
Abstract
Objectives
Successful implementation of diversity, equity, and inclusion (DEI) initiatives requires understanding the perspectives of diverse student populations. This study explored how graduate health and public health professionals perceive DEI and their implementation barriers and facilitators.
Methods
This qualitative freelisting study was conducted from June to August 2024 at a single urban academic institution in Pennsylvania. Eligible participants were current or recent graduate students in health or public health programs. Participants engaged in structured freelisting exercises, where they listed words, themes, and reflections related to 5 different DEI domains. Responses were coded by multiple researchers, and the Smith Salience Index was applied to quantify the importance of themes across participants.
Results
Thirty participants completed the study. The most salient themes were “inclusivity and representation” and “diverse and receptive leadership” as essential components of DEI. Participants expressed both positive and negative experiences. White and man-identifying participants more often emphasized positive aspects, while older, woman-identifying, and participants from racial and ethnic minority backgrounds highlighted the need for institutional “commitment, accountability, and buy-in.” The most frequently cited barrier to DEI was “lack of adequate funding and resources.”
Conclusion
Graduate health and public health professionals emphasized the importance of representation and leadership diversity in fostering inclusive environments. Institutional investment in DEI—particularly through recruitment, retention, leadership representation, and sustained funding—is critical to cultivating a workforce prepared to advance health equity for the communities they serve. Differences in perceptions by race, gender, and age underscore the need for tailored approaches to DEI implementation.
Introduction
Diversity, equity, and inclusion (DEI) are increasingly recognized as fundamental components of higher education and have shaped educational experiences of students. The term DEI originated during the American Civil Rights movement of the 1960s with the goal of expanding access to education and supporting diverse learning environments that benefit everyone.1,2 DEI in higher education encompass a broad range of policies and practices to create and sustain inclusive, equitable, and nondiscriminatory campus environments. 3 These programs aim to improve access and belonging of faculty and staff across multiple dimensions of identity (eg, race, ethnicity, gender, citizenship, gender identity, socioeconomic status, disability, sexual orientation, veteran status), based on evidence that diverse learning environments enhance educational outcomes for all. 3
DEI has been introduced into a range of disciplines and industries, from corporate culture to healthcare. The latter holds particular significance. A workforce that represents the demographics and language of the populations it serves improves quality of care and reduces inequities. For instance, racial and ethnic concordance between patients and clinicians has been linked to stronger therapeutic relationships and greater trust, while concordance in language improves treatment adherence and communication.4–9 Increased representation of Black primary care physicians at the population level is associated with lower all-cause Black mortality and higher life expectancy. 10
Because improving representation in clinical practice is rooted in who enters and succeeds within health professions education, DEI is a core mission of graduate medical and public health programs, as both a matter of equity on campus and as a driver of population-health outcomes and community well-being. However, DEI efforts remain embedded within predominantly white-dominant hegemonic institutions limiting its impact on traditional power structures and hierarchies. 11 Following the murder of George Floyd in May 2020 and U.S. Supreme Court ruling in Students for Fair Admission v. Harvard, which stated that “race-based admissions systems … fail to comply with the Equal Protection Clause” of the Fourteenth Amendment and Title VI of the Civil Rights Act of 1964, DEI was elevated to mainstream public consciousness, catalyzing national conversations around the role of DEI within institutions of power.12,13
Because DEI initiatives differ widely in their goals, design, and evaluation metrics, evidence regarding their effectiveness is mixed. However, individual programs with well-defined objectives and strong implementation have been associated with improved academic and professional outcomes, and may help reduce imposter syndrome, isolation, depression, and burnout, particularly among students from minority backgrounds.14,15 Resultantly, multiple academic organizations, including the Liaison Committee on Medical Education, American Association of Colleges and Universities, and the Council on Education for Public Health, recommend implementing programs that promote DEI.16–18 Despite ongoing efforts to promote inclusivity and fairness in academia, since 2023 attacks on DEI have escalated: state and federal policymakers have instituted policies, regulations, and investigations that have eliminated DEI programming altogether, cut or threatened to cut funding for institutions that do not comply with federal executive orders, and pursued investigations and legal actions that jeopardize the benefits these programs offer and all individuals they serve.19–24
Research exploring DEI in higher education highlights both the progress made and the challenges that remain. 25 Findings from a 2019 qualitative meta-synthesis emphasized the successful implementation of DEI initiatives, but it highlighted the need to address systemic barriers and promote inclusive practices throughout the academic journey. 26 Further, while exposure to DEI principles is increasingly common in graduate health and public health education, the depth of understanding and application of these efforts varies widely among students, suggesting the need for consistent and robust support to help students internalize the value of DEI.27–30 In general, experiences and perspectives are varied and highlight both successful and insufficient integration of DEI principles.31,32 While student study participants felt that diversity initiatives were effective, others viewed them as tokenistic, indicating a need for institutional authenticity.
Despite recent political contexts, the mission and values related to DEI must remain a priority for all academic institutions, as these efforts benefit the entirety of the campus community. While the need may be more urgent in institutions serving a larger proportion of students from racial and ethnic minority backgrounds, sustained commitment is essential everywhere. However, gaps remain in understanding perspectives on DEI at the graduate health professional level. Discerning graduate professional (physicians and nonphysicians) needs and interests can provide a better understanding of the cultural climate and promote engagement and innovation. 33 Graduate health and public health professionals occupy a distinct position. They deliver clinical care, conduct research, engage in quality improvement, and assume leadership roles within healthcare systems and academic institutions. As such, their perspectives on DEI are not only shaped by advanced professional training, but also directly inform how DEI principles are operationalized in patient care, research design, institutional policy, and educational leadership. Understanding DEI perspectives within this population is critical because their decisions have downstream effects on patient outcomes, workforce diversity, mentorship structures, and the inclusivity and generalizability of health research. Prior work has largely focused on undergraduate or preprofessional trainees or has evaluated discrete DEI initiatives, leaving limited insight into how more advanced trainees conceptualize DEI, perceive its relevance to their professional roles, and identify barriers and facilitators to its implementation. Therefore, we conducted a qualitative freelisting study of graduate health and public health professionals at a single academic institution in Philadelphia to explore attitudes toward DEI and to identify perceived barriers and facilitators to its implementation.
Methods
We followed the Standards for Reporting Qualitative Research reporting guidelines provided by the EQUATOR Network (Supplemental Material).
Study design
Freelisting is a standardized qualitative technique where participants list responses to specific questions about a topic to determine relative importance of terms and themes.34,35 In freelisting, participants are asked to respond to a question by listing all words and comments that come to mind. The goal is to elicit spontaneous and authentic responses to questions to provide a greater understanding of how individuals prioritize and emphasize concepts. We chose freelisting as we sought to capture participant perceptions and ideas without a priori checklists or interviewer prompting. Furthermore, freelisting efficiently identifies the boundaries and definition of a conceptual domain from the perspective of a target population. Lastly, freelisting allows for the rapid aggregation of qualitative data in a format that allows for effective comparisons across subgroups within the population.
In this study, freelisting was conducted to understand how graduate-level students in health and public health professions conceptualize DEI and perceive barriers and facilitators to DEI integration in academia. First, an in-depth freelisting interview guide was developed consisting of 5 freelisting questions and 6 demographic questions (race and ethnicity, age, sex assigned at birth, gender, and occupation).
Participants and recruitment
A sample of 30 study participants was recruited, above the minimum of 20 required to achieve thematic saturation.34,35 Current or recent students (within the past 3 years) enrolled in a health professional graduate program at the school of medicine within our institution were eligible for participation. Participants were recruited through group emails to graduate programs and via snowball sampling from June to July 2024. Purposive sampling was performed to obtain responses from students of diverse programs and demographics. All participants were enrolled in graduate programs at the University of Pennsylvania that are accredited through the Master and Certificate Pogram (MaC). These programs did not have specific DEI training requirements but did have policies regarding their commitment to diversity and inclusion. Participants were not required to have prior experience in DEI program to participate in the study.
Data collection
Our research team represents a diversity of racial, ethnic, gender, and professional identities and experiences within health professions education. These identities shaped how we approached the research questions, engaged with participants’ narratives, and interpreted emergent themes. Team members who identify as Asian (VA, WL, JH) brought firsthand experiences related to the model minority stereotype, proximity to structural privilege, and ongoing critical reflection on how these dynamics influence understanding of DEI discourse. Team members identifying as Latina/o/x or Black and Ethiopian-Jewish (LMG, MM, LS) contributed perspectives grounded in being underrepresented in medicine and having participated in and designed DEI initiatives intended to reduce barriers in educational and clinical environments. Most members have engaged with DEI programming either as recipients, facilitators, or both, which informed the types of probing questions asked during data collection and our attention to variation in perceived DEI quality. Most authors were current trainees in graduate health or public health degree programs (LMG, VA, JH, LS, WL, MM), which provided proximity and sensitivity to participant experiences. Some participants knew interviewers as they were classmates. However, none were graduates of the specific programs represented in this study, minimizing risk of direct role-conflict in interpretation. Collectively, these perspectives helped us remain attentive to power, representation, and equity across study design, analysis, and reporting. Authors LMG, VA, JH, LS, WL, and MM performed the freelisting interviews. Authors LMG, VA, and JH subsequently cleaned interview responses.
Participants were interviewed and audio-recorded via an approved virtual platform (Microsoft Teams™) after obtaining informed consent and were encouraged to be in a private setting. Study participants were asked freelisting questions related to their experiences with barriers and facilitators to achieving DEI in the academic setting. The Microsoft Teams transcription function was used to transcribe the interview audio. Transcripts were cleaned for clarity and typographical errors and then coded as described below.
Question development
Consistent with established freelisting methodology, we designed broad, open-ended questions intended to elicit comprehensive lists of terms reflecting students’ cognitive associations with DEI and campus inclusion. Two team members (SK and OC) drafted the initial questions based on the study aims. The full research team reviewed the questions to assess conceptual alignment, clarity, and cultural responsiveness. We conducted a pilot of the freelist questions with 6 students and iteratively refined phrasing to enhance comprehension and ensure that elicited responses reflected the intended domains. These participants were not included in the full sample as some students were a part of the study team. The final wording of questions was determined by consensus.
Coding strategy
Data were managed on an institutional secure password-protected cloud-based collaboration network and were analyzed between June and August 2024. Lists from each participant were compiled and numbered according to response order. Individual lists were compiled into 1 document for each question for data cleaning and analysis.
Three researchers were involved in all aspects of data cleaning and analysis (LMG, VA, and JH). All researchers involved in cleaning were clinicians and health services researchers. In the first round of cleaning, spelling and grammatical errors were corrected. Singular/plural forms or modified parts of speech of the same word were combined (ie, “resource” and “resources,” “optimism” and “optimistic”). In the second round, synonyms were combined (ie, “perspectives” and “viewpoints”). In the third round, words with similar themes were derived from the data without a priori set of codes by researchers. Discrepancies or disagreements were discussed among the entire research team until consensus was met and codes were condensed to less than 25 per question. A fourth investigator (SK, a health services researcher with deep expertise in freelisting and qualitative methods) reviewed all grouped terms and provided approval for finalized analysis.
Data analysis
Freelists for each question were analyzed using R Studio Version 4.3.0. The AnthroTools R package was used to generate frequency and salience scores for codes corresponding to each question separately. 36 Our primary outcome was Smith's S index (SSI), a type of salience index. Smith's S was used to calculate salience and considers both frequency of an item across all participants’ responses as well as its rank order.34–36 SSI is calculated by the summation of a response item's percentile rank divided by the total number of participants lists. A higher value indicates a theme or concept is prominent among the research participants. Scree plots were used to visualize the salience scores for items for each question by placing the SSI on the X-axis and the items on the Y-axis. 34
Subgroup analysis
We conducted subgroup analyses based on age, gender, and race. To provide comparative results while preserving anonymity of study participants, especially from racial and ethnic minority backgrounds, we aggregated each demographic characteristic into 2 subgroups (Age: at or below median 23-32 years, above median 33-40 years; Gender: Men, Women; Race: white, racial and ethnic minority).
Ethical considerations
This study was reviewed and approved by the institutional review board (IRB Approval No. 855949) of the University of Pennsylvania and determined that the proposal met eligibility criteria for IRB review exemption.
Consent to participate
All participants provided verbal informed consent to participate in this study. The requirement for written consent was waived by the IRB to facilitate conducting primary data collection by Microsoft Teams™.
Results
A total of 30 interviewees participated in the study, with a median age of 32 years (Interquartile Range = 2.75). Among them, 17 interviewees (57.5%) were 32 years old or younger, while 13 interviewees (43.3%) were older than 32 years, with ages ranging from 23 to 40 years. In terms of gender identity, 22 (73.3%) interviewees identified as women, and 1 interviewee (3.3%) identified as nonbinary. Over one-third of the interviewees identified as white (n = 12, 40.0%), followed by Asian (n = 8, 26.7%) and Black (n = 5, 20.0%). Most interviewees were physicians, comprising 21 individuals (70.0%). Four interviewees (13.3%) reported as nurses or researchers. Additional details are provided in Table 1. Most salient responses are shown in Table 2. Subgroup analyses are shown in Table 3.
Demographic Characteristics of Study Participants.

Abbreviations: SD, standard deviation; IQR, interquartile range.
aDoes not add up to 30 because individuals may identify with one or more racial background.
Responses to Freelist Interview Questions by All Participants.
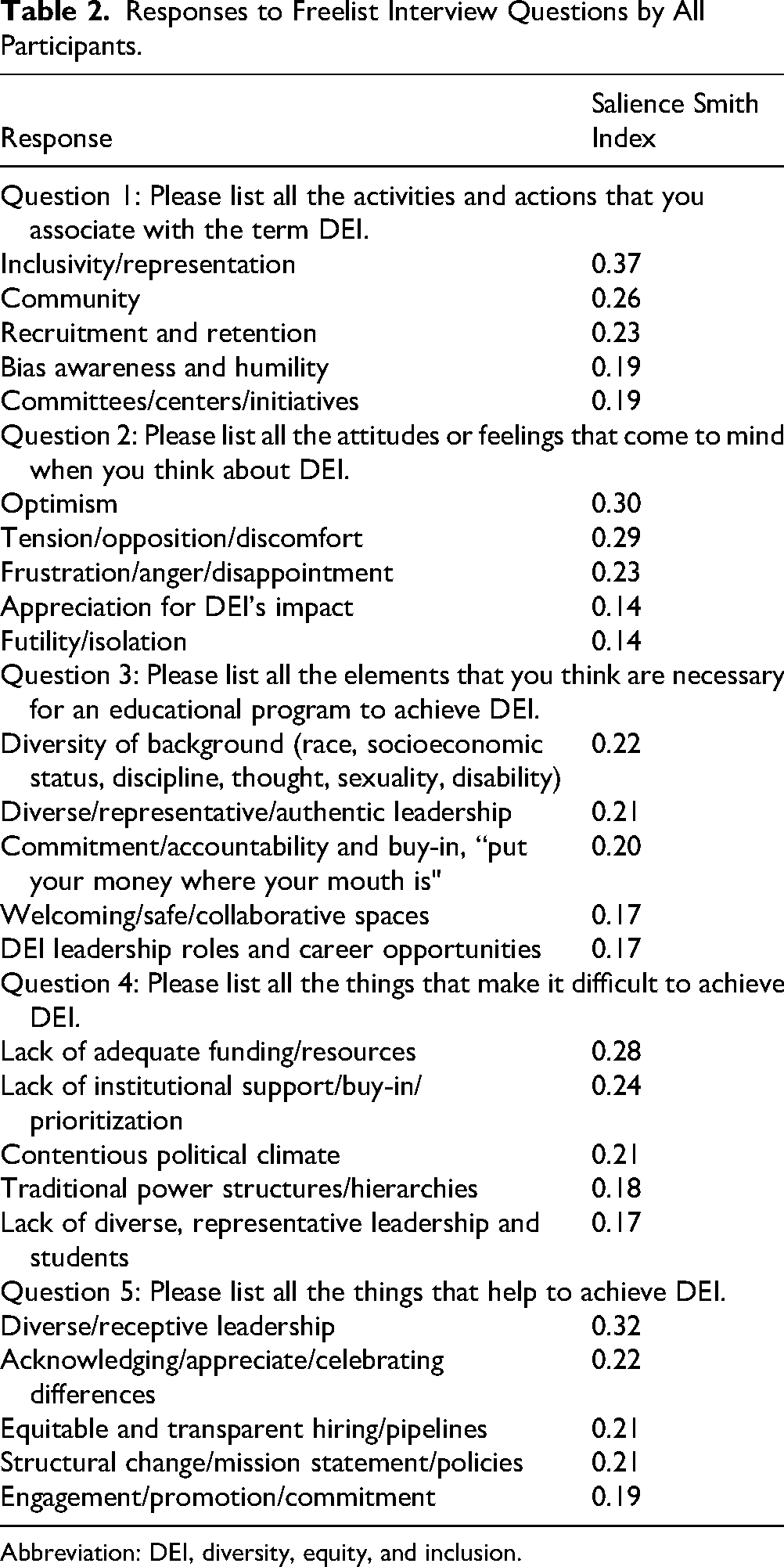
Abbreviation: DEI, diversity, equity, and inclusion.
Responses to Freelist Interview Questions by Age, Gender, and Race.
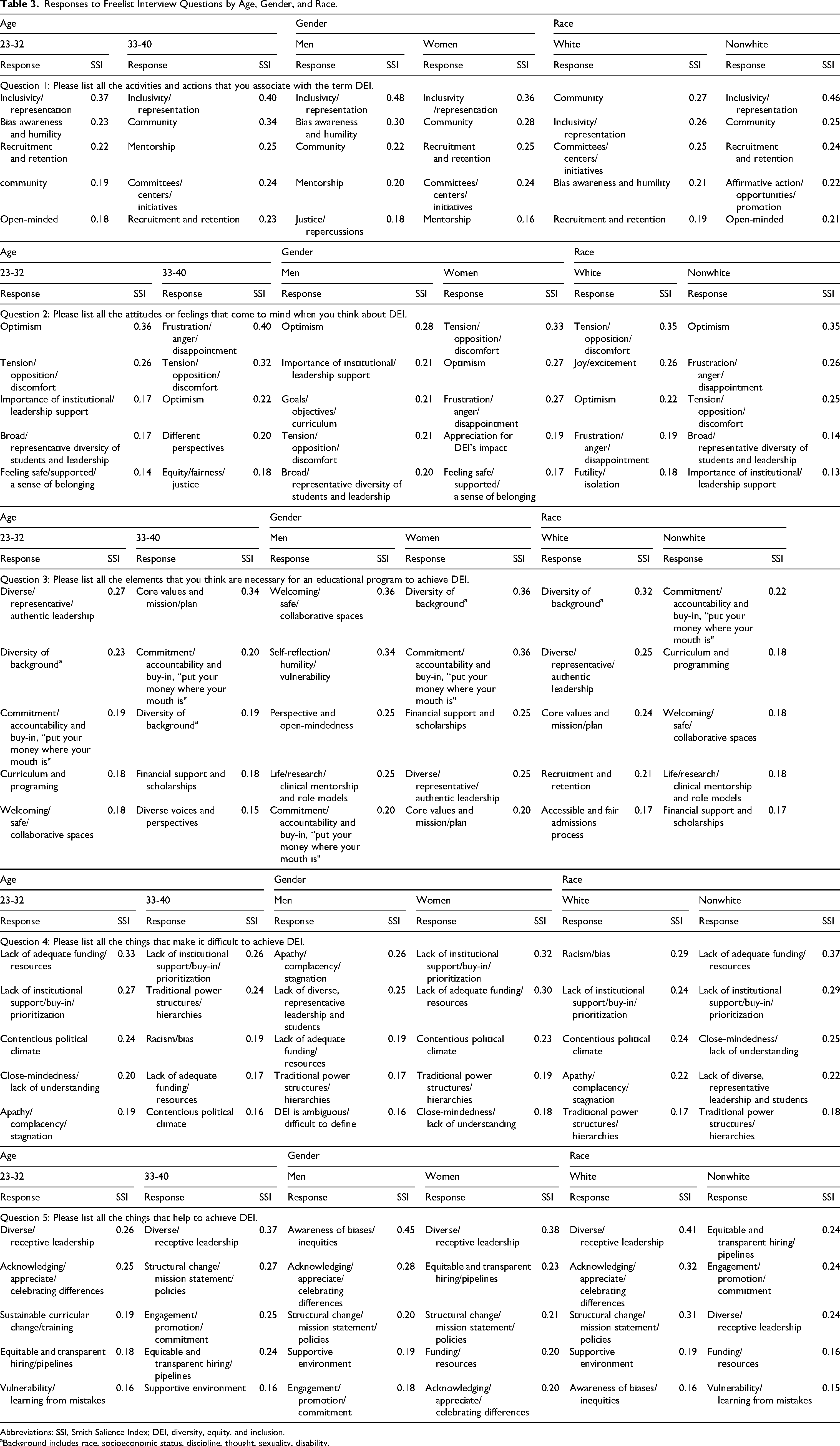
Abbreviations: SSI, Smith Salience Index; DEI, diversity, equity, and inclusion.
aBackground includes race, socioeconomic status, discipline, thought, sexuality, disability.
Question 1: Please list all the activities and actions that you associate with the term “DEI”
The most salient activities and actions associated with DEI included “inclusivity and representation,” “community,” and “recruitment and retention.” Notably, younger participants attributed greater salience to individual actions such as “bias awareness and humility” and “open-mindedness;” whereas older participants highlighted institution-led activities such as “mentorship” and the development of “committees/centers/initiatives.” A representative scree plot is provided in Figure 1.

Representative scree plot for freelist interview question 1: Please list all the attitudes or feelings that come to mind when you think about “diversity, equity, and inclusion.”
Question 2. Please list all the attitudes or feelings that come to mind when you think about “DEI”
The most salient attitudes and feelings towards DEI included “optimistic,” “tension/opposition/discomfort,” and “frustration/anger/disappointment.” Relative to women and participants from racial and ethnic minority backgrounds who echoed sentiments of frustration, white and man-identifying participants attributed more salience to “joy/excitement” and “optimism.”
Question 3: Please list all the elements that you think are necessary for an educational program to achieve, “DEI”
Participants identified “diversity of background” and “diverse/representative/authentic leadership” as critical to the success of DEI initiatives. A need for “commitment/accountability and buy-in” was more salient among older, woman-identifying, and racial and ethnic minority participants compared to younger, man-identifying, white counterparts, who focused on internal elements such as “self-reflection/humility/vulnerability” was necessary to achieve DEI.
Question 4: Please list all the things that make it difficult to achieve “DEI”
“Lack of adequate funding/resources” and “lack of institutional support/buy-in/prioritization” were the most salient issues listed across all participants. Students also identified “contentious political climate” and “traditional power structures and hierarchies” as salient issues that make it difficult to achieve DEI. Institutional barriers such as “traditional power structures/hierarchies” were more salient among older, racial and ethnic minority, and women participants compared to younger, white, and man-identifying participants who emphasized individual attitudinal barriers such as “close-mindedness” and “apathy/complacency/stagnation.”
Question 5: Please list all the things that help to achieve “DEI”
Similar to Question 3, individuals emphasized how “diverse and receptive leadership” is the most important to achieving DEI. In addition, “equitable and transparent hiring/pipelines” was identified as an important driver. “Equitable and transparent hiring/pipelines” and “engagement/promotion/commitment” were most salient among racial and ethnic minority participants. Younger and white participants noted individual practices of “acknowledging/appreciating/celebrating differences” and “vulnerability/learning from mistakes” as crucial to success. Lastly, both genders agreed that “structural change/mission statements/policies,” help achieve DEI.
Discussion
In this study, we used freelisting to explore graduate health and public health professional student perspectives on institutional DEI initiatives. We compared responses by self-reported age, gender, race, and ethnicity and identified key themes related to DEI. Participants overwhelmingly stressed the importance of multidimensional diversity and representation within both the student body and leadership personnel. Participants also generally expressed optimism toward DEI; however, some participants, particularly women and racial and ethnic minority individuals, expressed frustration due to the politicization and tension surrounding DEI. Younger, white, and man-identifying participants often emphasized individual-level characteristics for achieving DEI such as “bias awareness” and “open-mindedness.” Furthermore, white participants identified racism and bias as major barriers to DEI, often focusing on individual characteristics (eg, “close-mindedness”) and suggesting individual-level solutions. In contrast, older, racial and ethnic minority, and woman-identifying participants focused on systemic- and institutional-level factors, barriers, and solutions, suggesting that differences in perspectives may be driven by varying levels of experience, knowledge, privilege, and social status. Together, these findings extend existing literature by centering the perspectives of graduate health and public health professionals and elucidating how DEI is conceptualized during a critical period of professional identity formation and emerging leadership. While prior studies have largely examined undergraduate trainees or discrete DEI programs, this study highlights how advanced trainees conceptualize DEI at a stage marked by professional identity formation, growing research expertise, and emerging leadership roles. This population is uniquely positioned to translate DEI principles into clinical practice, research design, program implementation, and institutional leadership.
Importantly, differences in how participants in this study framed DEI suggest meaningful downstream implications. Participants who emphasized individual characteristics and individual-level solutions may be more likely to operationalize DEI through bias awareness in patient encounters or recruitment practices and to support trainings focused primarily on individual behavior change. In contrast, participants who framed DEI in systemic and institutional terms more readily acknowledged the interplay of structural, community, and individual factors shaping health, which may translate into research approaches that share power with communities, programmatic efforts that address structural barriers, and advocacy for institutional accountability. Additionally, while perspectives within this cohort largely mirror broader patterns reported in the literature, this study also highlights identity-based differences that help explain variation in engagement with DEI across training environments.
Participants clearly identified increased multidimensional diversity and representation within student body and leadership as vital to embracing DEI. Multidimensional diversity included race, socioeconomic status, discipline, thought, sexuality, and disability. Statements such as “inclusivity/representation,” “diversity of background,” and “lack of diverse and representative leadership and students,” were most salient across multiple domains highlighting the importance of this concept to students, reflecting an emphasis on creating environments exhibiting these qualities to foster a sense of belongingness. Our findings are consistent with existing literature. Multiple qualitative studies exploring health professionals’ perspectives on DEI programming have highlighted the necessity of increased minority representation to improve mentorship opportunities, sense of belonging, and exposure to varied lived experiences and perspectives.31,37,38 Adequate representation of underrepresented minorities in health professions in leadership through DEI programs is critical to fostering the success of students and early faculty.39–41 Race concordance between students and faculty has also been linked to improved workplace satisfaction and greater educational achievement.40,41
Further, in this study, younger, white, and man-identifying participants more often noted individual level characteristics, such as “bias awareness and humility” and “open-mindedness,” as salient actions or activities associated with DEI. These participants also highlighted individual level barriers of “close-mindedness” and “apathy/complacency/stagnation” and suggested individual level solutions, such as identifying teachable moments and celebrating differences. While important, this may represent a lack of knowledge or acknowledgment of structural barriers and potential unrecognized privilege conferred by existing institutional hierarchies. This may reflect a trend in which individual-centered narratives are used to deflect from structural and institutional reform.31,37,38,42–44 On the other hand, and consistent with prior literature, racial and ethnic minority and women-identifying participants, clearly highlighted lack of institutional buy-in as a barrier to achieving DEI, indicating that DEI may exist in-name-only, and the subsequent necessity of authentic investment and institutional accountability.31,37,38,42,43 Multiple studies have described lack of funding, time, resources, compensation, and institutional endorsement for DEI initiatives leading to ineffectual and often taxing interventions. 45 To counter this, medical societies such as the American Academy of Pediatrics have proposed ways for institutions to integrate DEI into their mission and allow for promotion of faculty involved in these initiatives. 46 Institutions must move away from a “check-box culture” toward authentic and intentional integration of DEI into the fabric of the institution.
Additionally, white participants attributed racism and bias as the most salient barrier to DEI implementation. Recognizing the role that racism and bias play in obstructing DEI efforts at systemic, institutional, and interpersonal levels is essential for nurturing effective allyship among individuals from dominant identities.43,44 Multiple institutions have integrated implicit bias training into their requirements for occupational enrollment; however, the impact of interventions on lasting behavior change that solely stress bias awareness is unconvincing. 47 In fact, most DEI interventions increase knowledge and awareness, though have not been linked to long-term provider behavior change or improved patient outcomes.28–30,42 Our findings may reflect exposure of students with dominant identities to these current institutional practices intended to address racism and bias, rather than an intrinsic knowledge of what is necessary or effective to authentically achieve DEI. As outlined in Public Health Critical Race praxis, developed by Ford and Airhihenbuwa, applying Critical Race Theory to public health requires a form of race consciousness that goes beyond surface-level awareness of bias. 44 Without critical approaches that interrogate power and history, and without attention to structural determinism, defined as the fundamental role of macro-level systems in shaping health, race consciousness alone is ineffective. 44 Aligning with student voice, newer recommendations endorse fostering humility among dominant group identities to address defensive reactions or responses to bias awareness trainings. 47 While limited, trainings focused on behavior change and progress tracking has been cited as more impactful, though these activities were mentioned by only a minority of participants. 48 Graduate-level students in health and public health professions may not have been provided opportunities or are unaware of programs that focus on managing biases and providing individualized feedback. This suggests a need for institutions to move beyond implicit bias training to more effective measures for promoting DEI.
Participants demonstrated conflicting attitudes and feelings toward DEI. Participants identified “optimism” when reflecting on DEI which may reflect an intrinsic desire to further DEI efforts, and an “appreciation for DEI's impact” while acknowledging external threats to its success. Women and racial and ethnic minority participants more often expressed negative emotions or feelings with DEI relating to the ongoing politicization and tension surrounding DEI and its efforts.19–24 This may correspond to disparate experiences of participants—specifically the continued racism and sexism experienced by minoritized groups despite existing DEI efforts and the unchanged and often unacknowledged privilege of white and man-identifying participants.45,49 Since January 2023, over half of states have introduced anti-DEI legislation, totaling 65 bills, with 10 states signing them into law.20,21 Medical societies and academic medical centers have also introduced measures to remove DEI programs from medical education.22,23 Resultantly, the resistance to DEI efforts has left many students feeling frustrated or disappointed, isolated, and as if efforts are futile. Furthermore, the onus of enacting DEI efforts is often placed on individuals from racial and ethnic minority backgrounds rather than institutional leadership. 50 This results in uncompensated and labor-intensive efforts by minoritized students to advocate for DEI amidst structures that intrinsically prevent these efforts from thriving. 50
Our findings suggest that while graduate health professionals broadly endorse DEI, meaningful differences in how DEI is conceptualized, between participants with dominant and minoritized identities, may shape engagement with and receptivity in institutional DEI efforts. DEI strategies that do not explicitly address power, accountability, and institutional responsibility risk being perceived as symbolic. Given the disproportionate representation of white men in healthcare leadership, these distinctions are salient for designing DEI initiatives that resonate across groups and translate into systemic change.
Strengths and Limitations
Methodologically, this study demonstrates freelisting as a flexible and efficient method for rapidly eliciting DEI perceptions across diverse participants. Freelisting allowed participants of the study to prioritize concepts in their own language and subsequently produce data that elicited both shared themes and meaningful subgroup differences. This approach may offer other researchers a scalable tool to assess DEI climate and identify implementation facilitators and barriers amid a rapidly changing sociopolitical context where rapid feedback is essential.
Our study has limitations. First, it was limited to a single academic institution, reducing its generalizability. Second, we recruited a convenience sample that, while diverse, cannot be assumed to be representative of the broader student populations within the participating academic programs and larger academic bodies. It was beyond the scope of this study to analyze and assess the demographic makeup of the graduate programs represented in this sample, we were therefore unable to assess representativeness, which may influence the transferability of our findings. However, relative to published demographics of health services researchers, our sample overrepresented individuals from racial minority groups, women, and Hispanic-identifying participants, suggesting that perspectives from historically underrepresented groups may be more prominently reflected in our findings. 51 Third, we pursued comparisons along race, gender, and age; however, to preserve confidentiality, binary categories were created. As such, nuanced experiences of individuals from different racial, ethnic, and gender diverse backgrounds were not captured in this study, though it will be a direction for future research. Fourth, while maintaining confidentiality was a top priority, we acknowledge that grouping participants into broad categories can create oversimplified representation, which overlooks individual experiences. Fifth, because participants were interviewed by fellow students, responses may have been influenced by social desirability bias, especially on this charged topic.
Nonetheless, our team included a very diverse group of interviewers, which likely increased participants’ trust and comfort during the interview. Further, we used a qualitative technique that allowed us to elicit unimagined attitudes and perspectives that can drive student-centered policy and programming to improve equity and quality in health education. Findings were generated from the perspective of recipients of DEI educational initiatives, which is aligned with evidence demonstrating that inclusive and participatory evaluation of programming promotes engagement and a shared understanding ultimately leading to stronger buy-in and better outcomes. 52
Conclusion
Taken together, our findings highlight the ways in which students differentially conceptualize DEI based on their identities and experiences and highlight the need for program leadership to consider how current structures, curricula, and institutional messaging shape these perceptions. Participants emphasized the importance of authentic institutional investment, opportunities to build cultural humility, and mechanisms that move beyond awareness toward meaningful behavior change. These findings contribute to a growing body of literature calling for intentional, equity-oriented approaches to DEI within graduate health and public health education.
Supplemental Material
sj-docx-1-mde-10.1177_23821205261433426 - Supplemental material for Healthcare Professionals’ Attitudes and Perspectives on Diversity, Equity and Inclusion in an Academic Culture: A Freelisting Study
Supplemental material, sj-docx-1-mde-10.1177_23821205261433426 for Healthcare Professionals’ Attitudes and Perspectives on Diversity, Equity and Inclusion in an Academic Culture: A Freelisting Study by Vivek A. Ashok, Lakeisha Mulugeta-Gordon, Jasmine Hwang, Weilu Song, Melissa Montoya, Luis E. Seija, Omaris Caceres and Shimrit Keddem in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We would like to thank Dr Marilyn Schapira and Dr Jim Guevara for their support on this project and for making suggestions throughout the study.
ORCID iDs
Author Contributions
Dr Shimrit Keddem conceptualized this piece; Drs Mulugeta-Gordon and Ashok managed the project and wrote the initial draft; Ms Caceres managed regulatory approvals and supported recruitment. Drs Mulugeta-Gordon, Ashok, Hwang, Montoya, and Seija, and Mr Song were involved in participant interviews and data management; Drs Mulugeta-Gordon, Ashok, and Hwang conducted coding and analysis; Mr Song and Dr Keddem were provided coding and data visualization support; Dr Keddem critically reviewed and revised the manuscript. All authors have approved the manuscript as submitted and agree to be accountable for all aspects of work.
Role of Funder/Sponsor
The funders had no role in the preparation, review, or approval of the manuscript and decision to submit the manuscript for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Resources and Services Administration, Agency for Healthcare Research and Quality, and American College of Surgeons (Grant Nos. T32HP46118-02, T32HP4611803-00, T32HS026116-07, T32HS26116-06, and Resident Research Scholarship).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study consist of sensitive qualitative interview transcripts. Due to concerns related to participant confidentiality and the sensitive nature of the topics discussed, these data cannot be shared publicly. Researchers with specific inquiries regarding the study may contact the corresponding author for additional information about the data collection process.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.