
Abstract
Introduction
The aim of our study was to evaluate the effect of clot length on both recanalisation and outcome in acute basilar artery occlusion (BAO).
Patients and methods
One hundred forty-nine patients with an acute basilar artery occlusion from the Basilar Artery International Cooperation Study (BASICS) were included. Clot length was assessed on computed tomographic angiography. Thrombus length was divided in tertiles and was related to recanalisation and outcome at 1 month, with Poisson regression. Modified Rankin scale scores of 4 or 5, or death were considered poor outcomes. Additionally, clot length was analysed as a continuous variable.
Results
Forty-nine patients (33%) had a short (4–11 mm), 50 (34%) an intermediate (12–22 mm), and 50 (34%) a long clot (≥23 mm). Multivariable analyses showed a significantly lower probability of recanalisation but no statistically significant difference in poor outcome for patients with a long clot compared with patients with a short clot (RR 0.64, 95% CI: 0.42–0.98 and RR 1.10, 95% CI: 0.88–1.37, respectively). No statistically significant differences were found for patients with an intermediate clot length compared with patients with a short clot length (RR 0.97, 95% CI: 0.75–1.25 and RR 1.11, 95% CI: 0.88–1.40, respectively). Analyses of clot length as a continuous variable showed a 10% reduction in chance of recanalisation and a 2% increase in risk of poor outcome with every centimeter increase in clot length (RR 0.90, 95% CI: 0.78–1.04 and RR 1.02, 95% CI: 0.98–1.05, respectively).
Conclusions
Clot length predicted recanalisation but not outcome at 1 month in patients with a BAO. We found 2% more poor outcome and 10% less recanalisation with every centimeter increase in clot length.
Introduction
Several imaging predictors of recanalisation and outcome after basilar artery occlusion (BAO) have been proposed.1,2 Amongst these imaging predictors, clot length has been shown to affect recanalisation rates of middle cerebral artery occlusion (MCAO)3–5 and BAO 6 after intravenous therapy (IVT) with recombinant tissue plasminogen activator (rtPA). Clot length measurements may be useful for neurointerventionalists when determining the appropriate size of a device to use and may assist in decision making of when to intervene. However, delaying or withholding intra-arterial treatment (IAT) in the presence of a short clot in MCAO seems undesirable in the light of the recent positive anterior circulation trials. 7 Unlike acute MCAO, BAO lacks a proven treatment strategy and, as a result, current treatment strategies of BAO vary widely between centres.8,9 Although recanalisation has been shown to be an important predictor of outcome in patients with BAO,1,10,11 recanalisation alone does not guarantee good outcome and functional independence.12,13
In contrast to the effect of clot length on recanalisation in IVT-treated patients with BAO, little research has been conducted to investigate the effect of clot length on clinical outcome in these patients. Therefore, the aim of our study was to evaluate the effect of clot length on both recanalisation and outcome in acute BAO.
Patients and methods
Study population
Patients from the Basilar Artery International Cooperation Study (BASICS) who met the inclusion criteria below were included. BASICS, the largest prospective registry of consecutive patients with acute symptomatic BAO confirmed by imaging, consisted of 619 patients. The BASICS protocol has been described previously. 14 The ethics committee of the University Medical Center Utrecht, The Netherlands approved the BASICS protocol. The requirement for additional local ethical approval differed between participating countries and was obtained if required. Verbal or written informed consent was obtained from the patient or patient’s representative, as required by national and local guidelines.
Inclusion criteria for the current study were confirmation of BAO on computed tomographic angiography (CTA). To ensure experience of centers in the performance and interpretation of CTA, we included patients who were recruited at sites that performed a CTA in at least 10 patients. CTA was performed according to the local protocol and studies had to be available in Digital Imaging and Communications in Medicine (DICOM) format of sufficient quality.
The primary outcome measures were recanalisation and poor outcome at 1 month. Recanalisation was defined as a patent basilar artery on CTA, magnetic resonance angiography (MRA) or transcranial Doppler (TCD) or a thrombolysis in myocardial infarction (TIMI) score of 2 or 3 on digital subtraction angiography (DSA). In IAT-treated patients, recanalisation was assessed at the end of the angiographic procedure. In patients receiving only antithrombotic treatment (which comprised antiplatelet drugs or systemic anticoagulation) or IVT, recanalisation was assessed in the hours to days after treatment. Recanalisation was not routinely assessed in patients who received no treatment. Poor outcome was defined as a modified Rankin scale (mRS) score of 4 or 5 or death.
Imaging analysis
Thrombus length on CTA was assessed with the 3D curved multiplanar reconstruction function in the v4.1.1 open-source OsiriX DICOM viewer (Figure 1). Scans were read centrally by EJRJH. When the clot extended into the vertebral artery and/or the posterior cerebral artery the total clot length was scored. When clot extended in both vertebral or both posterior cerebral arteries the shortest clot length was scored. Whenever the proximal or distal end of the clot could not be identified this was recorded and the largest identifiable clot length was scored.
Thrombus length assessment on CTA of a patient with a top of the basilar artery occlusion with clot extending into the left posterior cerebral artery.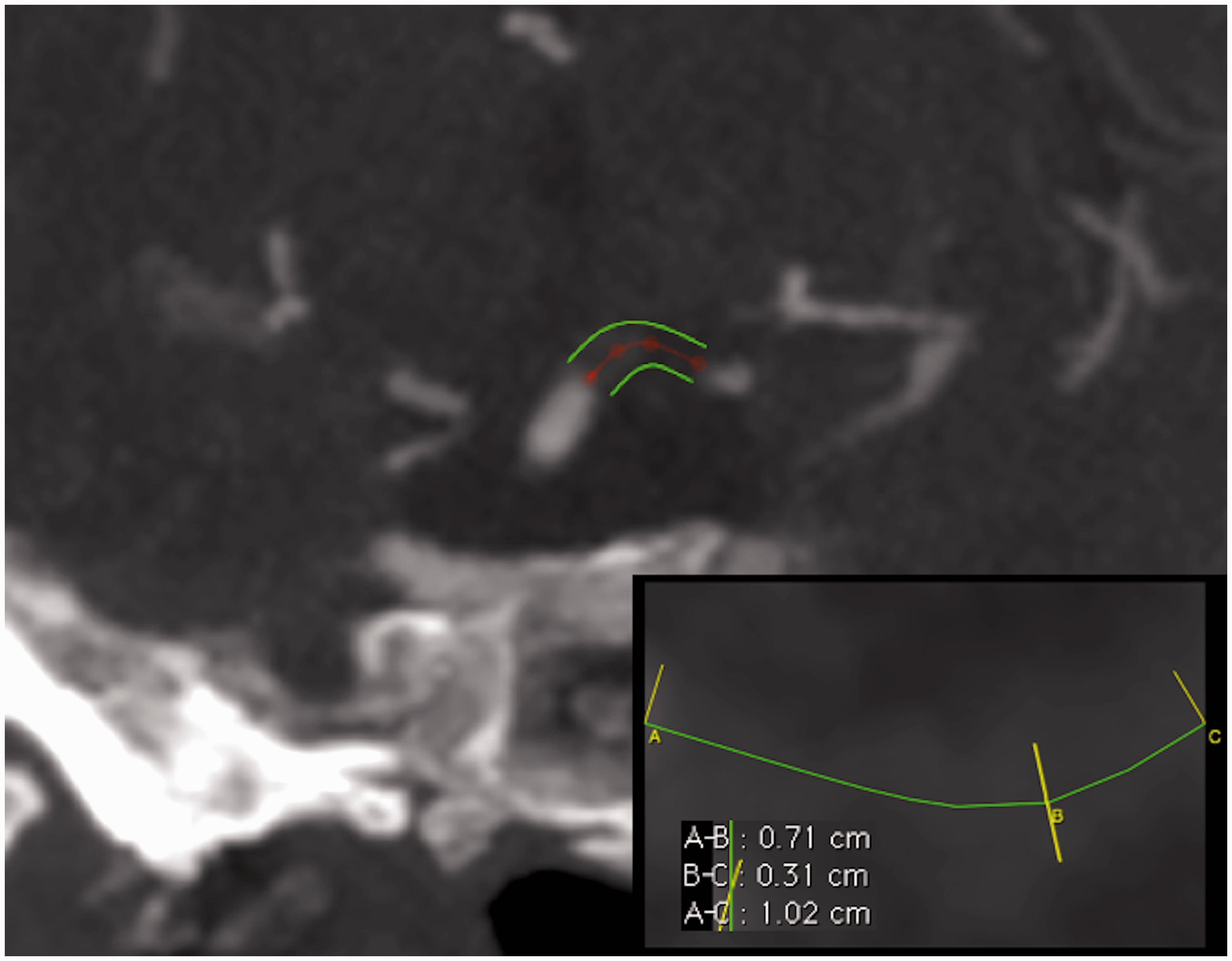
Data analysis
Baseline data are reported with standard descriptive statistics. Whenever the proximal or distal end of the clot could not be identified, 5 mm was added arbitrarily to the measured clot length. We defined three clot length groups of equal size. Short clot length was defined as 4–11 mm, intermediate clot length as 12–22 mm and long clot length as ≥23 mm. The frequency of poor outcome and recanalisation was compared among the three groups with risk ratios (RRs) and corresponding 95% CIs with Poisson regression. Additionally, in multivariable analysis, adjustments were made for the factors most affecting the crude risk ratio (RR). Treatment was categorised into five groups: antithrombotics without IVT or IAT; IVT; IVT followed by IAT; IAT alone, in combination with mechanical thrombectomy or mechanical thrombectomy alone and no treatment. Because the baseline National Institutes of Health Stroke Scale (NIHSS) is a reflection of the severity of the initial stroke and therefore, hypothetically, is affected by the clot length, it was not considered as a potential confounder in developing the multivariable model.15,16 Additionally, clot length was analysed as a continuous variable. Missing baseline data (<5% for each variable) were imputed with regression imputation for optimal adjustment for baseline differences between the groups of interest. 17
Results
Patient characteristics according to thrombus length group.
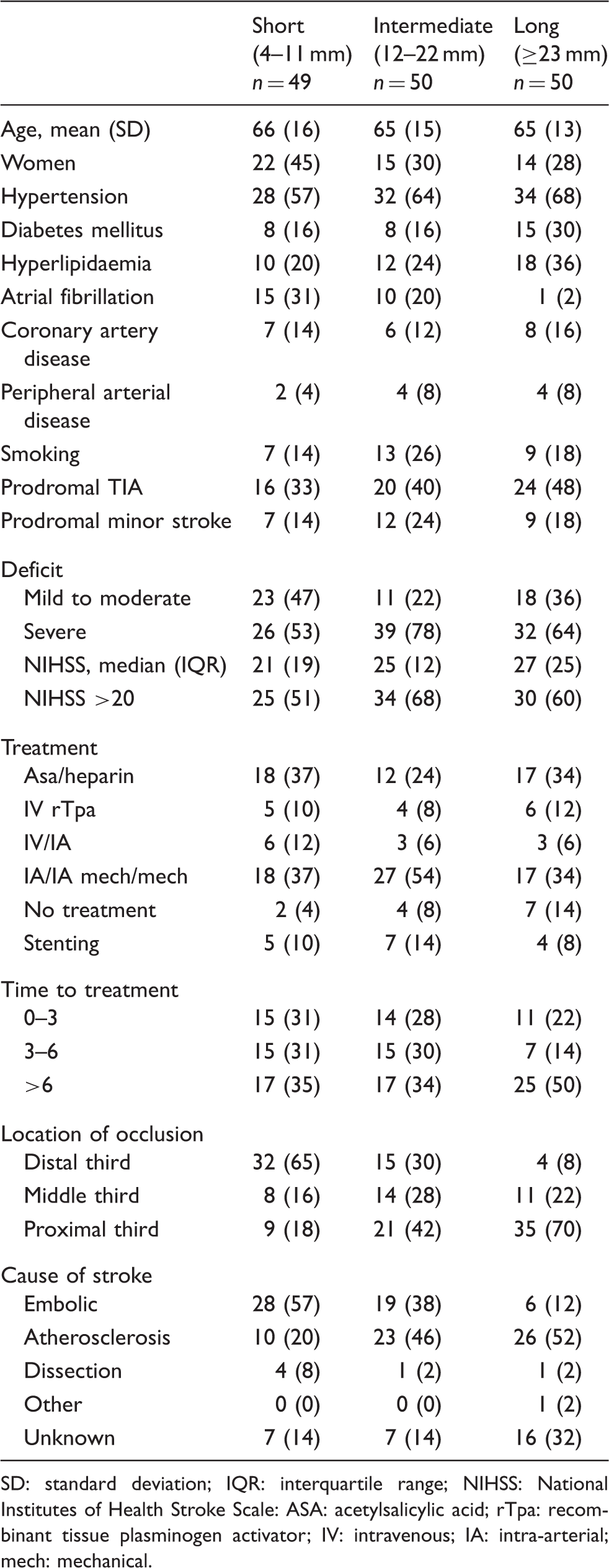
SD: standard deviation; IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale: ASA: acetylsalicylic acid; rTpa: recombinant tissue plasminogen activator; IV: intravenous; IA: intra-arterial; mech: mechanical.
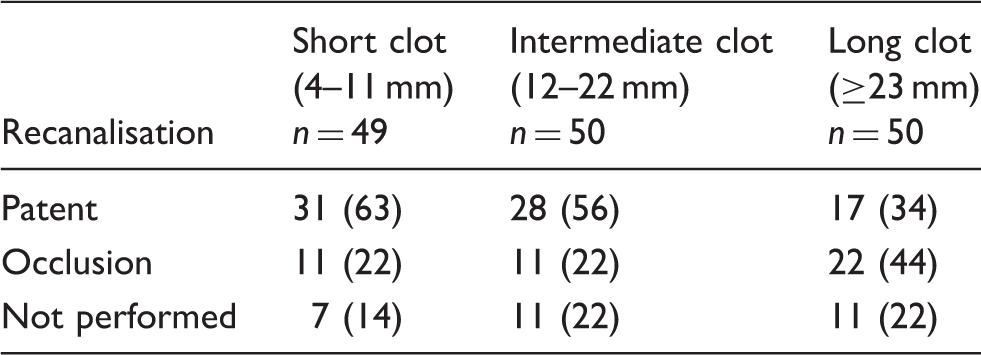
Recanalisation according to clot length group.
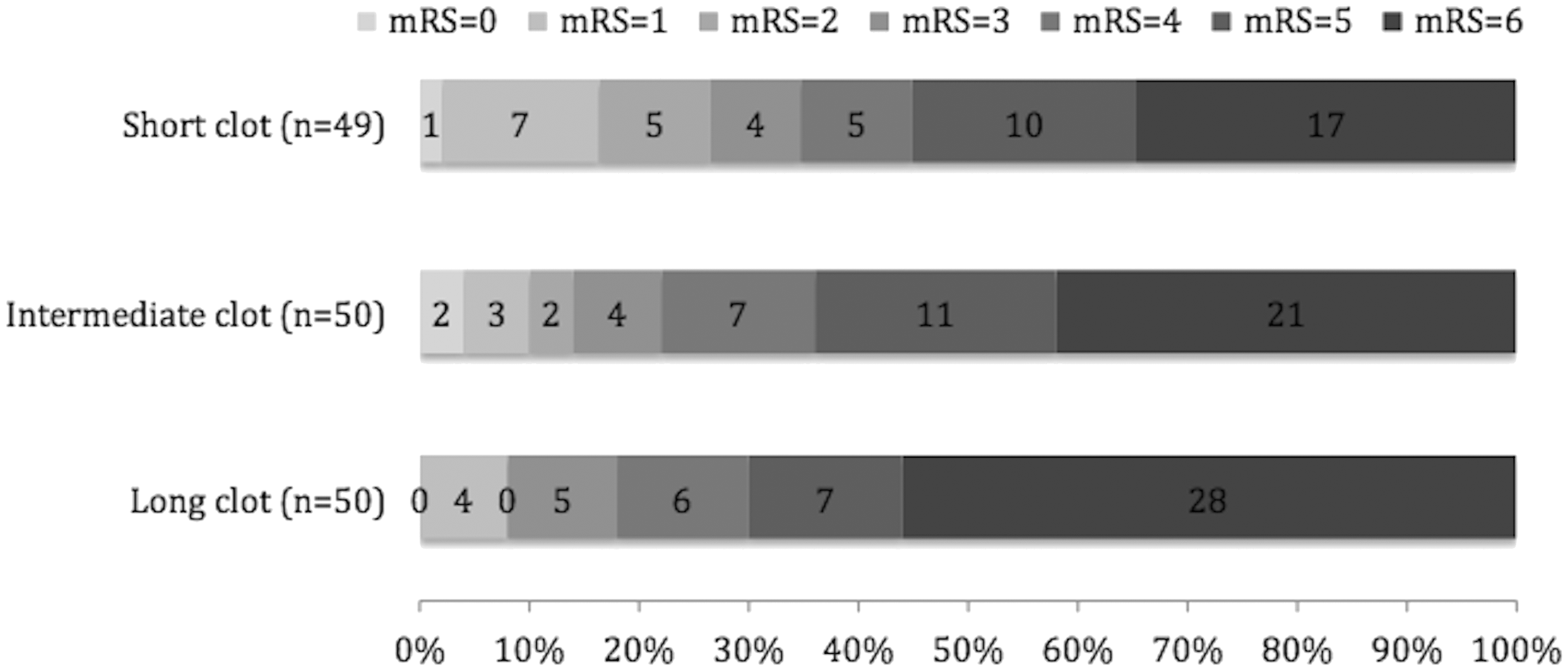
Distribution of modified Rankin scale at 1 month in the three different clot length groups.
Risk ratios for recanalisation according to clot length group—univariable and multivariable analyses.
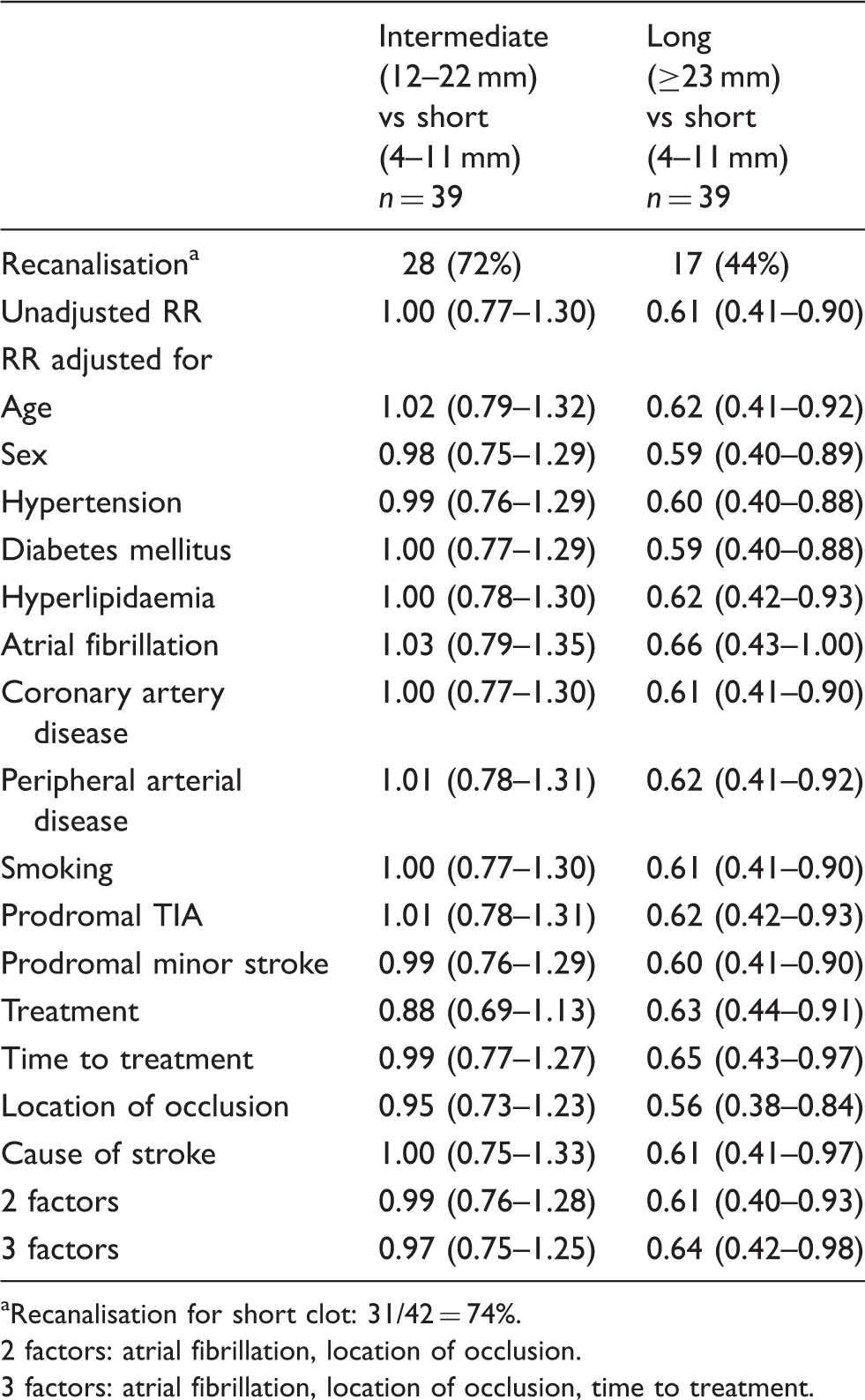
Recanalisation for short clot: 31/42 = 74%.
2 factors: atrial fibrillation, location of occlusion.
3 factors: atrial fibrillation, location of occlusion, time to treatment.
Risk ratios for poor outcome according to clot length group—univariable and multivariable analyses.
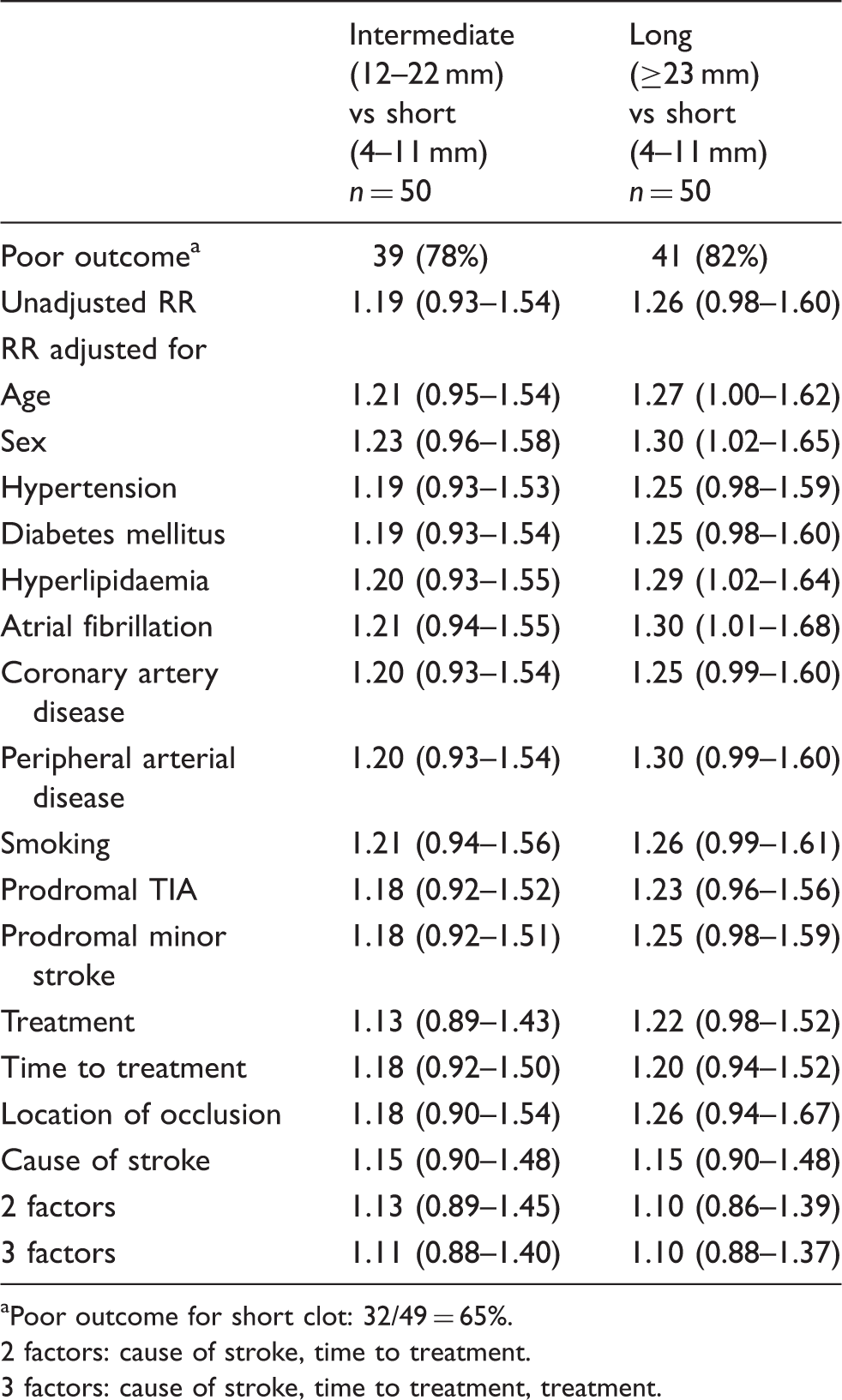
Poor outcome for short clot: 32/49 = 65%.
2 factors: cause of stroke, time to treatment.
3 factors: cause of stroke, time to treatment, treatment.
Additionally, clot length was analysed as a continuous variable. After adjustments for the three most important variables influencing the crude RR (cause of stroke, time to treatment, treatment for poor outcome and atrial fibrillation, location of occlusion, and time to treatment for recanalisation) we found a 10% reduction in chance of recanalisation with every centimeter increase in clot length and an 2% increase in risk of poor outcome (RR 0.90, 95% CI: 0.78–1.04 and RR 1.02, 95% CI: 0.98–1.05, respectively).
Comparison of the relation between clot length on one hand and outcome and recanalisation on the other between treatment groups yielded insufficient numbers for reliable conclusions.
Discussion
We found that increasing clot length independently predicted recanalisation but not outcome in patients with a BAO. Increasing clot length did not predict poor outcome at 1 month in these patients, defined as a mRS score of 4–6. In the analysis of clot length as a continuous variable, we found 10% less recanalisation and 2% more poor outcome with every centimeter increase in clot length.
The BASICS registry is the largest prospective registry of consecutive patients with an acute BAO. However, the observational design inherently incurs limitations to the current study. First, with 149 patients included the sample size is still relatively small. Second, the relatively higher percentage of patients in the intermediate and long clot length group that received no treatment and, as a consequence, less often received follow-up imaging is a potential confounder. Third, time of recanalisation assessment differed between treatment groups, potentially biasing recanalisation rates. Fourth, the choice of treatment was left to the discretion of the clinicians, and was inevitably influenced by the suspected prognosis and effect of treatment. Multivariable analysis can never adjust completely for systematic differences between clot length groups. The risk of poor clinical outcome did not differ statistically significant between the long clot length group and the short clot length group after adjustment for the factors most influencing the crude risk (cause of stroke, time to treatment and treatment type). Stroke etiology strongly affected outcome in univariable analysis. This finding is plausible as atherosclerotic disease not only affects the basilar artery but also potential collateral routes and brainstem perforators. In contrast to good outcome, the probability of recanalisation remained significantly higher in the short clot length group compared with the long cloth length group after adjustments for the factors most influencing the crude risk (atrial fibrillation, location of occlusion and time to treatment). A presumptive explanation for the lack of influence of treatment type on recanalisation could be the relatively low percentage of patients treated with mechanical thrombectomy (30 of 149 patients (20%)). Numbers of stenting were small and comparable between groups and, therefore, unlikely to have influenced the results.
Most earlier studies investigating clot length focussed on MCAO. An initial report found that a hyperdense thrombus longer than 8 mm on noncontrast computed tomography (NCCT) predicted nonresponse to intravenous thrombolysis. 4 Others have shown this relation to be more variable and reported that CT perfusion-derived length of occlusion in IVT-treated patients with proximal MCAO was an independent predictor of recanalisation after 24 h and outcome after 3 months. 5 This study also identified an optimal cut-off value of 12 mm length of occlusion in the M1 segment as a statistically significant independent predictor of recanalisation.
Little research has been conducted on the relationship between clot length, recanalisation and outcome in BAO. Our results support the earlier reported findings that thrombus length is independently associated with recanalisation in patients with BAO. 6 The earlier study, investigating only IVT-treated patients, reported shorter thrombi in patients with recanalisation compared with patients without recanalisation (mean 9.7 vs. 16.6 mm). The current study confirms these findings independently from treatment, which is important as current treatment of BAO varies widely between centers and most patients are not treated with IVT alone. 9 Our findings also support the results of another study, investigating prognostic signs of severity on computed tomography (CT) in patients with a BAO treated with IVT, IAT, IVT followed by IAT or without treatment. 18 This study reported longer clots in poor outcome patients (mRS 4–6) compared with favourable outcome patients (mean 16.5 vs. 11.4 mm) but the difference was not statistically significant, probably because of the small study sample (n = 37).
Longer clots will obstruct more vertebrobasilar (VBA) side branches and, as a consequence, will therefore induce more ischemic damage in the dependent brain tissue. Furthermore, with more obstructed VBA side branches, less collateral routes will be available, which has been shown to be an independent predictor of outcome. 19
BAO, in contrast to MCAO, still lacks a proven treatment strategy. Therefore, clot length measurement, in combination with other clinical and radiological predictors of recanalisation and outcome, may assist in treatment decision making. Recently, promising new CTA-derived thrombus characteristics were introduced in patients with anterior circulation stroke. Thrombus perviousness, which can be assessed by the simultaneous measurement of thrombus attenuation on NCCT and CTA, was shown to be strongly associated with outcome and recanalisation rate. 20 Another study demonstrated that presence of antegrade flow across a cerebral vessel occlusion on four-dimensional CTA is associated with an increased chance of vessel recanalisation. 21 Further research on thrombus characteristics in BAO should proceed and the results of the present study need to be validated in larger and randomised cohorts, like the currently recruiting randomised controlled BASICS trial. 22
Footnotes
Acknowledgement
We thank the BASICS Registry investigators.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Development of the BASICS database was supported by the Department of Neurology, University Medical Centre Utrecht, Utrecht, The Netherlands. This work was supported by the Dutch Heart Foundation to EJRJH (grant no. 2010B151).
Ethical approval
Ethical approval for the BASICS protocol was obtained from the ethics committee of the University Medical Center Utrecht, The Netherlands. The requirement for additional local ethical approval differed between participating countries and was obtained if required.
Informed consent
Verbal or written informed consent was obtained from legally authorised representatives before the study, as required by national and local guidelines.
Guarantor
EJRJH.
Contributorship
EJRJH wrote the first draft of the manuscript and analysed the data. AA participated in writing the protocol and data analysis. WJS, JAV, and LJK participated in writing the protocol. WJS, LJK, HPM and CW were concerned with patient recruitment in the BASICS registry. All authors reviewed and edited the manuscript and approved the final version of the manuscript.