
Abstract
Background & Aims
Poor sleep in young children imperils language learning and use. Both sleep and language problems are prevalent in early childhood. Speech-language pathologists are in a unique position to expand surveillance of sleep problems, which in turn may contribute to communication difficulties. We conducted a feasibility study of speech-language pathologist screening for behavioral sleep problems and sleep-disordered breathing symptoms at a multidisciplinary evaluation and treatment center.
Methods
Speech-language pathologists administered screeners to parents of 2–6-year-olds: the Short Form-Children's Sleep Habits Questionnaire (for behavioral sleep problems) which includes an item asking if the child has a sleep problem (yes/no), and the pediatric sleep questionnaire (for sleep-disordered breathing). Speech-language pathologists participated in pre- and post-screening focus groups. Pre-screening topics included professional preparation and clinical experience regarding pediatric sleep issues. Post-screening, speech-language pathologists provided feedback about the screening experience and feasibility of incorporating such screening into practice.
Results
Among 51 children, 31% (16/51) screened positive for sleep-disordered breathing, 78% for behavioral sleep problems (40/51), and 43% (12/28) per parent report. Parent-reported problems were associated with sleep-disordered breathing (p = 0.00) but not behavioral sleep problems (p = 0.24). During focus groups, speech-language pathologists reported no formal pediatric sleep training, high parent concern about sleep, and agreed that screening fit their professional mandate. Speech-language pathologists affirmed that the ≤15 min screenings integrated seamlessly into practice but that additional training, particularly for sleep-disordered breathing, was needed.
Conclusions
The prevalence of sleep problems in 2–6-year-olds presenting to speech-language pathologists was higher than in community samples, but consistent with data from young children with developmental disabilities. Speech-language pathologists endorsed the utility and feasibility of sleep problem screening and education in their clinical practice.
Implications
Integrating sleep problem screening and education into speech-language pathologist practice is feasible and could widen surveillance of both sleep problems and risk factors for developmental language disorders. Further research should include larger samples and other settings, e.g. home or school.
Keywords
Introduction
Sleep impacts myriad aspects of child development, including brain maturation, learning and memory, emotional regulation and weight (El-Sheikh & Sadeh, 2015). Conversely, sleep problems can contribute to and are co-morbid with developmental disorders (Beebe, 2016), including speech-language disorders. Early childhood is a peak time for both sleep (Moore & Bonuck, 2013; Williamson et al., 2019) and language problems (National Academies of Sciences, Engineering, and Medicine, 2016). Common sleep problems—short sleep duration, behavioral sleep problems (BSPs) and sleep-disordered breathing (SDB) impair social–emotional and cognitive function and increase obesity risk (Spruyt, 2018), beginning in preschool (Reynaud et al., 2018). New guidelines recommend 11–14 h of sleep for toddlers (ages 1–2 years) and 10–13 h for preschoolers (ages 3–5 years) over a 24 h period (i.e. including naps) (Paruthi et al., 2016). Yet, 20% of 2–5-year-olds in the only such national poll fell below this minimum (National Sleep Foundation, 2004); recent international data affirms this sleep deficit (Galland et al., 2018). BSPs refer to problems falling or staying asleep, e.g. bedtime resistance, trouble falling asleep without a parent, or night-waking (American Academy of Sleep Medicine, 2014). BSPs occur in ∼20% to ∼25% of toddlers and preschoolers (Moore & Bonuck, 2013). SDB ranges from snoring to obstructive sleep apnea (OSA) causing partial or complete cessation of breathing during sleep, which affects brain oxygenation, structure, and function (Walter & Horne, 2018). Peak ages for SDB are 2–8 years often due to adenotonsillar hypertrophy relative to airway size (Marcus et al., 2012), with the prevalence of 1% for OSA and 20% for parent report of habitual snoring (Bonuck et al., 2011a, 2011b). Despite differing etiologies, short sleep duration, BSPs, and SDB have comparable adverse effects on the developing child (Jan et al., 2010; Spruyt, 2018).
Sleep quality and duration are a risk for various domains of language learning and use (McGregor & Alper, 2015). Speech perception in young children is negatively affected by 1 h of experimentally induced sleep restriction (Molfese et al., 2013). Lower verbal working memory scores are seen among first graders with insufficient sleep and irregular bedtimes (American Academy of Sleep Medicine, 2014; Cho et al., 2015). Nighttime sleep duration is especially impactful—explaining 27% of the variance in language outcomes by 2 years of age in a cohort followed from birth (Smithson et al., 2018). Persistent short sleep from early to mid-childhood increases the odds of poor receptive vocabulary (OR = 2.67, 95% CI = 1.24–5.74) (Seegers et al., 2016). Among 8–9-year-olds tracked for 3 years, increasing sleepiness was associated with less growth in verbal comprehension (Bub et al., 2011). A recent meta-analysis found sleep duration in children to be significantly associated with cognition overall (r = .06), with even greater effects for full/verbal intelligent quotient score (r = .15) (Short et al., 2018). Thus, a diverse body of research supports links between sleep problems and language function in children.
SDB affects speech-language in multiple ways. Even mild SDB during early childhood affects electrical brain activity related to speech perception (Key et al., 2009). SDB is linked to lower measures of receptive language (Kurnatowski et al., 2006) and impaired language processing in preschoolers (Honaker et al., 2009). OSA is also associated with poorer oral, expressive, and receptive language particularly before school age (Correa et al., 2017). Adenotonsillar hypertrophy, which is a primary cause of pediatric SDB, can result in reduced oral motor functioning and subsequently lead to articulation difficulties (Lundeborg et al., 2009). SDB can result in the physical alternation of oral motor mechanisms (i.e. open mouth posture and anterior tongue placement compensatory to airway obstruction), which adversely affects articulatory placement for speech sounds. Functional impacts can be profound. A 2015 meta-analysis found that SDB was linked to a 12.3% decrement in language arts proficiency, with authors positing that deficits were most likely mediated through domains of executive function and/or language skills (Galland et al., 2015).
Language disorders and sleep problems in young children both manifest in poorer behavior and social–emotional competence. Short sleep duration from 0 to 4 years is associated with poorer emotional regulation according to a recent meta-analysis (Chaput et al., 2017). Children with language disorders have higher rates of behavioral problems than their typically developing (TD) peers (Curtis et al., 2018). The toddler and preschool years are a time of burgeoning language and emotional regulation development. Expressive language delays, in particular, are linked to social–emotional deficits (Horwitz et al., 2003; Tervo, 2007). Recent research finds that language ability in early childhood is bi-directionally associated with behavior (Girard et al., 2016) and emotional regulation (Williams et al., 2017).
The prevalence of sleep problems among children with attention deficit hyperactivity disorder (ADHD; Tsai et al., 2016), autism spectrum disorder (ASD) (Elrod & Hood, 2015) and related neurodevelopmental disorders (Angriman et al., 2015) ranges from 35% to 80%. Among preschoolers with developmental delays/disorders, the rate of BSPs is more than twice that of TD children (Reynolds et al., 2019). Among preschoolers undergoing tonsil and adenoid surgery for SDB, 27.5% screened positive for developmental delay pre-surgery; 6 months post-surgery developmental scores increased significantly (Goldstein et al., 2016). The childhood adenotonsillectomy trial (CHAT) of the effectiveness of adenotonsillectomy versus watchful waiting in 5–9-year-olds with OSA, found significantly improved caregiver reported behavior and quality of life at 7-month follow-up, but no significant impact on neurocognitive performance (Marcus et al., 2013). However, CHAT excluded children with neurological or psychiatric conditions affecting cognition or behavior. Thus, children who may have experienced adverse neurocognitive effects from untreated SDB in their first 5 years of life were excluded from CHAT. Among children with Down syndrome, ∼70% have SDB (Lee et al., 2018). Young children with Down syndrome and poor sleep show specific difficulties with expressive language (Edgin et al., 2015).
Approximately 11% of young children (aged 3–6 years) have a communication disorder; two-thirds of such disorders are for speech or language problems (Black et al., 2015). Thus, speech-language pathologists (SLPs) are likely the most common health professional seen by young children in the general population. As described above, the functional effects of poor sleep and many developmental disabilities (DDs) coincide with SLPs scope of practice: speech sounds production (e.g. articulation), communication (receptive and expressive), pragmatics (social aspects of communication and language use) and literacy (reading, writing, and spelling). In terms of SDB, SLPs are trained to assess craniofacial factors affecting speech. Notably, SLPs affirm their role in screening, diagnosing, and enhancing social communication among persons with ASD (American Speech-Language-Hearing Association, 2006). Yet, the discipline's curriculum does not typically include training about how sleep problems may interfere with speech-language development, or how to detect them (Margaret Rogers, personal communication, August 10, 2015).
Pediatric primary care providers rarely screen for sleep problems and often lack sufficient training to treat them (Honaker & Meltzer, 2016). Not surprisingly, parents may perceive limited utility to seeking help from health professionals (Cook et al., 2020) or in the case of a DD with a language component (e.g. autism) attribute the sleep problem to the DD itself (McLay et al., 2020). Thus, SLPs are in a unique position to expand surveillance of sleep problems in young children—problems which themselves may increase risk for communication difficulties (Archambault, 2018). This is especially true for the majority of young children who receive SLP services in the absence of diagnosed conditions that are highly co-morbid with sleep problems (e.g. autism and ADHD). Yet, to our knowledge, no research exists on screening for sleep problems by SLPs.
We conducted a mixed-methods study of SLP screening of a heterogeneous sample of 2–6-year-olds. The aims of this pilot study were to (1) explore the feasibility of SLPs’ integrating sleep problem screening into practice and (2) identify the prevalence of BSP and SDB symptom prevalence. The study employed SLP focus groups pre- and post-screening (aim 1) and validated tools to screen for BSPs and SDB (aim 2).
Materials and methods
Setting and recruitment
Setting: This study took place at a multidisciplinary evaluation and treatment center which serves individuals with physical, developmental, language, and learning disabilities from birth through adulthood. Children are first seen by a developmental–behavioral pediatrician, social worker, or psychologist for an initial clinical evaluation (ICE) to elicit a developmental history and parent concerns, from which clinical impressions and recommendations are made. After the ICE, ∼80% of children are referred for evaluation/treatment by an SLP due to a communication delay/disorder concomitant to another DD or physical condition, or as their primary complaint. The diagnostic profile of 2–6-year-olds seen by the SLP team is ASD (∼25%), global developmental delay/intellectual disability (∼15%), congenital syndrome (∼5%), motor impairment (5%), and primary language impairment (∼50%). Many also have co-morbid ADHD.
Recruitment: Families were enrolled by the SLP team during routine evaluation or treatment visits from October 2017 through December 2018. During enrollment, five to eight SLPs, of whom one to two were bilingual, recruited, and consented families. Eligibility criteria were: (a) age: child aged 2.0–6.11 years and (b) language: parents and children whose primary language for communication is English or Spanish. Parents were consented in English or Spanish. Two years was set as the minimum age because it aligns with the ages in which the study's sleep problems screeners (see below) were validated. Six years was set as the maximum, given a focus on early surveillance of sleep problems.
Procedures and measures
Clinical and language concerns: We obtained clinical and language data for enrolled families using the ICE (see above) form at intake, yielding clinical impressions and recommended testing. The ICE was supplemented by additional demographic and service use (such as early intervention) items. In addition, SLPs indicated the child's primary speech-language concerns as comprehension, morphosyntactic, pragmatic, semantic and/or speech-articulation.
Sleep problem screening: SLPs obtained the following sleep measures from eligible parents during routine evaluation or treatment sessions. Among the 51 participants in the study, three were administered sleep measures and other study materials in Spanish.
Short Form-Children's Sleep Habits Questionnaire (SF-CSHQ)–SLPs administered the SF-CSHQ as a screener for BSPs. The original CSHQ is a widely used multi-dimensional pediatric sleep questionnaire (PSQ), originally validated in 4–12-year-olds, with the internal consistency of 0.68–0.78 in community and clinical samples, respectively, and test–retest reliability of 0.62–0.79 (Owens et al., 2000). Subsequently, the CSHQ was deemed clinically useful in 2–5-year-olds with and without DDs (Goodlin-Jones et al., 2008). The 23-item SF-CSHQ retains the original CSHQ's behaviorally based items that are responsive to behavioral management but omits parasomnia (e.g. night terrors) and SDB items that are not. The SF-CSHQ cut-off of ≥30 is correlated (0.90–0.94) with the original CSHQ (Bonuck et al., 2017).
PSQ–SLPs administered the PSQ to screen for SDB. The PSQ was validated in 54 children aged 2–18 years with nocturnal polysomnography (PSG) confirmed SDB versus 108 (non-PSG) general pediatric patients. The PSQ's 22 items factor into three subscales: snoring, sleepiness, and behavior given a 0.33 cut-off (i.e. ≥8/22 positive items), with no age interactions (Chervin et al., 2000). The PSQ is rated as the most valid questionnaire-based assessment of pediatric SDB (De Luca Canto et al., 2014) with a sensitivity of 0.85 and a specificity of 0.87 (Chervin et al., 2000).
Global measures—parent-reported single-item measures are significantly associated with sleep problems, sleep logs, the CSHQ (Lycett et al., 2015) and may be more highly correlated with children's mood and functioning than objective sleep measures (e.g. actigraphy) (Anders et al., 2012). We asked three global items of a subset of the sample: whether the child currently has a sleep problem (yes/no/maybe); if “yes,” whether the sleep problem is mild, moderate, or severe, and; whether they had ever sought professional help for any concerns about their child's sleep (yes/no).
All parents received a sleep brochure in English or Spanish that explained: how much sleep children need and why, as well as sleep hygiene tips. The BSP and SDB screening data were entered into REDCap where they were scored by study staff, who informed the SLPs of the results. SLPs then provided parents of children screening (+) for SDB a brochure that explained the condition and its risks, and recommendations to have their child evaluated by their child's physician. The brochure includes a panel directed to the physician that explains the screening.
SLP focus groups: We obtained qualitative data from two focus groups with the SLP team, pre- and post-screening for sleep problems. The pre-screening group: (a) assessed prior education and training are: sleep problems in children, and (b) when and how sleep presents in clinical encounters. The post-screening group elicited: (a) feedback about the screening experience and (b) input about integrating sleep problem screening into SLP practice. In addition, SLPs completed brief surveys adapted from prior work (Bonuck et al., 2016, 2019). Survey items assessed SLPs’ training/job function, comfort levels, and practices with regard to sleep education and screening. Groups were audiotaped and transcribed.
Analysis
We present frequencies for demographic, clinical and language concerns, and the SLP survey data. We generated descriptive statistics for the SF-CSHQ and PSQ subscale, total and dichotomous (positive vs. negative screening) scores, i.e. ≥ 30 for the SF-CSHQ and ≥8 for the PSQ. Associations between dichotomous screening outcomes and demographic, clinical and language concerns were analyzed with chi-square or Fischer's exact tests. Analyses were repeated for the three global item measures as appropriate. Analyses were conducted in SAS. Focus group transcripts were uploaded into qualitative data analysis software (Dedoose 8.0.35, 2018, LA, California). Two authors (KB and KM) reviewed the transcripts, developed a code list, and coded the data.
The study had institutional review board approval. Parents completed written consents and the SLPs provided oral consent.
Results
Sample description (Table 1): The sample was comprised of n = 51 primarily English-dominant children (46/50; 92%), aged 2.0–6.8 years. Expressive/receptive language was the most prevalent communication concern (38/51; 75%) followed by unclear speech (28/51; 57%); pragmatics was the least common speech-language concern (18/51; 35%). Parents’ main behavioral concerns were over-activity (26/51; 51%) or inattentiveness (36/51; 71%), while the most common clinical impression apart from language issues were ASD (15/51; 29%).
Description of sample.

ASD: autism spectrum disorder; ADHD: attention deficit hyperactivity disorder.
Sleep problem scores and clinical characteristics (Table 2): The prevalence of SDB was 31% (16/51) as per the PSQ, while that of BSPs was 78% (40/51) as per the SF-CSHQ. We obtained global measures’ data from n = 28 parents, including for the question “Does your child have a sleep problem?” We consolidated “Maybe (n = 2)” and “Yes (n = 10)” responses to this question based on qualitative comments shown in Table 2, yielding 43% (12/28) of parents reporting that their child had a sleep problem. Among these 12 parents: eight described the problem as moderate or severe and eight had sought professional help for it (not shown). None of the sleep problem outcomes were associated with clinical characteristics, except for “Moody” behavior and scoring positive on the PSQ.
Sleep problem outcomes by clinical characteristics.
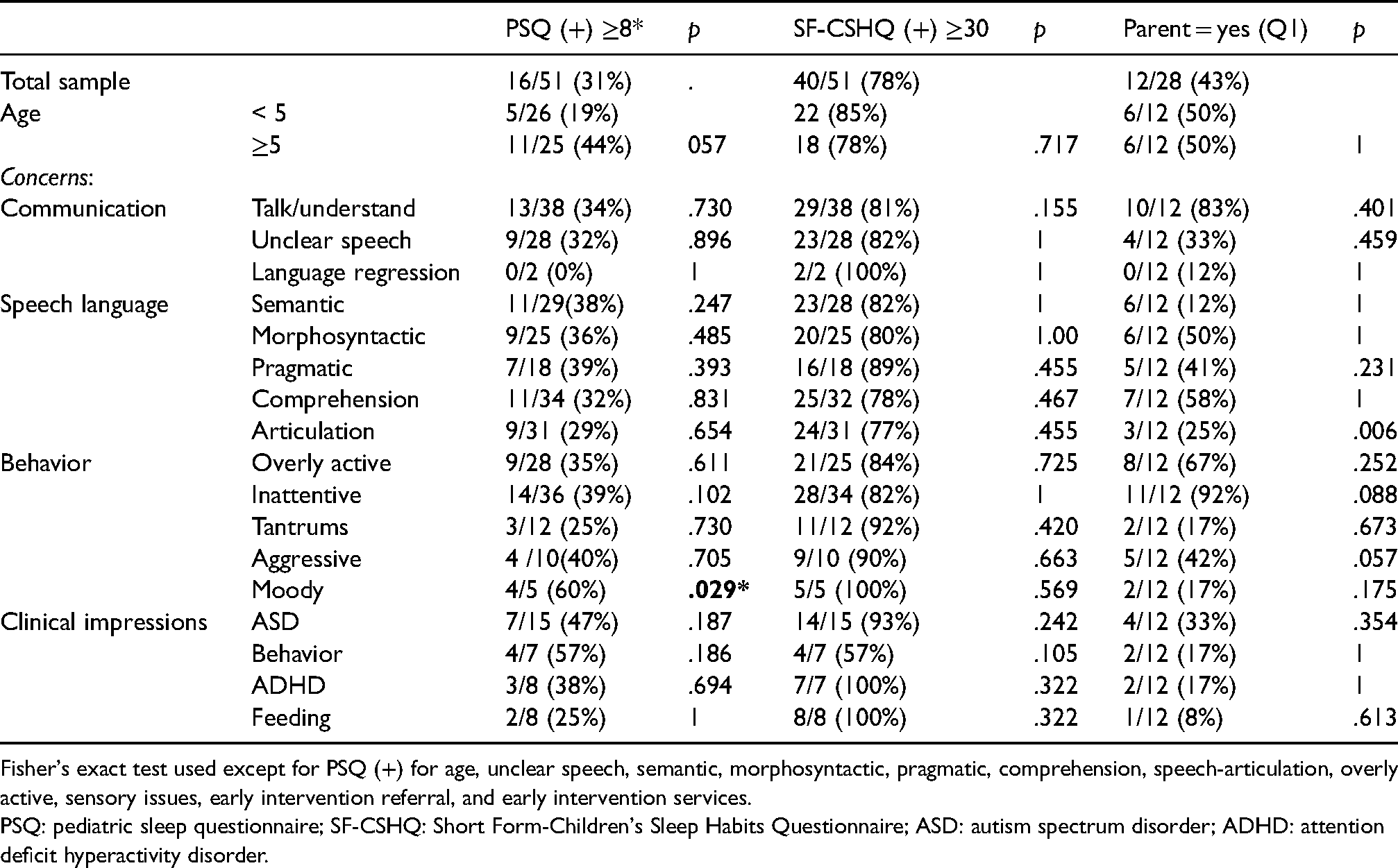
Fisher's exact test used except for PSQ (+) for age, unclear speech, semantic, morphosyntactic, pragmatic, comprehension, speech-articulation, overly active, sensory issues, early intervention referral, and early intervention services.
PSQ: pediatric sleep questionnaire; SF-CSHQ: Short Form-Children's Sleep Habits Questionnaire; ASD: autism spectrum disorder; ADHD: attention deficit hyperactivity disorder.
Qualitative comments by sleep problem outcomes (Table 3): Quite a few parents included (optional) comments with the global measures. Collectively, their comments bespeak keen awareness of their child's sleep problems (both SDB and BSP), high engagement with health professionals to resolve them, and concordance with screener outcomes. Notably, all parents responding “Yes” are: their child having a sleep problem had at least one positive screener score. Parent report of a child sleep problem was associated with PSQ outcomes for SDB (p ≤ 0.01), but not with SF-CSHQ outcomes for BSPs (p > 0.05).
Sleep problem outcomes by global measures.

PSQ: pediatric sleep questionnaire; SF-CSHQ: Short Form-Children's Sleep Habits Questionnaire; ASD: autism spectrum disorder; ADHD: attention deficit hyperactivity disorder.
Focus group surveys (Table 4): Pre- and post-screening surveys were completed by eight and six SLPs, respectively. Half the team remained constant across both surveys (the unit's composition shifted with staff changes). Despite near-universal agreement that screening for sleep problems in young children was within their scope of work (pre = 5/7; post = 6/7), none recalled this content from their training. All but one SLP was at least somewhat comfortable explaining how sleep quality/quantity affects communication and providing basic hygiene tips. Notably, during the pre-screening group, just half (4/8) were comfortable explaining how SDB affects language function. SLPs were slightly more likely to ask parents about sleep patterns (pre = 5/7; post = 3/6) and their child's nighttime breathing (pre = 3/7; post = 4/6), and least likely to refer a child for SDB (pre = 2/7; post = 2/6).
SLP pre-/post-screening surveys at focus groups.

SLP: speech-language pathologist; SDB: sleep-disordered breathing.
Qualitative analysis of focus group data: Four themes, described below, emerged from the focus group data: (1) SLP training and perception of pediatric sleep problems, (2) presentations in practice, (3) SLP views of implementing sleep guidance/screening, and (4) logistics of screening. Within quotes, bracketed grammar has been added for context.
SLP training and perception of pediatric sleep problems. No SLPs remembered “[anything] major related to sleep” in their training. One recalled “hearing about sleep and memory consolidation in adult neurology class,” while training on sleep apnea was limited to specific diagnoses, e.g. voice disorders or dysphagia, or a bedside questionnaire for adult patients. The few references to pediatric sleep recalled from training included, e.g. “you know, kids need their sleep.” Despite this lack of formal training, when asked to describe what might constitute a pediatric sleep problem, the SLPs accurately replied: “waking frequently in the night; can't fall asleep; apnoea; night terrors or night-waking; sleepwalking. [pre-screening group].” When asked how to increase the profession's knowledge about the links between sleep problems and speech-language, an SLP suggested “…if there was a stronger connection made then people would pay attention…there is very little evidence now.”
Presentations in practice. Both parents and SLPs raise sleep issues. One SLP noted, “…[that there was] fair discussion during evals that the kids will only sleep in the bed with them.” Another remarked that children sometimes come in “half asleep,” potentially impeding planned testing or treatment. An SLP might inquire how a child slept if she observed behavior out of the norm for that child. In response, “things would come up…like a shift in family structure…[or a child who] was hearing rats in the wall at night.” Presentation varied by age and diagnosis. “The younger the kids, the more often it [sleep] comes up.” With an older child who was tired, an SLP said she would “usually drop it if they are talking about a lot of typical teen stuff.” Regarding diagnoses, SLPs agreed that “[with] kids that are on the spectrum, it will come up.” In addition, an SLP might ask about sleep in children with feeding difficulties (given links between SDB and enlarged tonsils and adenoids) or who present as hyperactive (given links between ADHD and disrupted sleep patterns).
SLP views of implementing sleep guidance/screening. SLPs endorsed the idea of providing sleep education and screening: “I think it would be a good thing. I would consider it part of my profession (pre-screening).” Post-screening comments affirmed this view: The SLPs agreed that “there were a lot of kids with sleep problems.” They noted the impact of sleep for academics and feeding issues: “If these kids aren't sleeping, then who feels like sitting, learning, concentrating…same thing with the feeding group…if they aren't sleeping well…I’d rather sleep than eat.” The rapport built over weekly sessions would facilitate a role for SLPs in sleep education and screening: “…they’re [the SLPs] the people the parents trust…[they tell us things] they wouldn't have told their case manager.”
Logistics of screening. During the post-screening group, SLPs commented that the two screeners took about 10–15 min altogether to administer, depending upon the parent's literacy level. For parents, there was the sense that “asking about sleep was kind of routine for a doctor's appointment…they don't see a differentiation between us and the doctors.” Although there was some anxiety about the results and potential follow-up. To address this, SLPs agreed that it would have been preferable to score the screeners on the spot versus waiting for the research team to provide results. The SLPs suggested expanding the age range to school-aged children and ensuring that SLPs have “the right training and knowing who to refer to.”
Discussion
Principal findings
Sleep is a key foundation of healthy development. Sleep problems contribute to and co-occur with myriad developmental disorders including speech and language disorders (Jan et al., 2008). To assess the feasibility of SLP screening for sleep problems in young children we conducted a mixed-methods study at a multidisciplinary center for DDs. In focus groups, SLPs reported that despite a dearth of graduate curricula about pediatric sleep, parents often raised this topic with them, and that sleep education and screening fit within their scope of work. They were more confident in their knowledge of how sleep duration and quality affects language function as compared with effects for SDB. The prevalence of sleep problems identified by brief screening tools exceeded that of community samples (see below): 78% for BSPs and 30% for SDB. In addition, ∼40% of parents queried, responded “yes” when asked if their child had a sleep problem. Furthermore, half these parents commented about their child being diagnosed or treated for a sleep problem: melatonin (medication to promote sleepiness), overnight sleep study, adenoid removal, etc. Taken together, findings affirm the feasibility and utility of SLPs providing sleep education and screening with families of young children.
Comparison with other studies
The prevalence of sleep problems in our study—both BSP and SDB—while higher than community samples, aligns with findings in young children with developmental disorders. For example, community sample estimates of BSP prevalence are ∼20% to ∼25% at these ages (Moore & Bonuck, 2013; Morgenthaler et al., 2006; Owens & Mindell, 2011) but among preschoolers with ASD it was 78% (Reynolds et al., 2019). In this latter study, 61% of TD preschoolers and 67% of those with a developmental delay/disability (DD) other than autism also screened positive. Concerned that the CSHQ would over identify BSPs, researchers also reported prevalence using a higher cut-off corresponding to 25% of TD children. This conservative threshold yielded a lower rate of BSPs among children with ASD (47%), with DD + ASD (57%), and with DD w/o ASD (29%), compared to those who are TD (25%) (Reynolds et al., 2019). As we used a short form version of the CSHQ that excluded the parasomnia and SDB scales (in part because they were less cohesive than others) (Bonuck et al., 2017) the extent to which the SF-CSHQ over-identified children in our sample is unknown. Further use of the SF-CSHQ in community and clinical samples is warranted.
Regarding SDB, 30% of our sample screened positive on the PSQ. This prevalence is higher than the general population based on parent-reported estimates of 1% for sleep apnea and 20% for habitual snoring (Bonuck et al., 2011a, 2011b) and the PSQ (Sanchez et al., 2019). Even among same-aged children attending well-child visits near our locale, just 9% screened positive on the PSQ (Goldstein et al., 2011). Similar to BSPs, recent studies have found twice the rate of SDB in children with ASD versus community samples (Elrod et al., 2016; Hirata et al., 2016). In the first study of nearly 50,000 children aged 2–18 years, 9.4% of those with ASD had an SDB diagnosis in their medical records (Elrod et al., 2016). In a sample more similar to ours—2–6-year-olds with questionnaire defined SDB—28% of children with ASD had SDB (n = 193) versus 15% in community controls (n = 965) (Hirata et al., 2016). Thus, SDB rates appear to be elevated among children with DDs even in the absence of predisposing physical syndromes, e.g. Down Syndrome.
Strengths and limitations
This study has several strengths. It is the first to our knowledge to involve SLPs in sleep problem screening and to do so in routine practice. Relatedly, because SLPs are a trusted source of support, families may be more receptive to referral for further assessment and intervention from them. Conversely, access to a multidisciplinary team allowed clinicians to easily refer patients to a medical professional for follow-up. The study's mixed-methods which allowed for multiple perspectives and provided useful context is an additional strength. Finally, recognizing the existence of health disparities with regard to both insufficient sleep (Pena et al., 2016) and SDB (Harris et al., 2018), our study was set within a lower-income, ethnically diverse community. The study also has several limitations. Its small convenience sample limits generalizability to other communities and patient populations. In addition, results may not reflect a willingness on the part of parents and SLPs in other settings (i.e. home, school) to participate in sleep assessment, when they may have less access to interdisciplinary involvement and medical follow-up. Thus, the selected nature of our sample may further limit generalizability. In addition, the screener we used to assess BSPs may over-identify children.
Conclusions
Mounting research finds that sleep problems in early childhood have strong, persistent effects on cognitive, social–emotional, physical function, as well as communication disorders. To be sure, the “attributable risk,” i.e. how much children's sleep problems affect their speech-language or other functioning is unknown but is unlikely to be zero. Yet, sleep problem screening rarely if ever occurs in pediatric primary care (Honaker & Meltzer, 2016), early intervention (Bonuck et al., 2011a, 2011b), or school settings. These gaps in screening are missed opportunities to implement behavioral interventions that do not require a sleep expert (Lord, 2019) but which improve sleep in typically (Meltzer & Mindell, 2014) and non-TD children (Jan et al., 2008; Malow et al., 2013; Vriend et al., 2011) as well as myriad treatments for sleep-disordered breathing (Kaditis et al., 2016).
Disciplines such as dentists, child care providers, and school personnel—but not SLPs—have been proposed a primary care provider “extenders” for sleep problem screening and intervention (Sevecke & Meadows, 2018). SLPs are well-positioned to incorporate sleep education and screening into regular practice; many works in educational settings or practices alongside occupational and physical therapists where they work with children. The profession would potentially need to support changes to graduate curricula, including mapping such revisions to evaluation, intervention or other standards. SLP screening of sleep problems could potentially widen surveillance for sleep problems, as well as risk factors for speech-language and other developmental disorders.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the following organizations: American Sleep Medicine Foundation (161-FP-17), Department of Health and Human Services-Administration on Intellectual and Developmental Disabilities (90DDUC0035), and National Institutes of Health (R01HD082129).