
Abstract

-0012
PHARYNGEAL ELECTRICAL STIMULATION FOR EARLY DECANNULATION IN TRACHEOTOMISED STROKE PATIENTS WITH NEUROGENIC DYSPHAGIA (PHAST-TRAC): A PROSPECTIVE RANDOMISED SINGLE-BLINDED INTERVENTIONAL STUDY – SECONDARY OUTCOMES
1University Hospital Münster, Department of Neurology, Münster, Germany
2University Medical Centre Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, The Netherlands
3Schön Klinik Hamburg Eilbek, Zentrum für Neurologie und Neurorehabilitation, Hamburg, Germany
4University Hospital RWTH Aachen University, Section “Interdisciplinary Geriatrics”- Department of Neurology, Aachen, Germany
5Universitätsklinikum Gießen und Marburg GmbH, Neurologische Klinik, Gießen, Germany
6University of Milan-Bicocca, School of Medicine and Surgery, Milan, Italy
7Klinikum München Ost, Isar-Amper-Klinikum, Haar, Germany
8Median Klinik Berlin Kladow, Neurologische Rehabilitation, Berlin, Germany
9Vivantes Klinikum Neukölln, Neurologie, Berlin, Germany
10Kepler Universitätsklinikum, Klinik für Neurologie, Linz, Austria
11Phagenesis Limited, Department of Clinical Research, Manchester, United Kingdom
12University of Manchester and the Manchester Academic Health Sciences Centre, Centre for Gastrointestinal Sciences- Faculty of Biology- Medicine and Health, Manchester, United Kingdom
13National Hospital for Neurology & Neurosurgery, Therapy & Rehabilitation Services London, London, United Kingdom
14Kepler Universitätsklinikum, Klinik für Hals-- Nasen- und Ohrenheilkunde, Linz, Austria
15University of Nottingham, Stroke Trials Unit- Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
Dysphagia after stroke is common, especially in tracheotomised patients. In pilot trials, pharyngeal electrical stimulation (PES) reduced dysphagia after stroke.
Method
Dysphagic tracheotomised post-stroke patients were randomised to receive three days of PES or sham. The primary outcome was readiness for decannulation 24–72 hours after treatment. Patients with persisting dysphagia were then offered open-label PES. Additional predefined outcomes were adverse events (AEs), readiness for decannulation after receiving open-label PES, and length-of-stay in hospital. The trial was registered as ISRCTN18137204.
Results
The trial was stopped early for efficacy with 69 patients (PES 35, sham 34) randomised. PES was associated with more patients ready for decannulation then sham: 17 (48.6%) vs 3 (8.8%), odds ratio (OR) 7.00 (2.41–19.88), p = 0.00082). In predefined subgroups, significant interactions were present favouring PES in patients treated earlier after stroke, or with a shorter duration of mechanical ventilation. Open-label PES led 4 (26.7%) additional patients in the active group, and 16 (53.3%) in the sham group, to become ready for decannulation. Altogether, 58% of patients became ready for decannulation after PES. Treatment responders were discharged significantly earlier than non-responders: median 14 days [95% CI 12–15] vs. 36 days [95% CI 16–102] (p < 0.001). The proportion of patients with at least one SAE did not differ between the groups: 28.6% vs 22.9%, OR 1.30 (0.44–3.83), p = 0.79. No device-related SAEs were reported.
Conclusion
PES increased the proportion of patients with prior stroke and subsequent tracheotomy who were ready for decannulation, appeared safe and reduced hospital length of stay.
Trial registration number
ISRCTN18137204
-0014
VOJTA THERAPY IMPROVES POSTURAL CONTROL AND MOTOR FUNCTION IN EARLY REHABILITATION OF ACUTE STROKE PATIENTS – A RANDOMIZED CONTROLLED PILOT TRIAL
1Hospital Frankfurt Höchst, Department of Neurology, Frankfurt am Main, Germany
2University Hospital Heidelberg, Department of Neurology, Heidelberg, Germany
Background and Aims
Vojta therapy is a type physiotherapy that is based on reflex-locomotion and was originally developed for newborns with central coordination or spastic movement disorders. We thought to transfer the concept to adult patients with acute stroke. Vojta therapy has been reported to activate trunk and the deep muscles of the spine to regulate trunk stability and increase spinal rotation force, thereby enhancing postural control. We hypothesize, that Vojta therapy improves postural control and motor function in patients with ischemic stroke (IS) or intracerebral hemorrhage (ICH).
Method
We performed a randomized controlled, open-label, outcome-blinded trial. We included patients with imaging-confirmed IS or ICH, severe hemiparesis and randomly assigned them to Vojta therapy or conventional physiotherapy within 72 h after onset. Main exclusion criteria was restricted ability to communicate. Primary endpoint was the improvement of postural control measured by the trunk control test (TCT) on day 9 after admission.
Results
Between December 02, 2015 and July 05, 2017 we screened 778 and included 40 patients. Median age was 75 (66–80) years, 50% were women. The median improvement on TCT within 9 days was 25,5 points (=25,5%) (IQR 12,5–42,5) in the Vojta group and 0 (IQR 0–13) in the control group (p = 0,001). Secondary endpoints supported this result and will be presented.
Conclusion
This first randomized controlled trial of Vojta therapy in patients with IS or ICH demonstrates significant functional improvement by Vojta therapy compared to conventional physiotherapy at discharge. The longstanding effect of Vojta therapy needs to be proven in further trials.
Trial registration number
NCT 03035968
-0016
OPTIMIZING PATIENT SELECTION FOR ENDOVASCULAR TREATMENT IN ACUTE ISCHEMIC STROKE (SELECT): A PROSPECTIVE NON-RANDOMIZED MULTICENTER COHORT STUDY OF IMAGING SELECTION
1University of Texas at Houston, Neurology, Houston, USA
2Valley Baptist Medical Center, Neurology, Harlingen, USA
3Wellstar Health System, Neurology, Atlanta, USA
4University of Texas at Houston, Biostatistics, Houston, USA
5University of Alabama at Birmingham, Biostatistics, Birmingham, USA
6OhioHeatlh – Riverside Methodist Hospital, Neurology, Columbus, USA
7University of Kansas Medical Center, Neurology, Kansas City, USA
8Saint Louis University, Neurology, St. Louis, USA
9Florida Hospital, Neuroradiology, Orlando, USA
10Emory University, Neurology, Atlanta, USA
11Stanford University, Neurology, Stanford, USA
Background and Aims
Optimal imaging selection criteria for thrombectomy is unknown.
Method
In this prospective cohort study, consecutive anterior circulation LVOs up-to-24hours were enrolled, (1/16–2/18), at 9 centers. Patients received both NCCT and CTP with mismatch determination using RAPID software. Imaging selection modality was documented by treating physicians prior to thrombectomy. A blinded independent core-lab adjudicated imaging profiles (Good CT = ASPECTS ≥ 6, Good CTP = core-volume < 70 cc, mismatch-volume ≥10 cc and mismatch/ratio >1.2). The primary outcome (90day-mRS = 0–2) was compared between NCCT and CTP groups, and for different NCCT and CTP profiles.
Results
Of 445 enrolled, 341 received thrombectomy, 13% had ICA occlusions, 62%M1, and 18%M2. Physicians reported NCCT as selection modality in 41%, CTP in 59%, good outcome rates were similar (NCCT = 53.7% vs. CTP = 54.2%, aOR = 0.93, 95%CI = 0.39–2.26, p = 0.88).
86.7% had ASPECTS>6 and 88.8% had good perfusion profile (Table1) with comparable mRs = 0–2 (55.9% versus 58%, aOR = 2.37,95%CI = 0.51–10.92, p = 0.27). There was no interaction of imaging modality and outcome with time (0–6hrs versus 6–24hrs, p = 0.97).
17.6% would have been excluded from thrombectomy based on NCCT or CTP only; 42% of them had good outcome. 52.2% of patients who were excluded by NCCT but qualified by CTP had mRS = 0–2 after thrombectomy, and 27.8% of those excluded by CTP but were treated by NCCT had good outcome as compared to 27.3% and 0% of those with the same imaging profiles who did not receive thrombectomy. Thrombectomy did not confer good outcomes in patients with poor imaging profiles on both CT and CTP.


Conclusion
Good outcome rates were similar in CT versus CTP selected patients, however, both modalities excluded a similar number of patients who could potentially benefit from thrombectomy.
Trial registration number
NCT02446587
-0018
VARIATIONS IN PRACTICE PATTERNS AND OUTCOMES AFTER STROKE ACROSS COUNTRIES AT DIFFERENT ECONOMIC LEVELS: THE INTERSTROKE STUDY
1Glasgow Royal Infirmary, Academic Section of Geriatric Medicine, Glasgow, United Kingdom
2Health Research Board Clinical Research Facility- Department of Medicine, NUI Galway, Galway, Ireland
3Research Institute, St John’s Medical College, Bangalore, India
4Population Health Research Institute, McMaster University and Hamilton Health Sciences, Hamilton- ON, Canada
5Research Institute, Beijing Hypertension League Institute, Beijing, China
6Department of Cardiology, Instituto Dante Pazzanese de Cardiologia-, Sao Paulo, Brazil
7Research Institute, St John’s Medical College and Research Institute, Bangalore, India
8Division of Applied Medicine, University of Aberdeen, Aberdeen, United Kingdom
Background and Aims
Stroke increasingly affects people in low and middle-income countries (LMICs). Improvements in stroke care and outcomes have been reported in high income countries (HICs) but little is known about practice and outcomes in LMICs.
Method
We studied practice variations (treatments used and access to services) among INTERSTROKE study stroke patients. We supplemented individual patient data with a questionnaire about healthcare and service facilities at each participating hospital. Using multivariate regression analyses to account for patient case-mix and service clustering, we estimated the association between services available, treatments given, and patient outcomes (death or dependency) at one month.
Results
We obtained full information for 12,342 (92%) of 13,447 INTERSTROKE patients, from 108 hospitals in 28 countries; 2576 from 38 hospitals in 10 HICs and 9766 from 78 hospitals in 18 LMICs. LMIC patients more often (P < 0.0001) had severe strokes, intracerebral haemorrhage, poorer access to services, and lower use of investigations and treatments. Access to a stroke unit was associated (P < 0.0001) with improved use of investigations and treatments, access to other rehabilitation services, and improved survival without severe dependency (1.29; 1.14–1.44) which was independent of patient characteristics and other measures of care. Use of acute antiplatelet therapy was associated with improved survival (1.39; 1.12–1.72) irrespective of other patient and service characteristics.
Conclusion
Evidence based treatments, diagnostics, and availability of stroke units were less commonly available in LMICs. Access to stroke units and appropriate use of antiplatelet therapy were associated with improved recovery. Improved access to organised stroke care in LMICs are essential to improve outcomes.
Trial registration number
N/A
-0020
PUBLIC HEALTH AND COST CONSEQUENCES OF TREATMENT DELAYS IN ENDOVASCULAR THROMBECTOMY FOR STROKE BASED ON HERMES COLLABORATION DATA
1University of Calgary, Department of Radiology, Calgary, Canada
2University of Calgary, Department of Neurology, Calgary, Canada
3University of California-Los Angeles, Department of Neurology, Los Angeles, USA
4Erasmus MC- University Medical Center Rotterdam, Department of Neurology, Rotterdam, The Netherlands
5Academic Medical Center Amsterdam, Department of Neuroradiology, Amsterdam, The Netherlands
6University of Pittsburgh Medical Center, Department of Neurology, Pittsburgh, USA
7Hospital Germans Trias i Pujol, Department of Neurology, Barcelona, Spain
8University Hospital of Nancy, Department of Neurology, Nancy, France
9University of Melbourne, Department of Neurology, Melbourne, Australia
10Newcastle University, Department of Neurology, Newcastle, United Kingdom
11University of Glasgow, Department of Neurology, Glasgow, United Kingdom
12Altair Biostatistics, Altair Biostatistics, St Louis Park, USA
Background and Aims
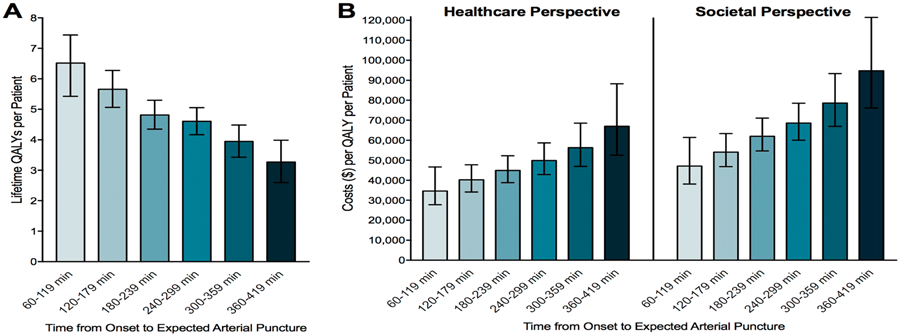
The benefit that endovascular thrombectomy (EVT) offers to stroke patients with large vessel occlusions is highly time-dependent. We determined the lifetime quality of life and cost consequences of delaying EVT administration.
Method
A Markov model estimated lifetime quality-adjusted life years (QALYs) of EVT-treated patients and associated costs based on puncture times. We applied United States healthcare and societal perspectives. Input parameters were based on best evidence (Table 1), including data from the HERMES collaboration. In addition to diminished outcomes with later EVT, the model also projects patients becoming EVT-ineligible over time.
Results
Lifetime QALYs decreased with time until puncture (Figure 1A). Within the first 6 hours, every hour of delay resulted in average losses of 0.65 QALYs. The healthcare and societal costs of each QALY yielded by EVT increased with time (Figure 1B). Within the first 6 hours, every hour of delay increased healthcare costs by $6,418/QALY and societal costs by $9,443/QALY. Within the first 3 hours, a treatment delay of 2 hours typically associated with drip-and-ship vs. mothership care delivery, would result in average losses of 1.7 QALYs per patient and extra healthcare and societal costs of $10,000/QALY and $15,000/QALY, respectively.
Conclusion
Every hour of delay reduces a patient's QALYs and substantially increases costs. Investments in improved pre-hospital triage and in-hospital workflow are likely to be highly cost-saving.
Trial registration number
N/A
0026
EFFECT OF INTRAVENOUS THROMBOLYSIS ON PATIENT REPORTED OUTCOME MEASURES IN STROKE PATIENTS WITH UNKNOWN TIME OF SYMPTOM ONSET – RESULTS OF RANDOMIZED, CONTROLLED WAKE-UP TRIAL
1Universitätsklinikum Hamburg-Eppendorf, Neurology, Hamburg, Germany
2Aarhus University, Neurology, Aarhus, Denmark
3Hospices Civils de Lyon, Service de Biostatistique, Lyon, France
4Hospices Civils de Lyon, Neurology, Lyon, France
5Medical Park, Neurology, Berlin, Germany
6Charité- Universitätsmedizin Berlin, Neurology, Berlin, Germany
7Universitätsklinikum Hamburg-Eppendorf, Neuroradiology, Hamburg, Germany
8University of Glasgow, Robertson Centre for Biostatistic, Glasgo, United Kingdom
9UZ Leuven, Neurology, Leuven, Belgium
10University of Glasgow, Institute of Neuroscience & Psychology, Glasgo, United Kingdom
11Institut d’Investgació Biomèdica de Girona IDIBGI, Radiology, Girona, Spain
12Florey Institute of Neuroscience and Mental Health, Neurology, Heidelberg, Australia
Background and Aims
There is a global trend towards evaluating the benefit of medical treatments on the basis of patient-reported outcome measures (PROMs). For intravenous thrombolysis, there is only scarce data on PROMs including health-related quality of life, and no such data is available with respect to IVT in patients with unknown time of symptom onset. WAKE-UP (Efficacy and safety of MRI-based thrombolysis in wake-up stroke: a randomised, double-blind, placebo-controlled trial) aimed at testing the efficacy and safety of MRI-guided IVT in ischemic stroke patients with unknown time of symptom onset. WAKE-UP also aimed at assessing the effect of thrombolysis on PROMs.
Method
WAKE-UP was an investigator initiated, European, multicentre, randomized, double-blind, placebo-controlled clinical trial. Patients with unknown time of symptom onset were studied by MRI. Patients with DWI-FLAIR-mismatch were randomised to either treatment with rtPA or placebo. As patient-centric secondary efficacy endpoints, PROMs were obtained 90 days after stroke including quality of life and functional health status assessed by the Euroqol-5D (EQ-5D), and depressive symptoms as assessed by the Beck Depression Inventory (BDI).
Results
A total of 503 patients were randomized in the trial. The primary endpoints of the trial will be presented in a separate talk. Here, specifically the effects of IVT on PROMs will be presented.
Conclusion
WAKE-UP is the first randomized controlled trial to provide information on the effect of IVT on patient-centric measures in stroke patients with unknown time of symptom. Trial results and their potential impact on clinical practice will be discussed.
Trial registration number
ClinicalTrials.gov number NCT01525290; EudraCT number 2011-005906-32
-0027
TELEREHABILITATION IN THE HOME VERSUS THERAPY IN-CLINIC FOR PATIENTS WITH STROKE
1University of California- Irvine, Neurology, Irvine, USA
2Chapman University, Physical Therapy, Irvine, USA
3University of California-Irvine, Institute for Software Research, Irvine, USA
4University of California-Irvine, Statistics, Irvine, USA
5Kessler Foundation, Stroke Rehabilitation Research, Saddle Brook, USA
6Kessler Institute for Rehabilitation, Stroke Rehabilitation, Saddle Brook, USA
7Case Western Reserve University, Physical Medicine and Rehabilitation, Cleveland, USA
8Burke Medical Research Institute, Brain Stimulation and Robotics Laboratory, White Plains, USA
9University of California-San Diego, Clinical Neurosciences, La Jolla, USA
10Brooks Rehabilitation Hospital, Physical Medicine and Rehabilitation, Jacksonville, USA
11Northwestern University, Physical Medicine and Rehabilitation, Chicago, USA
12University of Washington, Neurology, Seattle, USA
13Medical University of South Carolina, Health Science and Research, Charleston, USA
14Harvard University, Physical Medicine and Rehabilitation, Boston, USA
15Emory University, Rehabilitation Medicine- Division of Physical Therapy Education, Atlanta, USA
16Atlanta VA, Center for Visual and Neurocognitive Rehabilitation, Decatur, USA
Background and Aims
Occupational/physical therapy improves post-stroke outcomes in a dose-dependent manner. However, many patients receive suboptimal therapy doses for reasons that include cost, availability, and difficulty with travel. This problem is likely to increase with time given the aging population and increased post-stroke survival rates. Telehealth, defined as the delivery of health-related services and information via telecommunication technologies, can potentially address this unmet need. The current study examined the effect of a home-based telerehabilitation program designed to improve motor recovery and patient education in patients with stroke.
Method
Using a randomized, assessor-blinded, controlled, non-inferiority clinical trial, a total of 124 participants were enrolled across 11 US centers as part of the NIH StrokeNet clinical trials network. Entry criteria included arm motor deficits (arm motor Fugl-Meyer (FM) score 22-56 /66), stroke onset 4–36 weeks prior, and age ≥18. Those with significant depression, cognitive impairment, or communication deficits were excluded. Patients were randomized (1:1) to receive 6 weeks of intensive arm motor therapy either (a) in a traditional in-clinic setting or (b) via in-home telerehabilitation (rehabilitation services delivered to the subject's home via an internet-connected computer). Therapy intensity, duration, and frequency were matched across the two groups, with all participants assigned 36 sessions (18 supervised and 18 unsupervised), 80 minutes each (including a 10 minute break), over 6 weeks. The primary endpoint is within-subject change in FM score from the Baseline Visit to 30 Day Follow-Up Visit. Additional measures pertain to stroke education, secondary prevention, behavioral compliance, and patient motivation.
Results
Will-be-presented.
Conclusion
Will-be-presented.
Trial registration number
NCT02360488
-0029
LIFETIME BENEFIT AND COST CONSEQUENCES OF THE ACHIEVED GRADE OF REPERFUSION AFTER THROMBECTOMY FOR STROKE BASED ON HERMES COLLABORATION DATA
1University of Calgary, Department of Radiology, Calgary, Canada
2University of Calgary, Department of Neurology, Calgary, Canada
3University of California-Los Angeles, Department of Neurology, Los Angeles, USA
4Erasmus MC- University Medical Center Rotterdam, Department of Neurology, Rotterdam, The Netherlands
5Academic Medical Center- Amsterdam, Department of Neuroradiology, Amsterdam, The Netherlands
6University of Pittsburgh Medical Center, Department of Neurology, Pittsburgh, USA
7Hospital Germans Trias i Pujol, Department of Neurology, Barcelona, Spain
8University Hospital of Nancy, Department of Neurology, Nancy, France
9University of Melbourne, Department of Neurology, Melbourne, Australia
10Newcastle University, Department of Neurology, Newcastle, United Kingdom
11University of Glasgow, Department of Neurology, Glasgow, United Kingdom
12Altair Biostatistics, St Louis Park, St Louis Park, USA
Background and Aims
The benefit that endovascular thrombectomy (EVT) offers to stroke patients with large vessel occlusions depends strongly on reperfusion grade as defined by the eTICI (extended Thrombolysis in Cerebral Infarction) scale. We determined the lifetime health and cost consequences of reperfusion for patients, healthcare systems, and society.
Method
A Markov model estimated lifetime quality-adjusted life years (QALY) of EVT-treated patients and associated costs based on eTICI grades. The analysis was performed from a United States health care and societal perspective. Input parameters were based on best evidence, including patient data from the 7-trial HERMES collaboration. Starting age was set to 65 years. Sensitivity analysis was performed using Monte Carlo simulations.
Results
Lifetime QALYs increased for every grade of improved reperfusion (Figure 1A). On average, eTICI 3 resulted in 6.50 QALYs over the patients' lifetimes, whereas eTICI 2b (50-66%) yielded 4.80 QALYs. In contrast, healthcare and societal costs per QALY decreased by improved reperfusion (Figure 1B). The advantage of achieving eTICI 3 over eTICI 2b (50-66%) reperfusion results in average cost-savings of about $15,000/QALY and $20,000/QALY per patient incurred by healthcare systems and society.

Conclusion
Every grade of improved reperfusion grants stroke patients additional QALYs and substantially reduces healthcare and societal costs. Procedural strategies to achieve eTICI3 reperfusion should be assessed for safety and feasibility, even when initial reperfusion seems adequate.
Trial registration number
N/A
-0035
SOFTWARE-BASED, AUTOMATED CALCULATION OF THE ASPECT SCORE IN PATIENTS SUFFERING FROM EMERGENT VESSEL OCCLUSIONS IN THE ANTERIOR CIRCULATION – CLINICAL FEASIBILITY AND RELIABILITY
1Klinikum rechts der Isar, Department of diagnostic and interventional Neuroradiology, Munich, Germany
2Klinikum rechts der Isar, Department of Neurology, Munich, Germany
Background and Aims
The ASPECT Score has become the most widely used score for quantifying signs of infarction. Human readers are known to have a poor performance in recognizing early signs of infarction in CT. For the first time automatic tools for calculating the ASPECT score are available. One of these will be examined in the present work.
Method
In a first step, a gold standard was defined by two board certified neuroradiologists in 100 patients suffering from an occlusion in the anterior circulation in knowledge of the complete follow-up imaging. After 6 weeks, the ASPECT Score was again calculated by the two readers independently. In a final step, the CTs were analyzed using a commercially available software (RAPID-CT).
Results
Human readers showed a fair agreement with the gold standard (k = 0.574 and k = 0.556). RAPID-CT showed a significant better agreement (k = 0.896). If < 1h had passed between symptom onset and imaging, all readers showed only minimal agreement (Reader 1 & 2: k = 0.187 & k = 0.124; RAPID-CT: k = 0.169). RAPID-CT showed a substantial agreement (k = 0.775) after >1h, which increased to almost perfect agreement (k = 0.923) at the time window >4h. Human readers needed the >4h time interval to achieve similar results (k = 0.828 and k = 0.757).
Conclusion
Analysis of the ASPECT score with RAPID-CT is clearly superior to human readers. This is particularly the case in CTs with a small time interval between the onset of symptoms and imaging.
Trial registration number
N/A
-0036
TO SCAN OR NOT TO SCAN: FOLLOW-UP CT SCANNING FOR MANAGEMENT OF CHRONIC SUBDURAL HEMATOMA AFTER NEUROSURGICAL EVACUATION (TOSCAN) – A RANDOMIZED, CONTROLLED TRIAL
1University Hospital Bern, Neurosurgery, Bern, Switzerland
2University Hospital Bern, Neurology, Bern, Switzerland
3University Hospital Bern, Accounting, Bern, Switzerland
4University Hospital Bern, Neuroradiology, Bern, Switzerland
Background and Aims
Recurrence of chronic subdural hematoma after surgery is frequent. Scans after surgery show often substantial residuals, which may trigger re-operations. However, the benefit of post-surgical imaging for patient outcome remains unknown.
Method
We randomly assigned 361 patients with newly diagnosed chronic subdural hematoma, within 48 hours after surgery, to receive either clinical combined with radiological follow-up (CT scans 2 and 30 days after surgery; CT arm; n = 181) or clinical follow-up with scans only in case of neurological deterioration (no-CT arm, n = 180). The primary outcome was assessed after 6 months using the modified Rankin scale (mRS) with categorical scores ranging from 0 (no symptoms) to 6 (death).
Results
The proportion of patients who survived without severe disability (mRS 0–3) was 89% in the CT arm and 93% in the no-CT arm (OR 1.4, 95% CI 0.82-3.72, P = 0.15). Twelve patients in the CT arm and 8 patients in the no-CT arm died (P = 0.5). Re-operation for recurrent hematomas was performed in 59 patients in the CT arm and in 39 patients in the no-CT arm (P = 0.055). Complications occured in 26 patients in the CT arm and in 19 patients in the no-CT arm (P = 0.34). The follow-up protocol with CT imaging did not improve the primary outcome; the between-arm difference for mRS was not significant, neither as a categorical (P = 0.79) nor as a numerical variable (P = 0.37).
Conclusion
Routinely scheduled CT scans after neurosurgical evacuation of CSH are not superior to clinical neurological examination and CT scans only in case of clinical deterioration.
Trial registration number
NCT01624545
-0037
RELATIVE IMPORTANCE OF FACTORS INFLUENCING DECISION TO PROCEED WITH ENDOVASCULAR THERAPY IN STROKE PATIENTS RESULTS FROM AN INTERNATIONAL MULTIDISCIPLINARY SURVEY
1University of Calgary, Neurosciences, Calgary, Canada
2King Abdulaiziz University, Neurology, Jeddah, Saudi Arabia
3University of Calgary, Radiology, Calgary, Canada
4LMU Munich, Institute for Clinical Radiology, Munich, Germany
5University of Tennessee College of Medicine Chattanooga, Radiology, Chattanooga, USA
6Sree Chitra Tirunal Institute for Medical Sciences and Technology, Department of Neurology, Trivandrum, India
7Royal Melbourne Hospital, Department of Neurology, Melbourne, Australia
8The Royal Melbourne Hospital, Department of Radiology-, Melbourne, Australia
9University Hospital Bern, Neurology, Bern, Switzerland
10Mayo Clinic, Neurology, Rochester, USA
11Hyogo College of Medicine, Department of Neurosurgery, Nishinomiya, Japan
12Yonsei University College of Medicine, Department of Neurology, Seoul, Republic of Korea
13Yonsei University, Department of Radiology, Seoul, Republic of Korea
14Kovai Medical Center and Hospital, Radiology, Coimbatore, India
15Centre Hospitalier Universitaire de Lyon, Radiology, Lyon, France
16Bootstrap Analytics Inc., Principal, Calgary, Canada
17University of Clagary, Neurosciences, Calgary, Canada
18University of Toronto, Division of Neurology- Department of Medicine, Toronto, Canada
Background and Aims
What factors and their relative importance govern the selection for endovascular therapy (EVT) in real-world evidence are not well known.
Method
We conducted an international web-based survey to assess the decision to offer EVT. Ten key patient characteristics were used to construct case scenarios. Respondents saw ten pairs of patient scenarios, randomly generated from the ten patient characteristics and chose which patient (A or B or neither) was best suited for EVT according to their current practice. Hierarchical Bayes’ disaggregate discrete choice modelling was used to quantify the relative importance of patients’ characteristics in deciding to offer EVT.
Results
603 physicians (mean age 44 (SD 8.5) years, 83.5% men, 53.6% neurologists, 28.7% neuro-interventionists, 13.3% neurosurgeons, 4.7% other), from 38 countries participated. The most influential factor was the extent of ischemic change (ASPECTS/volume of infarct core) (26-28% of the choice). The next important factors were age, premorbid disability, baseline NIHSS score, and site of vessel occlusion (13-15% each). Time from onset was only modestly important (9%). Sex, carotid occlusion, comorbidities, and inconvenience (e.g. EVT at night) (1-3% each) were judged unimportant. Respondents were 17% less likely to favour treating a large M2 occlusion vs. M1, 53% less likely to favour treating low NIHSS score (≤5) vs. ≥11, and 74% less likely to favour treating low ASPECTS (≤4) patients or core >70cc vs. ASPECTS ≥8 or core < 30cc.
Conclusion
The extent of ischemic changes is a dominant factor in choosing EVT candidates. M2 occlusion is considered an appropriate EVT target.
Trial registration number
N/A
AS04-015
PHYSICAL ACTIVITY IN SUBACUTE STROKE – PHYS-STROKE
1University Medicine Greifswald, Neurology, Greifswald, Germany
2Charite, Neurology, Berlin, Germany
3Charite, Center for Stroke Research, Berlin, Germany
4Charite, 6 Department of Biostatistics and Clinical Epidemiology, Berlin, Germany
5Median Klinik Grünheide, Neurorehabilitation, Grünheide, Germany
6Beelitz-Heilstätten, Neurorehabilitation, Beelitz, Germany
7Vivantes Kliniken, Neurology, Berlin, Germany
8Evangelisches Geriatrie Zentrum Berlin, Geriatrics, Berlin, Germany
9Charite, Neurology, Belin, Germany
10Medical Park Berlin Humboldtmühle, Neurorehabilitation, Berlin, Germany
11Medical Park Berlin Humboldtmühle, Neurorehabiltation, Berlin, Germany
Background and Aims
Physical activity including treadmill-based, aerobic training is a rehabilitative therapy to improve walking abilities and functional outcome after stroke. The effect on activities of daily living of patients in the subacute phase of stroke is unknown [1].
Method
PHYS-Stroke was an investigator initiated, German, multicentre, randomized clinical trial [2]. 200 patients with subacute stroke (day 5–45 after stroke) were recruited from seven rehabilitation clinics, and randomized to receive 25 minutes of either treadmill-based, aerobic physical exercise (study intervention) or relaxation sessions (control intervention) five times per week for four weeks, in addition to standard rehabilitative therapy. Primary outcome was change of gait speed and the Barthel index at three months after stroke (co-primary endpoint). Safety endpoints were recurrent fatal or non-fatal cardiovascular events.
Results
A total of 200 patients was randomized in the trial (end of recruitment: April 30th, 2017; Database closed: Nov 10th, 2017), and will be included in the intention-to-treat analysis. Results for primary endpoints after 3 months will be presented, as well safety endpoints.
Conclusion
PHYS-Stroke is a clinical trial in the subacute phase adding relevant evidence to the question if aerobic training in subacute stroke improves gait speed and activities of daily life. Moreover, it will determine if the Intervention in the subacute phase after stroke is safe.
Trial registration number
ClinicalTrials.gov: NCT01953549
1. Physical fitness training for stroke patients. Cochrane Database Syst Rev, 2016.
2. Physical fitness training in Subacute Stroke (PHYS-STROKE)--study protocol for a randomised controlled trial. Trials, 2014.
Ongoing Trials Abstracts
-0008
CODE STROKE ALERT – DEVELOPMENT OF A NEW OPEN-SOURCE ELECTRONIC PLATFORM TO STREAMLINE ACUTE STROKE CARE
1Monash Health, Diagnostic Imaging, Melbourne, Australia
2Austin Health, Neurology, Melbourne, Australia
3Austin Health, Diagnostic Imaging, Melbourne, Australia
4Royal Melbourne Hospital, Diagnostic Imaging, Melbourne, Australia
5Northern Health, Diagnostic Imaging, Melbourne, Australia
6Monash University, Monash Institute of Medical Engineering, Melbourne, Australia
Background and Aims
Effective, time-critical intervention is crucial to mitigate stroke mortality and morbidity but is often hampered by systemic pre- or in-hospital delays. In the era of rapid reperfusion therapy for ischaemic stroke, there is urgent need to improve multi-disciplinary communication to synchronise and coordinate rapid clinical, imaging assessment, and therapeutic decision making across the entire stroke journey from initial emergency medical service (EMS) assessment to in-hospital management. We aim to develop an open-source platform that provides a purpose-built, efficient, user-friendly communication system that links EMS, stroke and neuro-interventional teams, aiming to reduce the time from first medical contact to cerebral reperfusion time.
Method
N/A
Results
The Health Insurance Portability and Accountability Act (HIPAA) compliant platform can be accessed by EMS and hospital staff involved in acute stroke care. When a new stroke alert is lodged by EMS, the application will prompt calculation of relevant clinical scores that aid decision making. An appropriate hospital is then recommended and pre-notified of impending stroke patient arrival. Empowered by geotagging, an estimated time of arrival is broadcast to all team members, ensuring effective communication between teams.
Conclusion
Code Stroke Alert will be available free to health networks globally to improve quality and timeliness of stroke care. Its open-source nature may promote future development of plug-ins and add-ons based on individual institutional needs, e.g. for Hospital Information System (HIS) or Picture Archive Communication System (PACS) integration. Furthermore, data logs are created, with an auditable trail of relevant quality improvement metrics with a view to overall system quality improvement.
Trial registration number
N/A
AS32-0008
PARAMEDIC ACUTE STROKE TREATMENT ASSESSMENT (PASTA) TRIAL: STUDY PROGRESS
1Newcastle University, Institute of Neuroscience, Newcastle upon Tyne, United Kingdom
2Oxford University, Medical Sciences Division, Oxford, United Kingdom
3Northumbria University, Faculty of Health and Life Sciences, Newcastle upon Tyne, United Kingdom
4Newcastle University, Institute of Health and Society, Newcastle upon Tyne, United Kingdom
5Swansea University, College of Medicine, Swansea, United Kingdom
6Manchester University, Division of Cardiovascular Sciences, Manchester, United Kingdom
Background and Aims
Rapid treatment of stroke can improve the chances of recovery. It is important that patients are assessed quickly to decide if it is appropriate to deliver thrombolysis treatment. This study is evaluating whether an enhanced assessment by paramedics could speed up treatment.
Study design
Multicentre cluster randomised trial with cost-effectiveness analysis and parallel process evaluation.
Setting
NHS ambulance services, emergency departments and stroke units within three regions of England and Wales.
Participants
Intervention paramedics deliver the PASTA pathway to adults within 4 hours of suspected stroke onset. Participants enrolled in the study are adults with confirmed stroke who were assessed by a study paramedic within 4 hours of onset.
Process evaluation: Semi-structured interviews with a subsample of participants and staff to gain insight into perceptions and experience of the PASTA pathway.
Results
Study progress: This study opened to recruitment in December 2015 and is currently running in 15 NHS Trusts. At 30 November 2017, 858 participants had been enrolled.
Conclusion
N/A
Trial registration number
ISRCTN12418919
AS32-0009
ROBOT ASSISTED TRAINING FOR THE UPPER LIMB AFTER STROKE (RATULS) TRIAL: STUDY PROGRESS
1Newcastle University, Stroke Research Group, Newcastle upon Tyne, United Kingdom
2Northumbria Healthcare NHS Foundation Trust, Stroke, Newcastle upon Tyne, United Kingdom
3Barking- Havering and Redbridge University Hospitals NHS Trust, Neurosciences, Romford, United Kingdom
4London North West Healthcare NHS Trust, Stroke, London, United Kingdom
5University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
6Northumbria University, Healthcare & Implementation Science, Newcastle upon Tyne, United Kingdom
7Oxford University, Oxford Academic Health Science Network, Oxford, United Kingdom
8Lay representative, n/a, Newcastle upon Tyne, United Kingdom
9Newcastle University, Institute of Health and Society, Newcastle upon Tyne, United Kingdom
10NHS Greater Glasgow and Clyde, Queen Elizabeth University Hospital, Glasgow, United Kingdom
11Massachusetts Institute of Technology, Mechanical Engineering, Cambridge, USA
12Newcastle University, Institute of Neuroscience, Newcastle upon Tyne, United Kingdom
13University of East London, NeuroRehabilitation Unit, London, United Kingdom
14Glasgow Caledonian University, Institute for Applied Health Research, Glasgow, United Kingdom
15University of Sunderland, Department of Pharmacy- Health and Wellbeing, Sunderland, United Kingdom
16Newcastle University and Newcastle Hospitals NHS Foundation Trust, Stroke Research Group, Newcastle upon Tyne, United Kingdom
Background and Aims
Robot-assisted training is a promising treatment for upper limb recovery following stroke. The RATULS trial is the largest trial to date to determine whether robot-assisted training improves upper limb function post stroke. Recruitment commenced 14.4.14 and here we report recruitment, attrition and intervention adherence to 15.12.17.
Method
A multi-centre randomised controlled trial, cost effectiveness analysis and process evaluation.
Inclusion criteria: Adults 1 week–5 years post first ever stroke, with moderate or severe arm weakness (Action Research Arm Test (ARAT) 0–39).
i. Robot-assisted training using the InMotion robotic gym system for 45 minutes, three times per week for 12 weeks (27 hours).
ii. Enhanced upper limb therapy provided by a therapy assistant, supervised by a therapist for 45 minutes, three times per week for 12 weeks (27 hours).
iii. Usual NHS care.
Outcomes are measured by a blinded assessor at 3 and 6 months. The primary outcome is the ARAT at 3 months. Target sample size is 762.
Results
Four study centres have recruited 713 participants, median age 61 years [IQR 51–79], 432 (61%) male, median time since stroke 248 days [IQR 114–556], median baseline ARAT 3 [IQR 0–12]. Three and 6 month outcome data are available for 584/663 (88%) and 517/624 (83%). 221 participants have concluded robot-assisted training and attended 6967/7956 (88%) sessions. 228 participants have concluded enhanced upper limb therapy and attended 6839/8208 (83%) sessions.
Conclusion
The RATULS trial results will be available mid 2019.
Trial registration number
ISRCTN69371850
AS32-0012
APACHE-AF: APIXABAN VERSUS ANTIPLATELET DRUGS OR NO ANTITHROMBOTIC TREATMENT AFTER ANTICOAGULATION-ASSOCIATED INTRACEREBRAL HAEMORRHAGE IN PATIENTS WITH ATRIAL FIBRILLATION. A RANDOMISED PHASE II CLINICAL TRIAL
1Radboudumc, Neurology, Nijmegen, The Netherlands
2University Medical Center Utrecht, Neurology, Utrecht, The Netherlands
3Albert Schweitzer Hospital, Neurology, Dordrecht, The Netherlands
4University Medical Center Groningen, Neurology, Groningen, The Netherlands
5Rijnstate Hospital, Neurology, Arnhem, The Netherlands
6Gelre Hospital, Neurology, Apeldoorn, The Netherlands
7Academic Medical Center, Neurology, Amsterdam, The Netherlands
8Amphia Hospital, Neurology, Breda, The Netherlands
9Zuyderland Hospital, Neurology, Heerlen, The Netherlands
10Maastricht University Medical Center, Neurology, Maastricht, The Netherlands
11Elisabeth-TweeSteden Hospital, Neurology, Tilburg, The Netherlands
12Onze Lieve Vrouwe Gasthuis – Location West, Neurology, Amsterdam, The Netherlands
13Medical Spectrum Twente, Neurology, Enschede, The Netherlands
14Erasmus Medical Center, Neurology, Rotterdam, The Netherlands
15Leiden University Medical Center, Neurology, Leiden, The Netherlands
Background and Aims
There is a lack of evidence on the optimal prevention of ischaemic stroke in patients with atrial fibrillation and a recent intracerebral haemorrhage (ICH) during treatment with oral anticoagulation. Treatment with a direct oral anticoagulant like apixaban might be an attractive alternative in terms of a lower risk of recurrent ICH than with a vitamin-K antagonist, while at the same time being effective for the prevention of ischaemic stroke.
Objective
To obtain reliable estimates of the rates of vascular death or non-fatal stroke in patients with atrial fibrillation and a recent anticoagulation-associated ICH who are treated with apixaban versus those who are not treated with oral anticoagulation.
Method
Study design
Multi-centre, phase II, randomised, open-label clinical trial with blinded outcome assessment.
Results
Status: Currently 41/100 patients randomized, with a mean age of 77 years (SD 7.5 years); 41% female, 16 with lobar and 25 with non-lobar ICH (December 2017).
Conclusion
Trial website: http://www.apache-af.com.
Trial registration number
Registration: NTR4526; NCT02565693.
AS32-0014
LIMITED SCALE, FEASIBILITY STUDY OF EMTENSOR G3 BRAIN IMAGING SCANNER FOR DIAGNOSTIC OF PATIENTS WITH STROKE. ONGOING MULTICENTER TRIAL
1Kepler Universitätsklinikum- Med Campus III, Neurology 2, Linz, Austria
2University Hospital Tulln, Neurology, Tulln, Austria
3Institute for Communications Engineering and RF Systems- Johannes Kepler University, Department of RF Systems, Linz, Austria
4Kepler University Clinic, Central Institute of Radiology, Linz, Austria
5EMTensor GmbH, EMTensor GmbH, Vienna, Austria
Background and Aims
Stroke is a medical emergency which requires immediate diagnosis and treatment. Up to now, CT or MRI are standardly used for imaging of stroke, but have potential side effects (radiation, accumulation of MR contrast medium). A novel brain-imaging method seems to be the electromagnetic tomography (EMT) using non-ionizing electromagnetic radiation. Goal of this trial is to examine the feasibility, sensitivity and specificity of EMT technology and Brain Imaging (BRIM) scanner generation 3 (G3) in patients with stroke. Primary Objectives: A: to assess safety and suitability of EMT BRIM G3 scanner in 5 healthy volunteers; B: to distinguish between ischemic and hemorrhagic stroke in stroke patients.
Method
Inclusion criteria: Part A: healthy volunteers aged 18–55; Part B: Males or females aged 18–90, CT or MRI verified stroke up to 48 h from onset; Both groups: BMI: 18–30 kg/m2, signed informed consent.
Electromagnetic tomography is performed with EMT-G3-Scanner, correlated to standard stroke imaging (CT or MR). Using unique antenna design, a complex electromagnetic field interacts with a biological object. This interaction changes the electromagnetic field analyzed by sophisticated, proprietary algorithms. By reconstructing a 3D distribution of the dielectric properties an image tensor is obtained.
Results
Part A of the trial is concluded- no adverse events in healthy volunteers were reported, EMTensors are obtained. Part B – recruitment of stroke patients is ongoing. Differentiation between ischemic and hemorrhagic stroke is developing.
Conclusion
Recruitment is planned to be finished till December 2018.
Trial registration number
N/A
AS32-0015
POST-STROKE DISEASE MANAGEMENT – STROKE CARD: BASELINE CHARACTERISTICS OF 1730 PATIENTS IN A RANDOMIZED CONTROLLED TRIAL AND CURRENT LITERATURE ON SECONDARY STROKE PREVENTION
1Medical University Innsbruck, Department of Neurology, Innsbruck, Austria
2St. John's Hospital – Sigmund Freud University, Department of Neurology, Vienna, Austria
Background and Aims
Patients with stroke or transient ischemic attack (TIA) are at high risk of future cardiovascular events. Despite compelling evidence about the efficacy of secondary prevention, a substantial gap exists between risk factor management in real life and that recommended by international guidelines. STROKE-CARD [NCT02156778] is a multifaceted comprehensive post-stroke disease-management-program with the objective of reducing recurrent cardiovascular events and improving quality-of-life (QoL) in stroke and TIA-patients based on an enhanced target level achievement in secondary prevention, systematic detection and treatment of post-stroke complications and patient self-empowerment.
Method
STROKE-CARD was designed as a block-randomized (2:1 ratio) pragmatic trial with blinded outcome assessment conducted in two study centres in Austria. It compares intensified (standardized 3-month visit and e-tool for risk factor management and detection of complications) versus usual post-stroke patient care and enrolled 2167 patients with acute ischemic stroke, excluding those with an mRS of 5, or high-risk TIA defined by an ABCD2-Score ≥3.
Results
The mean age of the population (n = 1730) was 68.8 years and 59.6% were males. 18% had a TIA, the median NIHSS of strokes was 3 (IQR = 5), and 23% reported a prior stroke or TIA. 20% of events were attributable to large-artery atherosclerosis, 25% to cardioembolism, and 21% to small vessel disease while 30% were of undetermined and 4% of other determined etiology (TOAST-classification). Median European-QoL-5-Dimensions-Index was 67.5. Patient characteristics were equally distributed in the two study groups.
Conclusion
STROKE-CARD will yield evidence on whether a pragmatic post-stroke intervention program is capable of preventing recurrent cardiovascular events and improving QoL.
Trial registration number
NCT02156778
AS32-0016
A TECHNOLOGY-ASSISTED, HIGH INTENSIVE, TASK-ORIENTED EXERCISE PROGRAM TO IMPROVE ARM AND HAND FUNCTIONS IN STROKE PATIENTS: STUDY PROTOCOL FOR THE TECHITO FEASIBILITY AND PILOT TRIAL
1Sunnaas Rehabilitation Hospital, Research Department, Bjørnemyr, Norway
2University of Oslo, Institute of Clinical Medicine- Faculty of Medicine, Oslo, Norway
3Oslo Metropolitan University, Department of Physiotherapy- Faculty of Health Sciences, Oslo, Norway
Background and Aims
Stroke patients with reduced arm and hand functions often experience increased dependence in activities of daily living, restricted social participation, and low quality of life. In this context, an intervention combining task-oriented exercises with orthosis in the community rehabilitation unit and home environment is hypothesized to increase perceived goal achievement, repetition, and intensity of exercises. The primary objective of the study is to evaluate the feasibility and clinical usefulness of the program in terms of patient compliance and outcomes improvement. The secondary objective is to compare the effectiveness of the program with or without the use of the orthosis in a randomized controlled trial (RCT).
Method
The study will first be carried out in a cohort of 30 stroke patients aged over 18 years regardless of lesion location and temporal evolution. Subsequently, the pilot RCT will include 30 first-time stroke patients in which the experimental group will receive an orthosis for use during the exercises. The intervention will be performed at a rehabilitation unit 3 times/week for 3 weeks and at home for 9 weeks. A comprehensive assessment will be performed at baseline, week 3, and week 12 following intervention. The primary outcome measure is the Action Research Arm Test. Secondary outcomes include Fugl- Meyer Assessment, Motor Assessment Scale, Nine-peg-hole test, grip-strength, modified Ashworth Scale, EQ-5D instrument, and Borg scale. Additionally, a qualitative evaluation will be performed.
Results
-
Conclusion
If the intervention proves effective, the proposed study will provide important information for clinicians and policymakers.
Trial registration number
Clinicaltrials.gov, NCT03396939. Registered on 11 January 2018.
AS32-0019
THE THALES (ACUTE STROKE OR TRANSIENT ISCHAEMIC ATTACK TREATED WITH TICAGRELOR AND ASPIRIN FOR PREVENTION OF STROKE AND DEATH) TRIAL DESIGN
1University of Texas at Austin, Dell Medical School, Austin, USA
2Paris Diderot University, Department of Neurology and Stroke Centre, Paris, France
3AstraZeneca, Research and Development, Gothenburg, Sweden
4Harvard University, Department of Biostatistics, Boston, USA
5Uppsala University, Department of Medical Sciences, Uppsala, Sweden
6Hospital Vall d’Hebron, Vall d´Hebron Stroke Unit, Barcelona, Spain
7Beijing Tiantan Hospital, Neurology Department, Beijing, China
Background and Aims
The SOCRATES trial reported a non-significant trend towards greater efficacy of ticagrelor versus aspirin in reducing stroke risk during 90-day treatment, with no increase in major haemorrhage. Dual antiplatelet therapy may be more effective in reducing the high risk of stroke after an acute ischaemic stroke or transient ischemic attack (TIA).
Method
The THALES trial (NCT03354429) is a randomised, double-blind trial in patients with acute ischaemic stroke or TIA. It evaluates whether ticagrelor (180-mg loading dose on day 1, then 90 mg twice daily on days 2–30) is superior to matching placebo among patients also receiving open-label aspirin (300–325 mg on day 1, then 75–100 mg once daily on days 2–30). The primary efficacy outcome is time to the composite end point of stroke or death through 30 days of treatment. The primary safety outcome is time to first severe bleeding event based on the GUSTO definition.
Results
Participants are ≥40 years of age with a non-cardioembolic ischaemic stroke (with a National Institutes of Health Stroke Scale score ≤5) or high-risk TIA (defined as an ABCD2 score ≥6 or with ipsilateral large-vessel stenosis ≥50%). Participants are randomised within 24 hours of the time last known free of new ischaemic symptoms, and study drug is initiated immediately afterwards. Approximately 13,000 participants will be randomised from about 460 sites worldwide to collect 770 outcome events.
Conclusion
The study was launched in Q1 2018 and is anticipated to complete randomisation by Q4 2019.
(Funding: AstraZeneca)
Trial registration number
THALES (NCT03354429)
AS32-0020
TREATING ANXIETY AFTER STROKE (TASK)—PROTOCOL FOR A NOVEL WEB-ENABLED RANDOMIZED CONTROLLED TRIAL
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
Anxiety affects a quarter of stroke patients. It can be disabling even after mild stroke and TIA. There is no definitive evidence to guide treatment for anxiety post-stroke/TIA. Access to post-stroke psychological care is difficult in many countries. We developed a centralized model to deliver telephone and web-supported anxiety therapies remotely.
Aim
To evaluate the feasibility of TASK anxiety treatments in a web-enabled randomized controlled trial (RCT)—a trial to be conducted entirely remotely using automated procedures.
Intervention & comparator
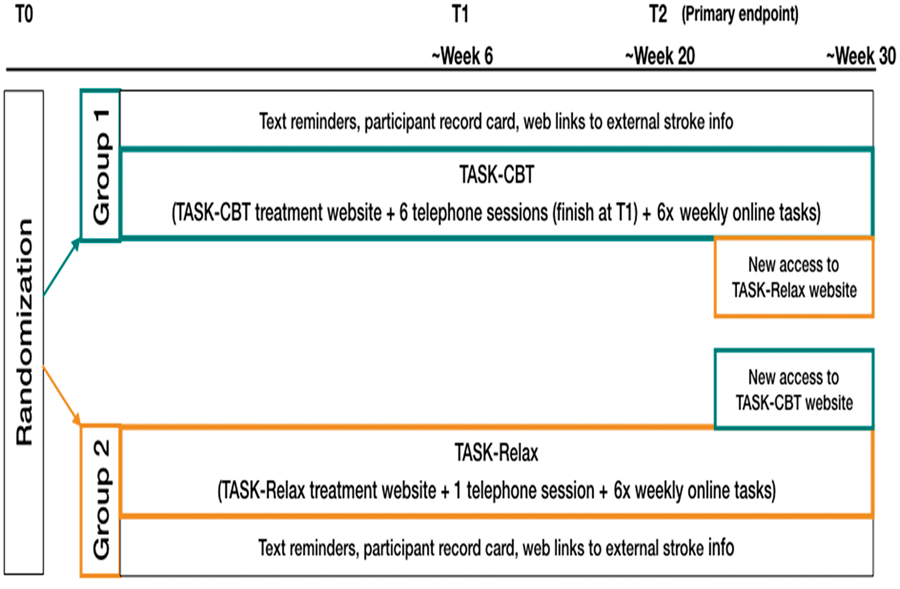
TASK-CBT: telephone-delivered cognitive behavioural therapy to treat specific feared situations in phobic anxiety and generalized anxiety; online multimedia psychoeducational content and weekly tasks
TASK-Relax: web-guided multimedia relaxation exercises, to be practiced daily for at least 5 minutes.
1) Recruitment rate per month; 2) % completed electronic consent; 3) time taken for remote eligibility confirmation; 4) completion rate of outcome measures at primary endpoint; 5) intervention fidelity
Conclusion
Feasibility of the TASK interventions and streamlined trial design can lead to more efficient large-scale RCTs in the future.
Trial registration number
Submitted for registration at clinicaltrials.gov (Record 2017/0253) awaiting approval and public release by research governance at institution
AS32-0030
ALTEPLASE-TENECTEPLASE TRIAL EVALUATION FOR STROKE THROMBOLYSIS (ATTEST 2)
1University of Glasgow, Glasgow, United Kingdom
2University of Edinburgh, Edinburgh, United Kingdom
3Oxford University Hospitals NHS Trust, Oxford, United Kingdom
Background and Aims
Data from small randomised trials suggest that the modified tissue plasminogen activator tenecteplase at 0.25mg/kg is potentially superior to intravenous alteplase, the only medical treatment currently approved for acute ischaemic stroke, with respect to both safety and efficacy in stroke, in addition to having simpler administration. NOR-TEST found no difference between alteplase and tenecteplase 0.4mg/kg but included predominantly minor strokes and a high proportion of mimics and TIAs. More data are required to establish the true risk-benefit profile compared with alteplase.
Method
ATTEST-2 will establish whether tenecteplase is superior to alteplase by undertaking a prospective randomised open blinded end-point (PROBE) trial in patients eligible for IV thrombolysis based on non-contrast CT imaging. Up to 60 UK centres will recruit 1870 patients. All UK regulatory approvals are in place. The ATTEST-2 study has been adopted onto the NIHR Clinical Research Network Portfolio. Study recruitment is ongoing and will continue until Feb 2020.
Results
Primary outcome is the distribution of modified Rankin Scale (mRS) outcomes at day 90, determined by the Rankin Focused Assessment method, analysed by ordinal distribution (“shift”) analysis of the of scores in intervention and control groups.
Conclusion
An agent with superior risk:benefit ratio to alteplase would potentially extend thrombolytic treatment to a greater proportion of patients than at present and reduce the need for mechanical thrombectomy. This trial will contribute to the optimisation of reperfusion strategies.
Trial registration number
ClinicalTrials.gov Identifier: NCT02814409
AS32-0032
THE EFFECTS OF VIRTUAL REALITY SYSTEMS ON BALANCE IMPAIRMENTS IN PATIENTS WITH CHRONIC STROKE: A SINGLE BLINDED RANDOMIZED CONTROLLED STUDY
1Izmir Katip Celebi University, Physiotherapy And Rehabilitation, Izmir, Turkey
2Dokuz Eylul University Facult Of Medicine, Neurology, Izmir, Turkey
3Dokuz Eylul University, School Of Physical Therapy And Rehabilitation, Izmir, Turkey
Background and Aims
Difficulty in balance maintenance is a particularly common problem for patients with stroke and recovery of balance is an essential component of independence in daily life activities following stroke. Several studies have researched the effectiveness of different physiotherapy interventions previously; however, research with good methodological quality is still needed. This study aimed to investigate the effects of traditional physiotherapy methods and virtual reality interventions on balance in patients with chronic stroke and compare the effectiveness of three different approaches.
Method
After the application of inclusion and exclusion criteria participants divided into three groups randomly. The first group receives a standard rehabilitation programme which include trunk stabilization and weight transfer exercises. Participants in video game group receive a 30-minute standard rehabilitation plus 30 minutes of balance training with Wii Fit. Third group receives 30 minutes of standard rehabilitation plus a 30-minute of balance therapy with Biodex balance system (Biodex, Inc, Shirley, NY, USA). All participants receive a total of 16 sessions, 2 times in a week for 8 weeks. We record Berg Balance Scale (BBS), Timed Up and Go Test (TUG), NeuroCom Balance Master System, Stroke Impact Scale Short Form (SIS-16), Fall Efficacy Scale (FES-I), and Physical Activity Enjoyment Scale (PACES) results of patients before and after the rehabilitation programmes. Differences within the groups will be shown using Wilcoxon test and differences between the groups will be indicated by use of Kruskal-Wallis Test.
Results
N/A
Conclusion
N/A
Trial registration number
N/A
AS32-0033
LONGITUDINAL STUDY OF YOUNG PATIENTS WITH EMBOLIC STROKE OF UNDETERMINED SOURCE (ESUS)
1Mcmaster University, Medicine Neurology, Hamilton, Canada
Background and Aims
Embolic strokes of undetermined source (ESUS) represent up to 20% of ischemic strokes and have a high rate of stroke recurrence. This new clinical construct is the basis for two large randomized clinical trials. By available estimates 15–20% ESUS patients will be <50 years and not included in these trials due to the respective trial designs.
We seek to determine the clinical characteristics of young-ESUS patients (<50 years) and to determine the rates of new onset atrial fibrillation, stroke recurrence, and death.
Method
Data will be collected from 1000 young-ESUS patients from 100 stroke research centers from different global regions. Patients will be followed up prospectively every 6months up to 18months via telephone
Results
We aim to describe clinical, laboratory and imaging characteristics of young-ESUS patients including antithrombotic therapy used and rates of new onset AF, recurrent stroke and death and predictors of these. The recruitment is planned to end in 2018 with follow up ending in 2019. Baseline characteristics of the young-ESUS patients will be presented at this meeting.
Conclusion
Following the completion and publication of ESUS related trials, clinical interest in the ESUS construct will increase exponentially. ESUS would become part of daily management of stroke patients. There will be intense clinical interest in knowing how young-ESUS patients compare to older ESUS cohorts. The young- ESUS registry will provide unique insights into this patient cohort.
Trial registration number
NCT03185520
AS32-0034
HYPRETENSION, AMYLOID, AND AGE ASSOCIATED KALEIDOSCOPIC BRAIN LESIONS ON CT/MRI UNDERTAKEN WITH STROKE REGISTRY (HAGAKURE): RATIONALE AND STUDY PROTOCOL
1Saga University Faculty of Medicine, Division of Neurology- Department of Internal Medicine, Saga, Japan
2Saga University Faculty of Medicine, Department of Radiology, Saga, Japan
3Saga University Faculty of Medicine, Department of Neurosurgery, Saga, Japan
Background and Aims
Sporadic cerebral small vessel disease (SVD)-related lesions on brain CT or MRI seem to be irregularly scattered, but known to be distributed with certain rules according to hypertensive, aging, and amyloid burden. Such mixed irregularities and regularity appears to like a pattern of kaleidoscope. The aims of this study are to explore clinical relevance of the SVD-related lesions on CT/MRI in stroke patients.
Methods
The
Results
Between September 2012 and August 2016, we enrolled 605 ischemic stroke patients and 196 ICH patients have been enrolled. The study is ongoing through 2019.
Conclusions
HAGAKURE study will provide novel risk stratification models for cerebro- and cardiovascular events, death, and care status after stroke by different SVD-related burden at baseline.
Trial registration number
N/A
AS32-0041
MR CLEAN-NO IV: INTRAVENOUS TREATMENT FOLLOWED BY ENDOVASCULAR TREATMENT VERSUS DIRECT ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE CAUSED BY A PROXIMAL INTRACRANIAL OCCLUSION
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Academic Medical Center, Radiology and Nuclear Medicine, Amsterdam, The Netherlands
3Maastricht UMC+, Neurology, Maastricht, The Netherlands
4Maastricht UMC+, Radiology, Maastricht, The Netherlands
5The Hague Medical Center, Neurology, The Hague, The Netherlands
6The Hague Medical Center, Radiology, The Hague, The Netherlands
7Catharina Hospital, Neurology, Eindhoven, The Netherlands
8Catharina Hospital, Radiology, Eindhoven, The Netherlands
9Erasmus University Medical Center, Radiology, Rotterdam, The Netherlands
10Erasmus University Medical Center, Neurology, Rotterdam, The Netherlands
Background and Aims
Several trials have shown that endovascular treatment (EVT) following intravenous alteplase (IVT) improves outcome of patients with acute ischemic stroke and a proximal intracranial occlusion. A recent meta-analysis of five randomized trials (Hermes collaboration, Lancet 2016), which also included patients with contraindications for IVT, showed that the effect of EVT is not influenced by IVT. The question arises whether IVT is beneficial in patients eligible for EVT.
Method
The MR CLEAN-NO IV trial is a multicenter, prospective, randomized, open-label, blinded-endpoint trial, comparing IVT followed by EVT with direct EVT in patients with a confirmed occlusion of the distal intracranial carotid artery, M1 or proximal M2. We aim to include 540 patients. The primary endpoint is the modified Rankin Scale score (mRs) at 90 days. Secondary endpoints include eTICI score, and Barthel score at 90 days. Safety endpoints include symptomatic intracranial hemorrhage and embolization in a new territory on angiography during EVT.
The primary effect parameter is the common odds ratio of the mRs, estimated by ordinal logistic regression. We will adjust for age, pre-stroke mRs, time from onset to randomization, stroke severity and collateral score. We will perform subgroup analyses for occlusion location, collateral score and thrombus perviousness, among others.
Results
Currently recruiting patients.
Conclusion
The MR CLEAN NO-IV trial will provide robust data on whether IVT is beneficial to patients who are eligible for EVT and who present to a comprehensive stroke center
Trial registration number
ISRCTN80619088
AS32-0047
SNIT STUDY: STROKE AND NUTRITION IN TIME
1Maastricht Universitair Medisch Centrum+, Neurology, Maastricht, The Netherlands
2Nutricia Advanced Medical Nutrion, Nutricia Research, Utrecht, The Netherlands
Background and Aims
Stroke patients suffer from multiple factors that may influence adequacy and quality of dietary intake. Impaired cognitive and communication skills as well as physical handicaps, may limit healthy dietary intake. Furthermore, stroke patients may have dysphagia. Hence, stroke is an important contributor to reduced diet intake and predisposes patients to a state of malnutrition, which has been shown an independent predictor of mortality and impaired recovery and should thus be avoided.
In this study, we aim to obtain comprehensive insights over time in the nutrient levels, nutritional intake and general nutritional status of patients with acute ischemic stroke either with or without dysphagia.
Method
This is an observational, single-centre, longitudinal study. A total of 50 subjects with an acute ischemic stroke with NIHSS>4 who are admitted to the stroke unit at Maastricht University Medical Center+, the Netherlands will be included in this study, of whom 25 subjects with dysphagia and 25 subjects without dysphagia.
By taking blood samples and recording food intake, we will measure the nutritional status and dietary intake during hospital stay as well as at two follow up visits during rehabilitation (6 and 13 weeks after admission). In addition, questionnaires will be used to determine level of independence (Barthel Index and modified Rankin scale) and quality of life (EQ-5D).
Results
Expected enrolment of the 1st patient: February 2018
Conclusion
The results from these observations will contribute to insights in the nutritional status of patients after a stroke and will aid improved nutritional management of the patients to prevent nutritional deficiencies.
Trial registration number
N/A
AS32-0048
NIH STROKENET EVOLVING NETWORK
1University of Cincinnati, Neurology and Rehabilitation Medicine, Cincinnati, USA
2Medical University of South Carolina, Public Health Sciences, Charleston, USA
3National Institutes of Health, National Institute of Neurological Disorders & Stroke, Rockville, USA
Background and Aims
The NIH StrokeNet consists of the National Coordinating Center that provides leadership and coordination of network activities; the National Data Management Center that coordinates centralized data collection and statistical support; 25 Regional Coordinating Centers that recruit, treat, and manage subjects; and the National Institute of Neurological Disorders and Stroke that provides administrative and scientific input. StrokeNet uses a central Institutional Review Board and also includes an Education Core for the training of fellows.
Method
StrokeNet is open to trialists with a proposal within or outside of the network. One innovative feature is the feasibility assessment that includes surveying sites for enthusiasm and availability of patients for trials; and an epidemiological study that applies eligibility criteria to the Greater Cincinnati/Northern Kentucky epidemiologic database.
Results
Of the 27 trial proposals investigators have submitted for review, 26% have been approved for funding (3 prevention, 2 acute, and 2 recovery trials). StrokeNet's first trial, DEFUSE 3, was halted early for efficacy. The ARCADIA trial began enrolling in January 2018. MOST and Sleep SMART trials will begin enrolling in mid-2018. In the past year, 26 of 27 StrokeNet fellows presented at a national meeting or published 58 first-author abstracts, 27 first-author manuscripts, and 23 submitted grants. In 2015–16, 92% trainees reported they will be “significantly involved” in research in new positions.
Conclusion
NIH StrokeNet has demonstrated the ability to design trials that are scientifically important, innovative, and feasible and to recruit at or ahead of expected rate. It is also a resource for development of stroke researchers.
Trial registration number
N/A
AS32-0049
VALUE OF ULTRASOUND CEREBRAL IMAGING FUSION IN VISUALIZATION OF CEREBRAL VASCULAR LEUKOENCEPHALOPATHY
1University Hospital Tulln, Neurology, Tulln, Austria
2Kepler University Hospital Linz, Neurology, Linz, Austria
3Asklepios Fachklinikum Brandenburg, Neurology, Brandenburg, Germany
Background and Aims
Cerebral small vessel disease (CSVD) is a common neurological disease and causes about 20% of all strokes and up to 45% of dementia, mood disturbance and gait problems.
Small vessels per se cannot be currently visualized in vivo. The diagnosis of CSVD has relied on imaging findings. The leading imaging techniques to visualize brain white matter lesions (WMLs) are brain magnetic resonance imaging (MRI) or computed tomography (CT). (US). With high-end ultrasound systems a very high image resolution is achieved. Ultrasound fusion imaging is a novel approach to evaluate brain tissue. Ultrasound is a safe, noninvasive, easily repeatable bedside investigation and offers a reliable opportunity to evaluate structures in real time.
Method
Fusion imaging (FI) was conducted with US Esaote – MyLab twice machine. Brain tissue was visualized transcranially using a sector transducer in B-Mode, followed by fusion of imported MR pictures (FLAIR sequence, DICOM format, performed with 1.5 Tesla MRI system, slice thickness 5mm, 10% gap). Electromagnetic (EM) tracking-based fusion imaging was performed.
Results
All consecutive patients presenting various degrees of leukoencephalopathy on brain MRI were included after giving written informed consent. Demographic data, relevant cardiovascular comorbidities and medications were documented additionally. Patients with normal brain MRI findings were used as control group.
Conclusion
FI was applied on 48 subjects, 36 patients with different grades of WML and 12 controls. The US images were analyzed. The main hypothesis was to evaluate the sensitivity of transcranial B-Mode US to detect different grades of WML using fusion imaging technique.
Trial registration number
N/A
AS32-0050
AN INTERVIEW STUDY OF THE REASONS PATIENTS HAVE TO CONSENT IN A RANDOMISED CONTROLLED STUDY (INTER-EFFECTS)
1Karolinska institutet, Dep of Neurosciences, Stockholm, Sweden
2Karolinska institutet, Dept. of Clinical Sciences, Stockholm, Sweden
3Karolinska institutet, Department of Clinical Sciences, Stockholm, Sweden
4KTH Royal Institute of Technology, Centre for Safety Research, Stockholm, Sweden
Background and Aims
Many randomised controlled trials (RCT) fail meeting their recruitment goals within time. One possible explanation for the recruitment problem is that people do not want to be part of a study. However little is known about the reasons for individuals acceptance or denials to participate in RCT.
EFFECTS (www.effects.se; NCT02683213 is a Swedish academic-initiated, multicentre, randomised, placebo-controlled trial of fluoxetine for stroke recovery. The trial will investigate whether routine administration of fluoxetine (20 mg daily), 6 months after an acute stroke improves patients functional outcome. EFFECTS collaborate with two other studies, FOCUS (UK) and AFFINITY (Australia, New Zealand, Vietnam). Each trial is funded independently and will report its own results.
We will use EFFECTS as a host study, and do a Trial within a Study (TWIST) called INTER-EFFECTS, an interview study, the aim is to identify and describe factors contributing to acceptance or denial to participation in a RCT.
Method
A qualitative descriptive study with individual interviews with patients who agreed or choose not to participate in EFFECTS.
Results
The result could be useful in clinical settings outside the field of stroke and could be applicable to a wide range of RCT studies. The study will add knowledge of the management of RCT.
Conclusion
Research about management of clinical trials and how to enhance recruitment to clinical trials is very important and this study can help identify barriers and find solutions to why patients say no to participate in RCT.
Trial registration number
The protocol is registered at the Northern Ireland Hub for trials methodology research.
AS32-0051
FRENCH ACUTE CEREBRAL MULTIMODAL IMAGING TO SELECT PATIENTS FOR MECHANICAL THROMBECTOMY
1Toulouse University Medical Center, Stroke Unit, Toulouse, France
2Bordeaux University Medical Center, Neurology, Bordeaux, France
3Bordeaux University medical Center, Diagnostic and Interventional Neuro-Radiology, Bordeaux, France
4Toulouse University Medical Center, Diagnostic and Interventional Neuroradiology, Toulouse, France
5Toulouse University Medical Center, Clinical Investigation Center, Toulouse, France
Background and Aims
Randomized controlled trial that did evaluate the efficacy of thrombectomy selecting patients based on the presence of a target mismatch (TMM) on multimodal imaging demonstrate a larger therapeutical effect than those who did not. Whether thrombectomy may be limited to the patients among which multimodal imaging is exhibiting a significant amount of penumbra remains controversial.
We aim to investigate in a prospective cohort of 220 patients treated by thrombectomy within 6–8 hours onset according to the current imaging recommendations, the relationship between the prevalence of TMM on pretreatment brain imaging with the rate of clinical recovery after thrombectomy.
Method
Prospective Multicentric Cohort Study. Consecutive patients eligible to a mechanical thrombectomy according to current recommendation will systematically undergo before treatment multimodal imaging (CTP or MRI) and will be treated according to the current recommendations that do not include the results of penumbral imaging.
Endpoint: Rate of good functional outcome (mRS 0–2 @ 3 months) according to the success of endovascular treatment and the prevalence of TMM (Extend IA definition) on baseline imaging.

Results
As for January 2018, 83 patients have been enrolled

Conclusion
Study may end by February 2019
Trial registration number
NCT03045146
AS32-0052
MR CLEAN-MED -- THE EFFECT OF PERIPROCEDURAL MEDICATION IN PATIENTS UNDERGOING INTRA-ARTERIAL TREATMENT FOR ACUTE ISCHEMIC STROKE: HEPARIN, ANTIPLATELET AGENTS, BOTH OR NEITHER
1Erasmus MC, Neurology, Rotterdam, The Netherlands
2Erasmus MC, Radiology, Rotterdam, The Netherlands
3Erasmus MC, Public Health, Rotterdam, The Netherlands
4Medisch Spectrum Twente, Neurology, Enschede, The Netherlands
5Maastricht University Medical Center, Neurology, Maastricht, The Netherlands
6Hagaziekenhuis, Radiology, Den Haag, The Netherlands
7Radboud University Medical Center, Radiology, Nijmegen, The Netherlands
Background and Aims
Rapid endovascular treatment (EVT) in patients with acute ischemic stroke with confirmed proximal intracranial occlusion has been proven safe and effective. Still, many patients do not recover despite recanalization. Yet, it is unknown whether periprocedural anticoagulant medication in patients treated with EVT can improve clinical outcome. The objective of this study is to assess the effect of acetylsalicylic acid (ASA) and unfractionated heparin, alone, or in combination, in patients who undergo EVT.
Method
MR CLEAN-MED is a multicenter, prospective, randomized, open-label, blinded-endpoint trial using a 2x3 factorial design. We planned to enroll 1500 patients with a clinical diagnosis of acute ischemic stroke and confirmed intracranial anterior circulation occlusion, who will undergo EVT with or without prior intravenous thrombolysis according to standard care. Study interventions: IV treatment with ASA (300 mg), low dose unfractionated heparin (loading dose of 5000 IU followed by 500 IU/hour × 6 hours) and moderate dose unfractionated heparin (loading dose of 5000 IU followed by 1250 IU/hour × 6 hours). Primary outcome is the score on the modified Rankin Scale 90 days after inclusion in the study. Safety endpoints include the occurrence of symptomatic intracerebral hemorrhage.
Results
First patient enrolled on January 22nd, 2018
Conclusion
We hypothesize that despite the potentially increased risk of (symptomatic) intracerebral hemorrhage, periprocedural ASA and unfractionated heparin alone or in combination will improve functional outcome of patients with acute ischemic stroke treated with EVT.
Trial registration number
ISRCTN 76741621
AS32-0053
CAROTID REVASCULARIZATION AND MEDICAL MANAGEMENT FOR ASYMPTOMATIC CAROTID STENOSIS: CREST-2 UPDATE
1University of Alabama at Birmingham, Biostatistics, Birmingham, USA
2Mayo Clinic, Neurology, Jacksonville, USA
3University of Maryland School of Medicine, Surgery, Baltimore, USA
4Brookwood Medical Center, Cardiology, Birmingham, USA
5Mayo Clinic, Neurology, Rochester, USA
6University of Miami Miller School of Medicine, Neurology & Stroke Program, Miami, USA
7Medical University of South Carolina, Neurology, Charleston, USA
8Mayo Clinic, Neurology, Phoenix, USA
9University of Alabama at Birmingham, Epidemiology, Birmingham, USA
10Mayo Clinic, Neuroradiology, Rochester, USA
11University of Alabama at Birmingham, Neurology, Birmingham, USA
12UCLA Medical Center, Vascular and Endovascular Surgery, Los Angeles, USA
13National Institute of Neurological Disorders and Stroke- National Institutes of Health, Health & Human Services, Bethesda, USA
Background and Aims
The applicability of prior randomized trials in the management of asymptomatic carotid stenosis to current treatment decisions has been questioned. The NINDS-funded CREST-2 will compare CEA and intensive medical management (IMM) versus IMM alone (n = 1240), and CAS and IMM versus IMM alone (n = 1240) in asymptomatic patients with ≥70% stenosis.
Method
CREST-2 consists of two parallel randomized clinical trials at ≈120 centers, including collaboration with NINDS StrokeNet. The composite primary outcome is stroke or death during the peri-procedural period or ipsilateral ischemic stroke thereafter up to 4 years. Cognitive status will be assessed periodically through computer-assisted telephone interviews. Centrally directed IMM includes tight control of blood pressure (per current guidelines) and cholesterol (LDL target < 70 mg/dl) as well as lifestyle coaching.
Results
As of January 8, 2018, 182 centers have been approved by the Site Selection Committee. Credentialing is ongoing, with 379 approved surgeons and 163 approved interventionists. An additional 184 interventionists have been approved to submit additional cases via the CREST-2 Companion Registry which provides a CMS-reimbursed pathway for full credentialing in CREST-2. 880 patients have been randomized, 429 (48.75%) patients in the endarterectomy trial, and 451 (51.25%) patients in the stent trial.
Conclusion
CREST-2 is designed to identify the best approach for asymptomatic carotid stenosis. An update will be provided regarding the numbers of patients randomized, centers certified, as well as surgeons and interventionists fully approved. The CREST-2 Registry will provide the option of CAS while enhancing interventionists’ credentials for participation in CREST-2.
Trial registration number
Registration: Clinicaltrials.gov NCT02089217
AS32-0054
ENDOVASCULAR ACUTE STROKE INTERVENTION – TANDEM OCCLUSION TRIAL (EASI-TOC): A TRIAL OF ACUTE CERVICAL INTERNAL CAROTID ARTERY STENTING DURING ENDOVASCULAR THROMBECTOMY FOR ANTERIOR CIRCULATION STROKE
1Centre Hospitalier de l'Université de Montréal, Neurosciences, Montreal, Canada
2Centre Hospitalier de l'Université de Montréal, Radiology, Montreal, Canada
Background and Aims
Tandem occlusion refers to stroke due to middle cerebral artery (MCA) or distal internal carotid artery (ICA) AND ipsilateral cervical ICA occlusion or near-occlusion. It is found in 12–30% of patients undergoing endovascular thrombectomy (EVT). Optimal acute management of the cervical ICA lesion is uncertain and may include no definitive revascularization versus acute stenting. Practice varies widely across centresand no randomized-control trial (RCT) data exist to guide decision-making.
Method
We propose a pragmatic, multicentre PROBE RCT of adult acute stroke patients undergoing EVT which will compare acute stenting for high-grade cervical ICA stenosis/occlusion versus deferred ICA intervention (if indicated). Treatment allocation will occur after confirmation of a tandem occlusion on initial non-invasive vascular imaging (CTA or MRA) but prior to EVT. A standard antiplatelet regimen will be strongly recommended. Anterograde and retrograde ICA stenting will both be permitted. Cross-overs will be allowed in cases of ICA “pseudo-occlusions” identified on CTA or MRA, but otherwise cross-overs will be strongly discouraged.
Primary outcome: Proportion of patients with a favorable mRS (0-2) at 90 days
Conclusion
The EASI-TOC study plans to begin recruitment by the Fall of 2018 and should provide data regarding the use of routine ICA stenting in acute stroke patients with tandem occlusions.
Trial registration number
N/A
AS32-0055
ESTABLISHING AN INTERNATIONAL DATABASE OF 5932 INDIVIDUAL PARTICIPANTS’ DATA FOR META-ANALYSES TO INFORM THE REHABILITATION AND RECOVERY OF PEOPLE WITH APHASIA AFTER STROKE (RELEASE PROJECT)
1Glasgow Caledonian University, Nursing- Midwifery and Allied Health Professions Research Unit, Glasgow, United Kingdom
Background and Aims
A co-ordinated approach involving >60 international collaborators facilitated the creation of a database on post-stroke aphasia (NIHR HS&DR-14/02/22). Individual Participant Data (IPD) meta-analyses will inform our understanding of uncertainties including predictors of recovery, prognosis and highlight interventions amongst targeted trial specific populations optimally suited to investigation within definitive randomized controlled trials. We aimed to create a large, international, research-based IPD archive to support the examination of post-stroke aphasia research uncertainties.
Method
We systematically searched for datasets containing IPD on ≥10 people with aphasia, time post-stroke and aphasia severity (Cochrane Stroke Group Trials, MEDLINE, AMED, CINAHL, Cochrane Library Databases [CDSR, DARE, CENTRAL, HTA], LLBA, EMBASE, and SpeechBITE). Two independent reviewers screened 5256 records, identifying 874 eligible datasets. We invited contributions from the Collaboration of Aphasia Trialists and other aphasia researchers. We double-extracted individual, aphasia, stroke and intervention data.
Results
Our database contains 5932 IPD from 174 primary research datasets across 28 countries (Table 1; 3944 IPD from 75 electronic datasets; 1988 IPD from 99 public domain datasets). Data on aphasia severity (Western Aphasia Battery AQ = 1099 IPD), naming (Boston Naming Test 809 IPD); auditory comprehension (Token Test = 1263 IPD), reading (Comprehensive Aphasia Battery subtest = 460 IPD) and writing (Aachen Aphasia Test subtest = 479 IPD) will inform our analyses.
Conclusion
Our RELEASE database will inform our analyses of aphasia recovery, predictors of recovery and components of effective therapeutic interventions.
Trial registration number
N/A
AS32-0056
PATIENT SELECTION PROTOCOL FOR LONG TERM INSERTABLE CARDIAC MONITORING
1Stroke Unit- Complejo Hospitalario de Toledo, Neurology, Toledo, Spain
2Arrhythmia and Electrophysiology Unit- Complejo Hospitalario de Toledo, Cardiology, Toledo, Spain
Background and Aims
The purpose of developing the present protocol is selecting patients who are candidates for long time monitoring with insertable holter with remote detection of dysrhythmias trying to increase the detection rate of paroxysmal atrial fibrillation in patients with cryptogenic stroke.
At the same time we correlate the existence of structural cardiac abnormalities or dysrhythmias detected during the hospital admission referred as minor cardioembolic risk factors with the existence of a potentially embolic silent arrhythmia
Method
We select those cryptogenic strokes who present: not lacunar stroke or different locations at the same time by CT/MRI, absence of extracranial or intracranial aterosclerosis causing ≥50% luminal stenosis in arteries supplying the area of ischaemia, no major-risk cardioembolic source of embolism, no other specific cause of stroke identified
Results
The diagnostic assessment includes: Brain CT or MRI, 12-lead ECG, precordial echocardiography with shunt detection, cardiac monitoring for ≥24 h with automated rhythm detection, imaging of both the extracranial and intracranial arteries supplying the area of brain ischaemia (catheter, MR, or CT angiography, or cervical duplex plus transcranial doppler ultrasonography).
We will select those patients with cryptogenic stroke with at least a finding of the following in the extension study: minor-risk potential cardioembolic sources detected by echocardiography and/or non-atrial fibrillation atrial dysrhythmias.
Conclusion
The implant is performed prior to discharge. To date, 15 patients have been implanted in 11 months with a detection rate of 20%. We believe that the screening based on such criteria can serve to reduce costs and better select those patients who are candidates.
Trial registration number
N/A
AS32-0057
DIRECT INTRA-ARTERIAL THROMBECTOMY IN ORDER TO REVASCULARIZE AIS PATIENTS WITH LARGE VESSEL OCCLUSION EFFICIENTLY IN CHINESE TERTIARY HOSPITALS: A MULTICENTER RANDOMIZED CLINICAL TRIAL (DIRECT-MT)
1Changhai Hospital- Second Military Medical University, Neurosurgery, Shanghai, China
2Changhai Hospital- Second Military Medical University, neurology, Shanghai, China
3Academic Medical Center Amsterdam, Radiology, Amsterdam, The Netherlands
4Academic Medical Center Amsterdam, Neurology, Amsterdam, The Netherlands
Background
Intravenous thrombolysis (IVT) combined with mechanical thrombectomy (MT) has been proven safe and effective in patients with acute ischemic stroke (AIS) of anterior circulation large vessel occlusion (ACLVO). Despite recanalization, a considerable proportion of patients do not recover. The incidence of symptomatic intracerebral hemorrhage (sICH) was similar between bridging therapy and IVT, suggesting that this complication could not be attributed to the MT, but rather to pre-treatment with IVT. Meanwhile, the incidence of intracranial atherosclerosis stenosis (ICAS) is higher in Asians. It is not clear whether ICAS modifies treatment effect or not.
Objective
First, to assess the effect of direct MT compared to bridging therapy in patients with AIS due to an ACLVO. Secondary, to assess treatment effect modification by presence of ICAS.
Method
Study design
This is a parallel group, RCT of direct MT versus bridging therapy, using a non-inferiority design. The trial will be executed in collaboration with MRCLEAN NO-IV investigators.
Study population
Patients with AIS of ACLVO confirmed by CTA. Initiation of IVT must be feasible within 4.5 hours from symptom onset. Age must be 18 or over and NIHSS 2 or more.
Results
NA
Conclusion
NA
Trial registration number
on going registering
AS32-0058
INSIST – IN SILICO TRIALS FOR TREATMENT OF ACUTE ISCHEMIC STROKE
1Academic Medical Center, Biomedical Engineering and Physics, Amsterdam, The Netherlands
2Academic Medical Center, Department of Radiology and Nuclear Medicine, Amsterdam, The Netherlands
3Erasmus Medical Center, Department of Radiology and Nuclear Medicine, Rotterdam, The Netherlands
4Universite de Geneve, Computer Science Department, Geneve, Switzerland
5Academic Medical Center, Center of Experimental and Molecular Medicine, Amsterdam, The Netherlands
6Academic Medical Center, Experimental Immunology, Amsterdam, The Netherlands
7The Chancellor- Masters and Scholars of the University of Oxford, Engineering Science- Institute of Biomedical Engineering, Oxford, United Kingdom
8Universiteit van Amsterdam, Institute of Informatics- Faculty of Science, Amsterdam, The Netherlands
9National University of Ireland, Biomedical Engineering, Galway, Ireland
Background and Aims
Endovascular randomized controlled trials (RCTs) have revolutionized management of acute ischemic stroke (AIS) patients with intracranial large vessel occlusion. Despite improved treatment, up to two out of three patients have poor functional outcome. In-silico clinical trials are computer-based simulation of RCTs and are a promising addition and alternative to the expensive RCTs that are or will be set-up to optimize treatment and patient selection.
Method
INSIST will model AIS,intra-arterial and intravenous treatment to realize in-silico AIS clinical trials [Figure1]. Libraries of virtual AIS patient populations based on clinical, imaging, histopathological and outcome data of stroke trials including MRCLEAN,MRCLEAN Registry and HERMES (totaling 4500patients) will be developed. In-silico models for thrombosis, thrombolysis, intra-arterial thrombectomy, microvascular perfusion, neurological deterioration after stroke will be integrated to form an in-silico clinical trial. The accuracy of in-silico clinical trials will be demonstrated by comparison with laboratory experiments and real-life RCTs.
Results

Conclusion
INSIST is an international, inter-disciplinary consortium to develop models for in-silico AIS trials. We hypothesize that in-silico modelling will allow understanding patient-specific (patho) physiology of AIS and interaction with treatment devices at relevant biological levels and treatment outcome. This knowledge can optimize second- and third-phase clinical trials, improve medical device and drug development, optimize personalized treatment, reduce animal experiments and will support faster implementation of these improvements in clinical practice. INSIST is funded under H2020. Grant:#777072. www.insist-h2020.eu
Trial registration number
N/A
AS32-0059
ENCOURAGEMENT-INDUCED REAL-WORLD UPPER LIMB USE AFTER STROKE BY A TRACKING AND FEEDBACK DEVICE: PROGRESS OF A MULTI-CENTER, ASSESSOR-BLINDED, RANDOMIZED CONTROLLED TRIAL
1University Hospital Zürich, Neurology, Zürich, Switzerland
2University of Twente, Biomedical Signals and Systems, Enschede, The Netherlands
3cereneo, Center for Neurology and Rehabilitation, Vitznau, Switzerland
Background and Aims
Effective paretic upper limb training post-stroke is characterized by intensity and specificity. Therefore, the best training is life itself, but motivation, compensatory function, and effort are often limiting factors. Feedback technology has the potential to encourage self-administered, intensive arm training in the patients’ home environment. The present study aims to investigate post-intervention and long-term efficacy of a wrist-worn activity-tracking device providing multimodal feedback on daily arm use in hemiparetic subjects >3 months post-stroke.
Method
A prospective, multi-center, assessor-blinded, randomized controlled trial. Sixty-two stroke patients will be randomized in two groups. The experimental group receives a wrist-worn activity-tracking device providing multimodal feedback on daily arm use for 6-weeks. Controls wear an identical device without feedback. Primary outcome is the change in patient-reported amount of daily life arm use from baseline to post-intervention, measured by the Motor Activity Log–14, Amount of Use subscale. Secondary outcomes are change in arm motor function, arm capacity, global disability, patient-reported quality of daily life arm use, and quality of life from baseline to post-intervention and 6-week follow-up, as well as compliance, activity counts, and safety. An intention-to-treat principle will be applied.
Results
Recruitment started in September 2017 and is expected to last until December 2018. Twenty-one patients have been recruited, of whom 14 have completed the study so far and one dropped-out (non-intervention related). There were no related (serious) adverse events.
Conclusion
A positive result of this study will underline the importance of feedback on daily life arm use after stroke.
Trial registration number
https://clinicaltrials.gov: NCT03294187
AS32-0060
STROKE SUPPORT ORGANISATION FACULTY TOOL
1Stroke Alliance for Europe, Secretariat, Brussels, Belgium
Background and Aims
The Stroke Alliance for Europe (SAFE) in partnership with the European Stroke Organisation is developing an exciting and new eLearning tool on advocacy training for its growing Stroke Support Organisation (SSOs) members. The eLearning tool focuses on teaching SSOs the skills needed to advocate for better prevention strategies, diagnosis and treatment for stroke, as well as aftercare of survivors and their families at a local and national level. Through the completion of the educational training on advocacy, SSOs can build their capacities and capabilities. This gives SAFE another opportunity to build on to its many activities and continue to invest in the future fight against stroke.
The eLearning platform will be:
• Available across Europe, with internet connection.
• Responsive, will adapt and work across multiple devices e.g. smartphone, tablets, desktops etc.
• Free to access.
• Include videos, animation and social media integration.
Log in and get a hands-on knowledge about:
1. What is a SSO; and what is its role?
2. What is advocacy and how is it done?
3. Use of evidence
4. The role of the patient voice
5. Health systems advocacy
6. Public advocacy
The first two modules will be publicly available from mid-April 2018 with the final four modules becoming available throughout 2018. The project is sponsored by Bayer.
The Stroke Alliance for Europe (SAFE) a non-profit-making organisation formed in 2004. It is the voice of stroke patients in Europe, representing a range of patient groups from 30 European countries. For more information about SAFE, please visit www.safestroke.eu.
Method
N/A
Results
N/A
Conclusion
N/A
Trial registration number
N/A
AS32-0061
STROKE ALLIANCE FOR EUROPE (SAFE)
1Stroke Alliance for Europe, Secretariat, Brussels, Belgium
Background and Aims
SAFE is an alliance of patient organisations from 30 European countries, fighting together against stroke in Europe.
SAFE published the Burden of Stroke Report in May 2017 in the European Parliament, providing insights on stroke care pathway across 35 European countries. Please visit www.strokeeurope.eu
The Stroke Action Plan for Europe 2018 to 2030 will set new recommendations for stroke prevention and the implementation of adequate stroke services in Europe. The Plan includes seven domain groups along the stroke care pathway, five of them from the Helsingborg Declaration, introducing the two new domains: Primary Prevention and Life after Stroke.
In partnership with ESO, SAFE is developing an eLearning tool on advocacy training for its growing number of member organisations. The focus is on training future stroke advocates for achieving better prevention strategies, diagnosis and treatment for stroke, as well as aftercare of survivors and their families.
SAFE signed a contract with Oxford University to deliver a research report on the Economic Impact of Stroke. The report will be presented in Spring 2019.
SAFE supports the European Union commitment to combat stroke with an advanced research programme, actively participating in six EU funded research projects:
• EuroHYP-1
• PRECIOUS
• PROOF
• SVDs@Target
• PRESTIGE-AF
• TENSION
For more information about SAFE, please visit www.safestroke.eu
Method
N/A
Results
N/A
Conclusion
N/A
Trial registration number
N/A
AS32-0063
A COMPARISON OF CENTRAL ADJUDICATION AND SITE ASSESSMENT OF OUTCOMES IN RANDOMISED STROKE TRIALS: THE `ADJUDICATING OUTCOMES IN STROKE TRIALS’ COLLABORATION (AOST)
1University of Nottingham, Nottingham Clinical Trials Unit, Nottingham, United Kingdom
2University of Nottingham, Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
In stroke trials a large variety of different kinds of outcomes are commonly adjudicated. However, there is a lack of evidence on the effect of adjudication on outcomes in stroke trials and if this has any impact on trial conclusions. Therefore, research is needed to understand the role adjudication has in stroke trials. We have developed the `Adjudicating Outcomes in Stroke Trials’ Collaboration (AOST) with the aim to answer the following question: What are the benefits and costs of adjudicating outcomes in stroke trials?
The first work package of AOST is a systematic review which aims to assess how adjudication of the primary outcome in stroke trials impacts on the primary treatment effect estimate.
Method
Randomised stroke trials that have a primary outcome which has undergone assessment by both site investigators and adjudicators will be included in this review. To assess the impact of adjudication on each trial, we will calculate the ratio of treatment effects (RTE). The RTE will be calculated as the treatment estimate using the site-assessed primary outcome versus the treatment estimate using the adjudicator-assessed primary outcome. Due to the majority of trials not reporting unadjudicated outcomes, individual patient data or additional trial results are needed from each trial before it can be included. Data collection will run until 30th June 2018.
Results
88 trials have been identified as being eligible for the review. At the date of submission, data have been received from 9 trials.
Conclusion
More data is required to sufficiently answer this important research question.
Trial registration number
N/A
AS32-0064
PROTOCOL FOR MAAESTRO: ELECTRONIC MONITORING OF ADHERENCE TO DIRECT ORAL ANTICOAGULANTS AND EDUCATIONAL, REMINDER-BASED INTERVENTION – A RANDOMISED CROSSOVER STUDY IN POLYMEDICATED ISCHEMIC STROKE PATIENTS
1University Hospital Basel and University of Basel, Department of Neurology and Stroke Center, Basel, Switzerland
2University of Basel, Department of Pharmaceutical Sciences, Basel, Switzerland
3University of Basel and Felix-Platter Hospital, University Center for Medicine of Ageing and Rehabilitation, Basel, Switzerland
4University Hospital Basel and University of Basel, Department of Clinical Research, Basel, Switzerland
Background and Aims
Non-adherence to direct oral anticoagulants (DOACs) remains a matter of concern, especially in the vulnerable population of polymedicated patients with a recent stroke. However, data on electronically monitored adherence and interventions to improve it are scarce. We aim to use electronic monitoring to: (i) accurately measure non-adherence to DOACs, identify predictors and reliable self-reporting strategies and evaluate its association with clinical outcomes, and (ii) assess the adherence-improving effect of an educational and reminder-based intervention in DOAC-treated patients after a recent stroke.
Method
This is a monocentric, randomized, crossover, open-label study. Adult polymedicated patients (≥ 3 drugs including DOAC), hospitalized for an acute ischemic stroke who are self-administering their drugs are eligible for participation. Adherence to DOACs will be monitored electronically throughout the 12-month-long study. After the initial 6-month observational phase following hospital discharge, patients will be counselled and given a multicompartment pillbox for use throughout the subsequent 6-month interventional phase. The pillbox will provide intake reminders (alarms) either during the first or the last 3 months of the interventional phase. Patients will be randomly allocated to alarms-first or alarms-last. A sample of 130 patients provides 90% power to show a 20% improvement with intake alarms in the primary endpoint of non-optimal timing adherence. Secondary endpoints include other adherence measures, self-reported adherence and clinical outcomes.
Results
The study has received ethical approval and enrollment is ongoing.
Conclusion
This study will investigate aspects of non-adherence and the effect of an adherence-improving intervention in the previously unexplored population of DOAC-treated patients with a recent stroke using electronic monitoring.
Trial registration number
NCT03344146 (ClinicalTrials.gov)
AS32-0065
A RANDOMIZED CONTROLLED TRIAL TO TEST EFFICACY AND SAFETY OF THROMBECTOMY IN STROKE WITH EXTENDED LESION AND EXTENDED TIME WINDOW (TENSION)
1Heidelberg University Hospital, Neuroradiology, Heidelberg, Germany
2Oslo University Hospital, Department of Internal Medicine and Cardiology, Oslo, Norway
3Hospices Civils de Lyon, Service de Biostatistique, Lyon, France
4Karolinska University Hospital, Neuroradiology, Stockholm, Sweden
5Medical University Innsbruck, Neuroradiolgy, Innsbruck, Austria
6Charles University Hospital, Radiology, Hradec Kralove, Czech Republic
7Hôpital Maison-Blanche- Université Reims-Champagne-Ardenne, Neuroradiology, Reims, France
8Stroke Alliance For Europe, Stroke Alliance For Europe, London, United Kingdom
9Aarhus University Hospital, Neurology, Aarhus, Denmark
10Comenius University’s Jessenius Faculty of Medicine and University Hospital, Radiology, Martin, Slovak Republic
11University of Hamburg, Neuroradiology, Hamburg, Germany
12Eppdata, Eppdata, Hamburg, Germany
13University of Hamburg, Neurology, Hamburg, Germany
Background and Aims
The benefit of thrombectomy in patients with large intracranial vessel occlusion of the anterior circulation has been shown in selected patients in previous randomized controlled trials, but patients with extended stroke lesions were excluded in the majority of these trials. TENSION aims to demonstrate efficacy and safety of thrombectomy in patients with extended stroke lesions in an extended time window or unknown stroke onset.
Method
TENSION is an investigator-initiated, prospective, open label, blinded endpoint (PROBE), European, two-arm, randomized, controlled, post-market study to compare the safety and effectiveness of thrombectomy as compared to best medical care alone in stroke patients with extended stroke lesions defined by an Alberta Stroke Program Early CT Scan score (ASPECTS) of 3–5 and in an extended time window (up to 12 hours, or unknown time of symptom onset). In an adaptive design study, up to 714 patients will be randomized.
Results
Outcomes: Primary efficacy endpoint will be clinical outcome defined by the modified Rankin Scale (mRS) at 90 days post-stroke. The main safety endpoint will be death and dependency (mRS 4–6) at 90 days. Additional measures include adverse events, functional health status, post-stroke depression and costs utility assessment.
Conclusion
TENSION will start enrolling in early 2018 and will be running in eight European countries. TENSION will provide evidence for effective treatment for severe stroke patients thereby improving functional outcome and quality of life of thousands of stroke patients.
Trial registration number
TENSION is registered at ClinicalTrials.gov (ClinicalTrials.gov Identifier NCT03094715).
AS32-0066
TREATMENT WITH EXENATIDE IN ACUTE ISCHAEMIC STROKE (TEXAIS) TRIAL: PROSPECTIVE, RANDOMISED, OPEN LABEL, BLINDED END-POINT STUDY OF EXENATIDE VS. STANDARD CARE IN POST STROKE HYPERGLYCAEMIA
1Monash University/Eastern Health Clinical School, Neurosciences, Melbourne, Australia
2Westmead Hospital- University of Sydney, Endocrinology, Sydney, Australia
3Florey Institute of Neuroscience and Mental Health, Statistics and Decision Analysis Academic Platform, Melbourne, Australia
4Australian Catholic University & St Vincent’s Health, Nursing Research Institute, Sydney, Australia
5The Florey, Stroke, Melbourne, Australia
6University of New South Wales, University of New South Wales, Sydney, Australia
7Sydney Medical School/The George Institute, Discipline of Medicine, Sydney, Australia
8The Florey, The Florey, Melbourne, Australia
9Royal Brisbane and Women's Hospital, Neurology, Brisbane, Australia
Background and Aims
Post-stroke hyperglycaemia (PSH) occurs in up to 50% of patients presenting with acute ischaemic stroke (AIS). It reduces the efficacy of thrombolysis, increases infarct size, and worsens clinical outcomes. Insulin-based therapies have generally not been beneficial in treating PSH as they are difficult to implement, may cause hypoglycaemia, possibly increase mortality and worse clinical outcomes. Exenatide may be a safer, simple, and more effective alternative to insulin in AIS.
Method
TEXAIS is a 3-year, Phase 2, multi-centre, prospective, randomised, open label, blinded end-point (PROBE) trial comparing Exenatide to Standard of Care. It aims to recruit 528 patients with a primary end point of major neurological improvement1 at 7 days defined as a ≥8-point improvement in NIHSS score, or NIHSS 0–1. Secondary outcomes of hyper- and hypoglycaemia at 5 days and NIHSS and mRS at 90 days will be measured. The treatment arm will receive Exenatide 5µg subcutaneously twice daily. The control arm will receive standard stroke unit care. Continuous glucose monitors will track the dynamic variability of glucose.
Results
Recruitment in TEXAIS has commenced with 10 patients enrolled to date.
Conclusion
TEXAIS aims to show that Exenatide is safe and effective in the treatment of PSH. It has been designed to be highly generalisable with an ability to enroll a large percentage of patients with AIS, regardless of admission blood glucose level, diabetes status, or stroke severity, with very low risk of hypoglycaemia.
Trial registration number
Australian New Zealand Clinical Trials Registry: ACTRN12617000409370p
AS32-0067
THE ATTEST STUDY: THE OPTIMAL AND COST EFFECTIVE APPROACH OF TRANSTHORACIC ECHOCARDIOGRAPHY IN ISCHEMIC STROKE OR TIA OF UNDETERMINED CAUSE
1Medisch Spectrum Twente, Neurology, Enschede, The Netherlands
2Medisch Spectrum Twente, Cardiology, Enschede, The Netherlands
3Academic Medical Center, Neurology, Amsterdam, The Netherlands
4Academic Medical Center, Cardiology, Amsterdam, The Netherlands
5Maasstad Hospital, Neurology, Rotterdam, The Netherlands
6Maasstad Hospital, Cardiology, Rotterdam, The Netherlands
7Elisabeth-TweeSteden Hospital, Neurology, Tilburg, The Netherlands
8Elisabeth-TweeSteden Hospital, Cardiology, Tilburg, The Netherlands
9Albert Schweitzer Hospital, Neurology, Dordrecht, The Netherlands
10Albert Schweitzer Hospital, Cardiology, Dordrecht, The Netherlands
11Twente University, Health Economics, Enschede, The Netherlands
12Medisch Spectrum Twente, Research Methodology, Enschede, The Netherlands
Background and Aims
The Dutch CBO guideline for stroke recommends transthoracic echocardiography (TTE) in all patients with ischemic stroke or TIA of undetermined cause. The scientific basis of this recommendation, however, is debatable. We aim to develop a prediction model to select patients who are most likely to have TTE abnormalities leading to alteration in management, improving the therapeutic yield of TTE in these patients.
Method
Seven Dutch hospitals will participate in this multicenter cross-sectional study, which will run for a period of three years. The population will consist of 1300 patients with TIA or ischemic stroke of undetermined cause after standard diagnostic evaluation. The primary outcome measure will be the proportion of patients with TTE findings resulting in management changes. A prediction model will be developed based on clinical findings and additional investigations to predict the primary study outcome in a derivation cohort consisting of 60% of the study population. Model performance will be externally validated in the remaining 40%. A cost-effectiveness analysis of the following strategies will be determined : 1) TTE in all patients; 2) TTE only in selected patients with an increased likelihood of therapeutically relevant TTE findings; 3) no TTE. A Markov model will be used to estimate life-long health effects and costs.
Results
Not available yet.
Conclusion
It is unclear whether routine use of TTE is useful in patients with TIA or ischemic stroke of undetermined cause. This study will provide data to identify the optimal and cost-effective approach of TTE in patients with TIA or ischemic stroke.
Trial registration number
NTR6993
AS32-0068
MULTICENTRE RANDOMISED TRIAL OF ACUTE STROKE TREATMENT IN THE AMBULANCE WITH A NITROGLYCERIN PATCH (MR ASAP)
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Isala, Neurology, Zwolle, The Netherlands
3RAV IJsselland, Ambulance, Zwolle, The Netherlands
4Rijnstate Hospital, Neurology, Arnhem, The Netherlands
5Albert Schweitzer Hospital, Neurology, Dordrecht, The Netherlands
6Leiden University Medical Center, Neurology, Leiden, The Netherlands
7Ambulance Amsterdam, Ambulance, Amsterdam, The Netherlands
8Erasmus MC University Medical Center, Neurology, Rotterdam, The Netherlands
9Radboud University Medical Center, Neurology, Nijmegen, The Netherlands
10Utrecht University Medical Center, Brain Center Rudolf Magnus- Neurology and Neurosurgery, Utrecht, The Netherlands
Background and Aims
Recent studies have suggested that administration of glyceryl trinitrate (GTN) via a transdermal patch in the first hours after stroke onset increases the chance of a favourable outcome, possibly through an increase in intracranial collateral blood flow and a reduction in blood pressure. MR ASAP aims to investigate the effect of transdermal GTN, started within 3 hours of stroke onset in the prehospital setting, on functional outcome at 90 days in patients with acute ischaemic stroke or intracerebral haemorrhage.
Method
Phase III, multicentre, randomised, open-label clinical trial with blinded endpoint assessment (PROBE). 1400 patients with suspected stroke and a systolic blood pressure ≥ 140 mmHg will be randomly allocated to transdermal GTN (5 mg/day), administered by paramedics in the prehospital setting within 3 hours of stroke onset and continued for 24 hours, or to standard care. This trial will be conducted in the Netherlands and will use a deferred informed consent procedure. The primary outcome is functional outcome, assessed with the modified Rankin Scale at 90 days.
Results
Ethics approval is obtained and enrolment will start April 3rd 2018.
Conclusion
MR ASAP will assess whether very early administration of GTN improves outcome after stroke in a setting where rates of intravenous thrombolysis and endovascular treatment for acute ischaemic stroke are high. The deferred consent procedure facilitates prompt GTN treatment and will prevent delay to revascularisation therapies. If early transdermal GTN treatment proves to be effective, this low-cost treatment can be readily implemented into daily clinical practice.
Trial registration number
ISRCTN99503308
AS32-0069
A FEASIBILITY STUDY OF PRISMS AND THERAPY IN ATTENTION LOSS AFTER STROKE (SPATIAL)
1The University of Manchester, Division of Neuroscience and Experimental Psychology, Manchester, United Kingdom
2University of the West of England, Faculty of Health and Applied Sciences, Bristol, United Kingdom
3The University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom
4The University of Manchester, Division of Population Health- Health Services Research & Primary Care, Manchester, United Kingdom
Background and Aims
Unilateral Spatial Neglect (USN) is a cognitive impairment of awareness of one side. This study investigates a brief intervention (Prism Adaptation Training (PAT)) within UK NHS occupational therapy (OT) to determine the feasibility and acceptability of PAT and of conducting a larger randomised controlled trial (RCT). The ultimate purpose is to enable people with USN to better engage in OT to maximise independence in activities of daily living.
Method
Mixed methods design: pragmatic, feasibility, multi-centre, stratified RCT with nested process evaluation and proof of concept exploration.
RCT Participants: ∼60 adult stroke survivors, 1–4wks post-admission with neglect, recruited from 6 sites; ∼40 carers.
Treatment condition is OT with PAT; control condition is OT without PAT, delivered 5 times weekly for 3 weeks.
Randomisation: random allocation into one of two study arms in a 3:1 (treatment: control) ratio, stratified by site. Researchers will be blind to group allocation.
Proof of concept: we will video the first session to examine the immediate effect of PAT on OT engagement.
Feasibility outcomes: recruitment, fidelity, acceptability, attrition.
Participant outcomes: standardised neglect tests and extended activities of daily living.
Process evaluation: 12 patients and 12 therapists will undergo qualitative interviews (after outcome assessments) to help us understand their experiences of PAT, including acceptability of PAT, plus the best setting for recruitment and application of PAT.
Results
This study is in set up. Funding is secured, an application for ethical approval is underway and sites are expected to open January 2019.
Conclusion
TBA (see above)
Trial registration number
IRAS Number: 232874
RfPB Grant Number: PB-PG-0816-20016
Registration: TBC
AS32-0070
RAPID INTERVENTION WITH GLYCERYL TRINITRATE IN HYPERTENSIVE STROKE TRIAL-2 (RIGHT-2): SAFETY AND EFFICACY OF TRANSDERMAL GLYCERYL TRINITRATE, A NITRIC OXIDE DONOR
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
2Patient Representative on behalf of University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
3London School of Hygiene and Tropical Medicine, Department of Medical Statistics, London, United Kingdom
4University of East Anglia, Norwich Medical School, Norwich, United Kingdom
5University of Newcastle, The Medical School, Newcastle, United Kingdom
6University Hospital of Leicester, Department of Cardiovascular Sciences, Leicester, United Kingdom
7Keele University, Institute of Science and Technology, Keele, United Kingdom
8University of Lincoln, School of Health and Social Care, Lincoln, United Kingdom
9University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Introduction
High blood pressure (BP) is common in acute stroke and is associated with poor outcome. Previous hospital-based trials testing the effects of BP lowering on functional outcome have been inconclusive. The PIL-FAST and RIGHT pilot trials confirmed the feasibility of performing single-centre ambulance-based stroke trials in the UK. In both RIGHT and a subgroup of patients recruited within 6 hours into the large ENOS trial, transdermal glyceryl trinitrate (GTN, a nitric oxide donor) lowered BP and reduced death or disability. Based on these results, the Rapid Intervention with Glyceryl trinitrate in Hypertensive Stroke Trial-2 (RIGHT-2) is testing the safety and efficacy of transdermal GTN in the pre-hospital setting.
Methods
Over 1430 Paramedics from 8 UK ambulance services serving over 50 comprehensive or primary stroke care centres are screening, consenting, randomising and treating 1050 patients presenting within 4 hours of FAST-positive stroke and with systolic BP >120 mmHg. Treatment comprises GTN or similar sham patch and is continued in hospital for 3 days. The primary outcome is the modified Rankin Scale at day 90. Secondary outcomes include vascular events, disability, quality of life, mood and cognition. Neuroimaging and biomarkers are examining potential mechanisms of action.
Conclusion
Experiences with the trial and baseline characteristics of the recruited patients-to-date will be presented.
Trial registration number
ISRCTN 26986053
AS32-0072
STUDY OF ANTITHROMBOTIC TREATMENT AFTER INTRACEREBRAL HAEMORRHAGE (STATICH)
1Oslo University Hospital, Department of Internal Medicine, Oslo, Norway
2University of Oslo, Institute of Clinical Medicine, Oslo, Norway
3Akershus University Hospital, Department of Neurology, Lørenskog, Norway
4Umeå University Hospital, Department of Public Health and Clinical Medicine, Umeå, Sweden
5Herlev Gentoft Hospital and University of Copenhagen, Herlev, Denmark
6Karolinska Institute- Danderyds Hospital, Department of Clinical Sciences, Stockholm, Sweden
Background and Aims
For patients with prior intracerebral haemorrhage (ICH), little is known about benefits and harms of using antithrombotic drugs (antiplatelets or anticoagulants) for prevention of ischaemic events. Guidelines variably endorse both starting and avoiding such treatment, and clinical practice is varying. We wish to examine the safety and efficacy of this treatment principle.
Method
STATICH is an investigator-led, multicenter, randomised-controlled, open, blinded end-point clinical trial of antithrombotic treatment for prevention of ischaemic events in patients with spontaneous, primary ICH who have indication for antithrombotic treatment.
Patients with an indication for antiplatelet drugs will be randomised to antiplatelet drugs vs. no antithrombotic drugs. Patients with atrial fibrillation who have indication for anticoagulation will be randomised to anticoagulants vs. no anticoagulants (antiplatelet drugs are allowed).
Patients will be followed for two years and contacted again at 5 and 10 years. The primary outcome variable is recurrent symptomatic ICH. Secondary variables include other intra- and extracranial haemorrhage, ischaemic events, death, and functional and cognitive outcome.
In an MRI sub-study we will examine the association between MRI findings (e.g. cerebral microbleeds) and effects of antithrombotic treatment on the risk of recurrent ICH.
Results
Patient enrolment will start in 2018 and last until 2020. Target recruitment is 500 patients from hospitals in Norway, Sweden and Denmark.
Conclusion
We will determine:
1. the effect of antithrombotic drugs on the risk of recurrent ICH.
2. whether there is an interaction between MRI findings and the effect of antithrombotic drugs on the risk of recurrent ICH.
Trial registration number
EudraCT number: 2014–002636-13
AS32-0073
THE TRIPLE THERAPY PREVENTION OF RECURRENT INTRACEREBRAL DISEASE EVENTS TRIAL (TRIDENT): CHALLENGES AND COLLABORATIONS
1The George Institute for Global Health, Academic Project Operations, Sydney, Australia
2The George Institute for Global Health, Cardiovascular Division, Sydney, Australia
3Radboud University Nijmegen Medical Centre, Neurology, Nijmegen, Netherlands Antilles
4University of Edinburgh, Clinical Brain Sciences, Edinburgh, United Kingdom
5Linkuo Chang Gung Memorial Hospital, Neurology, Taipei, Taiwan R.O.C
6University of Kelaniya, Pharmacology, Colombo, Sri Lanka
7The George Institute for Global Health, Professorial Unit, Sydney, Australia
8The George Institute for Global Health, Neurology, Sydney, Australia
9The George Institute China at Peking University, Health Science Centre, Beijing, China
Background and Aims
The incidence and prognosis of acute intracerebral haemorrhage (ICH) is strongly linked to blood pressure (BP) levels but many patients do not received effective BP control. TRIDENT evaluates a simple combination BP lowering regimen in ICH patients. The aim is to determine the effectiveness of more intensive long term BP lowering, on top of standard care, using a triple low-dose combination BP lowering ‘Triple pill” regime on the time to first occurrence of recurrent stroke in ICH patients.
Method
An international, multi-centre, double blind, placebo controlled, parallel-group, randomised controlled trial involving 4200 patients from 100+ sites globally. After a 2-week run-in period, patients are randomised to treatment and followed up 6-monthly for an average of 3 years. The Triple Pill is manufactured and packaged in Australia. Principal funding is from National Health and Medical Research Council (NHMRC) of Australia.
Results
Study set-up from June 2016 led to patient recruitment commencing September 2017. Currently, nine (9) countries at various stages of participation: Australia, Sri Lanka, the Netherlands, UK and Taiwan recruiting patients; Japan, Malaysia, Switzerland and Singapore are at various stages of approvals and initiation activities.
Conclusion
Site start-up has been challenging, in particular navigating ethics, regulatory, drug labelling and importation requirements in each country. To recruit ICH stroke patients in the post-acute setting, collaboration between neurology, neurosurgery and rehabilitation are required, with solutions tailored to individual sites.
Trial registration number
NCT02699645
AS32-0074
HEMODYNAMICS AND STROKE RISK IN SYMPTOMATIC INTRACRANIAL ATHEROSCLEROTIC DISEASE: A COMPUTATIONAL FLUID DYNAMICS STUDY
1The Chinese University of Hong Kong, Department of Medicine & Therapeutics, Hong Kong, China
2The Chinese University of Hong Kong, Shenzhen Research Institute, Shenzhen, China
3The Chinese University of Hong Kong, Department of Imaging and Interventional Radiology, Hong Kong, China
4University of California Los Angeles, Neurovascular Imaging Research Core and UCLA Stroke Center- Department of Neurology, Los Angeles, USA
5The First Affiliated Hospital of Zhengzhou University, Department of Neurology, Zhengzhou, China
6Nanjing Drum Tower Hospital- Affiliated Hospital of Nanjing University Medical School, Department of Neurology, Nanjing, China
7Nanjing Drum Tower Hospital- Affiliated Hospital of Nanjing University Medical School, Department of Radiology, Nanjing, China
Background and Aims
Patients with symptomatic intracranial atherosclerotic stenosis (ICAS) are at high risk of recurrent stroke despite of medical treatment. We aimed to investigate whether hemodynamic features of symptomatic ICAS might correlate with the risk of stroke relapse, using a computational fluid dynamics (CFD) model.
Method
This is a longitudinal observational study. We recruited patients with acute ischemic stroke or transient ischemic attack attributed to ≥50% ICAS confirmed in CT angiography (CTA) from 3 teaching hospitals. A CFD model was built in each case based on CTA source images, to reveal and quantify the hemodynamic features of the qualifying ICAS lesion. All patients were followed up for 1 year. The primary outcome is recurrent ischemic stroke within the same territory within 1 year. We shall analyze the associations between CFD model-based hemodynamic features of ICAS and the primary outcome, independent of vascular risk factors and medications.
Results
Patient recruitment and follow-up, and CFD modeling procedures have been completed. Overall, 301 patients were recruited; 244 patients (mean age 60.5 years; 63.5% males) with a successfully built CFD model and complete follow-up information were included in analysis. The median intracranial stenosis was 66%. The median post- and pre-stenotic pressure ratio across the ICAS lesions was 0.94. Eighteen (7.4%) patients had a primary outcome. Assessment of other hemodynamic features of ICAS lesions and statistical analyses are underway.
Conclusion
Findings of the current study may shed light on the mechanisms of refractory stroke in patients with symptomatic ICAS and inform secondary prevention of these patients.
Trial registration number
N/A
AS32-0075
SIMULATION-BASED TRAINING OF RAPID EVALUATION AND MANAGEMENT FOR ACUTE STROKE (STREAM) TRIAL (STREAM)
1University Hospital, Neurology, Frankfurt, Germany
2University Hospital, Neurology, Augsburg, Germany
3University Hospital, Neurology, Cologne, Germany
4University Hospital Charite, Neurology, Berlin, Germany
5University Hospital, Neurology, Tuebingen, Germany
6University Hospital, Neurology, Heidelberg, Germany
7University Hospital, Neurology, Hamburg, Germany
8University Hospital, Neuroradiology, Muenich, Germany
9University Hospital, Neurology, Muenich, Germany
Background and Aims
The aim of this trial is to investigate the effect of a multimodal intervention consisting of a rigorous peer-to-peer-review of the stroke team algorithm, applying principles of crew resource management (CRM) and up to three sessions of a stroke team simulation training with a debriefing focusing on team communication in a controlled prospective pretest-posttest design at seven tertiary care stroke centers in Germany.
Method
In the pretest period, the participating seven centers (tertiary care university hospitals with thrombectomy capacity 24/7/365) record the data of all consecutive patients receiving thrombolysis and/or thrombectomy of all direct-to-center patients during a 3-month period. During the intervention phase, leading employees of different professional backgrounds will be invited to a joint “training of multipliers” seminar. After reviewing and adapting current workflow improvements, up to three stroke team simulation trainings are held at the participating centers and teaching materials will be provided with the aim of permanently starting up regular stroke team simulation. In the posttest period process times are recorded again for three months.
Primary outcome measure is the median “door-to-needle” time, which will be verified by independent source data verification. Secondary outcome measures include the median thrombectomy process times of patients receiving thrombectomy and hemorrhagic transformation in the control imaging as a safety endpoint. Staff satisfaction improvement is assessed by means of a pre-designed questionnaire. https://clinicaltrials.gov/ct2/show/NCT03228251.
Results
The recruitment of this study is ongoing. Preliminary results of the observation phase I will be shown at the ESOC. Final results are expected in december 2018.
Conclusion
n/a
Trial registration number
NCT03228251
AS32-0076
DABIGATRAN VERSUS ACETYLSALICYLIC ACID FOR SECONDARY STROKE PREVENTION IN PATIENTS WITH EMBOLIC STROKE OF UNDETERMINED SOURCE: RATIONALE, DESIGN AND BASELINE DATA FROM RE-SPECT ESUS™
1University Hospital Essen, Department of Neurology, Essen, Germany
2University of California, UCSF Department of Neurology, San Francisco- CA, USA
3Duke Clinical Research Institute, Cardiovascular Medicine, Durham- NC, USA
4Boehringer Ingelheim International GmbH & Co. KG, Clinical Development Cardiometabolism, Ingelheim am Rhein, Germany
5Boehringer Ingelheim Ltd/Lte, Clinical Development Cardiometabolism, Burlington, Canada
6Boehringer Ingelheim Pharma GmbH & Co. KG, Clinical Research, Biberach, Germany
7Boehringer Ingelheim Pharmaceuticals Inc., Biostatistics, Ridgefield- CT, USA
8University of Miami- Miller School of Medicine Miami, Department of Neurology, Florida, USA
Background and Aims
The optimal antithrombotic treatment for the prevention of recurrent stroke in patients with embolic strokes of undetermined source (ESUS) is unknown.
Method
The phase III, double-blind, randomized RE-SPECT ESUS™ trial is comparing dabigatran etexilate 150 mg twice daily (or 110 mg twice daily in patients aged ≥ 75 years or with renal dysfunction) with acetylsalicylic acid (100 mg once daily) for secondary stroke prevention in patients with ESUS. Eligibility criteria include ESUS diagnosed within 3 months prior to randomization (6 months in selected patients), modified Rankin score ≤ 3 and age ≥ 60 years or 18–59 years with ≥ 1 stroke risk factor. The primary efficacy outcome is time to first recurrent stroke. The main safety outcome is time to first major haemorrhage.
Results
As of 22 February 2018, 5,390 patients were randomized and randomization has been closed; baseline characteristics are available for 5,386 patients (table). Duration of cardiac monitoring before inclusion: 0–19 hours, 20–47 hours, > 48–72 hours and > 72 hours in 0.6%, 82.6%, 5.5%, and 11.3% of patients, respectively. Updated baseline characteristics will be presented.
Conclusion
Findings from RE-SPECT ESUS will help physicians optimally treat patients with ESUS to prevent subsequent strokes.

Trial registration number
NCT02239120
AS32-0078
A REDUCTION IN TIME WITH ELECTRONIC MONITORING IN STROKE (ARTEMIS) TRIAL
1Leiden University Medical Center, Neurology, Leiden, The Netherlands
2Academic Medical Center, Neurology, Amsterdam, The Netherlands
3RAV Holland Midden, Emergency Medical Services, Leiden, The Netherlands
4Medical Spectrum Twente, Neurology, Enschede, The Netherlands
5Leiden University Medical Center, Clinical Epidemiology, Leiden, The Netherlands
6Julius Center – University Medical Center Utrecht, Clinical Epidemiology, Utrecht, The Netherlands
Background and Aims
Time is the most crucial factor for the clinical benefit of intravenous thrombolysis (IVT) and endovascular thrombectomy (EVT). The delay from notification at the Emergency Medical Services (EMS) dispatch office until initiation of acute treatment depends on logistics and collaboration between various caregivers in this trajectory (identified as ‘total system delay’ [TSD]). We aim to evaluate whether real-time audio-visual feedback to caregivers will reduce treatment delays.
Method
The ‘A Reduction in Time with Electronic Monitoring In Stroke’ (ARTEMIS) trial is a multiregional, multicenter, randomized open end-point trial. We will include consecutive, adult patients that are considered potentially eligible for IVT and/or EVT by the EMS dispatch office or paramedic on-site in three regions in the Netherlands. Real-time audio-visual feedback on actual TSD will be provided to caregivers through an automatic tracking system, using patient-specific Bluetooth wristbands and pre-mounted tablets throughout the entire trajectory. Randomization of real-time audio-visual feedback will be per patient. By including 75 EVT- and 225 IVT-patients in each arm (real-time audio-visual feedback vs. regular care), we will be able to demonstrate a 20-minute reduction on TSD to EVT and a 10-minute reduction on TSD to IVT.
Results
The study is ongoing in Leiden region since February 2018, with current inclusion number of 6 patients. It is expected that Amsterdam region will start in April 2018 and Twente region in May 2018. The study is ongoing through 2020.
Conclusion
The ARTEMIS trial will investigate whether real-time audio-visual feedback to caregivers within the acute stroke trajectory will reduce TSD to IVT and/or EVT.
Trial registration number
www.clinicaltrials.gov: NCT02808806
AS32-0079
ACUTE NEUROLOGICAL CARE IN NORTH-EASTERN GERMANY WITH TELEMEDICAL SUPPORT (ANNOTEM): THE EXTENSION OF TELENEUROLOGY TO NEUROLOGICAL EMERGENCIES BEYOND STROKE
1Charité – Universitätsmedizin Berlin, Neurology, Berlin, Germany
Background and Aims
Teleneurological networks offer the opportunity to transfer neurological expertise into areas with limited availability of neurologists as well as implementing regionally sustainable structures to improve patient care. With regard to stroke, such networks have been extensively evaluated in recent years. Within the framework of ANNOTeM, a teleneurological network structure for and beyond stroke has been established and will be evaluated. In addition to stroke, acute neurological diseases such as status epilepticus, meningitis/encephalitis, traumatic brain injuries and acute cross-sectional syndromes are considered as inclusion diagnoses.
Method
In order to achieve this goal, eleven regional hospitals in North-Eastern Germany, eight of them without specialized acute neurological care, have been integrated into a network with telemedicine assistance from three comprehensive neurology centers. In addition, quality of care program with specialized treatment units, staff education, standardised operating procedures, emergency patient transfer algorithms and new technologies (Tele-EEG using dry electrode caps). The evaluation will be carried out as a controlled study with a before-and-after comparison of process data, mortality and need for long-term care between July 2017 and February 2020. The primary analysis will be complement by a health economic evaluation.
Results
N/A (Ongoing trial)
Conclusion
Within the framework of the teleneurological network ANNOTeM, established processes of telestroke treatment have been transferred to additional relevant acute-neurological diseases and will be evaluated with respect to primary outcome parameters as well as health economics.
Trial registration number
DRKS00013067
AS32-0080
SWISS TRIAL OF INITIAL DECOMPRESSIVE CRANIECTOMY VERSUS BEST MEDICAL TREATMENT OF SPONTANEOUS SUPRATENTORIAL INTRACEREBRAL HEMORRHAGE: A RANDOMIZED TRIAL (SWITCH)
1Bern University Hospital and University of Bern, Department of Neurosurgery, Bern, Switzerland
2Helsinki University Central Hospital, Department of Neurology, Helsinki, Finland
3Medical University of Johannes Gutenberg University Mainz, Department of Neurosurgery, Mainz, Germany
4Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland
Background and Aims
Decompressive craniectomy (DC) is beneficial in patients with various diseases including malignant middle cerebral artery (MCA) infarction. In intracerebral hemorrhage (ICH), decompressive craniectomy without hematoma evacuation has only been evaluated in small retrospective studies with a trend towards reduced mortality. However, no randomized trial has ever assessed whether DC is beneficial in ICH. Therefore, the prospective randomized SWITCH trial was initiated in October 2014 to determine whether decompressive surgery and best medical treatment in patients with spontaneous ICH will improve outcome compared to best medical treatment (BMT) only.
Method
SWITCH is an international multi-center randomized trial. 300 patients will be randomized (1:1) into either DC and BMT or BMT alone. Main inclusion criteria are spontaneous ICH of deep origin, NIHSS≥10 and ≤30, GCS>7 and < 14 and ICH volume >30 and < 100. The primary endpoint is severe disability and mortality, measured with the modified Rankin score 6 months after ictus.
Results
Recruitment started in October 2014. We currently have 31 sites open in Switzerland and in 5 other European countries. 71 patients were so far successfully randomized into the trial.
Conclusion
After initiation of SWITCH, we could increase the number of open centers to 31 and currently 71 patients have been randomized into the SWITCH trial. Further centers are still highly welcome and we believe that maintaining a high recruitment will be key for successful completion of the trial.
Trial registration number
ClinicalTrials.gov Identifier: NCT02258919
AS32-0081
SOLITAIRE™ WITH THE INTENTION FOR THROMBECTOMY PLUS INTRAVENOUS T-PA VERSUS DIRECT SOLITAIRE™ STENT-RETRIEVER THROMBECTOMY IN ACUTE ANTERIOR CIRCULATION STROKE (SWIFT DIRECT)
1Bern University Hospital- Inselspital, Department of Neurology, Bern, Switzerland
2Toronto Western Hospital, Department of Medical Imaging, Toronto, Canada
3Alfried Krupp Krankenhaus Rüttenscheid, Clinic for Radiology and Neuroradiology, Essen, Germany
4University at Buffalo, Neurosurgery, Buffalo, USA
5Bern University Hospital- Inselspital, Department of Neuroradiology, Bern, Switzerland
6Vanderbilt University Medical Center, Department of Neurology, Nashville, USA
7Centre Hospitalier Universitaire de Toulouse, Hôpital Purpan, Toulouse, France
8UH Cleveland Medical Center, Department of Neurology, Cleveland Ohio, USA
9University of California, Department of Neurology, Los Angeles, USA
Background and Aims
Whether pre-treatment with intravenous thrombolysis (IVT) prior to mechanical thrombectomy (MT) with stent retrievers is beneficial has become a matter of debate. In a patient-level pooled analysis of five randomized controlled studies (HERMES collaboration) the treatment effect size of MT did not differ between patients receiving IVT and those treated with MT alone. SWIFT DIRECT aims to determine, whether direct MT in patients with proximal vessel occlusion in the anterior circulation is non-inferior to IVT and MT.
Method
The international, multicentre, randomised-controlled, two-arm, open label, blinded endpoint (PROBE) trial SWIFT DIRECT will randomize 404 patients into the experimental arm (direct MT; 202) or control arm (bridging thrombolysis; 202). The trial will only be performed in patients with immediate access to MT. Main inclusion criteria are signed informed consent, age >18 and < 86 years, confirmed ischaemic stroke, NIHSS ≥8 and < 30 and eligibility for IVT and MT. The primary outcome is functional independence (mRS) ≤2 at 90 days. Main secondary outcomes are mortality, change in NIHSS score post randomization, time to reperfusion (TICI ≥2b) and quality of life.
Results
The recruitment started in October 2017. Eleven patients have been enrolled by 25.03.2018. Over 30 sites in Switzerland, Germany, Austria, France, Spain, Finland and Canada will participate in this clinical trial.
Conclusion
If direct MT in patients with large artery vessel occlusion in the anterior circulation is as safe and efficacious as IVT and MT, this would have a relevant impact on future stroke management.
Trial registration number
NCT03192332
AS32-0082
EARLY VERSUS LATE INITIATION OF DIRECT ORAL ANTICOAGULANTS IN POST-ISCHAEMIC STROKE PATIENTS WITH ATRIAL FIBRILLATION (ELAN): AN INTERNATIONAL MULTICENTRE, RANDOMISED-CONTROLLED, TWO-ARM, ASSESSOR-BLINDED TRIAL
1Inselspital, Department of Neurology, Bern, Switzerland
2University Hospital Helsinki, Department of Neurology, Helsinki, Finland
3University Hospital Perugia, Department of Internal Medicine, Perugia, Italy
4University Clinics Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany
5University of Thessaly, Department of Internal Medicine, Larissa, Greece
6University Hospital Basel, Department of Neurology, Basel, Switzerland
7University Hospital Lausanne, Department of Neurology, Lausanne, Switzerland
8Cantonal Hospital Aarau, Department of Neurology, Aarau, Switzerland
9University Hospital and University of Bern, Clinical Trial Unit, Bern, Switzerland
10University Clinics Graz, Department of Neurology, Graz, Austria
11Oslo University Hospital, Department of Neurology, Oslo, Norway
12University of Glasgow, Department of Neurology, Glasgow, United Kingdom
Background and Aims
When to start anticoagulation in ischaemic stroke patients with atrial fibrillation (AF) is a relevant unanswered question. Direct oral anticoagulants (DOACs) are at least as effective as Vitamin K antagonists in reducing stroke and systemic embolism and have a lower risk of intracranial haemorrhage. The ELAN trial will determine the net benefit of early versus late initiation of DOACs in patients with acute ischaemic stroke related to AF with respect to stroke size.
Method
This international, multicentre, randomised-controlled, two-arm trial will randomise 2’000 patients into the experimental arm (early treatment; 1’000) or control arm (late treatment, 1’000). The time of DOAC initiation will vary depending on stroke size (i.e., minor, moderate, or major). Main inclusion criteria are signed informed consent, age >18 years, confirmed ischaemic stroke and AF and agreement of treating physician to prescribe DOACs. The primary outcome is a composite of major bleeding, recurrent ischaemic stroke, systemic embolism and/or vascular death at 30 ± 3 days after randomisation.
Results
Recruitment at 13 sites in Switzerland and 2 sites in EU has started in October 2017. Approximately 80 sites in 10 European countries will eventually be recruiting patients.
Conclusion
This pragmatic trial will add evidence to the best time of starting DOACs after ischaemic stroke in patients with AF. If earlier initiation of DOACs in patients with ischaemic stroke related to AF is shown to be safe and efficacious, this could have a major impact on better treatment adherence, length of hospital stay and patient outcome.
Trial registration number
ClinicalTrials.gov Identifier: NCT03148457
AS32-0083
RNA SEQUENCING ANALYSIS IN LARGE VESSEL OCCLUSION STROKE DATA BANK, HUMAN RNASA-LVOS BANK, THE FUTURISTIC FINGER PRINT RECOGNITION OF STROKE SOURCE
1Faculty of Medicine, stroke and interventional neurology, Alexandria, Egypt
Background
The source of embolic stroke, in thrombotic embolism, is of unknown origin in 30–40% of cases. Fortunately, Mechanical thrombectomy provide a direct method to retrieve the stroke-incriminated clots from stroke patients for possibility of exo-autopsy analysis.
Aim
collecting stroke-incriminated clots from definite known etiological sources, could build a matchable markers database (MMD) to identify the source of cryptogenic embolism in the near-future. Identification of that markers is done by novel RNA sequencing technology to identify the clot composition in direct way.
Method
This is a prospective double blinded controlled investigational REB-approved study of acute LVO ischemic stroke in patients receiving mechanical thrombectomy at a multiple centers. Immediately after thrombi will be retrieved by mechanical thrombectomy, they will be placed in RNA stabilization and storage solution (RNAlater). Each sample will be extracted for total RNA by the one approved regional university’s Human Genomics lab using a standard protocol. NanoDrop Microvolume Spectrophotometers and Fluorometer will be used for RNA quantification. Thrombi weight will be recorded among other clinical data,procedural data, and macroscopic clot morphology. Clots analysis will be divided into 2 groups where Group A : include clots with definite stroke etiology and submitted to the RNA analysis in blinded coded label. Group B: include all clots with unknown stroke etiology and submitted to RNA analysis in cryptogenic label.
Results
the trial will be conducted from 2018 to 2022. All analysis will be re-audited in central genome analysis lab of Alexandria University.
Conclusion
NA
Trial registration number
NA
AS32-0085
TIMING OF ORAL ANTICOAGULANT THERAPY IN ACUTE ISCHEMIC STROKE WITH ATRIAL FIBRILLATION: THE FIRST REGISTRY-BASED RANDOMISED CONTROLLED STROKE TRIAL
1Uppsala University, Department of Medical Sciences, Uppsala, Sweden
2Västerbotten County Council, The Swedish Stroke Register, Umeå, Sweden
3Uppsala University, Uppsala Clinical Research Center, Uppsala, Sweden
4Lund University, Department of Clinical Sciences- Neurology, Lund, Sweden
5Umeå University, Deptarment of Public Health and Clinical Sciences, Umeå, Sweden
6Karolinska Institutet, Deptarment of Clinical Sciences- Danderyd Hospital, Stockholm, Sweden
Background and Aims
Current guidelines do not provide evidence-based recommendations on optimal time-point to start non-vitamin K antagonist oral anticoagulants (NOACs) after ischemic stroke in patients with atrial fibrillation (AF). The TIMING study aims to establish the efficacy and safety of early vs. delayed initiation of NOACs in these patients.
Method
The TIMING study is a national, investigator led, registry-based, multicentre, open-label, randomised controlled study. The Swedish Stroke Register is used for enrolment, randomisation and follow-up of 3000 patients, who are randomized (1:1) within 72 hours from stroke onset to either early (≤4 days) or delayed (5-10 days) start of NOAC. Primary outcome is the composite of recurrent ischemic stroke, symptomatic intracerebral haemorrhage, or all-cause mortality within 90 days after randomisation. In an optional biomarker substudy, blood samples are collected from approximately half of the patients for central analysis of cardiovascular biomarkers after study completion.
Results
Enrolment of patients started in April 2017 and is anticipated to continue throughout 2019. Recruitment of stroke units is still ongoing. The independent Data Monitoring and Safety Committee oversaw study conduct in December 2017 without any recommendations of study changes. As of March 28, 2018, the 28 participating stroke units had included 129 patients.
Conclusion
The TIMING study addresses the ongoing clinical dilemma of when to start NOAC after ischemic stroke in patients with AF. By the inclusion of a randomisation module within the Swedish Stroke Register, the advantages of a prospective randomised study design is combined with the strengths of a comprehensive clinical quality register.
Trial registration number
ClinicalTrials.gov Identifier: NCT02961348.
AS32-0086
TELE-STROKE: PREHOSPITAL IDENTIFICATION OF PATIENTS WITH SUSPECTED STROKE USING ONSITE MOBILE TELEMEDICINE – FEASIBILITY (TELE-STROKE)
1University Hospital Basel, Neurology / Stroke Center, Basel, Switzerland
2University Hospital Basel, Emergency Center, Basel, Switzerland
3University Hospital Basel, Anaesthesiology, Basel, Switzerland
4University Hospital Basel, Medical Intensive Care Unit, Basel, Switzerland
5University Hospital Basel, Clinical Trial Unit, Basel, Switzerland
6University Hospital Basel, Information & Communication Technology, Basel, Switzerland
Background and Aims
One of today’s challenges in stroke medicine is to further decrease event-to-treatment-time. Our aim is to optimize triage of presumed stroke patients already before arrival at the hospital using a video link connecting ambulance and stroke specialist.
We hypothesize that door-to-needle-/-groin-puncture-time can be decreased by evaluating potential stroke patients via video as ER admission can be bypassed and patients with a suspected stroke can proceed directly to imaging.
Method
In this observational, prospective cohort-study 120 subjects will be analyzed to investigate feasibility of our local telestroke-concept. In the first two phases ten healthy subjects and ten stroke patients were examined and recorded in order to establish our protocol, using the RACE-Score (items: facial palsy, arm/leg motor function, head/gaze deviation, aphasia/agnosia). Consecutively 100 presumed stroke patients will be analyzed in acute settings as emergency department or ambulance and a decision is simulated: Either admission directly to imaging, or first to the ER for further clinical examination.
Results will be independently validated and compared to on-site-examination results. Ultimately RACE-Scores will be analyzed to define a cut-off-score for subsequent studies.
Technically a VIDYO®-connection is established between a mobile device (I-Phone 7S®) on-site and a personal computer, run by the stroke professional off site. A short briefing and the neurol.examination are recorded on a protected server. Stroke is defined as a focal neurological deficit with acute onset and presence of a corresponding vessel occlusion in angiography, signs of bleeding or early ischemic injury on CT, or corresponding lesion on diffusion weighted MRI (DWI).
Results
N/A
Conclusion
N/A
Trial registration number
NCT03370094
AS32-0087
DETERMINING OPTIMAL EARLY REHABILITATION AFTER STROKE (AVERT-DOSE): A MULTI-ARM COVARIATE-ADJUSTED, RESPONSE-ADAPTIVE RANDOMISED CONTROLLED TRIAL
1University of Melbourne, Stroke Division- The Florey Institute of Neuroscience and Mental Health, Heidelberg, Australia
2University of Melbourne, Statistics and Decision Analysis- The Florey Institute of Neuroscience and Mental Health, Heidelberg, Australia
3University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
4Christian Medical College, Department of Neurology, Ludhiana, India
5Monash University, Eastern Health Clinical School, Clayton, Australia
6Monash University, Penisula Clinical School, Clayton, Australia
7University of Newcastle, School of Health Sciences and Priority Research Centre for Stroke and Brain Injury, Newcastle, Australia
8Deakin University, Deakin Health Economics, Burwood, Australia
9Australian Catholic University, Nursing Research Institute, Sydney, Australia
10Monash University, Department of Medicine- School of Clinical Sciences at Monash Health, Clayton, Australia
11Auckland District Health Board, Allied Health, Auckland, New Zealand
12Norwegian University of Science And Technology, The Institute for Neuromedicine, Trondheim, Norway
13Singapore General Hospital, Physiotherapy Department, Singapore, Singapore
14University of South Australia, Sansom Institute for Health Research, Adelaide, Australia
15University Kebangsaan Malaysia, Department of Physiotherapy- Hospital Canselor Tuanku Muhriz, Kuala Lumur, Malaysia
16University of Sydney, Sydney Medical School, Sydney, Australia
17University of Melbourne, Professor of Translational Neuroscience, Parkville, Australia
18University of Melbourne, The Florey Institute of Neuroscience and Mental Health, Heidelberg, Australia
Background and Aims
In 2015, we completed the landmark, international RCT of early rehabilitation (The Lancet, 2015). We determined that too much training early interferes with stroke recovery and that most patients may be responsive to therapy if the right dose can be found (Neurology 2016). The aim of this study is to define the optimal early intervention regimens for people with mild and moderate stroke severity.
Method
We will use a multi-arm, dose-finding, Covariate-Adjusted, Response-Adaptive (CARA) Randomised Clinical Trial (Figure 1) in two specified mild and moderate stroke severity strata. We will test three separate rehabilitation intervention regimens in each strata against a pre-specified control to identify the intervention regimen that results in fewer disabled patients at 3 months post stroke (mRS 0–2). A sample size of 2,572 patients will allow us to independently observe pre-specified effects in these two strata with power 80% and significance threshold of p = 0.025. All analyses will be intention-to-treat. Patients with mild to moderate stroke will be recruited using our global trials network in Australia, New Zealand, Singapore, Malaysia, India and United Kingdom.
Results
The trial protocol is in final stages of development with site identification underway.
Conclusion
AVERT-DOSE will establish clear, definitive, early intervention protocols, that will ensure that stroke patients receive best evidence care, both here and in developing health service systems.
Trial registration number
Protocol under development
AS32-0088
COLCHICINE FOR PREVENTION OF VASCULAR INFLAMMATION IN NON-CARDIOEMBOLIC STROKE (CONVINCE) – A RANDOMISED CLINICAL TRIAL
1University College Dublin, Stroke Clinical Trials Network Ireland, Dublin, Ireland
2Mater Misercordiae University Hospital, Vascular Neurology, Dublin, Ireland
3Tel Aviv University, Sackler Faculty of Medicine, Tel Aviv, Israel
4Chaim Sheba Medical Center- Tel Hashomer, Joseph Sagol Neuroscience Center, Tel Hashomer, Israel
5Institute of Psychiatry and Neurolog, 2nd Department of Neurology, Warsaw, Poland
6University Hospital Inselspital- Bern., Acute Neurology and Stroke, Bern, Switzerland
7Hospital de Santa Maria, Department of Neurology, Lisbon, Portugal
8University of Calgary, Department of Clinical Neurosciences, Calgary, Canada
9Vilnius University Clinic of Neurology and Neurosurgery Republic Vilnius University Hospital, Department of Neurology, Vilnius, Lithuania
10University of Tartu- Institute of Clinical Medicine, Department of Neurology and Neurosurgery, Tartu, Estonia
11University Hospital of Copenhagen- Herlev Hospital, Department of Neurology, Copenhagen, Denmark
12UZ Leuven, Department of Neurology, Leuven, Belgium
13St. Anne's University Hospital, Neurology Department, Brno, Czech Republic
14Mater Misercordiae University Hospital, Acute Stroke Service, Dublin, Ireland
15Royal College of Surgeons ireland, Medicine, Dublin, Ireland
16Cleveland Clinic Abu Dhabi., Department of Neurology, Abu Dhabi, United Arab Emirates
17Newcastle University-, Stroke Research Group, Newcastle-Upon-Tyne, United Kingdom
18Universitat de Lleida- Hospital Universitari Arnau de Vilanova de Leida, Department of Neurology, Lleida, Spain
19Tel Aviv University, Sackler Faculty of Medicine-, Tel Aviv, Israel
20Joseph Sagol Neuroscience Center- Chaim Sheba Medical Center, Department of Stroke, Tel Hashomer, Israel
21University Medical Center in Utrecht, Department of Neurology, Utrecht, The Netherlands
22University Hospital Essen, Department of Neurology, Essen, Germany
23Health Research Board, Clinical Research, Multiple Sites, Ireland
Background and Aims
After ischaemic stroke/TIA, the 5-year recurrence risk is 20–25%. Arterial wall inflammation is important in the pathogenesis of non-cardioembolic stroke. Colchicine is an inexpensive anti-inflammatory agent, orally-available, with an established safety and efficacy profile. Experimental and clinical data suggest that low-dose colchicine may inhibit plaque inflammation and vascular events.
Method
CONVINCE is a randomised prospective open-label blinded endpoint assessment (PROBE) clinical trial of low-dose (0.5mg) colchicine plus usual care compared with usual care alone for the prevention of vascular events (non-fatal recurrent stroke/myocardial infarction/unstable angina or vascular death) after non-cardioembolic stroke/TIA. 3500 patients will be randomised and followed for a median of 36 months.
Patients older than 40 years with non-cardioembolic ischemic stroke/TIA, within 72 hours to 28 days of onset, will be included.
Results
Of 135 planned sites, 33 are recruiting across Ireland, UK, Spain and Belgium. 217 patients have been randomised (average 1/site/month). Tolerability is good (early discontinuation rates < 5%). No significant safety concerns have been identified. Site activations in Germany, Estonia, Lithuania, Poland, Netherlands, Portugal, Denmark, Switzerland, Czech Republic, Israel, Canada and UAE are under way.
Conclusion
CONVINCE is the first large RCT testing anti-inflammatory therapy for secondary prevention after stroke.
Trial registration number
NCT02898610
AS32-0089
TENECTEPLASE IN WAKE-UP ISCHAEMIC STROKE TRIAL
1UiT The Arctic University of Norway, Department of Clinical Medicine, Tromsdalen, Norway
2Hospital of Southern Norway, Department of Neurology, Kristiansand, Norway
3Oslo University Hospital, Department of Neurology, Oslo, Norway
4Bispebjerg Hospital, Department of Neurology, Copenhagen, Denmark
5Rigshospitalet, Department of Neurology, Copenhagen, Denmark
6Skane University Hospital, Department of Neurology, Malmö, Sweden
7Karolinska Institute, Department of Neurology, Stockholm, Sweden
8Helsinki University Hospital, Department of Neurology, Helsinki, Finland
9University of Tartu, Department of Neurology and Neurosurgery, Tartu, Estonia
10Vilnius University, Institute of Clinical Medicine, Vilnius, Lithuania
11University Hospital of Basel, Department of Neurology, Basel, Switzerland
12UCL Institute of Neurology, National Hospital for Neurology and Neurosurgery, London, United Kingdom
13University of Leicester, Department of Cardiovascular Sciences, Leicester, United Kingdom
14UiT The Arctic University of Norway, Department of Clinical Medicine, Tromsø, Norway
15Oslo University Hospital, Department of Cardiology, Oslo, Norway
Background and Aims
Patients with wake-up stroke have traditionally been considered ineligible for intravenous thrombolytic treatment. Tenecteplase has pharmacological advantages over alteplase, and can be given as a bolus. We are performing a pragmatic, CT-based, randomised-controlled, open trial of tenecteplase for patients with wake-up stroke; the Tenecteplase in Wake-up Ischaemic Stroke Trial (TWIST).
Method
Patients with wake-up stroke < 4.5 hours and without evidence of large infarct or proximal artery occlusion will be randomised to tenecteplase 0.25 mg/kg plus standard care or standard care alone. Plain brain CT and CT angiography will be done before randomisation and repeated on day 2. CT perfusion will be done at selected centres. Follow-up will be done at discharge (or day 7) and by telephone at 3 months.
The primary effect variable is functional outcome at 3 months, measured by the modified Rankin Scale.
Results
The target is to include 500 patients from centres in Norway, Sweden, Denmark, Finland, Estonia, Lithuania, UK, and Switzerland. Start of patient inclusion: June 2017. Planned study period: two years.
Study questions to be answered:
1. Can thrombolytic treatment with tenecteplase within 4.5 hours of wake-up improve functional outcome at 3 months?
2. Can findings on CT angiography or CT perfusion identify patients who benefit from such treatment, compared to patients without such findings?
Conclusion
TWIST will show whether patients with wake-up stroke can be treated with tenecteplase within 4.5 hours of awakening, and whether multi-modal CT can be used for identification of patients who benefit from treatment.
Trial registration number
ClinicalTrials.gov Identifier: NCT03181360
AS32-0090
ATRIAL FIBRILLATION IN CRYPTOGENIC STROKE THE NORDIC ATRIAL FIBRILLATION AND STROKE STUDY (NOR-FIB
1Østfold Hospital Trust, Department of Neurology, Grålum, Norway
2University of Oslo, Institute of Clinical Medicine, Oslo, Norway
3Oslo University Hospital, Department of Neurology, Oslo, Norway
4Oslo University Hospital, Department of Internal Medicine, Oslo, Norway
5Vestfold Hospital, Department of Neurology, Tønsberg, Norway
6Vestre Viken Hospital Trust, Department of Internal Medicine, Bærum, Norway
7More and Romsdal Hospital Trust, Department of Neurology, Molde, Norway
8Diakonhjemmet Hospital, Department of Internal Medicine, Oslo, Norway
9Stavanger University Hospital, Department of Neurology, Oslo, Norway
10Innlandet Hospital Trust, Department of Neurology, Lillehammer, Norway
11Nordland Hospital, Department of Neurology, Bodø, Norway
12Rigshospitalet University Hospital, Department of Neurology, Copenhagen, Denmark
13Firalis SA, Biomarker R&D, Huningue, France
14Østfold Hospital Trust, Department of Cardiology, Grålum, Norway
15Oslo University Hospital, Department of Cardiology, Oslo, Norway
Background and Aims
The optimal duration and timing of cardiac rhythm monitoring after cryptogenic stroke is unknown. Identification of reliable biomarkers indicating AF will be valuable in the selection of patients for prolonged cardiac rhythm monitoring. The purpose of the study is to assess the incidence of AF detection using implantable cardiac monitors (Reveal LINQ®) in patients with cryptogenic stroke or TIA and to identify biomarkers that can be used as predictors of incident AF.
Method
Our study is a multi-center prospective observational study of the occurrence of AF in cryptogenic stroke / TIA patients with implantable cardiac monitors for 12 months. Blood samples measuring biomarkers are taken in the acute phase and at 12 monthś follow-up. Estimated number of patients to be included in the study is 500.
Results
By March 2018, the total number of patients included in 11 out of 18 participating centres, is 76. Out of 76 included patients, AF or atrial flutter has been detected in 18 patients, resulting in detection rate of 23,7 %. The pilot study has identified biomarkers that seem to be useful for the detection of AF in cryptogenic stroke / TIA.
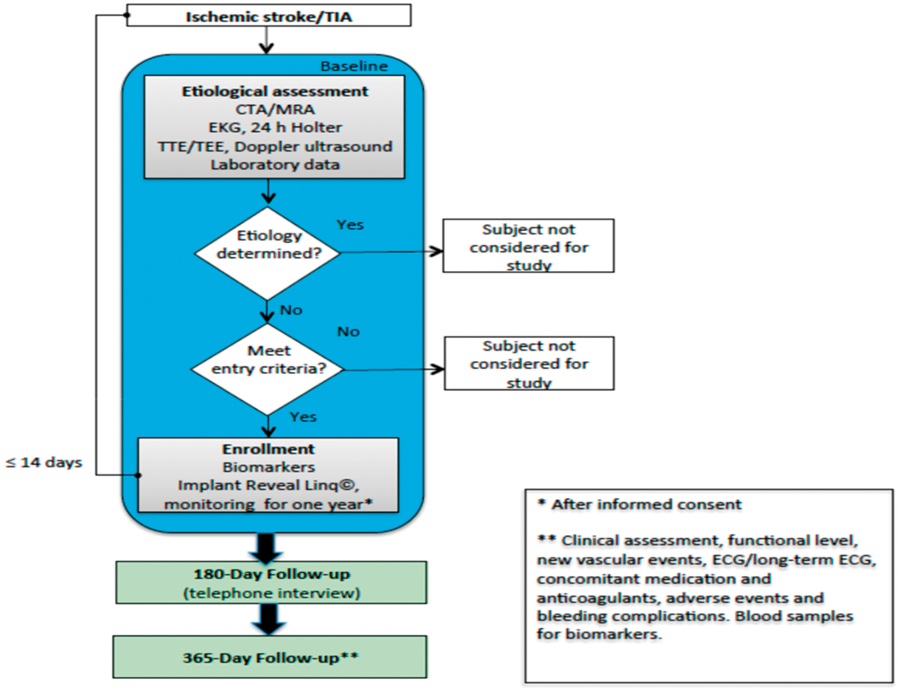
Conclusion
Updated interim analysis of included patients will be presented as well as new results from extended analyses of biomarkers.
Trial registration number
NCT02937077
AS32-0091
THE BENEFIT OF EXTENDING ORAL ANTICOAGULANT TREATMENT AFTER ACUTE CEREBRAL VEIN THROMBOSIS (EXCOA-CVT): A CLUSTER OBSERVATIONAL STUDY
1Centro Hospitalar Lisboa Norte – Hospital de Santa Maria, Neurology, Lisboa, Portugal
2Christian Medical College and Hospital, Department of Neurological Sciences, Vellore- Tamil Nadu, India
3Instituto Nacional de Neurologia y Neurocirurgia Manuel Velasco Suárez, Department of Neurology, Mexico City, Mexico
4Hospital H+, Neurology, Querétaro, Mexico
5Shiraz University of Medical Sciences, Clinical Neurology Research Center, Shiraz, Iran
6Hospital de São João – Centro Hospitalar São João, Neurology Department, Porto, Portugal
7Hospital das Clínicas – São Paulo University, Neurology Clinical Division, São Paulo, Brazil
8Academic Medical Center, Department of Neurology, Amsterdam, The Netherlands
9Hospital de Santa Maria-CHLN, Department of Neurosciences and Mental Health-Neurology-, Lisbon, Portugal
Background and Aims
After cerebral vein thrombosis (CVT) there is an increased risk of further venous thromboembolic events (VTEs). Guidelines suggest oral anticoagulation (OAC) for 3 to 12 months after a first episode of CVT, depending on event-related features and thrombophilic characteristics. Recommendations are extrapolated from extracerebral vein thrombosis, which may be inaccurate as the risk of thrombotic recurrence is different.
EXCOA-CVT is a prospective study with a cluster-randomised allocation design that aims to compare a policy of standard (3-6 months) versus extended (12 months) OAC in the prevention of VTEs after CVT.
Method
Participating centres are asked whether they have preference for any of the policy treatment options. Centres with no preference are randomly allocated for one of the two options. Adult subjects with confirmed CVT will be treated according to the approach allocated to their centre as soon as their acute clinical situation is stable and not more than 1 month after CVT diagnosis. Those with conditions judged by the investigator to be absolute indication for prolonged OAC will be excluded. Follow-up will be performed at 6, 12, 18 (telephone-interview) and 24 months. Primary efficacy outcome is any symptomatic and confirmed VTE (recurrent CVT or other systemic VTE) or death associated with venous thromboembolism. Primary safety endpoints include bleeding events (major/minor and according to the site), and death from any cause.
Results
At present, a total of 563 subjects with CVT have been included from 29 active centres.
Conclusion
The results of this study will provide crucial evidence regarding optimal duration of OAC after CVT.
Trial registration number
ISRCTN25644448
Miscellaneous
AS32-0026
MILD ENCEPHALITIS/ENCEPHALOPATHY WITH REVERSIBLE SPLENIAL LESION (MERS) IN ADULTS-A CASE REPORT AND LITERATURE REVIEW
1Beijing Chaoyang Hospital- Capital Medical University-, Department of Neurology- Beijing Chaoyang Hospital- Capital Medical University-, beijing, China
Background and Aims
Mild encephalitis/encephalopathy with reversible splenial lesion (MERS) is a rare clinico-radiological entity characterized by the magnetic resonance imaging (MRI) finding of a reversible lesion in the corpus callosum, sometimes involved the symmetrical white matters. Many cases of child-onset MERS with various causes have been reported. However, adult-onset MERS is relatively rare. The clinical characteristics and pathophysiologiccal mechanisms of adult-onset MERS are not well understood. We reviewed the literature on adult-onset MERS in order to describe the characteristics of MERS in adults and to provide experiences for clinician.
Method
We reported a case of adult-onset MERS with acute urinary retension and performed literature search from PubMed and web of science databases to identify other adult-onset MERS reports from Januarary 2004 to March 2016. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline was followed on selection process. And then we summarized the clinico-radiological features of adult-onset MERS.
Results
Twenty-nine adult-onset MERS cases were reviewed from available literature including the case we have. 86.2% of the cases (25/29) were reported in Asia, especially in Japan. Ages varied between 18 and 59 years old with a 12:17 female-to-male ratio. The major cause was infection by virus or bacteria. Fever and headache were the most common clinical manifestation, and acute urinary retention was observed in 6 patients. All patients recovered completely within a month.
Conclusion
Adult-onset MERS is an entity with a broad clinico-radiological spectrum because of the various diseases and conditions. There are similar characteristics between MERS in adults and children, also some differences
Trial registration number
N/A
AS32-0027
THE CLINICAL CHARACTERISTICS OF ACUTE CEREBROVASCULAR ACCIDENTS RESULTING FROM OVARIAN HYPERSTIMULATION SYNDROME
1Beijing Chaoyang Hospital- Capital Medical University-, Department of Neurology- Beijing Chaoyang Hospital- Capital Medical University-, beijing, China
Background and Aims
Ovarian hyperstimulation syndrome (OHSS) is a serious complication that occurs after the ovarian-induction treatment. Acute cerebrovascular accident is one of the most dangerous manifestations of the syndrome. However, the characteristics of stroke resulting from OHSS have so far not been well summarised in any study.
Method
We reported 2 cases of acute cerebrovascular accidents secondary to OHSS. And then we performed a literature search for reports on this type of stroke, and summarised their characteristics
Results
Thirty-six published cases of this type of stroke were reviewed. Thirty two out of 36 (88.9%) of the women were 35 years old or younger. Stroke in 28 out of 36 (77.8%) of these cases was caused by arterial thrombosis. In 17 out of 28 cases, the involved cerebral vascular branches were mainly middle cerebral artery (MCA) and internal carotid artery (ICA). The acute cerebrovascular accidents happened 7 and 9.25 days after embryo transplantation or 8 and 8.33 days after last human chorionic gonadotropin treatment respectively. The prognosis of patients was relatively good after anticoagulation and some supportive treatments.
Conclusion
The MCA and ICA are easily involved in stroke resulting from OHSS. The young age may be a risk factor for developing stroke secondary to OHSS. Once thromboembolism develops, administering appropriate therapy is crucial.
Trial registration number
N/A
-0025
TRETAMENT WITH ANGIOTENSIN II RECEPTOR BLOCKERS IMPROVES LANGUAGE RECOVERY AFTER ISCHEMIC STROKE: A PILOT STUDY
1JOrdan UNiversity of Science and Technology, Clinical Pharmacy/Faculty of Pharmacy, Irbid, Jordan
2JOrdan UNiversity of Science and Technology, Rehabilitation Sciences/Applied Medical Sciences, Irbid, Jordan
3JOrdan UNiversity of Science and Technology, Faculty of Medicine, Irbid, Jordan
Background and Aims
Speech recovery is one of the commonly overlooked parameters that have a significant impact on patient’s quality of life, which ultimately affects recovery and functioning after stroke. Unfortunately, there is a lack of data on the effectiveness of available pharmacologic interventions on speech recovery after stroke. The aim of this pilot study is to assess the effect of regularly prescribed secondary prevention drugs on speech recovery after stroke.
Method
Stroke patients referring to the speech rehabilitation clinic at King Abdullah University Hospital (KAUH) were recruited into the study after getting their informed consent. Patient's baseline language and speech in addition to their current medications were documented. Patients received speech and language rehabilitation and their recovery were evaluated.
Results
Forty patients were included in this pilot study. The median age of the participants was 62 years (33-73). Rehabilitation improved language recovery by about one fold (p < 0.001).
Treatment with ARBs enhanced the beneficial effect of language rehabilitation (38 vs.48; p < 0.01). None of the comorbid conditions or other commonly used drugs altered the beneficial effect of rehabilitation on language recovery.
Conclusion
Treatment with ARBs enhanced the prorecovery effect of language rehabilitation. Comorbid conditions did not alter the response to language rehabilitation therapy.
Trial registration number
N/A
AS32-0025
THE SIGNIFICANT EFFECTS OF CEREBRAL MICROBLEEDS ON COGNITIVE DYSFUNCTION: AN UPDATED META-ANALYSIS
1Beijing Chaoyang Hospital- Capital Medical University-, Department of Neurology- Beijing Chaoyang Hospital- Capital Medical University-, beijing, China
Background and Aims
Accumulated data suggests that cerebral microbleeds (CMBs) play an important role in the decline of cognitive function, but the results remain inconsistent. In the current study, we aimed to investigate the association between CMBs and cognitive function, as well as the various effects of CMBs on different domains of cognition.
Method
We searched through the databases of PubMed, Embase, Cochrane Library, and ScienceDirect. After a consistency test, the publication bias was evaluated and a sensitivity analysis was performed with combined odds ratios (OR) and standardized mean difference (SMD) of CMBs.
Results
A meta-analysis of 25 studies with 9343 participants total was conducted. Patients with CMBs had higher incidence of cognitive impairment (OR:3.5410; 95% confidence interval [CI] [2.2979, 5.4567], p < 0.05) and lower scores of cognitive functions (SMD: −0.2700 [-0.4267, −0.1133], p < 0.05 in Mini-Mental State Examination [MMSE] group and −0.4869 [−0.8902, −0.0818], p < 0.05 in Montreal Cognitive Assessment [MoCA] group). Our results also indicated that patients with CMBs had obvious decline in cognitive functions, for instance, orientation (SMD: −0.9565 [−1.7260, −0.1869], p < 0.05), attention and calculation (SMD: −1.1518 [−1.9553, −0.3484], p < 0.05) and delayed recall (SMD: −0.5527 [−1.1043, −0.0011], p = 0.05).
Conclusion
Our data suggested that CMBs might be an important risk factor for cognitive dysfunction, especially in the domains of orientation, attention and calculation and delayed recall functions. Prospective cohort studies with further investigations will be needed in larger samples.
Trial registration number
N/A
AS32-0006
ROSUVASTATIN PRESERVES BLOOD–BRAIN BARRIER INTEGRITY AND RESCUES HEMORRHAGE TRANSFORMATION CAUSED BY TISSUE PLASMINOGEN ACTIVATOR THERAPY IN MICE AFTER STROKE
1Jinan university, neurology, Guangzhou, China
Background and Aims
The SPARCLE trail showed intensive statin has proved to efficacious in preventing primary stroke risks, without any significant risk of ICH. The purpose of this study is therefore to investigate whether pretreated rosuvastatin prevents hemorrhagic transformation induced by rt-PA in a mouse model of focal ischemia/reperfusion.
Method
After intraperitoneal injected with normal or intensive rosuvastatin treatment, adult BALB/c-mice were subjected to MCAO/R. The neurological deficits, mortality, infarct volume, and HT status were assessed at 24 h with or without rtPA intravenously administered prior to reperfusion after MCAO 3h and 6h. Hemoglobin were respectively used for qualitative and quantitative detection of the hemorrhagic contents. The integrity of the blood brain barrier (BBB) were evaluated. Furthermore, molecualr docking analysis were performed to predict the interaction between BBB receptors and Rosuvastatin. Cerebral blood flow (CBF) was monitored prior to reperfusion and in the 24 hour period post reperfusion.
Results
The ischemia 3 h and 6 h mice showed apparent HT after 24 h reperfusion followed by rt-PA and filament withdrawal. Even though mortality rate was not significantly reduced, pretreatment of normal and intensive rosuvastatin ameliorated rt-PA-associated HT via preserved the integrity of the BBB and abundant of tight junction (TJ) proteins after cerebral ischemia through the PDGFR-α/MMP2 and LRP1/MMP3/MMP9 pathway. In contrast, rosuvastatin therapy significantly reduced HT with no apparently suppressed CBF recoverment.
Conclusion
Pretreated rosuvastatin possess protective properties against rt-PA-associated hemorrhagic transformation via maintenance of BBB integrity, reduce activity of tPA-PDGFR-α/MMP2 and tPA-LRP1/MMP3/MMP9 pathway, without impairing cerebral blood reflow.
Trial registration number
N/A
AS32-0011
CHRONIC KIDNEY DISEASE INCREASES STROKE CASES; WHERE IS THE HEPCIDIN ROLE?
1Medical University Sofia, Dept. of Clinical Laboratory and Clinical Immunology, Sofia, Bulgaria
2Medical University Sofia, Dept. of Medical Genetics, Sofia, Bulgaria
3Medical University Sofia, Department of Neurology, Sofia, Bulgaria
4NCIPD Sofia, Dept. of Immunology, Sofia, Bulgaria
5R.E.D. Laboratories N.V./S.A., R.E.D. Laboratories N.V./S.A., Zellik, Belgium
6University Aleksandrovska hospital Sofia, Clinical laboratory and clinical pharmacology, Sofia, Bulgaria
7Medical University Sofia, Department of Nephrology, Sofia, Bulgaria
8Medical University, National cardiology hospital Sofia, Sofia, Bulgaria
9Medical University, Department of Neurology, Sofia, Bulgaria
Background and Aims
Impairment of brain cognitive function is an early sign of atherosclerosis development. Chronic kidney disease (CKD) involves high number of population worldwide, which on its way increases brain-vascular diseases risk. Among the main reasons for increased stroke evidence in patients with CKD is iron homeostasis dysregulation.
Method
We included 41 patients with chronic kidney disease (stages II to IV) diagnosed at “Aleksandrovska” hospital, Clinics of Nephrology and Neurology; average age 50.1 ± 7.7. Their results were compared to age and sex matched healthy control patients with CKD and no atherosclerotic evidences. CBC, serum iron, ferritin, hsCRP, hepcidin were measured in the included groups. IMT was measured by electronic calipers and evaluated by automated software programs. MMSE, CERAD, A (TMT-A), B (TMT-B) test were used for cognitive function evaluation.
Results
We found increased serum hepcidin concentrations in CKD patients with atherosclerotic IMT changes (194.3 ± 11.9 μg/L) compared to control group (101.7 ± 9.4 μg/L); P < 0.001. A positive correlation was found in CKD patients with stroke between IMT and serum hepcidin levels (r = 0.699, P < 0.005). In patients with impaired kidney function cognitive dysfunction correlates to serum hepcidin positively (r = 0.798, P < 0.001).
Conclusion
Chronic kidney disease is connected to brain-vascular disease risk factors. Iron homeostasis disturbances are one of the main risk factors in atherogenesis. Early evaluation of hepcidin and cognitive disturbances as an atherosclerosis symptoms in chronic kidney disease patients is very important for clinical practice.
Trial registration number
Д-235/2017
AS32-0022
PROTECTIVE EFFECTS OF ACTIVATED PROTEIN C ANALOG IN A MURINE MODEL OF WHITE MATTER STROKE
1Zilkha Neurogenetic Insitute, Keck School of Medicine – University of Southern California, Los Angeles- CA, USA
2Dept. Molecular Medicine, The Scripps Research Institute, La Jolla- CA, USA
3Institute for Stroke and Dementia Research, Klinikum der Universität München- Ludwig-Maximilians-Universität- LMU, Munich, Germany
Background and Aims
Subcortical white matter stroke constitutes up to 30% of all stroke subtypes, occurs initially as silent infarcts in the white matter (WM), and contributes significantly to the development of vascular dementia. Activated protein C (APC) is a plasma serine protease that is capable of antithrombotic, anti-inflammatory, anti-apoptotic, and cell-signaling activities. 3K3A-APC, a recombinant variant of APC with reduced (>90%) anticoagulant activity, engineered to reduce APC-associated bleeding risk while retaining normal cell-signaling activity, has shown benefits in preclinical models of ischemic stroke with large infarcts involving large brain arteries and gray matter. A multicenter Phase 2 randomized clinical trial has enrolled 110 patients to assess the safety, pharmacokinetics, and efficacy of human recombinant 3K3A-APC in acute ischemic stroke patients following endovascular thrombolysis (NCT02222714). The aim of this study was to investigate the effect of 3K3A-APC on white matter stroke
Method
In the current study, a subcortical WM stroke model was induced by vasoconstrictor N5-(1-iminoethyl)-L-ornithine, dihydrochloride (L-Nio). L-Nio (Calbiochem) was injected into subcortical WM of the anterior cingulum (AC) of the corticolimbic circuit or the subcortical white matter ventral to the mouse forelimb motor cortex. Mice received 0.2 mg/kg intravenously of recombinant murine 3K3A-APC or saline at 4, 24, 48 and 72 h after stroke.
Results
The results indicate that 3K3A-APC significantly reduces infarct volume, protects blood brain barrier damage 3 days after stroke, and improves remote memory function 4 weeks after stroke, compared to vehicle.
Conclusion
These results demonstrate that 3K3A-APC might be an effective treatment for white matter stroke.
Trial registration number
N/A
AS32-0038
EVALUATION OF PREVELANCE OF ASPIRIN RESISTANCE IN PATIENTS WITH ISCHEMIC STROKE BY LIGTH TRANSMISSION AGGREGOMETRY
1Tehran University of Medical Sciences, Neurology Department- Iranian center of Neurological Research- Imam-Khomeini Hospital- Tehran- IRAN, tehran, Iran
2Mehr Labratory- No 39- MOGHADAS ARDABILI, Biochemistry, Tehran, Iran
3Mehr labratory. Moghadas ardabili- Tehran, Biochemistry, Tehran, Iran
4Tehran University of Medical Sciences, Acadamic Deputy, tehran, Iran
5Laleh Hospital- Tehran, Neurosurgery Departement, Tehran, Iran
6Tehran University of Medical Sciences, Neurology Department- Imam-Khomeini Hospital- Tehran- IRAN, tehran, Iran
Background and Aims
Aspirin is integral in the primary and secondary prevention of ischemic stroke. Moreover, ASA effectiveness is limited because 10–20% of patients with arterial thrombosis may develop recurrent vascular events while on ASA treatment.
Inadequate (poor) response to therapeutic doses based on laboratory tests; aggregation more than 70 %: has been referred to as aspirin resistance (1).
The Aim of this study was to evaluate the prevalence of Aspirin Resistance in ischemic stroke patients, visited in Tehran University of Medical Science affiliated hospital stroke Clinic from July 2016 to December 2017.
Method
In case series study, we evaluated Aspirin resistance in 142 patients with history of Ischemic stroke and consumption of Aspirin 80 mg for at least one week, in Tehran University affiliated hospital stroke clinic.
ASA Resistance is evaluated by adding Adenosin to Plasma Riched Platlate (PRP) and assayed by Light Transmission Aggregometry (LTA) with Chronolog Aggregometer Analyzer.
Results
The range of Aspirin aggregation in this study was from < 1.6% to 37% of the subjects tested,that was less than 70%,value accepted for ASA Resistance.
Patients who had Long time consumption of ASA, concomitant use of Aspirin with Metformin and Statin had low platlate aggrgationton.
Conclusion
Our study does not showed significant Resistance to Aspirin in patients who used aspirin as secondary prevention for ischemic stroke. These Data is tin accordance to results published by. Maree t (2), and Grinstein (3), who reported wide range of aspirin resistance between 1-% to 60% and 2–50% respectively.
Trial registration number
this study had a Grant from research Deputy oF Neuroscience Institute of Tehran University of Medical Sciences (95-04-54-33262)
AS32-0039
LATERALIZATION OF INSULAR INFARCTS IS NOT ASSOCIATED WITH LONG-TERM OUTCOMES
1National and Kapodestrian University of Athens, 1st Department of Neurology- Eginition Hospital, Athens, Greece
2Hellenic Cardiovascular Research Society, Stroke Division, Athens, Greece
3Mediterraneo Hospital, Department of Neurology, Athens, Greece
4National and Kapodestrian University of Athens, Department of Clinical Therapeutics, Athens, Greece
5University of Thessaly, Department of Medicine, Larissa, Greece
Background and Aims
Ischemic strokes (IS) involving the insular cortex have higher odds of unfavorable outcome. There is inconsistency whether the right or left insula is most associated with poor prognosis. The aim of our study was to investigate the association of insular infarct lateralization with long-term outcome in a large population of prospectively collected patients with first-ever IS.
Method
Dataset was derived from the Athens Stroke Registry. All cerebral infarctions involving the insular cortex or at least a portion of the insula were classified as insular. Cox-regression analysis was performed to investigate whether insular lateralization was a predictor for long-term outcomes.
Results
The study population consisted of 1212 patients (48% women, mean age: 72 years) with insular involvement visualized on brain imaging (46% with right insular stroke). At 5 years of follow-up, there were no significant differences in the rate of stroke recurrence (4.3% vs. 4.9%%, p = 0.68), new cardiovascular events including severe arrhythmias (4.3% vs. 6.2%, p = 0.16), mortality (adjusted OR 0.92, 95%CI 0.80-1.06) and death or dependency (adjusted OR 0.99, 95%CI 0.76-1.29) between right and left insular strokes, respectively.
Conclusion
Right and left insular lesions have similar long term outcomes in patients with first-ever IS.
Trial registration number
N/A
AS32-0040
CAROTID-FEMORAL PULSE WAVE VELOCITY IS ASSOCIATED WITH LATE OUTCOME IN ISCHEMIC STROKE PATIENTS
1Medical University of Gdansk, Department of Adult Neurology, Gdansk, Poland
2Medical University of Gdansk, Department of Hypertension and Diabetology, Gdansk, Poland
Background and Aims
Carotid-femoral pulse wave velocity (cf-PWV) is a surrogate measure of aortic stiffness and predictor of cardiovascular morbidity and mortality. Previously, we demonstrated the significance of cf-PWV as a dichotomous variable in predicting late outcome after ischemic stroke based on a 99-subject group analysis. In this study, we assessed the association between cf-PWV as a continuous variable and late outcome in a nearly doubled group of patients.
Method
We recruited 174 subjects admitted to the Department of Adult Neurology, Medical University of Gdańsk, Poland, within 24 hours from the ischemic stroke. In the final analysis, we used the following data: National Institutes of Health stroke scale (NIHSS) score evaluated on day 1; cf-PWV and blood pressure, on day 7; and modified Rankin scale (mRS) score, 3 months after stroke. mRS of 0 or 1 was defined as a favourable late outcome. cf-PWV (as a continuous variable) was compared between favourable and unfavourable outcome groups. The multivariate logistic regression analysis of the data included the possible main confounders.
Results
The median age was 63.1 (interquartile range [IQR], 56.6-70.1); median NIHSS, 6.5 (IQR, 3–8). In univariate analysis, cf-PWV was significantly lower in the favourable outcome group (9.8 vs. 11.0m/s, p = 0.01). In multivariate logistic regression, after adjustment for age, sex, mean blood pressure, NIHSS, and tissue plasminogen activator administration (tPA), cf-PWV remained significantly lower in the same group (odds ratio [OR], 0.85; 95% confidence interval [CI], 0.72-0.99; p = 0.04).
Conclusion
cf-PWV is associated with late outcome after ischemic stroke independently of MBP, NIHSS, age, sex, and tPA.
Trial registration number
N/A
AS32-0007
IS CAROTID STIFFNESS A POSSIBLE SURROGATE FOR STROKE IN LONG-TERM SURVIVORS OF CHILDHOOD CANCER AFTER NECK RADIOTHERAPY?
1University Clinical centre, Department of Vascular Neurology, Ljubljana, Slovenia
2Institute of Oncology, Radiotherapy Department, Ljubjana, Slovenia
Background and Aims
The risk for cerebrovascular late effects among childhood cancer survivors is considerable. According to recent studies it is not clear which marker could be reliable for the screening of cerebrovascular diseases among the long-term survivors of childhood cancer. The purpose of this study is to analyse arterial stiffness and intima media thickness as possible early markers of later occurring stroke.
Method
Twenty-three patients, treated for HD in childhood, were included. They had received radiation therapy to the neck with 20- 65 (med.30) Gy. Twenty-six healthy controls, matched in age, sex, BMI, arterial hypertension, smoking history and total cholesterol levels were compared. High-resolution colour-coded duplex sonography and power Doppler sonography of the carotid arteries were performed and intima –media thickness, number and quality of plaques were measured. Arterial stiffness indices were calculated.
Results
Plaque deposits and/or arterial wall calcinations were found in 24 out of 43 (55.8 %) vessels in cancer survivors group and 0 out of 52 vessels in the group of healthy controls (p < 0.01). We found significant group differences for all the stiffness parameters we used (P < 0.05), but there was no difference in intima–media thickness between cases and controls (p = 0.92). In a multivariate model, carotid pulse wave velocity was positively associated with smoking.
Conclusion
The arterial stiffness has appeared as a possible surrogate marker for stroke in long-term survivors of childhood cancer. Smoking habit might have an additional negative influence on vascular aging in the group of patients after neck radiotherapy.
Trial registration number
N/A
AS32-0010
THE EFFECTS OF COMPUTER BASED COGNITIVE REHABILITATION IN PATIENTS WITH VISUOSPATIAL NEGLECT FOLLOWING STROKE, BRAIN TUMOR, BRAIN INJURY OR OPERATION SEQUELAE: A SYSTEMATIC REVIEW
1Bispebjerg Hospital, Department of Neurology, roedovre, Denmark
2Bispebjerg Hospital, Department of Neurology, Copenhagen, Denmark
3University of Copenhagen, Department of Psychology, Copenhagen, Denmark
4Bispebjerg Hospital, Department og Neurology, Copenhagen, Denmark
Background and Aims
Objectives
To identify and evaluate existing literature concerning the effects of computer based cognitive rehabilitation (CBCR) on visuospatial neglect after four types of acquired brain injury.
Method
Databases Medline, EMBASE, PsycINFO, and CINAHL were searched with search strings developed for this review. Authors of relevant literature were contacted to detect supplementary unpublished data or articles not found by searching databases.
Results
No studies were identified that investigated the effects of CBCR in the rehabilitation of visuospatial neglect after acquired brain injury compared to a control group in a randomized, controlled setting.
Conclusion
Based on existing literature, it is not possible to conclude on the effects of CBCR in the rehabilitation of visuospatial neglect after acquired brain injury. Future studies need to be controlled and properly randomized, and compare CBCR to both passive and active control groups to clarify its effectiveness.
Trial registration number
N/A
AS32-0036
INFLUENCE OF ION-REFLEX PULSED MAGNETOELECTROPHORESIS EGB 761® ON THE BIOELECTRICAL ACTIVITY OF THE BRAIN OF PATIENTS WITH ISCHEMIC STROKE.
1Kazakh National Medical University, Department of Nervous Diseases №1, Almaty, Kazakhstan
2City Clinical Hospital № 1, Department of Neurorehabilitation, Almaty, Kazakhstan
3Kazakh National Medical University, Department of Nervous Diseases №2, Almaty, Kazakhstan
Background and Aims
In recent years more and more attention of researchers attracted neurostimulator effect of pulsed magnetic fields, such as transcranial magnetic stimulation. There is information about the increase of the functional activity of clock mechanisms of the brain under the influence of short-term local alternating magnetic field.
Method
There was study of bioelectrical activity of the cerebral cortex of 35 patients with IS in the early recovery period, aged 26 to 76 years with the help of electroencephalography recording. The study was carried out three times: before, after the first magnetic electrophoresis session, third record – at the end of 5 sessions.
Results
In the dynamics of treatment, signs of regression of disorganization of brain bioelectric activity in the form of a redistribution of frequency components toward the alpha-rhythm (35.7%) are noted with a decrease in slow-wave activity (delta up to 15.8%, theta to 24.2%).
Positive shifts in the delta range (mainly in the fronto-temporal lobes) have been noted as a decrease in the coherence coefficient (F3-F4 from 0.45 to 0.39, T5-T6 −0.43 to 0.37).
Patients noted improvement in general well-being, improvement of memory, attention, and synchronization of circadian rhythms of sleep.
Conclusion
The study showed a positive effect of ion-reflex impulse magnetic electrophoresis on the functional state of the brain, more successful neurorehabilitation of patients with IS in the early recovery period.
Trial registration number
N/A
AS32-0045
THERAPEUTIC CLOWNING IN NEUROLOGICAL INPATIENT REHABILITATION
1Humboldt University, Psychology, Berlin, Germany
2Brandenburgklinik, Neurology, Berlin, Germany
3Klinikum Ernst von Bergmann, Neurology, Potsdam, Germany
Background and Aims
Therapeutic clowning by trained professionals may enhance the effects of neurological rehabilitation. This pilot study examined the effects of therapeutic clowning on inpatients in a neurological rehabilitation hospital.
Method
Patients of two inpatient wards (n = 99) were consecutively recruited for the either the intervention group or the control group. Using a crossover design, allocation of patients to one of the groups switched during the recruitment period. The intervention group received two clown visits by trained clinic clowns per week, a minimum of three visits in total. Humour, actual mood, and well-being were assessed before the first visit, at discharge from the clinic, and followed up 6 months later. Additionally, the Resource Utilization Questionnaire was applied at follow-up to record the participant’s health care resources such as doctor’s visits, physiotherapy, psychotherapy.
Results
The results show that patients in the intervention group scored higher in cheerfulness on the State Trait Humour Inventory, and showed less utilisation of health care resources at follow-up.
Conclusion
This pilot study provided first evidence for proximal as well as distal beneficial effects of therapeutic clowning on rehabilitation. The results should be followed up by further randomized controlled studies.
Trial registration number
N/A, Pilot study
AS32-0018
AN ANALYSIS OF CAPILLARY BLOOD GLUCOSE LEVELS IN HOSPITALIZED PATIENTS WITH STROKE
1Institute of Cardiovascular and Medical Sciences, Stroke Medicine, Glasgow, United Kingdom
2NHS Greater Glasgow and Clyde, Department of Diabetes, Glasgow, United Kingdom
3Institute of Cardiovascular and Medical Sciences, Clinical pharmacology, Glasgow, United Kingdom
Background and Aims
People with acute stroke and diabetes mellitus may have episodes of hypoglycaemia (capillary blood glucose (CBG) < 4mmol/l) and hyperglycaemia (CBG > 15 mmol/l). Capillary blood glucose (CBG) levels may also vary within these more extreme ranges. We aimed to examine the relationship between episodes of hypoglycaemia, hyperglycaemia and variability in CBG (CBGv) with outcome in hospitalised patients with diabetes and acute stroke.
Method
We used routinely available clinical data from Scottish National Health Service records and from the Scottish Stroke Care Audit. All CBG measurements during a verified stroke admission were identified and episodes of hypoglycaemia and hyperglycaemia identified. CBGv was defined as the interquartile range (IQR) of all recorded CBG readings during the admission. We extracted outcome date for death, readmission to the hospital, and discharge destination and assessed the relationship with CBG measures using Cox-proportional hazards models and logistic regression.
Results
We included 3551 patients. Hypoglycaemia, hyperglycaemia and CBGv were associated with increased risk of death (HR = 1.3;1.05–1.6, HR = 2.06;1.7-2.5, HR = 1.13;1.09-1.17 respectively). Hypoglycaemia was associated with lower rate of readmission (HR = 0.85;0.70-0.10, p0.04) and CBGv with an increase (HR = 1.04,1.01-1.07, p < 0.001). The number of hypoglycaemic episodes (≥4) was associated with discharge to a destination other than (OR 2.25;1.45-3.5, p < 0.001).
Conclusion
Outcomes were worse in patients with stroke and diabetes who had episodes of hypoglycaemia, hyperglycaemia and greater CBGv. Close monitoring of blood glucose levels is needed along with strategies to minimise the number of episodes of hypoglycaemia and variability of blood glucose levels.
Trial registration number
N/A
AS32-0043
INSULIN RESISTANCE AND DYSLIPIDAEMIA ARE STRONGLY ASSOCIATED WITH ISCHAEMIC STROKE AND ASYMPTOMATIC CAROTID ARTERY STENOSIS IN NON-DIABETICS
1Special hospital for cerebrovascular diseases “St. Sava”- Belgrade, Stroke unit, Belgrade, Serbia
2Neurology Clinic- Clinical Centre of Serbia- Belgrade, Neurosonology Unit, Belgrade, Serbia
3Clinic for Endocrinology and metabolism- Clinical Center of Serbia- Belgrade, Department for diabetes, Belgrade, Serbia
Background and Aims
Decreased insulin sensitivity (IS) with compensatory hyperinsulinemia plays a crucial role in the pathogenesis of atherosclerosis, but their role in ischemic stroke (IST) has not yet been elucidated. This study was aimed to analyze IS as the indicator of atherosclerotic activity, as well as plasma insulin (PI) levels and dyslipidemia pattern in 100 patients with atherothrombotic IST confirmed on brain computerized tomography/magnetic resonance imaging- (group A), 100 patients with asymptomatic stenosis of one or both internal carotid arteries < 50%- (group B), and 50 healthy controls-(group C) Patients with diabetes mellitus and ischemic heart disease were excluded from the study.
Method
IS was determined by Homeostasis Assessment Model (HOMA-IR), PI levels were determined by Radioimunoassay. We measured total cholesterol, LDL and HDL cholesterol and trygliceride levels in all groups.
Results
IS was significantly lower in group A compared to group B and C (4.82+/−0.27 vs. 2.89+/−0.22, p < 0.05; 4.82+/−0.27 vs. 1.41+/−0.22, p < 0.001). PI levels were significantly higher in group A in comparison to group B and C (19.00+/−1.2 vs. 13.95+/−0.88, p < 0.05; 19.00+/−1.2 vs. 7.12+/−0.19, p < 0.01). Different patterns of dyslipidemia were observed in ACAS in comparison to IST.
Conclusion
Our results indicate that atherothrombotic IST as well as ACAS are strongly associated with decreased IS and increased PI levels, although all the patients were non diabetics. Also, different patterns of dyslipidemia between ACAS and IST were observed.
Trial registration number
N/A
AS32-0031
THE USE OF THE GEKO DEVICE AND THE ACTIVATION OF THE FOOT AND CALF PUMPS FOR PREVENTION OF VENOUS THROMBOEMBOLISM IN PATIENTS WITH ACUTE STROKE
1University Hospital of North Midland NHS Trust, Acute Stroke Unit, Stoke on Trent, United Kingdom
2Undergraduate School of Medicene- Keele University, na, Stoke on Trent, United Kingdom
Background and Aims
Venous Thrombo Embolism (VTE) prophylaxis using Intermittient Pneumatic Compression device (IPC) is not possible in all stroke patients, we changed our pathway to include the Neuromuscular Electrical Stimumaltion (geko™) device as an alternative for patients with acute stroke who had contradictions/not tolerate IPC. The aim of this audit was to assess the acceptability of this new practice for patients and staff and its impact on VTE.
Method
The audit included 455 patients admitted to the Acute Stroke Unit at Royal Stoke University Hospital RSUH)
All stroke patients who are immobile are given VTE prophylaxis, unless they are paliated, refusing the intervention, or fully anticoagulated. Every patient is reviewed daily on a nurse-led VTE ward round to monitor compliance with VTE prophylaxis.
Results
In total 6/455 (1.3%) patients developed symptomatic VTE (3 DVTs and 3 PEs) within 90 days. Of these, 4 patients (1.6%) were prescribed IPC, 1 patient (1.3%) was prescribed the geko™ device as a secondary intervention and 1 patient (1.5%) patient was prescribed anticoagulation. There was no DVT or PE in patients treated with the geko™ device as the primary VTE prophylaxis.
Conclusion
This audit shows a low incidence 1.3% of symptomatic VTE in a high risk population of all immobile stroke patients during the audit period. 36% had contraindications to or did not tolerate IPC. The number of patients treated with geko™ in this project was 35.6%, but, while limited, our data suggests that the geko™ device may be as effective as IPC in our patient cohort
Trial registration number
N/A
AS32-0023
STROKE DIAGNOSIS USING HINTS IN PATIENTS PRESENTING WITH ACUTE VESTIBULAR SYNDROME: A SYSTEMATIC REVIEW
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
2Nottingham University Hospitals NHS Trust, Stroke, Nottingham, United Kingdom
3Oslo University Hospital, Dept. of Neurology, Oslo, Norway
4Oslo University Hospital, Dept. of Geriatrics, Oslo, Norway
Background and Aims
Patients with posterior circulation stroke presenting with acute vestibular syndrome (AVS- vertigo, nausea/vomiting and gait unsteadiness) often have minimal clinical signs at the time of presentation. NIHSS is not reliable and CT scans cannot exclude acute posterior circulation ischaemia. A positive HINTS test with any of three signs: normal horizontal head impulse, direction changing nystagmus, and skew deviation of the eyes is suggestive of central cause including acute stroke. This systematic review examined the effectiveness of abnormal HINTS in posterior circulation stroke in patients presenting with AVS.
Method
We searched MEDLINE (1966 to 21 December 2017), EMBASE (1980 to December 2017), Web of Science and scanned bibliographies of relevant articles to identify studies on clinical features and diagnostic evaluation. We included studies in which HINTS was done primarily to identify posterior circulation stroke with diagnosis (infarct or haemorrhage) confirmed using magnetic resonance imaging (MRI).
Results
Six studies (644 patients) with AVS were identified. Two studies had patients with ABCD2 score of 4 and one study examined the relationship between truncal ataxia and posterior circulation stroke. Acute stroke was confirmed in 218 patients (29.8%). There was a 11-fold increased risk in posterior circulation stroke in those patients with a positive HINTS test compared to those with no abnormality (O.R. 11.50, 95% CI 3.50-38.32).
Conclusion
HINTS test appears to differentiate posterior circulation stroke from peripheral causes in AVS. Since posterior circulation stroke has the same risk of poor outcome as those of anterior circulation, methods to use HINTS in emergency settings need further investigation.
Trial registration number
N/A