
Abstract
Background
There is a paucity of data on trends of osteopathic medical students (OMS) matriculating into surgical specialties since the installation of the single U.S. graduate medical education (GME) accreditation system, which concluded in June 2020. This study examines the impact of major policy changes, particularly the transition of COMLEX Level 1 and USMLE Step 1 to Pass/Fail, on OMS match outcomes, with the goal of guiding current students pursuing surgical careers.
Methods
A systematic literature review was conducted using Rayyan, with bias assessed via the Cochrane risk of bias tool. National Residency Matching Program (NRMP) data from 2016, 2018, 2020, 2022, and 2024 were reviewed to document the number of OMS applicants and post-match statistics. Surgical specialties analyzed included General Surgery, Vascular Surgery, Neurological Surgery, Otolaryngology, and Orthopedic Surgery. NRMP pre-merger data were available for General Surgery, Neurological Surgery, and Orthopedic Surgery; Vascular Surgery and Otolaryngology data were available for 2020 and 2022 only.
Results
COMLEX-USA Level 1/2 and USMLE Step 1/2 scores generally decreased across the ACGME merger, with notable exceptions: Neurological Surgery reported higher COMLEX Level 2-CE scores; Orthopedic Surgery reported higher USMLE Step 2 CK scores; Vascular Surgery reported a higher Step 2 score between 2020 and 2022, though data were limited to a single applicant. Otolaryngology also demonstrated an increase in mean Step 2 scores. General Surgery, Neurological Surgery, and Orthopedic Surgery showed increased mean numbers of abstracts, presentations, and publications, while Vascular Surgery and Otolaryngology showed declines between 2020 and 2022.
Conclusions
The most consistent trend was an increase in research productivity among successful OMS matriculating into General Surgery, Neurological Surgery, and Orthopedic Surgery. While licensing scores generally declined, this may reflect applicant pool expansion post-merger. Ongoing research is needed to evaluate trends beyond 2024, particularly following the implementation of Pass/Fail Step/Level 1.
Introduction
Historically, the majority of osteopathic medical students (OMS) matriculated into primary care residency programs at increasing rates. 1 In 2020 and 2023, DO seniors comprised 20.85% and 22.5% of matched applicants in primary care specialties, respectively. 1 In contrast, from 2018 to 2023, DO seniors only comprised 1.11% to 1.05% of matched applicants into surgical subspecialties, respectively. 1 The Department of Health and Human Services projects there to be workforce shortages in most surgical subspecialties by 2025, specifically in general surgery, urology, orthopedic surgery, and ophthalmology. 2 More than 100 rural hospitals closed within the past decade partially due to loss of surgical services. 3 Consequently, the remaining urban hospitals are becoming burdened with more surgical cases due to the increasing number of patients coming in from neighboring rural and suburban areas. One way to alleviate this burden is to increase the number of osteopathic students matriculating into surgical subspecialties. Interestingly, the 2023 Osteopathic Medical Profession (OMP) Report showed a more than 30% increase in the number of osteopathic physicians in the United States in the past five years. 4 Prior to the creation of the Accreditation Council for Graduate Medical Education (ACGME) in 2020, osteopathic medical students encountered relatively few challenges as residency surgical specialty spots were equally available to both MD and DO students. However, after the inception of the ACGME/AOA merger, residency positions that were previously exclusive for DO graduates now became equally accessible to both MD and DO students, transforming the applicant pool to a more competitive environment due to the inclusion of MD students. 5 As a result, residency programs are now considering additional factors in their selection of prospective residents.
Current literature demonstrates that scoring above average on licensing exams is critical for both allopathic and osteopathic students matching into their first-choice residency and into more competitive specialties. 6 The quantity of research experience, which includes abstracts, presentations, and publications, is important in establishing oneself as a competitive applicant. A study published by Hasley et al indicated that medical students who matched into a highly competitive specialty, neurosurgery, had an average of 5.1 publications and a median of 4.0 publications per resident. 7 In a study regarding osteopathic students matriculating into orthopedic surgery, performance in rotating at a program directors’ (PD) institution, formality/politeness in interview, performance on ethical questions in interview, and COMLEX/USMLE Step 1/Step 2 scores were the top five residency criteria selection criteria. 8 This suggests that medical students applying to surgical subspecialty residency programs must display higher-level licensing exam scores along with research authorship. Using this foundation, we aim to provide a thorough examination of the patterns of osteopathic medical students’ matriculation into surgical special programs.
Through an extensive systematic review, our aim is to provide a comprehensive analysis of trends of matriculation of osteopathic medical students into surgical specialty programs. The findings of this research are intended to facilitate a deeper understanding and serve as foundational evidence for the prevailing trends of osteopathic medical students into non-primary care surgical specialty residency programs. The results can be utilized by prospective and current students, medical educators, physicians, and residency directors to advance diversity, equity, and inclusion initiatives of osteopathic medical students into non-primary care specialties within the medical community.
Methods
This systematic review was conducted in accordance with the PRISMA 2020 guidelines to examine trends in osteopathic medical student matriculation into surgical subspecialties following the ACGME/AOA merger and the transition of USMLE Step 1 and COMLEX Level 1 to Pass/Fail.
Data Sources and Study Design
Two data sources were used: (1) peer-reviewed literature and (2) publicly available National Residency Matching Program (NRMP) applicant-level data. NRMP data from the 2016, 2018, 2020, 2022, and 2024 Main Residency Match cycles were analyzed to document osteopathic senior applicant characteristics and post-match outcomes. Surgical specialties examined included General Surgery, Vascular Surgery, Neurological Surgery, Otolaryngology, and Orthopedic Surgery. Pre-merger NRMP data were available for General Surgery, Neurological Surgery, and Orthopedic Surgery, whereas Vascular Surgery and Otolaryngology data were available for 2020 and 2022 only.
Because all data were obtained from publicly available sources, Institutional Review Board approval and informed consent were not required, and no external funding was received.
Search Strategy
A comprehensive literature search was conducted in PubMed/MEDLINE, Embase, Web of Science, and Scopus to identify studies evaluating osteopathic medical students or physicians in relation to surgical specialties, internship and residency training, and residency match outcomes. Searches included articles published between January 1, 2012 and December 31, 2022. The final search was completed on December 31, 2022.
In PubMed, Medical Subject Headings (MeSH) and free-text keywords were combined. The full strategy was: (“specialties”[MeSH Terms] OR “surgical”[MeSH Terms] OR “specialties”[All Fields] OR “surgical”[All Fields]) AND (“internship”[MeSH Terms] OR “residency”[MeSH Terms] OR “internship”[All Fields] OR “residency”[All Fields] OR “residency program”[All Fields]) AND (“osteopathic students”[MeSH Terms] OR “osteopathic medicine”[MeSH Terms] OR “osteopathic physician”[MeSH Terms] OR “osteopathic”[All Fields] OR “DO”[All Fields] OR “osteopathic medical student”[All Fields]), limited to English-language publications from 2012 to 2022.
In Embase, exploded Emtree terms were used: (“osteopathic students”/exp OR “osteopathic medicine”/exp OR “osteopathic physician”/exp OR “osteopathic medical student”/exp OR “osteopathic”/exp OR “DO”/exp) AND (“residency match”/exp OR “match process”/exp OR “residency matching”/exp OR “residency placement”/exp) AND (“surgical specialties”/exp OR “specialties”/exp OR “surgical”/exp OR “internship”/exp OR “residency”/exp).
In Web of Science and Scopus, analogous keyword-based strategies were used, with Scopus restricted to publications after 2012. The study selection process is summarized in the PRISMA flow diagram (Figure 1).

PRISMA flow chart.
Eligibility Criteria
Studies were eligible for inclusion if they were peer-reviewed, published in English, and reported outcomes related to osteopathic medical students or physicians in surgical specialties, including residency match trends, licensing examination performance, or research productivity. Studies were excluded if they were editorials, commentaries, non-English publications, not specific to osteopathic applicants, or lacked relevant outcome data.
Study Selection
All records were imported into Rayyan for de-duplication and screening. Two reviewers independently screened titles and abstracts, followed by full-text review for eligibility. Disagreements were resolved by consensus. A total of 695 records were identified, 17 underwent full-text review, and 13 were included in the qualitative synthesis.
Data Extraction
Two reviewers independently extracted data from each included study. Extracted variables included study year, study design, surgical specialty, applicant characteristics, board score reporting, research productivity, and match outcomes. When data were unclear, original publications were reviewed for clarification.
Outcomes and Variables
The primary outcomes of interest were licensing examination performance (COMLEX and USMLE), research productivity (abstracts, presentations, publications, and research experiences), and residency match outcomes. Additional variables included surgical specialty, match cycle year, and study design. All reported values compatible with these outcome domains were collected.
Risk of Bias Assessment
Risk of bias was assessed using the Cochrane Risk of Bias Tool. Two reviewers independently evaluated each included study, with disagreements resolved by consensus. Results are summarized in Figure 2.

Risk of bias criteria.
Data Synthesis and Statistical Analysis
This study was not registered with PROSPERO or INPLASY because it analyzed publicly available NRMP data and retrospective literature to describe educational and workforce trends. NRMP and literature-derived data were summarized using descriptive statistics, including means, counts, and percentages. Data were grouped by surgical specialty and match cycle (pre-merger vs post-merger) to evaluate trends following the ACGME/AOA merger and the transition to Pass/Fail licensing. No meta-analysis, heterogeneity assessment, sensitivity analysis, or certainty grading was performed due to study design heterogeneity and the descriptive nature of available data.
Results
Literature Review Data
Seven of the nine authors (78%) considered the United States Medical Licensing Exam (USMLE) Step 1 “significantly important” for matching into residency subspecialties (Table 1).6,8-14 Heard 2022 reported in their study that residency programs recommended DO applicants to take the USMLE Step 1 exam in order to be considered “equal” to their allopathic counterparts. 11 Moreover, 67% of studies stated that taking the USMLE Step 2 CK exam may increase competitiveness to match residency subspecialties (Table 1).6,8,10-14 Regarding numerical values to target, Mitsouras 2019 reported that 53.9% of graduates matched into their first choice residency program had a mean USMLE Step 2 CK score of 228.1 points. 6 Stobart-Gallagher 2019 recommended test-takers to score above 240 points to match into emergency medicine, following the single accreditation system in 2020. 12
Main Characteristics of Studies Included in the Systematic Review.

Match Statistics Trends from NRMP Data upon STEP/LEVEL 1 Becoming Pass/Fail
DO Seniors that matriculated into General Surgery, Orthopedic Surgery, and Otolaryngology had a higher research volume compared to matriculants from previous years. General surgery residents had a high mean number of abstracts, presentations, and publications (6.9) post-merger compared to pre-merger in 2022 at 4.6. Similarly, the mean number of research experiences was higher for general surgery residents in 2024 compared to 2022 at 3.5 and 3, respectively (Table 2f). Orthopedic surgery residents followed this same trend. Post-merger, the mean number of abstracts, presentations, and publications post-merger (2024) for orthopedic surgery was 11.2, compared to 7 pre-merger (2022). The mean number of research experiences post-merger was 5.1, compared to 4 pre-merger (2022) Table 2h). Otolaryngology residents had a mean number of abstracts, presentations, and publications of 11.3 post-merger (2024), which was higher than the pre-merger at 8.5 (2022). Interestingly, the mean number of research experiences for otolaryngology post-merger was 4.5, decreased from the pre-merger of 11.2 (2022) (Table 2j).
Board Scores and Research.
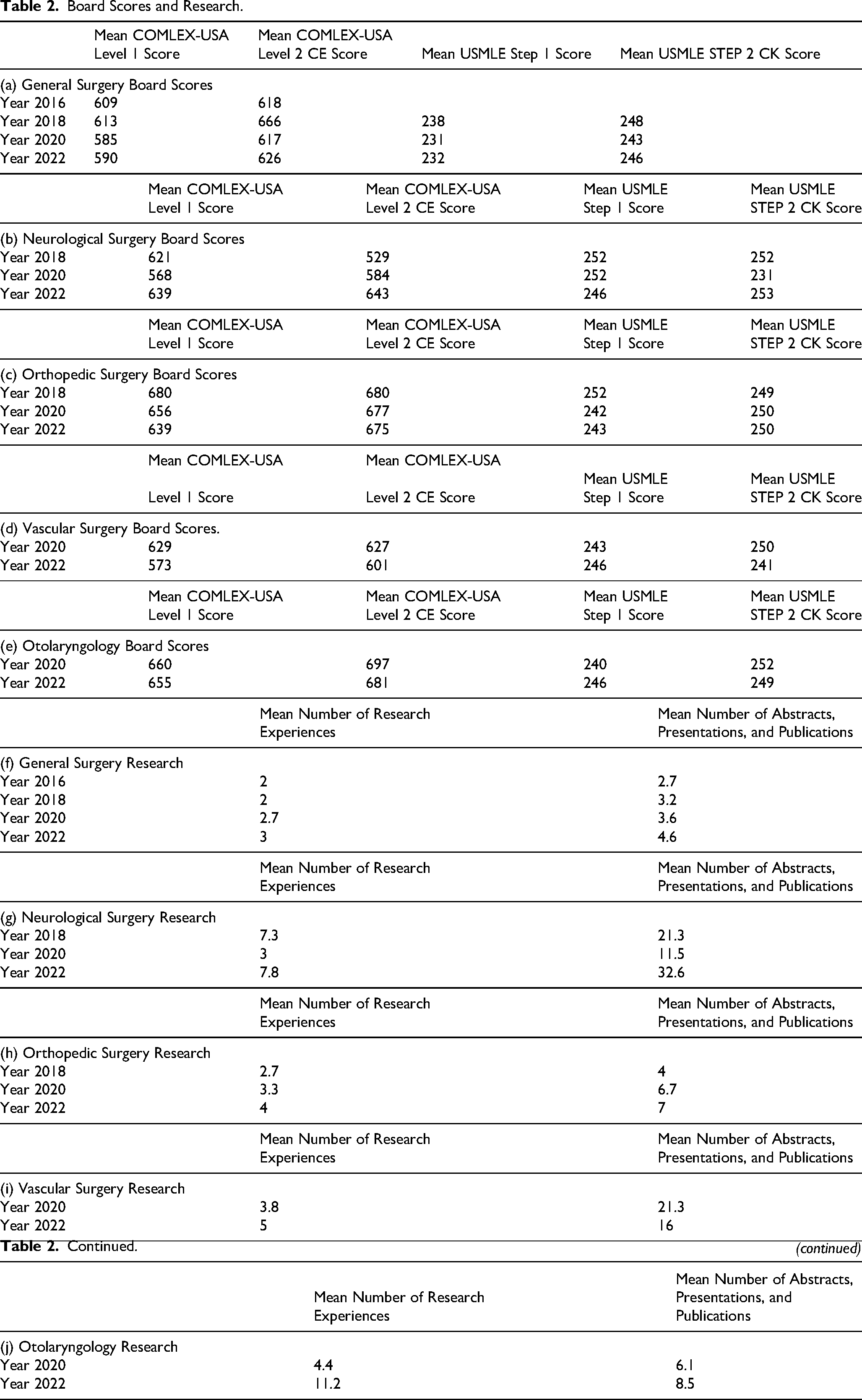
DO seniors that matriculated into neurological surgery and vascular surgery residency programs had a lower research volume compared to matriculants from previous years. Vascular surgery residents had a mean number of abstracts, presentations, and publications of 9 post-merger (2024), decreased from 15 in the pre-merger (2022). Similarly, the mean number of research experiences was 2.8 post-merger (2024), decreased from pre-merger at 5 (2022) (Table 2i). Incoming neurological surgery residents also displayed lower research volume. The mean number of abstracts, presentations, and publications post-merger was 23 (2024), lower than incoming neurological surgery residents had pre-merger at 32.6 (2022). Similarly, the mean number of research experiences post-merger for neurological surgery residents was 4 post-merger (2024), decreased from 7.8 pre-merger (2022) (Table 2g).
Match Statistic Trends from NRMP Pre-ACGME Merger (2016/2018) and Post-ACGME Merger (2020/2022) Were Analyzed
NRMP match statistics across the ACGME merger (2016-2018 to 2020-2022) reported a decrease in scores for the COMLEX Level 1 for General surgery, Neurosurgery, and Orthopedic surgery, Vascular surgery, and Otolaryngology (Table 2a-e).15-18 There was a decrease in COMLEX Level 2-CE scores post-merger for General surgery, Orthopedic surgery, Vascular surgery, and Otolaryngology; while there was an increase post-merger for Neurological surgery (Table 2a, c, d, e, and i).15-18 There was a decrease in USMLE Step 1 exam scores for General surgery, Neurological surgery, and Orthopedic surgery (2.a, 2.c, and 2.e).15-18 There was an increase in USMLE Step 1 exam scores from 2020 to 2022 for Vascular surgery and Otolaryngology (Table 2b and d).15-18 There was a decrease in USMLE Step 2 CK exam scores for General surgery, Neurological surgery, Vascular surgery, and Otolaryngology (Table 2a-d).15-18 There was an increase in USMLE Step 2 CK score for Orthopedic surgery across the ACGME merger (Table 2d).15-18 Finally, the mean number of abstracts, presentations, and publications increased across the ACGME merger for General surgery, Neurological surgery, and Orthopedic surgery (Table 2f-h).15-18 From 2020 to 2022, the mean number of abstracts, presentations, and publications decreased for vascular surgery and otolaryngology (Table 2g and h).15-18
ACGME Merger Effect on Matriculation (NRMP DATA)
Following the ACGME merger, the mean COMLEX-USA Level 1 score decreased for General surgery, Neurological surgery, Orthopedic surgery, Vascular surgery, and Otolaryngology (Table 2a-e).15-18 From 2016 to 2018, the mean score for General surgery was 611 points for successful matriculants (Figure 3a).15-18 From 2020 to 2022, the mean score for General surgery was 587.5 points (Figure 3a).15-18 This is almost a 4% decrease from the pre-ACGME merger NRMP data. The stark increase in number of students applying to surgical specialties across the merger may account for the variability in scores. In 2016 and 2018, 100 and 121 DO applicants participated in the ACGME match, respectively.15-18 Whereas in 2020 and 2022, there were 254 and 264 DO applicants post-ACGME merger.15-18 In 2018, the mean score for Neurological surgery was 621 points with three successful matriculants (Figure 3b).15-18 In 2020, two DO applicants matched with a mean score of 568 points (Figure 3b).15-18 In 2022, nine matriculants had a mean score of 639 points (Figure 3b).15-18 Therefore, while there was a decrease in mean scores, this does not account for the fact that there was an increased number of neurosurgical applicants. For Orthopedic surgery, the mean COMLEX-Level 1 score was 680 points with four matriculants (Figure 3c).15-18 From 2020 to 2022, the mean scores for Vascular surgery were 629 and 573 points, respectively (Figure 3d).15-18 The mean scores for Otolaryngology also decreased from 660 points in 2020 to 655 points in 2022 (Figure 3e).15-18

Board score and research trends.
Neurological surgery matriculants had a 16% increase in COMLEX-LEVEL 2 exam scores across the ACGME merger while mean scores decreased for General surgery, Orthopedic surgery, Vascular surgery, and Otolaryngology (Figure 3a-e).15-18 Pre-merger, Neurological surgery matriculants had a mean score of 529 points while post-merger, the mean score was 613.5 points which is a 16% increase (Figure 3b).15-18 For General surgery, the mean score pre-merger was 642 points while the mean score post-merger was 621.5 points which was a 3% decrease (Figure 3a).15-18 For Orthopedic surgery, the pre-merger score was 680 points for successful matriculants, and the post-merger mean score was 676 points which was a 0.6% decrease (Figure 3c).15-18 For Vascular surgery matriculants, there was a 4% decrease in scores from 627 in 2020 to 601 in 2022 (Figure 3d).15--18 ENT matriculants also had a 2.3% decrease from 697 in 2020 to 681 in 2022 (Figure 3e).15-18
Regarding USMLE Step 1 exam scores, General surgery, Neurological surgery, and Orthopedic surgery, matriculants reported a decrease across the ACGME merger (Figure 3a-c).15-18 For General surgery, there was a 3% decrease in scores from 238 points pre-merger to 231.5 points post-merger (Figure 3a).15-18
Neurological surgery matriculants reported a 1% decrease in mean USMLE Step 1 exam scores from 252 points pre-merger to 249 points post-merger (Figure 3b).15-18 Orthopedic surgery matriculants reported a 3.7% decrease in USMLE Step 1 exam scores across the ACGME merger from 252 points pre-merger to 242.5 points post-merger (Figure 3c).15-18 In contrast, Vascular surgery and Otolaryngology matriculants reported an increase in board scores from 2020 to 2022. In 2020, the mean USMLE Step 1 score for vascular surgery and Otolaryngology were 243 and 240 points, respectively (Figure 3d and e).15-18 The mean score in 2022 was 246 points for both surgical subspecialties (Figure 3d and e).15-18
General surgery, Neurological surgery, Vascular surgery, and Otolaryngology reported a decrease in USMLE Step 2 CK scores from 2018 to 2022 while Orthopedic surgery matriculants reported an increase in USMLE Step 2 CK scores (Figure 3a-e).15-18 Orthopedic surgery matriculants reported a 0.4% increase in board scores from 249 points in 2018 to 250 points post-merger (Figure 3c).15-18 General surgery saw a 1.4% decrease from 248 pre-merger to 244.5 points post-merger (Figure 3a).15-18 Neurological surgery matriculants reported a 7.5% decrease from 252 points pre-merger to 242 points post-merger (Figure 3b).15-18 Though, this might be a skewed result since only two matriculants matched in 2020 with an average score of 231 points while nine students matched in 2022 with a mean USMLE Step 2 CK score of 253 points (Figure 3b).15-18 In 2020, Vascular surgery matriculants reported a mean score of 250 points compared to a mean score of 241 points in 2022 (Figure 3d).15-18 In 2020, Otolaryngology matriculants reported a mean score of 252 points in 2020 compared to a mean score of 249 points in 2022 (Figure 3e).15-18
Across the ACGME merger, the mean number of abstracts, presentations, and publications increased for those that matched into General surgery, Neurological surgery, and Orthopedic surgery (Figure 3f-h).15-18 Vascular surgery and otolaryngology matriculants reported a decrease in the mean number of abstracts, presentations, and publications from 2020 to 2022 (Figure 3i and j).15-18 General surgery matriculants reported a 39% increase across the ACGME merger with a mean number of 4.1 research experiences post-merger (Figure 3f).15-18 Neurological surgery matriculants reported a 3.5% increase across the ACGME merger with a mean number of 22 research experiences post-merger (Figure 3g).15-18 Orthopedic surgery matriculants reported a 71.3% increase across the ACGME merger with a mean number of 6.85 research experiences post-merger (Figure 3h).15-18 Finally, while Vascular surgery saw a decline in the number of abstracts, presentations and publications from 2020 to 2022, this could be due to the fact that there was only one person who matched in 2022 (Figure 3i).15-18 In 2020, Vascular surgery matriculants reported a mean number of 21.3 abstracts, presentations and publications while in 2022, there was a mean number of 16 (Figure 3g).15-18 Otolaryngology matriculants reported a mean number of 11.2 research experiences in 2020 and 8.5 research experiences in 2022 (Figure 3j).15-18
Discussion
Research Volume
Following the ACGME/AOA merger, DO seniors who matched into General surgery, Neurological surgery, and Orthopedic surgery obtained a higher number of abstracts, presentations, and publications (Figure 3f-h).15-18 Based on match statistics data from 2016 and 2018, Matthews et al posits that for allopathic students, there is a statistically significant interaction between match success and the number of research accomplishments. 19 In contrast, there was no statistically significant interaction between being a DO student and matching success. 19 Notably, this research pertains to all specialties and is not specific for surgical subspecialties.
The merger provided more surgical residency positions for DO students. In 2018, 268 AOA positions were explicitly available for DO seniors in the following surgical specialties: General surgery, Neurological surgery, Orthopedic surgery, and Otolaryngology. 1 By 2023, there were a total of 3535 positions for DO and MD seniors made possible with the ACGME-AOA merger. 1 But even with increased availability, MD seniors occupied the majority of these positions. For example, from 2020 to 2023, match rates were higher for MDs than DOs in neurosurgery, thoracic surgery, plastic surgery, general surgery, vascular surgery, ENT, and orthopedics. 1 Although the ACGME/AOA merger ultimately increased the total number of residency positions available, the proportion of DO students matching into competitive surgical subspecialties decreased due to a larger applicant pool and greater competition from MD graduates, highlighting that increased positions do not necessarily translate to higher relative match rates for DO students.
Because research volume serves a significant role in match success for allopathic seniors, it is unsurprising that there is an increase in research volume for DO seniors across the ACGME merger who are matching into historically MD-dominant surgical subspecialties. 1 Therefore, it is highly advised that DO seniors who are applying to surgical specialties obtain research experiences in order to be considered competitive. Future research should be done to determine if there are statistically significant interactions between being a DO student, research volume, and matching into surgical subspecialties across the ACGME merger, especially given the growing number of positions in surgical subspecialties.
Research Volume After COMLEX and STEP Became Pass/Fail
The change to COMLEX Level 1 and USMLE Step 1 Pass/Fail system led to notable differences in how medical students demonstrate their competitiveness to residency subspecialties. General surgery, Orthopedic surgery, and Otolaryngology saw an increase in research volume in applicants. 20 Previously, COMLEX Level 1 and USMLE Step 1 scores carried significant weight in an applicant's level of competitiveness. With the advent of the Pass/Fail system, students must highlight other characteristics that differentiate themselves from their peers. This change is reflected in the higher research volume among DO Seniors who matriculated into General Surgery, Orthopedic Surgery, and Otolaryngology specialties compared to matriculants from previous years. This shift further suggests that applicants continue to place great emphasis on academic and scholarly achievements to strengthen their residency applications.
Board Scores
We hypothesized that COMLEX Level 2-CE and USMLE Step 2 CK scores would increase post-merger due to increased competitiveness with their allopathic counterparts. However, due to the bigger pool of applicants, it may be unsurprising that the standardized scores were only a few points lower post-merger for General surgery, Neurological surgery, and Orthopedic surgery with some fluctuations (Figure 3f-h).15-18 The major takeaway is there seems to be an ideal range that DO students should prepare for when sitting for their licensing examinations as seen in Figure 3.15-18 Therefore, while there is technically a minimal drop in points across the merger, there seems to be a rough estimate for “good numbers to hit” for a specific surgical specialty. Therefore, DO students should aim for these numbers when sitting for their licensing examinations.
Implications for Advising and Education
These findings have practical implications for advising osteopathic medical students interested in surgical subspecialties. Early exposure and advising during the first and second years of medical school may be particularly important in the post-Pass/Fail era, as students may need additional time to pursue research opportunities, build scholarly portfolios, and identify mentors within competitive surgical fields. Longitudinal mentorship, including guidance on research engagement, audition rotations, and application strategy, may help osteopathic students remain competitive following the transition to Pass/Fail licensing examinations. At an institutional level, targeted support structures such as protected research time, access to surgical faculty mentors, and transparent advising resources may further facilitate osteopathic student matriculation into surgical subspecialties.
Limitations of This Study
Limitations were that the literature search included language restrictions to only English articles. Additionally, various methodologies were utilized in studies meeting criteria and so the relationship of sample size and efficacy was not able to be successfully analyzed. Additionally, these are self-reported data. Several surgical subspecialties included in this analysis were characterized by small numbers of osteopathic matriculants in individual match cycles, particularly Vascular Surgery and Otolaryngology. In these specialties, year-to-year fluctuations in applicant counts may disproportionately influence mean values for licensing examination scores and research productivity, thereby limiting external validity. As a result, observed post-merger trends for these subspecialties should be interpreted cautiously and viewed as descriptive rather than representative of broader longitudinal patterns. In addition, this study did not include direct degree-matched comparisons between DO and MD applicants within the same surgical subspecialties. The absence of direct DO-MD comparative analyses limits contextual interpretation of relative competitiveness, board score expectations, and research productivity across degree pathways. In addition, while our study highlights research productivity as a factor in residency selection, the data available do not allow us to examine whether greater research output correlates with higher licensing exam scores, stronger residency evaluations, or long-term academic and scholarly success; an important area for future investigation.
Conclusion
Successful DO matriculants should possess key attributes, such as strong licensing examination scores and research experience. From 2018 to 2020, DOs matching into surgical specialties decreased by 3%, yet the osteopathic profession remains vital in meeting hospitals’ surgical demands. Advocacy and matriculation trend analysis can support DO applicants in securing surgical careers. Research volume increased across General Surgery, Neurological Surgery, and Orthopedic Surgery, aligning with trends among allopathic applicants. While licensing scores generally declined, this may reflect the larger applicant pool following the ACGME/AOA merger. Program directors emphasize the importance of audition rotation performance for surgical residency success. These findings underscore the importance of early, structured advising and longitudinal mentorship for osteopathic students pursuing surgical subspecialties, particularly in the post-Pass/Fail era. Institutional investment in research infrastructure and specialty-specific advising may further support osteopathic students navigating an increasingly competitive surgical match environment. Future studies should explore trends beyond 2022, considering the ACGME merger and the shift to Pass/Fail Level/Step 1 exams.
Supplemental Material
sj-docx-1-mde-10.1177_23821205261443551 - Supplemental material for Osteopathic Student Matriculation Trends in Surgical Subspecialties (2016-2024): A Systematic Review
Supplemental material, sj-docx-1-mde-10.1177_23821205261443551 for Osteopathic Student Matriculation Trends in Surgical Subspecialties (2016-2024): A Systematic Review by Bridgette Kielhack, Selena K. Cholak, Virgil K. DeMario, Vaishnavi J. Patel, Devki Patel, Kimberly Toumazos, Mark Quiring, Young Son and John Etlinger in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to thank the National Residency Matching Program (NRMP) for providing the publicly available match data, which was critical for conducting this analysis. We are grateful to Jefferson Health New Jersey for their support in this study.
Ethical Considerations
This study is a systematic review of previously published literature and does not involve human participants, identifiable private information, or intervention with living subjects. Therefore, it is exempt from Institutional Review Board (IRB) approval. All data analyzed in this review were obtained from publicly available sources in accordance with ethical research guidelines.
Consent to Participate
Not applicable. This study did not involve human participants, human data, or human tissue, and therefore no informed consent was required.
Consent for Publication
Not applicable. This manuscript does not contain data from any individual person, including images or videos, that would require consent for publication.
Author Contributions
B.K. and S.K.C. contributed to study conception and design, literature search and screening, data extraction, manuscript drafting, and manuscript revision. V.K.D. and V.J.P. contributed to data analysis, interpretation of results, and manuscript drafting and revision. D.P. and K.T. contributed to manuscript drafting and critical revision for important intellectual content. M.Q., Y.S., and J.E. provided subject matter expertise, supervised the study, and contributed to critical manuscript revision. All authors reviewed and approved the final manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data analyzed in this study were obtained from publicly available sources, including the National Residency Matching Program (NRMP) website and published literature. No new datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.