
Abstract
Background and aims
Although social resources and self-esteem are well-known predictors of subjective well-being in the general population, the relations among these factors have not yet been investigated in autism spectrum disorder (ASD). The present preliminary study sought to compare the levels of life satisfaction, self-esteem and perceived social support between adults with ASD and typically developing volunteers (TYP). It also examined whether self-esteem would moderate the effect of perceived social support on life satisfaction in adults with ASD.
Methods
Fifty-seven adults with ASD without intellectual disability and 60 age-matched TYP in the United Kingdom (UK) completed self-reported measures of perceived social support, global self-esteem, and life satisfaction.
Results
Results indicated that adults with ASD reported significantly lower levels of life satisfaction and self-esteem (but not social support) than TYP. Hierarchical regressions revealed that both social support and self-esteem were significant predictors of life satisfaction in adults with ASD. Self-esteem buffered the effect of perceived social support on life satisfaction.
Conclusions
This study corroborated a growing body of evidence that suggests that adults with ASD report lower levels of self-esteem and life satisfaction than TYP. In addition, it reported for the first time that global self-esteem influences the association between social support and life satisfaction in adults with ASD.
Implications
The present findings suggest that interventions aimed at enhancing self-esteem and cultivating social relationships could be important areas for intervention to improve the well-being of adults with ASD.
Research on autism spectrum disorder (ASD) has broadly shown poor psychosocial outcomes in adulthood (Lord et al., 2020; Pickles et al., 2020). Although most of the psychosocial research on adults with ASD has focused on objective aspects of well-being such as living conditions, unemployment, and adaptive functioning, it is important to note that well-being is a multifaceted construct that also encompasses a subjective dimension such as the degree of perceived life satisfaction (LS). LS is the global evaluation of the quality of one's life and is regarded as an important component of subjective well-being (Diener et al., 2003). Studies that have compared aspects of well-being in adults with ASD to neuro-typical (TYP) adults have shown that their LS is generally poor. For example, Schmidt et al. (2015) investigated a sample of 43 adults with ASD without intellectual impairment in Germany, using a quality-of-life self-reported scale. They found that ASD adults were generally less satisfied with their life than were non-clinical participants, and this trend of less satisfaction with life was particularly relevant in the areas of social aspects of life. More recently, Scheeren et al. (2022), using a Dutch autism cohort sample, reported that ASD adults with above-average intelligence reported lower general LS than the comparison community group. Further research is needed to identify predictors that may promote positive outcomes of LS in adults with ASD. Identification of correlates of subjective well-being is imperative to help us develop effective targeted interventions for adults with ASD.
The presence of perceived social support (PSS) has been shown to be associated with LS in neurotypical populations (Kong et al., 2015). Given its relationship with well-being, PSS has been examined in individuals with ASD. The results of these studies are inconsistent; for example, Bishop-Fitzpatrick et al. (2018) have shown that adults with ASD without co-occurring intellectual disabilities (N = 40; aged 18–44 years) self-report lower PSS compared to TYP, whilst others have shown that adults with ASD have PSS comparable to both TYP (Jennes-Coussens et al., 2006) and ADHD adults (Alvarez-Fernandez et al., 2017). While these initial findings suggest that some individuals with ASD may report lower social support, the relation between PSS and well-being in adults with ASD has only been investigated by one study of 46 newly employed adults with ASD who were participating in a supported employment program (Hedley et al., 2019). Results showed that self-reported PSS was associated with a measure of positive well-being. More research into the role of social support on the subjective well-being of adults with ASD is therefore needed.
Besides social support, global self-esteem is another widely examined predictor of LS in TYP (Diener & Diener, 2009). Research has shown that adults and adolescents with ASD show lower global self-esteem than TYP (McCauley et al., 2019). Interestingly, some studies in the neurotypical population have shown that self-esteem exhibits a moderating function between some psychological constructs (e.g., social support, perceived sexist events) and psychological well-being and distress (Kong et al., 2013; Moradi & Subich, 2004). It has therefore been proposed that self-esteem may have a “buffer” role which strengthens the effect of social support on LS as a moderator (Kong et al., 2013). Indeed, Chen and Bello (2017), using a sample of undergraduate students taking an introductory communication course at a public university in the US (N = 382, age range 18–30 years), found that providing social support on Facebook significantly improved LS among students with low self-esteem whilst providing social support on Facebook did not influence LS among students with high self-esteem. To the best of our knowledge, no study has examined the moderating role of self-esteem on the relationship between social support and LS in ASD. The present study was thus designed to fill this gap.
In summary, self-esteem and social support seem to be related to LS. However, the association of both factors with LS in ASD has, to our knowledge, not yet been studied. The present study aimed to investigate group differences between adults with ASD and typical controls in PSS, self-esteem, and LS. Additionally, it aimed to explore the unique contribution of PSS and self-esteem on LS of adults with ASD, and a potential moderating effect of self-esteem on the relationship between PSS and LS. To achieve the aims of the present study, the following research questions (RQ) were formed:
Are there significant differences in self-esteem, PSS, and LS between adults with ASD without intellectual impairment and TYP? Are PSS and self-esteem significant predictors of LS of adults with ASD without intellectual impairment? Does self-esteem moderate the association between social support and LS in ASD?
Method
Participants
The sample included 57 adults with ASD (19 females) between 18 and 45 years of age (M = 31.10, SD = 8.14) and 60 (28 females) TYP, matched on mean chronological age, between 19 and 44 years (M = 29.62, SD = 7.15). Adults with ASD were recruited from a university campus and from an employment support agency specialized for adults with ASD (both located in London, UK). An official letter from a general practitioner confirming ASD diagnosis was provided by each participant to establish eligibility. Additional inclusion criteria included age 18–45 years and an intelligence quotient (IQ) > 80, as assessed by the Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 2008). We focused on the 18–45 age range because research has found that physical and mental health problems in middle and older adulthood on the autism spectrum are higher than those found in younger adult samples (Bishop-Fitzpatrick & Rubenstein, 2019), and these may cloud interpretations of what is driving self-reported LS. The full-scale IQ of the sample of adults with ASD was average (M = 99.34, SD = 10.80). Exclusion criteria included the presence of any known comorbid medical conditions, physical disabilities, visual impairment, hearing impairment.
The TYP control group was recruited from a Greater London, UK, university campus and social media platforms. TYP reported that they did not identify with being on the autism spectrum and had never received a diagnosis of ASD. The exclusion criteria were (a) any physical disabilities, visual impairment, hearing impairment, or developmental disabilities; and (b) attending special education schools or classes. Demographic characteristics of participants are presented in Table 1. Adults with ASD and TYP did not differ significantly with regard to age, sex and race/ethnicity suggesting that group matching was successful. As expected, adults with ASD and TYP did differ significantly in terms of education and independent living. Ethical approval for the study was obtained, and all participants gave written informed consent (consistent with the Declaration of Helsinki) in compliance with the University of Greenwich Research Ethics Committee.
Demographic characteristics of participants.

Independent t-test or Fisher's exact test, two tailed.
*p < .05. **p ≤ .001.
Materials
Perceived social support
The Multidimensional Scale of PSS scale (MSPSS; Zimet et al., 1988) was used to examine the availability of social support from family, friends, and broadly defined significant others. The MSPSS consists of 12 items that are answered on a 7-point Likert-type scale ranging from 1 = strongly disagree to 7 = strongly agree. Questions include items such as “My family really tries to help me,” “I can count on my friend when things go wrong,” “I have a special person who is around when I am in need.” The total score was calculated, with higher values indicating higher levels of PSS. Cronbach's alpha coefficient was 0.84 in the current study.
Self-esteem
Self-esteem was measured by the Rosenberg Self-esteem Scale (RSES; Rosenberg, 1965), which is a 10-item self-report measure of global self-esteem. The scale includes questions such as “I take a positive attitude toward myself,” “I feel that I’m a person of worth, at least on an equal plane with others,” “I feel that I have a number of good qualities,” Each item is answered on a 4-point Likert-type scale. Scale scores are the sum of items (with reverse coding of relevant items) with higher scores indicating higher self-esteem. In the present study, the Cronbach alpha coefficient for the RSES was 0.84.
Life satisfaction
The Satisfaction with Life Scale (SWLS, Diener et al., 1985) was used to measure the cognitive component of subjective well-being. This was a 5-item questionnaire using a 7-point Likert scale ranging from 1 (totally disagree) to 7 (totally agree) and includes items such as “In most ways my life is close to my ideal,” “The conditions of my life are excellent.” A total score was obtained by adding up participants’ responses. Scores can range from 5 to 35, with higher scores indicating more satisfaction with life. In this study, Cronbach alpha coefficient was 0.78.
Data analysis
Variables were checked for normality and homogeneity assumptions of parametric tests and no violations were found. Independent samples t-tests were conducted to investigate whether there were any significant group differences in PSS, global self-esteem and LS between ASD and TYP (RQ1). Pearson's correlation coefficients were run to determine bivariate relationships between variables of interest. The relations between PSS, self-esteem, and LS were examined using hierarchical multiple linear regression predicting LS from PSS and self-esteem (after controlling for demographic variables) for the ASD group only (RQ2). Next, to test the moderating effects of global self-esteem on the relationship between PSS and LS in ASD (RQ3), a self-esteem × PSS interaction term was entered in the third step of the regression model. Before testing the moderating effects, the two predictor variables (PSS and global self-esteem) were standardized to reduce problems associated with multicollinearity between the interaction term and the main effects (Frazier et al., 2004). Thus, z-scores were calculated for PSS and global self-esteem. All analyses were conducted using IBM SPSS 26 (International Business Machines (IBM) Corp., 2019).
Results
Group differences in self-esteem, PSS, and LS
There was a significant difference in the scores of LS between the ASD (M = 13.30 SD = 3.73) and TYP (M = 19.01, SD = 6.60) groups t(117) = −3.187, p < .01. Based on the suggested cut-off points on SWLS, a score below 15 indicates dissatisfaction with life. Adults with ASD reported lower levels of LS than non-ASD adults (χ 2 = 9.3; df = 2; p < .05). Forty-seven individuals with ASD (78%) reported dissatisfaction with life, whereas only 23 TYP (38%) reported low LS. The two groups also showed significant differences in scores of global self-esteem t(117) = −2.122, p < .05. Adults with ASD reported lower scores of global self-esteem (M = 23.02, SD = 3.08) than TYP (M = 25.51, SD = 5.78). No significant differences were found between adults with ASD (M = 28.57, SD = 8.76) and TYP (M = 26.22, SD = 10.98) on scores of PSS t(117) = 1.098, p > .05.
Relations Between PSS, Self-esteem and LS in ASD
The relations between age, gender, education level, living status, self-esteem, PSS and LS were investigated using a series of Pearson's correlations in the ASD group only (Table 2). It was found that demographic variables did not correlate with LS. PSS (r = .423 p < .01) and self-esteem (r = .330, p < .05) were significantly correlated with LS in adults with ASD.
Intercorrelations among variables.
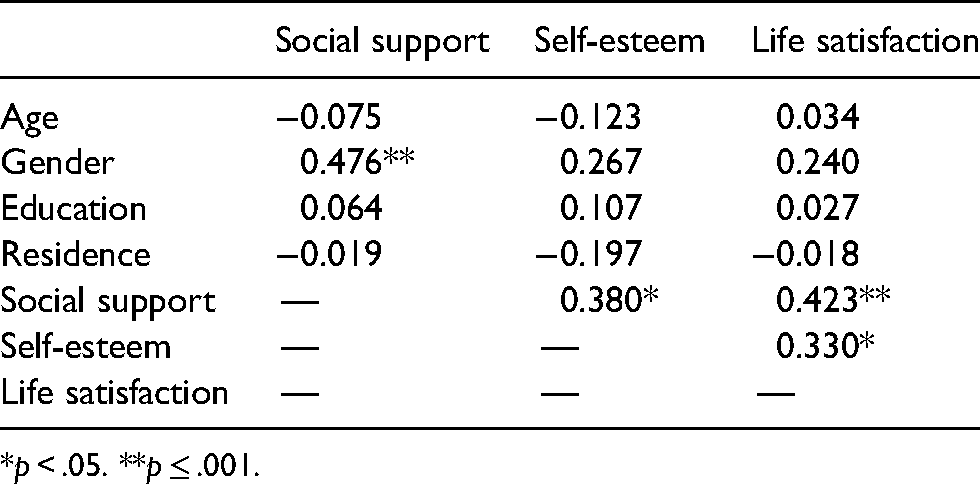
*p < .05. **p ≤ .001.
A hierarchical multiple regression analysis was performed to investigate the direct and moderating contribution of PSS and self-esteem to LS (Table 3). The results of the first block introducing demographic variables as controls was not significant R2 = .065, F(4, 53) = 1.783, p > .05. In the second step PSS and self-esteem contributed significantly to the variance of LS in ASD adults, explaining 19.4% of the variance ΔR2 = .178, F(6, 51) = 4.730, p < .05). It was found that both self-esteem and social support significantly predicted LS. To test for moderating effects the PSS × self-esteem interaction term was included in the third step of the regression analysis. Significant change in R2 for the interaction term indicates a significant moderator effect. Results indicated that the total variance rose to 43% showing a further 23.6% increase of the variance explained ΔR2 = .383 F (7, 50) = 8.965, p < .001.
Hierarchical multiple regression analyses predicting life satisfaction from self-esteem and perceived social support in adults with autism spectrum disorder (N = 57).

*p < .05. **p ≤ .001.
To clarify the PSS × global self-esteem interaction for LS in adults with ASD, we plotted the regressions of PSS on LS at high and low levels of self-esteem (Figure 1). We used the simple slope for the regression of LS on social support by using the high (1 SD above the mean) and low (1 SD below the mean) values for self-esteem. The relation between PSS and LS at high levels of self-esteem was non-significant (β = .096, p > .05). However, at low levels of self-esteem, the relationship between PSS and LS in adults with ASD was significant (β = .155, p < .05). Therefore, among adults with ASD, in those with low self-esteem, PSS significantly improved LS. In contrast, among adults with ASD with high self-esteem, PSS did not influence LS.

Effects of providing social support and self-esteem on life satisfaction in adults with autism spectrum disorder (ASD).
Discussion
The current study examined the role of PSS and global self-esteem on LS in a sample ASD adults without intellectual disability. This study corroborates a growing body of evidence that suggests that adults with ASD report lower levels of self-esteem and LS (but not PSS) than TYP (RQ1). It also expands the current literature in that it indicates that high levels of both PSS and self-esteem are significantly associated with LS in adults with ASD (RQ2). In addition, it reported for the first time that global self- esteem influences the association between social support and LS in adults with ASD (RQ3).
Consistent with prior research (McCauley et al., 2019; Scheeren et al., 2022; Schmidt et al., 2015), results indicated that adults with ASD without co-occurring intellectual disabilities have significantly lower levels of LS and self-esteem than TYP. The high prevalence of 78% in the current sample suggests that low LS in adults with ASD is a major issue. Therefore, mental health professionals should assess levels of subjective well-being in patients with ASD, especially in the presence of low self-esteem.
Adults with ASD did not report lower PSS scores than TYP. This finding is in agreement with prior literature which showed that adults with ASD might report comparable PSS to non-ASD individuals (Alvarez-Fernandez et al., 2017; Jennes-Coussens et al., 2006). Specifically, in Jennes-Coussens et al. (2006) 12 adults with Asperger's syndrome showed similar total PSS score relative to 13 TYP, whilst Alvarez-Fernandez et al. (2017) reported that adults with ASD presented significantly lower scores for social support from friends but not from family or significant others compared to adults with ADHD and TYP. Thus, the finding of the present study that adults with ASD without co-occurring intellectual disabilities do not experience significantly lower levels of PSS than TYP expands this line of research.
This is the first study to report that both social support and self-esteem explained a significant amount of variance in LS of adults with ASD. These findings indicate that attention for low self-esteem and social support could be part of interventions that target improvements in mental health for individuals with ASD. Although adults with ASD did not report low perceived support, they are still likely to derive benefits from social support which would in turn have implications for intervention planning.
This study also seems to be the first one to report that global self-esteem can act as a moderator of the relationship between social support and LS in ASD. This study complements Chen and Bello's (2017) finding, in typical adults, by suggesting that social support may be more important for LS in ASD adults with low self-esteem than for adults with high self-esteem. ASD adults with high self-esteem may already hold a positive view of themselves, and therefore probably do not need as many social resources. In contrast, individuals with low self-esteem may be able to enhance their self-worth when they receive more social support and accordingly increase their satisfaction with life. The validity of such an explanation, however, needs more research to determine the causal mechanisms driving the observed pattern of relations.
This study yields valuable information for the design of psychosocial interventions for adults with ASD. Previous studies showed that interventions specifically designed to enhance self-esteem in adults with ASD showed no significant change in self-esteem (Hesselmark et al., 2014; Spain & Blainey, 2017). The self-esteem × PSS interaction found in the present study and the study of Chen and Bello (2017) suggests that it could be possible that through the process of receiving or providing support, individuals with low self-esteem may gradually boost their self-esteem, and hence reap psychological benefits such as improved LS. We propose that targeting both PSS and self-esteem in future research on ASD, and in interventions, may provide considerable psycho-therapeutic power as well as explain important social psychological processes.
This study has a number of limitations, the main one being the small sample size. Unfortunately, accessing to a larger adult ASD sample is of great complexity. Other important aspects are the location of the participants, which is a single large city, and the fact that the specific sample consisted of adults with ASD without intellectual disability who has achieved adequate levels of independence through employment and/or university studies. This implies that our findings may only apply to populations that share the same characteristics with our sample. However, this setting invites us to perform future research where could be possible to design studies at a nationwide level. Another limitation worth mentioning is the subjective character implied in the evaluation through a self-report. Even when every participant from the first study had a ASD diagnosis, the instruments applied reflect their own perception of their own functioning which could be biased to their personal concept of standards. Finally, the data of the present study are cross-sectional, and thus findings cannot imply causal relationships. Future studies should assess bidirectional effects of social support, self-esteem and LS in order to tease out causality.
Despite these limitations, this study suggests that LS and self-esteem of individuals with ASD seem to be lower than in the general population. The current study also highlights the role of PSS and self-esteem on LS in ASD and provides support that improving these factors through targeted intervention for adults with ASD may indeed improve their well-being. Psychosocial interventions that teach skills to improve self-esteem and increase social support to ASD adults might help them achieve better subjective well-being and ultimately a better quality of life.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for the study was obtained (consistent with the Declaration of Helsinki) in compliance with the University of Greenwich Research Ethics Committee.
Informed Consent
All participants gave written informed consent.