint Antonius Ziekenhuis, Department of Neurology, Nieuwegein, The Netherlands
6Erasmus MC University Medical Center, Department of Neurology, Rotterdam, The Netherlands
Background and Aims
Direct presentation of patients with acute ischemic stroke to a comprehensive stroke center (CSC) reduces time to endovascular thrombectomy (EVT), but may increase time-to-treatment for intravenous thrombolysis (IVT). This dilemma, however, does not apply to patients who have a contra-indication for IVT. We examined the effect of direct presentation to a CSC on outcomes after EVT in this subgroup.
Methods
We used data from the MR CLEAN Registry, a nationwide EVT-database (2014-2016). We included patients who did not receive IVT and compared those directly presented to a CSC to patients transferred from a primary stroke center (PSC). Outcomes included onset-to-treatment times and 90-day mRS, and we adjusted for potential confounders.
Results
We analyzed 219/1488 patients. 113 (52%) were directly presented to a CSC. Contra-indications for IVT included anticoagulation use (52%), recent clinical event with increased bleeding risk (14%), and presentation >4,5 hours after onset (12%). Directly presented patients had less ICA-occlusions (16% vs. 36%, p = 0.001), while percentages of M1- and M2-occlusions did not differ. The direct group had higher onset-to-first-door times (median 83 vs. 60 min, p = 0.004), but lower first-door-to-groin times (median 93 vs. 168 min, p < 0.001; linear regression: unstandardized B = 62.1, 95%CI:49.3–74.8) and onset-to-groin times (median 190 vs. 241 min, p < 0.001; linear regression: unstandardized B = 56.4, 95%CI:43.5–69.3). However, mRS score at 90 days did not differ between groups (adjusted OR:1.07, 95%CI:0.60–1.91).
Conclusions
In patients who are not eligible for IVT, onset-to-treatment times were substantially better for patients directly presented to a CSC, but without a measurable effect on clinical outcome.
Trial registration number
N/A
E-Poster Discussion-Multidisciplinary Care II
AS14-026
FAMILY MEMBERS’ EXPERIENCES OF DYSPHAGIA AFTER A STROKE: A QUALITATIVE STUDY OF FAMILY MEMBERS LIVING IN LONDON
1St George’s University of London, Faculty of Health- Social Care and Education, London, United Kingdom
Background and Aims
This study explored family members’ (FM) experiences of living with a loved-one with post-stroke dysphagia. Dysphagic patients may require family assistance to modify food/drink or administer tube-feeds. In previous survey studies, dysphagia-diagnosis increased FMs’ burden. However, FMs’ experiences were not explored.
Methods
This qualitative study used one-to-one interviews with FM, exploring their experiences. FM were asked open questions about eating routines, dysphagia onset, their role, and future-hopes. Interviews were audio-recorded and transcribed. Transcripts were analysed thematically, determining key features of FMs’ experiences.
Results
Five spouses aged 60–95 participated. Patients had had strokes three months-three years ago. Six themes arose: ‘I do all of it’; making sense of dysphagia; emotional responses; reflecting on relationships; redefining lifestyle; and things that help.
Interpretation
Post-stroke dysphagia affects the patient and spouse. FM often manage alone, once healthcare professionals (HCPs) completed input and where paid carers’ support was inconsistent. This sometimes led to feeling fully responsible for their loved-one’s survival. FM problem-solved dysphagia effectively, yet expressed concern around lack of understanding of its nature and prognosis. Maintaining lifestyle normality was important, although FM acknowledged the need for adjustments. Dysphagia was one of numerous factors affecting participants’ lives. FM found strong relationships, friends/family and faith/religion facilitated coping.
Conclusions
FM can feel solely responsible for their loved-one’s dysphagia. HCPs could provide ongoing support for families. Maintaining normality regarding pre-existing beliefs and eating routines is important. HCPs should consider these in dysphagia-recommendations. FMs’ perspectives of the relative impact of dysphagia differ. Inter-disciplinary professionals should explore patient/family priorities.
Trial registration number
N/A
AS14-027
NURSE-STAFFING IMPOSED PATIENT IMMOBILITY IN A MULTI-SITE COMPREHENSIVE STROKE CENTER SAMPLE: ARE US STROKE CENTERS STAFFING STROKE PATIENTS RESPONSIBLY?
1University of Tennessee Health Science Center at Memphis, Department of Neurology, Memphis- Tennessee, USA
2Good Samaritan Medical Center, Department of Neurology, San Jose- California, USA
3Baptist Medical Center, Department of Neurology, Jacksonville- Florida, USA
4Hershey Medical Center- Pennsylvania State University, Department of Neurology, Hershey- Pennsylvania, USA
Background and Aims
Progressive mobility is an important aspect of stroke care for hemodynamically stable patients. We aimed to understand the amount of time stable stroke patients with mobility orders spent out of bed (OOB) in an accredited U.S. Comprehensive Stroke Center (CSC) sample.
Methods
Ethics approval was obtained for an observational study in stable stroke patients with physician OOB orders. Observations were collected of patient activity/24-hours without alerting nursing staff to study aims. Data were analyzed to determine independent predictors of time OOB and hospital length of stay (LOS).
Results
Four participating CSCs produced 336 patient observations; 66% were ischemic stroke, 34% ICH, averaging 63 + 14 (median 59) years and 51% were female. Median NIHSS at time of observation was 7 (IQR 3–14). Registered nurse (RN) to patient staffing averaged 1 RN to 4.5 + 1.5 patients; nursing assistants were available 85% of the time to help with mobility. Patients were OOB on average 45 + 104 minutes per 24-hours. Both the number of patients assigned per nurse (coefficient -8.8; p = 0.016), and NIHSS score (coefficient -1.9; p = 0.026) were significant independent predictors of time OOB. Median LOS was 7 days (IQR 4–26); number of patients/RN (coefficient 4.4; p < 0.001), NIHSS (coefficient 1.35; p < 0.001), and age (coefficient -.35; p < 0.001) were significant independent predictors of hospital LOS. The nurse staffing cut-point best optimizing mobility was 1 RN to < 4 patients.
Conclusions
Stroke patients with mobility orders spend a significant time in bed. While disability severity is an important contributor, inadequate RN staffing is associated with unnecessary nurse-imposed patient immobility and increased LOS.
Trial registration number
N/A
AS14-025
QUICKLY HOME AGAIN - PATIENTS’ EXPERIENCES OF EARLY DISCHARGE AFTER MINOR STROKE
1Acute Stroke Unit, Department of Neurology- Aalborg University Hospital, Aalborg, Denmark
2Clinical Nursing Research Unit, Department of Orthopaedic Surgery- Aalborg University Hospital, Aalborg, Denmark
3Clinical Nursing Research Unit, Aalborg University Hospital & Department of Clinical Medicine- Aalborg University, Aalborg, Denmark
Background and Aims
Patients with minor stroke are discharged early from hospital due to centralisation of acute stroke treatment and accelerated care pathway. They experience psychological, physical and cognitive issues during transition and in the months after discharge. Little is known about how early discharge affects stroke patients’ experiences of the transition from hospital to home. The purpose of this study was to explore the patients’ experiences of early discharge within 72 hours after stroke onset.
Methods
A qualitative study consisting of semi-structured interviews with 11 patients experiencing first time stroke two-four weeks after discharge. Data were categorised and condensed using a hermeneutic phenomenological approach.
Results
Four themes emerged: 1) Shocked, yet grateful 2) Everyday life is changed 3) Managing uncertainty 4) Seeking new horizons. The patients struggled to identify themselves as having had a stroke. They strived to find a new everyday life but they were challenged by existential concerns, mental fatigue and the fear of having a new stroke. Questions and misunderstandings arose after the discharge and the patients expressed a need for health professionals to support them and discuss unclear issues. Patients searched for others with similar issues in order to find a new sense of self.
Conclusions
Despite minimal physical and cognitive symptoms patients with minor stroke struggle with everyday life after discharge. There is a need for support from health care professionals after discharge with specialised knowledge of stroke. Patients also need to be offered an opportunity to meet other patients with minor stroke.
Trial registration number
N/A
AS14-042
“QASC EUROPE” THE FIRST EXPERIENCE IN ITALY: THE OBSERVATIONAL STUDY PHASE AT THE SAN CAMILLO HOSPITAL AND ANALYSIS OF THE COLLECTED DATA
1San Camillo Forlanini Hospital, Health Professions Department, Rome, Italy
2San Camillo Forlanini Hospital, Stroke Unit, Rome, Italy
3Health Directorate of the Lazio Region, Hospital and Specialist Network Area, Rome, Italy
4San Camillo Forlanini Hospital, Emergency Department, Rome, Italy
Background and Aims
Approximately 15 million people worldwide suffer a stroke each year.1 There is compelling evidence that improved patient outcomes are achieved through early intervention in acute stroke care including thrombolysis, endovascular clot retrieval2 and access to specialised in-patient stroke units. Hyperglycaemia, swallowing dysfunction and elevated temperature are physiological variables known to be associated with poorer stroke outcomes. Optimal management of fever, hyperglycaemia and dysphagia have been identified in international guidelines as priorities for inpatient stroke management.
The Quality in Acute Stroke Care (QASC) Trial, has shown in the countries where the study was conducted that multidisciplinary, nurse-led interventions to manage fever, hyperglycaemia and swallow difficulties following acute stroke significantly improved health outcomes. Results showed that supported implementation of the Fever, Sugar, Swallow (FeSS) Clinical Protocols resulted in 16% decreased death and dependency at 90-days, and in-hospital
The Italian study was conducted at the San Camillo Forlanini Hospital in Rome, which is an important hub of the regional Stroke network
Methods
In the first phase, we proceeded to audit the medical records of (n ° 42) patients hospitalized from June to August 2018 with diagnoses of ICD 10 acceptance.
Results
It was found that the detection of temperature and blood sugar in the first 72 hours after admission is made occasionally, while great attention is paid to the detection of swallowing disorders secondary to stroke.
Conclusions
The first results confirmed the importance of this treatment’s role in the management of this pathology
Trial registration number
N/A
AS14-015
A CONTENT VALIDITY STUDY REVEALING LACK OF IMPORTANT ITEMS AND DIMENSIONS IN 11 COMMONLY USED INSTRUMENTS FOR MEASURING POST-STROKE FATIGUE
1Lovisenberg Diaconal Hospital, Medical Department, Oslo, Norway
2Institute of Health and Society- Faculty of Medicine- University of Oslo, Department of Nursing Science, Oslo, Norway
3Norwegian University of Science and Technology NTNU, Department of Neuromedicine and Movement Science, Trondheim, Norway
4University of California, Department of Family Health Care Nursing, San Francisco, USA
Background and Aims
Post-stroke fatigue (PSF) is the most common symptom three months after stroke, and this disabling condition have major negative influence on rehabilitation and activities in daily life. There exists no patient reported outcome measure (PROM) that is specifically developed to diagnose and assess PSF, in turn, researchers use a wide variety of fatigue PROMs. However, insufficient attention have been given to the content of these PROMs, and the aims of this study are to evaluate content validity in individual fatigue PROMs, and to identify similarities and differences through cross-comparison of PROMs.
Methods
We used a novel mixed-methods approach to evaluate content validity in fatigue PROMs. The items in eleven PROMs where subject of a qualitative analysis with the aim to group items as similar or different. Further we used Jaccard similarity coefficient to investigate degree of overlap between PROMs.
Results
After analysis of the 156 items in eleven PROMs, we found 83 different items, each representing a distinct attribute of fatigue. Several important PSF-specific items was lacking, such as the presence of pre-stroke fatigue. These PROMs do not take into account the multidimensional nature of PSF and the overall overlap between instruments was low.
Conclusions
The current PROMs lack the specificity needed to accurately discern PSF from other fatigue types. This could potentially lead to erroneous prevalence estimates and slow progress in research aiming to investigate the mechanisms and potential treatments of PSF. Thus, there is a high need for a new PROM tailor-made to diagnose and assess PSF specifically.
Trial registration number
N/A