
Abstract
Introduction
In patients with stroke attributable to cervical artery dissection, we compared endovascular therapy to intravenous thrombolysis regarding three-month outcome, recanalisation and complications.
Materials and methods
In a multicentre intravenous thrombolysis/endovascular therapy-register-based cohort study, all consecutive cervical artery dissection patients with intracranial artery occlusion treated within 6 h were eligible for analysis. Endovascular therapy patients (with or without prior intravenous thrombolysis) were compared to intravenous thrombolysis patients regarding (i) excellent three-month outcome (modified Rankin Scale score 0–1), (ii) symptomatic intracranial haemorrhage, (iii) recanalisation of the occluded intracranial artery and (iv) death. Upon a systematic literature review, we performed a meta-analysis comparing endovascular therapy to intravenous thrombolysis in cervical artery dissection patients regarding three-month outcome using a random-effects Mantel–Haenszel model.
Results
Among 62 cervical artery dissection patients (median age 48.8 years), 24 received intravenous thrombolysis and 38 received endovascular therapy. Excellent three-month outcome occurred in 23.7% endovascular therapy and 20.8% with intravenous thrombolysis patients. Symptomatic intracranial haemorrhage occurred solely among endovascular therapy patients (5/38 patients, 13.2%) while four (80%) of these patients had bridging therapy; 6/38 endovascular therapy and 0/24 intravenous thrombolysis patients died. Four of these 6 endovascular therapy patients had bridging therapy. Recanalisation was achieved in 84.2% endovascular therapy patients and 66.7% intravenous thrombolysis patients (odds ratio 3.2, 95% confidence interval [0.9–11.38]). Sensitivity analyses in a subgroup treated within 4.5 h revealed a higher recanalisation rate among endovascular therapy patients (odds ratio 3.87, 95% confidence interval [1.00–14.95]), but no change in the key clinical findings. In a meta-analysis across eight studies (n = 212 patients), cervical artery dissection patients (110 intravenous thrombolysis and 102 endovascular therapy) showed identical odds for favourable outcome (odds ratio 0.97, 95% confidence interval [0.38–2.44]) among endovascular therapy patients and intravenous thrombolysis patients.
Discussion and Conclusion
In this cohort study, there was no clear signal of superiority of endovascular therapy over intravenous thrombolysis in cervical artery dissection patients, which – given the limitation of our sample size – does not prove that endovascular therapy in these patients cannot be superior in future studies. The observation that symptomatic intracranial haemorrhage and deaths in the endovascular therapy group occurred predominantly in bridging patients requires further investigation.
Introduction
Cervical artery dissection (CeAD) is a major cause of ischemic stroke in young adults. 1 Intravenous thrombolysis (IVT) is effective and safe in acute ischemic stroke. 2 This appears to be true also for acute ischemic stroke attributable to CeAD.3,4 However, observational data suggest that IVT may not be as effective in CeAD ischemic stroke as in non-CeAD ischemic stroke patients. 3 Moreover, observational data did not show a benefit of IVT versus best medical treatment without IVT for CeAD patients, indicating the legitimacy to search for more effective treatment options in particular endovascular therapy (EVT). 5 The reportedly lower effectiveness of EVT in CeAD as compared to other stroke causes might – to some extent – be explained by the frequent occurrence of occlusions of the large arteries affected by the dissection which was reported in up to 90% 3 and nearly half of them being accompanied by an occlusion of a large intracranial artery distally to the site of dissection (i.e. tandem occlusion). 3
Thus, patients with stroke due to CeAD might benefit particularly from EVT, considering that at least in anterior circulation stroke, in recent randomised clinical trials (RCTs), EVT (with or without IVT) has been shown to be superior to IVT alone in presence of large intracranial artery occlusion.6–11
Data comparing EVT versus IVT in patients with CeAD are not available from the aforementioned RCTs. Thus, observational, comparative data based on well-maintained, comprehensive registries might be helpful in this situation. With these considerations in mind, we analysed data from the prospective, observational, multicentre ‘SWISS’ (Swiss Intravenous and Intra-arterial Thrombolysis for Treatment of Acute Ischemic Stroke Registry) recanalisation registry to compare EVT versus IVT in patients with stroke attributable to CeAD and proven intracranial artery occlusion with regard to outcome and complication measures. Further, we performed a systematic review and meta-analysis across all studies, including our data, comparing EVT versus IVT in CeAD stroke patients.
Methods
Study population and study data
This study is based on the dataset of the prospective observational multicentre “SWISS” (
From 2007 to 2012, all consecutive patients with acute ischemic stroke from all causes with proven intracranial arterial occlusion who were treated with IVT and/or EVT in the Swiss stroke centres of Berne, Basel, Geneva, Zurich, Lausanne and St. Gallen were enrolled in local thrombolysis registries. Data of these local registries were then pooled to build the SWISS registry. A detailed description of variables and inclusion and exclusion criteria of the SWISS registry are outlined in the supplemental methods.
For the current study, we selected all patients with proven CeAD (internal carotid and/or vertebral artery) as cause of acute ischemic stroke. In line with prior research, CeAD was defined by the following, widely accepted diagnostic criteria: presence of a mural hematoma, aneurysmal dilation, long tapering stenosis, intimal flap, double lumen, or occlusion situated >2 cm above the carotid bifurcation revealing an aneurysmal dilation or a long tapering stenosis after recanalisation.3–5,12
We dichotomised patients into two groups: (i) patients receiving IVT only and (ii) those receiving any form of EVT with or without IVT.
The following – prospectively ascertained – data were extracted from the aforementioned SWISS registry: age; sex; presence of hypertension, hypercholesterolemia and diabetes mellitus; stroke-onset-to-treatment-time; stroke severity (i.e. National Institutes of Health Stroke Scale (NIHSS)); systolic blood pressure at baseline; functional three-month outcome as assessed by the modified Rankin Scale (mRS) and presence of post-treatment symptomatic intracranial haemorrhage (sICH). The following variables were reviewed and verified by local source data checks by the authors (i.e. ChT, RK, HM, AE, LS and GK): site of dissection (i.e. internal carotid or vertebral artery or both) and the presence or absence of (i) multiple dissections, (ii) complete occlusion of the dissected artery and (iii) tandem occlusions. Tandem occlusion was defined as occlusion of both the extracranial portion of the dissected artery as well as occlusion of a large intracranial artery distally to the site of extracranial dissection. Occlusion of the large intracranial artery was defined and distinguished as occlusion of (a) M1-M2 segment of the middle cerebral artery, (b) A1 segment of the anterior cerebral artery, (c) intracranial portion of the distal internal carotid artery, (d) the carotid-T-portion of the intracranial internal carotid artery, (e) the P1-P2 segments of the posterior cerebral artery and (f) the basilar artery. We distinguished ‘no recanalisation’ versus ‘recanalisation’ (i.e. the merged categories partial and complete recanalisation based on the criteria of thrombolysis in myocardial infarction 13 and thrombolysis in brain ischemia 14 ).
Treatment
Patients received (i) IVT or (ii) EVT, either alone or combined with IVT (bridging). The choice between IVT and EVT as well as the specific treatment in case of EVT was left to the discretion of the treating neurologists and neuroradiologists. Endovascular treatment included mechanical thrombectomy with devices available 2007–2012 (stent retrievers), thrombus aspiration, or percutaneous transluminal angioplasty. Intra-arterial application of urokinase or tissue plasminogen activator (tPA) as well as intracranial or extracranial stent placement was performed in selected patients.
Outcome
The primary outcomes of the current study were (i) excellent three-month outcome (i.e. mRS 0–1) and (ii) the occurrence of sICH. 15 Secondary outcome measures were (i) favourable three-month outcome (i.e. mRS 0–2), (ii) death from any cause during a three-month follow-up period and (iii) recanalisation of the occluded intracranial artery.
Statistical analyses
We compared patients treated with IVT only versus those with EVT (with or without prior IVT) with regard to (i) baseline characteristics and (ii) occurrence of outcomes measures. We used chi square test, Fisher exact test and Mann–Whitney test, where appropriate. Due to the small number of events and in order to avoid overfitting for occurrence of sICH, death and recanalisation, we performed unadjusted analyses only. Data were given as mean with standard deviation or median with interquartile range (IQR), where appropriate.
The association of IVT and EVT treatments and three-month outcome was assessed by using a binary logistic regression model with calculation of crude odds ratios (ORs) and 95% confidence intervals (CIs). Furthermore, based on results of prior research,3–5 we adjusted for stroke severity (NIHSS), age and sex.
Post hoc analyses
We exploratively compared bridging patients (EVT + IVT) versus pure EVT patients (EVT without IVT) with regard to primary and secondary outcomes. We also performed sensitivity analyses comparing (i) all EVT patients (with and without IVT) to IVT patients treated within 4.5 h since symptom onset and comparing (ii) bridging EVT patients to IVT patients with regard to the primary and secondary outcomes.
For all analyses, a P-value of 0.05 was considered statistically significant. Analyses were performed using SPSS, Version 22 (IBM, Armonk, NY, USA).
Meta-analysis
We performed a meta-analysis across existing studies comparing IVT and EVT in CeAD patients. For this, we first performed a systematic literature search of the pubmed© (www.pubmed.com) and the Embase© (www.embase.com) database using the following search term: (‘carotid artery dissection’ or ‘vertebral artery dissection’ or ‘cervical artery dissection’) and (‘thrombolysis’ or ‘tPA’ or ‘endovascular’ or ‘intra-arterial’ or ‘thrombectomy’). Second, the abstracts of all search results were reviewed for eligibility by a single rater (ChT). Inclusion criteria were as follows: (i) IVT-treated CeAD patients were compared to EVT-treated patients and (ii) three-month outcomes were reported as mRS, stratified to IVT versus EVT. Studies reporting on either IVT or EVT alone or using outcomes reported in the literature for comparison were excluded, as were studies which tested an intervention other than IVT versus EVT in parallel without reporting outcome independently to this other intervention. We also excluded case reports, case series and comments. Third, the reference lists of included publications and review papers were checked for additional possibly eligible studies. Forth, the final decision whether to include individual studies were based on the consensus of two raters (ChT and STE). Fifth, data about favourable (i.e. mRS 0–2) and excellent (i.e. mRS 0–1) three-month outcome were extracted from the full publications of the included studies. We additionally extracted data on the occurrence of death and symptomatic ICH in studies reporting separately on these outcomes in both treatment groups. In a random-effects Mantel–Haenszel model, treatment effects as risk ratios with 95% CI were calculated using ‘IVT’ as reference treatment. We quantified heterogeneity across the included studies using the I2 statistic. The meta-analysis was performed using the ‘Review Manager Software’ (RevMan, version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
Results
Patient characteristics
Baseline clinical characteristics of all patients with crude comparisons between patients treated with IVT versus EVT (with or without IVT).
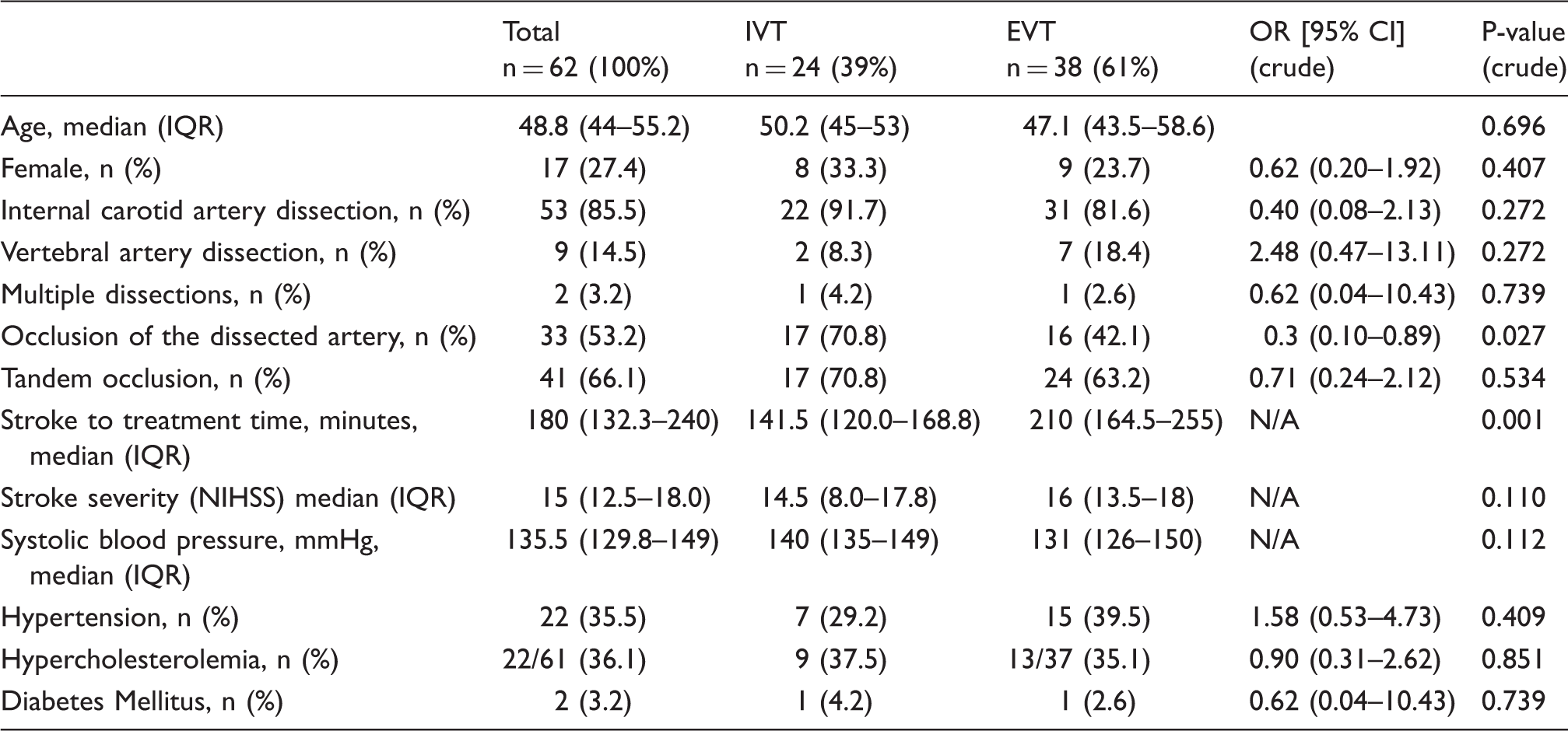
IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale.
Twenty-four patients (39%) received IVT alone and 38 patients (61 %) received EVT (25 with and 13 without IVT). Baseline characteristics did not differ significantly between groups, except for the variables ‘occlusion of the dissected artery’ which occurred more often in the IVT group (70.8) than in the EVT group (42.1%) and, ‘time–to-treatment,’ which was significantly longer in the EVT group (median 210 min (IQR 164.5–255), P = .001) than in the IVT group (median 141 min; IQR 120.0–168.8; Table 1). Patients in the EVT group had more severe strokes on average than patients treated with IVT only (median NIHSS: 16 (13.5–18) versus 14.5 (8.0–17.8)); however, this difference was not statistically different (P = 0.110, Table 1).
Details of endovascular treatment
Among the 38 EVT patients, 13 (34%) had mechanical thrombectomy (9 with stent retriever and 4 with other devices), 16 (42%) had thrombus aspiration and 9 (24%) received intra-arterial thrombolysis (IAT, intra-arterial urokinase or intra-arterial tPA). The latter were treated with IAT alone or in combination with other endovascular procedures. Two patients were intended to receive EVT, which was stopped as soon as complete arterial recanalisation had been proven by angiography. In 23/38 (61%) patients, EVT was performed after initial IVT (i.e. bridging therapy). Intracranial stenting was performed in 2/38 patients (5%, both basilar artery) and extracranial stenting of the dissected artery was performed in 22/38 patients (58%).
Primary and secondary outcome measures
Primary outcomes
Three-month outcome, complications and recanalisation data for all patients. Crude and adjusted comparisons of patients treated with IVT versus those treated with EVT including bridging.
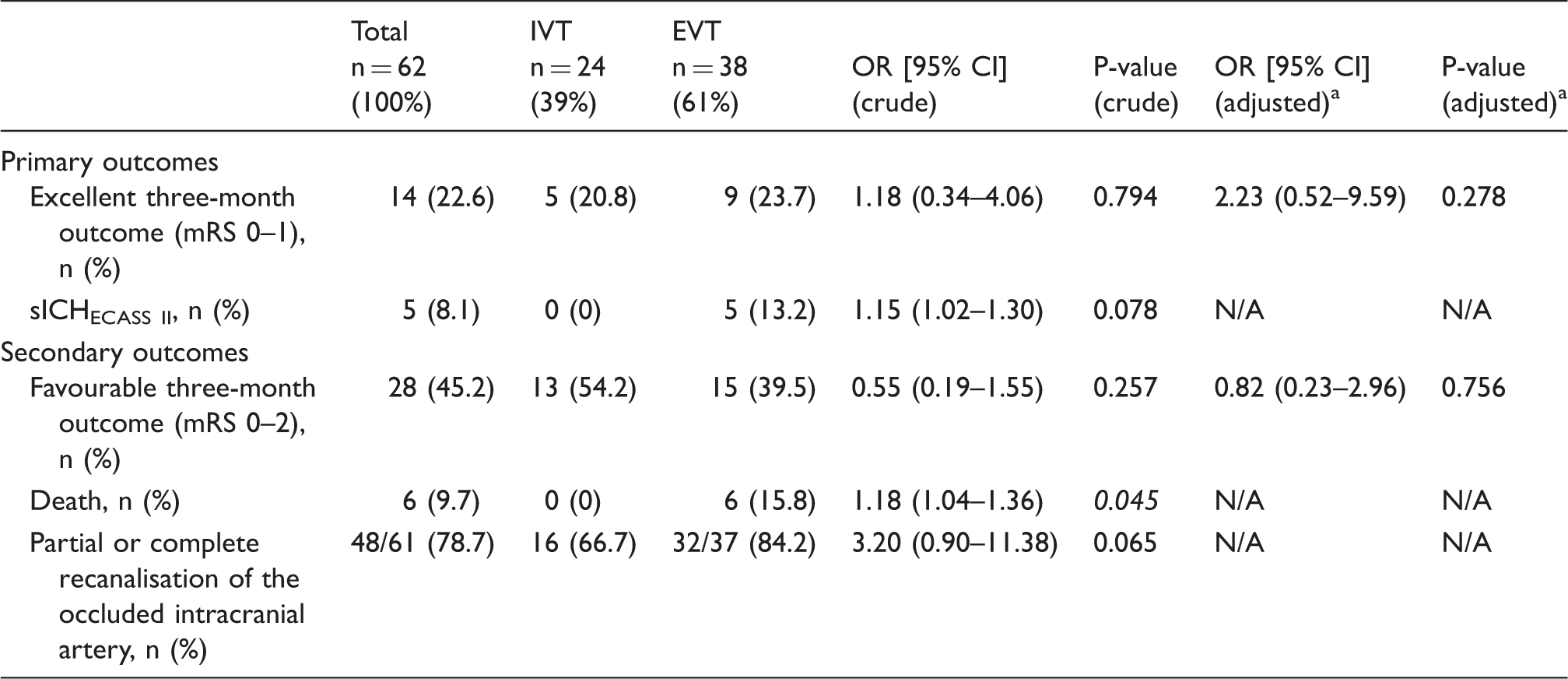
Adjusted for age, sex and stroke severity (NIHSS). NIHSS: National Institutes of Health Stroke Scale; sICH: symptomatic intracranial haemorrhage; IVT: intravenous thrombolysis; EVT: endovascular therapy; OR: odds ratio; mRS: modified Rankin Scale.
Secondary outcomes
Favourable three-month outcome was equally frequent in both groups (ORadjusted 0.82, 95% CI [0.23–2.96]; Table 2). None of the 24 IVT-treated patients and 6/38 EVT-treated patients (15.8%) had died at three months (ORunadjusted 1.18, 95% CI [1.04–1.36], punadjusted = 0.045; Table 2).
Intracranial recanalisation was achieved in 84.2% of the EVT and 66.7% IVT patients, (OR 3.2, 95% CI [0.9–11.38]; Table 2).
Post hoc analyses
Post hoc analyses comparing EVT-treated patients with and without bridging therapy with regard to primary and secondary outcomes.
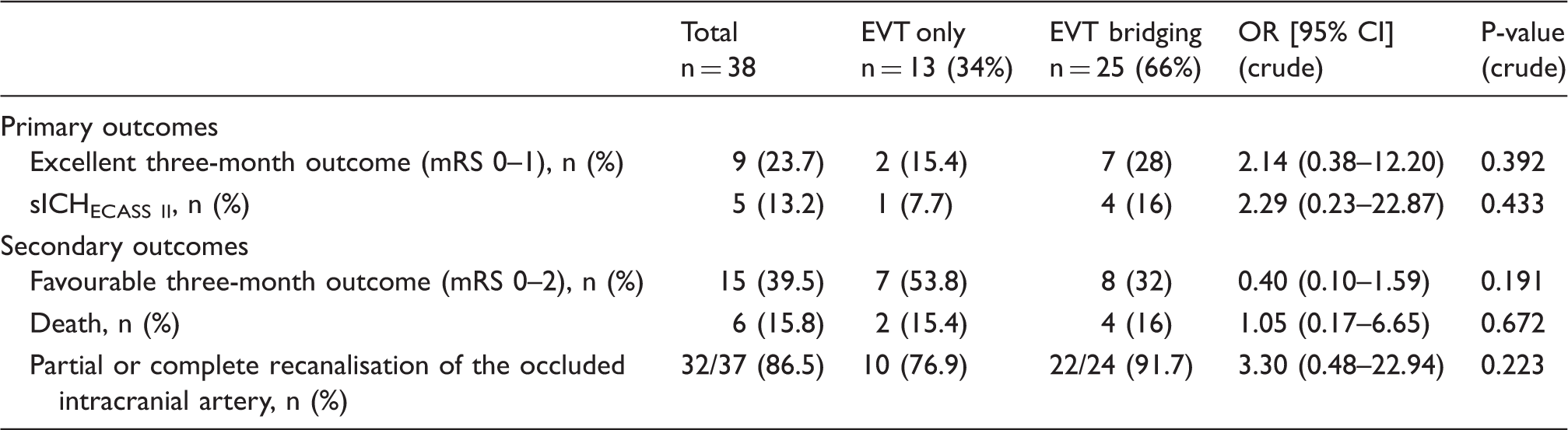
sICH: symptomatic intracranial haemorrhage; EVT: endovascular therapy; mRS: modified Rankin Scale.
Sensitivity analyses in the subset of patients treated within 4.5 h revealed a higher recanalisation rate among EVT patients (OR 3.87, 95% CI [1.00–14.95]), but no change among the key clinical findings. Likewise, comparing IVT patients with EVT bridging patients (excluding EVT only) with regard to our primary and secondary outcome measures did not reveal any major changes in our findings.
Meta-analysis
As of 20th October 2017, our literature search yielded 859 results. We identified seven studies which met the eligibility criteria for a systematic comparison of EVT versus IVT in CeAD.5,16–20 Figure 1 illustrates the process of identification of studies. One additional study was excluded after detailed review of the full publication because of incomplete reporting of three-month outcome with several missing data.
21
Another study focused on the effect of the implementation of stroke centre care on EVT in CeAD stroke patients.
22
Outcome data were not reported independently of the stroke centre care implementation. We contacted the corresponding author to retrieve the missing data; however, we could not obtain additional information. Thus, this study was excluded from our meta-analysis. In a sensitivity analysis, we added the available data of the latter study, which did not alter our main findings (data not shown).
Flow chart presenting the search results from a systematic literature search of the Pubmed and the Embase databases searching for studies comparing EVT to IVT in CeAD patients. Stepwise in-/exclusion of suitable or inappropriate studies.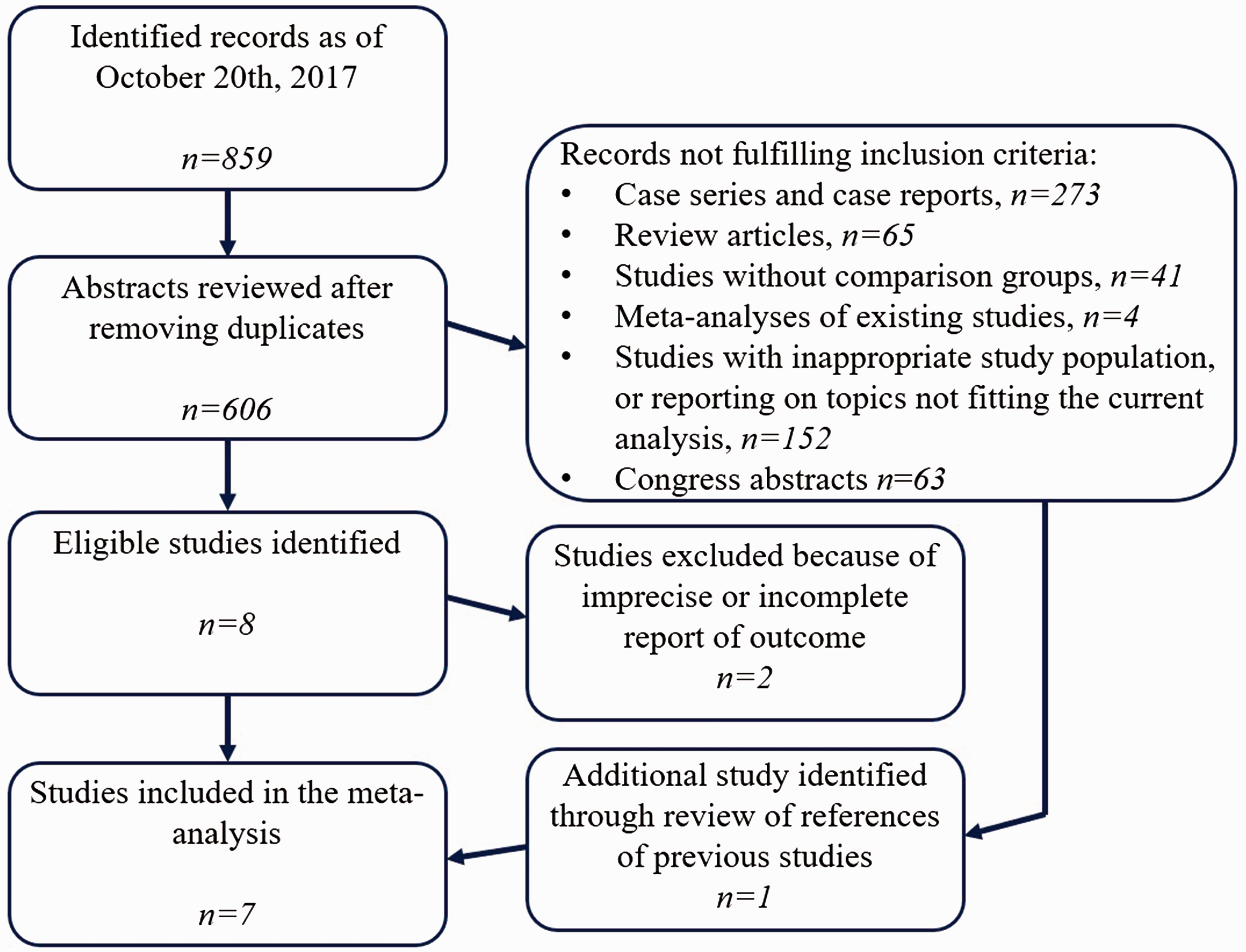
Including the current study, there were eight studies comparing EVT (n = 102) versus IVT (n = 110) in 212 CeAD patients.5,16–20,23 With regard to the occurrence of a favourable three-month outcome, there was no significant difference between both treatment groups (OR 0.97, 95% CI [0.39–2.44]; Figure 2). However, there was substantial heterogeneity in treatment effects across all studies (I2 = 35%). Additional data on excellent three-month outcome (i.e. mRS 0–1) were available in four previous studies as well as in our dataset (n = 66 EVT, 86 IVT patients) revealed no significant difference between these two groups (OR 0.89, 95% CI [0.38–2.09]; Supplementary Figure 1). Meta-analysis of the six studies (including our study) reporting on death at three months stratified to treatment groups did not show a significant difference between IVT- and EVT-treated patients (OR 0.81, 95% CI [0.16–3.97]; Supplementary Figure 2). For sICH, there were too few data (n = 5 patients) available for meta-analysis.
Meta-analysis of studies comparing IVT to EVT (with or without IVT) in CeAD patients. Data are numbers of patients with favourable outcome (i.e. mRS 0–2) at three-month follow up and Mantel–Haenszel random-effects risk ratios including 95% confidence intervals. Patients already included in previous analyses (Engelter et al.
5
) were excluded from this study for this meta-analysis.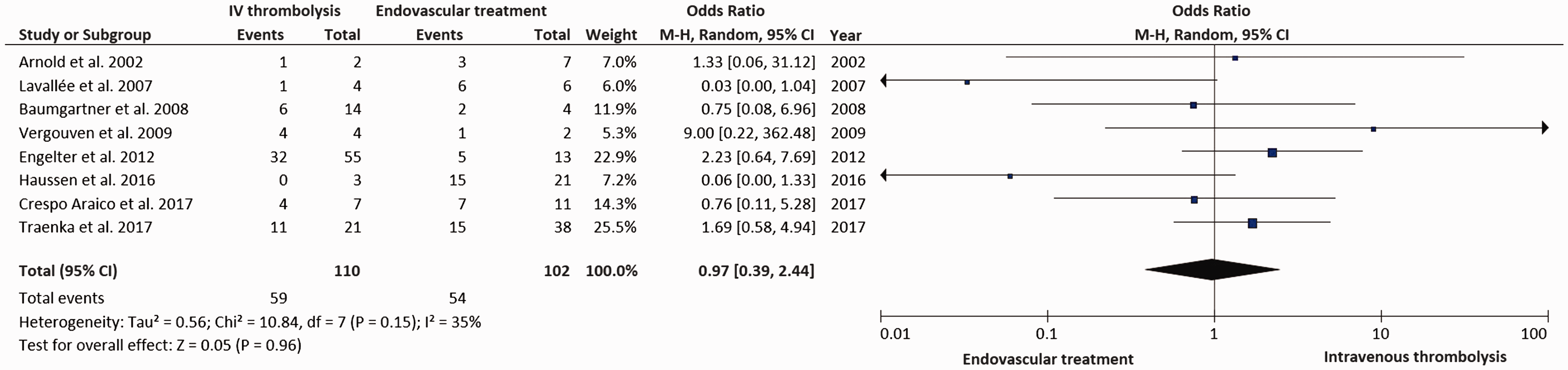
Discussion
The present study yielded the following key findings: (i) there was no signal of superior clinical efficacy of EVT over IVT in CeAD patients. Although comparable findings resulted from a meta-analysis across available study data, limitations in sample sizes urge for cautious interpretation of these findings which do not prove that EVT cannot be superior in future studies and (ii) sICH occurred exclusively in the EVT group and predominantly in bridging patients (i.e. EVT + IVT), a finding that requires further investigation.
Despite, to our knowledge, reporting on the largest cohort of EVT-treated CeAD stroke patients, our results have to be interpreted cautiously, as this analysis is based on observational, non-randomised data, and still the sample size is comparably small.
The lack of indicators for clinical superiority with regard to three-month functional outcome of EVT over IVT in CeAD was unexpected for two reasons: First, observational data suggested that CeAD patients seem to benefit less from IVT than non-CeAD stroke patients, 3 although IVT in CeAD stroke patients was shown feasible and safe.4,5 Second, in stroke of miscellaneous causes, EVT has been shown superior to IVT alone according to recent RCTs.6–11 These RCTs focussed on patients with occlusion of the anterior intracranial circulation, a feature which was present in more than 8 of 10 patients of our cohort, too.
Possible explanations for the missed clinical superiority in our study on data collected until 2012 include that the devices used for EVT in our study cohort (as well as in those included in the meta-analysis) do no longer reflect current standard. Our results seem to resemble those of the RCTs testing EVT versus IVT in stroke in 2013, which failed to show superiority at that time.24–26 Improvements in devices, the setting of EVT by the implementation of stroke centres and optimised treatment pathways leading to shorter delays in time to reperfusion, were considered key in explaining why two years after the neutral EVT-RCTs several RCTs did in fact prove superiority of EVT. Thus, our findings seem to indicate that the aforementioned factors are of utmost importance also for a stroke cause like CeAD in which IVT may be less effective than in other stroke causes. Indeed, for the successful usage of EVT in CeAD patients, the importance of the implementation of a stroke centre setting has recently been shown. 21 Further, a short time-to-treatment seems to matter, which – in median – was 69 min longer in the EVT treatment group compared with IVT-treated patients in our study. However, although stroke to treatment times in the MR CLEAN trial were more balanced between treatment groups than in our study, median time from stroke onset to EVT in our study was comparable to that in MR CLEAN. 6 Further, sensitivity analyses on patients treated within 4.5 h from symptom onset showing a significantly higher recanalisation rate in EVT than in IVT patients may indicate the importance of the variable of time for achieving recanalisation. This observation, which did not translate into a change in our clinical outcomes, suggests that the effect size might have been too small to be detectable in a relatively small population.
In addition, the high rate of patients with occlusion of the dissected extracranial artery – i.e. the frequent presence of tandem occlusions in CeAD stroke – might have contributed to our key finding. In ours, as well as previous IVT-/EVT-treated CeAD populations, >50% of patients had tandem occlusions.3,5,27 This rate is much higher than that reported in the RCTs and indicates lower odds for a favourable outcome, as tandem occlusion is a known negative outcome predictor.28,29
Numerically, with combined EVT/IVT more patients had excellent outcome and arterial recanalisation than patients treated with EVT only. In turn, four of five sICH occurred in EVT + IVT patients, a number which may have contributed to the high death rate in these patients. These observations may challenge the usefulness of prior IVT before EVT in CeAD patients. Furthermore, these findings are in line with the observed higher bleeding complication in 40 patients treated with bridging therapy (i.e. EVT + IVT) for stroke due to miscellaneous causes than in 40 patients with pure EVT. Interestingly, this difference did not involve sICH. 30
As novelty – and unlike previous studies comparing EVT to IVT in CeAD patients – we present comparative data on recanalisation rates. Recanalisation of the targeted intracranial artery is an important predictor of a favourable outcome in acute ischemic stroke patients. 31 In addition, although statistically not different in our primary analyses, it is encouraging that the recanalisation rate was much higher in the EVT patients than in the IVT patients. Furthermore, our recanalisation rate in EVT-treated CeAD patients resembled those of recent publications (39/44 (89%) 27 and 20/21 (95%) 19 ), which, however, lacked an own IVT-treated group for comparison.
We are aware of several limitations: First, this study is based on observational, non-monitored registry data which bear the risk of inclusion bias. Second, endovascular treatment in the participating centres was not standardised and different methods and devices were used to the discretion of the treating physicians which is likely to have influenced the overall treatment effect of EVT in this study. This is also true for the decision to either use EVT or IVT alone, which might have been affected by differences in time from stroke onset to treatment. Third, data included in this study were acquired until 2012. Since then, major improvements have been achieved in stenting and thrombectomy devices and techniques. Thus, our data as well as data included in the meta-analysis do no longer represent current standards. Fourth, data on collateral flow or brain parenchyma status (e.g. Alberta Stroke Program Early Computed Tomography Score, which modify outcome, were absent. Fifth, the interpretability of our meta-analysis is limited due to heterogeneity in study size and directions of effects with large CIs across studies.
Our study has the following strengths: (i) to our knowledge, we are reporting on the largest number of EVT-treated CeAD patients to date in a study comparing EVT to IVT in these patients; (ii) data in this registry were collected prospectively and data on three-month functional outcome were complete without loss-to-follow-up; (iii) in both patient groups, we were able to report on recanalisation rates and the presence of tandem occlusions; and (iv) the analysis on clinical outcome in our cohort and those of the meta-analysis yielded similar results. This similarity is reassuring and an argument against a spurious finding.
Conclusion
In this cohort study as well as in a meta-analysis of studies comparing IVT to EVT in CeAD patients, there was a trend towards higher recanalisation rates in EVT-treated patients. There was no clear signal of clinical superiority of EVT over IVT in this patient group, which, however, does not mean that EVT treatment in CeAD patients cannot ultimately be superior in future studies. Although, to our knowledge, being the largest cohort reporting on EVT-treated CeAD stroke patients, our results have to be interpreted cautiously, as this analysis is based on observational, non-randomised data. The observation that sICH in the EVT group occurred predominantly in bridging patients (i.e. IVT + EVT) requires further investigation. Our study as well as previous studies share the major limitation of including data which were acquired before recent major developments in EVT techniques and devices had been achieved. Analyses on EVT in CeAD based on contemporary, large and prospectively acquired datasets are needed and warranted to investigate if EVT is superior to IVT alone in CeAD patients, too.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Swiss National Science Foundation (33CM30-124119; 33CM30-140340/1).
Informed consent
Patients’ consent was waived.
Ethical approval
The SWISS thrombolysis registry has been approved by the ethics committee in Basel and in all participating centres if required.
Guarantor
ChT
Contributorship
ChT designed/conceptualised the study, analysed/interpreted the data, drafted the manuscript and collected data. STE initiated, designed, conceptualised and supervised the study, analysed/interpreted the data, revised the manuscript and collected data. All authors performed data collection, critical review of the manuscript and editing manuscript for content. All authors agreed on submission of the present version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.