
Abstract
Background
It is unknown which patients with non-traumatic isolated intraventricular hemorrhage should undergo angiographic imaging to detect an underlying macrovascular cause and which modality has the highest yield. We studied yield of angiographic examinations in patients with isolated intraventricular hemorrhage.
Methods
We reviewed medical records of patients with intraventricular hemorrhage admitted to the University Medical Center Utrecht between 2002 and 2012. We searched PubMed and Embase for studies on angiographic examinations in intraventricular hemorrhage until January 2014. We calculated yield of angiographic imaging and investigated influence of age, hypertension and anticoagulant use with meta-regression analysis.
Results
We identified 39 patients of whom 30 underwent an angiographic study. CTA suggested a macrovascular abnormality in nine patients, which was confirmed by DSA in seven. In the literature, we found 16 studies describing 209 patients. Pooled analysis showed a yield of 58% for DSA (95% CI 48–68%; 147 patients). One small study described the yield of CTA or MRA (0%; 4 patients). Yield of angiographic imaging decreased with increasing age (−2.6%; −5.0 to −0.2 per year increase) but was not affected by history of hypertension (−8.3%; −80.8 to 64.2) or anticoagulant use (−47.1%; −110.3 to 16.1).
Conclusion
The reported yield of DSA in isolated intraventricular hemorrhage is around 50% but varies considerably, probably due to differences in clinical judgment on the need for angiography performance. The yield is higher in younger patients but based on the available data, it is not possible to set age or other criteria for patients in whom DSA can be safely omitted.
Keywords
Introduction
Isolated intraventricular hemorrhage (IVH) accounts for around 3% of all non-traumatic intracranial hemorrhages in adults and is therefore a rare condition.1,2 Isolated IVH can originate from rupture of an underlying macrovascular abnormality, e.g. an aneurysm, arteriovenous malformation (AVM) or dural arteriovenous fistula (dAVF). Identification of such abnormalities has important therapeutic implications. Digital subtraction angiography (DSA) is the gold standard for detection of underlying macrovascular abnormalities, but less invasive computed tomography angiography (CTA) and magnetic resonance angiography (MRA) are increasingly applied. It is unclear in which patients with IVH angiographic studies should be performed and what the diagnostic accuracy is of non-invasive techniques. Also, yield of angiographic imaging might be influenced by patient characteristics, including age, pre-existing hypertension and use of oral anticoagulants.3,4 The purpose of this study was to investigate the yield of angiographic modalities in patients with isolated IVH and to study the influence of patient characteristics on this yield.
Methods
Case series
We reviewed the stroke database of the University Medical Center Utrecht for consecutive patients who had been admitted with isolated IVH between January 2002 and May 2012. We reviewed patient records for information on age, sex, diagnosis of hypertension and use of anticoagulants. Patients were considered hypertensive when they had a medical history of hypertension, used antihypertensive agents on admission or were discharged on antihypertensive medication. We reviewed non-contrast CT scans for signs of small vessel disease (SVD), which was defined as the presence of white matter lesions, or an infarct in basal ganglia, thalamus or posterior fossa. We extracted the number, type and yield of angiographic examinations.
Systematic literature search
We systematically searched PubMed and Embase up to January 2014 using synonyms of the following search terms ‘intraventricular hemorrhage’, ‘digital subtraction angiography’, ‘magnetic resonance angiography’ and ‘computed tomography angiography’ (NH, Supplementary Table 1). No language restrictions were added. Title and abstract were screened for relevant articles based on predefined inclusion criteria. Inclusion criteria were (1) IVH defined as non-traumatic hemorrhage confined to the ventricles, (2) inclusion of at least three consecutive patients, (3) reporting results of CTA, MRA or DSA. References and related citations of relevant articles were screened until no additional studies were found. The quality of the selected studies was assessed using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS), 5 and the Standards for the Reporting of Diagnostic accuracy studies (STARD). 6
Two authors (NH, CvA) independently retrieved information on case-finding methods, the number of included patients, age, sex, history of hypertension, use of anticoagulants, the applied angiographic modalities and their diagnostic yield. Diagnostic yield was defined as the proportion of angiographic examinations that identified a vascular abnormality as the cause of the IVH.
Statistical analysis
For each study, we calculated mean age, proportion of men, proportion of patients with hypertension, proportion of patients on anticoagulants and the yield of angiographic examinations with 95% CI. In the case series, we calculated sensitivity and specificity of CTA compared with DSA, with 95% CI. Inconclusive CTAs were considered as positive outcomes. We performed logistic regression to study the association between age, signs of SVD and presence of vascular malformations. We pooled the yield of angiographic examinations obtained from the case series with the estimates from the literature review using a random effects model. To investigate the association between age, hypertension, use of anticoagulants, and the yield, we performed meta-regression analysis weighted by the inverse variance. All statistical analyses were performed with SPSS version 22 or R version 3.0.3 for Windows (http://cran.r-project.org/).
Results
Case series
In our case series, we included 39 patients with isolated IVH (Supplementary Table 2). In 30 patients, one or more angiographic examination had been performed: CTA in 28 patients, MRA in five patients and DSA in nine. In seven of 30 patients (23%), a macrovascular cause was found, in five patients an AVM, and in two patients a dAVF. CTA had suggested the underlying macrovascular abnormality in nine patients, and it was confirmed by DSA in seven patients. Sensitivity of CTA was 100% (95% CI 56–100) and specificity 50% (95% CI 3–97%). No DSA was performed in any of the 18 patients with a negative CTA. In the five patients who underwent MRA, we found no underlying macrovascular lesions; in three of these patients, prior CTA had been negative as well. During a median follow-up of three months (range 0–132 months), we found no macrovascular abnormalities nor recurrent hemorrhage among 24 patients with non-fatal IVH, who did not undergo DSA. The odds of having a vascular malformation decreased with each year increase in age (OR 0.91, 95% CI 0.85–0.97). There was no significant association between signs of SVD and presence of a macrovascular abnormality (OR 0.45, 95% CI 0.08–2.69).
Systematic literature search
The literature search yielded 16 studies reporting on 209 patients with isolated IVH (Supplementary Figure 1).1,2,4,7–19 Thirteen studies described the yield of a single investigation, in all cases DSA. One study described DSA and performed MRA in one patient, 11 one study compared CTA with DSA, 19 and a single study reported on the diagnostic yield of CTA in addition to gadolinium-enhanced MRI/MRA. 7 Six studies had a prospective design.1,7,8,10,16,17 All studies except two based the diagnosis isolated IVH on initial CT imaging. Two studies also performed MRI, either in a subset of patients, 11 or in all patients. 7 Four studies specifically state that CT scans were reviewed by at least two radiologists.7,8,10,11 None of the included studies fulfilled all criteria for good quality of diagnostic studies according to the QUADAS-tool or STARD-checklist.5,6 Apart from two, none of the studies assessed the yield of one modality in comparison with another that was used as a reference standard,7,19 and most studies did not specify their selection criteria for angiography (Supplementary Figure 2).
Characteristics of 17 cohorts reporting on the yield of angiographic examinations in isolated intraventricular hemorrhage, including our own series.
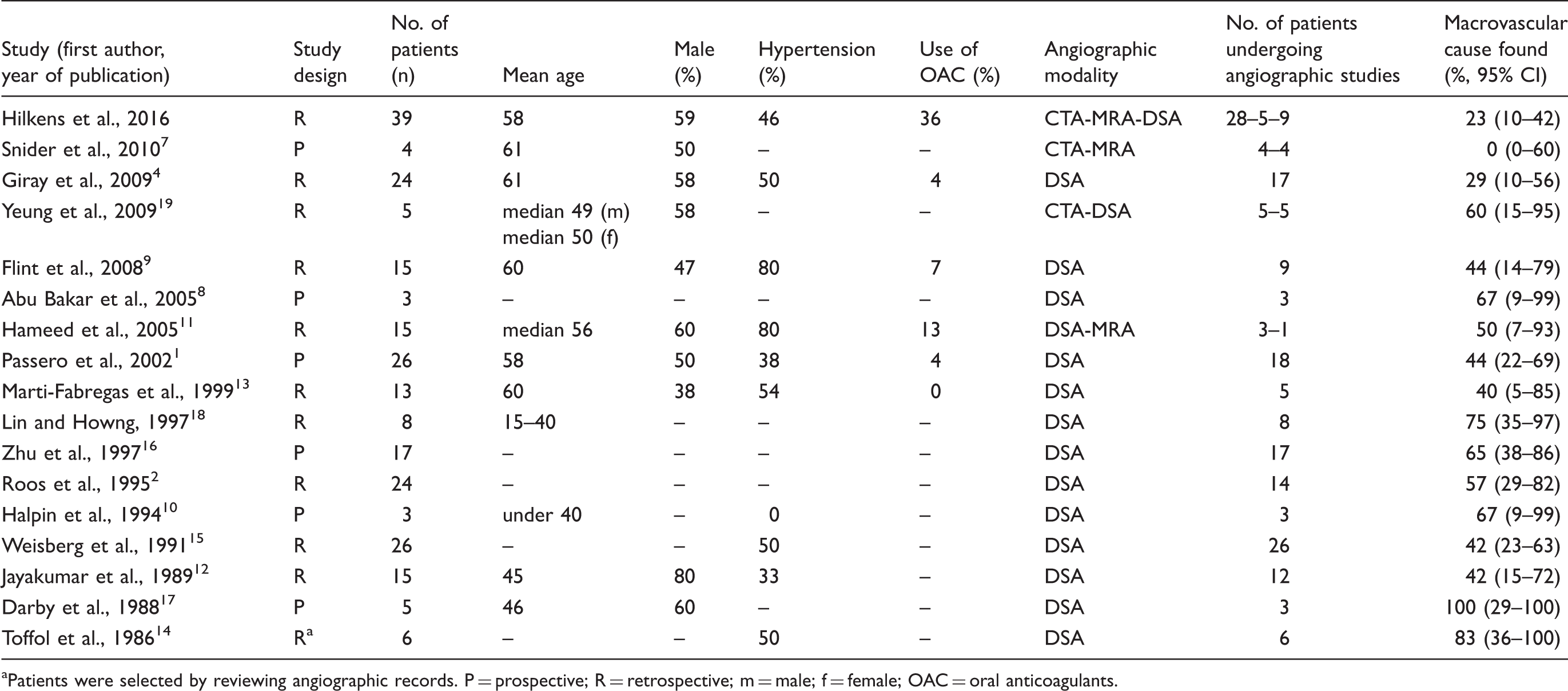
Patients were selected by reviewing angiographic records. P = prospective; R = retrospective; m = male; f = female; OAC = oral anticoagulants.
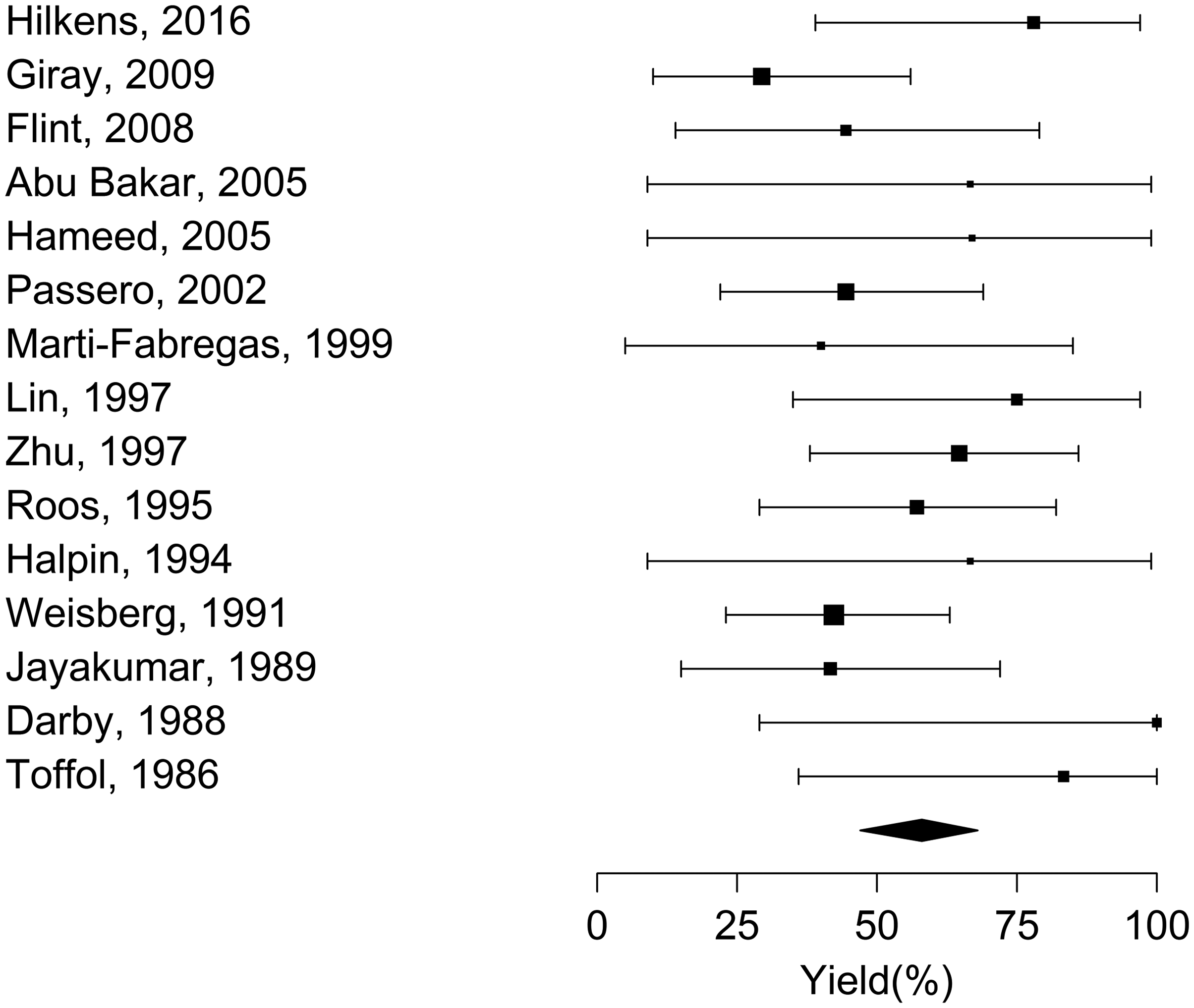
Pooled analysis of 16 studies reporting on yield of digital subtraction angiography.
Overall, 84 macrovascular abnormalities were identified: in 50 patients (60%) the cause of IVH was an AVM, in 28 (35%) an aneurysm, in five (6%) a dural AVF and in one patient moyamoya disease (1%). With each year increase in mean age per study, the yield of angiographic imaging decreased by −2.6% (95% CI −5.0 to −0.2). We found no effect of the proportion of patients with hypertension (−8.3%; 95% CI −80.8 to 64.2) or of patients on anticoagulants (−47.1%; 95% CI −110.3 to 16.1).
Discussion
In around half of the patients with IVH undergoing DSA, a macrovascular lesion is found, but the yield varies considerably between studies, which is probably explained by varying selection criteria. The yield of angiographic imaging increases in younger patients, whereas we found no effect of the presence of hypertension or the use of oral anticoagulants.
Accurate detection of underlying malformations is of great importance, since timely treatment may prevent recurrent hemorrhage. Although the yield was higher in younger patients, we could not set an age criterion for patients in whom DSA can be omitted based on our data; it is likely that also here bias by indication played a role in the studies included in the review and in our own cohort. Given the consequences of detection of an underlying malformation, DSA should probably be considered, in particular in younger patients, unless there are distinct contra-indications. Based on the available data, presence or absence of hypertension or use of oral anticoagulation should not be a criterion, but the lack of association is probably a result of indication bias. In our small case series, we could not find a significant association between SVD and presence of macrovascular abnormalities, while this was found in a large prospective study among patients with non-traumatic ICH. 20 This study showed a higher probability of finding a macrovascular cause among patients without signs of SVD. The absence of an association in our study might be explained by a lack of power.
CTA and MRA may be preferred imaging modalities due to their non-invasive character but their diagnostic accuracy in isolated IVH is unsettled. A recent Cochrane review investigated the yield of non-invasive imaging in patients with spontaneous parenchymal intracerebral hemorrhage. 21 Eleven studies, totaling 927 patients were identified that compared either CTA or MRA with DSA. Only five patients had isolated IVH. This meta-analysis showed a high sensitivity (95%; 95% CI 90–97%) and specificity (99%; 95% CI 97–100%) of CTA, and similar numbers for MRA, but results were limited by methodological drawbacks in some of the included studies. Given the small number of patients with isolated IVH included in this meta-analysis, generalizability to patients with isolated IVH is uncertain. A recent prospective cohort study of 300 patients with ICH (not including patients with isolated IVH) showed a lower sensitivity of CTA than found in the meta-analysis (74%; 95% CI 62–84%) and also a lower specificity (91%; 95% CI 86–94%) for detection of a macrovascular lesion as the underlying cause of ICH. 20
Several limitations of our study need to be addressed. First, most studies had small sample sizes and a retrospective design. Second, case finding methods varied among included studies, as well as selection criteria for angiography performance. This decreases comparability of the results and may partly explain the wide variation of yield of DSA. Third, information on age, history of hypertension and use of oral anticoagulants was only available at summary level, and no distinction was made between patients who did or did not undergo angiography. Also, some studies presented no information on risk factors and had to be excluded from these analysis. Fourth, not all patients included in our case series underwent angiographic imaging (CTA, MRA or DSA) nor was DSA performed in all patients with negative CTA. As a result, small vascular abnormalities may have been missed. A strength of our study is that we have summarized the available evidence in a systematic way with pre-specified inclusion criteria and without applying any language restrictions. Also, to the best of our knowledge, our case series of diagnostic yield in isolated IVH is the largest so far reported.
The results of this study suggest that the yield of angiographic examination is higher in younger patients with isolated IVH. The available data are insufficient to provide firm recommendations regarding in which patients what type of angiographic examinations should be performed, or in which patients angiographic examinations are not needed. Data on the yield of CTA and MRA in patients with isolated IVH are urgently needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CJJ van Asch was supported by a Dutch Heart Foundation grant (grant no. 2007B048, to CJM Klijn). CJM Klijn is supported by a clinical established investigator grant of the Dutch Heart Foundation (grant no. 2012 T077), and an Aspasia grant from The Netherlands Organisation for Health Research and Development, ZonMw (grant no. 015008048).
Ethical approval
The Medical Ethics Review Committee of the University Medical Center Utrecht reviewed the protocol and waived the requirement for ethical review.
Informed consent
N/A
Guarantor
CJMK.
Contributorship
CJMK initiated the study. NAH and CJJvA performed the literature search. NAH screened title and abstract for eligible studies. Uncertainties about eligibility were resolved by discussion with CJJvA and CJMK. NAH and CJJvA extracted data from identified articles. NAH performed the statistical analyses. All authors interpreted the data. NAH and CJJvA drafted the manuscript, which was critically reviewed and revised for important intellectual content by all authors.