
Abstract
Purpose
Many patients suffer a stroke at a significant distance from a specialized center capable of delivering endovascular therapy. As a result, they require rapid transport by helicopter emergency medical services, sometimes while receiving a recombinant tissue plasminogen activator infusion (drip and ship). Despite its critical role in the new era of reperfusion, helicopter emergency medical services remains a poorly evaluated aspect of stroke care.
Method
Comprehensive narrative review of all published articles of helicopter emergency medical services related to acute stroke care in the inter-hospital and pre-hospital settings, including technical aspects and physical environment implications.
Findings
Helicopter emergency medical services transports are conducted during a critical early time period when specific interventions and ancillary care practices may have a significant influence on outcomes. We have limited knowledge of the potential impact of the unusual physical factors generated by the helicopter on the ischemic brain, which affects our ability to establish rational guidelines for ancillary care and the delivery of specific interventions.
Discussion
Unlike the pre-hospital and hospital settings where stroke interventions are delivered, the inter-hospital helicopter emergency medical services transfer setting remains a “black box” for acute stroke care and research. This gap is particularly relevant for many patients living in rural areas, or in congested urban areas, that depend on helicopter emergency medical services for rapid access to a tertiary stroke center.
Conclusion
Addressing the helicopter emergency medical services stroke gap in clinical trials and acute care delivery would homogenize capabilities through all care settings, thus minimizing potential disparities in research access and outcomes based on geographical location.
Impact of air medical transport in acute stroke
This study was narrative review summarizing the field of helicopter transportation of stroke patients. A Pubmed search was conducted June 2016 using the search terms “Helicopter & stroke” and “HEMS & stroke” and “helicopter & cerebrovascular disorder” (to enhance capture before year 2000). These lead to 134, 13, and 131 articles, respectively. All articles were reviewed, and 19 were selected based on their relevance to this review.
Stroke is a common contributor to disability in the World, with over 16.9 million new patients affected each year. 1 Helicopter emergency medical services (HEMS) is an important element in the system for delivering acute stroke care for patients that suffer a stroke at a significant distance from a tertiary stroke center, approximately 20% of the US population,2,3 and many other areas of the world. In addition to intravenous recombinant tissue plasminogen activator (rtPA) treatment, endovascular mechanical thrombectomy (MT) recently became the new standard of care in patients with a stroke due to a proximal arterial occlusion. 4 But unlike widely available intravenous rtPA, MT is a complex therapy that requires specific equipment and human expertise only available at a limited number of tertiary centers in the United States. 5 Given the geographic dispersion of the US population, transfer of a great number of patients to an MT-capable center is required. 5 Because MT is a time-dependent therapy tied to viable ischemic penumbra within a short window of opportunity, 4 emergent HEMS is often required. 6
Consequently, HEMS is largely used in the United States for inter-hospital transfer from a community hospital to a comprehensive stroke center, often while receiving rtPA while in route to a tertiary center.7,8 It is also used in lesser amount for direct field to hospital operations, mostly in very remote (frontier) or isolated geographical situations,9,8 such as islands, sea, 10 or mountains. There are approximately 400,000 total HEMS missions flown a year in the United States. 11 A large 10-year sample of HEMS flights has shown a gradual increase in the ischemic stroke related missions which comprised 4% of the flight missions in 2011. 8 Based on that estimation, there are 16,000 ischemic stroke helicopter missions flown each year in the United States. However, that data might be an underestimation since it preceded the establishment of MT, which requires expeditious transportation.6,12 It is therefore expected that the use of HEMS will significantly increase with the widespread implementation of MT. The number of acute stroke-related fixed-wing operations is not known. But given the delays caused by the logistics and since airplane flights require out of hospital take-off and landing, fixed-wing operations are probably not a big additional contributor to acute reperfusion therapy.
Air medical crews are generally composed of flight paramedics and flight nurses, which are sometimes joined by emergency medicine physicians and residents. The procedures to be selected as part of a crew are rigorous, which results in a very skillful yet small number of professionals that cover a large spectrum of patients.13,14 As a result, HEMS is staffed by a group of highly trained professionals capable of delivering excellent care during critical early time periods when specific interventions and ancillary care practices may have a significant influence on outcomes. But despite the obvious and growing relevance of HEMS for acute stroke care, it remains a gap in knowledge and research capabilities (Figure 1).
HEMS: A gap in acute stroke delivery and research.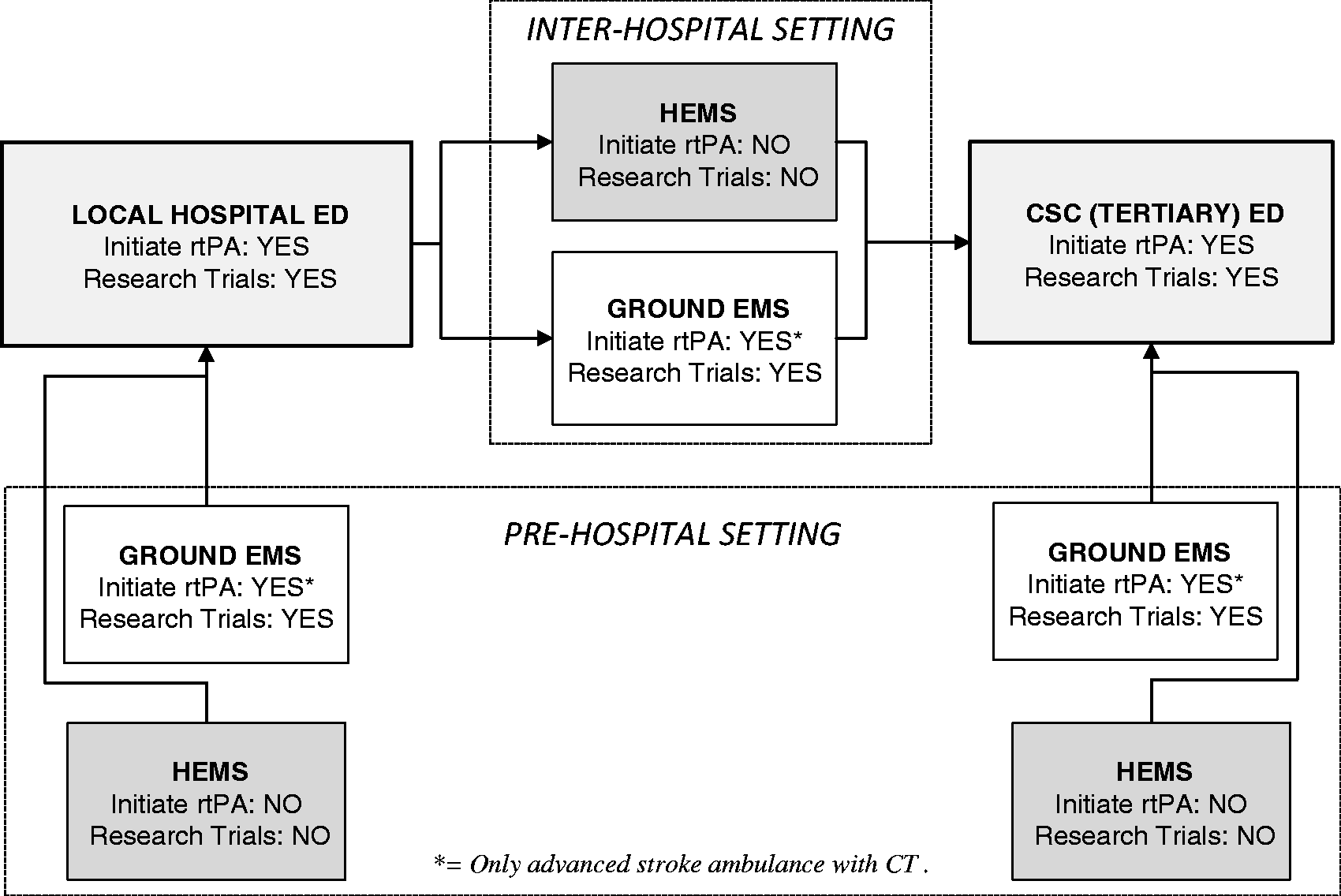
Inter-hospital HEMS in stroke
The most common (72%) use of HEMS in the United States applies to inter-hospital transfer. 8
Comparison between the pre-hospital and the inter-hospital stroke environments.
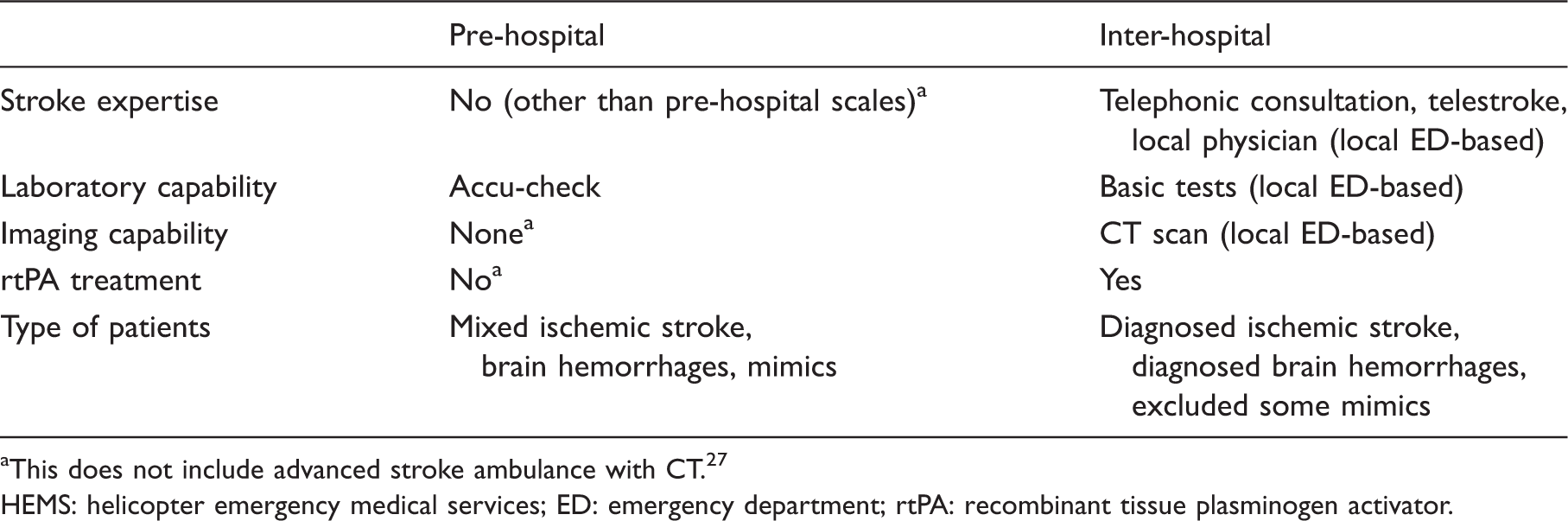
This does not include advanced stroke ambulance with CT. 27
HEMS: helicopter emergency medical services; ED: emergency department; rtPA: recombinant tissue plasminogen activator.
A variety of factors and local regulations play into determining the choice of using HEMS versus ground ambulances for inter-hospital transport. For example, in the United States the Emergency Medical Treatment and Active Labor Act authorize the referring physician to choose the mode of transport. The severity of symptoms, use of rtPA, and need for interventional therapy, as well as system limitations such as distance to the stroke center and availability of critical care air or ground ambulances all play a role.8,19 Beside the difference in speed, 16 HEMS-transported patients were receiving higher rates of IV thrombolysis locally 20 as well as more specialized care and interventions. 6 For these reasons, HEMS has been endorsed by the air medical community as the most appropriate method of inter-hospital transportation for acute stroke, 21 a recommendation that preceded the establishment of MT as the new standard of care. This has obviously become even more relevant now since for many patients living in rural areas, or in traffic congested urban areas, HEMS might be the best chance to arrive on time to an MT center. Alternatively, HEMS could be used to transport an interventionalist to treat the patient at hospitals that have the necessary equipment but lack the human expertise.
Still, HEMS has some intrinsic limitations. It is more vulnerable to weather conditions than ground ambulances. Bad weather might result in either not flying at all, or flying at an unjustifiably increased risk. A study showed 182 HEMS crashes in the United States during 1983–2005. 22 While that risk is still relatively low, crashes were more likely to occur in darkness and during instrument-based flying (bad weather). 22 To minimize this issue, flight crews are typically instructed to make their go/no-go decision solely based in operational aeronautical factors. They are deliberately kept blinded to the age and diagnosis of the patient until they are airborne in order to avoid medical/personal biases in their aeronautical decision. 23 Another important limitation is the cost. The use of HEMS for facilitation of intravenous thrombolytic treatment was analyzed regarding cost-effectiveness. A computer model based cost-analysis deemed HEMS to be cost-effective 24 when thrombolytic treatment was only started after transport. A small single center retrospective cohort study raised concerns about the benefit of HEMS unless endovascular therapy is considered. 25
Field to hospital use of HEMS
Direct field to stroke center is a pre-hospital HEMS approach that is most appropriate for very remote (frontier) states with little access to stroke-ready hospitals. 9 Local availability of a primary or comprehensive stroke center is of great importance in determining the destination for a HEMS scene transport. This approach was used for 28% of HEMS transports in one large cohort of 25,332 cases. 8 By transporting patients rapidly to a stroke center, it might allow the administration of rtPA 9 or MT. As this is a pre-hospital setting (Table 1), the patients seen are similar to that encountered by ground emergency medical services (EMS). This includes a combination of ischemic and hemorrhagic strokes, as well as stroke mimics.
Comparison between ground ambulances and HEMS.
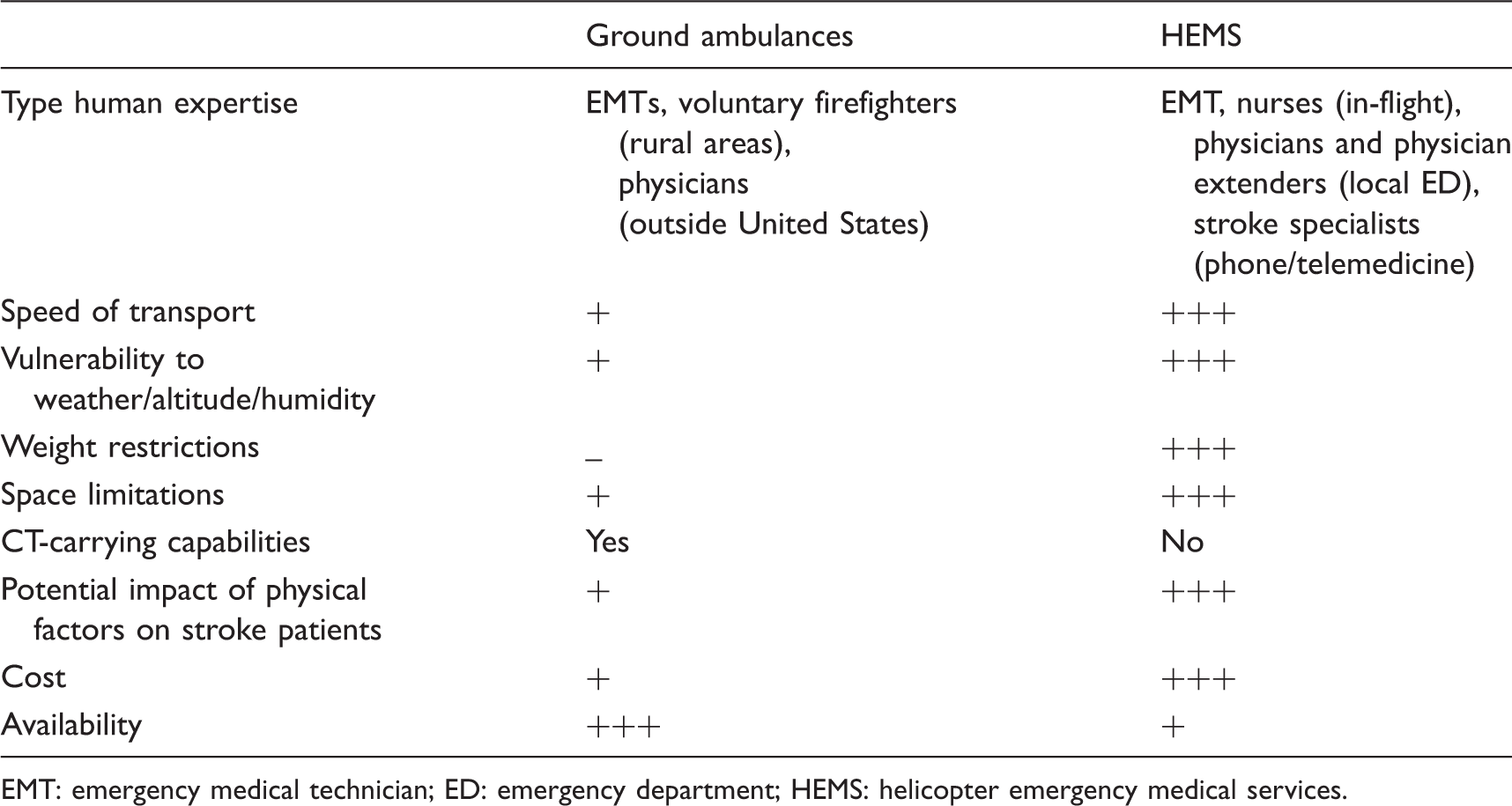
EMT: emergency medical technician; ED: emergency department; HEMS: helicopter emergency medical services.
Advanced pre-hospital stroke work-up and treatment
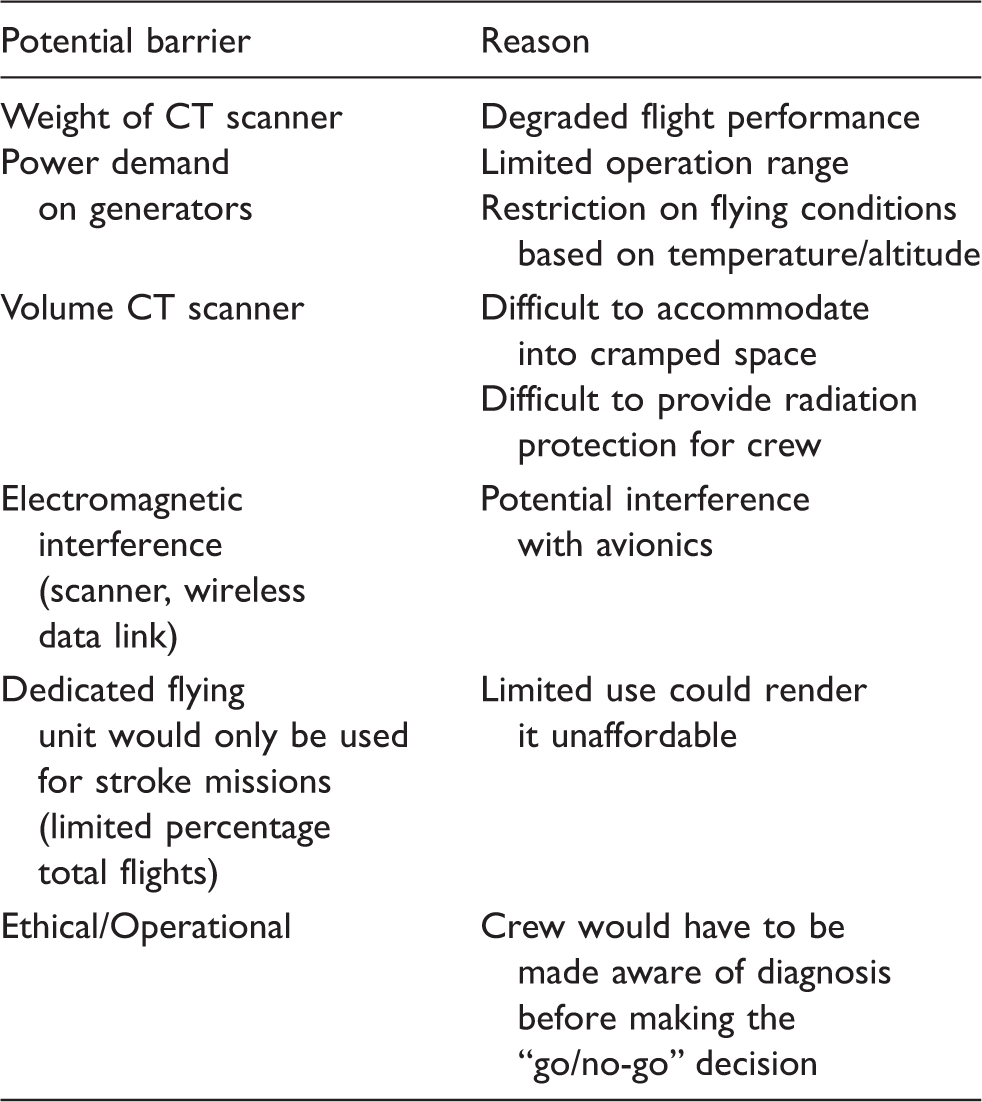
The new specialized stroke ambulance concept with CT and telemedicine capability 27 aboard ground ambulances allows diagnosis and early treatment before hospital arrival. Studies have shown relevant time-to-treatment reduction in intravenous rtPA application28,29 with much higher percentage of patients treated within 60 min from onset, 30 this approach is still rarely used and probably limited to the large metropolitan areas where their cost might be justified by the large volumes. 31 Keeping this in mind, it seems unlikely that CT-carrying stroke ambulances would be implemented in dispersed rural areas with a smaller density of strokes and sometimes limited human expertise (e.g. in the United States typically staffed by voluntary firefighters).14,32 HEMS could be an alternative to specialized stroke ambulances for rural areas, allowing the field initiation of rtPA in frontier states.27,33 So far, the main limitation for specialized stroke HEMS is the lack of imaging capability. A small study has shown the feasibility of transcranial Doppler (TCD) during HEMS, 34 but this technique requires expertise and is not sufficient to exclude intracranial hemorrhage before initiation of rtPA treatment.
Potential barriers to transform helicopters into CT-carrying advanced stroke ambulances.
Implications of the HEMS-specific physical environment
Potential effects of HEMS-associated physical factors.
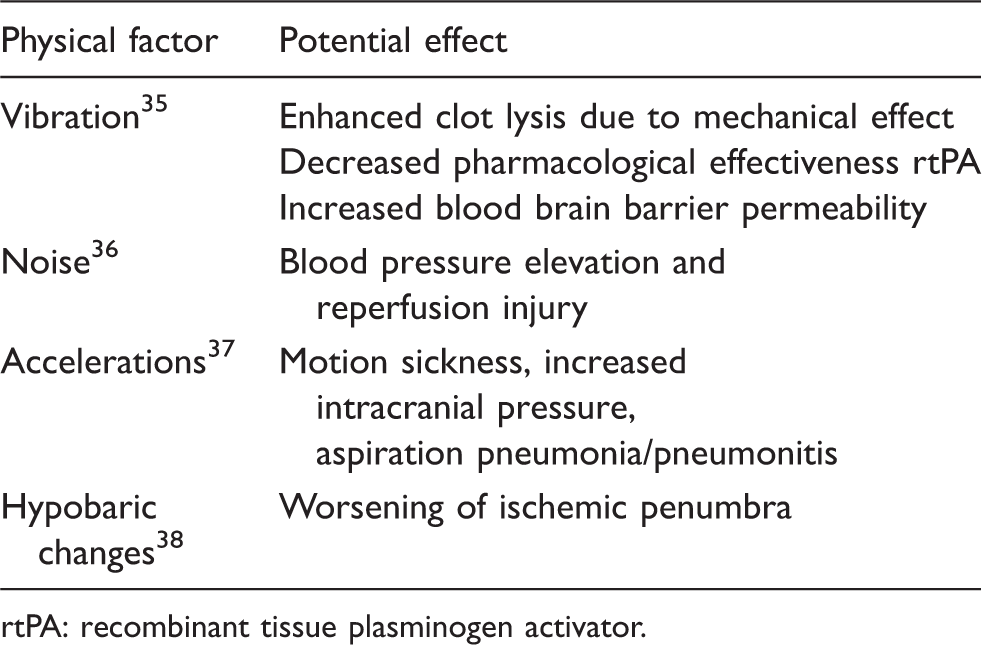
rtPA: recombinant tissue plasminogen activator.
Current ancillary care in patients transported through HEMS
The care of patients transported by HEMS is determined by the physician responsible for the medical oversight of that specific program. 43 In the absence of specific national guidelines, the local rules are typically inspired and adapted from the current guidelines of ground-based stroke management including post-rtPA care. 43 Treatment of patients within the HEMS environment is a combination of standard EMS care as well as ED and ICU level care. Traditional ground ambulance EMS care of stroke patients focuses on early recognition, rapid transport, and early notification to the receiving center. 43 HEMS units transporting patients directly from scene to a hospital typically follow these guidelines as imaging would not have been obtained to rule out hemorrhage. But the HEMS units transporting patients in an inter-hospital capacity are expected to provide care similar to an intensive care unit or an ED, with the obvious limitations of the helicopter capabilities. This includes appropriate blood pressure control, especially in the setting of tPA delivery, airway control, and early identification of complications. While there are ground critical care EMS services that can operate at a similar level to HEMS units, many regions of the country do not have these units available. They are especially scarce in rural regions. HEMS ancillary-care guidelines are typically based on expert opinion without necessarily taking into consideration the unique physical HEMS environment. 42
Inter-hospital HEMS: An underutilized clinical research opportunity
Pre-hospital HEMS research might be possible with a similar approach as that employed by ambulance based ground trials, 44 with the additional advantage of enhanced human expertise and limited amount of co-investigators that are needed. However, there is a much greater potential for research in the inter-hospital transfer. It provides a unique opportunity to test specific interventions to preserve the penumbra and mitigate reperfusion injury in transit. 23 Such interventions are particularly relevant for patients with relative access to intravenous (IV) rtPA, but distant from a center that could provide endovascular rescue therapy. Given the time-sensitivity of such interventions, it is important to minimize delays between IV and IA reperfusion treatments. Thus, a HEMS-delivered neuroprotective and reperfusion-mitigating strategy could potentially compensate for this delay, and help mitigate potential differences in outcome based on geographical location. 14 Also, HEMS provides an opportunity to help traditional tertiary-based acute stroke trials by expediting the informed consent process. Patients with stroke transported by HEMS who are incapacitated and unable to provide informed consent typically arrive to the tertiary center well before their relatives who use ground transportation.13,23 This temporal patient–surrogate dissociation inevitably results in either delays in enrollment, or ineligibility to enroll at all due to missing the time window. HEMS crews could significantly help this problem by screening and consenting surrogates and, therefore, enrolling subjects at the outside hospital ahead of their arrival to the tertiary institution. 23
The feasibility of HEMS-initiated research approach has been demonstrated in a single-center randomized controlled intervention pilot trial 23 in Iowa that may be generalizable to other academic-based helicopter services. The HEMS personnel from the University of Iowa showed an unanticipated degree of enthusiasm in becoming co-investigators in trials, including completing all the regulatory documents, training, and certification. 23 They also demonstrated an ability to screen patients using simple clinical and laboratory variables that are available at the time patients would be picked up at an outside hospital. 23 That included obtaining an accurate NIH Stroke Scale Score, 23 a finding that was later validated by an independent group. 45 The HEMS crews successfully obtained a signed consent for a low risk vehicle intervention for 52% of the approached subjects. The study also shows that the downtime of the outbound flight to pick up the patient can also be used to potentiate research. If the HEMS crews were successful in talking with the patient or family members about the study using the onboard 800 MHz radiophone before their arrival, the consent rate increased to 69% for a low-risk intravenous intervention. 23 This illustrates the benefit of advance notification about the study for promoting subsequent informed consent in a very time-pressured environment.
Another potential barrier to HEMS-based research, the oversight of institutional research board (IRB), was also addressed. We learned that the transfer of legal care to the tertiary emergency department occurs the moment the University based HEMS team arrives at the outside hospital and meets the patient. 23 Consequently, the University of Iowa IRB determined that research activities could also be initiated at that same time under the umbrella of the University IRB that supervises the emergency department. 23 In rural areas, HEMS services cover a large area with multiple community/critical access hospitals. Involving and certifying each of these institutions as research centers would be logistically problematic, if not impossible. Many of these small hospitals do not even have an IRB. Therefore, university-based IRB agreement is crucial for HEMS-based stroke research in order to ensure adequate subject protection. Because HEMS research is performed by a handful of experienced university-based HEMS crews that serve a large catchment area, it greatly facilitates maintaining their credentials and competence as co-investigators. 23
Based on this preliminary experience, and the accuracy of the diagnosis in this environment, inter-hospital HEMS provides a unique opportunity to test interventions to minimize penumbral expansion and reperfusion injury before arriving to the comprehensive stroke center (CSC). 23 It also provides an opportunity to test specific interventions for intracranial hemorrhages. Given the potential for interaction between the helicopter physical factors and reperfusion and BBB permeability, the ancillary care provided en route and the dosages of neuroprotective interventions might need to be adapted. 42
Summary/Conclusions
In the era of mechanical reperfusion, HEMS can be a powerful instrument for improving acute stroke delivery and research that is currently underutilized. The speed of HEMS may allow reperfusion for a large number of patients that would not have immediate access due to geography or traffic congestion. Also, HEMS critical early time period after a stroke where specific interventions to preserve penumbra and prevent reperfusion injury may have a significant influence on outcomes. The impact of physical factors generated by the helicopter on the ischemic brain needs to be studied. HEMS are also an opportunity to increase recruitment of patients in standard clinical trials. Addressing the HEMS stroke gap is necessary to homogenize the delivery of acute stroke care and research capabilities through all care settings, therefore minimizing disparities in outcomes based in geographical location.
Footnotes
Acknowledgements
We thank the AirCare crews from the University of Iowa for advancing stroke care and research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Ethical approval
Not applicable.
Guarantor
EL.
Contributorship
EL researched literature and conceived the study and wrote the first draft of the manuscript. All authors contributed to this review with substantial intellectual content, reviewed and edited the manuscript and approved the final version of the manuscript.