
Abstract
Background and aims
Over recent decades much research has focused on detecting predictors of different language trajectories in children with early language delay but there has been very little exploration of social communication trajectories in these children. We report a longitudinal study that investigated the predictive value and clinical significance of elicited body movement imitation and language for later social communication and language outcome in Late Talkers.
Methods
Participants were 29 German-speaking children who were identified with delayed onset and progression of language at two years and followed up at four years. Novel assessments of posture and gesture imitation were administered at Time 1, together with standardised language measures. All body movement imitation items involved self-other mappings, assumed to rely on sociocognitive capacities. At Time 2, children were assessed on standard language tests, together with parental reports of social communication.
Results
Early language skills at Time 1 were significantly associated with later language outcome and body movement imitation skills at Time 1 with later social communication outcome. Logistic regression analyses revealed that body movement imitation as well as language at Time 1 added significantly to the prediction of language outcome at Time 2, whereas only body movement imitation made a significant contribution to the prediction of social communication outcome at Time 2.
Conclusions and implications
Theoretically, results highlight the need to account for the heterogeneity of different language and communication trajectories in children with early language delay and point to the importance of sociocognitive difficulties observed in some of these children. Clinically, this study demonstrated that body movement imitation measures have the potential to improve the identification of pre-schoolers who are at risk of later social communication and language problems.
Introduction
Some otherwise typically developing toddlers have delayed onset and progression of language for no apparent reason. These children are widely referred to as Late Talkers (LT) in the literature (Rescorla & Dale, 2013). A substantial number of LTs move into the typical range on standardised language measures during the preschool period, but a subset continues with language impairments throughout the school years (Domsch et al., 2012; Ellis & Thal, 2008; Henrichs et al., 2011; Moyle, Weismer, Evans, & Lindstrom, 2007; Paul & Roth, 2011; Rescorla, 2011; Westerlund, Berglund, & Eriksson, 2006). LTs do not constitute a homogeneous group but present with varied profiles of language and/or social communication skills and deficits which change over time: some present with expressive language problems only, whereas others also evidence limited receptive language and/or social communication skills that border on Autism Spectrum Disorders (ASD) (Desmarais, Sylvestre, Meyer, Bairati, & Rouleau, 2008; Ellis & Thal, 2008; Hawa & Spanoudis, 2014; Paul & Ellis Weismer, 2013; Paul & Roth, 2011). But although some LTs and young children with ASD share common features, it is important to acknowledge that not all late-talking toddlers with social communication deficits meet diagnostic criteria for ASD. In this study, we focussed on toddlers who presented with delayed language and communication skills for no apparent reason and no child in this study had a clinical diagnosis of ASD.
The term LTs has been used in various ways. Traditionally, LTs have been identified by expressive language delay, using different language measures and cut-off criteria at different points in age. Some studies have excluded children with receptive delays, but this restricts generalisability of findings. The term LT as used in this study includes children with both expressive only and expressive–receptive delays as the exclusive focus on expressive delay runs the risk of covering only a certain proportion of children with late language emergence.
Clinically, it is important to identify LTs who are at high risk of significant language impairments when they get older, so that early intervention services can be directed to this subset. Consequently, much research has focused on detecting predictors of different language trajectories in young children with late language emergence. This has shown that prediction of language outcome is poor if reliance is only placed on expressive language measures, especially when using early parent-report measures of language development (Dale, Price, Bishop, & Plomin, 2003; Feldman et al., 2005; Henrichs et al., 2011; Westerlund et al., 2006). There is a need for multifactorial predictive risk models that include a wide range of verbal and nonverbal factors (Desmarais et al., 2008; Ellis & Thal, 2008; Hawa & Spanoudis, 2014; Olswang, Rodriguez, & Timler, 1998; Paul & Roth, 2011; Zambrana, Pons, Eadie, & Ystrom, 2014). To date, numerous perinatal (e.g. foetal growth (Rice, 2012; Zubrick, Taylor, Rice, & Slegers, 2007)), parental and demographic (e.g. maternal education (Dale et al., 2003), socioeconomic status (Horwitz et al., 2003) and child factors (e.g. limited symbolic play (Rescorla & Goossens, 1992)) have been studied. At a group level, all these factors seem to predict poor language outcome to some extent, but results are inconsistent and predictive value of outcome in individual cases is still too inaccurate to provide clinicians with a reliable guide in deciding which LTs should receive early language intervention (Dale et al., 2003; Henrichs et al., 2011; Rice, Taylor, & Zubrick, 2008; Westerlund et al., 2006). The more reliable risk factors appear to be a delay in language comprehension (Bishop et al., 2012; Ellis Weismer, 2007; Henrichs et al., 2011; Silva, 1980; Thal, Tobias, & Morrison, 1991; Zambrana et al., 2014), a family history of language and literacy difficulties (Bishop, Price, Dale, & Plomin, 2003; Lyytinen, Eklund, & Lyytinen, 2005; Reilly et al., 2010; Rice, 2012; Zambrana et al., 2014; Zubrick et al., 2007) and male gender (Henrichs et al., 2011; Horwitz et al., 2003; Reilly et al., 2010; Zambrana et al., 2014; Zubrick et al., 2007). It also seems to be generally accepted that the more risk factors are present, the higher the risk for persistent language deficits and the greater the need for clinical intervention (Desmarais et al., 2008; Ellis & Thal, 2008; Hawa & Spanoudis, 2014; Henrichs et al., 2011; Olswang et al., 1998; Paul & Roth, 2011). However, prediction at the individual level remains poor.
Nonverbal and social communication trajectories in Late Talkers
Some studies of children with delayed language emergence have looked beyond spoken language to consider nonverbal aspects and found that LTs received poorer scores than controls on measures of symbolic play (Rescorla & Goossens, 1992), imitation of pretend acts (Dohmen, Chiat, & Roy, 2013; Thal & Bates, 1988), imitation of postures and gestures (Dohmen et al., 2013), spontaneous use of gestures (Thal, Bates, Goodman, & Jahn-Samilo, 1997) and communicative acts (Bonifacio et al., 2007; Desmarais et al., 2008; MacRoy-Higgins & Kaufman, 2012; van Balkom, Verhoeven, & van Weerdenburg, 2010).
However, there has been very little exploration of these nonverbal trajectories across age; most studies in this area have been cross-sectional, or if looking at outcomes, have focused on spoken language trajectories. To our knowledge, only four studies have investigated relations between these types of nonverbal skills in LTs and their later language and/or social communication outcome using a longitudinal design.
Thal et al. (1991) followed-up language trajectories in a small group of 18-32-month-old LTs one year after they assessed them on two tasks which required the imitation of different types of pretend acts: the imitation of single pretend acts with appropriate and substitute objects and the imitation of sequences of pretend acts with appropriate objects (all designated as use of symbolic gestures). They found that the group of children who were categorised as true LTs (n = 4) at Time 2 (T2), i.e. those children who still demonstrated expressive language delay at follow-up, performed significantly worse than the group of late bloomers (n=6), i.e. those children who caught up with their typically developing peers, on both pretend imitation tasks at Time 1 (T1).
Zambrana et al. (2014) studied whether an integrative model of risk factors including limited early communication skills, family history of language difficulties, delayed language comprehension and male gender would predict later persistent, recovering and late-onset trajectories of language delay in a large population-based cohort study (n = 10,587). Children’s communication skills at 18 months were measured using four items from the Modified Checklist for Autism in Toddlers (Robins, Fein, Barton, & Green, 2001) and the Ages and Stages Questionnaire (Richter & Janson, 2007), asking parents about children’s abilities to use pointing to initiate different communicative acts and to spontaneously imitate different types of everyday actions. Language outcome at 3–5 years was assessed using a subset of questions of the Ages and Stages Questionnaire, a parental questionnaire that focuses on children’s oral language skills but also taps their abilities to use language in social contexts. Thus, the questionnaire seems to measure language forms and structures as well as language use but does not differentiate between different outcome profiles of language and social communication. Results showed that poor communication skills at 18 months were associated with all trajectories of language delay from 3–5 years, but the effects were small.
Pesco and O’Neill (2012) investigated the ability of the Language Use Inventory (O’Neill, 2007) to predict language outcomes of 348 children at 5–6 years who had been assessed with the Language Use Inventory at 18–47 months. Findings revealed a very respectable predictive validity of the Language Use Inventory for later language outcome for children aged 24–47 months but was less convincing for children aged 18–23 months. The Language Use Inventory is a 180 items parent report designed to measure children’s language use in everyday situations while focusing on oral language. Children’s language outcome was assessed using three standardised tests: the Diagnostic Evaluation of Language Variation – Norm Referenced (Seymour, Roeper, & de Villiers, 2005), designed to measure children’s syntactic, semantic and pragmatic skills; the Clinical Evaluation of Language Fundamental – Preschool, 2nd Edition (Wiig, Secord, & Semel, 2004), designed to measure different language skills at word and sentence level, and the Children’s Communication Checklist – 2nd Edition, U.S. Edition (Bishop, 2006), designed to measure children’s pragmatic skills in everyday situations. Children’s performance at T2 was categorised as presenting with language difficulties when they scored below the seventh percentile on one outcome measure or had been diagnosed with language difficulties since T1 according to parental report. Positive cases might therefore have presented with varied profiles of language and/or social communication problems which were not further specified by the authors.
Chiat and Roy (2008, 2013) evaluated the hypothesis that early sociocognition would predict later language and social communication outcome in young children referred to speech and language therapy services due to concern about language development. At the age of 2;6–4;0 (T1), three different sociocognitive skills, social responsiveness, joint attention and symbolic understanding, were measured using the Early Sociocognitive Battery (Chiat & Roy, 2006). All tasks were essentially nonverbal. Children’s language and social communication skills were followed up at the ages of 4–5 years (T2, n = 163) and 9–11 years (Time 3; T3, n = 108), using direct language assessment and different parental questionnaires tapping social communication. Difficulties with the Early Sociocognitive Battery were significantly associated with later social communication problems at T2 and T3 at group and case level, suggesting that deficits in sociocognition at 2;6–4;0 years contribute to children’s later social communication problems. At 9–11 years, four distinct subgroups with language impairment only (LI), social communication impairment only (SCI), both language and social communication impairments (LI-SCI) or neither problem, were identified. Investigation of developmental trajectories revealed that the three impaired groups (LI, SCI and LI-SCI) did not differ on language or parent ratings of social, emotional and behavioural difficulties when first seen. Only performance on the Early Sociocognitive Battery differentiated the children with and without social communication problems seven years later, at 9–11 years (Roy & Chiat, 2014). Nonetheless, the authors conclude that, while the Early Sociocognitive Battery is valuable, it is not sufficient to predict all deficits in social communication.
Overall, all four studies found some type of relation between early sociocognitive and/or nonverbal communication skills and later language or social communication outcomes in young children with a delayed onset of language. This suggests that early sociocognitive and nonverbal communication behaviours are promising predictors of children’s language and/or social communication trajectories with the potential to inform the decision-making process of speech and language therapists. Interestingly, most studies focus solely on children’s language outcomes, without looking separately at their social communication skills. This neglect is surprising, given that the heterogeneity of the population of children with specific deficits in language is well established (Leonard, 1998). It is also remarkable considering that most intervention programmes for children with late language emergence are designed to facilitate children’s and parents’ communication skills as a catalyst for everyday language and social communication (e.g. Hanen Training Program (Manolson, 1992)). The overview also highlights the struggle to find strong predictors for children aged 18–24 months, suggesting that 18 months might simply be too young to try and identify long-term problems. Recent findings provide some indication that the prediction of later problems improves with age (Dale & Hayiou-Thomas, 2013; Dollaghan & Campbell, 2009; Duff, Plunkett, Nation, & Bishop, 2015), but our understanding of how heterogeneous language and communication trajectories might change over specific age bands in toddlers with language delay remains limited.
The mapping theory
This study aimed to add to the understanding of the heterogeneity of early language and social communication trajectories. It investigated body movement imitation and general language skills of LTs as predictors of their later social communication and language outcomes and is rooted in the mapping theory (Chiat, 2001; Chiat & Roy, 2008). The mapping theory argues that language impairments must arise from a breakdown at some point in the mapping process, i.e. the discovery of forms, the discovery of meanings and the acquisition of connections between form and meaning which are specific to a language (Chiat, 2001). The theory focuses on two sets of early processing skills, sociocognitive and phonological, which are hypothesised to be crucial to this process. These skills have been associated with concurrent and later language and social communication abilities, and it is proposed that either or both may be the source of deficits in language. The sociocognitive hypothesis focuses on children’s abilities to use a range of pragmatic cues in order to infer the meaning intentions behind speakers’ utterances and hence discover the meaning of their words. These sociocognitive skills are therefore argued to have a ‘bootstrapping’ role in language. They are also crucial for social communication. It is therefore predicted that difficulties with sociocognition will affect the developmental trajectory through which language and social communication emerge. Since nonverbal imitation skills are assumed to rely significantly on sociocognitive abilities (Carpenter, Pennington, & Rogers, 2002; Tomasello & Carpenter, 2005) but do not involve the processing of structural aspects of language, we argue that difficulties with elicited body movement imitation provide a window onto sociocognitive abilities independently of difficulties with the processing of the structural aspects of language. To date, a wealth of studies have addressed nonverbal imitation deficits in children with ASD, who are known to have sociocognitive difficulties, but nonverbal imitation has barely been explored in LTs (see Dohmen et al., 2013 for more information).
The current study
Results from the initial phase of this longitudinal study, at T1, were reported in Dohmen et al. (2013). We compared typically developing children and LTs aged 2;0–3;5 years on a range of novel nonverbal imitation tasks that to a greater or lesser extent involved sociocognitive skills. It was hypothesised that at a group level the LT sample would perform significantly below the typically developing sample on imitation tasks categorised as ‘social’ (i.e. the imitation of body movements), while imitation tasks categorised as ‘instrumental’ (i.e. the imitation of actions on objects) would be no more challenging for the LT sample than the typically developing sample. In order to investigate whether and how imitation and language profiles might change over age, children were divided into three 6-months age bands within the typical and clinical samples (2;0–2;5; 2;6–2;11; 3;0–3;5). In line with our hypotheses, significant group differences were found for all body movement imitation tasks but not for the actions on objects tasks. However, while the majority of 2-year-old LTs scored substantially below their typically developing peers on body movement imitation, most 3-year-old LTs scored within the range of their typically developing peers. Group differences in the 3-year-old were due to a minority of children who emerged as outliers.
Here we report a follow-up study (T2) investigating the predictive value and clinical significance of elicited immediate body movement imitation tasks and receptive and expressive language tests for social communication and language outcomes two years after T1, when children were aged four years. All body movement imitation items involved self-other mappings which were assumed to rely on sociocognitive capacities. These tasks focussed exclusively on the demonstrator as a person and required the imitator to connect and engage socially with this unfamiliar person in a shared activity. The instrumental tasks involving objects or an observable functional outcome that did not differentiate the groups at T1 were excluded. We aimed to evaluate the following hypotheses:
Performance on general language tests at T1 will predict language outcome at T2. Performance on body movement imitation tasks at T1 will predict social communication and language outcome at T2.
Methods
Procedures
Approval for data collection at T1 was given by the City University School of Community and Health Sciences Research Ethics Committee (reference number: PhD/08-09/05) and approval for the follow-up study at T2 by the Central University Research Ethics Committee of the University of Oxford (reference number: MSD-IDREC-C2-2012-24). Participants were recruited to this study by paediatricians, speech and language therapists, phoniatricians and nursery teachers from clinical institutions and nurseries in the areas of Bonn and Magdeburg in Germany (Dohmen et al., 2013). Each participant was seen individually at the child’s home, nursery or clinic and parents gave signed consent for their own and their child’s participation prior to the assessments. Assessments at both phases were administered in a fixed order. At T1, children were seen for two or three sessions lasting 30–45 min, and at T2 for one or two sessions lasting 45–60 min. Questionnaires relating to the child’s general developmental history were given to parents at both stages to return in stamped addressed envelopes.
Participants
Twenty nine of the 30 children who were identified with delayed onset and progression of language at two years were followed up at four years (one child could not be contacted and was excluded from all analyses). We also excluded the six children available for follow-up who had been in a group of 15 children ages 3;0–3;5 at T1, as the attrition rate was so high. Thus, the current study reports data for 29 children reassessed two years after first being seen at ages 2;0–2;11. At the time of referral, all children had German as their main language, no significant history of general developmental delay or disorder, and met the criteria for delayed language development (see Language: T1 and T2). No child had a clinical diagnosis of ASD at T1 or T2.
Age (months) and nonverbal (NV) cognitive ability a of participants of the longitudinal study at T1 and T2 (n = 29).

Scores shown as standard scores (mean ± SD of 100 ± 15), n = number of participants.
Assessments
Body movement imitation
At T1, all children were assessed on a novel imitation battery that included a range of nonverbal (four body movement tasks and three action on object tasks; see Dohmen et al., 2013 for full details) and verbal (word, nonword and sentence repetition) imitation tasks. The imitation battery alternated between body movement, actions on objects and verbal tasks and was presented in two counterbalanced orders to control for fatigue and practice effects. All nonverbal imitation tasks were embedded in game-like contexts that were specifically designed to keep children at this young age engaged and to elicit immediate responses with a minimum of verbal instructions.
Body movement imitation tasks (23 items yielding a maximum score of 41).

Number of items per subtask with max. raw score in parentheses.
Facial postures and expressions (5 items) were scored with a simple pass–fail coding scale for attempt (1) or refusal (0) to imitate, since piloting revealed that it was not possible to reliably score these in a more graduated way (maximum total = 5). Manual postures (10 items), conventional gestures (4 items) and object-related gestures (4 items) have clearer components allowing for reliable differentiation of attempts to imitate and were scored using a more graduated coding scale for accurate (2), partial (1) and unrelated (0) imitation responses and refusal to imitate (0) (maximum total = 36). For the follow-up study, a body movement imitation composite score of all 23 items was derived by summing each child’s raw scores for all T1 posture and gesture tasks yielding a maximum raw score of 41 (henceforth referred to as body movement imitation score; see Table 2 for full scoring criteria).
Categorical classification on T1 body movement imitation
As reported in ‘Introduction’ section, significant differences between groups of typically developing children and LTs were found on all body movement imitation tasks at T1. An analysis of error patterns showed that the poorer performance of the LT sample stemmed from higher nonresponse rates and not from incorrect responses. Evidence from children’s compliance on the instrumental tasks revealed that noncompliance was selective, suggesting specific difficulty with the body movement imitation tasks rather than uncooperativeness (see Dohmen et al., 2013 for full details). Children in the typically developing and LT groups differed in terms of whether rather than how accurately they attempted to imitate body movements, in keeping with an almost bimodal distribution of children’s body movement imitation scores at T1 with a 10-point gap between the body movement imitation scores of 7 and the next score of 17 (minimum score = 0; maximum score = 32; mean = 8.41; SD = 11.36). Therefore, performance on the T1 body movement imitation task was categorised as ‘refusal’ or ‘attempt’. A receiver operating characteristics curve analysis revealed that the optimal cut-off point that maximise sensitivity and specificity was between a score of 1.5 (sensitivity = 0.91 and specificity = .72) and 2.5 (sensitivity = .82 and specificity = .78). Accordingly, a body movement imitation score ≤ 2 out of 41 was classified as refusal, a score ≥ 3 as attempt.
Language and social communication
All tests are validated, reliable measures of language and social communication ability in young children and are widely used in clinical practice in Germany.
Language: T1 and T2
At T1, children were assessed with the Sprachentwicklungstest für zweijährige Kinder (SETK-2) (Grimm, Aktas, & Frevert, 2000). The SETK-2 is a standardised test that was constructed to measure children’s general stage of language development between 24–35 months. It comprises four subtests to assess receptive and expressive language competencies: word comprehension, sentence comprehension, word production and sentence production. Children were classified as LTs when they performed at least 1.5 SD below average on one subtest and 1.25 SD below average on another subtest.
At T2, receptive and expressive language abilities of the follow-up sample were assessed on five measures drawn from standardised tests:
The TROG-D (Fox, 2009), the German version of the Test for Reception of Grammar (Bishop, 2003), measures the comprehension of sentences of increasing complexity. The subtests noun and verb production of the Patholinguistische Diagnostik bei Sprachentwicklungsstörungen (PDSS) (Kauschke & Siegmüller, 2009), in which children are asked to name pictured objects and events, assess expressive vocabulary skills. The subtest plural marker of the PDSS elicits the morphological plural marker. The subtest sentence repetition of the Sprachentwicklungstest fűr dreijährige Kinder (SETK-3-5) (Grimm & Aktas, 2001) measures morphosyntactic abilities.
Children were classified as having specific language impairment when they performed at least 1.5 SD below average on one subtest and 1.25 SD below average on another subtest. Thus, the same criteria for defining language deficits were applied to participants at T1 and T2.
Social communication: T2
Social communication skills were assessed using the Skala zur Erfassung sozialer Reaktivität (SRS) (Bölte & Poustka, 2008), the German version of the Social Responsiveness Scale (Constantino & Gruber, 2005) which has been standardised on 1436 German-speaking children. The rating scale was completed by a parent. It is designed to measure aspects of social interaction in five areas: social awareness, social cognition, social communication, social motivation and autistic mannerisms. In a clinical context, interpretation is based on a single score reflecting the sum of responses to all 65 questions and raw scores are converted to T-values according to gender of child and rater type (parent/teacher) (mean ± SD of 50 ± 10). The SRS manual specifies cut-off scores for categories of performance: ≤ 40 high social responsiveness, ≤ 60 normal social responsiveness, ≥ 61 mild to moderate impairment of social responsiveness, ≥ 76 severe impairment of social responsiveness. Children with mild to moderate impairments show social communication deficits which are sometimes associated with mild ASD, whereas a severe impairment is strongly associated with a clinical diagnosis of ASD. Based on these categories, children in the follow-up sample were classified as having social communication impairments (SCIs) if their T-value was ≥ 61.
Categorical classification on language and social communication: Follow-up sample
At T2, children in the follow-up sample were classified into four groups based on their categorical performance on language and social communication measures according to the cut-off scores for language impairment and social communication impairment described above: language and social communication impairment (LI-SCI), language impairment only (LI), social communication impairment only (SCI), typical language and communication development (TD) in line with the four-way categorisation used in Roy and Chiat (2014).
Results
Categorical performance on body movement imitation T1
The number of children who refused the body movement imitation task at T1 decreased with age: 61.1% of children in the younger (2;0-2;5: 11of 18) and 45.5% of children in the older (2;6-2;11: 5 of 11) age group were classified as refusers.
Categorical outcome on language and social communication T2
Since children in the LT sample at T1 had to fulfill the study’s criteria for delayed language development, by definition, each participant scored below the chosen cut-off on at least two language subtests at that time. At T2, according to the categorical cut-off scores for language and social communication described above, roughly two-thirds of children in the follow-up sample were classified as LI and/or SCI (62%, 18 of 29 children), including 31% (9) with LI-SCI; 21% (6) with LI only; and 10% (3) with SCI only, with the remaining one-third classified as TD (38%, 11of 29). Half of the 2;0–2;5 group emerged as TD (nine of 18), compared with only a fifth of the 2;6–2;11 group (18.2%, two of 11). A Fisher’s exact two-tailed test revealed that the percentage in the younger group was higher, but not significantly so (p = .13). Data for the 2-year-olds (n = 29) were grouped together to have a large enough sample for quantitative analysis. No child was identified with a severe impairment of social communication (score ≥ 76 on the SRS), indicative of an ASD diagnosis, nor had any child received an independent clinical diagnosis of ASD.
Associations between T1 predictor and T2 outcome measures using continuous scores
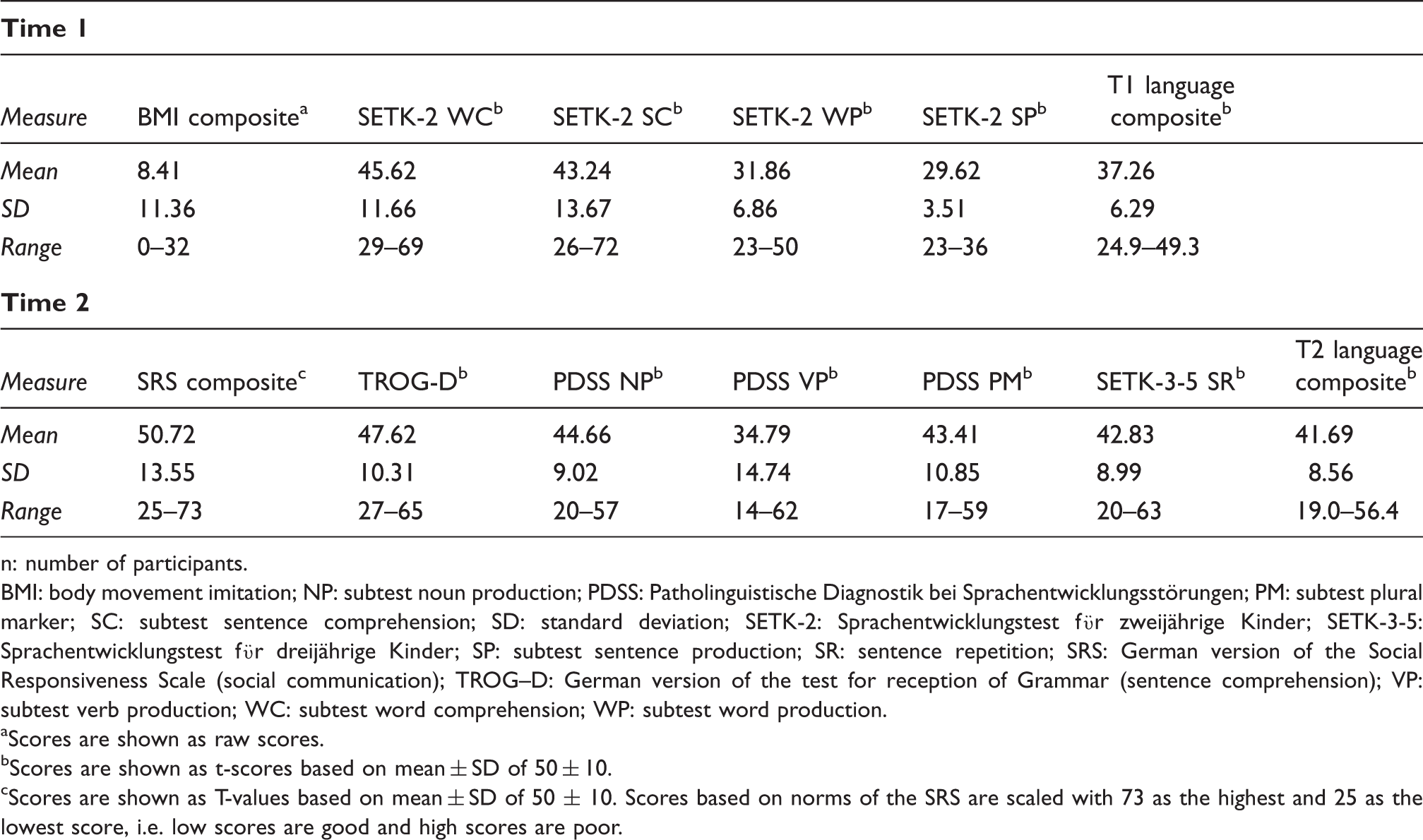
Continuous scores on body movement imitation (max = 41), language predictor measures and language and social communication outcome measures (n = 29).
n: number of participants.
BMI: body movement imitation; NP: subtest noun production; PDSS: Patholinguistische Diagnostik bei Sprachentwicklungsstörungen; PM: subtest plural marker; SC: subtest sentence comprehension; SD: standard deviation; SETK-2: Sprachentwicklungstest fϋr zweijährige Kinder; SETK-3-5: Sprachentwicklungstest fϋr dreijährige Kinder; SP: subtest sentence production; SR: sentence repetition; SRS: German version of the Social Responsiveness Scale (social communication); TROG–D: German version of the test for reception of Grammar (sentence comprehension); VP: subtest verb production; WC: subtest word comprehension; WP: subtest word production.
Scores are shown as raw scores.
Scores are shown as t-scores based on mean ± SD of 50 ± 10.
Scores are shown as T-values based on mean ± SD of 50 ± 10. Scores based on norms of the SRS are scaled with 73 as the highest and 25 as the lowest score, i.e. low scores are good and high scores are poor.
Spearman’s rho correlations were used to assess the strength of relations between continuous scores on T1 predictor and T2 outcome measures. In line with predictions performance on body movement, imitation at T1 was associated with social communication outcome at T2 (r = −.66; p ≤ .001, 95% CI −.39 to −.83), and performance on language measures at T1 was associated with language outcomes at T2 (r = .62; p ≤ .001, 95% CI −.33 to −.80). In contrast, correlations between performance on body movement imitation at T1 and language outcome at T2 (r = .29, p = .13, 95% CI −.59 to .09) and performance on language measures at T1 and social communication outcome at T2 (r = −.28, p = .14, 95% CI −.59 to .10) were not significant.
Relations between T1 body movement imitation and T2 language and social communication using categorical scores
Frequencies for categorical performance (n = 29) on T1 body movement imitation and T2 language and social communication.
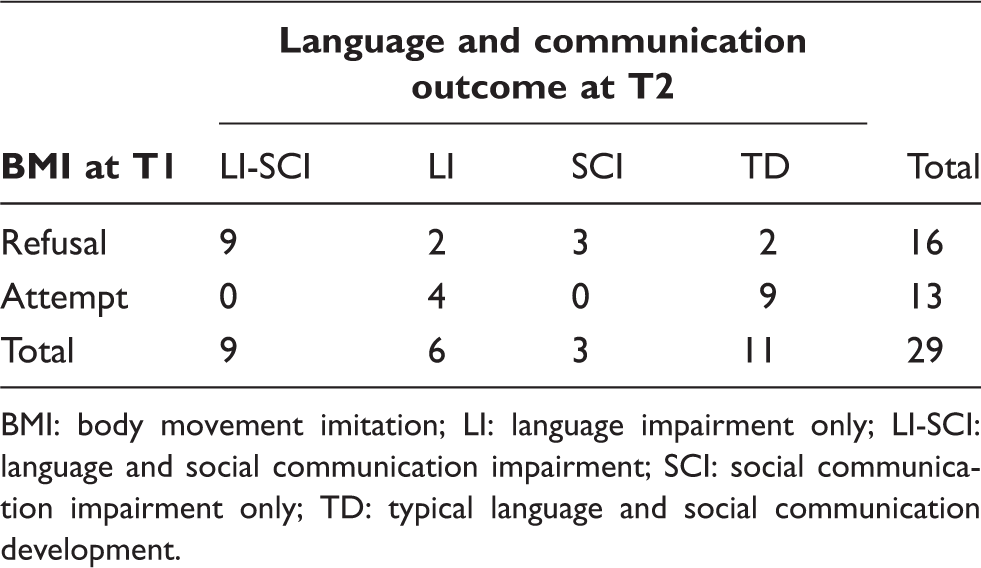
BMI: body movement imitation; LI: language impairment only; LI-SCI: language and social communication impairment; SCI: social communication impairment only; TD: typical language and social communication development.
As can be seen in Table 4 at follow-up, typical language was associated with typical social communication (TD n = 11) and impaired language was associated with impaired social communication (LI-SCI n = 9) in more than two-thirds of participants (n = 20, 69%). Fewer children were classified with LI only (n = 6), and cases of SCI only were rare (n = 3). Hence, it appears that at this young age social communication difficulties frequently co-occurred with impaired language.
Turning to the relation between T1 predictor and T2 outcome variables, a Fisher’s exact test revealed a highly significant association between the classification of body movement imitation at T1 and the profile of language and social communication outcome at T2 (p < .001; since more than 20% of cells had an expected count less than five, an exact contingency table analysis was conducted using the web source ‘statistics to use’ (Kirkman, 1996) as recommended by McDonald (2009)).
Outcome profiles of TD were in nine out of 11 cases (81.8%) associated with an attempt at body movement imitation at T1, irrespective of the strength and profile of children’s language delay at age two. In contrast, outcome profiles of SCI with or without co-occurring LI were all associated with refusal on body movement imitation at T1 (12 of 12; 100%). However, categorical performance on T1 body movement imitation predicted a third (2/6) only of T2 outcome profiles of LI correctly. Hence, performance on body movement imitation at T1 seems to be a very good predictor of later social communication difficulties but a rather poor predictor of ‘pure’ LIs. However, due to the fact that the majority of children with language problems also showed SCIs, performance on body movement imitation at T1 nevertheless predicted almost three quarters of children who presented with language difficulties at T2 (73.3%, 11 of 15).
Logistic regression: Contribution of age, language and body movement imitation at T1 for language and social communication outcome at T2
Logistic regression results for T1 predictors of T2 outcome (n = 29); discrete dependent variable: impaired development versus typical development.
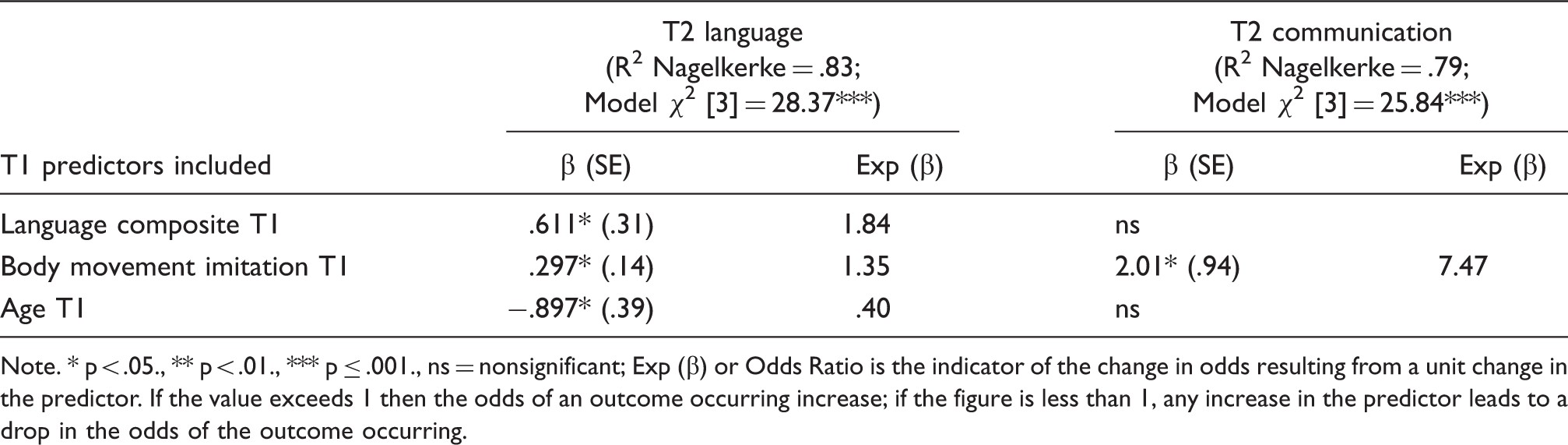
Note. * p < .05., ** p < .01., *** p ≤ .001., ns = nonsignificant; Exp (β) or Odds Ratio is the indicator of the change in odds resulting from a unit change in the predictor. If the value exceeds 1 then the odds of an outcome occurring increase; if the figure is less than 1, any increase in the predictor leads to a drop in the odds of the outcome occurring.
In the case of language outcome all three predictor variables added significantly to the amount of change explained by the model. The predictor language has an Odds Ratio (i.e. Exp (β)) of 1.84; the predictor body movement imitation has an Odds Ratio of 1.35. This indicates that when language scores at T1 are raised by one unit, participants are 1.84 times more likely to present with an outcome of typical language development at T2, and when body movement imitation scores at T1 are raised by one unit, participants are 1.35 times more likely to have a language outcome of typical language development at T2. The Odds Ratio value associated with age is 0.40, indicating that for every additional month in age at T1, participants are 0.40 times less likely to have an outcome of typical language development at T2 (i.e. to be identified with language impairment).
In the case of social communication outcome, only body movement imitation made a significant contribution to prediction. The Odds Ratio value associated with body movement imitation is 7.47, indicating that when body movement imitation scores at T1 are raised by one unit, participants are 7.47 times more likely to present with an outcome of typical social communication outcome at T2, once body movement imitation had been taken into account. The variables language and age did not make a statistically significant contribution to the model. Results not only confirmed body movement imitation as an exclusive and moderately strong predictor of later social communication outcome but in addition revealed a significant contribution of performance on body movement imitation to prediction of later language outcome.
Discussion
This longitudinal study followed up language and social communication outcomes in a sample of 4-year-old children who were identified as LTs at the age of 2;0–2;11. In line with previous findings, 50% of the LTs who were 2;0–2;5 at T1 had moved into the typical range by age four, whereas only 18% of the LTs who were 2;6–2;11 had normalised. This is on par with previous reports that only a subset of children who were identified as LTs at the age of two continues with language and/or social communication impairments when they get older (Domsch et al., 2012; Ellis & Thal, 2008; Henrichs et al., 2011; Moyle et al., 2007; Paul & Roth, 2011; Rescorla, 2011; Westerlund et al., 2006). However, the percentage of late bloomers in our study is lower than in most unselected population studies, especially when language status was identified using parental questionnaires to measure children’s language status (Dale et al., 2003; Henrichs et al., 2011; Zambrana et al., 2014), but consistent with previous reports of language and/or social communication outcomes of clinically referred samples (Chiat & Roy, 2008; Everitt, Hannaford, & Conti-Ramsden, 2009). This highlights the fact that the actual percentage of late bloomers seems to be related to specific recruitment criteria. At T2, children presented with varied profiles of language and/or social communication outcomes, confirming the heterogeneity of language and social communication skills and deficits observed in children with specific deficits in language. However, results also highlighted that at this young age language problems frequently co-occurred with social communication impairments.
The main aim of this study was to investigate the performance of LTs on early body movement imitation and language tests as predictors of their later social communication and language outcomes. To the best of our knowledge, no study has previously addressed this specific topic. As hypothesised, early language skills at T1 were predictive of later language outcome and body movement imitation skills at T1 were predictive of later social communication outcome. Findings further revealed that body movement imitation at T1 also contributed significantly to the prediction of language outcome at T2 (i.e. language impairment versus typical language development), whereas language skills at T1 did not contribute significantly to the prediction of social communication outcome at T2 (i.e. social communication impairments versus typical social communication development). Thus, different outcome profiles were associated with different verbal and nonverbal predictor variables. Results highlight the need to theoretically and clinically account for the heterogeneity of different language and communication trajectories in LTs. The current study confirms the need for future studies to look in more depth at specific sociocognitive and nonverbal communication abilities as predictor and outcome variable to understand more about the nature of early sociocognitive and communication problems and putative selective relations to later language and/or communication deficits in children with delayed language emergence, rather than focus exclusively on language skills (Chiat & Roy, 2013; Roy & Chiat, 2014). Outcomes also emphasised the necessity to define and measure sociocognitive and/or nonverbal communication variables with the same precision as one would expect when addressing language skills.
The finding that body movement imitation at T1, as a measure of sociocognitive capacities, is a unique predictor of later social communication outcome is in line with the sociocognitive hypothesis of the mapping theory (Chiat, 2001; Chiat & Roy, 2008) that early sociocognitive difficulties will affect the developmental trajectories of language and social communication. It is also consistent with results reported by Chiat and Roy (2008), who identified a measure of social responsiveness, joint attention and symbolic understanding as predictive of later social communication skills in a sample of toddlers who were referred to speech and language therapy services.
The finding that body movement imitation at T1 contributed to prediction of later language outcome is in line with findings of studies reported in the ‘Introduction’ section, which highlighted early sociocognitive and nonverbal communication behaviours as promising predictors of children’s language trajectories (Pesco & O’Neill, 2012; Thal et al., 1991; Zambrana et al., 2014). It also reinforces the case for multifactorial predictive risk models for later language outcome that consider a range of verbal and nonverbal factors (Desmarais et al., 2008; Ellis & Thal, 2008).
Limitations
In this study, we argue that difficulties with elicited body movement imitation may provide a window onto sociocognitive abilities since nonverbal imitation skills are assumed to rely significantly on sociocognitive abilities (Carpenter et al., 2002; Tomasello & Carpenter, 2005). A limitation is that no additional measures of social cognition were given at T1 (other than body movement imitation) in this study, and thus the body movement imitation’s concurrent validity with other social cognition measures can only be hypothesised. Further, results in this study are based on a rather small sample of participants and accordingly have to be interpreted with caution.
Conclusion
Imitation behaviour is multifaceted and a range of competencies are thought to be involved (Rogers & Williams, 2006). The nature of different imitation acts varies substantially, and not all competencies are necessarily involved in the same way for all types of imitation. The body movement imitation task reported in this paper seems to tap one or more specific competencies which appear to be particularly challenging for a group of children with delayed language emergence and are likely to be linked to skills underlying language and social communication acquisition. These competencies are required for the immediate elicited imitation of body movements in a particular setting. We would not assume children to show the same difficulties in different imitation tasks, e.g. spontaneous body movement imitation in a familiar environment or the imitation of actions on objects. This is supported by our finding of the initial phase of this study at T1 that refusal to imitate action on objects occurred only occasionally in the LT group and no child refused all items of this task (Dohmen et al., 2013). Results show that a large percentage of children in the LT group refused to imitate body movements. Based on the mapping theory, and on empirical evidence from research with typically developing children and children with ASD we argued that difficulties with body movement imitation may be indicative of sociocognitive deficits and that the ability to establish a sense of connectedness with the demonstrator is at the core of the imitation difficulties observed in the LT sample (Dohmen et al., 2013). However, at this stage of research and within the context of this paper it remains speculative what the refusal to comply with our body movement imitation task actually means. In addition, there might be the concern that refusal versus attempt to perform on the body movement imitation measure is a rather macro-level ‘marker’ of social cognition. Future research including independent measures of different sociocognitive skills, levels of anxiety and temperament is needed to bring to light possible explanations for children’s refusal to imitate body movements. This might clarify the finding that body movement imitation was a poor predictor of ‘pure’ language impairment, which was in line with findings on predictiveness of the Early Sociocognitive Battery reported in Roy and Chiat (2014). But despite this need for further research to find out why the body movement imitation task is predictive of children’s later language and communication outcomes, it is important to acknowledge that this measure is predictive. In the future it might therefore have the potential to improve the identification of the subset of pre-schoolers with late language emergence who are at risk to present with clinically significant social communication and language problems when they get older. Poor categorical performance on the body movement imitation task (i.e. refusal to imitate) might help to detect children with later social communication deficits and contribute to the detection of children who are at risk to present with persistent language impairments. In contrast, adequate categorical performance on the body movement imitation task (i.e. attempt to imitate) might serve as one indication for a positive prognosis, since the majority of LTs who attempted body movement imitation at T1 moved into the typical range on social communication and language assessments at T2. The administration of the body movement imitation task is quick, easy and requires no additional material and would therefore be suitable as part of a larger screening tool. In the context of a screening tool, a macro-level task could even be seen as an advantage. However, the need for replicating results of this study with a larger number of participants is emphasised before we find out whether a body movement imitation task has the potential to provide clinicians with additional information about which LTs would benefit from early intervention services.
Footnotes
Acknowledgements
We are extremely grateful to the families who gave generously of their time to make this study possible.
Authors’ contributions
AD designed the study, carried out recruitment and assessment of children, analysed the data, and wrote the first draft of the manuscript. DVMB, SC and PR advised on designing the study, analysing data and writing-up of the manuscript. All authors discussed, read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Economic and Social Research Council (ES/J001961/1) and the Wellcome Trust (082498/Z/07/Z).