
Abstract
Background & Aims
Early intervention efforts can be transformative for young children with autism, and parent involvement is an increasingly common component of many contemporary treatment models linked to enhanced long-term social communication and developmental outcomes. However, Spanish-speaking families face language barriers that limit opportunities to be trained in these strategies, directly contributing to disparities in their children's developmental outcomes. This study aims to address this barrier by exploring the feasibility, acceptability, and preliminary efficacy of a Spanish-translated and adapted pivotal response treatment (PRT) early intervention model.
Methods
Using a multiple baseline across participant experimental design, the primary objective of this investigation was to evaluate the impact of ongoing participation in a Spanish PRT workshop on parent fidelity (mastery) of treatment implementation and child verbal responses using behavioral coding and parent-report measures. The study included three children with autism aged 18–60 months and their caregiver(s). Parents completed questionnaires, four PRT instructional lessons, and six in-person coaching sessions. Parent–child interaction videos were recorded at intake and after each in-person session to monitor participant process.
Results
All participants met fidelity of implementation criteria (>80%) for the PRT strategies, demonstrating the ability to successfully implement the core intervention components. Parents also reported improvements in their self-perceived (a) comprehension of the PRT principles and (b) confidence in applying them effectively. Lastly, children demonstrated improvements in the frequency of their verbal responses.
Conclusions & Implications
These results suggest that the Spanish adaptation of PRT can effectively teach parents to understand and implement basic PRT components and facilitate language development in their autistic children.
Keywords
Early intervention is critical for targeting core areas of development for autistic children, including social communication, cognitive, and adaptive living skills. The current gold standard for early autism intervention, known collectively as Naturalistic Developmental Behavioral Interventions (NDBIs; Schreibman et al., 2015), refers to interventions for autistic children that occur in natural settings (i.e., play and daily routines), utilize naturally occurring learning contingencies to teach children developmentally appropriate skills, and incorporate parent/caregiver(s) in the therapeutic model. Recent meta-analyses of NDBIs found significant positive effects on social communication, play, and cognitive skills of children with autism when compared to other intervention approaches (Sandbank et al., 2020; Steinbrenner et al., 2020).
Pivotal Response Treatment (PRT)
PRT is an empirically validated NDBI that combines motivational strategies and behavior principles to target social communication skills and language in autistic children (Koegel & Koegel, 2019; Koegel et al., 2003). PRT is considered by the National Clearinghouse on Autism Evidence and Practice to be a Manualized Intervention Meeting Criteria for Evidence-Based Practice (Steinbrenner et al., 2020).
PRT is designed to be implemented in natural environments (i.e., home, school, and community settings) and woven into a child's natural daily routines (i.e., playtime, bedtime, meals, and bath time). It uses child-selected play items and/or activities to motivate children to verbally communicate and request items/activities by using natural exchanges and incentives. In other words, a child is incentivized to use language to gain access to highly desirable items, creating an opportunity for them to talk and use their language. Furthermore, by creating these language opportunities in natural contexts, it allows the child to quickly learn to use language and other social skills across multiple settings. Research indicates that PRT leads to improvements in language and social exchanges in autistic children (Gengoux et al., 2015, 2019; Gillett & LeBlanc, 2007; Ona et al., 2020).
A growing body of research demonstrates that PRT produces robust improvements in proximal language outcomes, such as spontaneous verbal initiations, mean length of utterance, and functional utterances coded during parent–child or clinician–child interactions (see Uljarević et al., 2022 for a recent review and meta-analysis of broad PRT outcomes). Randomized clinical trials (RCTs) and multiple baseline studies consistently report significant increases in these proximal communication behaviors following PRT (Barrett et al., 2020; Gengoux et al., 2019; Hardan et al., 2015; Mohammadzaheri et al., 2014; Vernon et al., 2012). In contrast, evidence for distal outcomes such as standardized language assessments and parent-report measures is more variable. Some studies have documented collateral gains on parent-reported vocabulary or adaptive communication measures (Gengoux et al., 2019; Hardan et al., 2015; Vernon et al., 2019) and receptive vocabulary/language tests (Vernon et al., 2019). Others have found limited or nonsignificant changes on broader standardized language measures (Gengoux et al., 2019; Vernon et al., 2019). This pattern suggests that while PRT reliably strengthens targeted, session-level communication skills, translation of these gains to broader, distal language measures may require longer-term treatment. Long-term clinical trials of similar NDBIs that use PRT as a foundational intervention framework, such as the Early Start Denver Model (ESDM; Dawson et al., 2010), have yielded desired distal language improvements.
Importantly, PRT involves parent/caregiver(s) as active agents in the intervention process. Parent involvement is a crucial component for children with autism because it increases their daily exposure to evidence-based strategies, supports skill generalization, and is linked with more favorable developmental outcomes (Bearss et al., 2015; Licona et al., 2022; McConachie & Diggle, 2007). Beyond benefits for children, parents themselves experience reduced stress, improved mental health, and greater self-efficacy when they are actively engaged in therapy efforts (Matson et al., 2009; Tarver et al., 2019). These findings are congruent with theories of parental self-efficacy (PSE; Ardelt & Eccles, 2001; Coleman & Karraker, 2003; Jones & Prinz, 2005) that espouse that parents who feel efficacious are more likely to engage in promotive parenting strategies. In PRT, parents acquire conceptual knowledge of effective strategies, learn to build closer interpersonal connections with their child, and use practical motivational components through didactic training, ongoing discussions, and live practice with their child, while receiving in vivo feedback from a trained clinician. These drivers align with current theories of empowerment (Christens, 2012; Zimmerman, 2000) that assert that there are four key components that drive empowerment: emotional empowerment (self-perceived ability to enact change), relational empowerment (leveraging a strong interpersonal partnership—in this case, an emerging parent–child connection), cognitive empowerment (skills and knowledge needed to act), and behavioral empowerment (actual actions needed to make the desired changes). Parents become efficacious and empowered while becoming highly proficient in PRT, ultimately resulting in improved language outcomes for their child (Koegel et al., 2003; Ona et al., 2020; Verschuur et al., 2014).
Underrepresentation of Spanish-Speaking Families in Parent-Mediated Efforts
The emphasis on parent involvement in early intervention, however, raises critical questions about equity and accessibility for non-English speaking families. Among the 35.8 million Spanish-speaking Latinos in the US, only 67% of Latino adults are proficient in English, making language barriers a significant obstacle in accessing parent-mediated interventions, such as NDBIs, for Spanish-speaking Latino families (Guerrero & Sobotka, 2022; Krogstad et al., 2015; Lim et al., 2021; Pew Research Center, 2021; St. Amant et al., 2018; Yu et al., 2004). Additionally, Spanish-speaking parents report feeling invalidated and dismissed when expressing concerns about their child's development and noted feeling pressure to “fight” for early intervention services due to language barriers (Malik-Soni et al., 2022; Pickard et al., 2024; Stahmer et al., 2019). The scarcity of Spanish-speaking intervention services limits parents’ ability to fully understand their child's needs and actively engage in the intervention process, ultimately impacting their ability to participate in their child's care.
The discrepancies that Spanish-speaking families face also extend into early intervention clinical research opportunities. For example, most autism intervention trials exclude Spanish-speaking families, often due to limited availability of bilingual clinical researcher teams, perceived challenges in recruitment, inconsistent availability of Spanish-language outcome measures, or simply to make trials easier to implement, exacerbating the limited access to well-established, effective intervention support for Spanish-speaking families (DuBay, 2022; Pickard et al., 2024). Given the role that parents and caregivers play in the success of NDBIs, it is critical to prioritize efforts to promote accessibility across linguistically diverse communities to ensure that all families can benefit from the life-changing impact of these models.
Linguistic & Cultural Adaptations of Autism Interventions
Spanish-speaking caregivers identified several possible solutions to alleviate the challenges associated with language barriers, including increasing the availability of interpreters, strategically hiring more bilingual service professionals and staff, and crafting all written clinical materials in Spanish (Flower et al., 2021). Language adaptations, particularly direct linguistic translations, can improve a family's likelihood of pursuing treatment, enhance intervention retention rates, and improve both acceptance of the intervention and understanding of a child's disability (Martinez-Torres et al., 2021). However, linguistic translation alone may be insufficient, and cultural adaptations such as tailoring the intervention to align with the values, norms, and lived experiences of the target population may further improve treatment acceptability and outcomes (Santarelli et al., 2001).
To this end, efforts have been made to adapt NDBIs across various linguistic and cultural settings. For example, Project Improving Parents as Communication Teachers (ImPACT; Ingersoll & Dvortcsak, 2010) has shown feasibility and effectiveness for children with social communication delays who speak a non-English language in countries, including India, the Netherlands, Zambia, China, Spain, and Iran (Akhani et al., 2021; Bejarano-Martín et al., 2022; Pierucci et al., 2023; Sengupta et al., 2020; Zwitserlood-Nijenhuis et al., 2023). More recently, a study piloting a Spanish-translated adaptation of Project ImPACT found high rates of treatment completion and caregiver satisfaction in addition to improvements in child social communication skills and caregiver self-efficacy. This study also documented real-time cultural adaptations, for example, integrating family centered cultural values into the intervention materials (Pickard et al., 2024). Other adaptations included tailoring Spanish dialect and metaphors to families’ countries of origin, incorporating cultural values such as familismo into sessions, and collaborating with extended family members in goal setting and practice. Similarly, the ESDM (Dawson et al., 2010) has also been culturally adapted in various countries, including India, China, Austria, and Italy (Colombi et al., 2018; Holzinger et al., 2019; Sengupta et al., 2020; Xu et al., 2018). In these studies, ESDM was modified by translating and adapting materials into the local language, embedding culturally familiar routines (e.g., play activities, songs, and foods), and simplifying session structure. These findings suggest that culturally and linguistically adapted parent-mediated interventions may not only improve access and acceptability across linguistically diverse individuals but also enhance caregiver self-efficacy and empowerment by increasing comprehension, relevance, and confidence in implementation.
While PRT early intervention exposure is associated with significant developmental benefits, the efficacy of this model, translated and adapted for delivery in Spanish, has yet to be investigated. A Spanish adaptation of PRT would bridge this language gap and empower Spanish-speaking caregivers with strategies to help their autistic children improve social communication skills.
Current Study
The primary objective of this study was to assess the acceptability, feasibility, and preliminary efficacy of a Spanish-language version of PRT for Spanish-speaking families, with a specific focus on both linguistic and cultural adaptations. Specifically, we examined the impact of Spanish PRT on parent fidelity of implementation (i.e., the extent to which they learn how to properly implement PRT) and on changes in child communication. We hypothesized that Spanish PRT would be acceptable, feasible, and efficacious for Spanish-speaking parents as measured by parent report and observed parent implementation of PRT skills. We further hypothesized that parents would demonstrate increased PRT fidelity and self-efficacy and that children would show corresponding improvements in language skills, as measured through behavioral observations.
Method
Participants
Participants in this study included three children (aged 45, 49, and 52 months) and their caregivers. All participants were recruited through a combination of targeted social media advertisements, emails to autism providers and clinics, and distribution of fliers in public locations (e.g., libraries and community centers). Recruitment materials were distributed and posted in both English and Spanish to allow a wider range of opportunities for individuals to learn about the study. This would allow English-speaking individuals to share the study information with Spanish-speaking families. Despite both English and Spanish recruitment materials, the remaining study components were conducted only in Spanish, including the screening process, informed consent, intake, intervention, and questionnaires.
The inclusion criteria included (a) parent concerns about child's language development; (b) a child's chronological age between 18 and 60 months; (c) a clinical diagnosis of Autism Spectrum Disorder; (d) Spanish as the parent/caregiver(s) primary language; (e) location within one-hour (∼40 miles) of the University of California, Santa Barbara and (f) access to a smartphone or computer to access online sessions and record parent/child videos. Parents could not participate if they had had prior professional training in PRT or another NDBI. The first three participants to meet the inclusion criteria were included in the study. Table 1 provides more detailed demographic information about the three child and caregiver participants, along with clinical baseline measures.
Descriptive Intake Data for Participants.

Note. CDI = communicative development inventories; SRS-2 = social responsiveness scale, second edition.
For families with two parents or caregivers, both adults were invited to attend the entirety of the education program; however, only the parent who identified as the primary caregiver was formally enrolled in the project and received direct training in the Spanish PRT intervention, submitted parent–child videos, and completed all parent forms.
Dyad 1
Child 1 was a 4-year-old Latina female who participated in the study with her 31-year-old biological mother. This child was diagnosed with autism and global developmental delay at 36 months and was receiving applied behavioral analysis and speech therapy services at the start of this intervention. She lived with her biological mother, father, and two older sisters. Child 1 and her mother attended all in-person coaching sessions at the University of California, Santa Barbara. They were occasionally accompanied by the child's biological father. On the communicative development inventories (CDI), Child 1 scored below the first percentile for Phrases Understood, 48th percentile for Understands and Says Vocabulary, and eighth percentile for Gesture Use. On the Social Responsiveness Scale, Second Edition 2 (SRS-2), Child 1 showed a moderate elevation in social communication challenges (t-score = 71) and restricted/repetitive behaviors (t-score = 75).
At intake, Child 1 was disengaged from her mother and preferred to play independently. Specifically, she was not observed to make eye contact or verbally engage with her mother during play. During baseline sessions, she displayed a calm and quiet demeanor. However, when her mother attempted to get involved in her play or played with a toy of her interest, Child 1 would become visibly upset and begin whining and crying. Her language production was characterized as primarily minimally verbal with occasional single-word utterances (e.g., “siéntate” [“sit down”] and “abre” [“open”]). Child 1's behavioral observations were consistent with the mother's reporting on standardized assessments.
Dyad 2
Child 2 was a 3-year-old Latino male who participated in the study with his 29-year-old biological mother. He was diagnosed with autism at 36 months and was not currently receiving any services or participating in interventions at the start of this research study. He lived with his biological mother, paternal grandmother, and younger sister. The research team conducted five of the six in-person sessions at a local park near Child 2's home because his mother did not drive. The intake and one intervention session were conducted at the University of California, Santa Barbara, when the child's aunt was available to drive them. On the CDI, Child 2 scored in the 99th percentile for Phrases Understood, 94th percentile for Vocabulary, and 80th percentile for Gesture Use. However, the SRS-2 indicated moderate social communication difficulties (T-score = 70) and restricted/repetitive behaviors (T = 72).
At intake, Child 2 displayed high levels of energy and was observed to run around the playroom, turn the lights off, throw toy items on the ground, and run out of the playroom. He moved quickly between toys and activities and did not engage in reciprocal play sequences with his mother. His mother was observed to follow him around the playroom and ask him questions about his play. He never responded to her questions or play bids. Child 2 was observed to engage in repetitive play sequences with a small beach ball as he repeatedly blew up the ball, put it near his right ear, and squeezed the air out of the ball. Furthermore, his language production was characterized as primarily one-word speech with occasional two-word phrase utterances (e.g., “allí esta” [“It's right there”], “sí” [“yes”], and “azul” [“blue”]) with occasional utterances of complete sentences (e.g., “No ma, esta es mía.” [“No mom, this one is mine.”]). Despite the mother reporting strong language abilities on the CDI, behavioral observations during sessions were more consistent with single-word use (and occasional chunked word combinations), highlighting a discrepancy between parent report and clinician observations.
Dyad 3
Child 3 was a 4-year-old Latino male who participated in the study with his 37-year-old biological mother. He was professionally diagnosed with autism at 36 months and was receiving speech therapy at the start of this intervention. He lived with his biological mother and father, two older siblings, and one younger brother. The research team conducted all in-person coaching sessions at a local park, near the family's home, to address transportation barriers. His mother indicated no clinically significant concern regarding his social communication on the SRS-2 (total T-score = 46), and she endorsed strong language skills on the CDI (99th percentile for Phrases Understood, 77th percentile for Vocabulary, and 94th percentile for Gesture Use). However, based on the clinician's clinical observations during the intake, the client demonstrated clear, clinically significant social communication difficulties consistent with autism, including limited eye contact, repetitive play sequences, and limited play initiations with the mother. Therefore, it is likely that the mother's reporting on baseline measures is an overestimation of the child's current language and social abilities and a minimization of any autism-related vulnerabilities.
At intake, Child 3 was observed to be calm and agreeable to all the mother's play suggestions. Although he was responsive to her play bids, his eye contact was limited, and he did not initiate any play sequences with her. His language skills were characterized as primarily phrase speech with occasional complete sentences (e.g., “El grande” [“the big one”], “Una, dos, y tres!” [“one, two, three”], and “Quiero esa” [“I want that one”]), although he demonstrated significant pronunciation challenges, making it difficult to understand him at times. Due to the mother's work schedule and the child becoming sick during treatment, the family completed all three of the instructional lessons but only completed four of the six in-person coaching sessions, ultimately completing 80% (8 of the 10) of the intervention before discontinuing the study.
Research Design
A multiple baseline across participant design was used to assess the preliminary efficacy of this brief 10-session Spanish PRT program by examining the functional relationship between PRT session completion and parent fidelity mastery. In the baseline phase, participants were assigned to either 3, 5, or 7 baseline probes in which parent–child play videos were captured to measure parent skills prior to the start of the PRT program (see procedures for more specifics on the videos). All participant families then completed the intervention phase and recorded additional parent–child videos.
Procedures
Participant Screening
Participants completed an online interest/screening questionnaire to determine initial study eligibility. In the questionnaire, parents answered a series of questions related to the eligibility criteria outlined previously in the participant section. Once the questionnaire was complete, the research team followed up via phone to either confirm eligibility and schedule the intake or to inform families that they did not qualify for the study based on their responses. A total of four families expressed interest in the study by completing the initial screening questionnaire. However, one family was excluded because the child fell outside the eligible age range; therefore, only three families signed consent and participated in the program. Active recruitment occurred over an 8-month period. Recruitment included sharing study details with Spanish-speaking community providers (i.e., pediatricians, psychologists, therapists, and teachers), posting flyers in predominantly Spanish-speaking neighborhoods, presenting at bilingual community events (e.g., libraries and community centers), and distributing information through social media and parent networks (e.g., Facebook parent groups).
Intake Session
During the intake session, researchers reviewed the study consent form with parents and discussed confidentiality limits and the voluntary nature of the study. Once the consent form was signed, researchers randomized the participant into a baseline condition and collected the first 5-min video of the parent and child playing together (see Baseline Parent–Child Play Video for more information). The parents were then asked to complete the following questionnaires during the intake session: demographics questionnaire, the MacArthur-Bates CDI—Primeras Palabras y Gestos Inventario 1 (Fenson et al., 2007), the SRS-2 (Constantino & Gruber, 2012), the Spanish Preschool Form, and a PRT Self-Efficacy Scale. The CDI and SRS-2 were used to characterize participants’ language and autism symptoms. At the end of intake, the second 5-min baseline video was collected.
Baseline Parent–Child Play Videos
Each family submitted 5-min baseline play videos using a secure box link for the remaining videos that were not collected during the intake session. Consistent with a multiple baseline experimental design (Gast et al., 2018), each family submitted a different number of baseline videos based on randomization (i.e., 3, 5, or 7). Parents were instructed to upload no more than two videos per day, to ensure adequate representation of child behavior across different times and contexts. For each baseline video, the primary caregiver was instructed, in Spanish: “For the next 5 min, please play with your child as you typically would at home. Your child is free to choose any activity or toy. We will let you know when the 5 min are up.” When families recorded the videos on their own (i.e., not in the clinic), they were given additional guidance to (a) remain indoors, (b) both parent and child should remain in the frame at all times, (c) minimize distractions (i.e., television in background and siblings joining), (d) keep track of video recording time, and (d) if possible, have a second person record the video to ensure both the parent and child stayed in view. Once parents completed the intake and submitted all baseline videos, they scheduled their online and in-person intervention sessions (i.e., instructional and coaching sessions).
Videos collected during the intervention phase were recorded by the lead research team member during in-person coaching sessions. The instructions for these videos were slightly modified and still delivered in Spanish: For the next 5 min, please play with your child using the strategies you are learning in this program. Your child is free to choose any activity or toy. We will let you know when the 5 min are up. All families received the same video recording instructions, regardless of baseline video randomization.
Spanish Cultural Adaptation and Translation of the Intervention
The instructional procedures and materials used in the intervention were culturally adapted and translated into Spanish by the lead author, a fluent and native Spanish speaker with lived experience in Hispanic/Latino culture, to ensure accuracy and cultural relevance of the Spanish-adapted program. Cultural and linguistic adaptation was accomplished in a meticulous, iterative process:
Each core PRT lesson (focused on a specific behavioral component of the intervention) was carefully reviewed. The researcher identified overlap between each core lesson and existing cultural values (Edwards & Cardemil, 2015; Lopez et al., 2023). For example, Familismo, or a strong emphasis on family relationships and interdependence, was used to center the parent–child relationship as the primary mechanism of change. Personalismo, or the importance of warm personal social relationships, was used to modify the procedures to focus on parental engagement and warmth as a driver of child responsiveness. Respecto, or an emphasis on respect for parents, elders, and authority figures, was used as a means to teach contingency so that children must make a polite request to receive the items they would like from their parents. The researcher identified ways to incorporate common Hispanic/Latino family activities, routines, play materials, and even food into the intervention process. This included using images of characters and people that reflect the appearance of Latino families. Additionally, in one of our teaching examples of an ABC sequence, familiar foods such as tortillas and plantains were incorporated to make the example culturally relevant and engaging. Cultural and linguistic relevance was further established by incorporating familiar examples, metaphors, and communication styles reflective of Hispanic/Latino families. For example, the Antecedent–Behavior–Consequence (A–B–C) acronym was adapted to the Antecedente–Comportamiento–Consecuencia (A–C–C) model to ensure linguistic relevance in Spanish. Once adapted and translated, the materials were reviewed and edited by two other fluent Spanish-speaking members of the research team to refine the cultural adaptations and translations. The team utilized the English–Spanish Glossary of Behavioral Terms as a resource to standardize the translation of common behavioral terminology, ensuring consistency and clarity (Virues-Ortega et al., 2014). This glossary was put together by fluent Spanish-speaking individuals from various Spanish-speaking countries and dialects, making it a comprehensive and inclusive resource for addressing linguistic diversity. During program implementation, parents participated in an informal iterative feedback process in which they were asked if the materials were clear, aligned with family routines and values, and if they had any questions, providing ongoing opportunities for the research team to further refine the adapted PRT model, address potential misunderstandings and misalignments, and improve the clarity of the material.
Spanish PRT Parent Workshop
The Spanish PRT intervention consisted of 10 one-hour-long sessions over a 3–4-week period. Each week began with a one-hour-long parent-only instructional session (i.e., sessions 1, 4, and 7) that focused on providing psychoeducation and PRT training to the parent utilizing a didactic approach. These sessions were led by a fluent Spanish-speaking clinician. The training material was adapted from the PRT Manual: Evidence-Based Early Intervention for Children With Autism (Vernon, 2020)[9] into a series of digital slideshow presentations that highlighted visual depictions of all PRT principles and intentionally used minimal text to reduce potential literacy barriers for parents. Although parent literacy level was not formally assessed in this study, the research team made this design choice as a proactive accessibility strategy, recognizing the variability in literacy levels in Spanish-speaking communities (Leyva et al., 2005; Reese et al., 2008; Yin et al., 2012). Instructional sessions were conducted virtually to reduce the burden of families having to travel to the clinic or arrange childcare.
The remaining sessions (i.e., sessions 2, 3, 5, 6, 8, and 9) were live in-person coaching sessions and consisted of a fluent Spanish-speaking training clinician, the parent, and the child practicing PRT in-person, either at our autism center, the family's home, or in a community setting (i.e., park), depending on the family's personal preference. During these sessions, the lead clinician provided a summary of the PRT principles, encouraged the parent to implement the strategies, and offered live feedback to the family regarding their use of the PRT skills. The following session outline was adapted from Bradshaw et al. (2017) and was followed during the in-person coaching sessions:
Check-in (5–10 min): The clinician checks in with the caregiver to discuss any updates about the child and address any questions or concerns the parent/caregiver may have. Identify Target Skill (5 min): The clinician and caregiver collaboratively identify a target skill to practice during the session (e.g., child choice, clear opportunity, and natural reinforcer). This skill is based on the topics introduced during the parent-only instructional virtual session. The parent can express which skills they would focus on, or the clinician can suggest skills they believe would be beneficial for the parent to practice based on previous sessions. Clinician Modeling (5 min): The clinician demonstrates the identified skill by playing with the child while providing a clear explanation and labeling of the PRT technique being used. Additionally, the clinician offers suggestions to the parent on how to implement the skill effectively during their practice. Parent Practice (20–25 min): The caregiver practices the identified skill, along with any other skills they have previously learned. The clinician observes and provides constructive feedback and suggestions for improvement. Recording a 5-min Video (5 min): The clinician records a 5-min play video toward the end of the session in which the caregiver and child engage in play while incorporating the learned PRT skills. Wrap-up (5 min): During this final segment, the clinician and parent work together to create goals for the parent to focus on before the next scheduled session. These goals should align with the skills practiced during the session.
The final session (i.e., session 10) was used as a concluding “wrap-up” session to answer any remaining questions regarding PRT and to collect the final 5-min play video as well as the treatment satisfaction form to assess perceived treatment usefulness and acceptability.
Postintervention and Follow-up Data Collection
After treatment, families were asked to submit a final 5-min video of the parent playing with the child 1–2 weeks following the completion of the program to measure maintenance of parent treatment mastery and child social communication. The videos were collected by either having the family record their own video and upload it to a secure cloud storage link or by remotely scheduling a session with the study team and having the study team record the interaction.
Data Collection and Behavioral Coding
In addition to the video collection during baseline, a 5-min video probe was recorded and coded for parents’ use of PRT skills and changes in child language production, after each of the six in-person coaching sessions. At the end of treatment, parents completed a treatment satisfaction questionnaire (Scale of Treatment Perceptions [SAP]) along with a study-specific self-efficacy form. Parents also provided written feedback, answering open-ended questions about the treatment. Parents submitted a final 5-min video probe 1–2 weeks posttreatment to measure treatment gains. The 5-min videos were coded for PRT Fidelity of Implementation (mastery).
Reliability
One independent undergraduate research assistant, who was masked to session type (baseline vs intervention) and session number, served as the primary behavioral coder for all primary outcomes. This primary coder was trained to code to 80% reliability using practice videos before coding for this project. Additionally, the primary investigator served as a secondary coder for reliability purposes. Reliability was scored for 25% of all baseline, intervention, and follow-up sessions. Interrater reliability is defined as the number of observer agreements divided by the total number of agreements and disagreements, yielding the total percent agreement. Reliability calculations were as follows: total agreement on fidelity = 0.91; parent-initiated language opportunities = 0.99; child verbal responses = 0.97; child choice = 0.96; child attention = 0.91; clear opportunity = 0.95; contingent reinforcer = 0.86; and natural reinforcer = 0.80.
Measures
Participant Characterization
Dependent Measures
PRT Components.

Note. PRT = pivotal response treatment.
Results
Intervention Fidelity of Implementation
All parents demonstrated clinically significant improvements to intervention fidelity, which are presented in Figure 1. During baseline, Parent 1 was observed to correctly implement PRT components about half of the time with a mean of 50.7% (standard deviation [SD] 0.9%). During intervention, Parent 1's PRT fidelity increased to a mean of 69.9% (SD 13.2%). Even though the mean did not cross the fidelity threshold, fidelity was attained at four distinct timepoints (7–10), as depicted in Figure 1. Hedge's g calculations on changes in fidelity from baseline to intervention yielded an effect size score of 1.73, which is indicative of a large effect. Parent 2 demonstrated a mean of 43.2% (SD 20.1%) fidelity during baseline. During intervention, their PRT fidelity increased to a mean of 85.2% (SD 9.18%). The baseline to intervention data yielded an effect size score of 2.81, which is also indicative of a large effect. Parent 3 demonstrated a mean of 42.4% (SD 18.2%) fidelity during baseline. During intervention, their PRT fidelity increased to a mean of 81.9% (SD 10.7%). The baseline to intervention data yielded an effect size of 2.56, which is indicative of a large effect. All parents scored above the 80% cutoff across the PRT fidelity components at least once during intervention. For Childs 1 and 2, 80% fidelity was maintained at follow-up.

Pivotal response treatment (PRT) fidelity of implementation.
Total Language Opportunities
Parent 1 initiated a mean of 13.6 language opportunities (SD 3.8) during baseline video probes, as shown in Figure 2. As anticipated, during the Spanish PRT intervention, her mean number of initiated language opportunities increased to a mean of 19.5 language opportunities (SD 6.7) per video. However, this increase was not maintained during the follow-up phase, with a noticeable decline to 12 language opportunities at this time point. During baseline, Parent 2 initiated a mean of 4.8 language opportunities (SD 2.7). While in the Spanish PRT intervention, Parent 2's initiated language opportunities increased to a mean of 22.5 (SD 10.1). At follow-up, Parent 2 maintained this increase with 27 language opportunities provided. Finally, Parent 3 initiated a mean of 16.0 language opportunities (SD 4.1). In the intervention phase, Parent 3's mean number of initiated language opportunities increased to 25.6 (SD 11.1). There was no follow-up data collected for Parent 3. The results of the parent-initiated language opportunities data are displayed in Figure 2.

Number of initiated language opportunities for all parent participants.
Child Verbal Responses
Child participant verbal responsiveness to parent-initiated language opportunities is depicted in Figure 3. Child 1 exhibited few verbal responses at baseline, responding to a mean of 8.3% (SD 4.8%) of parent-initiated language opportunities. After the introduction of the PRT intervention, her percent verbal responsiveness to parent language opportunities increased to a mean of 16.1% (SD 11.3%). Hedges’ g calculations on the percentage of child verbal responses yielded a score of .83, indicative of a large effect size. Child 1 maintained this increase at follow-up with a 17.0% response rate. During baseline, Child 2 demonstrated a mean verbal response rate of 19.2% (SD 21.9%). During intervention, his mean response rate increased to 59.7% (SD 22.1%). Effect size calculations yielded a score of 1.84, which is also indicative of a large effect size. At follow-up, Child 2's increase in verbal responses to parent language opportunities was maintained with a response rate of 67.0%.

Percent of child verbal response to parent-initiated responses.
Child 3 demonstrated the highest verbal responses at baseline, with an average of 49.9% (SD 15.1%) verbal responses to every parent-initiated language opportunity. During intervention, his verbal responses increased to an average of 67.6% (SD 10.2%). There was a decrease to 52% verbal responses to every parent-initiated language opportunity in the last recorded video (Study Timepoint 12) for this participant. Effect size calculations for Child 3's verbal responses yielded a score of 1.35, which is indicative of a large effect. Follow-up data were not completed for Child 3.
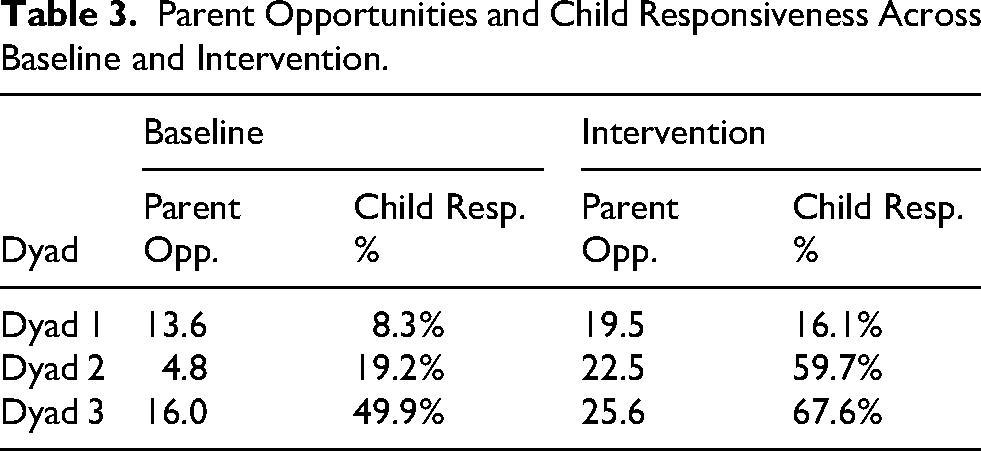
Additionally, Table 3 shows the average number of parent opportunities and the corresponding percentage of child verbal responses for each dyad across baseline and intervention phases. The table includes data for Dyads 1, 2, and 3, with child responsiveness shown as the percentage of parent opportunities that elicited a verbal response from the child.
Parent Opportunities and Child Responsiveness Across Baseline and Intervention.
Self-Efficacy
Parent 1 scored a 39 on the PRT Self-Efficacy form at baseline. As anticipated, at the end of the Spanish PRT intervention, her score increased to 51. Similarly, Parent 2 scored a 41 on the PRT Self-Efficacy form at intake and improved to a score of 49 at the end of the program. Lastly, Parent 3 scored a 42 on the PRT Self-Efficacy form at baseline, and her score increased to a 56 following the end of the Spanish PRT intervention. The results of the PRT Self-Efficacy form are displayed in Figure 4.

Parent self-rated treatment efficacy using a Likert scale of 1–7.
Treatment Satisfaction
Parent 1 rated the Family Fit, Safety, and Effectiveness of the study a 7 across all subdomains, indicating high levels of treatment satisfaction. Parent 2 rated the Family Fit of the study a 6.4, the Safety a 6.2, and the Effectiveness a 5.4. Parent 2 rated their overall treatment satisfaction a 6, indicating high levels of treatment satisfaction. Parent 3 completed 80% of the PRT workshop sessions but did not attend the final sessions and thus did not complete the treatment satisfaction form. The results of the Treatment Satisfaction measure are summarized in Figure 5.

Parent rated treatment satisfaction using a Likert scale of 1–7.
Discussion
The current study aimed to evaluate the acceptability, feasibility, and preliminary efficacy of a Spanish-translated PRT program for families who have a young child with autism. Our primary aim was to examine the impact of the program on parent fidelity of implementation and changes in child communication.
Results of our multiple baseline investigation were indicative of significant improvements in the fidelity of implementation, with all three parents meeting or exceeding the 80% fidelity threshold during the intervention phase, indicating they acquired the ability to skillfully implement the basic intervention strategies. Furthermore, all three parents indicated improvements in their self-reported comprehension of the PRT principles as well as their confidence in applying them effectively with their child. These findings not only highlight the ability of Spanish-speaking parents to accurately deliver an evidence-based intervention when linguistic adaptations are implemented, but it also provides evidence that these parents can rapidly learn the core components of PRT within a relatively short intervention period. Both parents with follow-up data maintained treatment gains and continued to demonstrate PRT strategies with at least 80% fidelity.
Additionally, there was a notable increase in the number of parent-initiated language opportunities demonstrated by all three parents. This indicates that parents became more confident and efficacious in their use of PRT and more skilled in providing clear and actionable prompts; thus, utilizing PRT strategies more frequently to motivate their child to communicate. We also saw a corresponding increase in child verbal responsiveness, indicating that children were more likely to respond to parent language bids during intervention compared to baseline. Child verbal responsiveness was also maintained in follow-up by Child 1 and Child 2. Follow-up data were not collected for Child 3. These promising outcomes highlight the program's effectiveness in enhancing child communication skills and may support longer-term gains in language development among Spanish-speaking autistic children.
Lastly, a high satisfaction with the treatment was indicated by both parents who completed the postintervention satisfaction survey, reflecting the program's acceptability, treatment satisfaction, and relevance to the needs of Spanish-speaking families with autistic children. Parent 1 and Parent 2 rated the treatment high in safety, efficacy, and overall family fit. Given that Parent 3 did not finish the intervention program due to external factors of work commitments and child illness, she did not complete the treatment satisfaction survey. While undesirable, this family's decision to discontinue participation highlights real-world challenges faced by full-time working parents when attempting to participate in clinical and research efforts. Participant satisfaction is crucial for continued engagement and adherence to intervention strategies for Spanish-speaking parents learning PRT.
Overall, findings from this study support our hypothesis that participation in a Spanish-translated PRT program would be associated with improvements in parent fidelity of implementation, corresponding gains in child communication, and increased parent efficacy using intervention strategies. Notably, results from this study are consistent with theories of PSE and empowerment (Ardelt & Eccles, 2001; Coleman & Karraker, 2003; Jones & Prinz, 2005), which suggest that as parents gain confidence in their ability to effect change, they are more likely to engage in effective parenting practices and take an active role in the intervention. In the context of this Spanish-translated PRT program, linguistic and cultural adaptations may have facilitated parents’ understanding of intervention principles and increased the relevance of the strategies to their daily lives; therefore, supporting both parent skill acquisition and confidence in implementation. As a result, parents developed conceptual knowledge of PRT strategies and learned how to effectively implement these skills through virtual teaching sessions, in vivo coaching, and continued home practice.
Limitations and Future Directions
Our PRT training program went through a rigorous Spanish translation process by a native, fluent Spanish-speaker who is also an expert PRT clinician, but one limitation is that we did not conduct a back-translation process with a different translator.
While the study's findings are promising, recruitment challenges posed a significant barrier for the researchers to complete the study. Efforts to reach and engage Spanish-speaking community members included disseminating information through social media, websites, flyers, and community providers who served predominantly Spanish-speaking individuals. Even with this multi-pronged approach, it proved very challenging to recruit eligible families to participate in the study, despite a sizable Spanish-speaking population in our local geographic region. In 8 months of active recruitment, only four families completed the interest form. Existing research literature suggests that community meetings and social media posts are preferred methods of communication for underrepresented individuals compared to flyers and websites (Erves et al., 2017). Furthermore, offering both monetary and nonmonetary incentives (i.e., transportation vouchers, assessment results, and a better understanding of health conditions that do not compromise study results) has been shown to enhance recruitment and retention in research (Langer et al., 2021). Continued efforts are needed to explore effective outreach strategies, such as attending community events and meetings, utilizing trusted lay health workers and other community members, and offering incentives that are culturally relevant to the Spanish-speaking community.
Importantly, participating families provided valuable insights into specific barriers to engaging in autism research. For example, they reported logistical challenges pertaining to accessing transportation and making childcare arrangements while they participated in the training sessions. Additionally, one mother expressed apprehension about being asked about her immigration status, a fear that is not uncommon among undocumented immigrant parents (Luelmo et al., 2022). Other concerns included feeling intimidated by entering a university setting, reporting a lack of understanding about the research process, and its potential benefits for their family. These barriers are consistent with the existing research findings (Stahmer et al., 2019; Williams et al., 2013) and highlight the need to address challenges such as transportation and childcare burdens (DuBay, 2022). Future projects should build in clear strategies to overcome these barriers. For example, some strategies may include conducting all sessions in accessible community settings instead of university or hospital research settings and/or providing a more comprehensive explanation of research during recruitment and intake sessions to ensure that participants clearly understand the process and potential benefits.
It is also crucial to reconsider the common eligibility requirement of a professionally rendered autism diagnosis prior to enrollment. On average, children in the US receive an autism diagnosis at five years of age (The National Autism Data Center, 2023). This requirement particularly disadvantages children from marginalized communities who face disparities in healthcare access and are diagnosed even later in life (Angell et al., 2018; Bishop-Fitzpatrick & Kind, 2017; Magaña et al., 2017). Future studies should strongly consider building in autism assessment and diagnostic confirmation for potential participants with suspected but unconfirmed autism. A seamless, comprehensive assessment > diagnosis > intervention support model would (a) directly help to alleviate late diagnosis disparities, (b) inform a more comprehensive understanding of the participant's strengths and vulnerabilities for treatment planning, and (c) immediately empower parents with highly effective intervention strategies.
While multiple baseline experimental designs are recognized as a rigorous means of empirical investigation according to the National Standards Project (The National Autism Data Center, 2023), this project needs large-scale replication. Given the promising results demonstrated by our three participating families, future research should focus on a larger cohort of participant families in a clinical trial design to replicate and build on the findings from this initial study. An RCT would also allow for robust statistical analysis of the impacts of a Spanish PRT program.
A larger trial would also allow researchers to consider the rich diversity and varying Spanish dialects within subgroups that make up the broader Spanish-speaking community. There are over 20 Spanish-speaking nations, each with its own standards (grammar, syntax, and pronunciation) and dialectical styles (formal, informal, and colloquial; Moreno-Fernández & Otero, 2008). Future research should aim to recruit Spanish-speaking families of various backgrounds (Puerto Rican, Cuban, Mexican, etc.) to understand what preferences and adaptations could optimize treatment efficacy within individual Spanish-speaking communities.
Conclusion
This study provides preliminary empirical support for a Spanish-translated PRT program, demonstrating emerging efficacy for enhancing parent fidelity of PRT skills and increasing short-term verbal responsiveness in autistic children. Our findings suggest that when language barriers are removed, caregivers can achieve high implementation fidelity and report increases in self-efficacy and empowerment, which directly translates into significant gains in verbal responsiveness for autistic children. Additionally, the positive treatment outcomes and high satisfaction rates among participants point to high acceptability of the intervention, which is a critical step toward bridging the gap in services for a group that has been historically underrepresented in parent-mediated literature.
This investigation's results are exciting as they demonstrate the feasibility of culturally and linguistically adapted interventions, which can lead to increased accessibility to autism services for Spanish-speaking communities. With 35.8 million Spanish-speaking Latinos in the US and only 34% of Latino immigrants speaking proficient English, autism intervention models such as PRT must be translated, culturally modified, and thoroughly tested for accessibility and feasibility (Krogstad et al., 2015). This is particularly crucial given the documented experiences of Spanish-speaking families feeling dismissed and powerless within systems that lack linguistic accommodations.
To our knowledge, this is the first time that a Spanish-translated PRT intervention package has been empirically investigated. Given the growing evidence supporting NDBIs as first-line interventions for autistic youth and the promising results of this study, future research should build on these findings to further refine and expand the reach of such programs for Spanish-speaking caregivers of autistic children, empowering them to effectively advocate for their children and participate fully in their care.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a University of California, Santa Barbara Academic Senate Faculty Research Grant.
Ethical Considerations
This study was approved by the UCSB Office of Research (approval no. 34-23-0336) on June 30, 2023. Informed consent was obtained via a written document and a formal signature.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.