
Abstract
Introduction
Mechanical thrombectomy within 6 h after stroke onset improves the outcome in patients with large vessel occlusions. The aim of our study was to establish a model based on diffusion weighted and perfusion weighted imaging to provide an accurate prediction for the 6 h time-window in patients with unknown time of stroke onset.
Patients and methods
A predictive model was designed based on data from the DEFUSE 2 study and validated in a subgroup of patients with large vessel occlusions from the AXIS 2 trial.
Results
We constructed the model in 91 patients from DEFUSE 2. The following parameters were independently associated with <6 h time-window and included in the model: interquartile range and median relative diffusion weighted imaging, hypoperfusion intensity ratio, core volume and the interaction between median relative diffusion weighted imaging and hypoperfusion intensity ratio as predictors of the 6 h time-window. The area under the curve was 0.80 with a positive predictive value of 0.90 (95%CI 0.79–0.96). In the validation cohort (N = 90), the area under the curve was 0.73 (P for difference = 0.4) with a positive predictive value of 0.85 (95%CI 0.69–0.95).
Discussion
After validation in a larger independent dataset the model can be considered to select patients for endovascular treatment in whom stroke onset is unknown.
Conclusion
In patients with large vessel occlusion and unknown time of stroke onset an automated multivariate imaging model is able to select patients who are likely within the 6 h time-window.
Keywords
Introduction
In stroke patients with large vessel occlusions, mechanical thrombectomy has great therapeutic potential if the procedure can be initiated within 6 h after stroke onset.1–3 In a meta-analysis of individual patient data from five large randomised controlled trials of mechanical interventions in acute stroke, the beneficial effect of thrombectomy was even present up to 7.3 h after stroke onset. 4 In selected patients based on neuro-imaging characteristics, core-clinical or core-perfusion mismatch, this time-window can even be extended as has been shown in the DAWN trial and is being studied in DEFUSE 3. 5 In these trials patients with highly favourable imaging patterns have been selected to evaluate the effect of thrombectomy regardless of time after stroke onset. However, many patients admitted with unknown stroke onset may not qualify for these criteria. Knowing or estimating the stroke duration will therefore remain of clinical importance. A large proportion of acute stroke patients are severely impaired, with or without aphasia, when they are admitted to the hospital. This hampers the documentation of the exact stroke onset time, although stroke onset or last seen normal time can often be obtained by relatives or bystanders. Patients without documentation of onset time or wake-up stroke patients are ineligible for this interventional treatment according to current guideline recommendations. The visual diffusion weighted imaging (DWI)/fluid attenuated inversion recovery (FLAIR) mismatch has been proposed as a predictor of stroke onset for the 4.5 h time-interval of thrombolysis, 6 but the prediction of stroke onset within the 6 h time-window has been less robustly studied. On the other hand, penumbral imaging with DWI and perfusion weighted imaging (PWI) is widely used in clinical trials to guide acute reperfusion therapy7–9 and some evidence exists that stroke lesion age can also be predicted from DWI imaging alone.10,11 Thus, the aim of our study was to evaluate whether information from imaging sequences used with penumbral imaging allows for identification of patients within 6 h from symptom onset. To this end, we aimed to establish a model based on relative diffusion weighted imaging (rDWI) and PWI to provide a prediction for the 6 h time-window in patients with large vessel occlusions.
Material and methods
Study population
We performed a retrospective analysis of data from the DEFUSE 2 8 and AXIS 2 12 studies. We refer to the original publications for more details about these two clinical trials.8,12 The study was performed according to the principles of the declaration of Helsinki. For the original studies the local institutional review boards approved the conducted research. In short, DEFUSE 2 was a prospective cohort of ischaemic stroke patients (NIHSS > 4) with large vessel occlusions who received endovascular therapy and a baseline magnetic resonance imaging (MRI) scan within 12 h after stroke onset. 8 The AXIS 2 trial included patients within 9 h after stroke onset in whom MRI could be performed and who presented with ischaemic stroke in the anterior circulation with a National institute of health stroke scale (NIHSS) 6–22. 12 For this substudy we selected patients with large vessel occlusions (internal carotid artery (ICA), proximal and distal middle cerebral artery (M1 and M2)).
Patients were included when DWI and PWI data were of sufficient quality, analysis of the diffusion imaging revealed a core lesion and calculation of perfusion imaging could demonstrate a region with persistent hypoperfusion within the core (to exclude patients with complete reperfusion at time of imaging).
Image analysis
Images were processed with RAPID (iSchemaView, Menlo Park), automated software for diffusion and perfusion imaging analysis. 13 The most optimal perfusion parameters to predict tissue that is critically hypoperfused, is still under debate.14,15 Tmax, the time to the maximum of the residue function, is the parameter most frequently assessed in clinical trials.7–9 The difference between the area that has a Tmax > 6 s on perfusion imaging and the area with Apparent Diffusion Coefficient (ADC) values under the threshold of 620 × 10−6 mm2/s on diffusion imaging, is currently considered as an operational definition of the tissue at risk and thus the mismatch.16,17 Hence, Tmax maps were calculated to determine the region of hypoperfusion. The area of critically hypoperfused tissue was segmented based on a threshold of Tmax > 6 s. 16 Co-registration of DWI and PWI was automatically done by RAPID software.
rDWI signal intensity maps (on the B1000 sequence) were calculated in a voxel-based manner as described previously for relative fluid attenuated inversion recovery imaging (rFLAIR) signal intensities. 18 The midline was defined manually and brain masks were derived from RAPID software based on ADC thresholds. 13 For every voxel the rDWI signal intensity was determined as the ratio of the signal intensity in that voxel and the median signal intensity of a sphere with radius 15 mm around the homologue voxel in the contralateral hemisphere.
The ischaemic core was segmented by RAPID, based on an ADC threshold lower than 620 × 10−6 mm2/s.16,19 The non-reperfused core was defined as voxels belonging to the core region with persistent hypoperfusion (Tmax > 6 s). We delineated this region as the region of interest to measure the descriptive values (median and interquartile range (IQR)) of the rDWI signal intensities. We studied the association between time from stroke onset and rDWI signal intensity within this area: the non-reperfused core. In reperfused tissue we could not make any assumption on the duration of hypoperfusion hampering the analysis of the change of DWI signal intensity over time as a result of reduced cerebral perfusion. Hypoperfusion intensity ratios (HIR, as continuous variables) were also included in the prediction model, since previous research has shown that the HIR is a marker of collateral status as determined by Digital Subtraction Angiography (DSA). 20 The HIR is calculated by the ratio of Tmax > 10 s volume to the Tmax > 6 s volume. 20
In the DEFUSE 2 trial vessel occlusions were rated on DSA or magnetic resonance angiography (MRA) if DSA was lacking. In the AXIS 2 trial only MRA images were available for determining the site of the arterial occlusive lesion.
Figure 1 illustrates the described imaging modalities in a patient with a middle cerebral artery (MCA) occlusion.
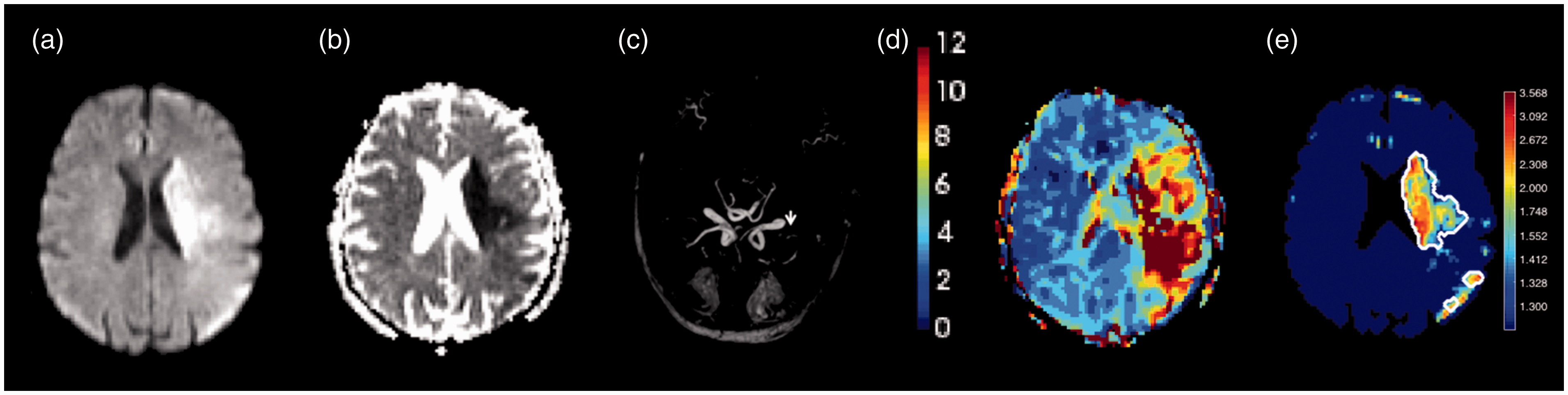
Overview of the different imaging sequences. Example of a patient with a left sided stroke in the area of the middle cerebral artery. (a) Diffusion weighted imaging (B1000). (b) Apparent diffusion coefficient. (c) Magnetic resonance angiography shows an occlusion of the left MCA (white arrow). (d) Tmax map. (e) rDWI map (white contour depicts area of non-reperfused core).
Statistical analysis
We designed the predictive model in the DEFUSE 2 dataset (derivation cohort) and performed a validation in the AXIS 2 data (validation cohort). A logistic regression model with the 6 h time-epoch as dependent variable was constructed. The model included age, HIR, core volume (ml), Tmax > 6 s volume (ml), parameters of rDWI (median and IQR) and the interaction terms of HIR with median rDWI and IQR rDWI (since the data were not normally distributed), as explanatory variables. We performed backward logistic regression to select significant explanatory variables. This model is based on the Akaike information criterion (AIC) to provide a balance between the goodness of fit of the model and the number of parameters required. Receiver operating characteristic (ROC) curves were calculated with Youden index to define the optimal threshold. The ROCs were compared with the Delong’s test for non-correlated ROC curves. 21
In a second approach the two cohorts were merged. A predictive model was constructed with the similar backward logistic regression. Since a validation cohort was lacking we internally validated the second model with the Leave-one-out cross validation (LOOCV). 22 Therefore we repeated the calculation of the coefficients of the logistic regression with leaving one patient out each time and determined the cross-validated predictive values.
In general, a Chi-square test was used to compare categorical data and a Mann–Whitney U test for continuous variables. P-values < 0.05 were considered significant. Statistical analysis was done with R (R Foundation for Statistical Computing, Vienna, Austria) and Matlab_R2012B.
Results
Patient characteristics
We included 91 patients from DEFUSE 2 and 90 patients from AXIS 2 in this study. Patients included in AXIS 2 had a larger core volume (41 ml vs. 26 ml) and presented at a later time-point after stroke onset (median 330 min vs. 270 min). Clinical characteristics of the two cohorts are shown in Table 1.
Clinical characteristics.
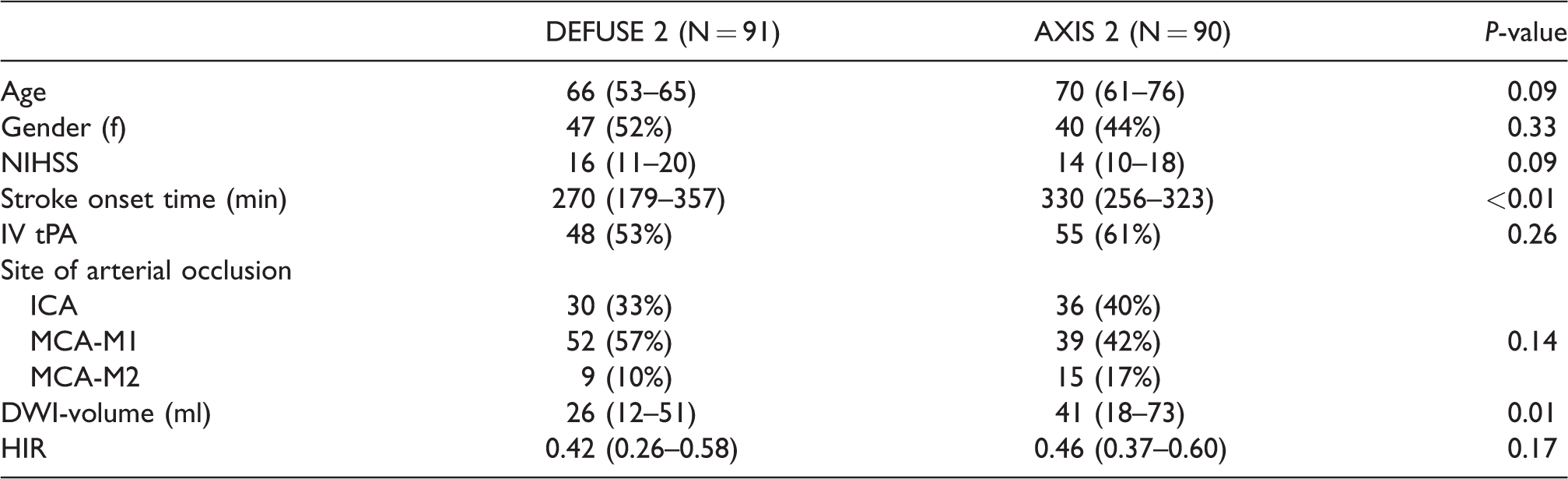
Data are median (IQR) or n (%).
NIHSS: National institute of health stroke scale; ICA: internal carotid artery; MCA: medial cerebral artery; DWI: diffusion weighted imaging; HIR: hypoperfusion intensity ratio; IQR: interquartile range.
Derivation cohort
The derivation cohort from DEFUSE 2 included 69 (76%) patients presenting within 6 h after stroke onset and 22 (24%) patients beyond this time-point. After selection of variables by backward logistic regression, the following explanatory variables were retained in the final model to predict stroke onset in the 6 h time-window: IQR and median rDWI, HIR, core volume (ml) and the interaction between median rDWI and HIR. Details of the model are presented in Supplementary Table 1. The area under the curve (AUC) of the corresponding ROC curve was 0.80 (95%CI 0.69–0.90; Figure 2). Youden index yielded 0.76 as the most optimal threshold. The predictive model classified 69 patients (76%) in the correct time-window (before vs. after 6 h) as shown in Table 2 with the other predictive values.
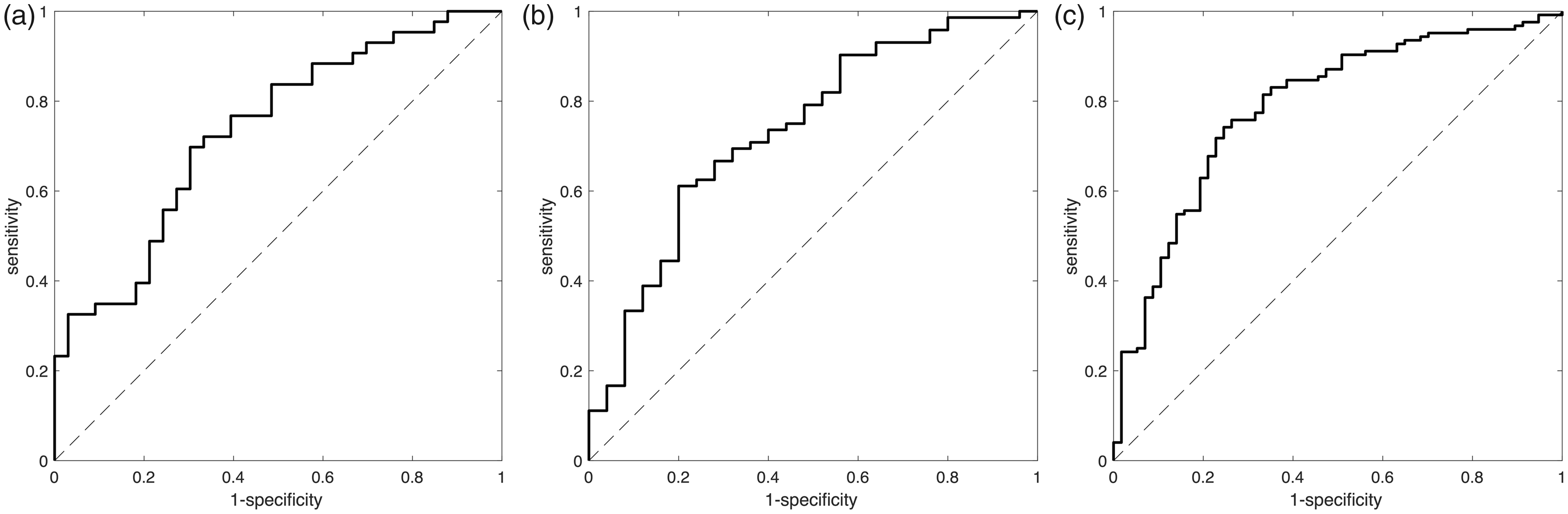
Receiver operating characteristics (ROC) analysis for the 6 h time-window. (a) Derivation cohort (N = 91, AUC = 0.80). (b) Validation cohort (N = 90, AUC = 0.73). (c) Total cohort (N = 181, AUC = 0.79).
Predictive values of the derivation and validation cohort.

PPV: positive predictive value; NPV: negative predictive value.
Validation cohort
In the validation cohort the distribution in the two time epochs was more even: 55 (61%) patients who presented within 6 h of symptom onset and 35 (39%) patients after 6 h. The predictive model designed in the derivation cohort yielded an AUC of 0.73 (95%CI 0.62–0.84; Figure 2). This AUC was not different from the AUC obtained in the derivation cohort (Delong’s test for two independent ROCs, P = 0.40). The accuracy of the model in correctly categorizing patients within or outside the 6 h time-window was 66% (Table 2).
Secondary analysis in the total cohort
In the previous analyses we validated the predictive model in an independent cohort of patients supporting our aim to establish a model based on DWI and PWI to provide an accurate prediction for the 6 h time-window. Since some heterogeneity existed when comparing the two cohorts, we decided to design a new model to redefine the most optimal threshold. Therefore we pooled all data to develop a model over a larger population aiming to improve the model for clinical implementation and increase the robustness. In the total cohort of 181 patients, 124 (69%) patients presented within the 6 h and 57 (31%) patients beyond 6 h of stroke onset. We constructed a model in which IQR and median rDWI, HIR, and the interaction term between median rDWI and HIR, were retained after backward logistic regression (Supplementary Table 2). This yielded an AUC of 0.79 (95%CI 0.72–0.86) with an optimal threshold of 0.69 (Figure 2). This model correctly categorised 134 patients (74%). After internal cross-validation the predictive value was confirmed with an AUC of 0.76 and accuracy of 70%. Predictive values are presented in Table 3.
Predictive values of the total cohort with the results of the leave-one-out cross-validation.

PPV: positive predictive value; NPV: negative predictive value; LOOCV: leave-one-out cross-validation.
Discussion
In patients presenting with an acute stroke caused by a large vessel occlusion, a multivariate automated imaging model can identify patients within the 6 h time-window with a moderate accuracy but high positive predictive value. Since a substantial subset of patients is admitted without known stroke onset a predictive model to identify patients within 6 h is of interest to increase the rate of patients who could benefit from endovascular therapy. The required imaging sequences and automated analysis are short in duration enabling fast therapeutic decisions and already part of evaluation for endovascular stroke treatment in many stroke centers. The derived model was validated in an independent cohort and both datasets contained multicenter imaging data underscoring the validity and application potential in clinical practice.
In both the derivation and validation cohort a good specificity was obtained, implying that only a limited amount of patients presenting outside the current time-window of 6 h for thrombectomy would be treated based on our model. This finding is reassuring since the predictive model should avoid selecting patients for a treatment which is not beneficial or could even be harmful. 23
The predictive model was designed based on data from DEFUSE 2, which was a prospective study in patients with large vessel occlusions who received endovascular therapy. To validate our results we selected similar patients from AXIS 2 in whom large vessel occlusions were documented on non-invasive neuroimaging. Both the median and IQR parameters of the rDWI maps were retained in the final model. Previously, relative DWI, both measures of dispersion and central value, has been shown to be associated with time from symptom onset in human and animal studies.10,11,24 These findings can be explained by the T2 signal inherent to the DWI images, which is similar to the FLAIR hyperintensity which is known to be correlated with time in the early time-window after stroke onset. 6 The association of the IQR rDWI with time from symptom onset could reflect the increase in heterogeneity during progression of the stroke lesion in the early phase after onset.
The additional explanatory value of collateral status as assessed by the continuous HIR and the interaction between the HIR and median rDWI may appear surprising. However, this effect, i.e. the modification of the relationship between the median rDWI intensity and time from symptom onset by collateral status, appears similar to the interaction between rFLAIR and HIR as we previously reported. 18
In the derivation cohort (DEFUSE 2) 76% of patients were correctly classified by the predictive model. In the validation cohort the accuracy dropped to 66% but did not differ from the accuracy in the derivation cohort. Nevertheless, we decided to study potential explanations (e.g. heterogeneity between the two cohorts) for this trend towards the reduced predictive value of the model. DEFUSE 2 was a trial which only enrolled patients with large vessel occlusions compared to AXIS 2 in which large vessel occlusion was not an inclusion criterion. For the purpose of this study we selected a subgroup of the AXIS 2 population with evidence of large vessel occlusion on MRA. Patients recruited in DEFUSE 2 presented earlier compared to patients in AXIS 2 since the distribution of patients in the time-window before vs. after 6 h was more skewed towards the later time-interval with only 24% of patients in the time-window beyond 6 h. Core volumes were smaller in DEFUSE 2 which might suggest that patient with large cores were less likely to be enrolled in DEFUSE 2 compared to AXIS 2. Since investigators in DEFUSE 2 were not blinded for the MRI results this selection bias could have occurred. To strengthen the prediction model for clinical implementation, we decided to pool the two cohorts and develop a new model in this larger cohort to increase the external validity with a more robust threshold. Visually this improved the ROC curve, which was reflected in a more balanced sensitivity and specificity (0.73 and 0.75 respectively). After internal cross-validation this accuracy was maintained.
Our study has certain limitations. First, ideally the sample size of the derivation cohort would have been larger increasing the power to identify predictive variables. To overcome this limitation we developed a second predictive model in the overall cohort of patients in which the same variables were retained. The model was internally validated, but external validation would have been superior.
Second, the model is designed based on an MRI approach, i.e. DWI and perfusion MRI, which might reduce its clinical application. Multimodal Computed Tomography (CT) imaging (e.g. by CT, CT angiography and CT perfusion) might be able to provide similar insight in tissue status, core and penumbral tissue, and could outperform MRI by terms of accessibility.17,25–27 However in many centers MRI is available for acute stroke patients and DWI still remains the most accurate imaging sequence to diagnose acute ischaemic stroke (with no correlate on CT imaging) and estimate the presence of irreversible ischaemic brain tissue. 28 CT perfusion is more easily available and characterised by shorter imaging time compared to MRI. However the imaging time and automated post-processing to select patients based on CT, CTA and CTP might not be so much shorter in duration compared to DWI, PWI and MRA. 27
Third, the model can only predict stroke onset within 6 h, but for selected patients this time-window might be too narrow. 4 In ESCAPE and REVASCAT patients were randomised beyond 6 h although the amount of patients in this later time-interval was limited.29,30
Fourth, the clinical relevance could be debated based on recent findings from the DAWN trial which provided evidence for patient selection based on core vs. clinical mismatch in the time-window up to 24 h (mostly patients with unknown time of stroke onset). However in this trial patients were selected based on small infarct cores and therefore a majority of patients with unknown stroke onset time, who might still benefit from endovascular therapy, will not fulfill these DAWN-criteria. Our model could be applied in clinical practice to identify patients with larger core lesion volumes when stroke onset is unknown, since the imaging pattern suggests an early presentation (and therefore a treatment effect can be expected). Next, the results of the DEFUSE 3 trial in which patients with a favourable mismatch profile presenting between 6 and 16 h of symptom onset were randomised to conservative vs. endovascular treatment will be of great interest. 5 Results of DAWN and DEFUSE 3 could provide information on the importance of imaging selection of patients in whom stroke onset time is unknown. Probably a combination of time and tissue status yields the best overall estimation for the expected benefit of endovascular therapy in individual patients. Therefore, we believe it is still worthwhile to be able to predict the time of onset regardless of the outcome of these trials. The predictive model constructed with information on DWI and PWI might provide a useful tool in selecting patients for endovascular therapy when stroke onset time is unknown.
Last, the accuracy to predict the 6 h time-window remained moderate which likely is a reflection of the heterogeneity in the evolution of the ischaemic stroke lesion in individual stroke patients.
To summarise, we have constructed an automated imaging model to identify stroke patients with large vessel occlusions who are within the 6 h time-window after stroke onset. After validation in a larger independent dataset the model can be considered to select patients for endovascular treatment in whom stroke onset is unknown.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Anke Wouters and Götz Thomalla – receiving grant from European Union (FP7/2007–2013 nr. 278276 WAKE-UP). Patrick Dupont, Stephanie Kemp, Rico Laage, Maarten Lansberg – none. Soren Christensen – consulting work for iSchemaView.
Bo Norrving – fees paid to the institution from SYGNIS for steering committee work in the AXIS2 trial. Vincent Thijs – receiving fees for serving on the steering committee of the AXIS 2 trial. Gregory Albers – consultant of iSchemaView, Covidien and Lundbeck. He has an equity interest in iSchemaview. Robin Lemmens – senior clinical investigator of FWO Flanders.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DEFUSE 2 was funded by a grant from NINDS. R01 NS03932505 (G.Albers).
Informed consent
For the original studies the local institutional review boards approved the conducted research.
Ethical approval
The study was performed according to the principles of the declaration of Helsinki.
Guarantor
AW.
Contributorship
SK, BN, RL, ML, GA, VT acquired the data. AW, PD, RL, SC, GA, VT, ML analysed and interpreted the data. All authors were involved in drafting and revising the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.