
Abstract
Background
This feasibility study explored the implementation of the diagnostic teaching feedback tool over a ten-day period in an undergraduate physiotherapy course at the Bern University of Applied Sciences. The main goal was to evaluate how feasible it is to incorporate the tool and its ability to facilitate short-term instructional development aligned with learner-oriented instruction (LOI).
Method
One course instructor, one external observer, and a cohort of physiotherapy students participated. Data were collected twice using questionnaires completed by students, the lecturer (self-evaluation), and the observer, enabling multi-perspective comparison.
Results
Feasibility was partially achieved: the tool was administered and analyzed within the planned timeframe, but student acceptance was below targets (attrition 17%, adherence 83%). Regression analyses revealed only small to moderate associations between teaching dimensions and Objective Structured Clinical Evaluation performance, and no clear evidence of LOI enhancement.
Conclusion
Discrepancies between perspectives and low engagement highlight the need for motivational strategies, structured reflection, and observer training. Future research should utilize larger samples, randomized designs, and supplementary assessments to evaluate effectiveness.
Introduction
Teaching quality is widely recognized as one of the most influential school-related factors in enhancing student achievement, ranking second only after family background in determining student learning outcomes. 1 High-quality teaching is both responsive and reflective, adapting to students’ learning processes and individual styles while fostering independence and autonomy. 2 In higher education, teaching quality is a key driver of student success and institutional effectiveness, encompassing instructional clarity, engagement, and responsiveness to diverse learner needs. 3 To ensure comprehensive assessment, evaluation systems increasingly integrate student evaluations, peer reviews, and learning analytics. 4 However, concerns about the validity and impact of student evaluations of teaching (SETs) persist, 5 prompting calls for multi-perspective approaches that combine outcome-based education (OBE) and reflective practice.
Despite these developments, traditional pedagogical methods, often characterized by teacher-centered instruction (TCI), continue to dominate in many higher education contexts, including physiotherapy education. 6 TCI prioritizes content transmission and passive reception, which can foster surface learning and impede the development of deep learning. In contrast, learner-oriented instruction (LOI) emphasizes active engagement, autonomy, metacognitive skills, and constructive alignment, enabling students to take greater responsibility for their learning.7,8 Although LOI strategies such as flipped classrooms have gained popularity, their adoption in physiotherapy programs remains limited.9,10
The Bern University of Applied Sciences (BFH) operates under a mandate from the Bernese Cantonal Government (2017-2020) to offer research-based, practice-oriented programs and prioritize systematic quality development in teaching (Bern, 2016). The Diagnostic Teaching Feedback (DTF) instrument currently used at BFH primarily serves summative purposes, such as quality assurance and institutional reporting. However, its potential for learning promotion depends on whether results are integrated into formative feedback loops that inform teaching adjustments. While semester examinations provide an indication of students’ learning outcomes, they do not directly measure the quality of learning support. Therefore, additional instruments are necessary to measure dimensions of autonomy, interaction, and engagement that support LOI principles.
Measuring the effectiveness of LOI typically involves student self-reports, classroom observation, and learning-oriented assessments that incorporate peer and self-evaluation.11,12 Rubrics assessing autonomy and interaction further support the shift toward active student-centered learning environments. 13 One promising tool for evaluating and improving classroom instruction is the DTF instrument, originally developed for secondary education and later adapted for higher education. 14 The DTF provides structured, evidence-based feedback from multiple perspectives, including students, colleagues, and self-assessments, with the aim of fostering reflective teaching practices and supporting learning-oriented instruction.
However, empirical evidence on the effectiveness of the DTF in promoting LOI within physiotherapy education is scarce. This gap is particularly relevant given the growing emphasis on active learning in health professions education. To address this issue, the present study explores the feasibility of implementing the DTF in an undergraduate physiotherapy program at the BFH-SHP. Specifically, it examines whether structured, multi-perspective feedback can support improvements in TCI and encourage LOI principles such as autonomy, engagement, and metacognitive development.
Building on this rationale, the primary aim of this feasibility study was to evaluate the practicality of integrating the DTF tool and its potential to foster short-term instructional development aligned with LOI within the BFH undergraduate PT education. A secondary goal was to examine early indications of effect sizes associated with its implementation, offering an initial understanding of its pedagogical influence. Guided by these aims, the central research question was: ‘What impact does the DTF have on instructional development and learning processes when applied twice within ten days?’. To address this overarching question, sub-questions examined whether the DTF could be implemented as intended, whether its application led to observable changes in teaching quality, and whether specific dimensions of the DTF were associated with student performance. Together, these questions provide a foundation for understanding both the practical and educational implications of the DTF in physiotherapy education.
This study was designed as a feasibility investigation due to its exploratory nature and the involvement of two lecturers, two sessions, and a single student cohort. While these parameters limit generalizability, they are appropriate for assessing implementation processes and identifying practical considerations prior to larger-scale trials. The primary aim was to determine whether the DTF can be integrated into physiotherapy education and whether short-term changes in teaching practice emerge when feedback is provided twice within a 10-day period. By focusing on feasibility rather than definitive outcomes, this study offers preliminary insights that can inform future research on evidence-based strategies to enhance teaching quality in health professions education.
Methods
Study Design
This research was designed as a prospective, single-arm, non-randomized feasibility study using a quasi-experimental pre–post approach. This feasibility study was conducted in the spring semester of 2018 at the School of Physiotherapy, BFH-SHP (Switzerland). Reporting followed the GREET guidelines for educational interventions. 15 A clinical trial registration number was not applicable because this study did not involve patient interventions or clinical outcomes; it was a feasibility study conducted in a higher education setting focusing on instructional development rather than clinical treatment.
The DTF method evaluates teaching quality through three complementary perspectives: (i) students’ feedback, (ii) lecturer self-assessment, and (iii) peer observation. All perspectives use the standardized questionnaire t comprising five dimensions of instructional quality: (1) classroom management (CM) (with five items), (2) learning-friendly atmosphere and motivation (with six items) (3) clarity and structuring (ST) (with five items), (4) activation (with six items) and (5) lesson outcomes (with five items). 16 Each item is rated on a 4-point Likert scale (1 = strongly disagree to 4 = strongly agree, neutral point at 2.5). 17
Study Flow
This study was structured into five distinct phases to evaluate the impact of DTF on the quality of TCI in undergraduate physiotherapy education (see Figure 1).

Structured overview of the feasibility study and different phases.
Phase 1 involved recruitment and an initial information session, during which the study's objectives and inclusion criteria were explained to participating students. Prior to the intervention, the DTF diagnostic questionnaires were reviewed in detail with the students and the two participating higher education lecturers, the course instructor and an external observer to ensure clarity and consistency in understanding.
Phase 2 focused on the preparation and delivery of the first TCI session. Learning objectives and teaching materials were provided to students via a learning platform (Moodle). The first TCI session, lasting 90 min, was conducted in a lecture hall. Immediately following the session, the quality of instruction was assessed using the DTF from three perspectives: students (via an online survey open for three days), the course instructor (through self-assessment), and the external observer (manual evaluation conducted during the session).
Phase 3 involved analyzing feedback from the first session. The results were reviewed from all three perspectives to identify strengths and areas for improvement. These insights informed us of the planning of the second TCI session.
Phase 4 consisted of executing the second 90-min TCI session, incorporating revised learning objectives and didactic strategies based on previous feedback. The same DTF-based evaluation process was repeated.
Phase 5 focused on the final analysis of the second session's evaluations. The collected data were utilized to assess changes in instructional quality and the extent to which the revised TCI encouraged active and self-directed learning.
Participants
This study involved 53 undergraduate physiotherapy students (42 women and 11 men) in their second semester enrolled in the ‘Musculoskeletal System 1’ module. This module covers the theoretical fundamentals of musculoskeletal diseases, as well as the causes and mechanisms of inflammatory and degenerative processes in the lower limb and spine, including related examination and treatment techniques. The following TCI lectures took place during the module: six in anatomy, two in biomechanics, and two in physiology. Two anatomy TCI units were selected for evaluation. The volunteering anatomy teacher (course instructor) and the visiting teacher (external observer) both had over 19 years of academic teaching experience. All participants were orally informed in advance and provided written informed consent.
Inclusion and Exclusion Criteria
Participants were eligible for the study if they met the following criteria:
Undergraduate physiotherapy students enrolled in the second semester of the ‘Musculoskeletal System 1’ module at BFH-SHP in the spring semester of 2018. Attendance in the two selected TC anatomy sessions included in the study. Ability to complete the online DTF questionnaire within the defined survey time window (3 days). Provision of written informed consent to participate in the study. Higher education lecturer and peer observer with minimum professional experience in teaching (15 + years in your study), willingness to participate, and ability to complete the DTF self- or peer-evaluation.
Participants were excluded if any of the following applied:
Students not enrolled in the second-semester physiotherapy course (e.g., students from other cohorts). Students who did not attend one or both of the selected TCI sessions. Students who did not complete the DTF questionnaire within the defined response window. Students or faculty who declined or did not provide written informed consent. Individuals not involved in the selected teaching sessions, that is, external students or lecturers who were not part of the two anatomy TCI units.
Primary Outcome: Feasibility
The a priori set criteria of success were aligned with the main feasibility objective and included recruitment rates, student acceptance, preparation time for the second TCI lesson, as well as the completeness of data collection and analysis (Table 1). Recruitment was successful, with 53 s-semester physiotherapy students enrolled in the ‘Musculoskeletal System 1’ module. Student acceptance was evaluated using attrition and adherence rates. The attrition rate was calculated by comparing the number of students who participated in the first evaluation phase with those who completed the second evaluation phase. Adherence was calculated using the formula proposed by Rogan et al., 18 which takes into account the actual number of completed survey days in relation to the maximum possible number of survey days. For this study, the actual number of survey days was 88 (44 students multiplied by two survey days), while the maximum possible number was 106 (53 students multiplied by two survey days). These indicators provided insight into the practicality of implementing the DTF within the physiotherapy curriculum.
Measurement Method and Target Parameter of the Primary Outcome.

Secondary Outcome
Instructional Quality
The secondary outcome assessed the potential effect size of the DTF on the quality of TCI. The DTF, created within a German educational project funded by the Standing Conference of the Ministers of Education and Cultural Affairs, is based on constructivist learning theory. It aims to enhance instructors’ diagnostic competencies and responsiveness to classroom heterogeneity, thereby supporting a shift from content-centered to student-centered teaching. Constructivist approaches emphasize active knowledge construction by learners, making the DTF particularly relevant for higher education settings.
All ratings were entered into the DTF Excel-based application, Version 6.0, 19 which generated visual comparative profiles across the three perspectives. The tool is intended for visualization, formative interpretation, and identification of strengths and opportunities for improvement rather than inferential statistics testing. Analyses explored whether structured, multi-perspective feedback could foster more responsive and reflective teaching practices aligned with constructivist, LOI principles.
Screening and Diagnostic Approach
The initial step involves screening for strengths and weaknesses in teaching practice. This diagnostic assessment forms the basis for planning two key areas:
Professional development measures (e.g., targeted training or in-depth information), and Further development of teaching strategies and instructional design.
Repeated Measurement and Development Tracking
Repeated application of teaching diagnostics enables monitoring of instructional development over time. The DTF plays a dual role by supporting both individual teaching improvement and broader school development initiatives. Central to the DTF approach are mutual classroom visits, which foster collaborative reflection and professional growth. Tandem formation between lecturers promotes peer learning and continuous professional development.
Interpretation and Evidence-Based Action
Interpretation of results relies on visual changes in the profile curve generated by DTF. The first measurement represents the baseline inventory, providing a starting point for evidence-based interventions. Following this first analysis, targeted measures are implemented to address identified weaknesses and reinforce strengths. The second measurement visualizes changes and informs the evaluation of implemented strategies.
Desired Outcomes and Possible Patterns
Expected outcomes included:
Positive changes in areas initially rated unfavorably (<2), and Stability in areas that were already strong (>3.5) at baseline.
Other possible patterns included stagnation, general improvement or decline, area-specific changes, and trade-offs where improvement in one domain coincides with deterioration in another. These patterns are documented and analyzed to guide iterative refinement of teaching practices.
Figure Interpretation
Figure 2a and b visualizes the five DTF dimensions of teaching quality: classroom management, learning-fostering atmosphere, clarity and structuring, activation, and lesson outcome. Each cluster of columns represents these dimensions across three perspectives: students, course instructor, and external observer. Column height reflects mean ratings on the 4-point Likert scale. Two measurement points (Sessions 1 and 2) allow comparison over time. Discrepancies within clusters indicate perceptual differences among stakeholders, while changes between sessions illustrate potential effects of feedback and instructional adjustments. Error bars show standard deviations, highlighting variability within each group. These visual profiles serve as diagnostic tools for identifying strengths, weaknesses, and development patterns rather than for inferential statistical testing.

DTF data sheet analysis. (a) DTF sheet 1. (b) DTF sheet 2.
Learning Process of Undergraduate Physiotherapy Students
At the end of each semester, undergraduate physiotherapy students at BFH-SHP sit for a written examination and a practical assessment using the Objective Structured Clinical Evaluation (OSCE). For this feasibility study, the grades from the written and OSCE examinations in the first semester were used to provide a statistical overview of the learning progression within the cohort PHY17. In the literature, grades are frequently used as indicators of academic achievement and learning success due to their reliable prognostic validity and ease of access. 20
Analysis of the Data
Descriptive statistics (means, standard deviations, medians, interquartile ranges) were calculated for all five dimensions of the DTF questionnaire across three perspectives: students, lecturer, and peer observer. Although the DTF questionnaire uses a four-point Likert-type scale, it was treated as quasi-metric, assuming equal intervals between response options. 21 The scale is bipolar, ranging from 1 (‘I fully disagree’) to 4 (‘I fully agree’), with a theoretical neutrality point at 2.5.
Statistical Analysis
To assess changes in instructional quality between the first and second TCI sessions, paired t-tests were conducted for each perspective and dimension. The learning process of undergraduate physiotherapy students was examined using grades from the written examination and the practical OSCE assessment at the end of the first semester. These grades served as dependent variables in the analysis. In addition to descriptive statistics, a linear regression analysis was conducted to determine whether a statistically significant relationship exists between the independent variables’ quality indicators of instructional practice (Classroom Management, Learning-Conducive Climate and Motivation, Clarity and Structure, and Activation) and the dependent variables (written exam grades and OSCE grades). Pearson correlation coefficients (r) were calculated to assess the strength and direction of bivariate relationships prior to regression modelling. The regression analysis aimed to identify the predictive value of these instructional quality dimensions for student performance outcomes. Assumptions of linearity, normality, and homoscedasticity were checked before interpreting the regression results. The following conclusions can be drawn about the effect size and direction of a regression analysis, where r = ±1 corresponds to a perfect linear relationship, r = 0 corresponds to no linear relationship, r < 0 corresponds to a negative, inverse relationship, and r > 0 corresponds to a positive relationship. Statistical significance was set at P < .05.
Visual interpretation of the results was conducted using EMU (Excel®), which generated comparative graphs. Scores from the first TCI session served as baseline values for comparison with the second session. Statistical analyses were performed using IBM SPSS Statistics Version 22.0 (IBM Corp., Armonk, NY, USA).
Ethics
The study complied with Swiss legislation and the principles of the Declaration of Helsinki. As the research involved a voluntary, non-interventional survey using fully anonymized data and entailed no foreseeable risks for participants, it did not fall under the scope of the Swiss Human Research Act (HRA; Article 2, paragraph 1). Consequently, no approval or review by the Cantonal Ethics Committee of Bern was required.
All participants received written information about the study and provided informed consent prior to participation.
Results
Participants
Data from the same cohort of 44 undergraduate physiotherapy students were collected at the first examination (Phase 2) and again at the second examination (Phase 4). The mean age of the volunteering students was 22.3 years (SD 2.3).
Primary Outcome
On both TCI days, 44 out of 53 students completed the DTF questionnaire. The students’ attrition rate was 17% and adherence was 83%. Table 2 represents the students’ acceptance outcome results. Missing values after three days after the last TCI session was less than 5%. The lecturer was able to prepare the second TCI based on the analysis of the first TCI with DTF analysis within the seven-day time frame (Table 2).
Multiple Regression Analysis at Time T0 for OSCE Grades and Teaching Characteristic Item 9.

Abbreviation: OSCE, objective structured clinical examination. *p < .05.
Secondary Outcome
Instructional Quality
The first three columns in Figure 2a and b represent the scores on the different items from different perspectives (i.e., student, course instructor, external observer). The last two columns (Measurements 1 and 2) show the same scores but of different perspectives in just one graph.
The quality dimension CM showed values ranging from 2.5 to 4 across all items from the studentś perspective, while those values ranged from 2 to 4 across all items from the perspective of the higher education lecturer and observer. From the studentś perspective, no important changes were observed between the two measurement points. From the perspectives of the higher education teacher and observer, item 4 (‘students obviously knew what they should do at all times’) was reduced by 2 category units at the second measurement point. The deviation between the students’ perspectives and teachers’ perspectives was 1 category unit.
Regarding the quality dimension CL, the item scores from a student's perspective ranged from 3 to 4, and the scores were very similar at the two measurement points. From the perspective of the course instructor and external observer, these values ranged from 2 to 4, with both reporting an improvement of one category unit (from 2 to 3) on item 7 (‘I was kind to the students’) between the first and second measurement points. This improvement was confirmed by the students’ perspective, who reported an improvement on this item from 3 to about 3.3. The quality dimension ST indicated that the values from the students’ perspective ranged from 2.5 to 3.5. From the viewpoint of the course instructor and external observer, these values ranged from 3 to 4. Again, from the students’ perspective, the score values remained quite similar at both time points. The external observer noted an improvement over the ten-day period for 3 out of 5 items (all increasing from 3 to 4), but the course instructor reported improvement only in item 16 (‘Students clearly knew what they were learning in this lesson’) (from 3 to 4). The deviation between the students’ perspective and that of both teachers for this latter item 16 at the second measurement point was approximately 1.3 category units (2.7 compared to 4 and 4 respectively).
From students’ perspectives, score values for the quality dimension activation ranged from 1.3 to 2.5. Aside from items 21 and 22, scores at the second measurement point shifted slightly to the right on the graph. From the views of both higher education teachers, the values ranged from 1 to 2 (for items 17 to 21), but for item 22, they ranged from 3 to 4.
From both the course instructor and external observer's perspective score values decreased over the ten-day period (from 2 to 1) for most items, but not for item 22 which improved from 3 to 4. For item 19 (‘Students worked on tasks in groups’) students’ score value (neutral score = 2.5) deviated from both the course instructor and external observeŕs score value with 1.5 category units (2.5 vs 1 and 1 respectively) at the second measurement point. For item 22 (‘Students were concentrated during the whole lesson’), students’ score value (neutral score = 2.5) deviated from course instructor and external observeŕs score value with 1.5 category units (2.5 vs 4 and 4, respectively) at the second measurement point.
From students’ perspectives, score values for the quality dimension activation ranged from 1.3 to 2.5. Aside from items 21 and 22, scores at the second measurement point shifted slightly to the right on the graph. From the views of both higher education teachers, the values ranged from 1 to 2 (for items 17 to 21), but for item 22, they ranged from 3 to 4. There was a clear deviation for item 25 (‘Students felt comfortable in this lesson’) between the students’ score and the one from the course instructor and external observer at time point 1 (3 vs 2 and 2 respectively) and at time point 2 (3 vs 4 and 4 respectively). Item 27 (‘The instruction was appropriate with regard to the heterogeneous learning abilities of the students’) was inversely scored by the course instructor and external observer when moving from measurement point 1 (4 vs 3 respectively) to 2 (3 vs 4 respectively).
Secondary Outcome
Assessing a Possible Effect Size of DTF on the Learning Process of Undergraduate Physiotherapy Students
No differences were found between the first and second measurements in terms of teaching quality. The regression analysis conducted in this feasibility study included written test question grades and OSCE exam grades as dependent variables, and all five teaching quality dimensions as independent variables (Supplementary Tables 1-4). Only statistically significant results are reported.
Table 2 presents the evaluation at time point T0 for OSCE grades. The adjusted R2- value for the dimension Learning-Promoting Climate & Motivation is 0.124, indicating that the model explains 12.4% of the variance in OSCE performance. According to Cohen, 22 this represents a medium effect size. The F-statistic for this model is 0.118, supporting the interpretation of a modest but meaningful relationship between this teaching characteristic and practical exam performance.
The beta values for item 9 are standardized coefficients, which allow for easy comparison across variables. Beta weights represent changes in standard deviations: if item 9 increases by one standard deviation, OSCE grades increase by 0.038 standard deviations. Beta values typically range between −1 and +1, with larger absolute values indicating stronger relationships. In this case, the beta value is moderate. The significance level for item 10 is 0.029, which is below the 0.05 threshold, suggesting a statistically significant linear relationship between item 9 and OSCE grades. Table 3 demonstrates a linear correlation between item 13 at time T1 and multiple-choice grades. The adjusted R2 value for clarity and structure is .075, indicating a small effect size.
Multiple Regression Analysis at Time T1 for Multiple-Choice Grades and Teaching Characteristic Item 13.

At T1, the linear correlations for OSCE grades are presented in Table 4 for items 8 and 21. The adjusted R2 values are 0.014 for learning-promoting climate & motivation and 0.086 for activation and promotion, both indicating small effect sizes. The beta coefficients for items 8 and 21 fall within the moderate range.
Multiple Regression Analysis at Time T1 for OSCE Grades and Teaching Characteristics.
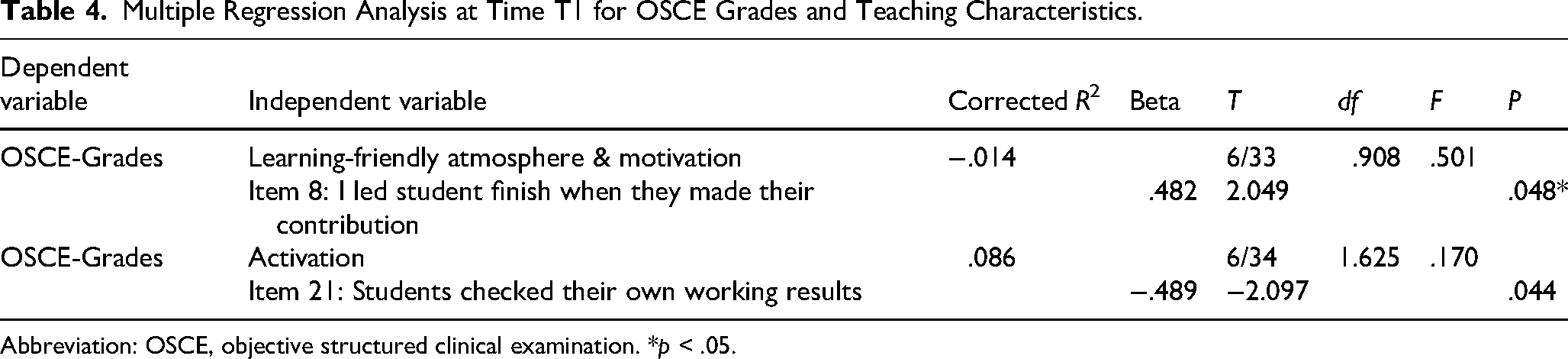
Abbreviation: OSCE, objective structured clinical examination. *p < .05.
Discussion
This feasibility study examined whether the DTF diagnostic feedback tool could be integrated into undergraduate physiotherapy education at BFH-SHP and whether short-term changes in teaching quality and learning processes could be observed within a ten-day cycle. The study objectives were aligned with the Bernese Cantonal Government's mandate for BFH (2017-2020), which prioritizes research-based, practice-oriented programs and systematic quality enhancement in teaching (Bern, 2016). Within this institutional framework, three areas guided the research design: (1) feasibility, (2) instructional development, and (3) learning outcomes.
The primary aim was to assess whether DTF could be implemented within a ten-day cycle, while secondary aims focused on its potential to foster instructional improvement and reflect learning progress.
Peer observation, based on classroom visitation, are considered to be indicators of effective teaching, and hence a criterion for validating SET.23,24 Peer ratings were not related to student ratings, suggesting that peer ratings may not be indicators of effective teaching. 25 This present study demonstrated the difference between students and observers and lecturers. Ward 26 pointed out methodological problems with the survey of peer evaluations. The presence of a colleague in the classroom influences the teacher's performance and threatens the procedure's external validity. In order to minimize these issues, periodic peer evaluations should be conducted.
Feasibility was demonstrated in terms of implementation; however, student participation and adherence were below predefined targets. The attrition rate of 17% exceeded the 5% threshold, and student responsiveness on both evaluation days was 80%, below the targeted 90%. Prior literature suggests that students often endorse the value of evaluating teaching yet doubt that their feedback leads to meaningful change, which may reduce engagement. 27 This attitude likely contributed to the lower-than-expected responsiveness and signals a need to clarify the formative purpose of feedback and to show visible instructional adaptations after feedback cycles. Such perceptions can bias the quality and utility of feedback tools 28 and should be addressed through communication strategies and integration of feedback activities into course requirements.
The study contributes to longstanding debates on the relationship between peer observation, student evaluations, and teaching effectiveness. While earlier work has treated peer observation as an indicator of teaching quality and a criterion for validating student evaluations,23,24 other studies have found weak or no relationships between peer and student ratings. 25 Our findings, discrepancies between the perceptions of students, course instructor, and external observers are consistent with reports of methodological limitations in peer evaluation, including observer effects and compromised external validity when a colleague is present in the classroom. 26 To mitigate these risks and improve reliability, periodic peer evaluations, adequate observer training, and multiple observations per instructor are recommended. 29
The second aim, short-term instructional development, was only partly supported. Across both measurement points, DTF evaluations revealed notable discrepancies between students, lecturers, and observers. Students reported slight improvements in activation, whereas lecturer and observer ratings declined in several dimensions, underscoring the subjective nature of instructional quality assessments. 30 These divergences likely reflect contextual and perceptual differences among stakeholder groups23,26 and highlight the need for structured reflection sessions that align expectations, make criteria explicit, and support the adoption of LOI principles.
The third aim, changes in learning processes, was not supported. Regression analyses revealed only small to moderate associations between teaching dimensions and OSCE performance (adjusted R2-values between 0.014 and 0.124), suggesting limited predictive power. While correlations allow interpretation, they do not establish causality. Future studies should supplement questionnaires with focused knowledge assessments and utilize cluster-randomized designs with control groups to enhance validity and enable more reliable comparisons. Although rarely used in educational research, 31 randomized controlled trials remain the gold standard for establishing causal relationships.
Intervention Fidelity and Active Engagement
Although Phase 4 confirmed that the revised learning objectives and didactic strategies were implemented, the paper offers only limited information about the specific nature and extent of these modifications
Feedback from the first session suggested that excessive content and an unsuitable didactic approach restricted opportunities for active engagement. To address this issue, the lecturer reportedly reduced objectives and created more time for interaction; however, the extent and consistency of these adaptations remain unclear. Without systematic fidelity reporting, such as structured self-reports or observation protocols, it is difficult to attribute observed differences to DTF feedback rather than contextual factors. 32 Evidence from health professions education underscores that active learning requires time and space for processing rather than passive reception. Effective strategies include Think-Pair-Share, 33 Problem-Based Learning,34,35 Case-Based Learning. 36 Peer Instruction, 37 and Flipped Classroom approaches. 38 Simulation-based learning and structured reflection further enhance engagement and self-regulation.39,40 Future studies should combine fidelity tracking with these activation strategies to clarify the mechanism linking feedback, instructional adaptation, and learning outcomes.
Strengths and Limitations
This present feasibility study offers actionable insights for educators and curriculum developers. First, it seems feasible to integrate multi-perspective feedback tools like DTF into undergraduate physiotherapy education. However, implementation may require strategies to improve student engagement and clarify the formative purpose of feedback. Secondly, discrepancies between perspectives emphasize the need for structured dialogue and collaborative reflection to align expectations. Thirdly, institutional support for iterative feedback cycles and observer training is vital to improve reliability and impact. Lastly, integrating motivational strategies and barrier management into implementation plans could boost adherence and acceptance.
There are, however, also several limitations that may constrain interpretation of the results of this study. The study involved a single lecturer, two sessions, and one cohort, limiting generalizability. Potential biases related to expected grades, gender, and cultural factors may have influenced ratings. Additionally, the observer conducted fewer visits than recommended for reliable peer evaluation, 29 and inter-rater reliability was not established.
Implications for Practice: The findings of this feasibility study yield actionable recommendations for educators and curriculum developers seeking to integrate diagnostic feedback tools into health professions education:
Clarify the Formative Purpose of Feedback: Explicitly communicate how student feedback informs instructional improvement and demonstrate visible changes after each cycle to enhance trust and engagement. 27
Increase Student Engagement in Feedback Processes: Link feedback participation to reflective assignments or portfolio tasks, and explain its impact on course design and assessment alignment to improve responsiveness and reduce attrition. 41
Facilitate Structured Reflection Sessions: Convene short, collaborative debriefs among students, lecturers, and observers to reconcile perceptual discrepancies, align expectations, and advance LOI.23,26
Combine Feedback with Active Learning Strategies: Embed proven activation methods, for example, Think-Pair-Share, 33 Case-Based Learning, 36 Peer Instruction, 37 and simulation-based activities 40 to strengthen the link between instructional adaptation and learning outcomes.
Ensure Institutional Support for Iterative Feedback Cycles: Provide observer training, allocate time and resources for repeated cycles, and monitor fidelity through structured self-reports or observation protocols to improve reliability and impact.29,32
Manage Barriers Proactively: Reduce excessive content to create time for interaction, use digital tools for feedback collection and reporting, and address logistical constraints (timing, workload) to improve adherence and acceptance,.28,35
Collectively, these recommendations offer a pragmatic framework for embedding DTF into physiotherapy education, while addressing common challenges related to engagement, reliability, and instructional impact.
Implications for Future Research
Future research should employ larger samples, multiple lecturers, and mixed-method designs to triangulate quantitative and qualitative data. Enhancing observer training and integrating feedback into structured reflection sessions could strengthen the tool's formative potential.
Conclusions
In this limited sample of undergraduate physiotherapy students at BFH-SHP, this feasibility study demonstrates that DTF is feasible for capturing diverse perceptions of teaching quality and for supporting reflective practice. However, its effect on learning outcomes remains inconclusive. Based on these findings, we recommend integrating DTF into regular teaching cycles as a formative feedback tool combined with structured, multi-perspective reflection sessions and explicit instructional adaptation plans. Implementing DTF within iterative feedback loops, supported by observer training and alignment with active learning strategies, may strengthen its impact on instructional quality and learner engagement. Future research should employ larger and randomized study designs, combined with complementary assessment strategies, to rigorously evaluate effectiveness and to identify essential components for improving teaching quality in health professions education.
Supplemental Material
sj-docx-1-mde-10.1177_23821205261437325 - Supplemental material for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education
Supplemental material, sj-docx-1-mde-10.1177_23821205261437325 for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education by Slavko Rogan, Ron Clijsen and Jan Taeymans in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205261437325 - Supplemental material for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education
Supplemental material, sj-docx-2-mde-10.1177_23821205261437325 for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education by Slavko Rogan, Ron Clijsen and Jan Taeymans in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-3-mde-10.1177_23821205261437325 - Supplemental material for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education
Supplemental material, sj-pdf-3-mde-10.1177_23821205261437325 for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education by Slavko Rogan, Ron Clijsen and Jan Taeymans in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-4-mde-10.1177_23821205261437325 - Supplemental material for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education
Supplemental material, sj-pdf-4-mde-10.1177_23821205261437325 for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education by Slavko Rogan, Ron Clijsen and Jan Taeymans in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-5-mde-10.1177_23821205261437325 - Supplemental material for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education
Supplemental material, sj-pdf-5-mde-10.1177_23821205261437325 for Feasibility of a Multi-Perspective Diagnostic Teaching Feedback Tool in Undergraduate Physiotherapy Education by Slavko Rogan, Ron Clijsen and Jan Taeymans in Journal of Medical Education and Curricular Development
Footnotes
Author Contributions
S.R. and J.T. developed the study design, S.R. conducted the study, the data were analyzed by S.R., R.C. and J.T. Figure 1 is created by S.R., ![]() and b are created by R.C. S.R wrote the manuscript text, R.C and J.T. reviewed the text.
and b are created by R.C. S.R wrote the manuscript text, R.C and J.T. reviewed the text.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.