
Abstract
Introduction
One third of patients with acute stroke have aphasia. The majority receive speech and language therapy. There is evidence for a beneficial effect of speech and language therapy on restoring communication, but it is unknown whether and how efficacy of speech and language therapy is influenced by timing of treatment. We studied whether speech and language therapy early after stroke by way of intensive cognitive-linguistic treatment is more effective than no speech and language therapy in the Rotterdam Aphasia Therapy Study-3, a multicentre randomised single-blind trial.
Methods and patients
Stroke patients with first-ever aphasia were randomised within 2 weeks of onset to either 4 weeks of early intensive cognitive-linguistic treatment (1 h/day) or no language treatment. Hereafter, both groups received regular speech and language therapy. Primary outcome was the score on the Amsterdam-Nijmegen Everyday Language Test, measuring everyday verbal communication, 4 weeks after randomisation. Secondary outcomes were Amsterdam-Nijmegen Everyday Language Test at 3 and 6 months. The study was powered to detect a clinically relevant difference of four points on the Amsterdam-Nijmegen Everyday Language Test.
Results
Of the 152 included patients, 80 patients were allocated to intervention. Median treatment intensity in the intervention-group was 24.5 h. The adjusted difference between groups in mean Amsterdam-Nijmegen Everyday Language Test-scores 4 weeks after randomisation was 0.39, 95% confidence interval: [−2.70 to 3.47], p = 0.805. No statistically significant differences were found at 3 and 6 months after randomisation either.
Conclusion
Four weeks of intensive cognitive-linguistic treatment initiated within 2 weeks of stroke is not more effective than no language treatment for the recovery of post-stroke aphasia. Our results exclude a clinically relevant effect of very early cognitive-linguistic treatment on everyday language.
Introduction
Aphasia occurs in about one third of stroke patients and has severe consequences for verbal communication and quality of life.1,2 Several randomised controlled trials (RCT) have reported a benefit of speech and language therapy (SLT) over no treatment for patients with aphasia due to stroke. 3 Hence, most patients receive SLT as part of their rehabilitation program.
The relationship between timing of SLT, i.e. the interval between stroke onset and start of treatment, and its efficacy is unclear. 4 In a meta-analysis comparing studies with different starting points of SLT, the average effect size in studies evaluating treatment initiated in the first 3 months after stroke was larger than that in studies performed in a later stage. 5 However, this analysis was mainly based on uncontrolled and non-randomised studies. The efficacy of early initiated SLT has been studied in four trials with contradictory findings; two large studies were neutral, two smaller suggested an effect of early treatment.6–9 The need for more research on the effect of timing of SLT was explicitly accentuated in a Cochrane Review on efficacy of SLT for post-stroke aphasia. 10
In the early phase after stroke, impairment-based cognitive-linguistic treatment (CLT) is often preferred over other types of SLT, as it targets specific linguistic functions supposedly stimulating functional neural networks.11–13 As most recovery occurs within the first 3 months after stroke,5,14–16 standard practice early after stroke often comprises CLT. 17 When linguistic performance reaches a plateau, SLT may be continued with compensatory treatment instead of CLT.
There is some evidence suggesting that high-intensity treatment may be more effective than less frequent therapy.3,18,19 However, the feasibility of high-intensity treatment is questionable, as in several trials compliance with treatment was significantly lower in intervention groups with intensive language treatment. 3
Experts in language rehabilitation suggest a best-practice regime of early initiated intensive CLT.13,17 Scientific evidence underpinning this recommendation is frail. The objective of the Rotterdam Aphasia Therapy Study (RATS)-3 was to study whether early intensive CLT for 4 weeks is more effective than no language treatment in the first 4 to 6 weeks after stroke, and whether this approach generates a long-lasting benefit.
Methods
Essential elements of the study design are described below. Detailed methods were published elsewhere and are provided as online Appendix 2. 20
RATS-3 is a prospective multicentre controlled clinical trial with randomised treatment allocation, open label treatment and blinded evaluation of the primary outcome measure (PROBE-design). Fourteen regional networks for integrated stroke care across the Netherlands participated (online Appendix 1). Within 2 weeks of stroke onset, patients were randomised to 4 weeks of either intensive CLT or no language treatment. After 4 weeks, both groups received regular SLT.
The study protocol was approved by the Medical Ethical Committee of the Erasmus MC (MEC-2005-347) and the study was registered in the Netherlands Trial Register (NTR3271).
Participants
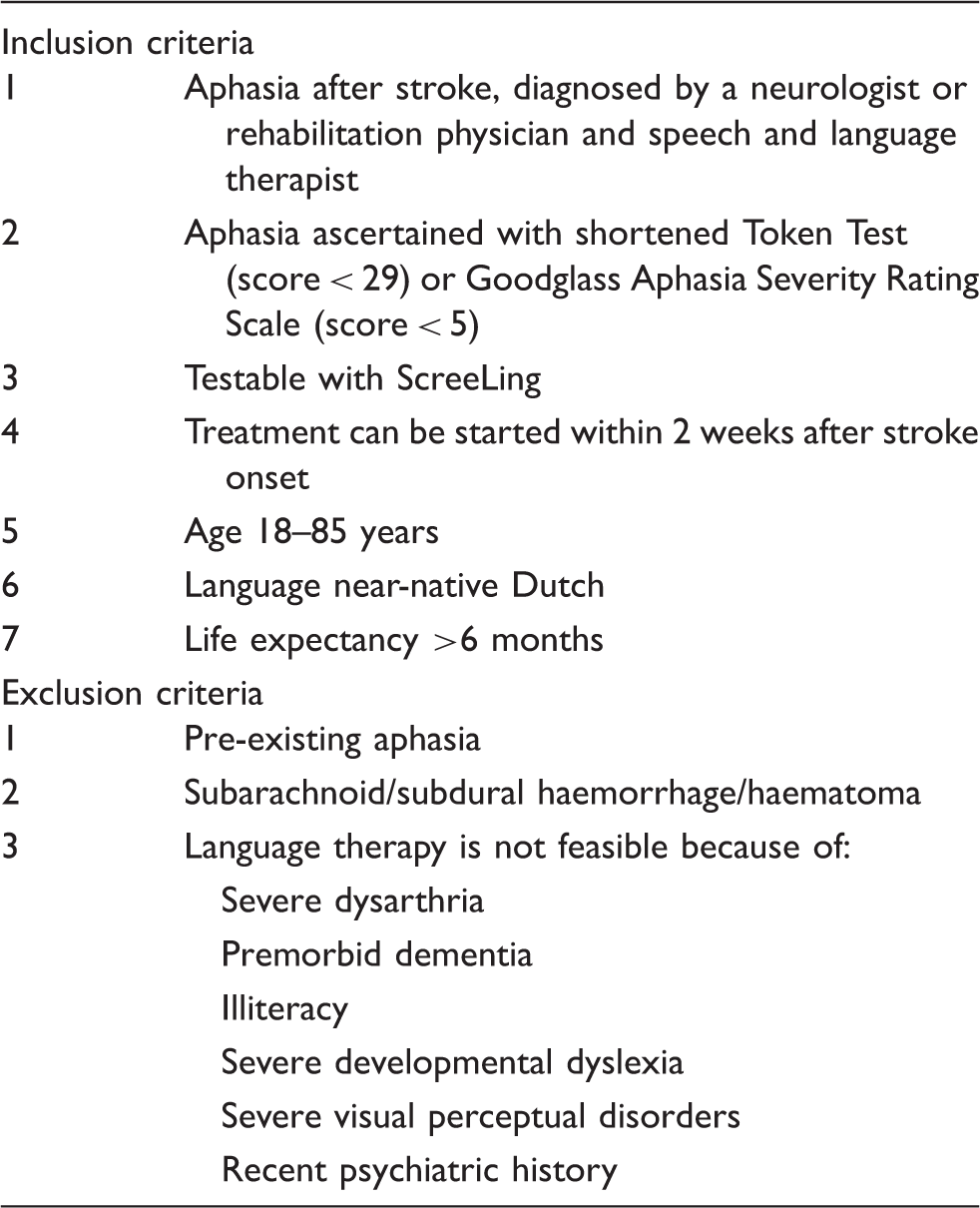
Eligibility criteria for RATS-3.
Randomisation
The trial-coordinator verified inclusion criteria and, after written informed consent was obtained, included and randomised participants within 2 weeks of stroke onset. Independent trial-assistants concealed computer-generated allocation sequences in consecutively numbered, opaque, sealed envelopes. Randomisation was stratified according to baseline aphasia severity (Aphasia Severity Rating Scale: ASRS-score 0–2 = severe; ASRS-score 3–4 = moderate/mild) and including centre.
Baseline tests
At baseline, a short test battery was conducted including the ScreeLing, the 36-item Token Test and a semi-standardised interview for eliciting spontaneous speech, which was rated with the ASRS. 20 An experienced SL-therapist blinded to treatment allocation classified the spontaneous speech samples as fluent or non-fluent. Baseline characteristics and the Barthel Index were recorded, as well as treatment with intravenous alteplase, as this is associated with rapid recovery from stroke. 21
Intervention
Patients in the intervention-group were to receive at least 1 h of CLT every day of the week for a period of 4 weeks. The hour of treatment could be delivered in more than one session per day, if preferable. We chose an intervention period of 4 weeks for three reasons. First, intervention in the control-group had to reflect usual care in the Netherlands, where SLT for aphasia starts on average 3 to 6 weeks after onset. Second, we specifically aimed to study the effect of early initiated treatment. With a maximal inclusion period of 2 weeks and a 4-week intervention period, this early phase was not exceeded. Last, we expected that a longer intervention period with high intensity would be too burdensome for many patients. Treatment was directed at semantics using the therapy program BOX 22 and/or phonology using the therapy program FIKS 23 to improve word finding deficits. Participating SL-therapists had ample experience in using both Dutch therapy-programs and carefully selected exercises for face-to-face treatment and homework, registered as part of the total amount of treatment provided. The control-group received no language treatment during the first 4 weeks after randomisation. Minimal counselling was allowed, aimed at preventing communication problems and included elaborate information about aphasia and providing communication advice. Concise diagnostics for therapy goal setting was allowed also. The trial-coordinator had at least two-weekly contact with the SL-therapists to ensure no treatment was provided in the control-group and to monitor compliance in the intervention-group. After 4 weeks, further SLT was left to the discretion of the local SL-therapist in both groups.
Assessments
An extensive linguistic test-protocol was conducted at three time-points; 4 weeks, 3 months and 6 months after randomisation, with the following tests for language and communication: Amsterdam-Nijmegen Everyday Language Test (ANELT) for everyday functional verbal communication, 24 a semi-standardised interview from the Aachen Aphasia Test (AAT) rated with the reliable and valid ordered categorical six-point ASRS, the ScreeLing, the Token Test and the Boston Naming Test. The battery also included tests for semantic processing: Semantic Association Test (SAT), verbal version; Comprehensive Aphasia Test (CAT), word comprehension; and Category Fluency; and for phonological processing: Nonword repetition and Auditory Lexical Decision from the Psycholinguistic Assessment of Language Processing in Aphasia (PALPA) and Letter Fluency. In addition, we assessed general functional outcome with the EQ-5D-3L for quality of life, and the modified Rankin Scale (mRS) and Barthel Index for level of independency.
Outcomes
Primary outcome was the ANELT A-score ‘understandability’ (range: 10–50, higher scores equal better performance), measuring the adequacy of verbal communication, 4 weeks after randomisation. This valid and reliable test was chosen to verify whether the impairment-based CLT generalises to everyday communication. 24 All ANELTs were audio-recorded and rated by two independent assessors, blinded to intervention and time-point. The mean of these two scores was used for analyses. Secondary outcomes were scores on the linguistic tests, EQ-5D-3L and mRS at 4 weeks, and scores on the ANELT-A, the linguistic tests, EQ-5D-3L, and mRS at 3 and 6 months after randomisation.
Sample size
We considered a four-point difference between both groups on the ANELT-A a clinically worthwhile treatment effect. This is 50% of the critical difference for individual improvement and half a standard deviation of average ANELT-A scores in previous RATS trials.24–26 We estimated that a sample of 150 participants would provide 84% power to find a statistically significant treatment effect at a 5% two-sided significance level.
Statistical analyses
Primary analyses were performed on intention-to-treat basis. In addition, on-treatment analyses were performed, with on-treatment being defined for the intervention-group as having accomplished at least the intended intensity of 28 h in 4 weeks and for the control-group as having received no language treatment during 4 weeks after randomisation. We used linear regression to analyse the treatment effect as a mean difference in ANELT-A scores between the intervention and control-group 4 weeks after randomisation, adjusted for age (years), sex, education (high or low), baseline aphasia severity (ASRS-score), type of stroke (ischaemic or haemorrhagic), location of stroke (right or left hemisphere) and baseline Barthel Index score. Linear regression was also used to analyse the effect of treatment on the specific linguistic measures and measures of general functional outcome at 4 weeks, 3 months and 6 months after randomisation, with the same adjustments as in the primary analysis. For the ordered categorical variable mRS, we used multivariable ordinal logistic regression. Post-hoc subgroup analyses were performed with the variables used for baseline-adjustment (online Appendix 3). The results were combined with available evidence from previous trials on early aphasia treatment in a meta-analysis (online Appendix 4).
Results
Baseline characteristics of participants in RATS-3.
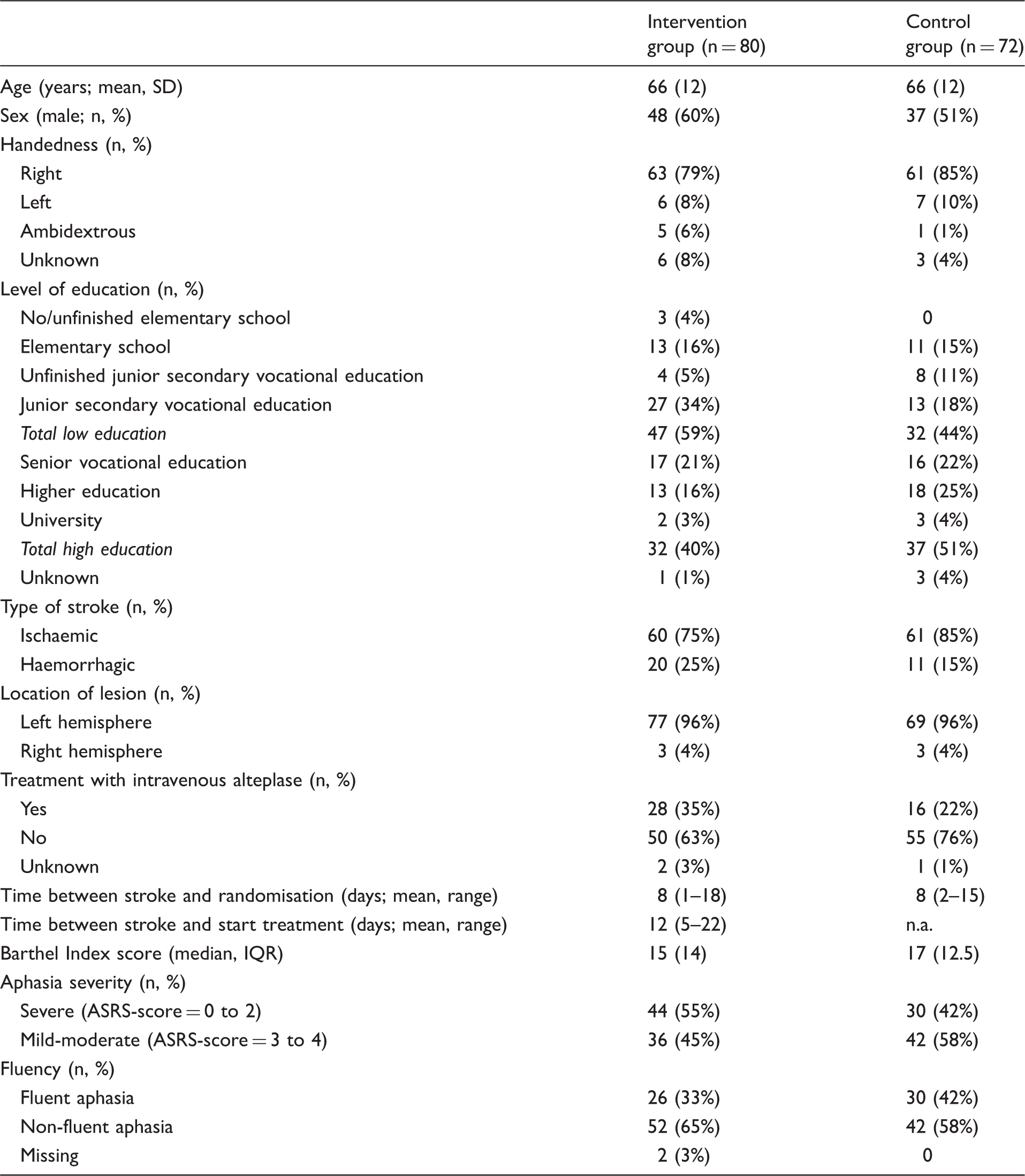
SD: standard deviation; n: number; IQ: Interquartile Range; ASRS: Aphasia Severity Rating Scale; n.a.: not applicable.
In the intervention-group, two patients died in the intervention period, and in the control-group, one patient died in the intervention period and one just afterwards, before testing could be performed (Figure 1). During follow-up, in each group two patients died. Five participants from the intervention-group did not receive the allocated treatment; one was very ill and four refused intensive treatment. In the control-group, 10 participants refused deferred treatment and received regular SLT. The trial-coordinator did not interfere with treatment, and details on the content of SLT provided to these patients were not recorded.
Flow-chart Rotterdam Aphasia Therapy Study-3.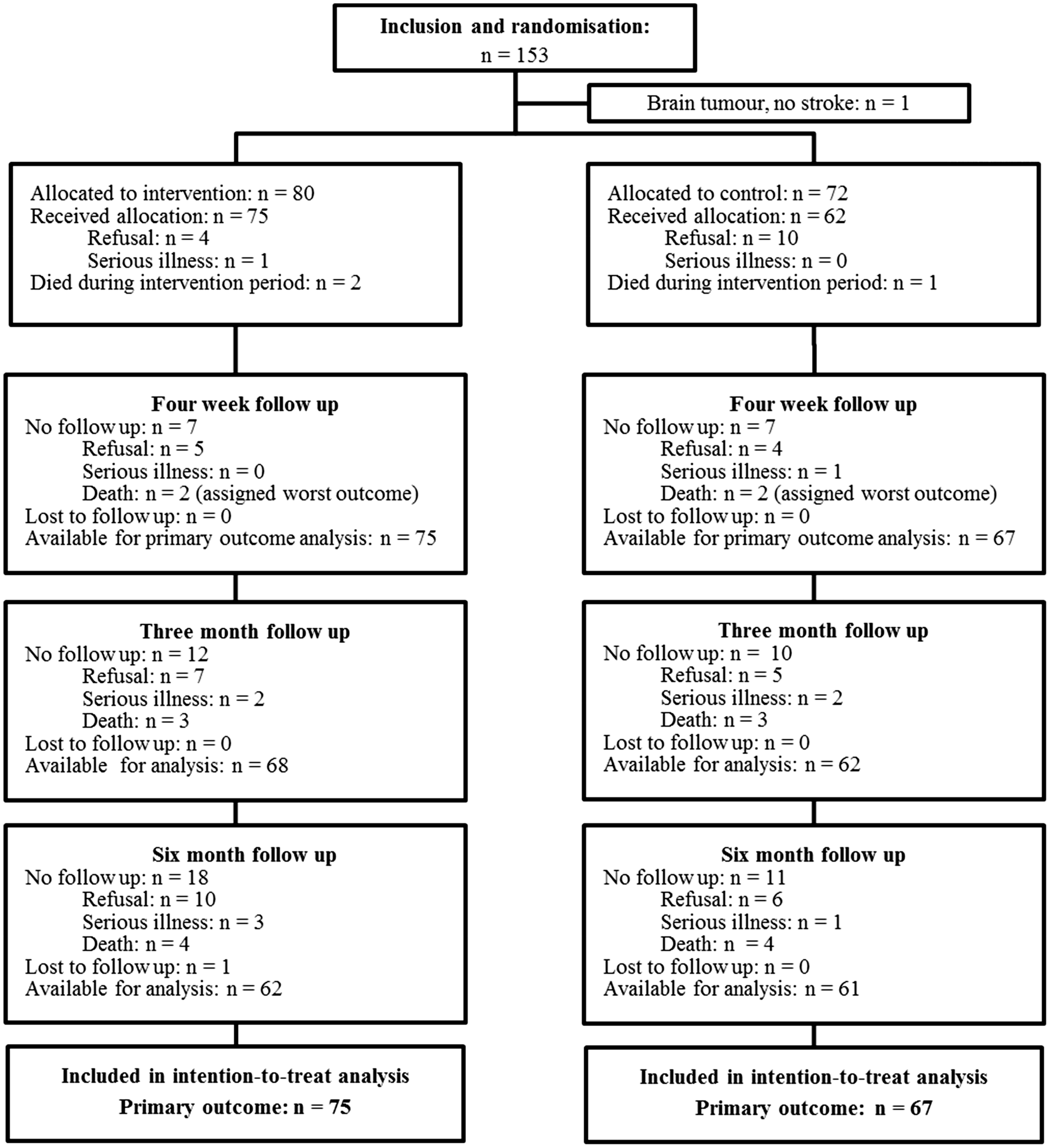
Compliance
A treatment intensity of 28 h in 4 weeks in the intervention-group was achieved by 23 of 80 patients (29%). The median treatment intensity was 24.5 h in 4 weeks (IQR: 9.5) (Figure 2).
Distribution of treatment intensity in the intervention group (total number of hours in 4 weeks).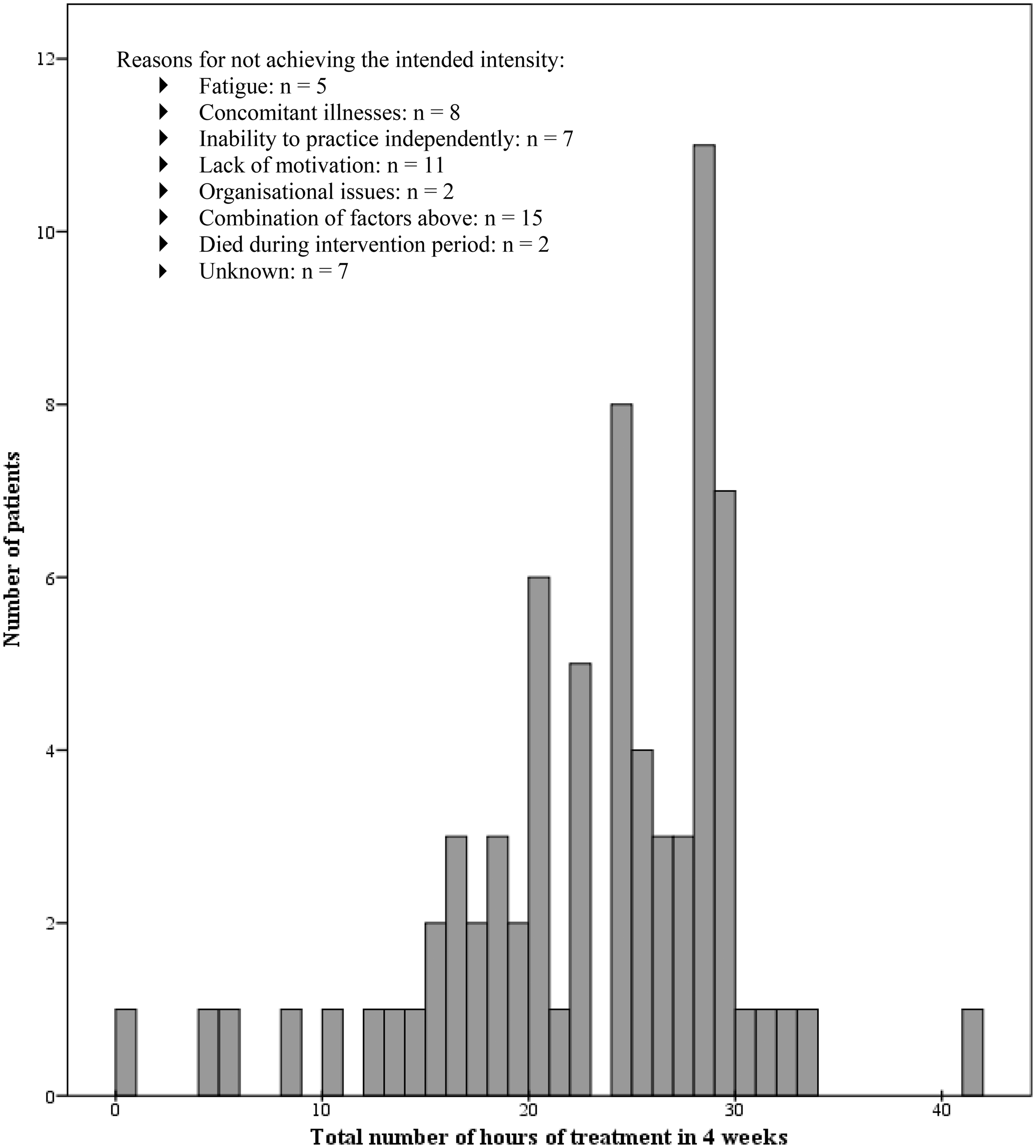
Intention-to-treat analysis
The mean score on the primary outcome, the ANELT-A at 4 weeks, was 33.2 in the intervention-group and 36.2 in the control-group, with a difference of −3.01; 95% confidence interval (CI): [−7.15 to 1.14]. Baseline aphasia severity and baseline Barthel Index were strong prognostic factors in the regression model (online Table 3). The adjusted mean difference in scores on the ANELT-A was 0.39; 95% CI: [−2.70 to 3.47], p = 0.805 (Figure 3). There were also no statistically significant differences on the ANELT-A between groups at 3 months (adjusted difference = 0.54, 95% CI: [−3.04 to 4.12], p = 0.767) and 6 months (adjusted difference = −0.41, 95% CI: [−3.70 to 2.89], p = 0.807) after randomisation (Figure 3).
Differences in outcome and treatment effect between intervention and control on the ANELT-A. 95%CI: 95% Confidence Interval; ANELT: Amsterdam-Nijmegen Everyday Language Test; unadj. diff: unadjusted differences *) Statistically significant at a 95% confidence level ◊) Primary outcome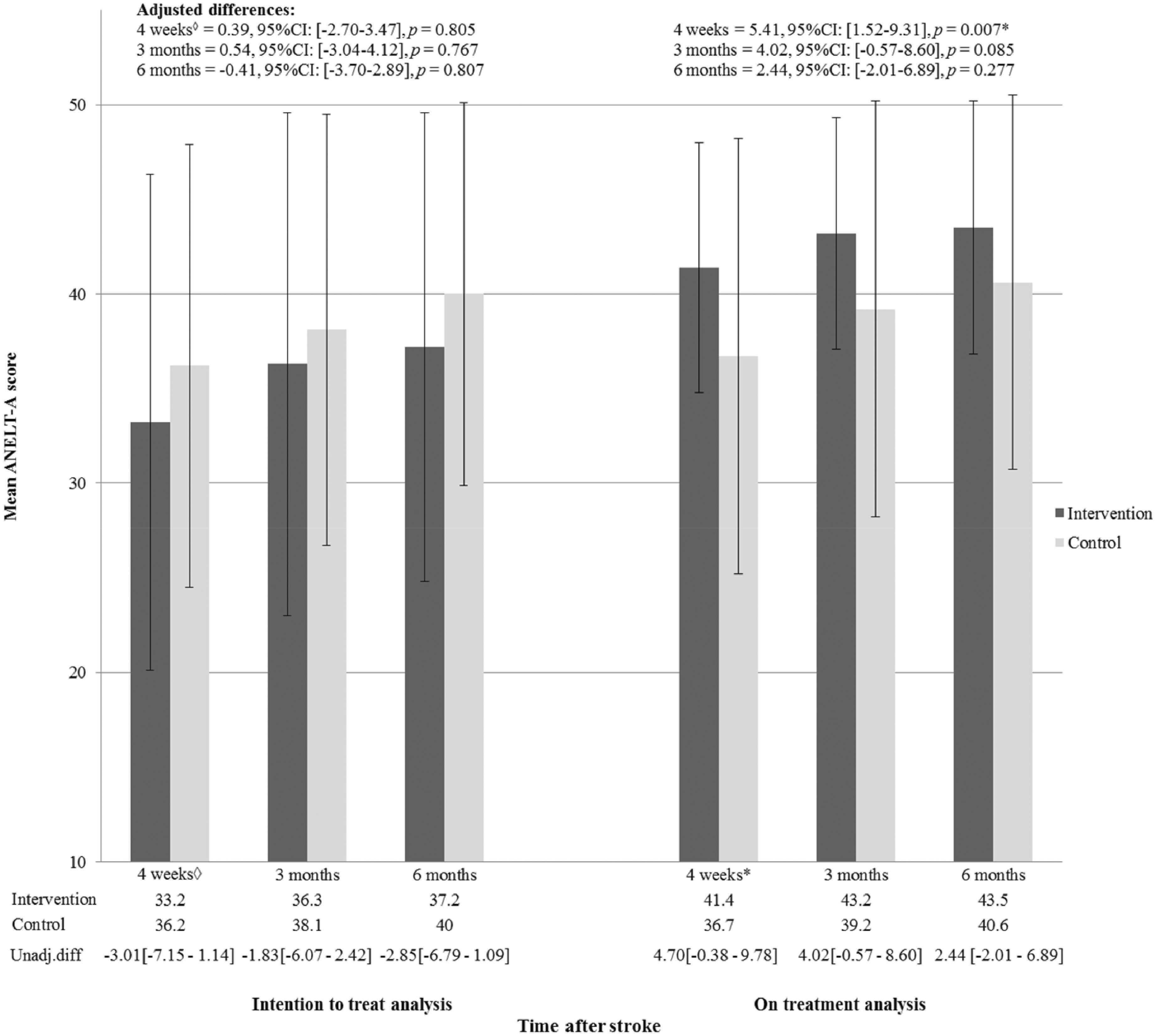
No statistically significant treatment effects were observed on the linguistic tests and on the measures for general functional outcome, at any time-point (online Table 4). Post-hoc subgroup analyses are provided as online Appendix 3. The meta-analysis showed no beneficial effect of early SLT (online Appendix 4).
On-treatment analysis
In the on-treatment analysis, we included all patients of the intervention-group who received at least the prespecified intensity of 28 h in 4 weeks (n = 23, 29%) and all subjects in the control-group who did not receive any treatment (n = 62, 86%). Baseline characteristics of the intervention and control-group included in the on-treatment analyses were similar (online Table 5).
When on-treatment criteria were applied, the intervention-group reached significantly higher scores than the control-group after 4 weeks on the primary outcome ANELT-A (adjusted difference = 5.41, 95% CI: [1.52 to 9.31], p = 0.007); SAT verbal (adjusted difference = 3.57, 95% CI: [0.36 to 6.78], p = 0.030) and CAT word comprehension (adjusted difference = 3.64, 95% CI: [0.58 to 6.69], p = 0.020) (Figure 3, online Table 6). On all other outcome measures and time points, results did not differ from those of the intention-to-treat analyses.
Discussion
Principal findings
In this multicentre RCT in 152 patients with aphasia due to stroke, we found that 4 weeks of early intensive CLT did not result in better everyday verbal communication than no early language treatment. The 95% CIs for the adjusted differences between groups did not include the pre-specified clinically relevant difference of four points on the ANELT-A, which allows us to conclude that early intensive CLT is not effective.
This contradicts the findings from two smaller RCTs in which a benefit of early intensive treatment was reported. In 59 patients, 30–80 min of impairment-based SLT per workday for 4 weeks initiated 3 days after stroke improved communication more than usual care (<80 min per week). 7 Although nearly 20% of the patients in the intervention-group did not achieve the minimum treatment intensity of 150 min per week, the authors conclude that daily treatment is feasible early after stroke and, if tolerated, is effective for recovery of aphasia. In another study, 12 patients were randomly allocated to 2 weeks of either 1-h sessions of impairment-based SLT on workdays starting on average 2.2 days after stroke or no SLT. 8 In addition to statistically significant better scores on the AAT subparts Naming and Written language processing in the early treatment group, the authors report significant differences between groups in post treatment recruitment of brain areas on functional MRI scans. However, this is a very small trial with only six participants per treatment-arm.
Our findings are in line with those from two larger RCTs on early initiated SLT. In a trial among 123 patients, Laska et al. found no effect of 3 weeks of early intensive impairment-based SLT on ANELT-A scores 3 weeks and 6 months after stroke onset. 6 Bowen et al. randomly allocated 170 stroke patients with communication deficits to either agreed best-practice SLT or social support provided by trained volunteers for 16 weeks starting on average 2 weeks after stroke onset. 9 They found no differences regarding functional communication at follow-up and conclude that SLT is not more effective than social support. This trial differs from ours, as stroke patients with either aphasia, dysarthria or both were included, which makes the results difficult to interpret. Furthermore, treatment intensity was tailored to the individuals’ needs and possibilities. Consequently, treatment intensity was on average only 1.5 h per week, which may not have been sufficient to reach a sizeable treatment effect.3,18,19
While the concept of early language rehabilitation after stroke is attractive, the summary of evidence in our meta-analysis shows that SLT, whether or not intensive, when started within 4 weeks after stroke onset, is not more effective in improving verbal communication or language functioning, than regular, less intensive or deferred treatment.
Strengths and weaknesses
Strengths of RATS-3 are its large size, multicentre design, a clearly defined clinically relevant intervention contrast, and representative cohort of patients with post-stroke aphasia. The treatment programs used in the intervention-group are frequently applied in daily practice in the Netherlands and have good potential to generate an effect on language recovery, as exercises are directed at facilitating word finding, an essential problem in aphasia. Consequently, results of our trial are highly generalizable to daily practice. We could have opted for a more distinct intervention contrast by actively limiting all language-related activities in the control-group, e.g. reading, writing and computer use, but that would not reflect daily reality. In fact, our aim was to study whether intensive CLT, added to language-related activities people with aphasia engage in naturally, is effective for the recovery of aphasia.
Many efficacy studies on impairment-based treatment have used impairment-based language tests as outcome measures, e.g. naming or word-comprehension, as these are closely related to the intervention being studied. 27 However, scores on linguistic tests are rather artificial and do not necessarily reflect adequate functional communication in daily life, which should be the ultimate goal of aphasia treatment. 3 Therefore, a relevant and reliable measure of communication, most closely reflecting the patients’ sense of recovery and return to normal functioning, is preferable. 10 Hence, in line with our previous trials, both in which we found that improvement on the ANELT-A was correlated with improvement at the impairment level, we used the ANELT-A as primary outcome measure.16,25,26
Our study has limitations. Although we accomplished a high median treatment intensity of 24.5 h in 4 weeks, achieving the intended intensity of 28 h appeared a major challenge. Even with a strictly protocolled treatment regime and highly motivated SL-therapists who were frequently contacted by the trial-coordinator, less than 30% of the intervention-group achieved the requested intensity. Patients were often too tired or ill to practise 1 h per day, even if treatment was spread over the day. Although poor adherence to the protocol was mainly caused by patient-related issues, organisational problems such as limited availability of therapists, or priority given to motor rehabilitation also played a role, albeit minor. Although this trial was no feasibility study, the results demonstrate that even if intensive treatment had been found more effective for selected patients, feasibility is improbable for all stroke patients with aphasia early after onset. This is in line with findings from the most recent Cochrane review. 3
Patient selection seems essential to generate a potential beneficial effect of early intensive CLT on recovery of aphasia, as the on-treatment analyses did show a limited effect. However, this finding should be interpreted with great caution, as on-treatment analyses could only be performed in patients in the intervention-group who could tolerate intensive treatment, whereas the control-group comprised both patients who may and may not tolerate this intensive regime.
Completeness of follow-up for the primary outcome was 93%, which is in line with other studies in this field. 3 At 6 months after stroke, 19% of participants had refused follow-up testing. This may have reduced the validity of our findings, but the measurements at 3 and 6 months follow-up are secondary outcomes and are in line with the primary outcome.
Implications
Despite the lack of unequivocal proof for a beneficial effect of early SLT, deferring treatment in aphasia due to stroke has long been considered unethical. 28 However, early after stroke, patients may suffer from concomitant illnesses or fatigue and may not tolerate intensive impairment-based treatment. Our findings demonstrate that it is not detrimental to delay CLT in the first weeks after stroke onset in these vulnerable patients, which also occasionally happens unintentionally due to waiting lists or lengthy diagnostic pathways.
However, our findings do not justify the conclusion that the work of SL-therapists is redundant in the first weeks after stroke, as patients with aphasia and their proxies definitely need guidance and help in coping with their deficits early after stroke. In times of radical changes in health care policy and budget cutbacks, SL-therapists are urged to utilise their limited resources effectively for patients with acute stroke. Instead of focusing on impairment-based treatment, they might better put more emphasis on counselling and providing communication support, which are essential for coping with communication problems and prevention of social isolation. CLT may be more effective later in the course of this disabling condition.
Future research
Future studies should aim to find the optimal timing of commonly used treatment types, either impairment-based or functional approaches. New studies may be focussed on patient selection also, as results from our on-treatment analyses indicate that some patients might benefit from early intensive treatment. International cooperation is one way to conduct large aphasia trials that allow for more reliable pre-specified subgroup analyses, which is of great importance to identify factors contributing to treatment success and may enable individualisation of SLT.
Conclusion
Our study shows that 4 weeks of intensive CLT aimed at semantic and phonological processing started within 2 weeks after stroke onset does not improve the recovery of aphasia, either in the short or long term.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE Form for Disclosure of Potential Conflicts of Interest (available on request from the corresponding author) and declare no competing interests. LL has received a fellowship of the Brain Foundation Netherlands. DD, PK, EV and FN are employees of the Department of Neurology of the Erasmus MC. This department has received grants from Zawabas Fund, Coolsingel Fund, Dura Fund, Blokland Fund and the Erasmus MC Care Research Fund for conducting this trial.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RATS-3 was funded by a fellowship granted to LL by the Brain Foundation Netherlands (project number: 2011(1)-20) and grants from Zawabas Fund, Coolsingel Fund, Dura Fund, Blokland Fund and the Erasmus MC Care Research Fund. The funding sources of RATS-3 had no role in study design, data collection, data analysis, data interpretation or writing of the report. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Ethical approval
Ethical approval for this study protocol was obtained from the Medical Ethical Committee of the Erasmus MC (MEC-2005-347).
Informed consent
Written informed consent was obtained from all participants or their next of kin before inclusion in the study.
Trial registration
The study protocol for this randomised controlled trial was registered in the Netherlands Trial Register (NTR3271).
Guarantor
FN is guarantor and takes responsibility for the accuracy of the manuscript.
Contributorship
RATS-3 was conceived by EV, DD, LL, PK and MS. LL was principal investigator of this trial and FN was trial-coordinator. FN primarily acquired and analysed the data. SG and DB were local principal investigators of centres that recruited more than 10% of the study population and critically reviewed the manuscript. HL and FN conducted statistical analyses. EV, MS, DD, PK, LL, HL and FN interpreted the data. All data and statistical analysis reports were available to all authors. FN drafted the first version of the manuscript. All authors critically read and revised the manuscript. The final version of the manuscript was approved by all authors.
Acknowledgements
We thank Marjolein de Jong-Hagelstein and Carolina Mendez Orellana for contributing to the conception and outset of RATS-3. We acknowledge all participating centres in the Netherlands for recruiting patients and treating them according to the trial protocol. We are thankful to Irma Adbegovic, Liset Bergevoets, Yvonne Hendrick, Nienke Wolthuis and Marjolein Zomerdijk for their work as blinded ANELT assessors.
Data sharing
Anonymous data can be requested from the corresponding author with a detailed description containing the aims and methods of the study for which the data are intended to be used. Data will be contributed to the project titled: ‘REhabilitation and recovery of peopLE with Aphasia after StrokE’ (RELEASE) funded by the National Institute of Health Research in the UK (NIHR). Informed consent was not obtained from participants for data sharing, but the data will be anonymised and risk of identification is low.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.