
Abstract
Background and aims
The daily challenges of caring for a child with autism spectrum disorder affect many areas of everyday life and parental well-being, as well as parents’ ability to manage the needs of the family and the child concerned. A better understanding of parents’ perception of their child’s characteristics can allow better support for them and individualize intervention protocols in a more accurate way. The main objective of this study is the evaluation of the perception of stress by parents of children with autism compared to parents of children with specific language impairment.
Methods
The parents of 87 children aged between 2 and 6 years were included in this study, 34 children with a specific language impairment diagnosis and 53 children with an autism spectrum disorder diagnosis (ASD) or at risk of developing it. They were asked to complete a self-report on perceived stress and rating scales on adaptive/problematic behaviours, executive functions and sensory profile of the child.
Results
The results reveal that parents of ASD children, compared to the control group, showed significantly higher levels of stress, mainly due to the difficulty of managing unexpected events, the feeling of loss of control over one's life and the fear of not being able to cope with the adversities they were experiences. The most critical area, both for ASD and control group, concern the executive function related to emotional reactions.
Conclusions
Thus, we argue that the difficulties in self-control, sensory modulation and emotional regulation, represent an element of stress for parents of children with developmental disorders.
Introduction
Children with autism spectrum disorder (ASD) usually have difficulty with social communication and interaction, restricted interests, and repetitive behaviours; often they also show impairment in understanding others' intentionality, in symbolic play and in imitation skills (Hyman et al., 2020). To support the development of these abilities, they are now introduced increasingly early into treatment paths that should be personalized, calibrated on the child's level of development and relevant to the objectives of the treatment; treatments are mostly intensive, some more closely centred on the child, others mostly emphasizing parental involvement (Granger et al., 2012; Lyra et al., 2017; Weitlauf et al., 2014; Zwaigenbaum et al., 2015).
In addition to the line of research on autism's core symptoms and treatments, over the years studies have investigated the impact that the characteristics of children with ASD have on parental figures. Some have found a higher incidence of psychopathological disorders in parents (Bonis, 2016), including depression, anxiety and stress-related symptoms, compared to parents of children with typical development (Ingersoll & Hambrick, 2011; Jones et al., 2013; Lau et al., 2014; Silva & Schalock, 2012; Zablotsky et al., 2013), with Down syndrome (Dabrowska & Pisula, 2010) or other disabilities (Hayes & Watson, 2013; Reed & Osborne, 2013; Zablotsky et al., 2013).
With reference to stress, different studies have shown higher levels of parental stress in families of children with ASD than in children with typical development or with other disabilities (Agazzi et al., 2017; Hayes & Watson, 2013; Lecavalier et al., 2006). Children with ASD exhibited more problematic behaviours than children without disabilities, and their parents showed higher levels of stress. However, stress seemed more related to the severity of problematic behaviour or conduct disorder than to the type of disability or severity of symptoms (Hill-Chapman et al., 2013; Rivard et al., 2014; Schieve et al., 2011). Such research shows that it is more difficult for parents to take care of their child than most children of the same age, even if they are less annoyed by the things their children do and get less angry with them.
Falk et al. (2014) also highlighted a significant relationship between a child’s aggressive behaviour and maternal depression, especially in parents with low social support; while the severity of the symptoms of autism seemed to correlate more with maternal anxiety, especially in younger mothers.
These results suggest that the relationship between ‘child-centred variables’ (externalizing behaviours and severity of autism symptoms) and parental psychopathological symptoms may be mediated by other variables, which need to be investigated. One of these variables is the executive functioning (planning, working memory, cognitive flexibility, response initiation and inhibition, impulse control and self-monitoring of tasks and actions) of ASD children (Hutchison et al., 2016), which seems to be the basis of the management difficulties that parents report, especially since executive dysfunction seems to be closely related to the severity of repetitive behaviours and restricted interests. Specifically, the areas of cognitive flexibility and the planning of actions during problem solving (Panerai et al., 2014) seem to be more compromised, aspects usually associated with reduced adaptability, in particular with socialization, and a lack of behavioural regulation capacity in everyday situations. These deficits, in the study of Panerai et al. (2014) are present in all ASD subgroups, both those with and without intellectual disability; for this reason, they are described by the authors as a typical feature of autistic disorders.
These authors have shifted the focus of their interest on adaptive functioning, noting significant deficiencies in all ASD children, identifying the presence of a deficit especially in the social sphere.
The results described so far support the need to consider the combination of the ‘objective’ severity of the autistic symptomatology and the ‘perception’ that the parent of the ASD child has of such severity, as this could favour a better personalization of the path of treatment, in which the parent is usually also involved. This co-participation is based on Vygotsky's (1934) concept of proximal development zone: an area of skills that is just beyond the child's current ability, but where the child can move through the involvement of a caregiver.
As reported by Hutchison et al. (2016), the child's experiences in the surrounding environment, including social and affective interactions, modify the child's behaviour and vice versa. These bidirectional influences, therefore, can determine changes over time both in the child's behaviour, in the parent's representations of the child and his or her disorder, and consequently in the child-parent interactions, triggering a virtuous circle.
The present study will therefore investigate the difficulties that preschool children with ASD could manifest in executive functioning in daily life, assessed indirectly through parenting reports, in adaptive behaviour, in the sensory profile and in the behavioural-relational profile, compared to children without ASD who have specific language disorders. The second objective will be to investigate the relationship between the level of stress perceived by the parents of ASD children, compared to the parents of children with speech disorders, and the characteristics of the child's neurodevelopment, in order to better understand how to better individualize the strategies of treatment that will be proposed to these children.
Method
Participants
The study included 87 children aged between 2 and 6 years of age. At intake, 34 children (39%) have a specific language impairment diagnosis (SLI); 20 children aged between 31 and 49 months of age (23%) have an autism spectrum disorder diagnosis; 33 children between 18 and 30 months of age (38%) have a classification of “at risk” of developing a spectrum disorder. This classification reflects the early diagnosis criteria of ADOS-2 and Diagnostic and Statistical Manual of Mental Disorders (DSM-5, APA_American Psychiatric Association, 2013). Children with SLI represented the Control group, children with ASD or at risk of ASD, represented the ASD group (see Table 1).
Characteristics of the sample.

Legend: SLI = Specific Language impairment.
The two groups differ in the age of first diagnosis (3.6 vs. 2.6 years old), but they do not differ in the average time spent in therapy at the time of recruitment in this research (14.7 vs. 16.5 months). 23.5% of the control group and 26.4% of the ASD group started a therapeutic path less than six months previously; 17.6% of the control group and 18.9% of the ASD group started 6–12 months previously; 41.2% of the control group and 30.2% of the ASD group started 12–23 months previously; 17.6% of the control group and 20.8% of the ASD group started 24–42 months previously. The two groups do not differ in terms of gender (percentage of males: 85.3% vs. 88.7%), nor by order of parentage or number of siblings. The general distribution of the ASD sample is in line with the most recent estimates indicating a prevalence of males in a 4: 1 ratio compared to females (ISS_ISTISAN Reports, 2013; Morbidity and Mortality Weekly Report, 2014).
Most children are first born and about 38% are an only child. Fewer than a third had complications during pregnancy (for example, placenta praevia, maternal hypertension, gestational diabetes), but they had no postnatal problems; the children of the two groups do not differ in birth weight. In 13% of the cases in the ASD group children have a twin and in 18% of cases familiarity is reported for spectrum disorders, that is a percentage significantly higher than that found in the control group (8.8%).
In terms of socio-economic status, the two groups do not differ either by country of origin (mostly Italian), or by parental marital status, in fact almost all of them have been married or cohabiting on average for eight-nine years; in both groups the majority (between 47% and 52%) of mothers have a secondary school diploma or a degree (between 30% and 44%); finally, about two thirds of mothers are in stable employment.
Procedures
Parents and children with certified diagnoses received by health services delivered by the National Health System through public hospitals, or private facilities under contract with the National Health System were recruited and included in this study. The data were collected in the 2018–2019 period.
The exclusion criteria were as follows: (a) neurological diseases or focal neurological signs; (b) severe sensory impairments (e.g., blindness and deafness); (c) history of severe perinatal asphyxia, head injury or epilepsy; (d) positivity to the examination of the high-resolution karyotype, DNA analysis for X-Fragile or positive screening tests for metabolic disorders.
Neurodevelopmental disorder diagnoses were based on DSM-5 criteria (APA_American Psychiatric Association, 2013) and prepared following clinical interviews, physical examinations and psychodiagnostic assessments, carried out by the multidisciplinary teams of the reference Centre.
Informed consent was obtained from all parents (Helsinki Declaration). This research respected the ethical guidelines and legal requirements of the country in which it was conducted. The research also met the ethical standards of the American Psychiatric Association (APA).
At the time of recruitment for this study, all the children were assessed in order to update an assessment of their autistic symptoms, psychomotor development, cognitive, linguistic and emotional functioning; their parents were given rating scales and questionnaires for assessing the adaptive skills, the executive functions, the sensory and behavioural/relational profile of the children, and for investigating parental stress.
Instruments
ADOS-2 – Autism Diagnostic Observation Schedule – Second Edition
The ADOS-2 (Lord et al., 2012) is a semi-structured, standardized assessment of communication, social interaction, play and restricted and repetitive behaviours which provides a series of activities designed to elicit behaviours directly related to the autism spectrum disorder diagnosis. The Toddler Module, for children between 12 and 30 months of age who do not consistently use phrase speech, provides ‘ranges of concern’ reflecting the extent to which a child demonstrates behaviours associated with ASD.
ABAS-II-Adaptive Behavior Assessment System – Second Edition
The ABAS-II (Harrison & Oakland, 2003) is a commonly used referenced tool designed to assess adaptive skills in individuals from birth to 89 years of age. The Parent Form used in this study measures nine adaptive skill areas (M = 10; SD = 3) covering three domains: Conceptual (CON: Communication + Functional Academics + Self‐Direction), Social (SOC: Leisure + Social), and Practical (PR: Community Use + Home Living + Health and Safety + Self‐Care). The ‘General Adaptive Composite’ (GAC) score that represents a commonly referenced score for the individual (M = 100; SD = 15) is also calculated from all nine skill areas.
BRIEF-P-Behavior Rating Inventory of Executive Functions-Preschool Version
The BRIEF-P (Gioia et al., 1996) is a standardized rating scale developed to provide an understanding of everyday behaviours associated with specific domains of executive functioning (EF) in children aged two to five years. The BRIEF-P consists of a single Rating Form, designed to be completed by parents, teachers, or other caregivers, with 63 items on a three-point rating, each one rated as ‘Never’, ‘Often’, ‘Never’, depending on how often they observe a specific behaviour, in five non-overlapping scales. The scales form a Global Executive Composite (GEC) and three overlapping summary indexes. The Inhibitory Self-Control Index (ISCI) is composed of the Inhibit and Emotional Control scales, the Flexibility Index (FI) is composed of the Shift and Emotional Control scales, and the Emergent Metacognition Index (EMI) is composed of the Working Memory and Plan/Organize scales.
SSP-Short Sensory Profile
The Short Sensory Profile (McIntosh et al., 1999) is a caregiver questionnaire which contains 38 items organized into seven subscales reflecting responsiveness to sensory input across sensory modalities including: tactile sensitivity, taste/smell sensitivity, movement sensitivity, under-responsivity/seeking sensation, auditory filtering, low energy/weakness and visual/auditory. Parents indicate their perception of the frequency with which their child exhibits atypical behaviour responses to sensory stimulation on a five-point Likert scale ranging from 1 (always) to 5 (never). Higher scores represent higher functional performances. The SSP total score and the score on each subscale can be used to classify children’s level of sensory abnormality: Typical, Probably Difference, or Definite Difference. The Sensory Profile was standardized on more than 1200 children; the short version derived from it has a reliability of .90 and a discriminating validity >95% in identifying children with and without atypical sensory processing patterns; it has an internal consistency of the factors within the scale ranging from .70 to .90.
ASDBI – ASD Behavior Inventory
The ASDBI (Cohen & Sudhalter, 2005) is a standardized rating scale designed for parents and teachers which allows one to make an assessment of relational behaviour and some other symptomatic aspects typical of children with ASD, referring to different life contexts. Through 188 items, it allows to evaluate the domain of contact/isolation problems (Sensory/Perceptual Approach Behaviours, Rituals/Resistance to Change, Social/Pragmatic Problems, Semantic/Pragmatic problems, Arousal problems, Fears, Aggressiveness) measuring the difference in the behaviour of typical children compared to what is usually observed in ASD children. The ASDBI was standardized on 369 parents and 277 teachers of children with ASD. The reliability for the parent sample ranged from .38 to .91. Clinical validity was assessed through comparison with the ADOS.
Perceived Stress Scale (PPS)
The PSS (Cohen et al., 1994; Mondo et al., 2019) is a 14-item self-report measure designed to assess the degree to which life situations are appraised as stressful. Specifically, items are designed to measure the extent to which one’s life is perceived as unpredictable, uncontrollable and overloading. The questions are general in nature and therefore exempt from specific content of any subpopulation and concern feelings and thoughts relating to the past month. Each item is rated on a five-point Likert scale ranging from 0 = Never to 4 = Very Often. The higher the score, the greater the overload stress, as well as the perceived discomfort. The validation sample consists of 2387 people over the age of 18, residing in the U.S.
Statistics
In order to evaluate the differences between groups, analyses of the unifactorial (ANOVA) and multivariate (MANOVA) variance were conducted. The effect size was calculated using the partial eta squared whereby η2 = 0.02 is considered a small effect, 0.13 a medium effect, and 0.23 a large effect (Pierce et al., 2004). In order to analyze the changes in the time of the measures based on categorical variables, an analysis of the Chi-square was carried out. To evaluate the correlations between the scores obtained in different measurements, correlational analyses were conducted. The level of significance was set at p < 0.05. All statistical analyses were performed using the software version 21.0 of SPSS.
Results
Descriptive statistics
The differences between groups compared to the ages (in months) of acquisition of the first stages of development were analyzed. No significant differences emerged between the control group and the ASD group with respect to the age of achievement of the control of sitting posture (5.7 ± 1.8 months vs. 6.0 ± 1.5 months; P = .38), of the movement on all fours (8.1 ± 1.9 months vs. 9.0 ± 2.1 months; P = .07), the first autonomous walking (13.9 ± 3.1 months vs. 14.2 ± 2.7 months; P = .60) and the appearance of the first words (i.e mum or dad) (13.3 ± 6.5 months vs. 16.1 ± 9.7 months; P = .16) . However, a significant difference emerged in relation to the appearance of the first sentences, which appeared later in the children of the ASD group (23.5 ± 8.0 months vs. 32.6 ± 9.7 months; F(1,85) = 13.09; P < .001; ƞ2 = .21). In addition, the parents of the control group declared that they started to recognize the existence of a problem in the development stages on average six months later than the parents of the ASD group (26.8 ± 6.9 months vs. 20.5 ± 6.1 months; F(1,85) = 18.97; P < .001; ƞ2 = .19).
Symptomatological characteristics of the children
Adaptive skills (ABAS-II)
Parents of children from both groups completed the ABAS-II rating scale for assessing the child's adaptive skills in the Conceptual (CON), Practical (PR) and Social (SO) domains. The scores of each scale are expressed in weighted points (mean 10 and sd 3), so the higher the score, the better the adaptive skills of the child. The children of the ASD group show significantly lower adaptive abilities than the children of the control group (Wilks’ Lambda = 5.48; p < .001) in all the areas assessed (see Table 2); the covariate ‘age of the child’ (P = .28), which was not significant, and the covariate ‘months of therapy’ (P < .05), which has a significant effect on the areas of the Practical domain were checked: as the months of therapy increase, the scores in the Home Living (F(1,85) = 7.695; P < .01), Health and Safety (F(1,85) = 4.774; P < .05) and Self Care (F(1,85) = 6.305; P < .05) improve.
Mean (sd) differences between groups on test scores.

Legend. ABAS-II = Adaptive behavior assessment system; BRIEF-P = Behavior Rating; Inventory of Executive Function; ASDBI = ASD Behavior Inventory.*P< .05; **P< .01.
Executive Functions (BRIEF-P)
The scale assesses the child's executive functioning in the daily context of home life. The scores of each scale are expressed in T points (mean 50 and sd 10), thus scores T > 65 indicate the presence of difficulties in executive functioning. The children of the ASD group show significantly more impaired inhibition, shift, working memory and planning abilities than children in the control group (Wilks’ Lambda = 0.85; p < .001) (see Table 2); however, there are no significant differences between the groups in the area of emotional regulation (F(1,85) = 2.348; P = .16); the covariates ‘age of the child’ (P = .15) and ‘months of therapy’ (P = .13) were not significant.
Sensory Profile (SSP)
The parents of the children of both groups completed the Sensory Profile Short Form rating scale which assesses the child's ability to modulate sensory inputs. The scores of each scale are expressed in raw points; a higher score corresponds to a more adequate ability of the child. The children of the ASD group show a significantly lower regulation of the sensory response than the children of the control group in three areas assessed (See Table 2): Tactile Sensitivity (F(1,85) = 5.203; P < .05), for which they express greater discomfort during moments of personal care or react excessively to physical contact; Hypo-Responsivity/Seeking Sensation (F(1,85) = 9.569; P < .01), for which they seek sensory stimulation, manipulate objects and things in a more stereotyped way; Auditory Filtering (F(1,85) = 9.893; P < .01), for which for example they are more bothered by background noises, such as fan, refrigerator, etc. or by sudden noises, in front of which they can show bizarre reactions. The covariate ‘age of the child’ (P = .08) and the covariate ‘months of therapy’ (P = .27) were checked, but were not significant.
Symptomatology in the relational area (ASDBI)
The scale assesses the presence of problematic contact/isolation behaviours, observed in the daily context by the parents of both groups. The scale scores are expressed either in T points (mean 50 and sd 10) or in percentile points, so T scores> 60 and percentile> 75 indicate the presence of severe difficulties. As can be seen in Table 2, the symptoms of the children of the ASD group are described as significantly more problematic than those manifested by the children of the control group in some areas: in fact, they show more symptoms in the area of sensory/perceptual approach behaviours (F(1,85) = 10.510; P < .01), such as, for example, staring at objects, pica, repetitive toy play. The children of the ASD group also show greater difficulties in reacting to environmental changes and in the manifestation of ritualism (F(1,85) = 5.087; P < .05). They also show greater pragmatic and social problems (F(1,85) = 10.960; P < .01), for example in the way of approaching other people, of social self-awareness, of inappropriate reactions to the other.
Correlations between autistic symptoms and behavioural characteristics of ASD children
The relationships between the severity of the symptoms assessed at the time of diagnosis (measured through the three ADOS-2 scores: total, SA and RRBs) and the different areas of cognitive, adaptive and behavioural development the child shows at moment of research, were calculated. As shown in Table 3, low cognitive profile scores (IQ) correspond to high and severe ADOS-2 scores. Also compared to adaptive skills (ABAS-II), high and severe scores of ADOS-2 correspond to lower scores in the area of community use (CU), of functional academics (FA), of home living (HL), health and safety (HS), self-care (SF) and socialization (Soc).
Correlation between ADOS-2 scores (Total, SA and RRBs) and Intellective Quotient, Adaptive Behaviour (ABAS-II), Sensory Profile and Behavioural characteristics (ASDBI) of the child with ASD (N = 53).
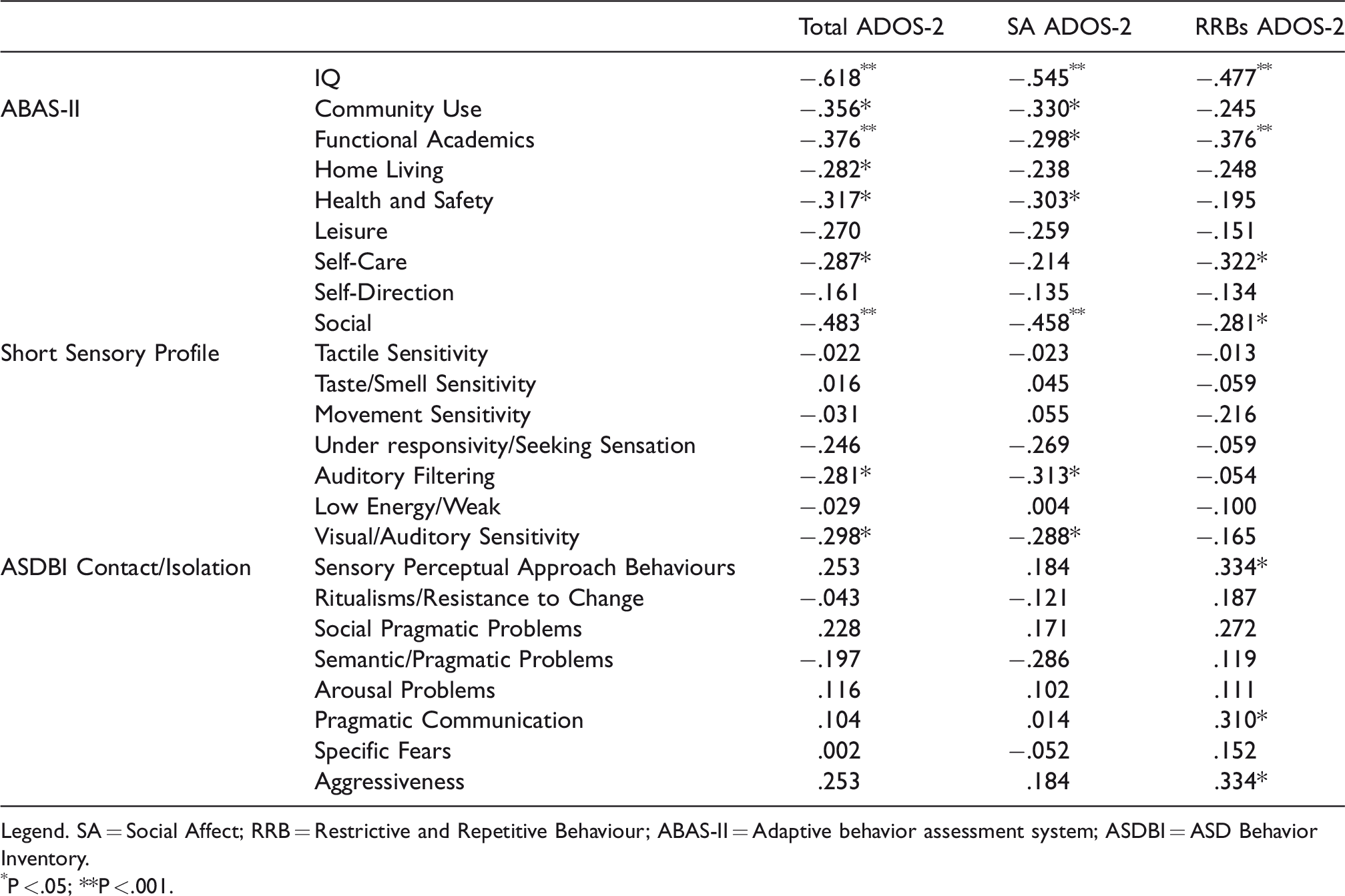
Legend. SA = Social Affect; RRB = Restrictive and Repetitive Behaviour; ABAS-II = Adaptive behavior assessment system; ASDBI = ASD Behavior Inventory.
P < .05; **P < .001.
From the questionnaires that evaluate sensory behaviours of the child (SSP) it emerges that severe ADOS-2 scores correspond to weaker attention skills in contexts where there is background noise (auditory filtering) and excessive general auditory reactivity (visual/auditory sensitivity).
Finally, from the questionnaire on symptomatic contact and isolation behaviours that the child shows at home (ASDBI) it emerges that the high scores of the Social Affects subscale of ADOS-2 correspond to greater alterations in the sensory perceptual approach, of pragmatic communication and aggressiveness.
Perceived parental stress
The scale assesses the stress perceived by parents; the higher the score, the greater the presence of stress reported in the last month. From the data analysis, no significant correlations emerge between the ADOS-2 scores of the children of the ASD group and the level of Stress Perceived by their parents (r = −.10). The parents of the ASD group generally obtained significantly higher and clinical scores of perceived stress than the parents of the control group (control group = 12.9 ± 5.4 vs ASD = 16.1 ± 7.1; F = 4.64; p < .05); the covariates ‘age of the child’ (P = .29) and ‘months of therapy' (P = .98) were not significant. From the qualitative analysis of the answers given to each item it emerges that there are three questions to which parents of ASD children answered with higher scores, thus indicating greater stress: No. 1 (how often did you feel out of your mind since something unexpected happen?) (F(1,51) = 6.43; p < .05); No. 2 (how often did you feel you were not able to control important things in your life?) (F(1,51) = 6.18; p < .05) and No. 10 (how often did you feel that difficulties were accumulating to such a point that you could not overcome them?) (F(1,51) = 11.64; p < .05).
The relationships between the profile of parents’ perceived stress and the adaptive, executive, sensory and behavioural characteristics of the child were then analyzed in the two study groups. Significant correlations are shown in Table 4. As for autonomies (ABAS-II), a higher level of perceived stress is related to greater adaptive difficulties of self-control in the child only in the control group. All other areas of ABAS-II do not show significant correlations with the scores at the Perceived Stress Scale. As for executive functioning (BRIEF-P: inhibit, shift, emotional regulation), in both groups the child's greatest difficulties correlate with greater parental stress. Compared to the Sensory Profile (SSP: Tactile Sensitivity, Under-Responsivity/Seeking Sensation and Visual/Auditory Sensitivity), more alterations of the child correlate with greater stress of the parent only in the control group. Finally, in both groups, greater behavioural symptoms (ASDBI: Sensory/Perceptual Approach Behaviours, Arousal Problems, Specific fears, Aggressiveness), correlate with higher stress levels.
Correlations between Perceived Stress Scale scores and Adaptive Behaviour (ABAS-II), Sensory Profile (SSP), Executive Functions (BRIEF-P) and Behavioural characteristics (ASDBI).

Legend. ABAS-II = Adaptive behavior assessment system; BRIEF-P = Behavior Rating Inventory of Executive Function; ASDBI = ASD Behavior Inventory.
P < .05; **P < .001.
Discussion
From the data analysis retrospectively collected with the parents, it appears that the children of the ASD and Control groups do not differ in terms of the achievement of the very first stages of development of postural control, the first autonomous walking and the appearance of the first single words. The combination of words and the appearance of the first sentences, however, seems to be later in the children of the ASD group, in line with other studies that have investigated the understanding and phrasal expression in autism (Luyster et al., 2005).
Significant differences also emerged in the descriptions that parents of the ASD and control groups make of their children in relation to adaptive skills. As found also by other authors (Joseph et al., 2002; Kanne et al., 2011), the children of the ASD group are described as having less ability in the conceptual, social and practical domains. The difficulties in the latter domain are manifested in the domestic context, in the use of the external environment, in self-care and in the regulation of safety behaviours, and were related to the duration of the therapy of the child; a longer period of treatment corresponds to fewer difficulties in the practical domain. In the literature, the association between adaptive behaviour and symptoms of autism seems to be confirmed, particularly in younger children (Golya & McIntyre, 2018; Kanne et al., 2011), although some research highlights that behavioural, social and linguistic difficulties associated with ASD in preschool can make the measurement of adaptive skills particularly unstable and subject to changes over time (Joseph et al., 2002; Rapin, 2003).
Similarly, more significant impairments emerged in the children of the ASD group compared to the executive functions assessed in the family context, in particular in the inhibition, shift, working memory and planning skills. However, no differences emerged in the area of emotional regulation. These results are in line with the data present in the literature, but as also emerges from a recent meta-analysis (Demetriou et al., 2018), contrary to what one might expect, the individual subdomains of executive functions are compromised to a different extent and not homogeneous in the autistic population.
With respect to the sensory profile, the research results demonstrate significantly greater difficulties in children of the ASD group compared to the control group. Hyper-and hypo-reactivity to sensory input are currently included as key features of autism in the DSM-5 (APA_American Psychiatric Association, 2013). The children of the ASD group showed severe difficulties in the areas of Tactile Sensitivity, so they express greater discomfort during moments of personal care or react excessively to physical contact; in the Under-Responsivity/Seeking Sensation for which they seek sensory stimulation, manipulate objects and things in a more stereotyped way and in the area of Auditory Filtering, so, for example they are more bothered by background noises, caused by fans, refrigerators, etc., or by sudden noises, which can lead them to show bizarre reactions.
As might be expected, from the results obtained through the rating scale on problematic Contact/Isolation behaviours, detected in the daily context by parents, it emerges that in the children of the ASD group more symptoms are described in the Sensory Perceptual Approach Behaviours, such as example, gaze fixation, use of the mouth for the exploration of inedible objects, repetitive handling behaviours. Furthermore, the children of the ASD group also show greater difficulties in reacting to environmental changes and in the manifestation of Ritualism, greater Social-Pragmatic difficulties, for example in the way of approaching other people, of inappropriate reactions to the others and greater symptoms of impaired excitability and aggression, for example motor restlessness, sleep regulation and aggressive attitudes towards self or others. When the level of stress perceived by parents was investigated through the Perceived Stress Scale, it emerged that the parents of ASD children, compared to the control group, showed significantly higher levels of stress, mainly due to the difficulty of managing unexpected events, the feeling of loss of control over one's life and the fear of not being able to cope with the adversities they were experiencing. This is consistent with previous studies showing that parents of ASD children report higher stress levels than both parents of children with typical development and those of children with other disabilities (Baker-Ericzén et al., 2005; Blacher & McIntyre, 2006; Rivard et al., 2014).
However, the stress level of the parents was not related to the severity level of the autistic symptomatology, assessed through the ADOS-2 score, nor to the adaptive skills of the child with ASD; this data differs from what is usually reported in some studies, which identify among the factors associated with parental stress, the severity of autistic symptoms and the level of functioning of children (Hall & Graff, 2011; Ingersoll & Hambrick, 2011, Miranda et al., 2019). In this research, stress detection tools are used aimed at detecting the stress experienced by the parent with respect to his or her parental role. In the present study, on the other hand, was used the Perceived Stress Scale, which instead aims to measure the perception of stress that an adult experiences, with respect to the changes that have occurred in his or her life, without focusing exclusively on the parental role. The results of this research are in fact in line with the research that shows that parents of children with ASD report stress levels more correlated to personal aspects rather than to the symptomatic characteristics of the child or to the parent-child relationship (Rivard et al., 2014). The severity of autistic symptoms represented, according to these authors, a predictor of paternal, but not maternal, stress.
The analysis of the data instead shows that the stress perceived by the parents is related to the executive functioning of the child, so the parents of children with greater dysfunctions in the areas of inhibition, shift and emotional regulation were more stressed. In the literature, the research is quite consistent in considering the impairment of executive functions as one of the central aspects of the autism spectrum disorder (Craig et al., 2016; Demetriou et al., 2018). It is interesting to note that in the present research the areas that were most critical, both for children with autism and for those with speech disorders, concern the so-called ‘hot’ executive functions, which are usually activated to regulate emotional reactions and motivation, during stressful situations or in emotionally significant contexts. This also seems to be confirmed by the significant correlations between the stress perceived by the parent and the behavioural symptomatology (assessed through the ASDBI) concerning the methods of Sensory/Perceptual Approach Behaviours, problems of excitability of children.
The multiple relationships between the child's emotional and behavioural characteristics and the stress perceived by the parent were also investigated in a recent study (Miranda et al., 2019), in which the authors analyzed a sample of school-aged children (from seven to 11 years). They conclude that mothers' support, as well as active coping strategies and emotional support are all elements that mothers need to deal with stress, and represent valid mediators capable of significantly reduce parental stress in managing the behavioural difficulties of ASD children.
Therefore, supporting the ways in which caregivers adapt to the signals of children is an important strategy, which has now become a key element of treatments for autism mediated by parents. Some authors (Shire et al., 2016) observed that during parent-child play interactions, parental responsiveness and joint attention increased after a cycle of intervention mediated by parents compared to standard psycho-educational interventions.
The results of this study must be interpreted in the light of its methodological limitations. For example, the tool used to measure stress assesses parental perception and should be accompanied by measures that can highlight other stress and resilience factors that could modulate parental well-being. Furthermore, the correlational design does not allow the determination of the causal relationships between perceived stress and characteristics of children. It should be further investigated how these relationships can influence each other, in order to adapt and personalize therapeutic interventions more, shifting the focus of treatment from the pathological symptom of the child to what some authors describe as family maladaptation, understood as the continuous discrepancy between needs of the child and the family's ability to deal with them (Miranda et al., 2019).
Conclusions
The study just described therefore highlighted how much the difficulties that children with ASD manifest in adaptive skills, sensory profile and executive functioning are often more evident and clinically more significant than in children with SLI. The level of stress perceived by the parents is also less related to the specific clinical symptomatology, and more connected to the difficulties that children show at a behavioural level (problems of excitability, specific fears, aggressive behaviour), in emotional regulation and generally in the emotional component of the executive operation. Hence the reflection on how much this relationship can create a vicious circle, in which the child's behavioural and affective regulation difficulties can favour the increase of stress in the parents, and consequently how high stress levels reduce the parenting coping skills in management, but also in understanding the child's problem behaviours. This suggests the importance of including parents in children's therapeutic paths, not so much as ‘educators’ or ‘therapists’ of their children, but as fundamental parts of a meaningful relationship, in which they can work to transform the vicious circle into a virtuous one. In this way, the parent is supported in understanding the meanings of the symptom and how it manifests in the child, is helped to understand how to manage it. This should consequently increase the self-efficacy experiences in the parent, and consequently reduce the perception of stress due to the loss of control over one's life. Future studies will provide crucial information on possible support programs that could be implemented for families.
Footnotes
Acknowledgements
This article is based on the activities of the Institute of Ortofonologia (IdO) of Rome. We are grateful to the psychologist, child psychiatrist, speech therapist, parents, and children whose participation made this work possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.