
Abstract
Objective
In large-vessel occlusion, endovascular therapy is superior to medical management alone in achieving recanalisation. Reducing time delays to revascularisation in patients with large-vessel occlusion is important to improving outcome.
Patients and methods
A campaign was implemented in the Central Denmark Region targeting the identification of patients with large-vessel occlusion for direct transport to a comprehensive stroke centre. Time delays and outcomes before and after the intervention were assessed.
Results
A total of 476 patients (153 pre-intervention and 323 post-intervention) were included. They were treated with either intravenous tissue plasminogen activator or endovascular treatment (alone or in combination with intravenous tissue plasminogen activator). Endovascular therapy patients’ median system delay was reduced from 234 to 185 min (adjusted relative risk delay 0.79 (95% confidence interval: 0.67–0.93)). The in-hospital delay was the main driver with an adjusted relative risk delay of 0.76 (confidence interval: 0.62–0.94), while pre-hospital delay was almost significantly reduced with an adjusted relative delay of 0.86 (confidence interval: 0.71–1.04). This was achieved without increasing the intravenous tissue plasminogen activator-treated patients’ delay. Significantly more patients treated with endovascular therapy in the post-interventional period achieved functional independence (62% versus 43%), corresponding to an adjusted odds ratio of 3.08 (95% confidence interval: 1.08–8.78).
Conclusion
Direct transfer of patients with suspected large-vessel occlusion to a comprehensive stroke centre leads to shorter treatment times for endovascular therapy patients and is, in turn, associated with an increase in functional independence. We recorded no adverse effects on intravenous tissue plasminogen activator treatment times or outcome.
Keywords
Introduction
In acute ischaemic stroke (AIS), reperfusion can be achieved with intravenous (IV) tissue plasminogen activator (tPA) 1 or endovascular therapy (EVT). 2 Both treatments are critically time dependent.3,4 In patients with a large-vessel occlusion (LVO) and severe neurological deficit, EVT is superior to IV tPA as successful recanalisation is achieved in 70–80% of EVT cases, 5 but only in 30% of IV tPA cases. 6 Delivery of EVT is challenged by transport of the patient to a capable facility, and clear pre-hospital and inter-hospital transport guidelines are essential to minimising time delays. With better logistics, treatment can be offered more rapidly and to more patients.7–9
The aim of the present study was to reduce system delay by educating and training medical dispatch staff and paramedics (emergency medical service, EMS) in recognising suspected LVO and by introducing subsequent direct transport to a comprehensive stroke centre (CSC). We wanted to shorten time to EVT (‘groin puncture’) accepting the risk of extending time delay to IV tPA treatment, since these patients could bypass a closer primary stroke centre (PSC). The effect of this intervention on time delays was followed for 18 months and compared with the 10 months leading up to the intervention.
Methods
Setting and design
The study was a population-based before-and-after study conducted in the Central Denmark Region among patients with AIS who were admitted for reperfusion therapy with IV tPA and/or EVT. The Central Denmark Region covers an area of approximately 13,000 km2 (5000 square mile) and has a catchment population of 1.3 million. In the Western part of the region, AIS is treated at a PSC with IV tPA capabilities. In the Eastern part of the region, a CSC has both IV tPA and EVT capabilities. The two centres are 120 km (75 mile) apart (see Figure 1).
Map of Denmark in left upper corner focusing on Central Denmark Region with the largest towns and the number of inhabitants. The total number of inhabitants is 1.3 million. The comprehensive stroke centre is marked by the white hospital in Aarhus in the Eastern part of the region. The primary stroke centre (PSC) is marked by the red hospital in the Western part, in the city of Holstebro. The distance between the two hospitals is 120 km (75 mile). If a patient living at the ‘X’ on the map suffers a stroke and is admitted to the PSC, he is subjected to a long transportation and in-hospital delay if endovascular therapy (EVT) is needed (black line). Bypassing (white arrow) would result in shorter delay to endovascular treatment (EVT).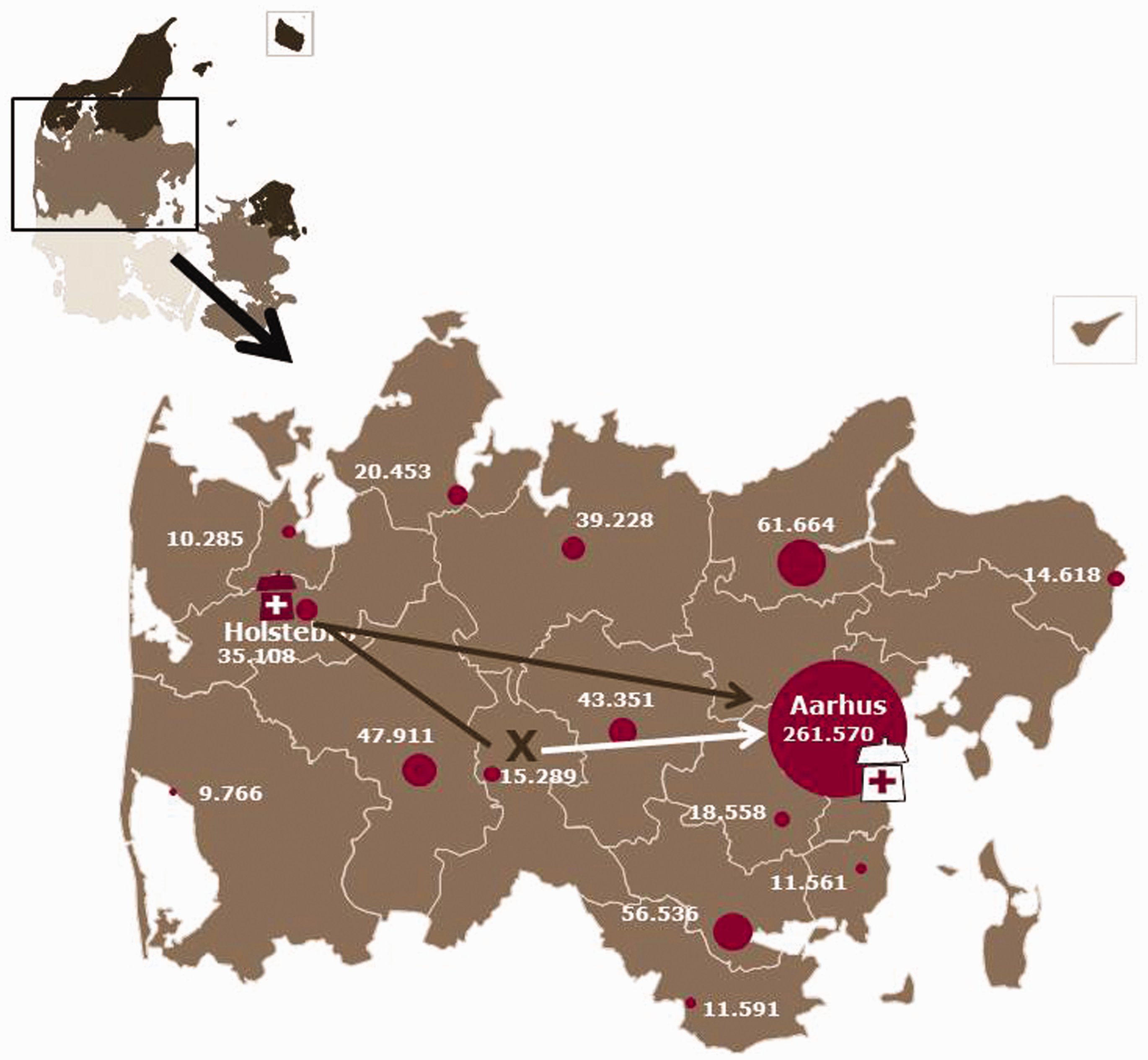
The study period was divided into a pre- (1 June 2011–31 March 2012) and a post-interventional period (1 April 2012–30 September 2013) reflecting the timing of the education, training and triage campaign.
The study was based on data obtained from the Danish Stroke Registry and the EMS. The Danish Stroke Registry is a clinical registry which holds data on patient characteristics and care, including IV tPA and EVT, for all acute stroke patients in Denmark. 10 The EMS holds pre-hospital data from all operating agencies. Unambiguous individual-level linkage between the databases used in the present study was possible using the civil registration number, a unique 10-digit personal identification number assigned to every Danish citizen. The study was approved by the Danish Data Protection Agency (record no. 1-16-02-440-13).
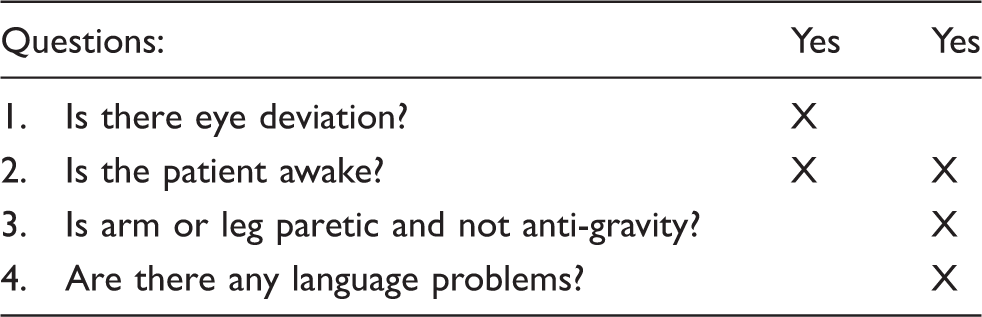
The screening tool that dispatchers and ambulance personnel used to screen for LVO (‘big stroke’). If questions 1 + 2 were answered positively or if questions 2 + 3 + 4 were answered positively, the patient was transported directly to the comprehensive stroke centre under suspicion of ‘big stroke’.
Study population
Excluded were self-presenters, patients without EMS data, patients referred from outside the region, patients without time data and AIS patients not treated with acute revascularisation therapy. A flow chart of the study population is presented in Figure 2. We identified a total of 476 eligible patients who received revascularisation therapy; 153 patients in the pre-interventional period and 323 in the post-interventional period.
Flow chart presenting study patient inclusion. DSR: Danish Stroke Registry.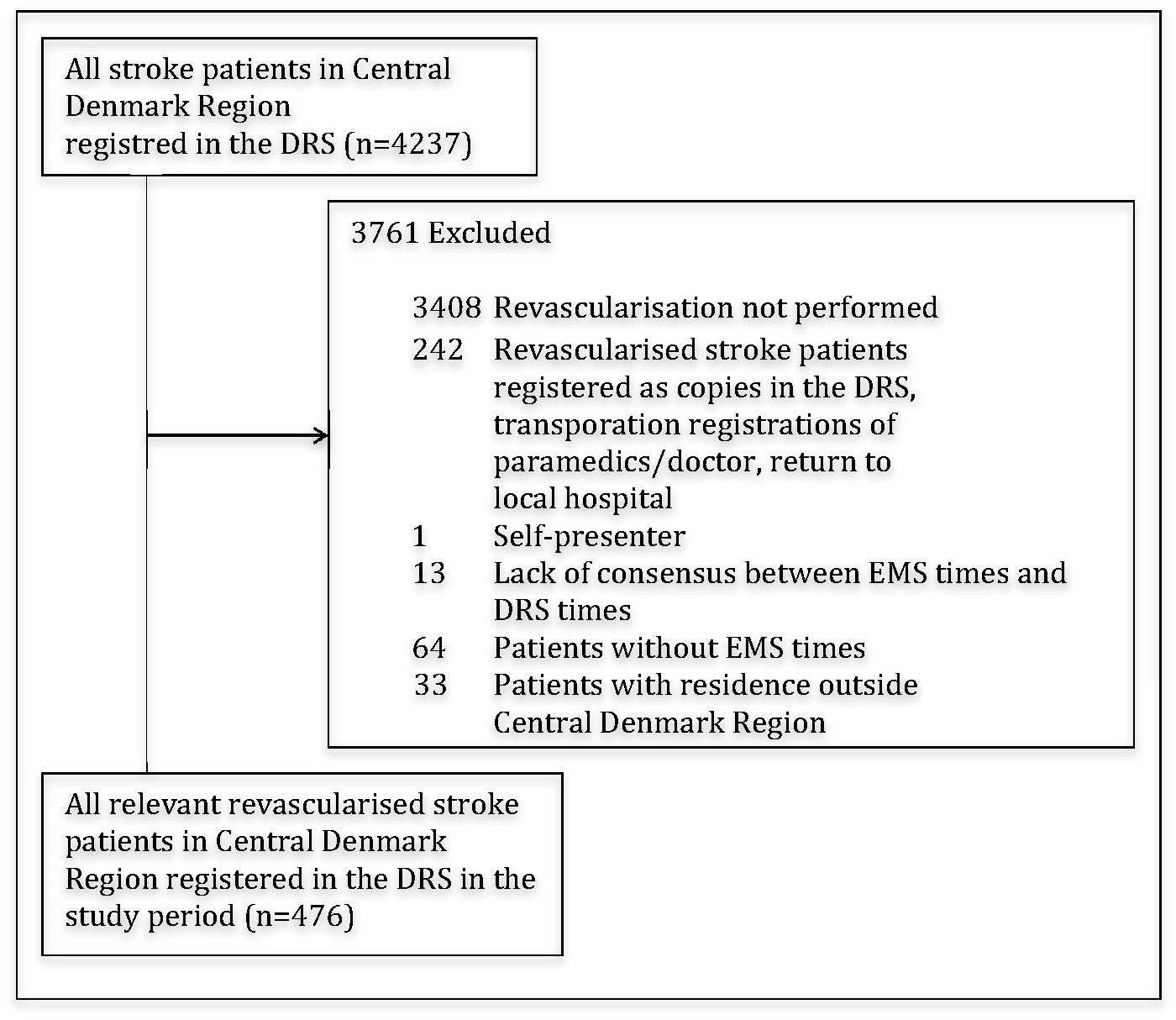
Patients were considered potentially eligible for IV tPA if treatment could be performed within a maximum of 4.5 h after symptom onset, blood pressure ≤ 185/110 mmHg, international normalised ratio ≤ 1.7 and after imaging had excluded intracranial bleeding or a very large infarct (more than a third of the middle cerebral artery territory). EVT was recommended in conjunction with IV tPA treatment if a proximal artery occlusion was seen (internal carotid artery, basilar artery, the main stem or second division of the middle cerebral artery), presenting National Institute of Health Stroke Scale (NIHSS) was at least 10, groin puncture could be made less than 6 h after symptom onset and the patient was living independently. The local guidelines for IV tPA and EVT treatment did not change during the study periods.
Outcomes
Patient delay is defined as the time period from symptom onset to the first contact to the EMS. Pre-hospital delay is the time period from the first EMS contact to arrival at the first hospital. In-hospital delay is the time period from arrival at the first hospital to initiation of IV tPA infusion (for IV tPA patients) or groin puncture for EVT patients, whether this was preceded by IV tPA or not. Note that for a LVO patient, in-hospital delay includes transfer from PSC to CSC. Pre-hospital and in-hospital delays are collectively referred to as system delay, while the whole period from symptom onset to treatment initiation is coined treatment delay.
For EVT patients admitted to the PSC, IV tPA was initiated before inter-hospital transportation (‘drip-and-ship’). This has been the standard procedure since 2010. The calculation of various delays was based on pre-hospital data registered by the EMS providers (Falck A/S and Response A/S, Aarhus, Denmark) and data registered in the Danish Stroke Registry.
The modified Rankin Scale (mRS) was assessed in the outpatient clinic at 90-day follow-up in both the pre-interventional and post-interventional group.
Statistical analysis
Dichotomous data are presented as percentages. Continuous variables are presented as medians with corresponding interquartile ranges (IQR). Patients were stratified according to type of reperfusion method (IV tPA and EVT alone or in combination with IV tPA, respectively). Time delays were compared using multivariable linear regression. A log transformation of the time delays was made in order to obtain normal distribution.
Logistic regression was used to calculate crude and adjusted odds ratios (OR) for a 90-day mRS score 0–2 comparing the post-interventional group with the pre-interventional group. In addition, a multivariate ordinal logistic regression was used to estimate the crude and adjusted OR of any improvement in mRS in the post-interventional group compared with the pre-interventional group. Adjustments were made for sex, age, baseline characteristics, admission NIHSS, distance from pickup address to the nearest revascularisation centre, type of revascularisation therapy, quarter (season) of year and hours stratified into four groups: 1: 24.00–05.59, 2: 06.00–11.59, 3: 12.00–17.59 and 4: 18.00–23.59. All statistical analyses were performed using Stata 13.0 (StataCorp, College Station, Texas).
Results
Characteristics of patients before and after the intervention.
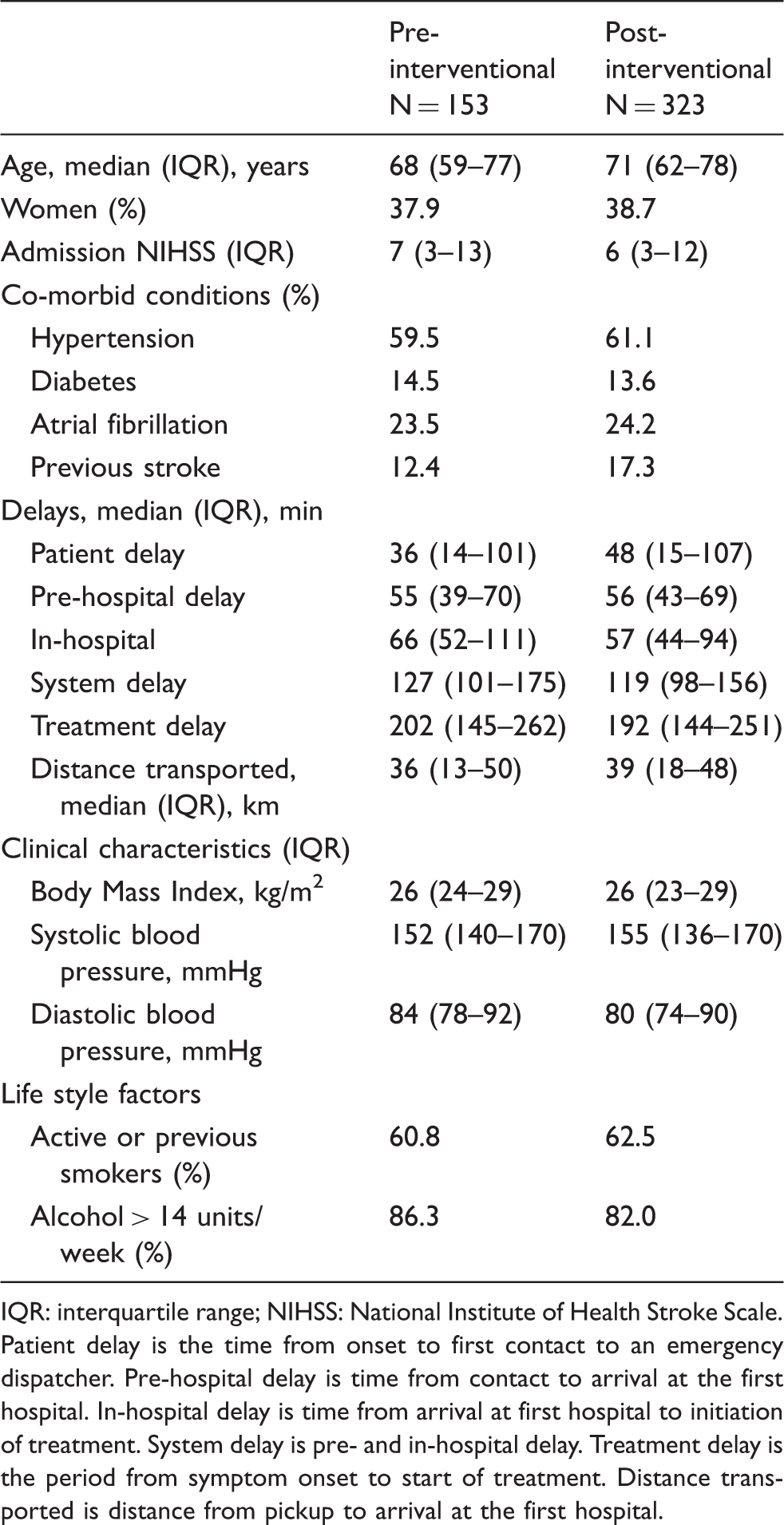
IQR: interquartile range; NIHSS: National Institute of Health Stroke Scale.
Patient delay is the time from onset to first contact to an emergency dispatcher. Pre-hospital delay is time from contact to arrival at the first hospital. In-hospital delay is time from arrival at first hospital to initiation of treatment. System delay is pre- and in-hospital delay. Treatment delay is the period from symptom onset to start of treatment. Distance transported is distance from pickup to arrival at the first hospital.
Time delays before and after the intervention for patients treated with endovascular therapy (EVT) alone or with intravenous (IV) tissue plasminogen activator (tPA) and IV tPA only.
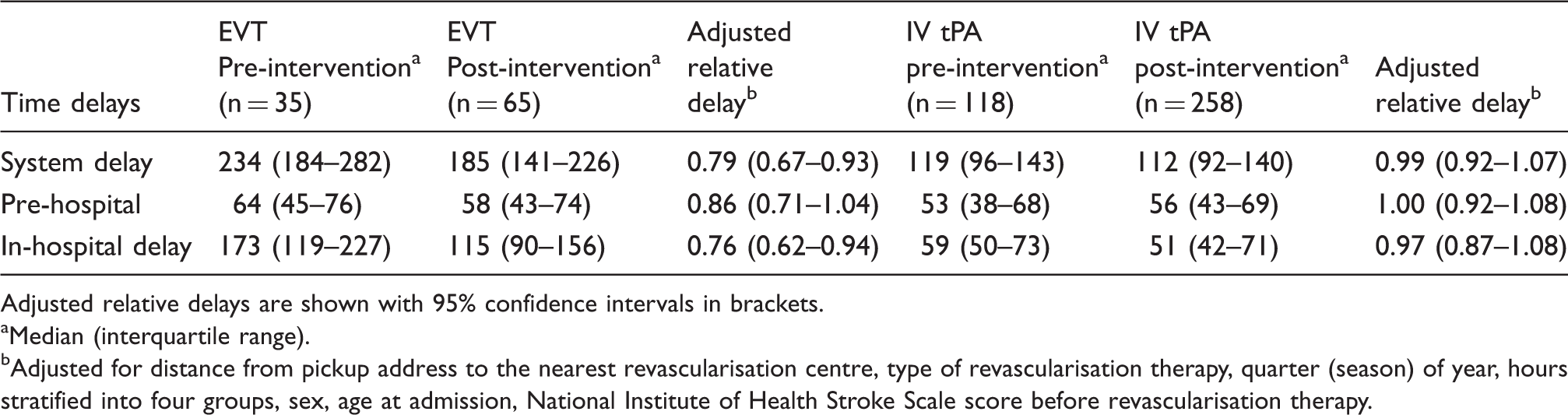
Adjusted relative delays are shown with 95% confidence intervals in brackets.
Median (interquartile range).
Adjusted for distance from pickup address to the nearest revascularisation centre, type of revascularisation therapy, quarter (season) of year, hours stratified into four groups, sex, age at admission, National Institute of Health Stroke Scale score before revascularisation therapy.
Reducing EVT patients’ delay could potentially increase delay in patients eligible for IV tPA through bypass of the PSC if LVO was suspected. However, the present study found no increase in either the pre-hospital or in-hospital delay for the IV tPA patients (adjusted relative delay 1.00 (95% CI: 0.92–1.08) and 0.97 (95% CI: 0.87–1.08), respectively). The rate of good outcome (mRS 0–2) among the patients who bypassed the PSC and were treated with EVT was not significantly different from the outcome of patients admitted from the catchment area of the CSC (p = 0.42.)
Percentage of intravenous (IV) tissue plasminogen activator (tPA) and endovascular therapy (EVT) treated patients achieving a modified Rankin Score (mRS) of 0–2 at 90 days after the stroke in the pre- and post-interventional period, respectively.
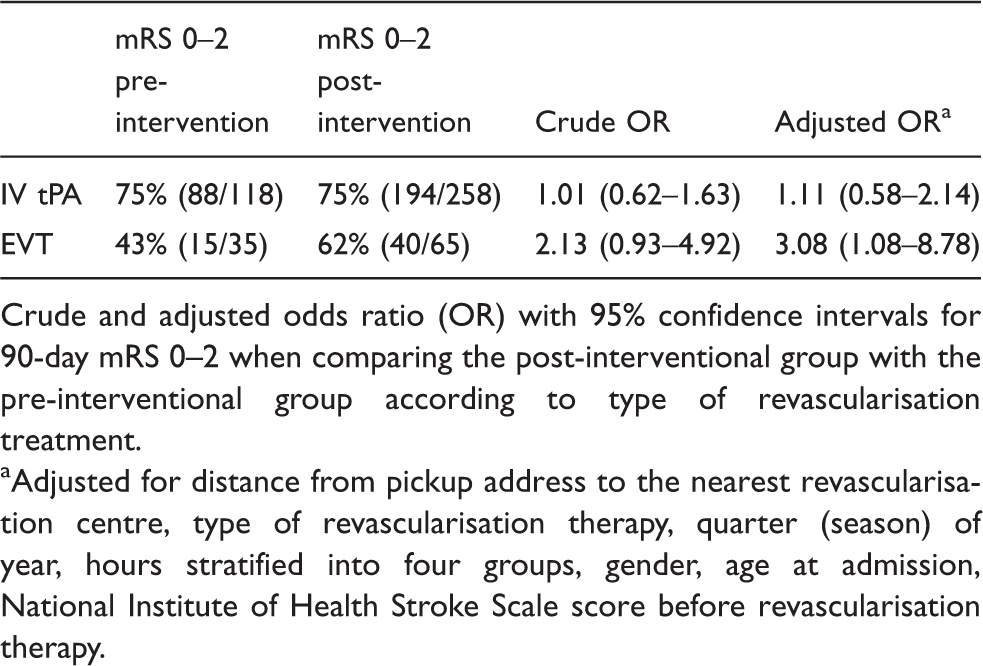
Crude and adjusted odds ratio (OR) with 95% confidence intervals for 90-day mRS 0–2 when comparing the post-interventional group with the pre-interventional group according to type of revascularisation treatment.
Adjusted for distance from pickup address to the nearest revascularisation centre, type of revascularisation therapy, quarter (season) of year, hours stratified into four groups, gender, age at admission, National Institute of Health Stroke Scale score before revascularisation therapy.
For patients treated with EVT, shift analysis using multivariate ordinal logistic regression showed a non-significant difference between the post-interventional and the pre-interventional group in terms of overall distribution of mRS scores; adjusted common OR 1.88 (0.88–4.02).
Figure 3 shows the pre- and post-interventional outcome.
Modified Rankin Scale at 90 days comparing the pre- and post-intervention group for patients treated with endovascular therapy alone or with intravenous tissue plasminogen activator. **Adjusted for distance from pickup address to the nearest revascularisation centre, type of revascularisation therapy, quarter (season) of year, hours stratified into four groups, sex, age at admission, total National Institute of Health Stroke Scale score before revascularisation therapy.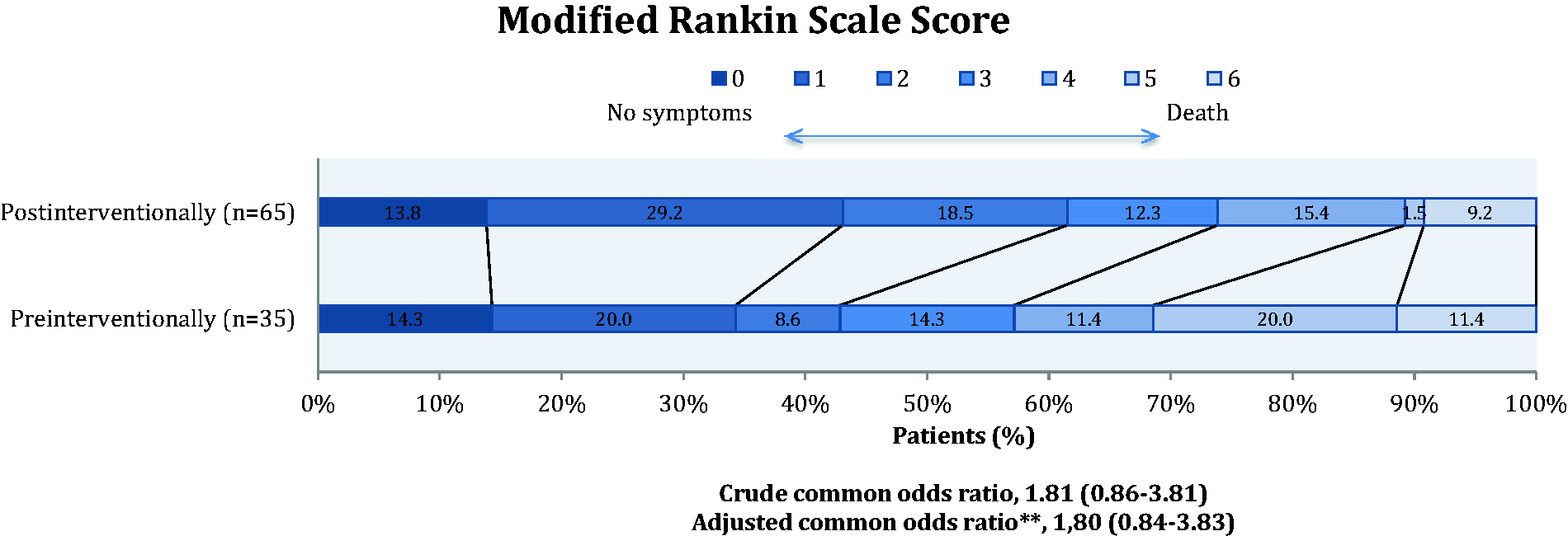
Discussion
Introduction of a simple pre-hospital stroke triage and education and training of EMS personnel allowing them to recognise LVO was associated with a significant reduction in system delay. This reduction was driven largely by a reduction in in-hospital delay. Pre-hospital delay did not change significantly. Since in-hospital delay is time from arrival at the first hospital to groin puncture for EVT patients, direct transfer to CSC would result in reduction in in-hospital delay. The reduction in delay for EVT patients was achieved without significantly prolonging the delay for IV tPA patients who bypassed the PSC due to suspicion of LVO. The reduction in delay for EVT patients was associated with a significant increase in the proportion of patients reaching functional independence after the stroke without changing functional independence in patients eligible of IV tPA only.
The saying ‘Time is brain’ is true for all strokes, 11 but especially so for LVO, the most severe form of stroke.12,13 The chance of a good outcome is strongly associated with time delay before treatment. 4 Furthermore, EVT recanalises a LVO more successfully than IV tPA alone, and therefore early triage to a CSC is critical.
Patient delay is a significant source of lost time for AIS patients. Half of the pre-hospital delay is related to hesitation in seeking medical assistance after symptom onset. 14 Moreover, activation of services other than EMS further delays care. A study from the United Kingdom showed a median 123 min delay from symptom onset to arrival at the hospital for those calling the EMS, which should be compared with a median 432 min delay for patients who first consulted their primary care physician. 15 In Japan, a public campaign focusing on stroke symptoms reduced pre-hospital delay but did not increase the proportion of patients treated with IV tPA. 16 Predictors of a patient- and pre-hospital delay include severe stroke, lower age and admission by EMS.17,18
In case of suspected LVO, it is more likely that EMS will be notified by a bystander than via initial contact to the primary care physician. 19 In an effort to reduce pre- and in-hospital delay, an ambulance fitted with a computed tomography scanner was launched in Berlin. 20 IV tPA can thus be given quickly and transportation to a CSC can be initiated more rapidly. This solution is expensive and might only be cost effective in densely populated areas characterised by high stroke rates. 21
Pre-hospital scoring systems identifying LVO already exist22,23 but only the rapid arterial occlusion evaluation (RACE) scale 24 has been evaluated in the pre-hospital setting. Still, the RACE scale was not valuated in 60% of patients by EMS, possibly because of its complexity. We developed a simpler triage protocol (Table 1) identifying LVO in collaboration with EMS to ensure ease of use, minimal time consumption and the scale’s usefulness over the phone for the dispatcher. After our study was initiated, the Cincinnati Prehospital Stroke Severity Scale was introduced. 25 There are similarities between this scale and ours. One such similarity is the item eye turning as the underlying pathophysiology is an extensive lesion including cortical regions involving the frontal eye field. This scale has not been tested in pre-hospital settings yet. Future studies are necessary to develop and examine which scoring system is the most sensitive for identifying patients with LVO while still being user friendly in the pre-hospital setting.
A quality improvement initiative aiming at reducing door-to-needle time (in-hospital delay) was successful and associated with an increase in the proportion of patients with door-to-needle times of 60 min or less (29.6 to 53.3%), a lower in-hospital mortality, reduced incidence of symptomatic intracranial haemorrhage and an increase in the percentage of AIS patients who were able to be discharged to home. 26 In this initiative, one of the strategies during both time periods was pre-notification of the hospital. In our setting, we advocate that informing the entire stroke team that a ‘big stroke’ is arriving be part of the routine practice.
The intervention was focused on the pre-hospital setting, and in-hospital delay was significantly reduced in the post-intervention period. As mentioned, direct transfer to CSC would result in reduction of in-hospital delay, since this delay is measured from admission to the first hospital to final treatment. The CSC has performed EVT since 2004 and since 2010 with 24/7 coverage, so it is unlikely that a training effect reduced in-hospital delay.
An important aspect of our study was its focus on correct selection and visitation of patients with suspected LVO to a CSC. This approach could have prolonged transport (pre-hospital delay) for those patients who needed treatment with IV tPA only if they bypassed a more closely located PSC. However, this was not the case since treatment delay for the IV tPA patients was not changed significantly.
The reduction in system delay for patients undergoing EVT translated into a significantly improved functional outcome at 90 days. This is in line with the results reported in the newly published, successful EVT trials which focused on achieving better outcomes by shortening treatment delay.5,27,28 The findings of these studies all suggest that acceleration of treatment time is essential in gaining a better prognosis. The distance the patients were transported to the first hospital did not seem to change in the post-intervention period, but looking at the map, Figure 1, it can be seen that for many patients the distance to the first hospital is not different, but the bypass patients are saved a long transportation to the CSC after initial admission at the PSC.
An important limitation of our study is the comparison of sequential periods because the two time periods are sensitive to confounders that evolve over time. The procedures related to door-to-needle time are smoothed over time, and that might be part of the reason for the shorter in-house delay that we recorded in the latter time period. We support a randomised approach as seen in cardiology. 29 Also, the used questionnaire has not been validated yet, but this is planned as a part of an ongoing project. The available scales were not suitable for use by a dispatcher.
In conclusion, our study provides proof of concept that a triage system designed to identify patients with LVO can shorten system delay for EVT patients significantly, particularly the in-hospital delay, resulting in a better outcome. The study also demonstrates that this can be achieved without increasing delay for the IV tPA group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a grant from TrygFonden Denmark. Tryg Fonden Denmark had no influence on the study design, data collection, presentation of data or the conclusions made.
Ethical approval
N/A
Informed consent
The study was approved by the Danish Data Protection Agency (J. No. 1-16-02-440-13). Ethical approval was waiver since this is not required using register data.
Guarantor
CZS
Contributorship
GA, SPJ, CZS conceived the study. NFM collected data with MR and MSA. NFM drafted the first manuscript with CZS and SH. Statistical analysis was done by NFM and SPJ. All authors reviewed and edited the manuscript and approved the final version.