
Abstract
Introduction
Outcomes in stroke patients are improved by a co-ordinated organisation of stroke services and provision of evidence-based care. We studied the organisation of care and application of guidelines in two neighbouring health care systems with similar characteristics.
Methods
Organisational elements of the 2015 National Stroke Audit (NSA) from the Republic of Ireland (ROI) were compared with the Sentinel Stroke National Audit Programme (SSNAP) in Northern Ireland (NI) and the United Kingdom (UK). Compliance was compared with UK and European guidelines.
Results
Twenty-one of 28 ROI hospitals (78%) reported having a stroke unit (SU) compared with all 10 in NI. Average SU size was smaller in ROI (6 beds vs. 15 beds) and bed availability per head of population was lower (1:30,633 vs. 1:12,037 p < 0.0001 Chi Sq). Fifty-four percent of ROI patients were admitted to SU care compared with 96% of UK patients (p < 0.0001). Twenty-four–hour physiological monitoring was available in 54% of ROI SUs compared to 91% of UK units (p < 0.0001). There was no significant difference between ROI and NI in access to senior specialist physicians or nurses or in SU nurse staffing (3.9/10 beds weekday mornings) but there was a higher proportion of trained nurses in ROI units (2.9/10 beds vs. 2.3/10 beds (p = 0.02 Chi Sq).
Conclusion
Whilst the majority of hospitals in both jurisdictions met key criteria for organised stroke care the small size and underdevelopment of the ROI units meant a substantial proportion of patients were unable to access this specialised care.
Introduction
It is generally accepted that better organisation of stroke services results in better outcomes for stroke patients.1,2 Accordingly, modern stroke care is often highly structured, utilising models of care and protocols 3 derived from evidence-based guidelines.4–8 However, interpretation of guidelines and how they are implemented and thus consequent development of services may differ between health services. The island of Ireland is divided into two government authorities the Republic of Ireland (ROI) and Northern Ireland (NI), which is a component of the United Kingdom. Stroke services in each area have developed separately; the NI health service being a component part of the larger UK National Health Service (NHS) and the ROI being governed by the Irish Health Service Executive (HSE). In an analysis of the second Irish National Stroke Audit (2nd NSA) carried out in the Republic we compared services between the two jurisdictions in terms of resources provided and concordance with European and UK guidance, specifically with NI but with reference to the UK where NI data unavailable.
Methods
The 2nd NSA was performed in 2015 under the auspices of the Irish National Clinical Programme for Stroke Care (CPSC). 9 The audit was designed to collect data on patient care and outcome measures that were consistent with Irish National Guidelines and the previous iteration of the national audit in 2008. 10 It was also designed to allow comparison with other local European health systems. Data were collected in a format to permit comparison with published European Stroke Organisation (ESO) guidelines and recommendations.3,6 Due to the close proximity and similar healthcare structure, results were also compared with data from UK audits, both the seven UK Royal College of Physicians Audits 1998–201111,12 and the current continuous Sentinel Stroke National Audit Programme (SSNAP) which has operated since 2014 and data from which is published quarterly. SSNAP collects clinical data prospectively for every stroke patient along the stroke care pathway up to 6 months and includes a biennial acute organisational audit providing a view of the quality of stroke services in the acute setting. The UK and Ireland have very similar health systems in terms of organisation and medical training structures.
The 2nd NSA comprised of two components. The first was an organisational audit comprised of a questionnaire sent to senior administrators and lead stroke clinicians followed by an inspection visit by teams from the national programme consisting of senior specialist medical, nursing and therapy staff representing the CPSC to confirm and clarify reports provided. The second component was a chart audit of a representative sample of individual patients who had received acute stroke care in hospitals over two, 3-month periods 1 January 2014 to 31 March 2014 and 1 July 2014 to 30 September 2014. Chart audit was performed by medical, specialist nursing and therapy staff from each hospital with a superaudit of random chosen centres performed by staff from the CPSC to ensure consistency across sites. The tool was approved by an expert working group prior to dissemination, many of whom had been involved in prior national audits or audits in other jurisdictions. The tool was also reviewed by national quality assurance organisation and was trialled in four hospitals prior to final revisions and national dissemination. The audit was also conducted in association with an independent non-governmental organisation, the Irish Heart Foundation, to permit external scrutiny and validation of the process.
The organisational audit document included 46 core questions with multiple sub-sections relating to the structure, staffing and operation of the service. The chart audit document included 77 core questions to be completed for each subject. Each hospitals admitting 20 or more acute strokes (ICD, 10 codes: I61, I63 and I64, including sub-categories) in the previous year was requested to complete the organisational audit and hospital chart audit on between 25 and 40 consecutive patients admitted during the periods outlined, depending on the number of patients admitted.
Organisational data were compared with published Irish and ESO guidelines and SSNAP data published for NI and UK hospitals for the period April 2013 to March 2014. Patient data were also assessed for concordance with guidelines. Individual patient data was not available for NI for the time period in question and these results were compared with overall UK data. Collected NSA data was initially recorded on paper audit forms and all data were sent to an independent organisation for data entry and tabulation. SSNAP is published online at the organisation’s website. Quantitative results for the Irish and NI/UK audits were statistically evaluated and compared using relative risks (RR) and chi-square statistic to estimate scale of discrepancies and to compare proportions. In comparing staffing levels, chi squares were applied after converting ratios to proportions using the published total bed numbers.
Results
Data for 874 patients was audited in the ROI of 6035 total strokes (14.5%) admitted to Irish hospitals in 2014. These were compared with 74,307 in the UK SSNAP which collects prospective data on stroke admissions for England, Wales and Northern Ireland.
Twenty-seven hospitals in Ireland were found to have admitted 20 strokes or more in 2013 (median 177, range 56–412) and were audited. Twenty-one (78%) of these were found to have stroke units using the three core elements required by the European Stroke Organisation definition, that is a discreet area of a defined ward used exclusively for stroke, specialist medical, nursing and therapy staff and regular multidisciplinary team meetings. 3 This compared with 10 of 10 (100%) in Northern Ireland. One NI hospital that reported a 10-bed stroke unit used solely for care beyond 72 h and utilised a thrombolysis bypass process was excluded from our analysis, although acute stroke patients were potentially repatriated to the hospital earlier than 72 h on occasion. All remaining Northern Irish were self-categorised as combined units. In contrast, 10 of the ROI units categorized themselves as acute, the remained as combined. On inspection it was found that most of the acute units in the ROI also provided substantial post-acute care usually influenced by the availability of unoccupied rehabilitation beds to transfer patients to and the distinction between acute and combined units was unclear.
There were 152 stroke beds available for acute care across NI and 150 in ROI. The number of stroke beds per head of population (on 2011 census data from both areas) was 1 per 12,037 for NI and 1 per 30,633 for ROI, representing 2.5 times the number of acute beds per head of population in NI. This compares with 1:20,874 for the United Kingdom as a whole. Direct admission to a stroke unit/high dependency bed reported in 66% of patients in NI versus 40% in ROI and 75% in the UK as a whole (RR 2.4 (95% CI 2.3–2.5), UK vs. ROI). Fifty-seven percent of UK patients were admitted to the stroke unit within 4 h compared to 11% of patients in ROI (RR 2.0 (95% CI 2.0–2.1)). Fifty-four percent of patients in ROI received care in a stroke unit at sometime post-stroke compared to 96% of patients in the UK (RR 11.5 (95% CI 10.6–12.5)). Complete comparable data for stroke unit admission for NI was not available. All units in NI and ROI had multidisciplinary team meetings to review stroke patients’ care at least weekly.
Capacity for investigation, physiological monitoring and staffing within stroke units differed significantly between jurisdictions. Twenty-four hour CT imaging was available in all sites in ROI and 99% of sites in the UK including all sites in NI. However, capability for 24-h physiological monitoring was available in 54% of units in ROI compared to 91% of UK units (RR 5.1 (95% CI 4.7–5.5)).
Comparison of specialists managing stroke patients, ROI versus UK (chi square statistic)
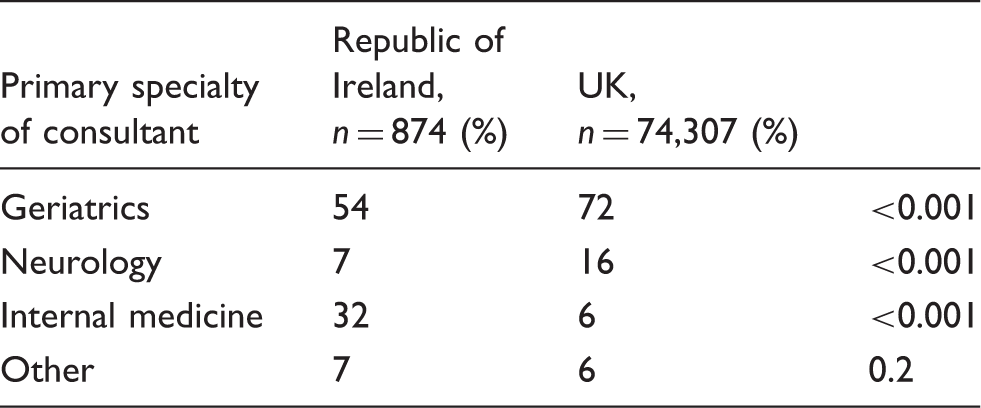
Note: n: number of patients.
Ratio of allied health professionals per 10 stroke unit beds.
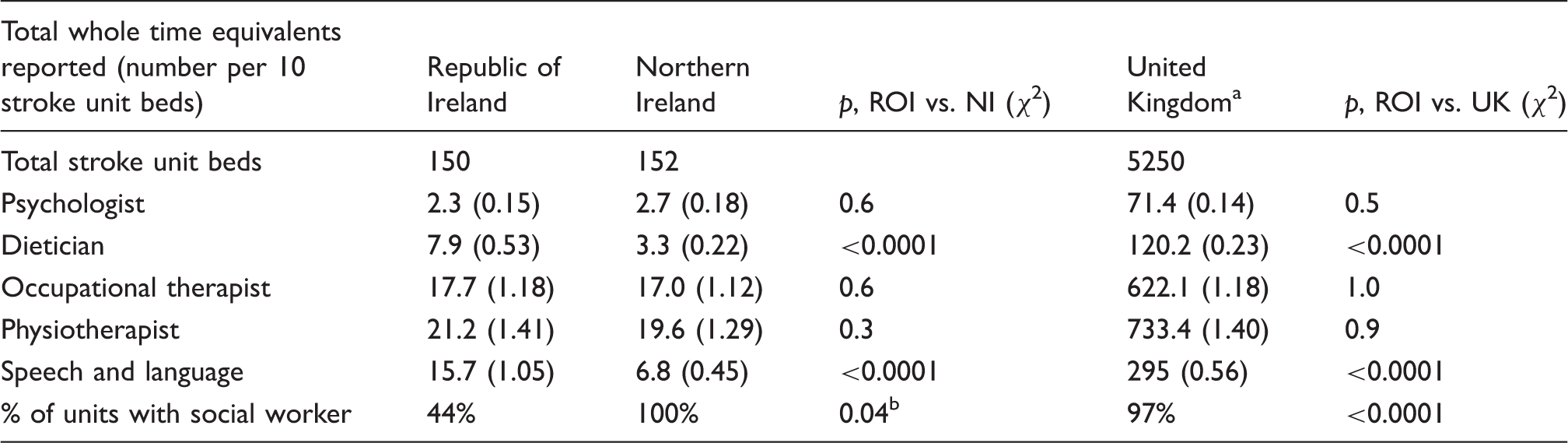
Including both Great Britain and Northern Ireland.
Fisher’s exact statistic.
All units had local ambulance arrangements for transfer of suspected strokes and pre-notification of Emergency Departments. Thrombolysis including redirect policy to intervention sites is available in 100% of sites in NI versus 96% in ROI, with a reported thrombolysis rate of non-haemorrhagic strokes of 15.1% (NI) versus 10.9% (ROI) (p = 0.3). Rates of intra-cerebral haemorrhage were 12.5% in NI versus 15.1% ROI (p = 0.5). Patients have access to early supported discharge (ESD) in 73% of NI sites compared to 15% in ROI, translating to 21% (65/312) of all discharged patients using an ESD service in NI versus 5% (41/743) in ROI (RR 3.8 (95% CI 2.6–5.5)).
There was no consistent means in differentiating outcomes between ROI and the UK. Inpatient mortality was not significantly different, ROI versus UK, 14% versus 15.8% (RR 0.9 (95% CI 0.1–1.1)). However, this may be influenced by the availability of home care and early supported discharge services between countries.
Discussion
Whilst the majority of hospitals in both Northern Ireland and the Republic of Ireland met key elements of the definition of stroke unit care there were significant deficits in staff levels in both countries. In the ROI whilst the majority of hospitals were found to have stroke units, the relatively small size of units and lower resource meant that a substantial proportion of patients were not able to fully access the specialised stroke care provided.
The study has some limitations. Data collection in the ROI audit was similar to previous UK Sentinel Audit methods, 12 that is physical auditing of patient charts. However, this differs from current SSNAP practice where data collection is online and thus less subject to bias from deficiencies in note keeping, data coding, etc. Charts were audited by local staff and whilst the audit group repeat audited charts in a number of randomly chosen hospitals, data collection errors may still have occurred. Errors may also have occurred in classification of stroke unit type. Some smaller hospitals in ROI were not included in the audit if they were subject to an ambulance redirect policy for stroke patients. These hospitals admitted less than 1% of all strokes in 2014 rending operation of effective stroke units or services impracticable. They were excluded from the analysis.
Units in ROI were frequently classified as acute however many of these units relied on off-site rehabilitation units for their patients and where delays in transfer were encountered many provided prolonged rehabilitation on-site leaving them closer in definition to combined stroke units. There were no dedicated onsite stroke rehabilitation units in ROI at the time of the audit. In NI, there is much clearer designation of acute and rehabilitation beds within combined stroke units on acute hospital sites. So it is likely that the number of beds available in acute services is overstated. Realistically not all beds, within large combined stroke units in particular, are able to manage patients in the early phase of their stroke. Whilst our intention was to compare data from ROI on patient care with NI and UK data, most NI hospitals were not recording care data routinely to SSNAP in 2014 which was not consistent with practice in the remainder of the UK.
A previous study has compared the management of stroke between cohorts of patients in two individual hospitals in the Republic of Ireland and Northern Ireland, 14 but these were not necessarily representative of stroke care nationally. We designed the study to enable us to collect data that would be suitable for comparison with both previous Irish National Audit data but also with ESO and UK data to allow us to determine the quality of organisation and care by international standards. Accordingly, the audit tools used were detailed and comprehensive including elements to permit comparison with ESO, UK and Irish guidelines which differ slightly in some elements. Self-reported organisational audits were validated by site visits conducted jointly by members of the CPSC audit team and clinicians nominated by the Irish Heart Foundation.
Our study demonstrates the challenges and difficulties in trying to implement evidence-based care for stroke patients. Guidelines in respect of acute interventions are typically strongly evidence based with support from randomised controlled trial data. 4 It is therefore easier to establish strict guidelines and thus measure against them. Whilst the evidence for stroke units is also strong and the components that represent stroke unit care are agreed,2,6 it is sometimes difficult to make an arbitrary call as to whether a hospital meets criteria or not. Both ESO and American Stroke Association guidelines3,15 have tried to address this by establishing different levels of stroke unit care based on criteria agreed using Delphi processes but conclusions based on such processes have limitations for example questions have been raised about the evidence in the ESO guidelines for having transcranial Doppler available 24/7? 3
The other issue is in resource allocation. At first glance there is little difference between Irish and UK facilities. Notwithstanding that all 10 sites in NI have stroke units versus 78% of sites in ROI, the ratio of nurse and AHP staffing to bed is not dissimilar. Nursing levels in both in ROI and NI were low compared with guideline recommendations. This is important because of the reported association between nursing levels and patient mortality recently reported from UK. 16
The significant difference between jurisdictions is in the numbers of properly staffed beds available to cater for case load. While acknowledging the practicalities of providing stroke unit care in hospitals that admit small numbers of stroke cases per year, there is little benefit in a hospital having a designated stroke unit if an individual cannot routinely expect to be admitted and cared for there. Furthermore, it is important to stress that there is a difference between stroke beds being available for admissions on site and the quality of access to these beds. Access is limited by fluctuations in acuity of stroke casemix, bed availability and staffing levels.
The CPSP was implemented in the Republic of Ireland at a time of the worst economic crisis in the history of the state. Over the period 2009–2013 health service funding was cut by approximately 20%, 17 so to have improved the organisation and delivery of stroke care to the extent it has was somewhat of an achievement. However, many of the changes were made by reallocating and re-designating resources and accordingly in many cases services have been developed that just bring them into line with the guidelines, that is the guidelines were used as a target and whilst they are specific as to the components of good stroke care, they mention little about extent of such care. It is important therefore that in further iterations of guidelines specific recommendations are included as a necessity to provide adequate beds within stroke units and that these beds be accessible by all patients who need them. In doing so we can help avoid the situation where health services and hospitals can achieve a level of compliance with guidelines but still be unable to provide adequate care for a large proportion of their population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was performed under the auspices of the Irish National Clinical Programme for Stroke and the Irish Heart Foundation. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
As a national audit conducted by a health service entity responsible for care quality, ethical approval was not deemed necessary for the Irish element. UK data were obtained through publically available published data.
Informed consent
No patient identifiable data were collected in either country and no additional procedures performed as part of the study thus informed consent was not required.
Guarantor
JH.
Contributorship
All authors were members of the Audit project team and contributed to the design and conduct of the study. PMcE, JMcC and JH wrote the paper. All other authors have reviewed and been given the opportunity to edit the paper.