
Abstract
Background
The purpose of this study was to evaluate the feasibility of a personal narrative intervention based on neurocognitive principles and experientially based learning for improving the personal narrative language abilities of a school-age child with Down's syndrome.
Method
A single-case design using contemporary statistical techniques was employed to complete this study. The participant was 8 years 8 months at the time of the study and he participated in a 14-week personal narrative intervention. Personal narrative samples were collected at the beginning of each intervention session prior to instruction. Narrative samples were scored for narrative quality, language productivity, and lexical diversity.
Results
As a result of the intervention, the participant demonstrated moderate-significant increases in narrative abilities for narrative quality, language productivity, and lexical diversity.
Conclusions
The use of a personal narrative based on neurocognitive principles and experientially based learning may be feasible for improving the personal narrative language abilities of school-age children with Down's syndrome.
Introduction
Down Syndrome (DS), caused by a trisomy of chromosome 21, is the most common non-inherited genetic cause of intellectual deficit (ID). The genetic disruption also results in a disordered language system manifesting in different degrees of impairment across the domains of phonology, semantics, morphology, syntax, and pragmatics (Abbeduto et al., 2007; Martin et al., 2009; McCabe & Bliss, 2003; McCabe & Marshall, 2006).
Studies of language intervention for individuals with DS often focus on improving speech intelligibility, phonological awareness, or receptive and expressive knowledge of grammar, syntax, or vocabulary in decontextualized contexts (Smith et al., 2020). This research suggests that decontextualized instruction can be useful in bringing about improvements in various aspects of language; however, there are at least three reasons why decontextualized language instruction may not be the ideal first intervention option for individuals with DS. First, individuals with DS consistently demonstrate poor generalization of newly learned skills to novel, untrained contexts (Burgoyne et al., 2012). Second, language skills are rarely used in isolation during authentic conversational contexts (Ukrainetz, 2015 p. 49). Rather, a speaker must integrate knowledge across language domains to communicate even the most elementary messages to listeners. Alternatively, the listener must also be able to process and integrate incoming verbal information to make sense of messages for which they are the recipient. The most basic social interactions require knowledge of how to understand and use language to learn, share, and engage with others. Often, individuals with DS have difficulty integrating information that they learn in isolation and generalize skills into social contexts. Even if we can bring about isolated change in language abilities for individuals with DS, it is unlikely that teaching them outside of authentic contexts will transfer to meaningful communicative contexts that require discourse-level language proficiency (Gillam et al., 2012; Miller et al., 1999). Finally, and perhaps most importantly, a robust body of research has shown that individuals with DS tend to seek out social experiences more often than other individuals with intellectual deficits and/or demonstrate a strong preference for socially oriented interactions (Fidler & Nadel, 2007; Jahromi et al., 2008; Reed et al., 2011; Rosner et al., 2004). The overall importance of social interactions to individuals with DS makes discourse-level language abilities an essential goal for intervention. Although social skills are often viewed as an area of strength for individuals with DS, there are significant qualitative differences in their social cognitive abilities that impact the development of socially competent behavior (Abbeduto et al., 2001).
To illustrate, Abbeduto et al. (2001) investigated domain asynchrony (i.e., skills that are “especially impaired” when compared to other skills) and syndrome specificity (features most likely associated with DS when compared to others with intellectual disabilities). They explored domain asynchrony and syndrome specificity in social cognition tasks for individuals with DS and Fragile X. Social cognition was measured using traditional 1st and 2nd order theory of mind (TOM) tasks in a narrated story that required individuals to answer questions about the beliefs of characters related to the location of objects and what each character did (or did not) know or observe during the story. Theory of mind measures may be used to assess foundational skills for performing social tasks such as meeting the needs of a listener, creating coherent and complete narratives, comprehension monitoring, understanding others’ feelings and perspectives, and participating in tasks involving deception. The findings of this study underscore the importance of discourse-level language abilities for social-communicative competence in children with DS. In terms of domain asynchrony, performance on the TOM tasks of individuals with DS appeared to be “asynchronous” or “more impaired” than expected given their nonverbal cognitive skills (measured using the Stanford-Binet; Thorndike, 1986). Evidence from TOM tasks demonstrated that social cognitive impairment was “syndrome specific,” with individuals with DS performing significantly more poorly on tasks measuring TOM than individuals with Fragile X (Abbeduto et al., 2001).
Socially competent behavior requires the successful coordination of multiple social-cognitive, linguistic, and contextual factors to meet the dynamic demands of various social situations (Brinton & Fujiki, 2005; McCabe & Meller, 2004). The emerging evidence suggests that limitations in social-cognitive skills and expressive language combined with insufficient contextual supports (inherent in decontextualized intervention) may decelerate the development of social competence among individuals with DS (Iarocci et al., 2007). To mitigate the influence of these factors, language intervention activities should 1) consider the specific strengths and weaknesses of individuals with DS (Grieco et al., 2015); 2) incorporate opportunities to practice discourse-level skills that involve the integration of multiple domains of language (Iarocci et al., 2007); and 3) be conducted in authentic contexts to facilitate the development of language to support social competence (Burgoyne et al., 2012).
We were able to locate only one discourse-level intervention study that incorporated these considerations into their approach. In this study, Finestack et al. (2017) explored the effects of a personal narrative intervention for four children with DS between the ages of 10–15. The instruction targeted three grammatical (microstructure) goals (elaborated noun phrases, advanced verb phrases conjunctions) and three discourse-level (macrostructure) goals focused on improving abilities in producing personal narratives (the use of character, setting, actions, dialogue, mental states). The researchers developed scripted accounts of personal events (n = 18; one per session) that contained at least five examples of the week's targeted grammatical goal; five examples of the week's personal narrative goal (macrostructure); were 15 sentences in length and contained less than 200 words. The clinicians introduced and explained weekly goals and presented a picture representing the modeled personal narrative on an iPhone or iPod Touch(iTouch), which served as a visual cue to support recall of the story.
The interventionist told the pre-developed scripted story and reviewed it again to highlight the grammatical and narrative goals that were the focus of that session. Next, participants were asked to retell the modeled personal narrative as the interventionist pointed out the essential macrostructural elements. The participants were encouraged to use the visual cue to support their retell and were eventually introduced to a second visual support in the form of a narrative map. The narrative map contained cells with cue words “when, where, who, what, talking, and feelings” to represent the macrostructure elements that were the intervention's overall focus (i.e., setting, character, action, dialogue, mental states).
During each session, participants were asked to imitate 12 sentences that contained the targets they were learning to practice using them. The last aspect of each session involved supporting students through a series of steps to create their own narrative based off of pictures of a recent event in their life. The clinician assisted in locating a picture of an event they had stored on their iPhone/iTouch from the activity that they had participated in and creating a story using the narrative map with assistance from the interventionist. They were asked to complete a narrative map for their personal event. After they had drafted the story, students being reminded to use the dialogue, mental state, discourse, and grammatical targets they had been working on when telling their story.
The consistent use of microstructure (measured in mean length of utterance in morphemes) and macrostructure targets (measured using a researcher designed rubric) was observed to improve for two of the four participants with DS that were maintained over time. To examine more closely whether or not students used targeted macrostructure elements in their personal narratives, researchers examined retells for the presence of wording related to wh-components (who, what, where, and when). This measure showed that 3 of the 4 participants demonstrated gains in their use of macrostructure.
We drew upon many of the study procedures utilized by Finestack et al. (2017) to design our intervention activities, with some modifications based on neurocognitive principles of language processing and experientially based learning (van der Schuit et al., 2011). Neurocognitively-based interventions include 1) memory components to support storage and retrieval of newly learned concepts and vocabulary from long term memory (LTM); 2) unification components to support the integration of newly learned information with information already in LTM; and 3) control components to make use of relative strengths and mitigate weaknesses that contribute to learning difficulties. These procedures, activities, and supports are described in the section detailing our intervention approach below and are also shown in Table 2.
Language Facilitation Technique Descriptions
The purpose of the current project was to evaluate the feasibility of a personal narrative intervention based on neurocognitive principles and experientially based learning for improving personal narrative language abilities of a school-age child with DS. We asked the following research questions:
Does the use of a personal narrative intervention increase the complexity of personal narratives used by children with DS as measured by the children's ability to produce a Complete Personal Narrative Event (CPNE) using the CPNE rubric? Does the use of a personal narrative intervention increase language productivity in personal narratives told by children with DS to familiar and unfamiliar listeners and measured by total number of utterances (TNU) and mean length of utterance in morphemes (MLUm)? Does the use of a personal narrative intervention increase the use of diverse vocabulary used in personal narratives told by children with DS as measured by verbs per utterance (VPU) and number of different words (NDW)?
Method
Participant
The Internal Review Board at Utah State University reviewed this project and approved the procedures. The participant, Daniel (pseudonym), was 8;8 years of age and had a diagnosis of Down syndrome (DS). He was in the third grade at the time of the study. He was recruited through convenience sampling from a local university speech and language clinic. Daniel had been receiving individual speech and language intervention since the time he was four years of age. During the course of the study, he was also receiving speech and language intervention at his school three times a week for 20 min each session. He was not receiving narrative intervention at his school or in the clinic, nor had he ever received a discourse-level intervention. Daniel communicated primarily using simple sentences (MLU = 1.8) and was a native monolingual English speaker.
Prior to being recruited for this study, Daniel completed the Clinical Evaluation of Language Fundamentals – Fifth Edition (CELF-5; Wiig et al., 2013). He received a core language index score of 45 which placed Daniel's overall performance in the very low range. Daniel demonstrated difficulties in understanding spoken information, following verbal directions, answering questions about a story he had just heard, and understanding and producing different word classes. He demonstrated difficulty with the use of a variety of semantic classes, and word structure. This indicated that he had difficulty with forming and understanding compound and complex sentences. He also completed the Clinical Assessment of Articulation and Phonology – Second Edition (Secord & Donohue, 2013). He received a standard score of <55, indicating a severe articulation disorder. Further analysis revealed a phonological disorder characterized by consonant cluster reduction, stopping of fricatives, and final consonant deletion. His past speech therapy had targeted early and middle eight speech sounds (i.e., t, ŋ, k, g, f, v, ‘t͡ʃ’ and d͡ʒ) as well as consonant clusters (e.g., bl and pl). His mother reported that she noticed he had difficulties answering ‘wh’ questions like, “What did you do today at school?”. She expressed a desire for Daniel to be able to answer these types of questions so that she could better understand his wants, needs, and his perspective regarding the experiences he had when she was not present. Audiology assessments completed prior to this intervention revealed that Daniel did not have any presence of hearing impairment.
Daniel was given the Test of Narrative Language – Second Edition (TNL-2; Gillam & Pearson, 2017) and asked to generate a personal narrative describing an event he participated in with the clinician to obtain baseline information on his narrative proficiency. Daniel received a scaled score of 2 on the TNL-2 with a percentile rank of <1. His narrative language ability index was 50. Before beginning intervention, Daniel participated in three baseline sessions (three separate days over a week). After the baseline sessions were conducted, he attended 25, 50-min intervention sessions over the course of 14 weeks.
Procedures
Baseline procedures
Three baseline sessions were completed prior to the onset of intervention. During these sessions, Daniel participated in an experientially based activity (e.g., playing basketball) with the clinician. This activity lasted for approximately five minutes. Following the activity, the student and clinician walked to a separate room where an unfamiliar listener (i.e., an adult who did not participate in the activity) elicited a personal narrative by saying, “Tell me all about what you just did.” The unfamiliar listener waited for the student to respond to the verbal prompt. The graphic organizer to be used during the intervention sessions to follow baseline sessions was available for the student during the baseline session (described below). Daniel did not make use of the graphic organizer during the baseline sessions. No other prompting was provided.
Each story elicited during baseline and intervention was digitally recorded and uploaded to a secure server. They were transcribed by research assistants who were blind to the purpose of the study according to the Systematic Analysis of Language Transcripts conventions (SALT; Miller & Iglesias, 2010). Utterances from the student and examiner were transcribed verbatim. The utterances were segmented into communication units (c-units) consisting of a main independent clause and all clauses subordinated to it. In addition, the transcripts were coded for grammatical morphemes and mazing of unfinished/filler words and phrases following SALT conventions. A second research assistant reviewed each SALT transcript. The transcribers met to review each transcript, and reached consensus for transcription disagreements related to words, c-unit segmentation, and coding of grammatical morphemes and mazes. Interrater reliability was calculated for 100% of the transcripts from the study and was found to be 95.6%.
Intervention procedures
This study was approved by the Institutional Review Board (IRB) at the University. Language treatment was provided one-on-one by a graduate-level student clinician during two 50-min sessions per week over 14 weeks. The intervention was provided in a University clinic under the direction of the first author and a clinical supervisor employed by the University. Each intervention session was video and audio recorded. The first author observed all of the video recordings of the intervention sessions to calculate fidelity of implementation using a checklist designed to accompany each lesson. This checklist was used to ensure that all aspects of the lesson were being taught. If fidelity fell below 85% for any lesson, a short meeting was held with the interventionist after the lesson to talk about what was omitted. The research team made sure that any omitted information was introduced in the following session. A random sample of 20% of the videotaped sessions was reviewed by a research assistant who did not observe the lesson in person. The averaged fidelity across all of the intervention sessions idelity was 94.5%.
Outcome measures
Narrative outcome measure
A rubric was designed to evaluate the personal narratives produced by the student. Items measuring character, setting, initiating event, attempt/action, and consequence were adapted from The Monitoring Indicators of Scholarly Language (MISL; Gillam & Gillam, 2013). The revised measure included these items as well as an additional item to record the mention of asupplies/tools/toys used during the activity. These elements were combined to form a total score reflecting a complete personal narrative event (CPNE). The scale was scored using a dichotomous rating to indicate that the element was present (score of 1) or absent (score of 0). To receive a score of 1 for character, the participant was required to name both characters (i.e., themselves and the clinician). For setting, Daniel was required to state where the activity took place (e.g., playroom). To receive a score of 1 for the ‘supplies’ element, the participant was required to name all of the items used to complete the activity (e.g., baseball and baseball bat). For initiating event, the participant needed to state why the activity was being completed (e.g., we wanted to play baseball). The participant received a score of 1 for attempt if they made a statement about what actions were taken during the activity (e.g., we threw the baseball; I hit the baseball). A score of 1 was awarded if the participant made a statement about the outcome of the activity (e.g., I won the game). The total possible score ranged from 0 to 6.
Language productivity
Personal narratives obtained during baseline and at each intervention session were analyzed using the Systematic Analysis of Language Transcripts (SALT) software using the standard measures report function from the transcripts. Two measures were calculated automatically in SALT to measure language productivity. These were total number of utterances (TNU) and mean length of utterances in morphemes (MLUm). Total number of utterances was calculated by counting the number of communication units (c-units) that were included in the narrative. A c-unit consists of the main clause (i.e., subject and verb clause) and any other clauses subordinated to it. The mean length of utterance was calculated by finding the sum of the number of morphemes in each c-unit and calculating the average of morphemes across utterances.
Lexical language diversity
Two measures were calculated automatically in SALT to measure lexical diversity using the same procedures used to calculate productivity. These measures included verbs per utterance (VPU) and number of different words (NDW). Verbs per utterance was calculated by counting the number of verbs in each c-unit and calculating an average across all utterances, yielding the final VPU count. Number of different words was calculated by counting each novel word in a transcript.
Control Variable
The accurate production of /r/ in initial word position served as a measure of experimental control. The intervention provided in the clinic did not target any speech sound errors over the course of the 14 weeks of narrative intervention, and this sound was not targeted during speech therapy sessions provided in other settings (e.g., school SLP services). Each opportunity for the production of /r/ in initial word position was identified by coding all of the personal narratives collected at baseline and during each intervention session by a research assistant. A total number of the occurrences of the /r/ sound in the initial positions of words was calculated for each sample from the final transcripts. Once these words were identified, a trained research assistant listened to each audio recording and determined how many of the possible occurrences of /r/ were correct. A percentage was then obtained by dividing the number of correct productions of /r/ in the initial position by the total number of opportunities for /r/ to be produced in initial word position. This was calculated for each sample separately. Once this process was completed, a second research assistant listened to the audio recordings and double coded the correct production of /r/ in initial position of words. Interrater reliability was calculated on 100% of the scoring protocols by counting the number of disagreements, subtracting the disagreements from the total number coded and dividing by the total number of possible occurrences of /r/ in each transcript separately. An average was then calculated across all of the samples. Interrater reliability and was calculated to be 96%.
Description of the intervention
The intervention was designed to incorporate memory, unification, and control activities and procedures, each of which is listed in Table 1. We addressed memory components by 1) including icons to represent “story elements” that were the focus of each lesson (character, setting, action, material, ending/landing); 2) using a graphic organizer with the icons embedded in a way that depicted the temporal relationships between them; 3) and utilizing a story “script” called a story frame to provide repetitious verbal models that were structurally similar to support verbal working memory.
Neurocognitive-based learning procedures and activities

Based on van der Schuit et al. (2011).
Unification activities and procedures included 1) experiential play activities for meaningful learning; 2) anchored instruction organized around a central theme (Vakil et al., 2003; Verhoeven & Aarnoutse, 2000); and 3) interactive storytelling activities presented as “Curtain Time” to the student. These activities were designed to allow multiple, supported opportunities for Daniel to use language for meaningful communication purposes (Hargrave & Senechal, 2000), to capitalize on relative strengths in observational learning (Reed et al., 2011), and a preference for socially oriented interactions (Conway & Pisoni, 2008; Jahromi et al., 2008; Reed et al., 2011).
Control components were addressed by 1) obtaining data on daily performance, 2) explicitly linking language to authentic actions within the experiential play activities; and 3) allowing for “rehearsal time” in the form of scaffolded opportunities for practice in recounting events with individualized environmental supports (icons, graphic organizer, story frames, language facilitation procedures). These supports were designed to help mitigate areas of potential weakness including verbal working memory, attention (Breckenridge et al., 2013), and instrumental learning (manipulating the environment to meet their needs (Grieco et al., 2015; Reed et al., 2011).
Daniel participated in 6 instructional lessons, designed to explicitly teach each of the 6 aspects of a personal narrative that combined to construct a CPNE (character, setting, action, materials, ending/landing). Each lesson involved participation in activities involving sports/games that Daniel had indicated an interest in, as reported by his parents (mini-golf, basketball, bowling, hopscotch, balloon tennis, and soccer). During all aspects of intervention, language facilitation procedures were used to highlight different aspects of a personal narrative and to increase his language productivity and diversity. Each of the language facilitation techniques is listed in Table 2. A language facilitation strategy was selected prior to each intervention session by the clinician and first author. The clinician aimed to use the facilitation technique in at least 50% of their utterances throughout the session. Each technique was the target in at least two sessions during the intervention phase. An average of language facilitation use was taken on 20% of the sessions during the intervention. The clinician used the targeted language facilitation technique on average in 62% of their utterances.
In the first six sessions, a “scripted” fictional narrative depicting a golf activity that Daniel would later participate in as a portion of the intervention was used to teach story elements. During the lessons, icons were used to explicitly teach Daniel to use each element to create a complete personal narrative episode. The clinician taught the elements by showing him the icons in a modeled narrative by saying: “This is an icon or a symbol for the characters in our story [hold up or point to character icon.] The character is the
Once the story element lessons were complete, each session followed the same format, including 1) personal narrative performance tracking, 2) introduction of the experiential activity for that day, 3) participation in the experiential activity, 4) rehearsal time, and 5) curtain time. Each of these activities is described below.
Personal Narrative Performance Tracking. At the beginning of each intervention session, a narrative elicitation procedure was followed that was identical to baseline sessions. This was used for data collection and to monitor personal narrative growth. Careful control of the activities was employed such that activities used during performance tracking were not addressed during the intervention procedures. The participant engaged in an “in clinic” activity with the graduate student clinician prior to any intervention being completed. This activity lasted for five minutes. Following this activity, Daniel and the graduate-student clinician went to a meeting room where the first author was also present. There, the first author followed the baseline narrative elicitation procedure and said, “Tell me all about what you just did.”. After the student attempted to recount the event, the first author prompted the recall by pointing to the icons within the graphic organizer and asking the following questions:
“Who played” “Where did you play?” “What did you use to play?” “What did you do?” “What happened at the end?”
Recall that all activities used during the narrative performance tracking were different than the activities used during intervention.
Introduction of Experientially Based Activity. A new activity was introduced for intervention purposes. We utilized experientially based activities that we engaged in with the participant in order to teach Daniel to create a personal narrative (as per Finestack et al., 2019). The clinician introduced the activity for that session by showing a picture of the activity and saying, "The people in this picture are playing _____ (e.g., mini-golf). We can play ______ (e.g., mini-golf) just like them. When we play games, we like to remember what we have done so that we can tell someone else all about our fun! We are going to learn about some icons to help us remember the fun parts of the game. An icon is a picture that helps us remember parts of our game. Let's go play ______ (e.g., mini golf).”
Experientially Based Activity. During the activity, each icon representing each aspect of the personal narrative was introduced using a script. For example, to introduce the characters in the activity, the clinician said: “My name is_______. And your name is ______. We are the
Rehearsal Time. Daniel and the clinician returned to their original meeting room immediately after the experientially based activity was completed for rehearsal time. First, Daniel was given a graphic organizer containing the icons representing each of the elements of the activity. Then, the clinician used a pictographic planning procedure to assist him in recreating the event by drafting each part into the graphic organizer. An example of what the clinician said while drawing pictures on the graphic organizer with the participant is as follows: “Daniel and
Once the graphic organizer was complete, the clinician prompted him to retell the personal narrative. During the recount, the clinician encouraged Daniel to use the graphic organizer by pointing to each aspect of the story in sequential order. A script (shown in Appendix C) was used to ensure that the verbal model was consistent and was used repeatedly throughout this portion of the session to support his memory of the event. The clinician continued prompting Daniel until he included all of the components represented on the graphic organizer. This procedure continued until he was able to successfully recount the event included on the CPNE rubric, three times in a row without omitting an element.
Curtain Time. Curtain time occurred immediately after rehearsal time. During this activity, Daniel was asked by the clinician to recount the activity to a communicative partner who had not been present during the activity or rehearsal time (mother, university clinic supervisor). After asking him to tell his partner about the event, the clinician left the room. The new partner pointed to the graphic organizer with the pictographic plan drafted on it and asked Daniel to tell her what he had done with the clinician saying, “Tell me all about what you just did’.
Data analysis
A procedure defined by Kratochwill et al. (2010) was used to analyze the data from this project. The data was first observed to determine if there was a predictable pattern during the baseline phase. Then, the baseline and treatment phases were observed to determine the presence of predictable patterns. After this analysis within phases, the data was analyzed to determine whether the evidence was present that the intervention phase was associated with the expected change in narrative proficiency scores (i.e., CPNE scores). The following features were used within phases and between phases to determine data patterns: (a) level (i.e., mean scores), (b) trend (i.e., the slope of lines fitted to the data), (c) variability of scores, (d) immediacy of effect, (e) overlap, and (f) consistency. Percent of non-overlapping data (i.e., percent of data points at the intervention that is at or above the highest scores at baseline) was calculated to support the findings of the visual analysis. In addition, Tau-U was calculated for all outcome measures (Parker et al., 2011). This is a technique that measures nonoverlap while adjusting for trend and produces an effect size statistic.
Results
Daniel
Visual data for Daniel's narrative proficiency using the CPNE measure is presented in Figure 1. Scores for language productivity (i.e., TNU and MLUm) are presented in Figures 2 and 3. Scores for lexical diversity (i.e., VPU and NDW) are presented in Figures 4 and 5. Scores for the control variable (i.e., correct production of /r/ in initial position of words) are included in Figure 6. In addition, examples of Daniel's stories prior to, during and after the completion of intervention are included in Appendix D.

Scores for narratives produced prior to each intervention session.

Scores for total number of utterances produced prior to each intervention session.

Scores for mean length of utterance in morphemes produced prior to each intervention session.

Scores for verbs per utterance produced prior to each intervention session.
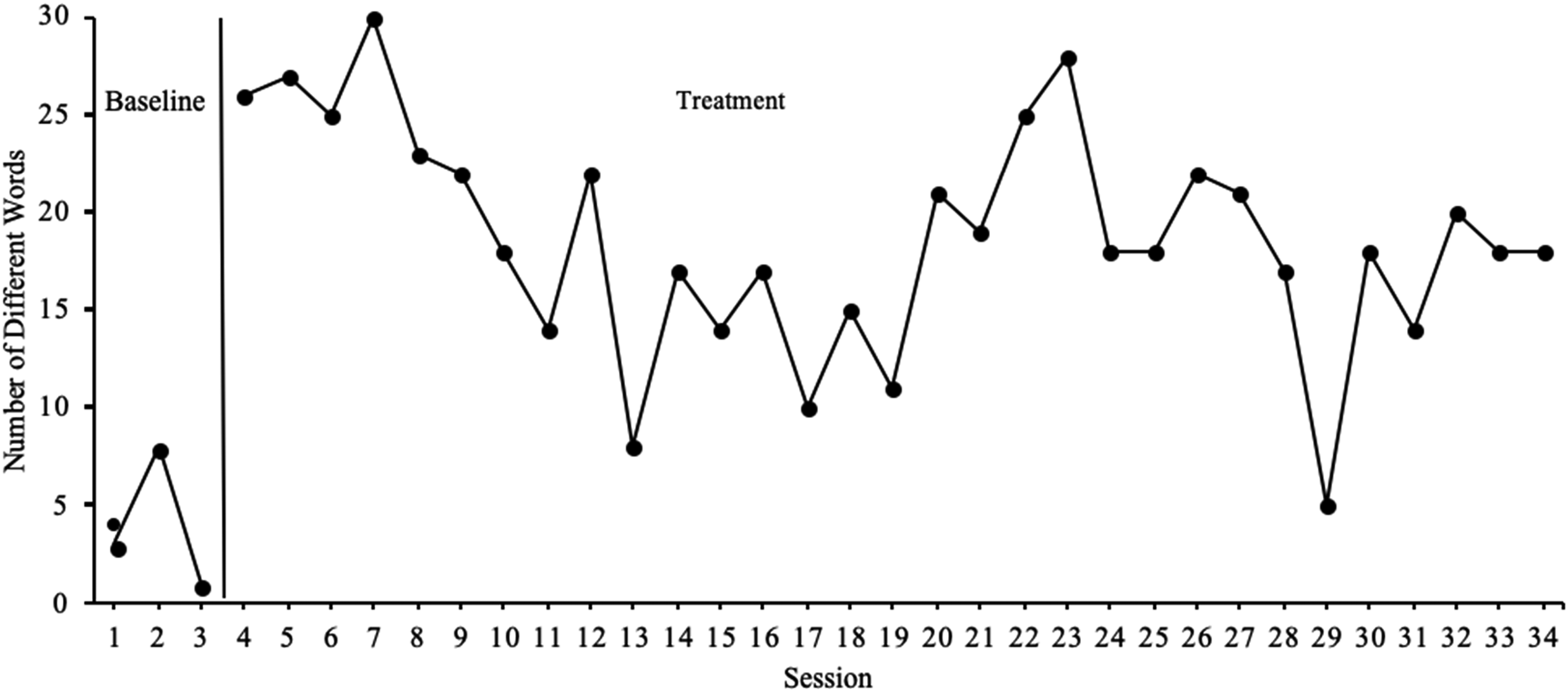
Scores for number of different words produced prior to each intervention session.

Scores for percent of correct production of /r/ produced prior to each intervention session.
Baseline
Personal narratives (CPNE) scores during baseline followed a flat trend. He obtained baseline CPNE scores of 0 out of a total of 6 for each of the three baseline sessions. No variability was observed in scores for the CPNE measure.
Daniel's scores for TNU followed a decreasing trend in the baseline. As shown in Figure 2, during the first baseline session he produced a total of 2 utterances to describe the activity he had participated in. For the second session, he produced 3 utterances. In the final baseline session, Daniel produced 1 utterance. As shown in Figure 3, in the first baseline session, Daniel received an MLUm score of 2. In the second session, he received a score of 4.33. In the final baseline session, he received a score of 1. Thus, a moderate amount of variability was observed for the MLUm measure during the baseline.
As shown in Figure 4, Daniel's scores for VPU followed a decreasing trend. In the first baseline session, he received a VPU score of .5. In the second session, he received a VPU score of 1. In the final session, Daniel received a VPU score of 0. A moderate amount of variability was observed within the second baseline session.
As shown in Figure 5, Daniel's scores for NDW followed a decreasing trend. In the first session, he received a score of 3. In the second session, he received a score of 8. In the final baseline session, he received a score of 1. A moderate amount of variability was observed for NDW within the baseline phase.
Daniel's ability to use /r/ in initial positions of words followed a descending trend before the intervention was implemented (see Figure 6). His highest baseline score was observed in the first baseline session when he demonstrated 14% accuracy in the production of the /r/ phoneme in word initial position. During the second session, Daniel demonstrated 9% accuracy of the production of /r/. In the final session, he demonstrated 2% accuracy of the production of /r/. A small amount of variability was observed in this measure during the baseline.
Intervention
Daniel's CPNE scores followed an increasing trend throughout the intervention and were moderately variable during this phase. A clear change in level was observed at the first data point (from a score of 0 to a score of 2) directly following the implementation of the intervention. Daniels CPNE scores during treatment were moderately variable but followed an upward trend. PNOD was 100% with a Tau-U score of 1 (p = .005), indicating that his ability to recount a personal narrative event to an unfamiliar listener improved significantly as a result of the intervention.
Regarding language productivity, Daniel's scores for TNU were observed to be highly variable throughout the intervention phase. A clear change in level was also observed following the phase change. Though a decreasing trend was observed for this measure across the intervention phase, the final scores in this phase were above the highest scores observed at baseline. All but three of Daniel's stories produced during intervention received a total number of utterance scores above the highest score at baseline, which resulted in a PNOD of 90.4% and a Tau-U score of .946 (p = .007). This indicated that Daniel's TNU scores improved significantly as a result of the intervention.
A clear change in level was observed from the baseline to intervention phases for the MLUm measure. Though a decreasing trend was observed throughout the intervention session, the scores received toward the end of the intervention were above the highest score at baseline. All but nine of his stories during intervention received scores above the highest at baseline, which resulted in a PNOD of 71% and a Tau-U score of .806 (p = .022). This indicated that Daniel's MLUm scores moderately improved following the implementation of the intervention.
Regarding lexical language diversity, a change in level was observed between the last baseline measure and the first measure at baseline for the VPU measure. Daniel's scores were moderately variable and followed a descending trend. All but 12 of Daniel's stories received a VPU score above the highest observed at baseline, resulting in a PNOD of 61.3% and a Tau-U score of .828 (p = .019). This indicated that Daniel's VPU scores moderately improved following the implementation of the intervention.
For NDW, a clear change in level was observed following the implementation of the intervention. Daniel's scores during this phase were highly variable and followed a decreasing trend. However, the scores Daniel received toward the end of the intervention phase were higher than the highest score observed at baseline. All but two of his stories during baseline received scores for NDW above the highest score observed at baseline, which resulted in a PNOD of 93.6% and a Tau-U score of .967 (p = .006). This indicated that Daniel's NDW scores significantly improved following the implementation of the intervention.
Daniel obtained scores for the production of /r/ that followed a flat trend throughout the intervention. No change in level was observed from baseline to the intervention phase. The scores were observed to be slightly variable, however, none of the scores during the intervention phase exceeded the highest score at baseline. This resulted in a PNOD of 0% and a Tau-U score of -.774 (p = .028) which indicated that Daniel's scores for the production of /r/ did not demonstrate a change as a result of the intervention.
Discussion
The purpose of this study was to determine if a personal narrative intervention was a feasible approach to improving the quality of personal narratives, language productivity, and language diversity for a verbal child with DS. The intervention was based on neurocognitive principles of language processing (i.e., memory, unification, and control) and utilized experientially-based learning aimed at teaching language abilities in authentic contexts. We aimed to answer three research questions related to language proficiency in the context of personal narratives.
The first research question asked whether Daniel demonstrated observable, measurable improvements in his ability to create personal narratives related to real-life events that he participated in during the intervention sessions. His early stories were short, did not include the story elements of interest, and were not informative to a listener asking about the events he and the clinician participated in. Over the course of the 14-week intervention, Daniel's stories increasingly included all of the aspects of personal narratives taught when relayed to his clinician and to unfamiliar listeners asked to interact with him. His mother also reported anectodally that he was using the elements taught during sessions to convey events he had experienced in school. For example, he reported to his mother that he was angry about another student using the slide on the playground when he (Daniel) wanted to do so. He was noted to sometimes include the names for the icons used to represent each aspect of the personal narrative when conveying events saying, “The characters were me and Lilly, and the setting was the playground. She wouldn’t let me slide and I was angry.”
This represented a significant improvement over previous conversations in which he either did not respond to “What happened on the playground today” or responded saying, “I played, or I don’t know.” His mother reported that he was more likely to produce stories with all of the elements taught if she provided him with the graphic organizer used during the intervention. During the course of the intervention, the clinician reported that she was able to elicit stories from Daniel about personal events that occurred at home or in school. For example, the clinician asked Daniel what he did over a holiday weekend. When he responded that he did not know, the clinician showed him the graphic organizer and Daniel relayed a personal event of an interaction he had with his cousins over the holiday. The implications of this finding has important social implications.
Because he was able to increase the quality of information he was able to share he was able to participate in a successful dialogic communicative interaction that he previously had not been able to engage in (Fujiki et al., 1996). Ultimately, this may improve Daniel's social relationships with his parents, family members and peers by improving the nature of those social interactions (Brinton & Fujiki, 2005). The second research question aimed to determine if the personal narrative intervention was associated with increases in language productivity and complexity as measured using TNU and MLUm. Daniel was observed to talk more after participating in the intervention program, as illustrated by increases in TNU (total number of utterances). He was also shown to use more complex language as measured using MLUm. Prior to instruction, Daniel did not contribute many statements or comments about his experiences with the clinician. The utterances he did use were simple and short in nature (i.e., low MLUm). In addition, most of his utterances were in response to direct questions or prompts with few, if any, being spontaneously initiated. In terms of complexity, Daniel's average MLUm before intervention was well below expectations for his age (2.4). However, after intervention his MLUm was observed to almost double (5.2).
Anecdotally, Daniel's mother reported that all of these language skills were being noted in the home and in the school environment. She commented that his improvements were compelling in that they occurred in only 14 weeks of intervention, and resulted in the use of consistent, functional language in authentic conversational contexts. In addition, Daniel's mother reported that she noticed differences in the sentences he used at home. She said that instead of using one or two words to communicate his wants and needs to his family, he started to combine three- and four-word phrases to communicate and to initiate conversation more frequently.
The final research question asked whether the personal narrative intervention was associated with increases in language diversity (lexical diversity). Recall that anguage diversity was measured by tracking the verbs used in each utterance as well as the number of different words that Daniel used in his utterances. On average during baseline, Daniel was observed to omit verbs from his utterances in most cases. In fact, any of his utterances consisted of single words that were usually nouns. Shortly after beginning intervention, Daniel was observed to begin to use verbs at the rate of at least one per utterance. This improvement was associated with an increase in the number of different words Daniel used in his utterances as well . Recall that during baseline, Daniel produced only 18 different words to describe his experiences with the clinician in the clinic. For example, he frequently used simple noninformative words repeatedly (e.g., use of ‘and’) in his utterances. After intervention, Daniel began to incorporate vocabulary related to the specific activities he was completing. Anecdotally, his mother reported that he was using more complete sentences (i.e., subject + verb + object) in interactions at home andshe was better able to understand what he was trying to communicate than before his participation in the intervention.
Clinical implications
Children with DS often demonstrate strength in social skills. Their social cognitive abilities impact the development of socially competent behavior – specifically related to discourse-level language proficiency. Individuals with DS often “seek out” more social experiences as compared to other individuals with intellectual deficits (Fidler & Nadel, 2007; Jahromi et al., 2008). One way clinicians and families can support their children's desire to interact socially is to address areas of deficit within meaningful communicative contexts that require discourse-level language abilities (Hofmann & Muller, 2021). It is important to improve personal narrative proficiency for students with DS because these interactions are critical for successful communicative exchanges between the student and their parents, friends, and acquaintances (Brinton & Fujiki, 2017).
This study provided preliminary evidence of a personal narrative intervention that may be effective for children diagnosed with DS. The approach to intervention could easily be adapted for use within school therapy sessions. The manualized procedures provide the structure needed to address language goals based upon the individual's strengths and needs. Though the intervention is manualized, it allows clinicians to make decisions about the degree of verbal and visual prompting that is needed for each individual client. This allows clinicians to follow manualized steps within an intervention without ignoring their clinical expertise. In addition, this intervention provides the neurocognitive support necessary for children with DS to successfully learn and maintain language skills.
Although the overall procedures seemed effective for improving the language of this child with DS, we recommend that clinicians consider the frequency as well as the length of the intervention this child received during the study. It may be necessary for the clinician to hold shorter, more frequent intervention sessions in order to adapt to school environments and to secure a change in some features of narrative language.
Limitations and future directions
Methodological limitations must be taken into consideration. The small sample size of one participant raises concerns regarding the presence of confounding variables. These factors are mitigated by the use of a control variable not addressed within the intervention. However, it may have been beneficial to collect more information on the current and past treatment the participant was receiving in order to provide a clearer picture of the effects of the narrative intervention used. An additional limitation of this study is that no post-intervention probes were administered to determine whether gains were maintained after treatment. Follow up measures may be used in future studies to document the long-term impact of the intervention.
Finally, In addition, following single-subject research guidelines, it is important to demonstrate three separate responses to intervention in order to control for internal threats to validity. Though the experimental design aimed to address control of these variables (i.e., maturation, history, etc.), the causality cannot be concluded from this study alone. It is necessary to utilize this intervention with more participants in order to make any conclusive remarks regarding the effectiveness of this intervention. Threats to external validity include individual traits (i.e., the individual studied may be atypical as compared to the larger population of individuals with DS), lack of ethnic and socioeconomic diversity, etc. The results from this case study may not be generalizable to other children with DS.
Results from this preliminary study indicate that further investigation is warranted with single-subject designs to investigate the procedures with a larger sample size. Children with DS are diverse and present with various combinations of ability levels and characteristics that may respond differently to aspects of the intervention. This approach could potentially be used as an introduction to other discourse types like fictional story generation. Fictional stories are used very often within academic tasks to teach different concepts. Extension of the knowledge gained in this intervention to fictional narratives may promote generalization and maintenance of the skills gained. Further research is necessary to explore the feasibility of this transition from personal to fictional narrative use.
Conclusions
Many previous studies of language intervention for individuals with DS have found that using decontextualized instruction can be effective in increasing abilities in various aspects of language. However, poor generalization of skills taught in decontextualized contexts is often observed (Burgoyne et al., 2012). In addition, these interventions are often employed in contexts that do not involve authentic conversational contexts. For example, massed practice on a particular skill (e.g., the use of past tense verbs in sentences) in a limited context (e.g., after being presented with models and picture prompts) is not an uncommon condition under which to teach isolated language skills (Gillam & Gillam, 2014; Kamhi, 2014). Producing a sentence that contains a past tense verb in response to seeing a picture is not an authentic, communicative task. In theory, the clinician would incorporate additional activities to help the student learn to use the target, in this case past tense verbs, in sentences used to communicate with others. However, there is limited evidence that children with DS or other intellectual disabilities profit from decontextualized approaches such as this over the long term (Miller et al., 1999).
The intervention in this study was designed to incorporate receptive and expressive knowledge of grammar, syntax, and vocabulary in discourse-level contexts that emerged from in experientially based activities. Key features of the intervention addressed memory, unification, and control components in order to establish the supports Daniel needed to expand his language abilities in authentic activities (van der Schuit, Segers, van Balkom, & Verhoeven, 2011). These features have been shown to provide the scaffolding children with DS may need to address deficits in cognition, including attention, organization, memory, and recall (Chapman & Hesketh, 2001; Jarrold & Baddeley, 2001; Patterson et al., 2013; Silverman, 2007). Multi-modal forms of support (i.e., verbal cues, use of icons, and graphic organizers) were used in experientially based activities to help Daniel recognize, identify, and recall important aspects of the activities he and the clinician participated in. Experientially based activities were repeated multiple times in order to allow him to practice new language skills in functionally appropriate contexts.
Each of the intervention sessions employed five different activities (i.e., 1) personal narrative performance tracking, 2) introduction of the experiential activity for that day, 3) participation in the experiential activity, 4) rehearsal time, and 5) curtain time) that allowed the participant to have multiple exposures to different vocabulary words, language facilitation techniques, and prompts that helped them be successful in using verbal rehearsal to practice the recount of the activities they performed. The combination of these strategies was determined to be effective for the child that participated in this intervention.
The current intervention was designed using the work of Finestack et al. (2017) as a guide. Remember that their intervention targeted three grammatical (microstructure) goals (elaborated noun phrases, advanced verb phrases conjunctions) and three discourse-level goals (macrostructure) focused on improving abilities in producing personal narratives (the use of character, setting, actions, dialogue, mental states). Eighteen scripted accounts of possible personal events were created and one was used in each of their sessions to model the use of targeted grammatical and story structure elements. The clinicians introduced and explained weekly goals and presented a picture representing the modeled personal narrative on an iPhone or iTouch, which served as a visual cue to support recall of the story. In addition, narrative maps were introduced at different points for each of their participants when it became evident that this support was necessary. The results from this study demonstrated the importance of providing children with DS with repeated exposure to narrative targets and the use of visual supports.
This current intervention differed from the narrative intervention developed by Finestack et al. (2017) for children with DS because of the focus on (a) using experientially based activities within the session to unify and teach story grammar as well as grammatical elements, and (b) use of multi-modal forms of support to address specific deficits in attention, organization, memory, and recall. The personal narrative events that the child was asked to portray were completed during the session. This allowed the clinician to provide the participant with reminders of the aspects of the activity they would need to recall later (e.g., characters, setting, etc.) and use visual supports throughout the activity to help with attention and memory. In addition, the visual supports (i.e., icons) that were provided during the session were also included in the graphic organizer the participant used during the ‘rehearsal time’ and ‘curtain time’ aspects of the intervention session. A script was used during each session with only the content of the story grammar elements varying across the experiential play activities. This paired with verbal rehearsal for the child seemed to increase his ability to retain information about specific story grammar elements and increase his ability to recall these elements when rehearsing and telling his story.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix A. Story Grammar Icons
Appendix B. Graphic Organizer
Appendix C. Story Script
_______ and So we got our supplies [Supplies] and went into the ________ [Setting] to play ______ [Initiating Event]. So that's what we did. We played _________ [Action]. And ___________ won [Landing].
Appendix D. Example Stories Baseline and Intervention
Baseline Story Example 1.
E What did you just do? E Tell me what you just did. C Basketball. E Basketball? E Tell me what you just did. C Soccer. E {Gasp} what else? C That/'s all. C Really that/'s all. C {Laughs} I won. C Get picture. C (Uh a*) Sarah and Gabe. C There it go/3 s. C And a X we have a ball and (g*) golf club. C And we have (gwa* golf c*) golf hole. C And they gives two X (with with) with the floor. C And (we play) we play (on the) with (our couch) our couch X. C And there it go/3 s again. C And we play the (uh uh) a golf hole and give a ball. C And we have a golf (uh) club. C That/'s our ball and that/'s our win/ing golf hole. C That/'s our (h*) hit/ing it (th*) the ball in. C (A*) and we have a golf club and we golfs too. C Characters. C Sarah and I. C Supplies it's a golf hole a golf ball a golf (uh) club golf flag. C What/'s that? E Setting. C Oh. C Setting. C Setting our playhouse. C (We wa* we) we want to play playroom. C We hit the ball. E Nice. C And we hit a ball. E Tell me what you and Miss Sarah did. C We play mini_golf. C No no. C We play/ed (uh hmm) I play (uh) I play (uh) pin/s bowling ball bowling! C And I win got two. C Sarah got one. C And bowling pin/s. C And (we) we play/ed. C Supplies a bowling_ball bowling_pin/s. C Characters Sarah and Gabe. C (And I) We play/ed in the playroom. C And our take_off (we we) we roll it. C And our action we hit the ball. E Is that all? C Yeah. E Tell me your story. C (Hailey) Sarah and I we want to play
basketball. C (Uh) We want to play basketball. C (We) we need/ed a basketball basketball
hoop. C (H*) our setting (we) we go (um) playroom. C (Um uh) we play ball. C I won! E Tell me about what you just did. C (Terry) Tara and I we want/ed to play bowling. C We pick a ball. C Supplies we need/ed a bowling_pin/s and bowling. C (We play we play) we play playroom. C Our action we threw the ball. C No no. C (We) put my hand/s and roll it. C And I won eighty and zero.
Baseline Story Example 2.
Intervention Example 1.
Intervention Example 2.
Intervention Example 3.
Intervention Example 4.
Intervention Example 5.