
Abstract
Purpose
This study aimed to investigate the impact of fathers’ and mothers’ involvement in treatments by speech-language pathologists (SLPs) on parent–child communication, play, and feelings of caregiver emotional load in families with children diagnosed with autism spectrum disorder (ASD).
Methods
Data from 51 families, including 51 fathers and 51 mothers, were analyzed, focusing on measures of involvement in treatments, parent–child play, parent–child communication experience, the child's communication skills, and feelings of caregiver emotional load. Pearson correlations were conducted to explore associations between parental involvement, child variables, and parental factors. Path analysis was employed to delineate the relationships between parental involvement and treatment outcomes.
Results
Mothers exhibited significantly higher scores in involvement in treatments and feelings of caregiver emotional load compared to fathers, while no significant difference was found in parent–child communication experience. Both fathers and mothers demonstrated direct association between involvement in treatment, enhanced play and better communication experience with their children. Only fathers demonstrated direct associations between involvement in treatment and reduced caregiver emotional load, as well as improved communication skills in their children. The involvement of fathers in treatment mediated the association between paternal education level and the child's gender to treatment outcomes. Communication experience with the child was negatively associated with parental feelings of emotional load.
Conclusions
Active involvement by both parents is important for supporting parent–child play and communication. Fathers, in particular, experience benefits from involvement in treatments by SLPs, including decreased feelings of emotional load. These findings underscore the significance of considering demographic factors such as parental gender, education level, and the child's gender when designing SLP treatments for children with ASD and guiding their parents
Introduction
Autism is diagnosed based on two main groups of symptoms: (a) challenges in social communication and (b) the occurrence of repetitive behaviors and limited interests (APA, 2013, DSM-5). Autism is a neurotype that encompasses children and adults across the globe. Individuals on the autism spectrum often experience unique differences in communication and social interaction, frequently accompanied by intense interests in a variety of subjects. This diversity is considered a natural aspect of human experience (Bottema-Beutel et al., 2021). However, language difficulties, including receptive and expressive language, are also common among autistic children (Kjelgaard & Tager-Flusberg, 2001).
Over the past decade, there has been a notable rise in the prevalence of autism spectrum disorder (ASD), indicating that more children are being diagnosed and acknowledged as having this condition (Maenner et al., 2023; Centers for Disease Control and Prevention, n.d. https://www.cdc.gov/autism/data-research/index.html; Shaw et al., 2023). As of now, 1 in 31 children aged 8 years in the United States is diagnosed with autism (Shaw et al., 2025). As a result, parenting a child with autism has become an increasingly common experience for many families.
Given the importance of early language and communication skills for long-term participation in academic and social activities (Hus & Segal 2021; Kasari et al., 2006, Kasari et al., 2008, Kasari et al., 2010; Kover et al., 2016; Maksimović et al., 2023), speech-language pathologists (SLPs) play a vital role in providing early intervention services to autistic preschoolers (Binns et al., 2021; Denne et al., 2018; Green et al., 2006). Family-centered care is a best practice for autistic preschoolers, emphasizing collaboration between families and professionals (Christian, 2016; Crais et al., 2006). Also, active parental involvement is crucial for enhancing therapeutic outcomes, increasing exposure to therapeutic strategies in everyday life, and supporting the child's progress (Bearss et al., 2015; Beaudoin et al., 2014; Bradshaw et al., 2017; Burrell & Borrego, 2012; Klatte et al., 2020; Kuravackel et al., 2018; Liao et al., 2014; Rieth & McGowan, 2018; Zwaigenbaum et al., 2015).
However, research often focuses on mothers, neglecting the role of fathers in the treatment of autistic children (Rankin et al., 2019). This underrepresentation of fathers in scientific research on the treatment of autistic children is especially significant, given recent perspectives that highlight the importance of inclusivity in autism research across various dimensions, including race, ethnicity, socioeconomic status, and gender (Girolamo et al., 2023). Moreover, very few studies have examined the roles of mothers compared to fathers in the treatments provided by SLPs for the same child (Flippin & Hahs-Vaughn, 2020). This distinction is crucial for controlling additional confounding variables that may occur when mothers and fathers are parents to different children.
Various studies have suggested that mothers of autistic children identified themselves as the primary caregivers, while fathers played an indirect role in their child's life, primarily providing financial support for the family, participating in parental decision making, and providing mothers with breaks from parenting responsibilities (Ostfeld-Etzion et al., 2016; Ozturk et al., 2014; Rankin et al., 2019; Robinson et al., 2015). In assessments of the involvement of couples consisting of mothers and fathers of autistic children aged 2 to 7 in their child healthcare treatments, it was observed that mothers tended to show more interest in their child's treatment plans, attended therapy sessions more regularly, and made greater efforts to maintain contact with therapists compared to fathers (e.g., Sharabi & Marom-Golan, 2018). To our knowledge, the only study that examined the participation of both mothers and fathers in speech-language therapy involved parents of school-age autistic children (Flippin & Hahs-Vaughn, 2020). In this study, it was noted that fathers had fewer interactions with SLPs and were less involved in the assessment and planning phases compared to mothers. Additionally, fathers reported lower satisfaction levels than mothers regarding communication and planning with the therapists (Flippin & Hahs-Vaughn, 2020).
The present study aims to explore the involvement of fathers and mothers in therapy sessions led by SLPs for preschoolers with autism. Additionally, it seeks to identify the relationships between parental involvement in treatment and possible outcome variables including parent–child play, communication, and caregiver emotional load for both mothers and fathers. In the following sections of the introduction, we will elaborate on each outcome variable possibly associated with treatment involvement, emphasizing the differences and similarities between mothers and fathers.
Parental Gender and Parent–Child Play
Play is crucial for child development (Lai et al., 2018) and therefore serves as a fundamental component in the treatments provided by SLPs for children with ASD. However, fathers and mothers may differ in their styles of play (Robinson et al., 2021; Vallotton et al., 2020).
Notably, studies evaluating play interactions between parents and their autistic children suggest some dissimilarities between fathers and mothers (e.g., Perzolli et al., 2023). Fathers exhibited low-to-moderate levels of interactional behaviors with their autistic children when assessed with the Parental Behavior Rating Scale-Turkish Version (Arslan & Dicken, 2020). Fathers of autistic preschoolers were less reactive than mothers in terms of responsiveness, affect, attention, and initiation measures (Karaaslan, 2016). Fathers of neurotypical children and autistic children demonstrated less direct support compared to mothers and were less involved (Ostfeld-Etzione et al., 2016). Mothers tended to incorporate play moments into daily routines, while fathers’ opportunities for play were not necessarily embedded within other daily tasks (Román-Oyola et al., 2018). Autistic preschoolers were found to engage in significantly more relational play activities (e.g., stacking, sorting, putting toys into or on top of one another) in interactions with their mothers than in unsupported or father–child play (Flippin & Watson, 2011). However, similar proportions of responsive play behaviors were observed for both fathers and mothers (Flippin & Watson, 2011). Also, when fathers were trained to interact with their child with ASD, there were important improvements in play and social skills (Louis & Kumar, 2015). While previous studies primarily analyzed specific parent–child interactions (e.g., Flippin & Watson, 2011; Perzolli et al., 2023), it is also important to assess the frequency and diversity of play activities of fathers and mothers who are parents of children with ASD.
Parental Gender and Parent–Child Communication
Parent–child communication is an important aspect of treatment by SLPs of autistic children (e.g., Dromi, 2018). However, fathers and mothers may engage in different communication styles with their child. Fathers were reported to exhibit different interaction styles in communicating with their children, such as using less child-directed speech, speaking less frequently to infants who were later identified as autistic (Cohen et al., 2013), and being less verbally responsive overall (Flippin & Watson, 2015). Research has also indicated that fathers of children with ASD tend to make fewer statements during interactions compared to mothers, while the children demonstrate more vocal or verbal initiations toward the fathers (El-Ghoroury & Romanczyk, 1999). Overall, children and secondary-caregiver fathers experienced more communication breakdowns than experienced by children and mothers who were primary caregivers (Tomasello et al., 1990). Fathers also issued more commands or instructions than mothers, while mothers were more likely to employ prompts to stimulate their children's speech, particularly if they had high support needs (Konstantareas et al., 1988).
Finally, the communication difficulties of autistic children are transactional. That is, they influence not only the child, but the child's communication partners as well (Wetherby & Prizant, 2000). The child's communication skills may include initiating and sharing information with adults and other children. The communication experience of the parent with the child may involve a range of emotions and perceptions. Parents may feel enjoyment when successfully connecting with their child, but they may also encounter frustration due to challenges in communication. However, to date, to the best of our knowledge, no study has assessed the communication experiences of parents with their autistic children.
Parental Gender and Perceived Emotional Load
In the scientific literature, the term caregiver burden refers to the weight of responsibility carried by a family member caring for a loved one. To promote more inclusive language and avoid ableism, we will use the term perceived emotional load, which includes the emotional and psychological toll experienced by the family caregiver and encompasses various aspects, including the caregiver's physical and mental wellbeing, its impact on their personal life, family dynamics, employment, and social interactions (Graessel et al., 2014). The literature consistently highlights that continuous caregiving for a family member often constrains the caregiver's personal, social, and professional life. This perceived emotional load can manifest itself in the form of physical and emotional symptoms experienced by the caregiver and may also strain the relationship between the caregiver and the care recipient (Graessel et al., 2014; Pinquart & Sörensen, 2003; Sörensen et al., 2002).
Raising young autistic children can amplify parental feelings of stress and the perceived emotional load (Di Renzo et al., 2022; Graessel et al., 2014; Hayes & Watson 2013; Hoefman et al., 2014). Compared to parents of typically developing children, parents of autistic preschoolers face challenges both at home and in the community. They are at an increased risk of financial strain and even have a higher divorce rate (Depape & Lindsay, 2015). Parents of autistic children report having more mental health issues compared to parents of children with other developmental difficulties, experiencing greater stress and emotional load, as well as more difficulties in their relationships (Ang & Loh, 2019; Rankin et al., 2019). A study conducted by Hoefman et al. (2014) found that 40% of mothers of autistic children reported symptoms of depression. Depression may hinder optimal caregiving because high levels of stress and depression could negatively impact the parent–child relationship (Ang & Loh, 2019; Di Renzo et al., 2022; Pisula & Porębowicz-Dorsmann, 2017). Environmental systems can contribute to this perceived emotional load, as many interventions often fail to support the unique abilities of autistic children. Instead, they predominantly focus on deficits and the need for these children to conform to neurotypical standards (Cherewick & Matergia, 2024; Schuck et al., 2021).
There is some disagreement in the literature regarding the difference in parental stress based on the gender of the parent. While some studies did not find significant differences in stress levels between mothers and fathers (Davis & Carter, 2008; Hastings, 2003), other research has produced mixed results. While there is evidence that fathers exhibit more stress than mothers (Rankin et al., 2019; Rivard et al., 2014), Soltanifar et al. (2015) suggested that mothers experience higher stress levels than fathers. Furthermore, there are studies indicating that, in order to reduce stress, mothers seek more social support compared to fathers, while fathers tend to use avoidance strategies (Mount & Dillon, 2014). However, the assessment of perceived emotional load of fathers and mothers who are parents of autistic children is lacking.
The Present Study
The point of departure for the present study was that treatment of autistic children led by SLPs focuses on enhancing communication skills, encompassing speech, language, and social communication. Parental involvement in treatments led by SLPs might be associated the ways in which parents interact with their autistic child, promoting improved communication experiences, increased play, and reduced perceived emotional load (Noyan Erbaş et al., 2020). Nonetheless, existing literature falls short in exploring the parental involvement of fathers and mothers in their child's speech-language therapy led by SLPs.
Accordingly, the research objectives of the present study were (a) to assess fathers and mothers’ involvement in therapy led by SLPs and (b) to identify the extent to which fathers’ and mothers’ involvement in in treatments by SLPs is associated with parent–child play, the parent–child communication experience, the child's communication skills, and parents’ feelings of emotional load. In line with the current scientific literature, we hypothesized that mothers would be more involved in treatments led by SLPs. However, in view of the lack of previous studies on the association between involvement in treatment and parent–child play, the parent–child communication experience, the child's communication skills, and feelings of emotional load among fathers and mothers, the present study undertook an exploratory approach. Our examination aimed to provide a deeper understanding of the ways involvement in treatments by SLPs impacts both fathers and mothers as caregivers of young children with ASD.
Research Questions
What differences are there between mothers’ and fathers’ levels of involvement in speech-language treatment for children with ASD?
Are there any additional differences between mothers and fathers regarding parent–child play, perceived emotional load, identification of the child's communication skills, and the parent–child communication experience?
How does parental involvement in treatment relate to parent–child play, the caregiver's perceived emotional load, communication skills of the child and parent–child communication experience for both mothers and fathers?
What are the contributions of child variables (such as age and gender) and parental variables (including education and age) on involvement in treatment and on the outcome variables, including parent–child play, the caregivers’ perceived emotional load, the child's communication skills, and the parent–child communication experience for both mothers and fathers?
Method
Population
The population of the current study consisted of 51 married heterosexual couples who were the biological parents of children diagnosed on the autistic spectrum. The participants (n = 102) included 51 fathers (men) and 51 mothers (women). All pairs of parents lived together in the same household. The inclusion criteria for the study were that the child had received an official ASD diagnosis by a developmental physician and a psychologist and had been receiving treatment by an SLP for at least 1 year at the time the parents filled out the questionnaire.
Family Demographics
The fathers’ average age was 39.23 (SD = 6.45) and the mothers’ average was 36.10 (SD = 4.88). All parents belonged to the middle socioeconomic status (SES) based on the neighborhood where they lived and their years of education. The families of the children with ASD lived in neighborhoods that were rated by the Israel Central Bureau of Statistics as belonging to 6 to 8 on the socioeconomic scale ranging from 1 (the lowest socioeconomic status) to 10 (the highest socioeconomic status). A significant majority of parents (72.5%) self-identified as secular, followed by 13.7% who categorized themselves as traditional. The remaining participants self-identified as religious. Family and child demographics are described in Table 1.
Demographics of Participating Families (n = 51).

ASD: Autism spectrum disorders.
Child Demographics
The children included 39 boys and 12 girls. All the children were monolingual and Hebrew was the only language spoken at home. The age range of the children diagnosed on the autistic spectrum was between 2.1 and 7.6 years (M = 4.14, SD = 1.29). All children attended preschool education programs. Two children had a nonidentical twin brother whose development was typical. The children had normal hearing and vision and had no additional developmental conditions such as cerebral palsy, syndromes, or a developmental intellectual disability.
Speech-Language Therapy Sessions
Most parents indicated that speech-language therapy was held in the child's special kindergarten (n = 21, 41%) without their presence. However, parents were provided with short treatment summaries and written instructions on how to support their child's treatment goals at home. Other parents indicated that speech therapy took place in a developmental center (n = 7, 14%) in the parents’ presence. The remaining parents indicated that therapy was held in a private speech clinic (n = 20, 39%) or in another location (e.g., home or other; n = 3, 6%), in the parents’ presence. The sessions were held once a week for 45 min. The strategies employed were holistic developmental approaches to early childhood intervention, including the Hanen approach, the developmental, individual, differences, relationship-based approach (DIR), and the naturalistic developmental intervention (NDI (Dromi, 2018). The targeted outcomes included training on how to facilitate play, encourage engagement, increase turn-taking and responsiveness, communicate effectively with the child, and provide appropriate language modeling. These aspects are essential for fostering a supportive environment that promotes child development and language acquisition. By focusing on these outcomes, caregivers can enhance their interactions with children and support their overall growth and learning. Parents were encouraged to implement the skills and strategies introduced during sessions at home, thereby reinforcing learning through naturalistic interactions. Specifically, parental involvement included modeling play behaviors, encouraging engagement through questions, and maintaining open lines of communication with their child.
Materials
Background Questionnaire
The purpose of the background questionnaire was to gather essential details about both the parent and the child. It consisted of eight sets of questions intended to gain insight into the parents’ profile, covering such aspects as age, gender, educational attainment, religious affiliation, cultural background, the number of hours each parent spent alone with the child during the week, and the extent to which each parent perceives himself/herself as the main caregiver. Additionally, the questionnaire included 14 questions in Hebrew aimed at understanding the child's profile, which comprised such details as age, sex, the number of siblings in the family, developmental milestones, and the child's educational setting as presented in Appendix A.
Questionnaire on Parental Involvement in Treatment
The original questionnaire for involvement in treatment in general was developed in Hebrew and adjusted to address treatment by SLPs (Ingber, 2004). The questionnaire consists of 22 statements that assess parental involvement in their child's treatment plan with the speech and language pathologist. Parents were asked to rate each statement on a five-point Likert scale, ranging from 1 (‘absolutely not’) to 5 (‘always’). For example, one of the statements in the questionnaire was “I actively engage in the decision-making process concerning my child's treatment plan with the SLP.” Parents were asked to express their agreement with this statement by marking their response on the provided Likert scale. Benchmarks for interpretation are as follows: A score of 1 indicates no involvement, 2 suggests infrequent involvement (a few times), 3 reflects moderate involvement (sometimes), 4 signifies a high level of frequency (often), and 5 denotes consistent occurrence (always). The total scores could range from as low as 22 to as high as 110. Mean scores for each participant and group could vary between 1 and 5, with higher scores indicating greater parental involvement.
The questionnaire was originally designed for parents of hearing-impaired children (Ingber, 2004). Consequently, one comment that followed statement 10, which was related to hearing aids (“Do you ensure your child wears his/her hearing aids?”), has been omitted from the original version. The question “Do you participate in any volunteer activities?” has also been excluded. For the complete questionnaire, see Appendix B. The original questionnaire exhibited a high level of internal consistency, with a Cronbach's alpha value of α = .84 (Ingber, 2004). In the current study, the questionnaire demonstrated even stronger internal consistency, with α = 0.93.
The Hebrew Version of the Zarit Caregiver Burden Scale
Caregiver burden was assessed using the short version of the Hebrew Zarit Caregiver Burden Scale (ZBI; Iccovich, 2012); see Appendix C. In this context, we will refer to “burden” as the perceived emotional load. The original questionnaire was aimed to assess the burden of caregivers who treat cognitively intact but physically frail older family members. Primary caregivers were asked if they agreed with the 12 statements, with scores for each item ranging from 1 (never) to 5 (nearly always). For the purpose of the present study, which was aimed to assess the perceived emotional load by parents raising a child with ASD, the word relative in each statement was changed to child. For example, the statement in the original questionnaire “Do you feel that because of the time you spent with your relative that you do not have enough time for yourself,” was changed as follows: “ Do you feel that because of the time you spent with your child that you do not have enough time for yourself?”. Parents were asked to express their agreement with each statement by marking their responses on the provided Likert scale. The benchmarks for interpreting are as follows: a score of 1 indicates no burden at all (never), 2 suggests a very minimal level of burden (rarely), 3 reflects occasional feelings of burden (sometimes), 4 signifies frequent experiences of burden (almost always), and 5 indicates a constant and significant level of burden (always). The total scores could range from as low as 12 to as high as 60. Mean scores for each participant and group could vary between 1 and 5, with higher scores indicating greater perceived emotional load reported by caregivers.
The H-ZBI short version demonstrated good psychometric properties similar to those of the English version (Iecovich, 2012). Internal consistency of Cronbach's alpha was high (α = 0.85) and the measure showed good convergent and exploratory validity due to significant correlations other measures (Iecovich, 2012). In the current study, the questionnaire demonstrated high internal consistency, with α = 0.87.
The Parent Play Questionnaire
The original questionnaire was translated from English to Hebrew and also underwent reverse translation (Ahmadzadeh et al., 2020). We used the first scale of the questionnaire: Frequency and diversity of parent—child play. This part of the questionnaire addressed the frequency and diversity parents played with their child during the past 2 weeks and included 12 statements. For example, “[thinking] back over the past two weeks, please indicate how often you played an active physical game (lifting or swinging your child, rough and tumble) with your child.” The statements were followed by a Likert scale from 1 (never) to 6 (several times a day). The benchmarks for interpretation are as follows: a score of 1 indicates no play (never), 2 suggests infrequent play (once a week or less), 3 reflects moderate engagement in play (a few times a week), 4 signifies regular participation (approximately once a day), 5 denotes frequent play (multiple times a day), and 6 represents very frequent play (several times each day). The total scores potentially range from as low as 12 to as high as 72. Mean scores for each participant and group potentially vary between 1 and 6, with higher scores indicating more frequent and diverse play.
Four statements (9–12) were added to the original eight items because the present study assessed older children. These statements addressed symbolic play, role play, as well as building games and board games (see Appendix D). The scores of this section reflect both frequency and diversity in the types of parent—child play.
Internal consistency of Cronbach's alpha in the original study was high with α = 0.80. In the current study, the subscale demonstrated even higher internal consistency, with α = 0.89.
The Parent–Child Communication Questionnaire
This questionnaire was originally developed in Hebrew to assess the communication experience of the parent with his/her child and the child's communication skills (Besser-Leshem, 2024). It was initially piloted by five clinicians and researchers with expertise in ASD and was revised based on feedback from this group before the questionnaire was administered (Besser-Leshem & Segal, in progress). The questionnaire includes 13 statements (see Appendix E). Six statements address the communication experience of the parent with the child (e.g., I enjoy communicating with my child.), and seven statements addressed the child's communication skills (e.g., Strangers understand my child's wishes). The statements are followed by a Likert scale from 1 (I do not agree at all.) to 7 (I definitely agree.). The total scores potentially range, from as low as 13 to as high as 91. Mean scores for each participant and group potentially vary between 1 and 7, with higher scores indicating better communication skills and more positive communication experiences.
Principal components analysis (PCA) was run on the 13 items. The PCA revealed two components with eigenvalues <1, and explained 34.18% and 29.98%, of the total variance for the first and second component, respectively. Items 1, 6, 7, 11, 12, and 13 belonged to component 1: parent's communication experience with the child (α = 0.87), and items 2, 3, 4, 5, 8, 9, and 10 belonged to component 2: Child's communication skills (α = 0.95).
Procedure
The study was approved by the Tel-Aviv University Ethics Committee (Proposal No. 0006461-1). All participants completed an online informed consent form. The participants in the current study were recruited primarily through social media groups for parents of children diagnosed with autism or by word of mouth. Each pair of parents participating in the study received a unique code to ensure that both the mother and the father belonged to the same family. The complete questionnaire, which included the five questionnaires detailed above, was administered using the online platform Qualtrics. Potential participants were allowed to read about the study, ask questions via email, or speak with the researchers before deciding whether to participate. Each parent was asked to complete the questionnaire separately from their partner and to refrain from sharing their responses until both questionnaires had been submitted. Each child's mother and father filled out the questionnaire within the same week. The completion of the questionnaire required approximately 20 min and was done at the participants’ convenience.
All the data collected through the questionnaire was anonymous. Upon submission, the questionnaires were reviewed to ensure completeness. Upon completion, the participants’ responses were entered into SPSS software (version 27), where statistical analyses were subsequently performed.
Data Analysis
IBM SPSS version 27.0 and IBM AMOS Graphics software version 27.0 were for used statistical analyses. Statistical significance was set at p < .05. The results for each questionnaire were computed and a comparison between fathers and mothers was conducted using paired two-tailed t-tests. Pearson and biserial correlations were then conducted to examine which associations between fathers and mothers’ involvement in treatments, child variables (e.g., age and gender), and parental variables (e.g., age, number of children in the family, and parents’ level of education and number of hours at home) and outcome measures (including parent–child play, parent–child communication experience, the child's communication skills, and feelings of emotional load) were significant. In order to evaluate the contribution of child variables, parental variables, and involvement in treatment to the outcome variables, a path analysis was used. Only significant correlations were included. A path analysis is a statistical method used to determine complex relationships between variables. It combines correlations and regression analysis and can test theoretical models using the data collected. Model fit was assessed using the following goodness-of-fit indices: chi-square, comparative fit index (CFI), Tucker–Lewis index (TLI), and root mean square error of approximation (RMSEA). A nonsignificant chi square, CFI, and TLI ≥.95, and RMSEA equal to or <.06 (Hu & Bentler, 1999; Tabachnick & Fidell, 2001) are indicative of an acceptable fit. The standardized path coefficients (β) were assessed to examine the statistical significance and directions of path estimates between the variables in the model.
Results
To address the first and second research questions regarding the differences between mothers’ and fathers’ involvement in treatment and the impact of involvement in treatment on outcome variables—including parent–child play, perceived emotional load, the child's communication skills, and the parent–child communication experience—a series of paired t-tests was conducted for both mothers and fathers. The mean results of the scales of involvement in treatment, parent–child play, the caregivers’ perceived emotional load, and the parent–child communication experience are summarized in Table 2. Mothers scored significantly higher (M = 3.63) than fathers (M = 3.04) on the Parental Involvement in Treatment questionnaire [t(50) = 4.44, p < .001]. These results indicate that both fathers and mothers exhibit moderate involvement (3 = sometimes on the Likert scale for this questionnaire), with mothers demonstrating a greater level of involvement in treatment compared to fathers. Mothers scored significantly higher (M = 3.69) than fathers (M = 3.16) on the Parent Play Questionnaire [t(50) = 3.46, p < .001]. These results indicate that mothers engage in play moderately (a few times a week) with their children, demonstrating more frequent play activities compared to fathers, who scored at the lower end of moderate engagement. Mothers had higher scores (M = 2.61) compared to fathers (M = 2.30) in the Zarit Caregiver Burden Scale suggesting that they experienced more feelings of emotional load. According to the benchmarks, mothers’ scores indicate that mothers are experiencing occasional feelings of burden (sometimes), while fathers report feelings that lean toward minimal burden (almost never). However, no significant difference was found between fathers and mothers pertaining to the communication-experience questionnaire and the child's communication skills. This suggests a high level of similarity among parents in their perceptions of the communication experience with their child and in their evaluations of the child's communication abilities.
The Means and Standard Deviations (SD) of Each Measure, Along With the t-Values and Cohen's d.
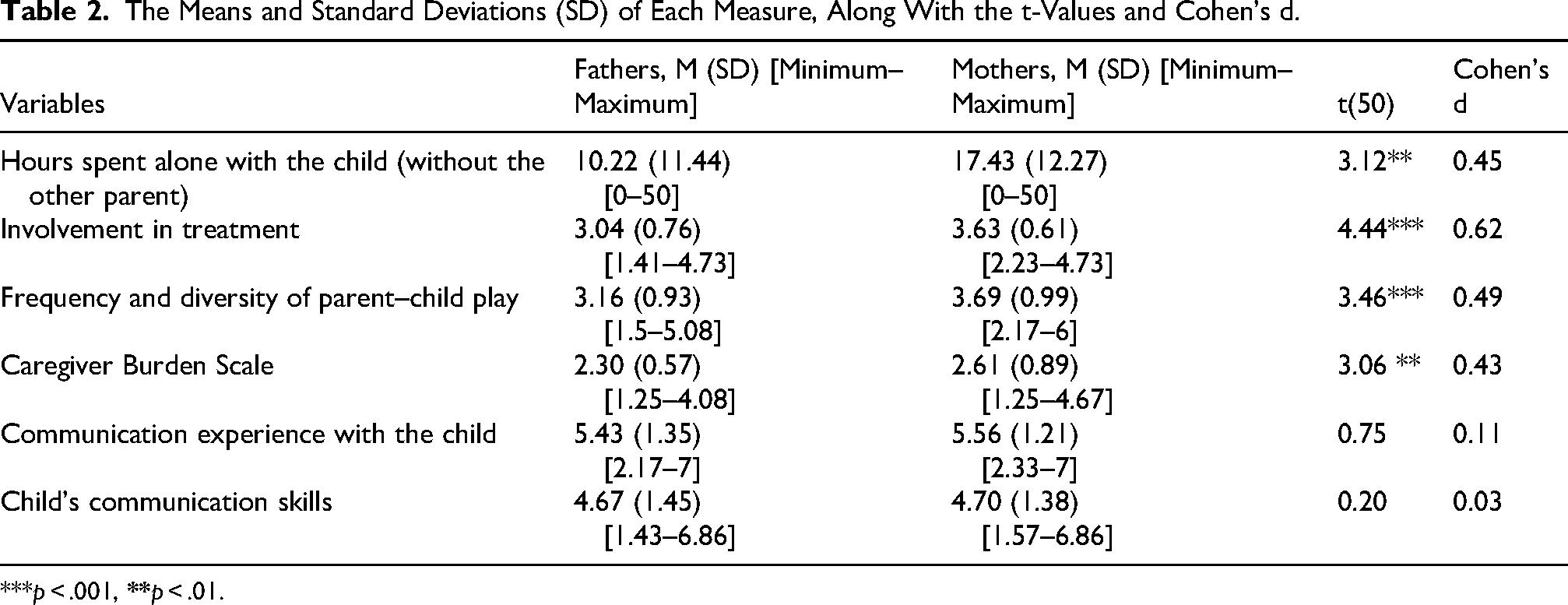
***p < .001,
To address the third research question regarding the associations between parental involvement in treatment outcomes such as parent–child play, caregiver perceived emotional load, the child's communication skills, and the parent–child communication experience, a series of Pearson correlations was conducted. Additionally, we included Pearson and Biserial correlations to examine which associations between fathers and mothers’ involvement in treatments, child variables (e.g., age and gender), and parental variables (e.g., age, number of children in the family, and parents’ level of education and number of hours at home) and outcome measures (including parent–child play, parent–child communication experience, the child's communication skills, and feelings of emotional load) were significant. Correlations that examined the relationships between fathers’ and mothers’ involvement in treatment, child variables (e.g., age and gender), and parental variables (e.g., education, age, number of children, and hours at home), as summarized in Tables 3 and 4.
Pearson and Biserial Correlations Between Fathers’ Involvement in Treatment, Child Variables and Parental Variables.

***p < .001; **p < .01; *p < .05.
Pearson and Biserial Correlations Between Mothers’ Involvement in Treatment, Child Variables, and Parental Variables.

***p < .001; **p < .01; *p < .05.
For mothers, the only significant, positive strong correlation for involvement in treatment was with play (r = 0.47, p < .001). This means that mothers who were more involved in treatment played with their children more frequently. For fathers, however, child gender, number of children, play, communication experience, communication skills, and feelings of burden, were all associated with involvement in treatments (r = 0.34, −0.30, 0.58, 0.30, 0.41, and −0.29, p < .05). These correlations suggest that fathers of boys tended to be more involved in treatment compared to fathers of girls (r = 0.34), fathers were more involved in treatment when the number of children in the family was smaller (r = -0.30), fathers who were more involved in treatment tended to play with their children (r = 0.58) more frequently and had a better communication experience with their children (r = 0.30), assessed their children as having better communication skills (r = 0.41) and had less feelings of emotional load (r = −0.29).
To address the fourth research question regarding the contributions of child and parental variables to involvement in treatment and its effects on outcome variables—including parent–child play, caregiver perceived emotional load, the child's communication skills, and parent–child communication experience—path analysis was conducted separately for mothers and fathers using the variables that showed significant correlations with treatment involvement. The results are presented in Figures 1 and 2.

Path analysis for the effects of child and material variables and involvement in treatment on play, communication experience, communication skills, and feelings of burden. The standardized path coefficients (β) are represented with straight arrows and Pearson’s correlations (r) are represented with curved arrows. All the associations presented were significant (p <.05).

Path analysis for the effects of child and paternal variables and involvement in treatment on play, communication experience, communication skills, and feelings of burden. The standardized path coefficients (β) are represented with straight arrows and Pearson’s correlations (r) are represented with curved arrows. All the associations presented were significant (p <.05).
Incorporating path analysis is essential because it allows for the examination of complex relationships among variables beyond simple correlations. While correlations can indicate associations between variables, they do not reveal the causal pathways or the direction of these relationships. Path analysis can identify direct and indirect effects, helping to clarify how child and parental factors are related to treatment involvement and subsequently impact outcome variables. This depth of path analysis provides a more comprehensive understanding of the dynamics at play. Path analysis is therefore a crucial step in exploring the intricacies of parental involvement in treatment for children with autism spectrum disorder.
Model-Fit indices for the group of mothers indicate that the model fits the data well, with χ2(9) = 6.82 and a p-value of .66, suggesting no significant discrepancies between the model's predicted values and the observed data. The CFI is 1.00, indicating an excellent fit, while the normed fit index (NFI) stands at 0.93, reflecting a good fit. Additionally, the RMSEA is 0.00, which is ideal, and the TLI is 1.05, further supporting the model's strong fit. The results of the path analysis for the group of mothers indicate that maternal involvement in treatment is positively associated with two key aspects of child development: play (β = .47) and the communication experience with the child (β = .17). This suggests that mothers who are more engaged in treatment are more likely to play with their children more frequently, and report a better communication experience with their children. Additionally, child age is positively associated with the child's communication skills (β = .22), indicating that as children grow older, their communication abilities tend to improve. Overall, these findings highlight the importance of maternal involvement in treatment to enhance both play and communication, as well as the natural progression of children's communication skills with age.
Model-Fit indices for the group of fathers indicate that the model fits the data well, with a χ2(9) = 17.31 and a p-value of .37, suggesting a good fit. The CFI is 0.99, reflecting an excellent fit, while the NFI is 0.87, indicating an acceptable fit. Additionally, the RMSEA is 0.04, which signifies a good fit, and the TLI is 0.98, further supporting the model's adequacy. Overall, the model demonstrates significant relationships among the variables and is strongly supported by the fit indices. Note that the number of children in the family was not included in the final model since it has no significant effect on the other variables. The results of the path analysis for the group of fathers highlight several significant relationships between paternal involvement in treatment and various aspects of child development and parental experience. Notably, greater involvement in treatment is associated with decreased perceived emotional load (β = −.29) and increased engagement in play (β = .48), better communication experience with the child (β = .34), and higher judgment of the child's communication skills (β = .43). This suggests that when fathers are more involved in treatment, they generally feel less overwhelmed and more capable of positively interacting with their children. They also perceive their child as having better communication skills. Additionally, child gender is associated with paternal involvement in treatment (β = .34), with fathers more involved in the treatment of boys.
Child age is positively correlated with communication experience (β = .44) and communication skills (β = .41), indicating that as children grow older, their ability to communicate improves, while there is a negative association with play (β = −.28), suggesting a decrease in playfulness or play activities as children age. Paternal education level is also positively associated with both involvement in treatments (β = .30) and play (β = .26), implying that higher education may enhance fathers’ engagement and playfulness with their children. Additionally, paternal involvement mediates the effects of child gender and paternal education on various aspects, including perceived emotional load, playfulness, communication experiences, and the development of communication skills in children.
Discussion
The first and second research questions referred to differences between mothers and fathers in involvement in treatment, and in variables that are possibly related to involvement in treatment including play, perceived emotional load, and the communication experience with the children. The main findings of the present study revealed several important trends. Mothers tended to exhibit more involvement in treatments compared to fathers and they also played with their children more frequently and reported more feelings of emotional load compared to fathers.
The finding that mothers exhibited more involvement in treatments aligns with prior research that has consistently shown fathers to be less engaged than mothers in the upbringing of children with ASD (Rankin et al., 2019). Moreover, the existing literature highlights the greater involvement of mothers in general therapy plans, including more regular attendance at therapy sessions, and stronger efforts on their part to maintain contact with therapists compared to fathers (e.g., Sharabi & Marom-Golan, 2018). Fathers were also found to have fewer interactions with SLPs and were less active in the assessment and planning stages compared to mothers (Flippin & Hahs-Vaughn, 2020). In the present study, mothers were not only more involved in treatments led by SLPs but also engaged in more play with their children. This may be explained by the fact that they spent more time alone with their child (see Table 2) and/or because their perception of their parental role differed from the fathers’ perception of their role. Previous studies on fathers’ interactions with children with ASD primarily analyzed specific parent–child interactions and assessed responsiveness. The results were varied. Some studies revealed no differences in engagement and responsiveness between fathers and mothers (e.g., El-Ghoroury & Romanczyk, 1999), while in other studies, fathers demonstrated lower scores in these domains than mothers (Arslan & DiKen, 2020; Karaaslan, 2016). However, the present study is the first to assess the frequency and diversity of play activities among fathers and mothers who are parents of children with ASD.
Importantly, the mothers in the present study reported higher levels of feelings of emotional load compared to the fathers. This is consistent with some previous findings. For example, mothers reported more involvement in the treatment of their children with ASD and higher levels of stress compared to fathers (e.g., Soltanifar et al., 2015; Tehee et al., 2009). However, no differences were observed between fathers and mothers in the child's communication skills or in their parental communication experience with their child. Thus, fathers and mothers provided similar evaluations of their child's skills and reported similar communication experiences with their child.
The third and fourth research questions addressed the associations between involvement in treatment, and outcome variables including play, perceived emotional load, and fathers’ and mothers’ communication experiences with their children. The active participation of both mothers and fathers in treatments led by an SLP was found to be directly associated with more parent–child play activities, as well as with reports on better communication experiences compared to fathers and mothers who were less involved in treatment (as shown in the path analysis Figures 1 and 2).
In treatment by SLPs, play can serve as a therapeutic goal on its own or as a method of intervention to achieve linguistic and communicative objectives (Gibson et al., 2021; Kent et al., 2020; Qiu et al., 2019; Westby, 2022). Typically, when SLPs work with young children with ASD, they offer parents both direct guidance and opportunities to observe beneficial play and communication activities with their children (e.g., Rust & Thanasiu, 2019). Research has emphasized the significance of parent-mediated and play-based counseling interventions to address social communication challenges in children with ASD (e.g., Rust & Thanasiu, 2019) and to enhance self-efficacy in parent–child play interactions (Román-Oyola et al., 2018). Parents actively engaging in coaching processes or guided educational treatments that employ strategies to optimize their child's play opportunities demonstrated increased competence and higher levels of effectiveness and responsiveness. However, it is noteworthy that most research on parent–child play has focused on mothers and not on fathers (e.g., Perzolli et al., 2021).
Although previous studies generally suggest that parental guidance improves parent–child interactions, including language and social skills (Gibson et al., 2021; Kent et al., 2020; Qiu et al., 2019; Westby, 2022), most studies assessed mothers (e.g., Louis & Kumar, 2015; Naidoo & Govender, 2022; Praphatthanakunwong et al., 2018; Zwaigenbaum et al., 2015) and only a few studies assessed fathers (Donaldson et al., 2011). Also, previous studies did not address the parent–child communication experience, which refers to the extent of success, enjoyment, and frustration the parent experiences while communicating with the child. The present findings suggest that when parents, both mothers and fathers, are more involved in treatments led by SLPs, their communication experience tends to be better compared to parents who are less engaged in SLP led treatment, regardless of the parent's gender.
Another noteworthy finding is that the communication experience with the child was negatively associated with feelings of emotional load for both fathers and mothers. Parents who reported a better communication experience with their child tended to experience reduced feelings of emotional load. These findings underscore the crucial role of positive communication experiences in everyday life as a significant factor linked to reduced feelings of emotional load. Consequently, SLPs who focus on enhancing parent–child communication indirectly contribute to alleviating feelings of burden experienced by parents. This highlights the importance of prioritizing interventions that foster effective communication between parents and their children with ASD, as this can have a positive impact on parental feelings of emotional load and overall family dynamics.
Another important finding was that among the fathers, but not among mothers, involvement in treatments exhibited direct associations with the child's communication skills. This suggests that involvement in treatments led by SLPs may have aided fathers specifically in focusing on their children's communication abilities and identifying more nuanced communication skills. Additionally, within the fathers’ cohort, engagement in treatments was associated with reduced feelings of emotional load. This could be explained by proposing that active participation in treatments by SLPs facilitated more effective and less frustrating parent–child communication, supported positive behaviors, enhanced understanding of the child's needs and intentions, reduced misunderstandings, and consequently alleviated feelings of emotional load.
The observation that only fathers, and not mothers, exhibited a direct association between involvement in treatments and reduced feelings of emotional load suggests that other factors may influence maternal perceptions of emotional load. Additional factors that were not examined in the present study but were reported to be associated with feelings of emotional load in mothers of children with ASD include social support, as well as autism-related behavioral challenges and the child's level of disability (Cetinbakis et al., 2018; Sharabi & Marom-Golan, 2018). These factors could contribute to the experiences of emotional load among mothers of children with ASD. In light of these findings, it is important to explore tailored interventions aimed at reducing feelings of emotional load for mothers.
Notably, within the fathers’ group—but not among the mothers—an indirect relationship was identified between the child's gender and the father's education level, on the one hand, and feelings of emotional load, parent–child play, the communication experience with the child, and the child's communication skills, on the other hand, with involvement in treatment acting as a mediating variable (Figure 2).
The association between the child's gender and fathers’ involvement in treatments by SLPs, indicates that fathers tend to be more involved in the treatments of boys. This trend warrants further investigation, and adjustments in guidance given by SLPs should be considered to encourage greater participation of fathers of girls with ASD. Additionally, the level of the fathers’ education was directly correlated with their involvement in treatments, suggesting that fathers with higher education levels were more actively involved. This observation is consistent with prior research, such as the study conducted by Sharabi and Marom-Golan (2018), which demonstrated a positive impact of parental education level on involvement, particularly among fathers.
Indeed, within the cohort of fathers, involvement in treatments emerges as a significant mediating factor between the child's gender and the father's education level, influencing various aspects such as feelings of emotional load, parent–child play, communication experiences, and the child's communication skills. This suggests that fathers of boys who are more involved in treatments, also report more play and better communication with their child, as well as a reduction in feelings of emotional load, compared to fathers who are less involved in treatment. Similarly, fathers with higher levels of education tend to exhibit increased involvement in treatments, resulting in enriched play and communication experiences with their child and a decrease in feelings of emotional load.
The identification of involvement in treatment by SLPs as a mediating factor emphasizes the special significance that fathers derive from interventions by SLPs and highlights the crucial need to include fathers into habilitation programs. By recognizing and encouraging paternal involvement, SLPs can better address the unique needs and challenges faced by fathers of children with ASD, ultimately contributing to more effective outcomes for both fathers and their children. This emphasizes the importance of inclusive and comprehensive approaches in supporting families of children with ASD.
Limitations and Future Research
The present study examined the relationship between parental involvement in treatment by SLPs and its association with various aspects of parent–child play, communication, and feelings of parental emotional load. Notably, the study did not explore other variables, such as the severity of autistic characteristics and social support (Benson, 2006; Sharabi & Marom-Golan, 2018). Incorporating these variables could enrich our understanding of the dynamics at play in such interactions. Moreover, gathering input from therapists and teachers could offer valuable insights beyond parental perspectives. Also, therapists often integrate principles from diverse treatment methodologies including the Hanen approach, developmental, individual, differences, the DIR, and the NDI, that are common for young children in Israel (Ferman & Segal, 2024). It is therefore challenging to categorically identify treatments based on distinct approaches.
It is important to acknowledge that the study's findings are based on correlational data, which inherently limits the extent of possible conclusions regarding causality. To delve deeper into causal implications, longitudinal studies tracking the different variables over time or utilizing more qualitative approaches for in-depth exploration should be conducted. Future studies of parents from low SESs and comparisons between families from high and low SESs may also facilitate a better understanding of the possible interactions between SES, gender, and parents’ involvement in treatments.
Clinical Implications
The current study emphasizes the central role of parental involvement in treatments led by SLPs, particularly in fostering parent–child communication and facilitating diverse play experiences. It emphasizes the significance of involving parents of both genders in these treatments to enhance opportunities for mutual play and communication with their child. Specifically, supporting fathers of children with ASD is highly relevant in light of the changing roles of fathers in the family (Dette-Hagenmeyer et al., 2014). Therefore, it is essential for practitioners, including SLPs, family therapists, and teachers, to prioritize the inclusion of both parents in therapeutic interventions. Notably, involving fathers in treatments is associated with reduced feelings of emotional load, thereby contributing to a more positive family climate.
The results also highlight the necessity of considering parental gender, education level, and the child's gender when designing treatment plans. Special attention should be paid to involving fathers of girls and fathers with lower education levels to ensure comprehensive support and involvement.
In light of these findings, it is hoped that both SLPs and teachers will pay attention to the similarities and differences between fathers and mothers in the treatment process in order to achieve optimal outcomes for the entire family unit.
Footnotes
Author Contributions
NK and OS contributed to the design and implementation of the research. NK was responsible for data collection and authored the initial draft. OS conceived the original idea and supervised the project and played a key role in analyzing the results and writing the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Research data supporting this publication are available by request from the authors.
Appendix
Appendix B. Questionnaire on Parental Involvement in Treatment
SLP: speech-language pathologist.
No.
Items
Not at all
A few times
Sometimes
Often
Always
I look for information and I am updated on everything related to my child's functioning
1
2
3
4
5
I regularly maintain contact with my child's SLP, in person, by phone, or in writing
1
2
3
4
5
I regularly update my SLP with information about my child and family
1
2
3
4
5
I make sure that my child attends kindergarten regularly
1
2
3
4
5
I watch the therapy given to my child by the SLP
1
2
3
4
5
I attend meetings with the SLP and other parents
1
2
3
4
5
I attend regular meetings with the SLP to receive guidance and reports
1
2
3
4
5
I participate actively in my child's therapy session with the SLP
1
2
3
4
5
I ask the SLP for guidance in order to help and facilitate my child's development
1
2
3
4
5
I implement the SLP's professional recommendations
1
2
3
4
5
I participate in the process conducted by the SLP of diagnosing and evaluating my child
1
2
3
4
5
I participate in making decisions about my child's therapy plan in treatments by the SLP
1
2
3
4
5
I share my child's therapy plan with the SLP treatment with the extended family
1
2
3
4
5
I am aware of my child's needs and of changes in his/her functioning
1
2
3
4
5
I make sure to stay updated with relevant information about my child's functioning, development, and rights
1
2
3
4
5
I set expectation that are appropriate to my child's condition
1
2
3
4
5
I look for additional therapeutic alternatives for my child
1
2
3
4
5
I critically evaluate the recommendations provided by the SLP
1
2
3
4
5
I coordinate between all the therapists that treat my child and our family, including the SLP
1
2
3
4
5
I am in contact with other families for information and support
1
2
3
4
5
I initiate ideas to improve the quality of the services provided by the SLP
1
2
3
4
5
I am ready to accompany and support other families involved in SLPs’ therapeutic programs
1
2
3
4
5
Appendix C. The Hebrew Version of the Zarit Caregiver Burden Scale
No.
Items
Never 1
Almost never 2
Sometimes 3
Never 4
Almost never 5
Do you feel that you do not have enough time for yourself?
Do you feel stressed between caring for your child and trying to meet other responsibilities?
Do you feel angry when you are around your child?
Do you feel that your child currently affects your relationship with family members or friends in a negative way?
Do you feel strained when you are around your child?
Do you feel that your health has suffered because of your involvement with your child?
Do you feel that you do not have as a much privacy as you would like because of your child?
Do you feel that your social life has suffered because you are caring for your child?
Do you feel that you have lost control of your life since your child's ASD diagnosis?
Do you feel uncertain about what to do about your child?
Do you feel that you should be doing more for your child?
Do you feel that you could do a better job caring for your child?
Appendix D. The Parent Play Questionnaire
Thinking Back Over the
No.
Mode of playing
Never
Less than once a week
Once or twice a week
Several times a week
Once or twice a day
Several times a day
1.01
Active physical play—e.g., lifting or swinging your child, rough and tumble
1.02
Gentle physical play—e.g., tickling, moving child's limbs, playing finger games, such as “this little piggy”
1.03
Play with toys—e.g., grasping/holding/shaking toys, putting rings on a stack, or building blocks
1.04
Pretend games—e.g., make a toy dog bark, talk on a toy telephone, move a wooden block as if it is a car
1.05
Turn-taking play without toys/other objects—e.g., peek-a-boo, pat-a-cake, “where's baby's eyes?,” and “I spy”
1.06
Play with books—e.g., pointing to pictures in books and magazines, reading to your child
This is a quality control question—please select “Never”
1.07
Noisy play—e.g., banging saucepans or children's instruments
1.08
Singing—e.g., singing nursery rhymes
1.09
Symbolic play, e.g., feeding and bathing a doll
1.10
Role-playing games, e.g., doctor and patient, and teacher and students
1.11
Building games, e.g., building blocks, magnets
1.12
Board games, e.g., puzzle or memory game
Appendix E. The Parent–Child Communication Questionnaire
No.
Item
1 Do not agree at all
2
3
4
5
6
7 Strongly agree
I understand my child's intentions and desires
Strangers understand my child's desires
My child initiates communication (turns to me, asks for help, etc.)
My child can communicate effectively with adults who don’t know him/her well
My child can communicate effectively with same-age peers
I enjoy communicating with my child
I feel that my child understands me
My child participates in communication with family members during family activities
My child can share experiences with me (e.g., kindergarten events)
My child can share an emotional experience with me
My child and I can have a conversation
Communicating with my child frustrates me
I feel that I can communicate with my child