
Abstract
Introduction
Endovascular treatment of acute ischemic stroke is more effective when performed quickly. In this report, we describe quality interventions to ensure fast endovascular treatment times in the ESCAPE (Endovascular Treatment for Small Core and Anterior circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times) trial.
Methods
An “audit and feedback” intervention using webinar and letter was used to improve treatment time over the course of the trial. The time metrics were computed tomography-to-groin-puncture (target < 60 min) and computed tomography-to-first-reperfusion (target < 90 min). Each site was provided with their data for computed tomography-to-groin-puncture and computed tomography-to-first-reperfusion for all their patients that were randomized to the treatment arm, and their median time was compared to the overall median times of all sites in the trial. We assessed for changes in treatment time over the course of the trial.
Results
There were 165 patients enrolled into the endovascular arm from 22 sites. The computed tomography-to-groin-puncture time dropped from 57 to 47 min (p = 0.14) while computed tomography-to-reperfusion time dropped from 89 to 81 min (p = 0.48). Over the course of the trial, the absolute treatment benefit increased by 7.8% (p < 0.001).
Conclusions
An “audit and feedback” intervention throughout the conduct of the ESCAPE trial was a feasible way to ensure fast treatment times. Quality improvement processes should continue as standard practice beyond the trial to encourage good patient selection and the best clinical outcomes.
Keywords
Introduction
Endovascular treatment for acute ischemic stroke has been shown to be beneficial compared to usual care.1–4 In the ESCAPE (Endovascular Treatment for Small Core and Anterior circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times) trial, quality improvement measures to ensure efficient workflow were established from the outset. 5 As fast reperfusion has been shown to result in better outcomes,6–8 efficient workflow and fast treatment9,10 were required in ESCAPE; study sites only enrolled patients when the pre-set benchmarks could be met: (1) qualifying non-contrast CT (computed tomography) to groin puncture of 60 min or less and (2) CT to reperfusion of 90 min or less. The time of the first slice of the non-contrast brain CT scan was used as the start time. 11
Because efficient workflows are difficult to enforce in a large multi-center international trial and in an effort to maintain adherence to these criteria, the ESCAPE trial had a structured quality assurance process to ensure that these benchmarks were being met. The purpose of this report was to describe the use of a quality improvement process within an endovascular stroke trial and to assess the impact of our quality assurance processes to maintain or improve the efficiency of workflow.
Methods
An “Audit and feedback” intervention design 12 was used to maintain treatment times during the course of the trial. We set targets of median CT-to-arterial access time of 60 min and median CT-to-reperfusion time of 90 min. A supportive coaching approach led by the trial principal investigators was used. Our audit and feedback intervention was comprised of a webinar (Adobe Connect, Adobe Systems, San Jose, CA) immediately followed by an email to feedback data generated for each site during the course of the trial. All site investigators and sub-investigators involved in the enrollment of patients into the trial were invited to the webinar. The webinars were 30-min in length, interactive and included a short presentation of each site’s own interval time data and a comparison with the median performance of the entire trial. The webinar was followed by discussion of strategies to maintain and improve treatment times. Treatment time feedback included a comparison against the overall median treatment times across all centers. Some sites did not complete the audit and feedback intervention because the number of patients they enrolled was small (<2 in the treatment arm), which was because the site became active in the trial late or the hospital served a small catchment area. There was a site visit conducted with each site prior to the site enrolling patients, which provided detailed instruction on efficient CT-to-groin-puncture and CT-to-reperfusion workflow.
After each webinar, key messages and action plans linked to strategies for performance improvement were provided in a letter and emailed to each of the site personnel along with their performance summary. Figure 1 shows an example of detailed feedback. A similar process was undertaken to improve the quality of patient selection by imaging.
Site performance slide that was shared during the webinars, and emailed with a letter to the sites.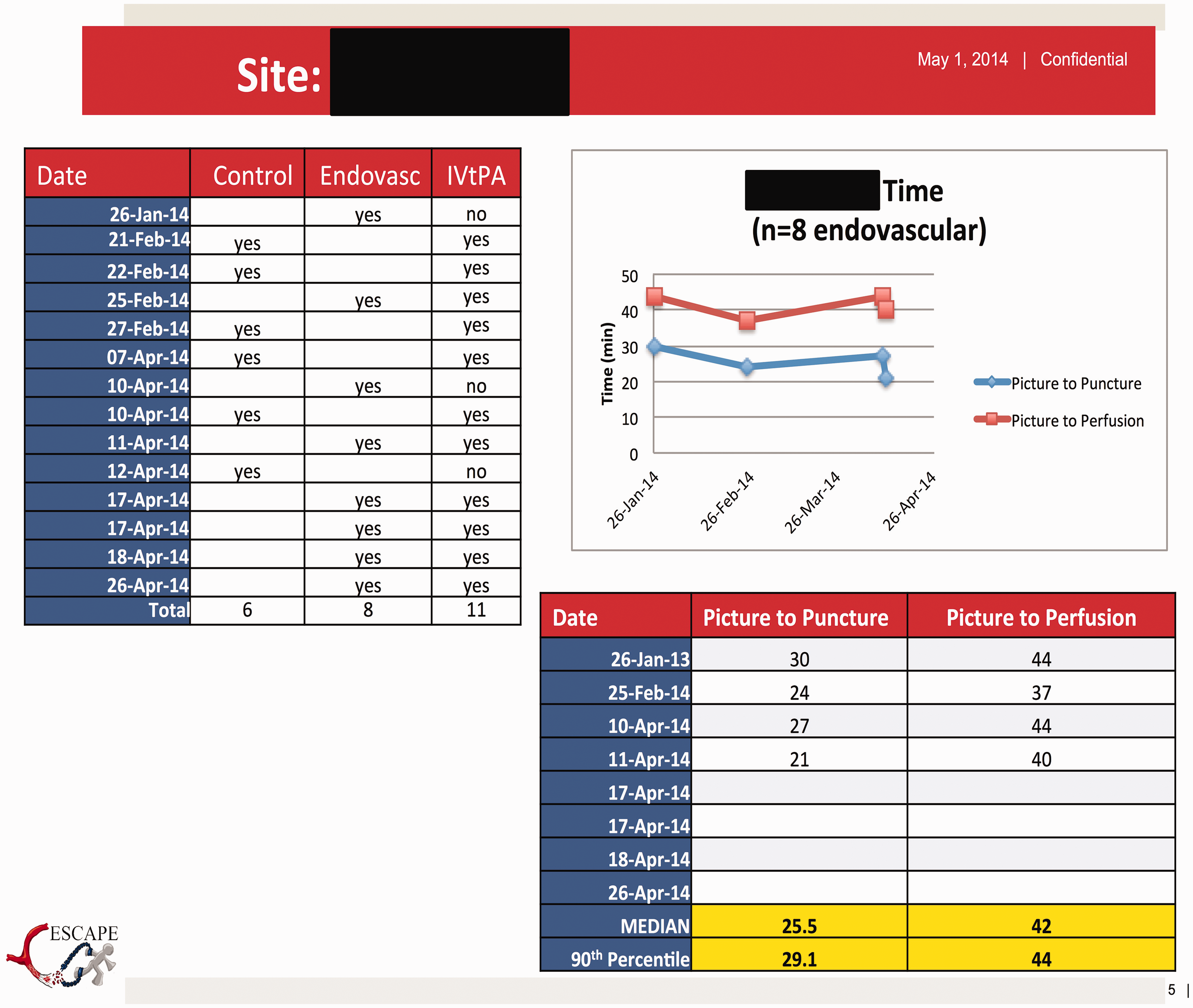
This “audit and feedback” intervention was a nested prospective cohort study within the ESCAPE trial. The evaluation instruments of the study involved a mixed methods approach utilizing both quantitative and qualitative data. Changes in treatment were analyzed as a time series over the course of the study. The overall cumulative change in effect size over the course of the trial was also investigated to determine the clinical significance of the change on outcome.
Statistical methods
The improvement in treatment time for both CT-to-groin-puncture and CT-to-reperfusion was statistically evaluated using an exponential trend model (Tableau Software, Seattle, WA). The overall improvement in effect size was calculated using cumulative probability of mRS 0–2 at 90 days in the order of randomization by treatment group and the absolute risk difference between the two groups (Stata 14, StataCorp, College Station, TX). The cumulative probability was assessed as a linear function of time to estimate the change in effect size over time, beginning after the first 75 patients had been enrolled to allow for instability in the group effect size in the early phases of the study.
Results
The “audit and feedback” intervention for efficient treatment times was completed with 16 sites (out of a total of 18 sites that recruited patients into the treatment arm). Of these 16 sites, three sites had the intervention completed twice. The repeat webinar was completed with the top enrolling sites when the schedule permitted for both the central principal investigators and the target site; it was only completed for three sites as the trial was stopped early. The mean number of people that attended the webinars from the target site was 5.3, and key discussion points included: difficulty in fast treatment during off-hours; pre-notification allowing for faster treatment times; and improving system processes such as moving the patient directly to CT-scanner upon arrival. The target sites raised these discussion points without a preset script or prompts by the webinar host or trial principal investigator. The investigators disseminated information about lessons learned and experience from single sites to all sites in the trial through direct communication.
The exponential trend model showed a reduction in CT-to-groin-puncture time of 6.2 min for every 100 patients enrolled into the treatment arm (p = 0.14; Figure 2 top). CT-to-reperfusion time decreased 4.6 min for every 100 patients enrolled into the treatment arm (p = 0.48; Figure 2 bottom).
(Top) CT-to-groin puncture times over the course of the trial with the exponential trend model. The goal line is indicated with a dashed line at 60 min. (Bottom) CT-to-reperfusion times over the course of the trial with the exponential trend model. The goal line is indicated with a dashed line at 90 min. All the sites that enrolled patients into the endovascular arm are shown with different colors.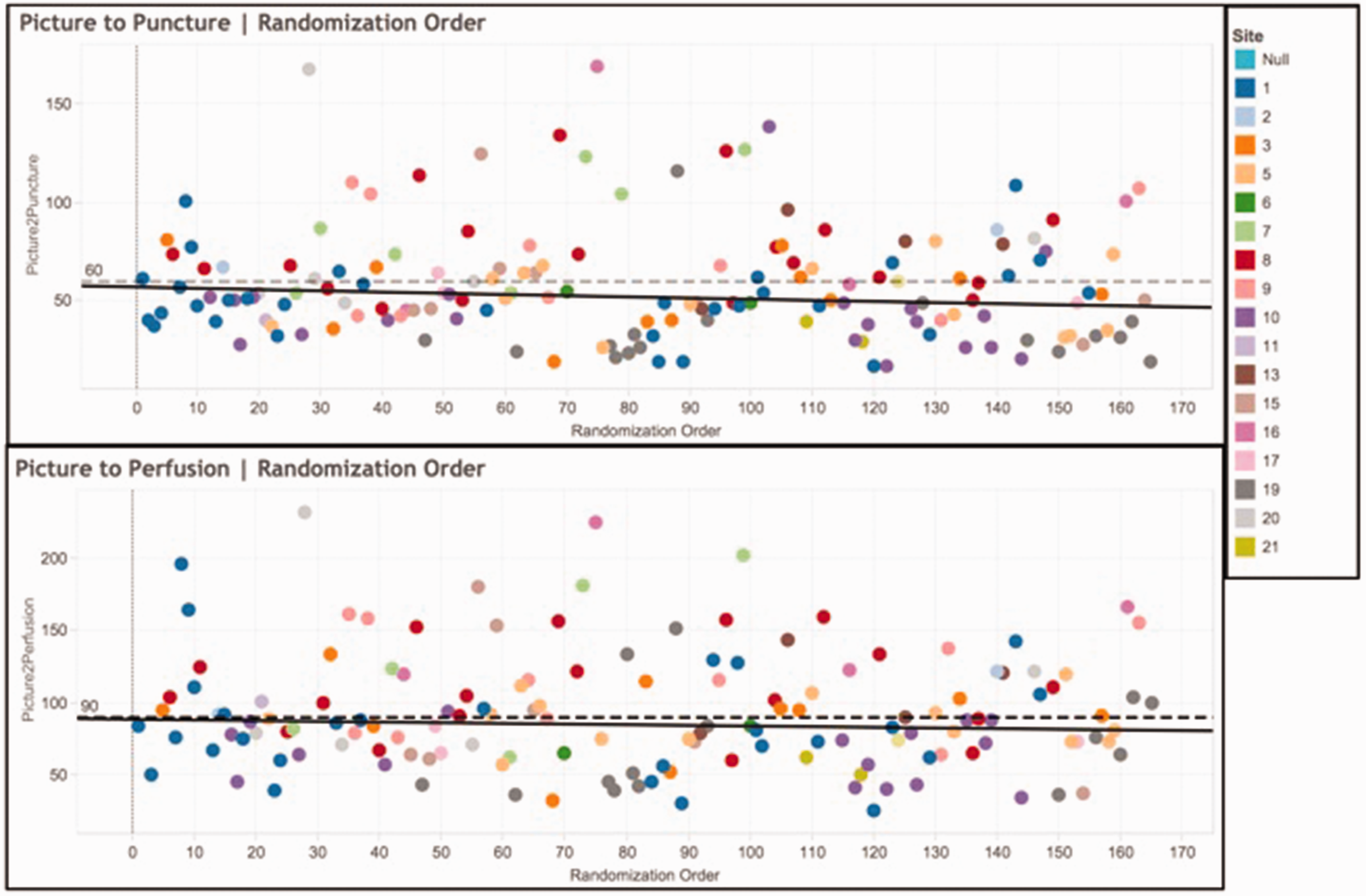
The trial effect size for the cumulative probability of mRS 0–2 at 90 days increased by an absolute improvement of 3.8% per 100 subjects enrolled over the course of the trial (p < 0.001), from 16.0% at the 76th patient to 23.8% at the 315th patient. In the control group, there was a slower improvement at 1.5% per 100 subjects enrolled and so the average absolute risk difference improved 2.2% per 100 subjects enrolled over the course of the trial (p < 0.001; Figure 3). No effect was shown with imaging quality improvement measures.
The change in effect size over the course of the trial. Upper panel shows the cumulative probability of mRS 0–2 at 90 days in the order of randomization by treatment group. The upper line is the endovascular group, the lower line is the medical group. The bottom panel shows the absolute risk difference (effect size). The linear trend line reflects an estimated line of best fit with 95% confidence intervals derived after excluding the first 75 subjects enrolled.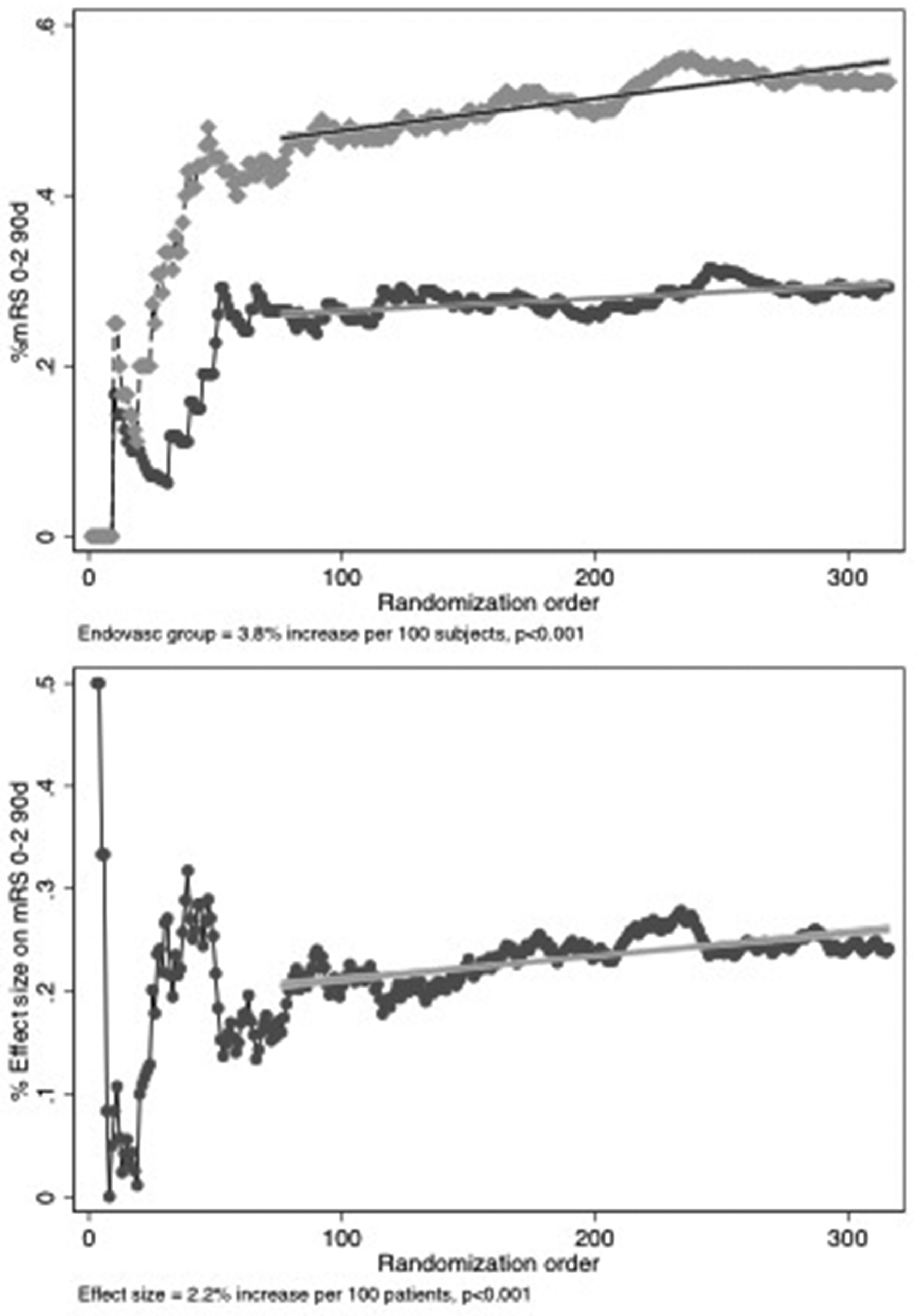
Although imaging was used as the key bio-marker for enrolment into the ESCAPE trial, it is still critical to have fast door-to-CT times. The median door-to-CT time in the trial was 19 min (IQR 13–28) in the treatment arm and 18 min (IQR 9–30).
Conclusions
The use of an “audit and feedback” approach is a feasible approach in maintaining quality in imaging-based patient selection and the speed of treatment. The quality improvement approach in the ESCAPE trial was associated with both faster treatment times and adherence to the protocol stipulated time targets. In turn, this was associated with improving outcomes over the course of the trial.
The ESCAPE trial treatment times were best-in-class when compared with other similar trials. The median onset to first reperfusion time in ESCAPE was 241 min compared with 332 min in the MR CLEAN trial, 2 248 min in the EXTEND-IA trial, 3 252 min in the SWIFT PRIME trial, 4 and 325 min (mean) for the IMSIII trial. 6 Similarly, the workflow efficiency was faster in the ESCAPE trial with a median CT-to-groin-puncture time of 51 min compared with 93 min in the EXTEND-IA trial, and 58 min in the SWIFT-PRIME trial. We believe that this difference can be attributed to the setting of target interval times and to quality assurance processes that were adopted to meet those targets. The absolute treatment time improvements were not statistically different, but this may be due to a floor effect, as treatment times were relatively short at the start and could only improve moderately despite variation in patient factors. These fast initial interval times likely reflect site selection decisions.
The trial was halted early due to overwhelming efficacy of the treatment effect and therefore, there was reduced power to show an effect of improving interval times. However, the average change in speed of treatment over the course of the trial is clinically meaningful and is approximately consistent with the observed improvement in clinical benefit based upon the predicted effect of faster treatment derived from past trials.8,6
A learning effect was present in the trial with improving outcomes in both the endovascular and control groups. However, the widening treatment effect size persisted over and above the improvement in the control group. Other reasons may have contributed to an improving treatment effect such as improving endovascular treatment technique, something which we could not easily measure and therefore not adjust for. While we cannot conclude that the quality improvement process was the single reason why we observed improving outcomes over time, it is plausible that it is a major contributing cause. Quality improvement measures within clinical stroke trials are important components of the trial process and ultimately, trial success. Finally, quality improvement processes should also continue as standard practice at each site beyond the clinical trial to ensure the best clinical outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew Demchuk received fees from Covidien outside of the work proposed. Mayank Goyal received personal fees from Covidien outside the submitted work. Michael Hill personal fees from Merck, and non-financial support from Hoffmann-La Roche Canada Ltd outside the submitted work. He also owns stock in Calgary Scientific Inc., a company that focuses on medical imaging software. Tudor Jovin received personal fees from Air Liquide, personal fees and other support from Silk Road Medical, Inc., personal fees and non-financial support from Covidien Neurovascular, and non-financial support from Stryker Neurovascular outside the submitted work. Alexandre Poppe received personal fees from Covidien, BMS-Pfizer, Octapharma, and Boehringer Ingelheim outside the submitted work. Daniel Roy received grant support from Covidien, Stryker, Codman, and Microvention outside the submitted work. Frank Silver received personal fees from Boehringer Ingelheim outside the submitted work. John Thornton received grant support from Synapse Medical and personal fees from Neuravi outside the submitted work. David Williams reports personal fees from Boehringer Ingelheim, Bayer, and Daiichi-Sankyo outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Covidien, University of Calgary (Hotchkiss Brain Institute, Department of Clinical Neurosciences, Department of Radiology, Calgary Stroke Program), Alberta Innovates Health Solutions, Heart & Stroke Foundation.
Ethical approval
Ethics approval was received by each institution that participated in the ESCAPE trial.
Informed consent
Informed consent was received from each patient throughout the ESCAPE trial. This sub-study did not collect any additional consent.
Guarantor
Dr. Michael D. Hill.
Contributorship
Noreen Kamal and Michael Hill conceived this study. Noreen Kamal led and coordinated the study and wrote the initial draft of the manuscript. Michael Hill, Bijoy Menon, Muneer Eesa, Andrew Demchuk, and Mayank Goyal led the quality improvement webinars with the sites. Karla Ryckborst ensured data collection and quality. Alexandre Poppe, Daniel Roy, John Thornton, David Willioams, Leanne Casaubon, Frank Silver, Kenneth Butcher, Ashfaq Shuaib, Jeremy Rempel, Tudor Jovin, and Biggya Sapkota worked at their sites to improve efficiency and patient selection. All authors contributed to edits of this manuscript.