
Abstract
Introduction
To assess the cost-effectiveness of stent-retriever mechanical thrombectomy and intravenous tissue plasminogen activator compared with intravenous tissue plasminogen activator alone in patients with acute ischaemic stroke due to large vessel occlusions in Spain.
Materials and methods
Clinical data were taken from the SWIFT PRIME clinical trial. A lifetime Markov state transition model defined by the modified Rankin Scale score was developed to estimate costs and health outcomes (life years gained and quality adjusted life years). A Spanish National Health System perspective (direct medical costs) was considered. Resource utilisation and utilities were obtained from available published data and endorsed by an expert panel. Costs (€, 2016) were obtained from various Spanish sources. Deterministic and probabilistic sensitivity analyses were performed.
Results
Stent-retriever thrombectomy after intravenous tissue plasminogen activator was associated with better outcomes (1.17 life years gained and 2.51 quality adjusted life years) and savings of €44,378, resulting in a dominant therapy over intravenous tissue plasminogen activator alone. A net monetary benefit of €119,744 was obtained considering a willingness-to-pay threshold of €30,000/quality adjusted life year gained. The combined therapy was also dominant in all sensitivity analyses, deterministic and probabilistic.
Discussion
The results were consistent with a previously published cost-effectiveness analysis and reinforce the likeliness of the selection of stent-retriever mechanical thrombectomy plus intravenous tissue plasminogen activator over intravenous tissue plasminogen activator alone.
Conclusion
Stent-retriever thrombectomy after intravenous tissue plasminogen activator is a dominant alternative over intravenous tissue plasminogen activator alone (more effective and less costly) for the treatment of acute ischaemic stroke patients with large vessel occlusions in the Spanish setting.
Keywords
Introduction
Global stroke burden is increasing, and it is one of the largest contributors to disability and mortality worldwide. 1 In 2014, stroke was the most common cause of death in women and the third most common cause in men in Spain, 2 and it is related to a substantial economic burden as a result of high hospitalisation costs and long-term care due to stroke-related disability. A recent study showed that the one-year follow-up direct healthcare cost per patient with ischaemic stroke admitted to stroke units in Spain was €8,623, out of an overall cost of €27,597, mostly due to informal care. 3 Another study estimated the cost of acute management and rehabilitation of cardioembolic stroke patients in €13,139, with the highest costs related to hospital stay and rehabilitation therapies. 4
For the last 20 years, the only evidence-based therapy for acute ischaemic stroke was intravenous tissue plasminogen activator (IV t-PA), administered within 3 h or up to 4.5 h after ischaemic stroke.5,6 Recent randomised clinical trials demonstrated the efficacy of adding mechanical thrombectomy to IV t-PA,7–11 which led European scientific societies to recommend mechanical thrombectomy, primarily with stent retrievers, after intravenous thrombolysis within 4.5 h if eligible, for the treatment of acute stroke patients with large artery occlusions in the anterior circulation within 6 h 12 or even up to 8 h after symptom onset. 11
The Solitaire Revascularisation Device is a stent retriever for mechanical thrombectomy in acute stroke treatment, which was the only or the most used device in four of these recent clinical trials.8–11 Recent meta-analyses assessed studies in which stent retrievers (mostly Solitaire) were used and showed that acute ischaemic stroke patients treated with a stent retriever after IV t-PA experienced significant improvement in independent functional outcomes (modified Rankin Scale [mRS] 0–2) at 90 days13,14 and an increased likelihood of complete recanalisation/reperfusion in comparison with IV t-PA alone. 15
Apart from clinical evidence, it is also necessary to assess cost-effectiveness so that decision-makers have complete information to include new therapies in our health system. The aim of this analysis was to evaluate the cost-effectiveness of mechanical thrombectomy with a stent-retriever device (Solitaire) after IV t-PA compared to IV t-PA alone in acute ischaemic stroke patients with confirmed occlusions in the proximal anterior intracranial circulation and absence of large ischaemic core lesions in Spain.
Material and methods
Model structure
A Markov model was designed to represent the evolution of acute ischaemic stroke patients according to the treatment received: mechanical thrombectomy with Solitaire stent retriever after IV t-PA and IV t-PA alone. It was based on the pragmatic review of previous models in stroke care in consultation with clinical experts, with a similar structure to the model used in the United Kingdom technology appraisal of alteplase. 16
The model included seven health states describing the different degrees of disability defined by the mRS scores (0, no symptoms; 6, death). During each cycle, in a fixed period of time during the follow-up, patients transited from one health state to another or remained in the same state. The model had a two-phase structure: an acute phase and a rest-of-life phase (Figure 1). The acute phase described patients’ management and outcomes from stroke onset to 90 days. All treatment effects were assumed to occur within this phase. Patients were then assigned a mRS score at 90 days after stroke. To allow for half-cycle correction, patients were also previously assigned a mRS score at 7–10 days after stroke or at discharge. A half-cycle correction is often used to compensate for patients’ transitions from one health state to another, which usually occurs at the beginning or end of a cycle, whereas transitions actually occur in the middle of each cycle on average.
17
The rest-of-life phase directly followed the acute phase from 91 days after stroke to the end of patients’ life. This phase included two different cycle lengths: from day 91 to a year after stroke and one-year period afterwards.
Markov model structure.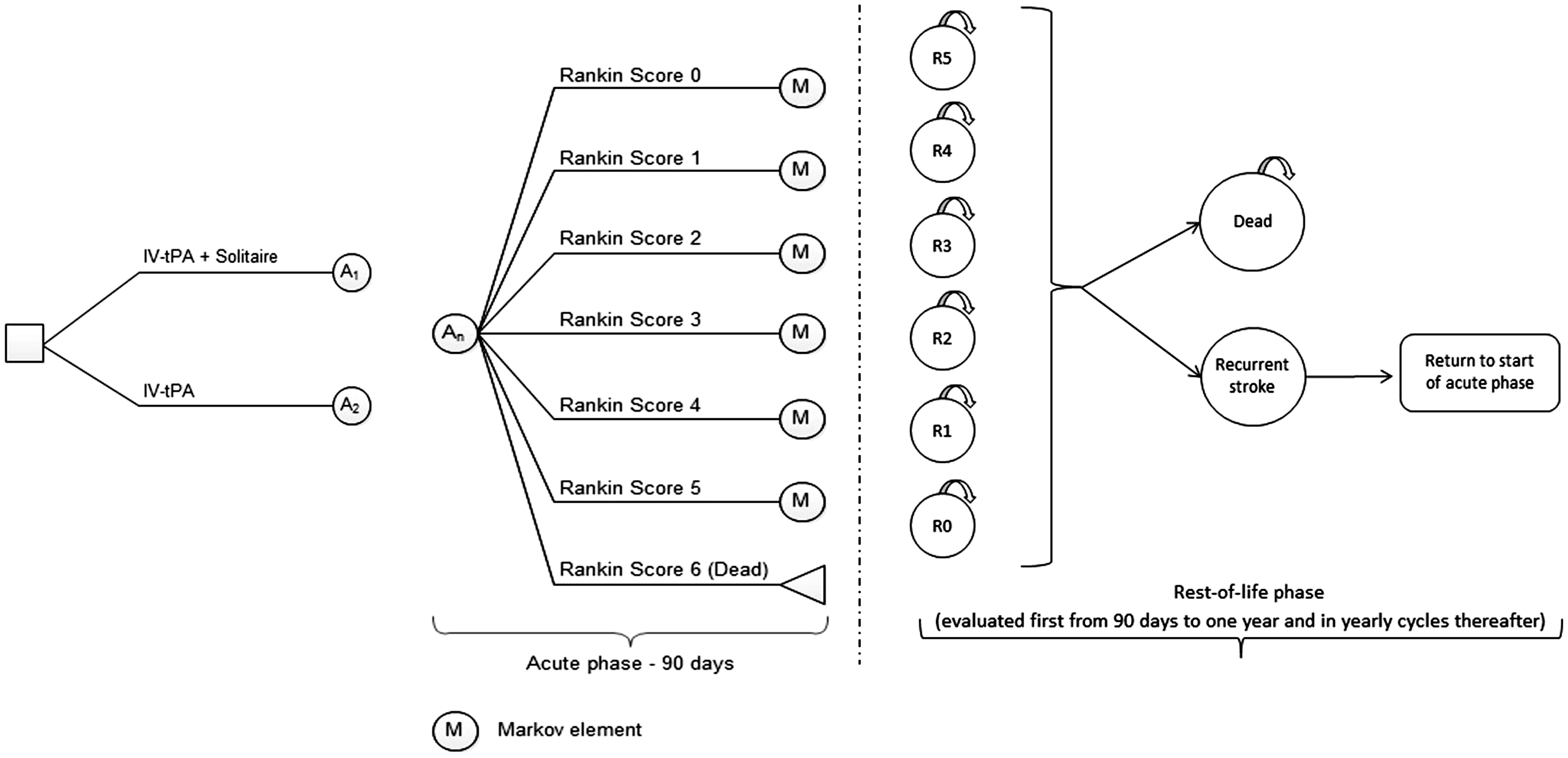
During the acute phase, it was assumed that patients were at no risk of recurrent stroke, whereas in the rest-of-life phase, a patient remained in the same mRS health state as that at 90 days until either a recurrent stroke or death occurred. 18 If a recurrence occurred, patients entered the acute phase again. In this case, transitions to health states were restricted to mRS scores equal to or greater than the previous mRS score. Risk of recurrent stroke was the same across all mRS scores with a maximum of one recurrent stroke per cycle.
Patient population
The acute ischaemic stroke patients included in the model had confirmed occlusions in the proximal anterior intracranial circulation and absence of large ischaemic core lesions and had to be able to undergo mechanical thrombectomy within 6 h from symptom onset. Patients’ characteristics were based on the SWIFT PRIME trial 10 population and a starting age of 66.
Clinical effectiveness
Clinical efficacy data and utility values.
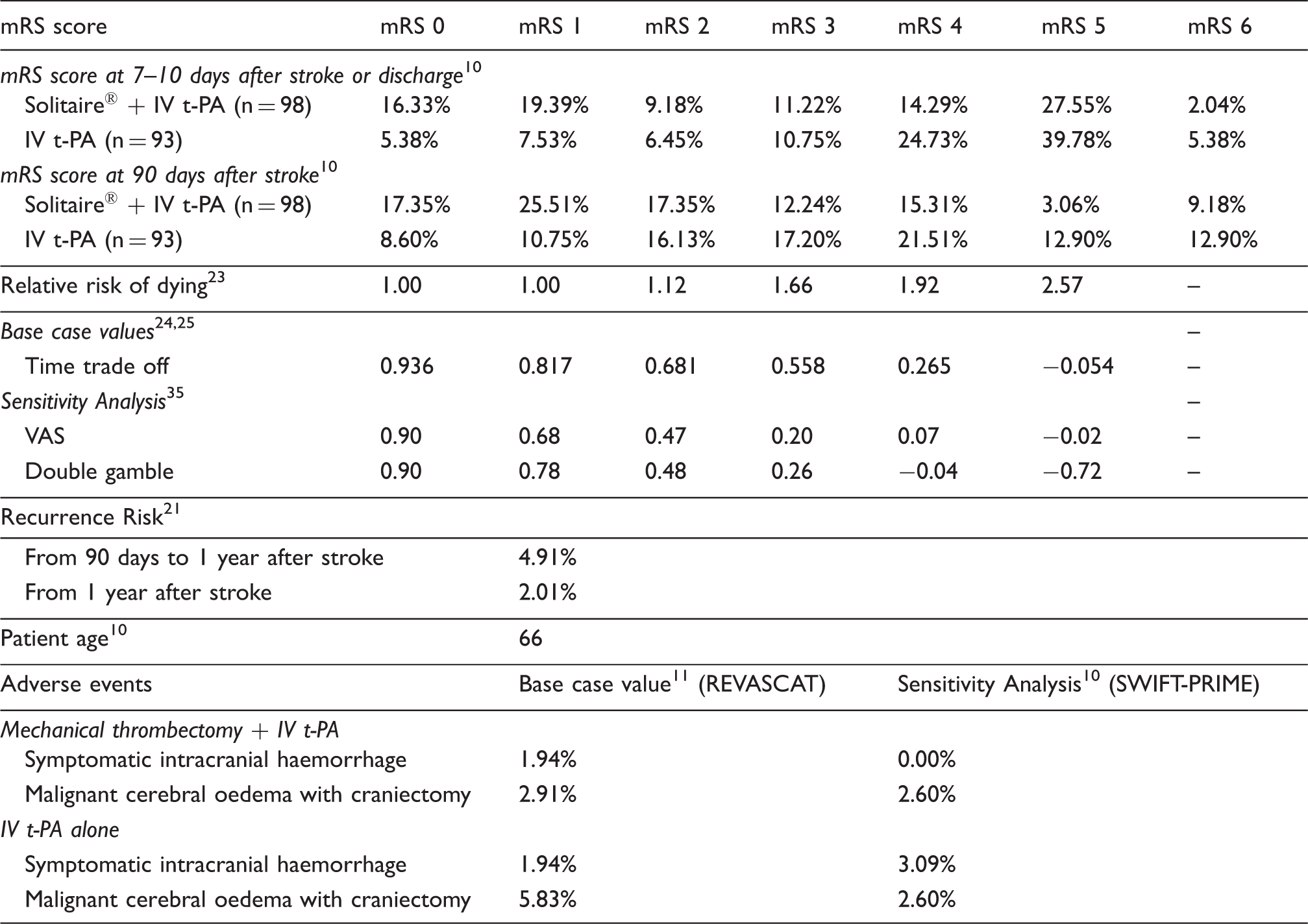
IV t-PA: intravenous tissue plasminogen activator; mRS: modified Rankin scale; VAS: visual analogue scale.
Quality of life
The quality-adjusted life year (QALY) is a measure which reflects both quantity and quality of life lived, calculated by weighting the life years gained (LYG) by the utility value. Utilities were assigned to health states and are often expressed as a numerical scale with extreme values of 0 (death) and 1 (optimal health). Negative utilities would indicate that living in this state is considered worse than death. Utility values for each health state, described in Table 1, were based on patients in the Oxford Vascular Study.22,23
Costs
Acute and long-term management costs.
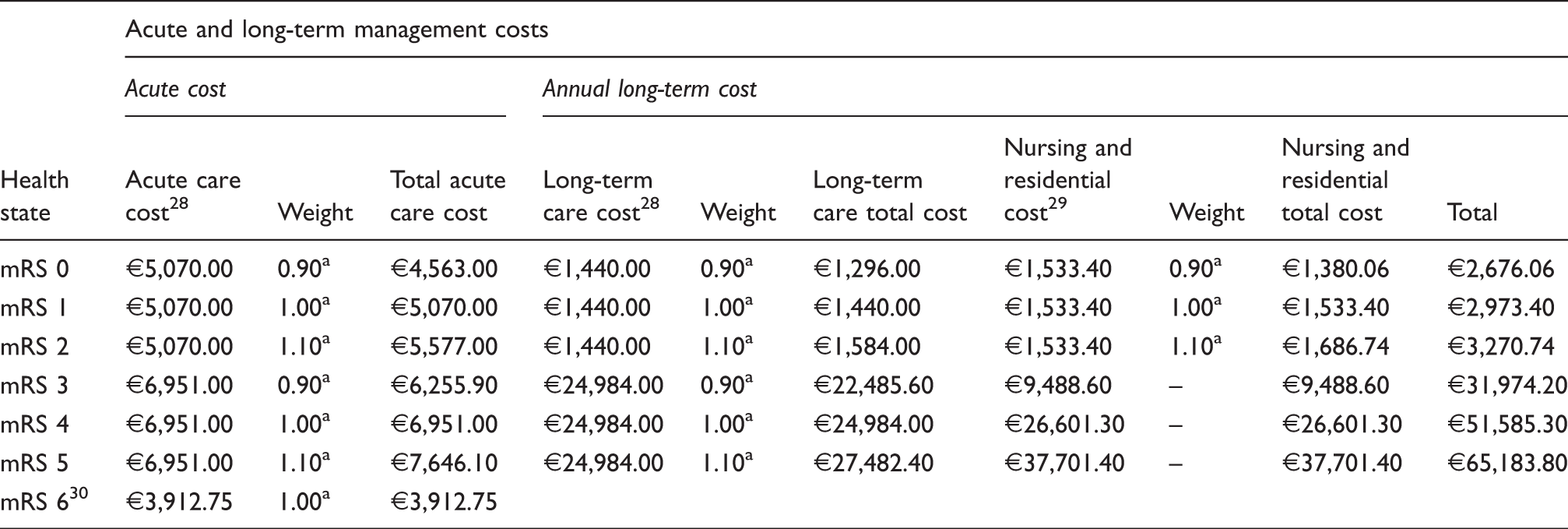
mRS: modified Rankin scale.
Weights informed by expert clinical opinion.
Treatment costs and adverse event management costs.
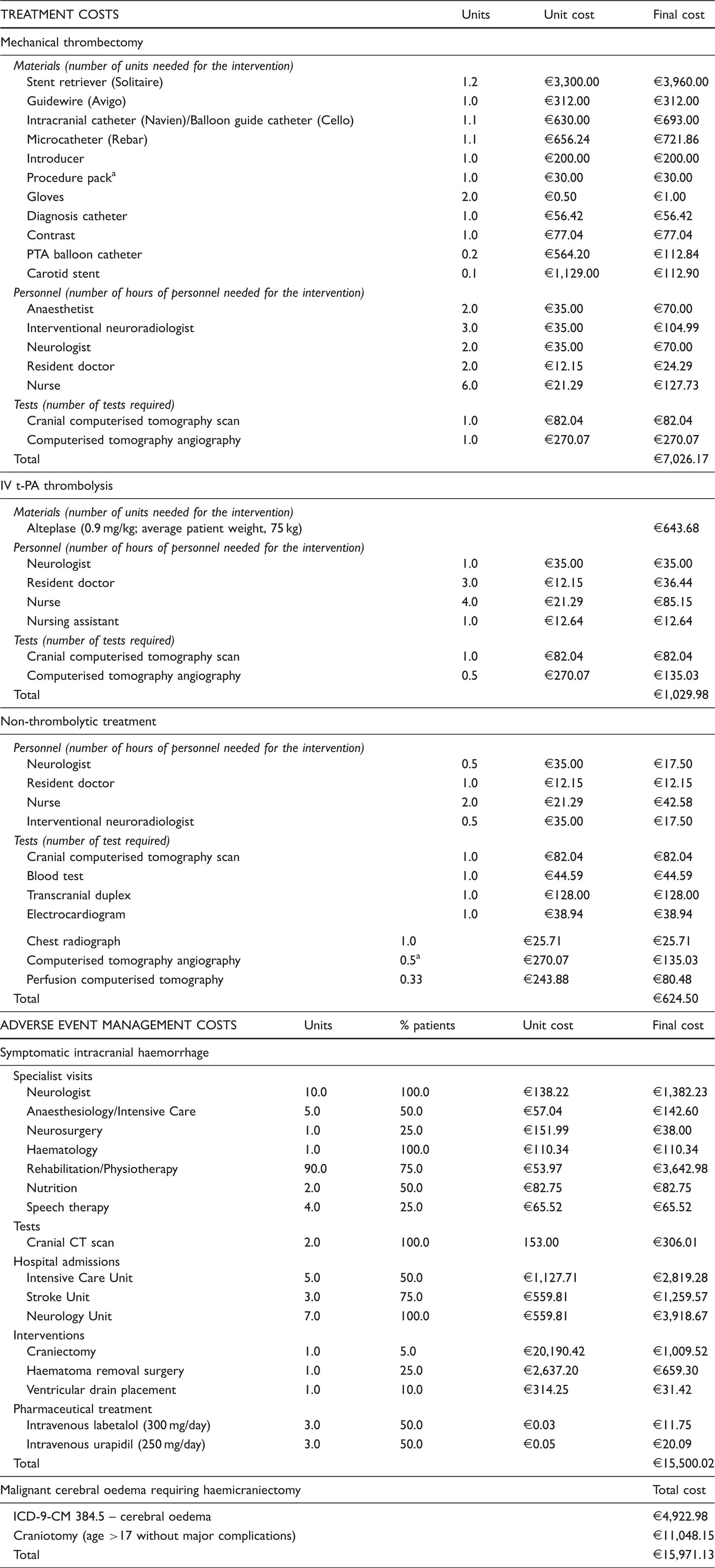
CT: computed tomography; IV t-PA: intravenous tissue plasminogen activator; PTA: percutaneous transluminal angioplasty.
It is estimated that half of the patients will not respond to IV t-PA and physicians will want to rule out a large arterial occlusion by performing a computerised tomography angiography.
Concerning adverse event management costs, symptomatic intracranial haemorrhage cost was obtained from resource use (€15,500). Malignant cerebral oedema requiring craniectomy was calculated considering the Diagnosis Related Group costs of cerebral oedema and craniectomy intervention cost (€15,971). 31
Cost-effectiveness analysis
The model calculated total costs and health outcomes per treatment arm for a hypothetical cohort of 1,000 patients. A lifetime horizon was considered in the base case scenario of this analysis.
The cost-effectiveness of mechanical thrombectomy after IV t-PA versus IV t-PA alone was assessed by the incremental cost-utility ratio (ICUR), comparing both costs and QALYs generated by these alternatives

Alternatively, the results were expressed by net monetary benefit (NMB), which included the commonly used cost-effectiveness threshold in Spain of €30,000/QALY gained,32,33 which is the willingness to pay for the additional QALYs obtained with the more effective treatment

A positive NMB value would indicate that combined therapy of stent-retriever mechanical thrombectomy and IV t-PA would be an efficient treatment option for acute ischaemic stroke according to the cost-effectiveness threshold.
Alternative scenarios and sensitivity analysis (SA)
Alternative scenarios considered different time horizons than lifetime (base case scenario): 1, 2, 5, 20 and 25 years. These analyses were also conducted including formal care costs.
Deterministic and probabilistic SAs were conducted to assess the robustness of the results. One-way deterministic SA varied the value of one base case input at a time, especially those with the greatest uncertainty: number of Solitaire devices required (1–2), discount rates (0–5%), starting age (55–75), health states utilities 34 (values obtained from visual analogue scale [VAS] and Double Gamble methods), recurrent stroke rates at 90 days (0–10%) and one year (0.5–5%), relative risk of dying (double). All costs varied by 10 and 25%. A probabilistic SA was also undertaken to assess the joint uncertainty in the model parameters (1,000 simulations). The value of each key parameter would vary within a specific probability distribution assigned to each parameter: mRS score at 90 days (Dirichlet), mortality relative risks (Lognormal), utilities (Beta) and costs (Gamma).
Results
Results of cost-effectiveness analysis (base case and alternative scenarios).
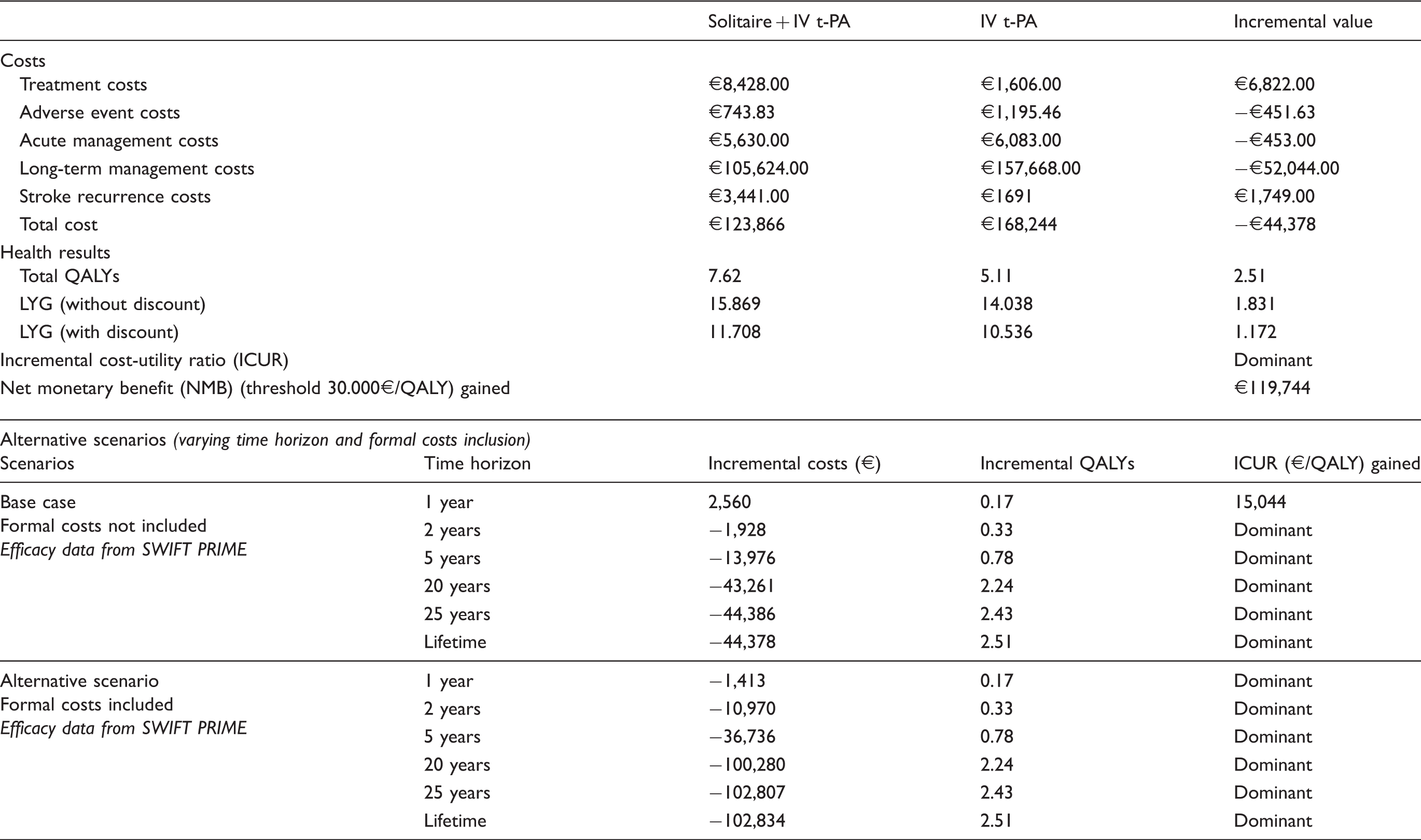
IV t-PA: intravenous tissue plasminogen activator; LYG: life years gained; QALY: quality-adjusted life year.
Alternative scenarios showed that in time horizons of two years and beyond, regardless of including formal care costs, mechanical thrombectomy after IV t-PA was always a dominant treatment option versus IV t-PA alone. Considering a one-year time horizon, the combined therapy had a ICUR of €15,044/QALY gained versus IV t-PA if formal care costs were not included, and it was dominant if formal care costs were considered (Table 4).
The robustness of the results was assessed with both deterministic and probabilistic SA. The deterministic analyses resulted in fewer costs and increased efficacy (more QALYs) for the combined therapy of the Solitaire device and IV t-PA versus IV t-PA alone. A positive value of NMB was always obtained in performing these analyses. The use of different utility values did not change the results (−€44,378 and 3.43 [double gamble] or 2.37 QALYs [EVA]). The starting age, utility values, discount rate and relative risk of dying were the key drivers of the analysis. Probabilistic analysis results also showed that mechanical thrombectomy plus IV t-PA was a dominant treatment alternative with lower associated costs and better health outcomes in 100% of the simulations performed. The results of both deterministic and probabilistic analyses are described in Figure 2.
Results of deterministic (a) and probabilistic (b) sensitivity analyses.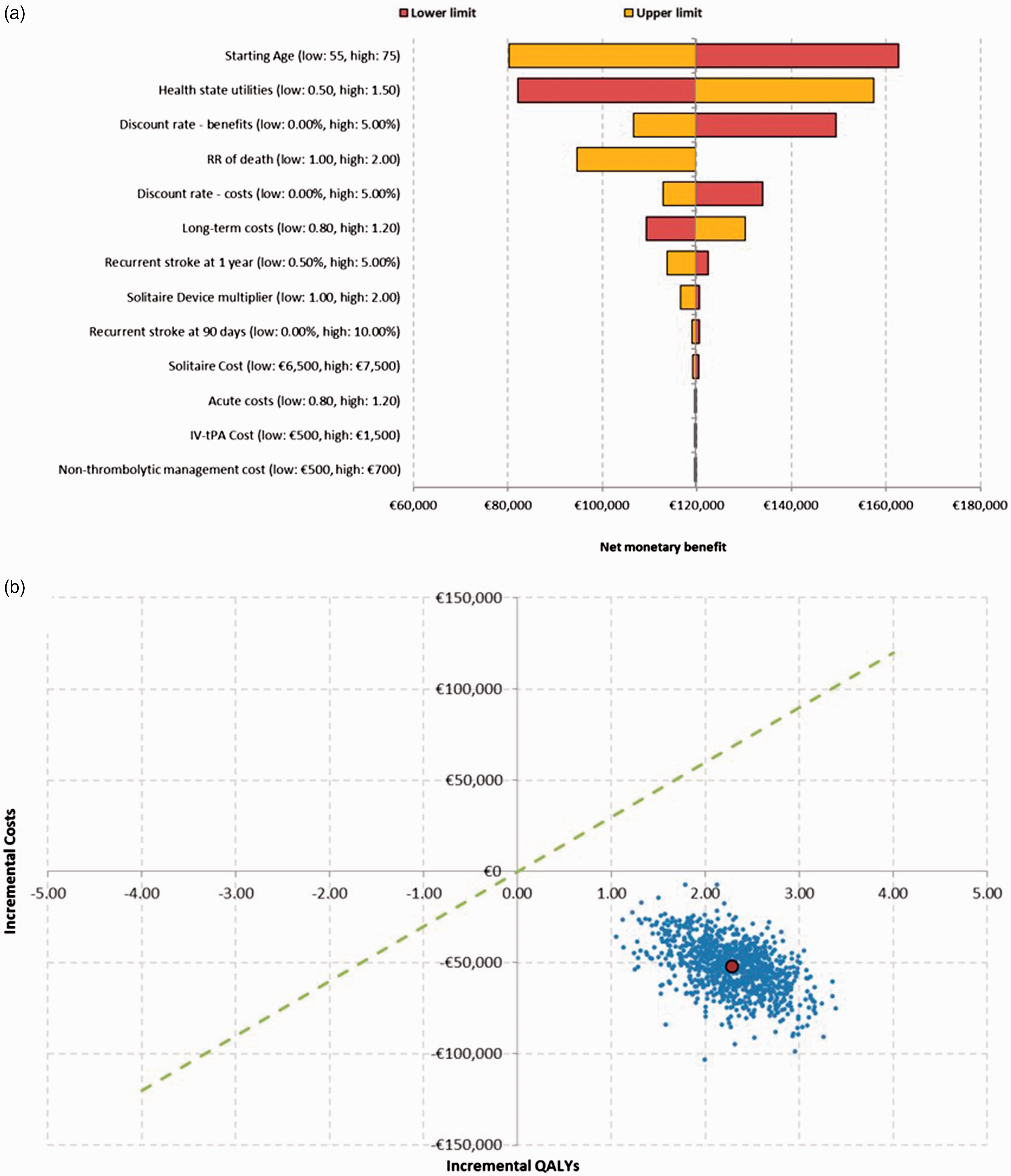
Discussion
The management of patients with acute ischaemic stroke has improved greatly over the last two decades with better imaging techniques and new interventions, such as intravenous thrombolysis and/or endovascular treatment. The narrow time window available for an effective treatment with IV t-PA and the difficulty of breaking down the blood clots in patients with large vessel occlusions have encouraged the emergence of new interventional approaches to extend this treatment period and achieve better outcomes in artery recanalisation and functional independence.
Despite the failure of the first generation of mechanical embolectomy devices in demonstrating a significant improvement over intravenous thrombolysis,26,35,36 the following stent-retriever trials achieved better results in recanalisation rates and functional outcomes.7–11 Thus, endovascular treatment with stent retrievers after IV t-PA has become the gold standard of acute ischaemic stroke treatment in patients with large vessel occlusions. 12
The results of this study showed that combined treatment of mechanical thrombectomy with a stent retriever device and IV t-PA for the treatment of acute ischaemic stroke in Spanish patients resulted in a dominant treatment alternative because of better health outcomes with a gain of 1.17 QALYs and lower costs with savings of €44,378 over IV t-PA alone during the patients’ lifetime. This treatment was associated with an NMB of €119,744, when a €30,000/QALY gained threshold was considered. When different time horizons were selected, stent-retriever mechanical thrombectomy after IV t-PA was always considered cost-effective and, over a two-year period, it was also a dominant therapy (less costly, more effective). The inclusion of long-term formal costs related to nursing and residential care resulted in a dominant therapy for all time horizons considered including the first year of analysis. Deterministic and probabilistic SA results showed robustness of the model inputs and revealed that the addition of endovascular treatment with stent retrievers to IV t-PA was a dominant alternative in 100% of the simulations.
A major strength of this analysis is that efficacy data were based on evidence from a randomised clinical trial data (SWIFT PRIME) which was stopped early due to proven efficacy. The only treatment alternatives considered in the study were Solitaire and IV t-PA. Inclusion of recurrent stroke in the model was an additional strength of the model because it assures that all clinical outcomes and related costs following a stroke were included. Additionally, the model related each mRS health status to patient outcomes of mortality, quality of life and resource use. Individual mRS scores, instead of combined dependence levels, better described the patients’ pathway.
However, this study was not exempt from some limitations. Efficacy data were taken from only one clinical trial contributing to meta-analyses. Because it was stopped early, it may have overestimated the effect of treatment. Although estimates are likely to be unaffected by the thrombectomy, they may lead to a reduction in difference between treatment and control over time in stroke survivors. The starting age of patients in SWIFT-PRIME was 66 years old, which seems to be lower than clinical practice. Thus, a reduction in benefits might occur in older patient populations, as shown in the deterministic SA, but a positive net benefit can still be achieved. Patients remain in the same mRS level unless they have a stroke recurrence, but mRS score could also be affected by age and comorbidities. However, these factors would vary equally in both treatment arms with no differences on incremental benefits. For cost estimation of acute and long-term management of stroke patients, costs per dependency levels by Barthel Index were converted into mRS, and therefore, they could not be completely representative of each mRS health state. These costs also needed to be weighted by ±10% to discriminate management costs between different mRS scores. However, despite the lack of available detailed cost data, these assumptions allowed the model to represent differences in management costs for the different disability degrees a patient could have. Additional costs related to patient transportation to centres where endovascular treatment is available were not included due to limited available information. However, these costs could apply in some situations. Utilities have been given by mRS score, but as a limitation, this scale has little bearing on pain and discomfort and anxiety/depression EQ-5D dimensions.
The model allowed the inclusion of only two adverse events. Symptomatic intracranial haemorrhage and malignant cerebral oedema requiring craniectomy were selected because they had the greatest impact on costs. The rest of the reported adverse events, such as vasospasm, were not included in the model, as they were not considered significant according to the expert panel. Adverse event rates for the base case scenario were selected from the REVASCAT Spanish trial, which assessed the efficacy of the inclusion of stent-retriever mechanical thrombectomy to standard medical management. Despite being obtained from a different study, these rates could be more representative of Spanish patients and management. These events contribute to short- and long-term costs, and their incidence was similar in both arms in SWIFT PRIME trial; therefore, they are unlikely to contribute to cost differences between treatments. Consequently, an SA with SWIFT PRIME rates was performed, and the results barely varied, in which combined treatment was still a dominant alternative for stroke management.
A cost-effectiveness study was published recently in the United Kingdom using the same model as in the present analysis. 37 This study showed that stent retriever use after IV t-PA is a dominant treatment alternative versus IV t-PA alone, leading to a savings of £33,190 and increased health benefits of 2.31 QALYs gained and a 98.6% likelihood of cost-effectiveness according to a threshold of £20,000/QALY gained. Most of the clinical parameters included in this study were used in the present analysis, having different sources of adverse events rates (SWIFT PRIME study) and resource use and cost estimation. Analyses for the United States and Italy have also been performed with this model resulting in combined therapy as a cost-effective option.38,39
Additional cost-effectiveness analyses of mechanical thrombectomy for the treatment of acute ischaemic stroke and Health Technologies Assessment agencies reports have also been recently published for various NHSs.40–48 These studies included efficacy data from a single randomised clinical trial (SWIFT PRIME or MR CLEAN) or from meta-analyses of several endovascular treatment randomised clinical trials and considered standard of care or IV t-PA only as the study comparator. Most of them had a healthcare and/or social care perspective. Despite the different results obtained in each study, the results are consistent with the present analysis, and all concluded that mechanical thrombectomy associated with the standard treatment/IV t-PA was a cost-effective alternative versus the standard treatment or IV t-PA alone.
Conclusion
Mechanical thrombectomy using the Solitaire stent-retriever device in combination with intravenous thrombosis with IV t-PA resulted in a dominant alternative (less costly, more effective) versus IV t-PA alone for the treatment of acute ischaemic stroke in patients with confirmed occlusions in the proximal anterior intracranial circulation and an absence of large ischaemic core lesions. It was a cost-effective option in all assessed scenarios from the Spanish NHS perspective.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AD was the recipient of an unrestricted grant from Covidien (currently Medtronic) for conducting REVASCAT trial. MAdM, TS and PC declare that there is no conflict of interest in this work. AG has provided services to Medtronic Ibérica, S.A. as a consultant. FdA-N and MAC are developing their professional activity in PORIB, a consultancy firm, which specialises in economic evaluation of health technologies, which has received economic funding by Medtronic Ibérica, S.A. to conduct this project. MA is currently employed by Medtronic Ibérica, S.A. The authors hereby declare that this economic support has not interfered with the development of this project. The authors state that the sponsor did not participate or influence the analysis of the present study or the interpretations of its results.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by Medtronic Inc.
Ethical approval
Not applicable.
Informed consent
No patients were recruited nor patient-level clinical data were used in this analysis.
Guarantor
Fernando de Andrés-Nogales.
Contributorship
FdA-N, MAC and MA researched literature and conceived the study. AD, MAdM, TS, AG and PC provided additional literature and validated the design and results of the model. FdA-N and MAC performed the analysis and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.