
Abstract
Introduction
The overall aim of the present study was to explore perceived life satisfaction in persons with stroke, from admission to specialised rehabilitation until follow up 1 year post-discharge. The secondary aim was to evaluate possible external and internal explanatory factors for perceived life satisfaction.
Patients and methods
A prospective, descriptive study of specialised rehabilitation of persons with stroke. Persons with a primary diagnosis of stroke were enrolled in the study.
Results
Overall, total score on LiSat-11 showed that life was perceived as satisfying by 11% on admission, 21% at discharge, 25% at 6 and 31% at 12 months after discharge from rehabilitation, reported by 230 participating persons with stroke. Repeated measurement indicated significant differences of total life satisfaction between clinics, also when controlled for disability and severity. The items “sexual life,” “health,” and “vocational life”/“financial” were most dissatisfying at the various reported time points. The linear regression analysis revealed an equal amount of internal and external explanatory factors at the different time points, explaining between 16% and 41% of the variations.
Discussion and conclusion
The perceived life satisfaction was reported as low/dissatisfying at the four stated time points in all the participating clinics. Four items were especially vulnerable post-stroke: vocational situation, sexual life, physical health and mental health. Both internal and external factors contributed to life satisfaction, such as gender, severity of stroke, marital status, country, models of rehabilitation, occupational status, length of stay (LOS), number of therapies and hours in therapy. However, there were significant differences between clinics, indicating that unidentified factors may also influence life satisfaction.
Introduction
Improvements in rehabilitation and medical interventions have significantly decreased mortality for persons with stroke. 1 Consequently, it has become important to evaluate the quality of life (QoL) of individuals who have survived a stroke event using outcome metrics other than mortality. One important aspect of QoL is life satisfaction. Life satisfaction is described as an emotion; having an optimistic attitude to one’s life as a whole. Overall life satisfaction comes from within, based on the individual’s personal values and the relationship between aspirations and achievements. 2 It is also related to internal factors, such as to what extent basic needs are met or how a person experiences a sense of coherence; that is, to what extent is life experienced as comprehensible, manageable and meaningful.3–5 In addition, life satisfaction also depends on external socio-cultural factors such as personal finance, the environment, access to social and health services, the current political system and cultural influences.6,7 Both external and internal aspects are dynamic and may change or develop with different goals, needs, time and/or context.
Culture, identified as a global influencing factor, directs the attention to different sources of information with which to judge life satisfaction, thus affecting subjective appraisal. 8 It has been argued that individualistic cultures direct attention to inner states and feelings, such as positive or negative emotions, while in collectivistic cultures the attention is directed to outer sources, that is, adhering to social norms or fulfilling one’s duties. 8
The present study examines life satisfaction after surviving a severe stroke and receiving specialised rehabilitation in one of nine different clinics in seven countries. Such a study was possible through the ongoing Sunnaas International Network (SIN) stroke study, a multinational comparative study on the components of specialised stroke rehabilitation in nine clinics in Norway, PR China, the United States, Russia, Palestine, Israel and Sweden. 9 The characteristics of the specialised rehabilitation units in the different clinics, the therapies provided and the respective principles for admission and discharge have been described earlier. 10 Specialised rehabilitation was found to differ between the clinics, in both staffing, admission and discharge routines, length of stay in hospital/clinic (LOS) and therapies provided. Nevertheless, all the clinics admitted severely disabled persons with stroke and provided therapies and care that improved physical impairments and activities, although the magnitude and duration of their effects differed. 10
Objective
The overall aim of the present study was to explore perceived life satisfaction in persons with stroke, from admission to specialised rehabilitation until follow up 1 year post-discharge. The primary aim was to elucidate the similarities and differences in perceived life satisfaction between the nine different clinics, and to examine possible changes in perceived life satisfaction in a longitudinal perspective. The secondary aim was to evaluate possible external and internal explanatory factors for perceived life satisfaction. External factors are defined as country/culture, models of rehabilitation and societal influences. Internal factors are defined as personal and contextual factors.
It was hypothesised that persons with a newly acquired stroke would report only a low level of satisfaction with life. Furthermore, both internal and external factors were hypothesised to influence life satisfaction, and it was expected that internal factors could be influenced by rehabilitation. That means that improved function and increased independence would lead to improved perceived life satisfaction.
Methods
Design
The design was a prospective, descriptive study of specialised rehabilitation of persons with stroke. The study was registered in Clin Trials Gov: NCT 01732679.
Subjects
Persons with a primary diagnosis of stroke, as defined by the World Health Organization (WHO) were consecutively enrolled in the study from September 2012 to September 2014. 11 Inclusion criteria were that the patients had a severe first-time stroke, defined as a Modified Rankin Scale (mRS) score 3–4, were in need of specialised rehabilitation post-stroke and participated voluntarily. Patients with subarachnoid haemorrhage, malignancy, or other severe medical conditions in combination with stroke were excluded.
Outcome measures
Descriptive data of patients with stroke admitted for inpatient rehabilitation to the participating hospitals were obtained from medical records.
Perceived satisfaction with life was evaluated according to the generic Life Satisfaction Checklist (LiSat-11). 12 The LiSat-11 entails one global item and ten domain specific items capturing life satisfaction. LiSat-11 may be self-administered or used as an interview tool, rated on a six-step ordinal scale ranging from very dissatisfying (=1) to very satisfying (=6). In the present study, LiSat-11 was used in a one-to-one interview between tester and patient. The scale has been tested for reliability and validity, and related normative data exist for the Swedish population aged 18–74 years 12 and also for patients seen as medical rehabilitation cases for chronic pain, 13 acquired brain injury, 14 spinal cord injuries 15 and stroke. 16 Results are categorised as “satisfied” for scores ranging from 5 to 6 and “dissatisfied” for scores ranging from 1 to 4. 12 LiSat-11 may be divided into four gender-independent descriptive domains; closeness (sexual life, partner relationship and family life); health (ability to care for self/activities of daily living (ADL), physical health and mental health); spare time (leisure, contact with friends and acquaintances); and provision (vocational and financial situations). 12 The LiSat-11 items are considered separately but in this study a total score, summarising all item scores ranging from 1 (dissatisfied) to a maximum of 66 (satisfied) was added. 17
Performance in the ADL was evaluated with the Barthel Index (BI) or the Functional Independence Measure™ (FIM), as used in the clinic. FIM can be divided into motor (FIM-M) and cognitive (FIM-C) components.18,19 FIM was originally developed to address issues of sensitivity and comprehensiveness discovered in the use of the BI. Subsequent studies have demonstrated that the psychometric properties of FIM and BI are similar. 20 Thus, a dichotomisation of FIM-M scores to lower (0–55) and higher scores (56–91), comparable to BI 0–59 and 60–100 (19), has been used for all time points. The degree of disability and severity of stroke were evaluated with the modified Rankin Scale (mRS) and the National Institute of Health Stroke Scale (NIHSS), on admission and at discharge from the inpatient rehabilitation units.21,22 Four assessment sessions were performed: on admission, at discharge and then at 6 and 2 months after discharge from the specialised rehabilitation clinics.
Statistical analysis
All the analysis was performed using SPSS, version 23. Descriptive statistics were used to identify patients’ demographics, and test results were given in percentages and mean with standard deviation (SD). A correlation analysis between item “life as a whole” and the total score was performed to establish associations.
Repeated measurements were performed with a general linear model to analyse possible differences between clinics and models of rehabilitation in perceived life satisfaction on the different time points. Disability and occupational status were entered as covariates. A Bonferroni correction was used for interactions in comparison for main effects and confidence intervals adjustments. To evaluate explanatory factors for life satisfaction a standard linear regression analysis was performed. LiSat-11 items, with low and significantly different scores, were consecutively entered as dependent variables. Age, gender, marital status, occupational status; working/not working, country, medical condition, NIHSS, mRS, ADL, models of collaboration; intra-, multi- and inter-disciplinary models, length of stay, number of different disciplines of rehabilitation per day and hours in therapy; time in respective therapy in hours/minutes were entered as independent variables to establish explanatory internal and external factors. The significance level was set at p < 0.05 and, where a Bonferroni correction was used, to p < 0.01.
In addition, logistic regression analyses were performed with “life as a whole” and total score at discharge as dependent variables, coded as unsatisfactory from 1 to 3, satisfactory from 4 to 6. Age, gender, marital status, occupational status, country, medical condition, NIHSS, mRS, ADL, models of rehabilitation, length of stay, amount of therapy and hours in therapy were used as independent factors for the evaluation of predictors for outcomes.
Ethics
Approval of the local ethical committees in each country was obtained in 2012, including from the Regional Ethics Committee of Health South-East in Norway (2012/768). Information on the aim of the study was given to the participants both verbally and in writing, and written informed consent was obtained.
Results
Demographics at baseline in the various settings: Sunnaas, Norway, China Rehabilitation Research Center, China, Rusk Institute, US, Policlinica 2, Russia, Sheba medical, Israel, Bethlehem Arab Society Rehabilitation, Palestine, El Wafa, Gaza, Högsbo-Sahlgrenska university Hospital, Sweden and Sichuan Bayi, China.
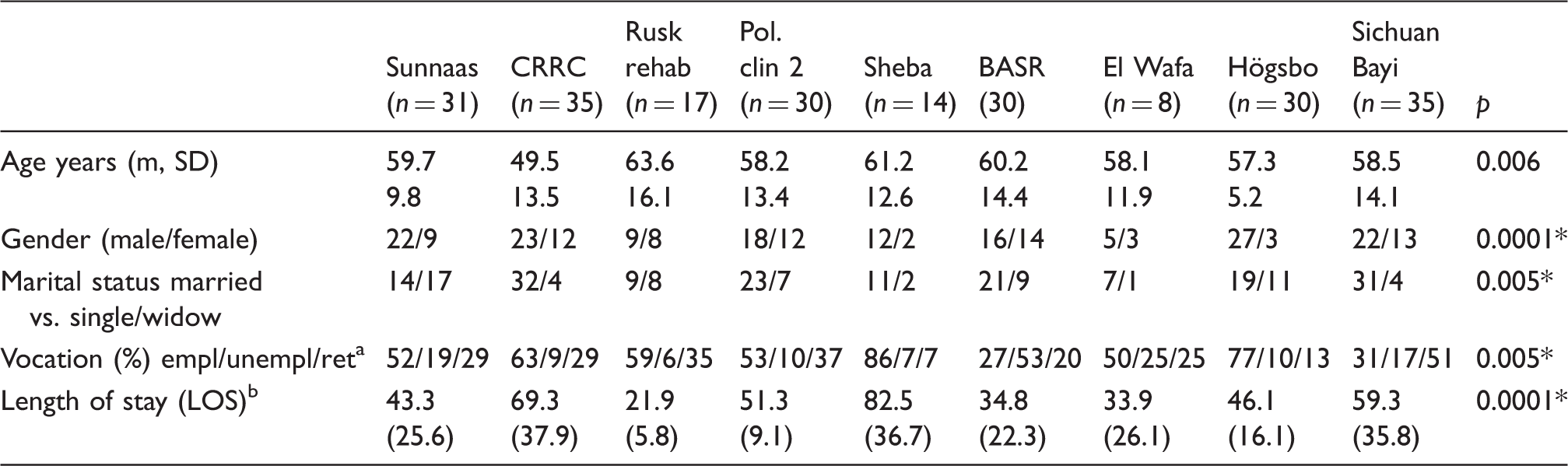
Note: Significance with a Bonferroni correction p < 0.005.
Employed/unemployed/retired.
LOS presented in days.
Life satisfaction for the whole sample presented in percentages.
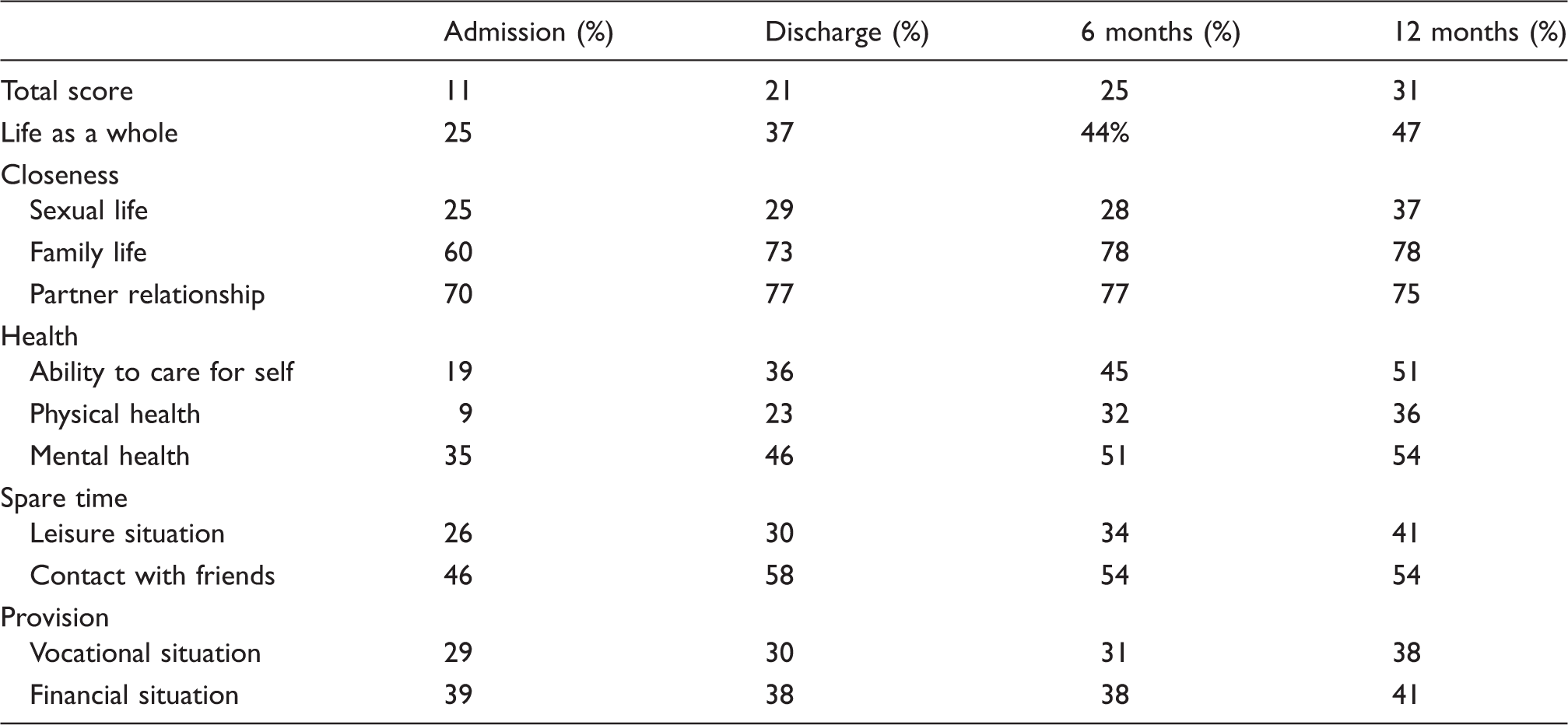
Note: LiSat-11 items divided into the domains: closeness, health, spare time, and provision, according to Melin, 28 on admission, discharge, 6 and 12 months after specialized stroke rehabilitation. In addition, the first item in LiSat-11, ‘Life as a whole’, and total score, the summing up of all items, are presented separately.
In the domains closeness, health, spare time and provision, it was found that provision was perceived as least satisfactory, whereas closeness was rated highest. The items “sexual life” (closeness), “mental health” (health) and “vocational life”/“financial” (provision) were most dissatisfying at the various reported time points, with significant differences between them, looking at the sample as a whole.
The percentage of satisfaction in light of the principal items of LiSat-11 on admission (adm) and at 12 months post-discharge (pd).
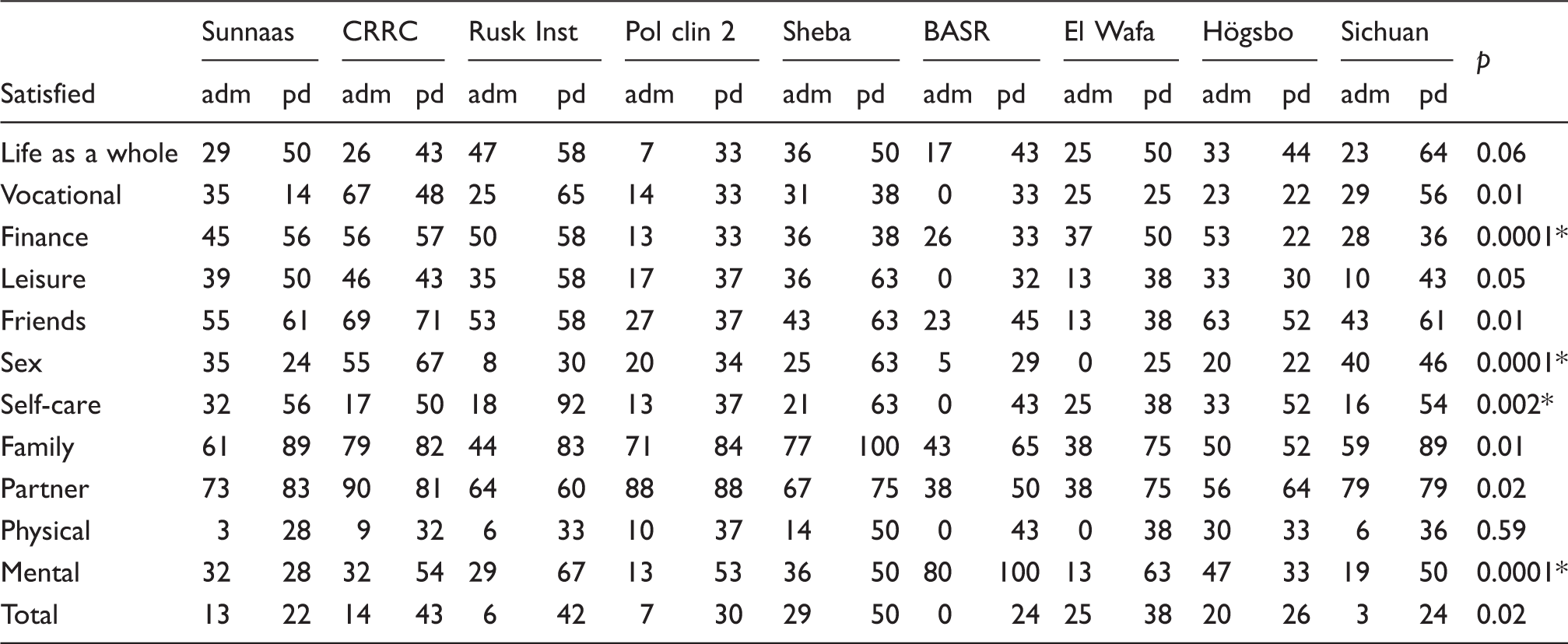
Note: Significant differences are given for repeated measures of the respective items between clinics with a Bonferroni correction.
p < 0.005.
Regression models of internal and external explanatory factors for the LiSat-11 items scored least satisfactorily over time: vocational, financial, sexual, physical and mental at discharge, 6 and 12 months post-discharge, p < 0.05.
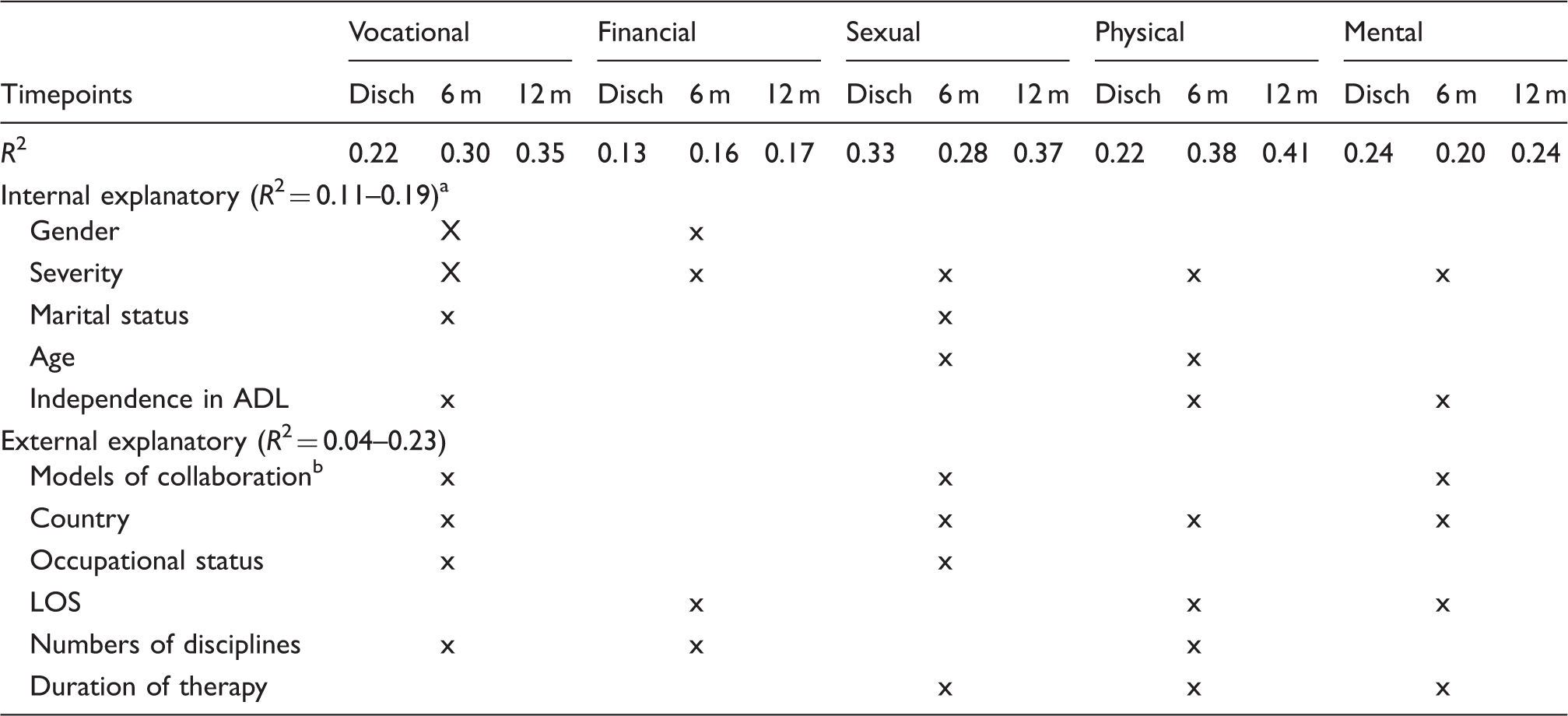
Note: LOS: length of stay.
Internal and external explanatory factors that contributed to variations over time within brackets, p < 0.05 (x).
Intra-, multi- and inter-disciplinary collaboration models.
Logistic regression models indicated stroke severity (NIHSS total score) with an odds ratio of 1.2 (95% CI = 1.1–1.3) as the primary predictor for LiSat-11 total and Life as a whole score, predicting 17–28% (χ2 = 36.4, p < 0.0001) and 19–26% of the variation (χ2 = 36.2, p = 0.0001), respectively.
Discussion
The perceived life satisfaction of persons with severe stroke was scored as low/dissatisfying in the majority of the items during and after specialised rehabilitation. Vocational satisfaction, sexual life physical health and mental health had the highest percentage of individuals reporting dissatisfaction irrespective of the diversity of the clinics. 20 These findings are in line with other studies and underline the global aspect of low satisfaction with life after brain injury.6,23,25 Viitanen et al. 16 found that 61% of long-term stroke survivors had decreased general and/or domain-specific satisfaction with life compared to two reference groups of the healthy elderly. Low satisfaction was mainly reported with life as a whole, sexual life, leisure and ability to perform activities of daily life. 16
Life satisfaction and independence in functional activities
Lower health-related quality of life (HRQoL) or satisfaction with life may also be related to functional capacity, as persons with lower functioning ability often report a lower QoL 26 and satisfaction with life 27 than persons better able to perform. In this respect, a certain hierarchy exists. Significant impacts on the physical and mental domains of generic HRQoL have been reported to be the result of stroke severity, disability, gender, social support and having had a previous stroke. 18 Four items in LiSat-11 (vocational situation, sexual life, physical health and mental health) were perceived as especially vulnerable post-stroke, reflecting complex disability in the patients in the participating specialised rehabilitation clinics (Tables 2–3). However, it may also reflect that the rehabilitative efforts not sufficiently target patient participation in order to optimise self-efficacy, coping and strategies for functioning.
Life satisfaction and time post-stroke
The longitudinal progression indicated stable, slightly improved life satisfaction in the items “life as a whole,” “financial situation,” “leisure,” “contact with friends and acquaintances,” “family life,” and “mental health.” This development may be explained by adaptation to the new situation, indicating a relatively uniform process, although significant differences were found between the clinics, due to circumstances and development.
Satisfaction with “life as a whole” was reported to be low but stable (50/50) post-discharge. However, some clinics reported lower scores 30/70, indicating differences that may be explained by external factors (Table 3). The tendencies in the longitudinal profile were similar in the total score, but the latter indicated lower total life satisfaction (Table 3). In addition, the association between the two was moderate to good, indicating that the overall life satisfaction item and the total score with 10 items only overlapped partially.
Life satisfaction and vocational situation
Results for the item “vocational situation” indicated that work-related outcomes after stroke continued to be unsatisfactory in the majority of the participating clinics, possibly explained by lack of co-operation or difficulties in co-operating between social and medical/health services. Return to work is often the primary aim of rehabilitation. 28 This imposes requirements on existing social services, employers and the possibilities for adaptations to the workplace and vocational training post-stroke and needs collaboration in the rehabilitation team as well as with the social services. In addition, many of those with stroke who were included were retired, varying from 7% to 50% in the various clinics, though mean age was below retirement age in each of the countries (Table 1). Thus, health issues may have been present before the first stroke occurred, making it even more difficult to return to work.
Life satisfaction and financial security post-stroke
In some countries, persons with stroke were dependent on their families or spouses for financial support, which could put a strain on the family situation. We might have speculated that countries with more comprehensive disability benefits would report higher financial satisfaction, and those countries without such benefits or in a situation of crisis would report lower financial satisfaction post-stroke. However, “financial situation” was reported as dissatisfying in all the clinics, although the participating countries had wide cultural differences, differences in social policies and health insurance systems. Differences reported seemed to be connected with external factors, like work opportunities and other social security measures.
Life satisfaction and intimacy
All responders reported that satisfaction with “sexual life” was very low, and although improving slightly over time it remained low compared to studies with other diagnoses. 15 Thus, this finding confirms that stroke seems to affect sexual life more frequently than other neurological disabilities do. 6 In a recent qualitative study of sexuality 5 years after stroke, Nilsson et al. 29 found that some patients experienced decreased sexual interest and function, attributed to sensory difficulties, pain or fatigue, while others expressed a positive change in sexual life, enjoying more intimacy despite physical difficulties. Open communication with their partners and time were significant factors in the coping process. 29 Furthermore, opportunities for patients to discuss issues of sexuality with healthcare professionals are limited, although there has been an expressed need for such opportunities to be provided.
Poor health, low physical functioning and dependency, all internal factors, may have an effect on partnership and on sexual life. 30 Therefore, one may speculate that efforts in rehabilitation should ideally be made to improve services so that both couples and single persons with stroke can meet future challenges in a constructive and positive way in recovery after rehabilitation.
Life satisfaction and self-efficacy
The item “ability to manage self-care” clearly supported the positive development in and outside rehabilitation in the direction of improved functioning and independence in a longitudinal aspect, independent of cultural differences, and in line with many studies on rehabilitation after stroke.30,31 Nevertheless, it also confirmed that life after rehabilitation is not back to life as it used to be, but necessitates changes and adaptation, that is, coping. Given the individual and dynamic construct of perceived life satisfaction, it is important to enroll the individual with stroke and their families early in rehabilitation to ensure self-efficacy and the best possible outcome from rehabilitation.
Persons with stroke reported dissatisfaction with “contacts with friends and acquaintances” and their “leisure situation.” This may relate to physical health and dependence in ADLs, but also to external factors like opportunities to participate in different activities, offered services and possibilities, transport to and from leisure venues and ease of accessibility. 31 Other important factors can be related to psychological health such as co-morbidities, depression and anxiety. In addition, changes in self-esteem or self-confidence, gender roles, feelings of stigmatisation and attitudes in the patient’s social network may contribute to reduced psychological health.
Both internal and external factors contributed to explaining the results for the categories provision (vocational, financial), closeness (sexual life) and health (physical and mental health items) (Table 4). The significant differences in reported life satisfaction between clinics suggest that other, unidentified factors may influence life satisfaction such as the dynamic aspects of life concerning time and goal orientation.
Possible cultural differences
The participating clinics varied in size of the institutions, and number of personnel, collaboration models employed and methods/approaches used in rehabilitation. 10 It has been suggested that models and time-intensity in therapy have a positive effect on rehabilitation outcomes in specialised rehabilitation. 32 However, on the one hand, the explanatory values of these external aspects on life satisfaction were insignificant and small at 4–6%. On the other hand, internal factors, like gender, occupational status, severity of stroke and independence in ADLs influenced and explained life satisfaction to a much higher degree, 17–64%. These results indicate and support the need for specialised rehabilitation to improve ADLs and lessen the impact of stroke severity as well as improving life satisfaction. Furthermore, it supports an item-by-item use when choosing the LiSat-11 checklist for clinical care and in research work.
To determine to what extent individualistic cultures influenced the results, here possibly defined as the Western versus the Eastern more collectivistic cultures, there were no clear divisions. Family, friends and to a certain extent partners were related to higher reported life satisfaction in the majority of clinics, indicating a strong position for positive effects irrespective of individualistic versus collectivistic culture. In addition, in the majority of clinics, patients reported dissatisfaction with sexual life, indicating negative effects universally.
LiSat-11 – The checklist as tool
The name “LiSat-11” checklist may give the impression of being just a “reminder” of questions to go through in a conversation with patients. According to its definition, a checklist is a type of informational job aid used to reduce failure by compensating for potential limits of human memory and attention. It helps to ensure consistency and completeness in carrying out a task. The LiSat checklist has expanded from 8 to 11 items and ranks the levels of satisfaction. It may be argued that it is an outcome measure rather than a checklist, 33 and as such LiSat-11 can be and are used in research as well as in clinical care to complement the identification and exploration of important domains in the life of the patient.
Limitations
There are limitations to the present study. The sample size is small in some of the participating clinics. Persons with stroke admitted to specialised rehabilitation have a severe disability, are younger than the general population of stroke and there were more men than women included in the study. The interpretation and generalisation of results to the average post-stroke population must therefore be made with caution. However, the unique contribution from the clinics in several countries gives a useful insight into rehabilitation for stroke under varied circumstances. Strength of the study is the close collaboration that existed between the included countries with workshops, meetings and new techniques for discussion and communication, thus making it possible to work with a complicated design.
Conclusion
The overall aim of the present study was to explore life satisfaction in persons with severe stroke in need of specialised rehabilitation, using the instrument LiSat-11; from admission to specialised rehabilitation to 1-year post-discharge. The perceived life satisfaction was scored as low/dissatisfying in the majority of the domains at all four measured time points in all participating clinics. Four items were especially likely to be seen as unsatisfactory post-stroke: the vocational situation, sexual life, physical health and mental health. Both internal and external factors contributed to life satisfaction, such as gender, the severity of stroke, marital status, country, models of rehabilitation, occupational status, LOS, number of therapies and hours in therapy. However, there were significant differences between clinics, indicating that unidentified factors may also influence life satisfaction.
Footnotes
Acknowledgements
We would like to thank all the patients in the respective centres for their participation in this study. We also would like to thank our research personnel: Anne Marthe Sanders, Li Chao Jinzi, David Gordon, Nathalie Jenkins, Yael Amzallag, Deng Wanying and Linda Johansson for their help with the data collection. Furthermore, we are grateful to our contact persons, Arkady Rutgayzer and Edmund Shehadeh, for valuable help with the study. The SIN stroke group includes the following authors: Åsa Lundgren-Nilsson, Department of Clinical Neuroscience, Faculty of Medicine, University of Gothenburg, Göteborg, Sweden; Tong Zhang, Neurorehabilitation Department, China Rehabilitation and Research Center, Beijing, China; Tamara Bushnik, Department of Rehabilitation Medicine, Rusk Institute, New York, USA; Maria Panchenko, No2 Policlinica, Petrozavodsk, Karelian Republic, Russia; Ofer Keren, Sheba Medical Hospital, Tel Aviv, Israel; Samir Banura, Betlehem Arab Society Rehabilitation (BASR), Betlehem, Palestine; Khamis Elessi, El Wafa, Gaza, Palestine; Deng Wanying, Sichuan Bayi Rehabilitation Center, Chengdu, Sichuan, China
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the respective clinics concerning personnel for the intervention and testers. Project investigator and technical assistant were funded by Sunnaas Rehabilitation Hospital. The Norwegian Research Council and Sunnaas Rehabilitation Hospital co-funded group meetings.
Ethical approval
Approvals of the local ethical committees in each participating country were obtained in 2012, including from the Regional Ethics Committee of Health South-East in Norway (2012/768). The trial was registered in Clin trials gov.: NCT01732679.
Informed consent
Written informed consent was obtained from all subjects before the study.
Guarantor
BL.
Contributorship
Birgitta Langhammer was involved in concept, design, drafting of manuscript, analysis and interpretation of data. Katharina S Sunnerhagen, Johan K Stanghelle, Susanne Sällström, Frank Becker, Kerstin Fugl Meyer were involved in interpretation of data, drafting and critical revision. SINs group was involved in collection of data, discussion and interpretation of data. All authors reviewed and edited the manuscript and approved the final version of the manuscript.